
Real-World Evidence for Treat-and-Extend Regimen of Ranibizumab Therapy for Macular Oedema Secondary to Branch Retinal Vein Occlusion

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
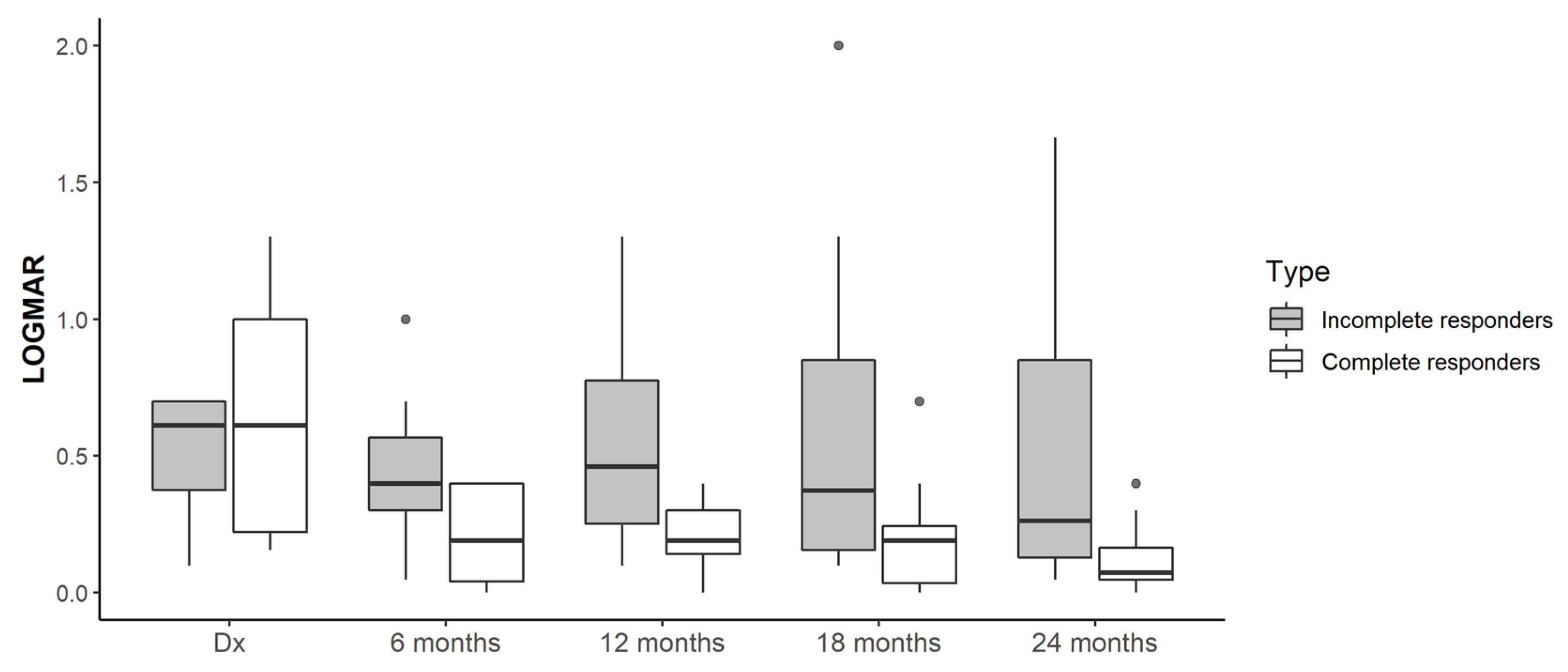
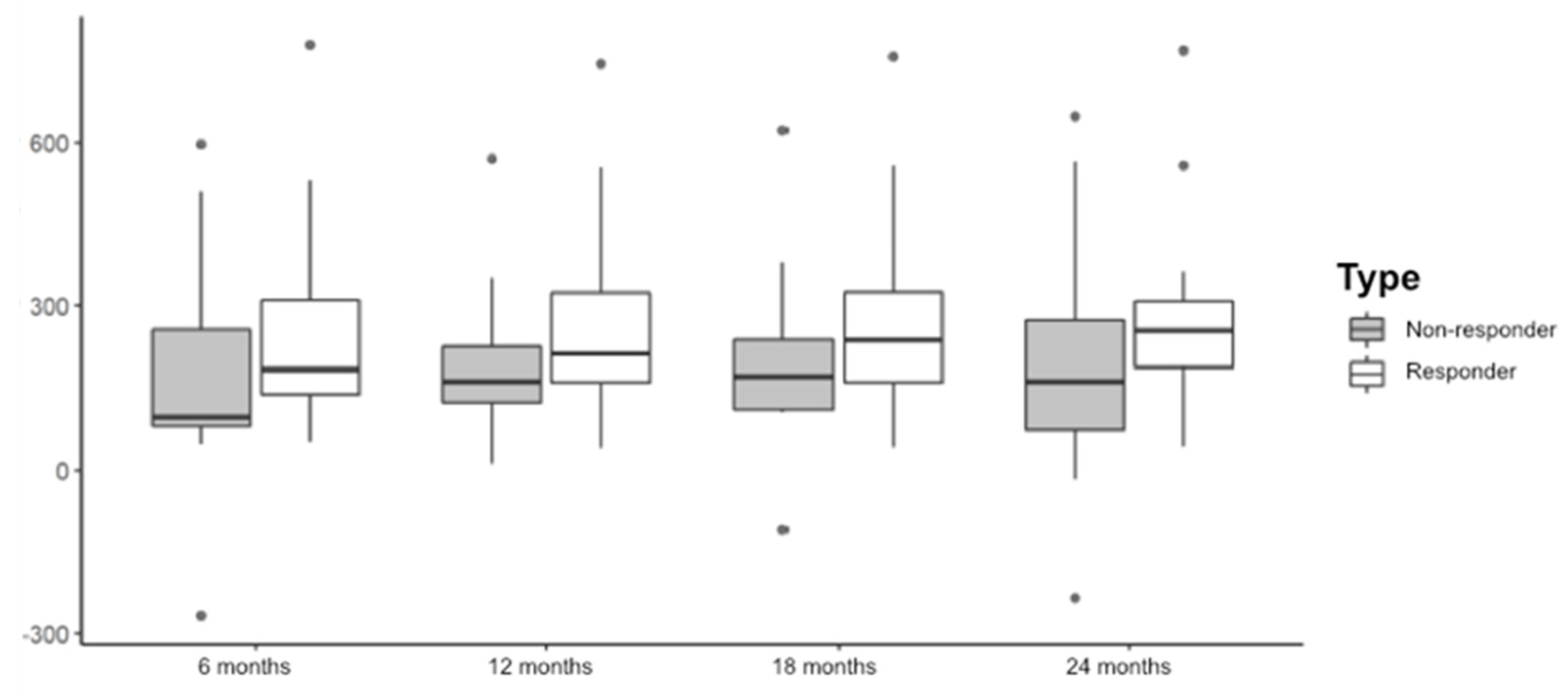
2.2. Treatment Response: BCVA Outcomes and CMT
2.3. Injections of Ranibizumab
2.4. Type of BRVO and Comorbidities
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Patients and Study Design
4.2. Variables to Study
4.3. Treat-and-Extend Regimen (T&E)
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mitchell, P.; Smith, W.; Chang, A. Prevalence and associations of retinal vein occlusion in Australia: The Blue Mountains Eye Study. Arch. Ophthalmol. 1996, 114, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The preva-lence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajor, A.; Pielen, A.; Danzmann, L. Retinaler Venenverschluss—Wann, womit und wie therapieren? Klin. Mon. Augenheilkd. 2017, 234, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.L.; McIntosh, R.L.; Lim, L.; Mitchell, P.; Cheung, N.; Kowalski, J.W.; Nguyen, H.P.; Wang, J.J.; Wong, T.Y. Natural history of branch retinal vein occlusion: An evidence-based systematic review. Ophthalmology 2010, 117, 1094–1101.e5. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.; Chung, C.Y.; Kim, R.Y. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.M.; Kaiser, P.; Michels, M.; Soubrane, G.; Heier, J.S.; Kim, R.Y.; Sy, J.P.; Schneider, S. Ranibizumab versus ver-teporfin for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1432–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prünte, C.; Fajnkuchen, F.; Mahmood, S.; Ricci, F.; Hatz, K.; Studnicka, J.; Bezlyak, V.; Parikh, S.; Stubbings, W.J.; Wenzel, A.; et al. Ranibizumab 0.5 mg treat-and-extend regimen for diabetic macular oedema: The Retain study. Br. J. Ophthalmol. 2015, 100, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Chang, L.K.; Klancnik, J.M.; Yannuzzi, L.A.; Sorenson, J.; Slakter, J.S.; Freund, K.B.; Klein, R. Prospective study of intravitreal Ranibizumab as a treatment for decreased visual acuity secondary to central retinal vein occlusion. Am. J. Ophthalmol. 2009, 147, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Campochiaro, P.A.; Bhisitkul, R.B.; Ho, A.C.; Gray, S.; Saroj, N.; Adamis, A.P.; Rubio, R.G.; Murahashi, W.Y. Sustained benefits from Ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology 2011, 118, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.L.; Boyer, D.S.; Heier, J.S.; Brown, D.M.; Haller, J.A.; Vitti, R.; Kazmi, H.; Berliner, A.J.; Erickson, K.; Chu, K.W.; et al. Intravitreal Aflibercept for macular edema following branch retinal vein occlusion. Ophthalmology 2016, 123, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Campochiaro, P.A.; Yau, L.; Li, Z.; Saroj, N.; Rubio, R.G.; Lai, P. Ranibizumab for macular edema due to retinal vein occlusions. Ophthalmology 2012, 119, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Danyliv, A.; Glanville, J.; McCool, R.; Ferreira, A.; Skelly, A.; Jacob, R.P. The clinical effectiveness of ranibizumab treat and extend regimen in nAMD: Systematic review and network meta-analysis. Adv. Ther. 2017, 34, 611–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosogi, M.; Morizane, Y.; Shiode, Y.; Doi, S.; Kumase, F.; Kimura, S.; Hosokawa, M.; Hirano, M.; Toshima, S.; Takahashi, K.; et al. Results of a treat-and-extend regimen of intravitreal ranibizumab injection for macular edema due to branch retinal vein occlusion. Acta Med. Okayama 2018, 72, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Hosogi, M.; Shiode, Y.; Morizane, Y.; Kimura, S.; Hosokawa, M.; Doi, S.; Toshima, S.; Takahashi, K.; Fujiwara, A.; Shiraga, F. Two-year results of intravitreal ranibizumab injections using a treat-and-extend regimen for macular edema due to branch retinal vein occlusion. Acta Med. Okayama 2019, 73, 517–522. [Google Scholar] [PubMed]
- Arai, Y.; Takahashi, H.; Inoda, S.; Sakamoto, S.; Tan, X.; Inoue, Y.; Tominaga, S.; Kawashima, H.; Yanagi, Y. Efficacy of modified treat-and-extend regimen of Aflibercept for macular edema from branch retinal vein occlusion: 2-year prospective study outcomes. J. Clin. Med. 2021, 10, 3162. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-G.; Jeong, W.J.; Park, J.M.; Kim, J.-Y.; Ji, Y.-S.; Sagong, M. Prospective trial of treat-and-extend regimen with afliber-cept for branch retinal vein occlusion: 1-year results of the PLATON trial. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 2879–2886. [Google Scholar] [CrossRef] [PubMed]
- Hufendiek, K.; Pielen, A.; Framme, C. Injektionsstrategien bei der Anwendung intravitrealer VEGF-Inhibitoren: “Pro Re Nata versus Treat and Extend”. Klin. Mon. Augenheilkd. 2018, 235, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Hladíková, Z.; Klofáčová, E.; Kalvodová, B. Two-year follow-up results of patients with macular oedema due to retinal vein occlusion treated with Ranibizumab. Czech Slovak Ophthalmol. 2017, 73, 43–51. [Google Scholar]
- Campochiaro, P.A.; Sophie, R.; Pearlman, J.; Brown, D.M.; Boyer, D.S.; Heier, J.S.; Marcus, D.M.; Feiner, L.; Patel, A. Long-term outcomes in patients with retinal vein occlusion treated with Ranibizumab. Ophthalmology 2014, 121, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Ashrafzadeh, S.; Gundlach, B.S.; Tsui, I. The impact of non-ophthalmic factors on intravitreal injections during the COVID-19 lockdown. Clin. Ophthalmol. 2021, 15, 3661–3668. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Treatment | 6 Months n (%) | 12 Months n (%) | 18 Months n (%) | 24 Months n (%) |
|---|---|---|---|---|
| Didn’t require additional treatment | 2 (10%) | 2 (10%) | 4 (20%) | 6 (30%) |
| Continue ranibizumab in T&E regimen | 18 (90%) | 14 (70%) | 10 (50%) | 7 (35%) |
| Intravitreal dexamethasone | 1 (5%) | 2 (10%) | 2 (10%) | 2 (10%) |
| Switch to another anti-VEGF | 1 (5%) | 1 (5%) | 3 (15%) | 5 (25%) |
| Focal Laser | 0 (0%) | 1 (5%) | 1 (5%) | 0 (0%) |
| 0–6 Months | 6–12 Months | 12–18 Months | 18–24 Months | |
|---|---|---|---|---|
| Overall (n = 20) | 4.75 ± 0.55; (4–6) | 2.50 ± 0.95; (1–4) | 2.10 ± 1.45; (0–5) | 1.40 ± 1.10; (0–4) |
| Complete responder group (n = 13) | 4.77 ± 0.439 (4–5) | 2.38 ± 0.961 (1–4) | 1.54 ± 1.33 (0–3) | 0.92 ± 0.954 (0–2) |
| Incomplete responder group (n = 7) | 4.71 ± 0.756 (4–6) | 2.71 ± 0.951 (1–4) | 3.14 ± 1.069 (2–5) | 2.29 ± 0.756 (2–4) |
| p-value (complete vs. incomplete responders) | p = 0.705 | p = 0.442 | p = 0.023 | p = 0.007 |
| Diagnosis | 6 Months | 12 Months | 18 Months | 24 Months | |
|---|---|---|---|---|---|
| BCVA x̄ ± SD; (min-max) Overall (n = 20) | 0.60 ± 0.36; (0.01–1.30) | 0.30 ± 0.25; (0.00–1.00) | 0.34 ± 0.33; (0.00–1.30) | 0.37 ± 0.50; (0.00–2.0) | 0.29 ± 0.44; (0.00–1.66) |
| Complete responders to ranibizumab (n = 13) | 0.66 ± 0.42; (0.15–1.30) | 0.20 ± 0.17; (0.00–0.40) | 0.20 ± 0.12; (0.00–0.40) | 0.19 ± 0.21; (0.00–0.70) | 0.12 ± 0.12; (0.00–0.40) |
| Incomplete responders to ranibizumab (n = 7) | 0.51 ± 0.23; (0.10–0.70) | 0.46 ± 0.29; (0.05–1.00) | 0.55 ± 0.43; (0.10–1.30) | 0.64 ± 0.68; (0.10–2.00) | 0.55 ± 0.62; (0.04–1.66) |
| p-value (complete vs. incomplete responders) | 0.521 | 0.148 | 0.047 | 0.098 | 0.057 |
| CMT x̄ ± SD; (min–max) Overall (n = 20) | 559.85 ± 198.61; (318–1042) | 334.70 ± 106.16; (263–703) | 310.00 ± 80.31; (242–527) | 308.10 ± 88.75; (241–532) | 305.85 ± 111.78; (224–658) |
| Complete responders to ranibizumab (n =13) | 567.15 ± 196.17; (318–1042) | 311.46 ± 72.70; (263–528) | 299.15 ± 73.62; (242–527) | 293.15 ± 74.19; (241–527) | 283.62 ± 75.19; (224–524) |
| Incomplete responders to ranibizumab (n = 7) | 546.29 ± 218.23; (367–888) | 377.86 ± 147.56; (274–703) | 332.71 ± 93.42; (253–486) | 335.86 ± 112.04; (246–532) | 347.14 ± 158.75; (240–658) |
| p-value (complete vs incomplete responders) | 0.606 | 0.096 | 0.451 | 0.500 | 0.812 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Fernández, C.A.; Campo-Gesto, A.; López-López, A.; Gayoso-Rey, M. Real-World Evidence for Treat-and-Extend Regimen of Ranibizumab Therapy for Macular Oedema Secondary to Branch Retinal Vein Occlusion. Pharmaceuticals 2022, 15, 59. https://doi.org/10.3390/ph15010059
Rodríguez-Fernández CA, Campo-Gesto A, López-López A, Gayoso-Rey M. Real-World Evidence for Treat-and-Extend Regimen of Ranibizumab Therapy for Macular Oedema Secondary to Branch Retinal Vein Occlusion. Pharmaceuticals. 2022; 15(1):59. https://doi.org/10.3390/ph15010059
Chicago/Turabian StyleRodríguez-Fernández, Carmen Antía, Ana Campo-Gesto, Aida López-López, and Mónica Gayoso-Rey. 2022. "Real-World Evidence for Treat-and-Extend Regimen of Ranibizumab Therapy for Macular Oedema Secondary to Branch Retinal Vein Occlusion" Pharmaceuticals 15, no. 1: 59. https://doi.org/10.3390/ph15010059
APA StyleRodríguez-Fernández, C. A., Campo-Gesto, A., López-López, A., & Gayoso-Rey, M. (2022). Real-World Evidence for Treat-and-Extend Regimen of Ranibizumab Therapy for Macular Oedema Secondary to Branch Retinal Vein Occlusion. Pharmaceuticals, 15(1), 59. https://doi.org/10.3390/ph15010059