
Empagliflozin—A New Chance for Patients with Chronic Heart Failure


Abstract
:1. Introduction
2. Heart Failure
3. Empagliflozin as a Representative of SGLT2-Inhibitors
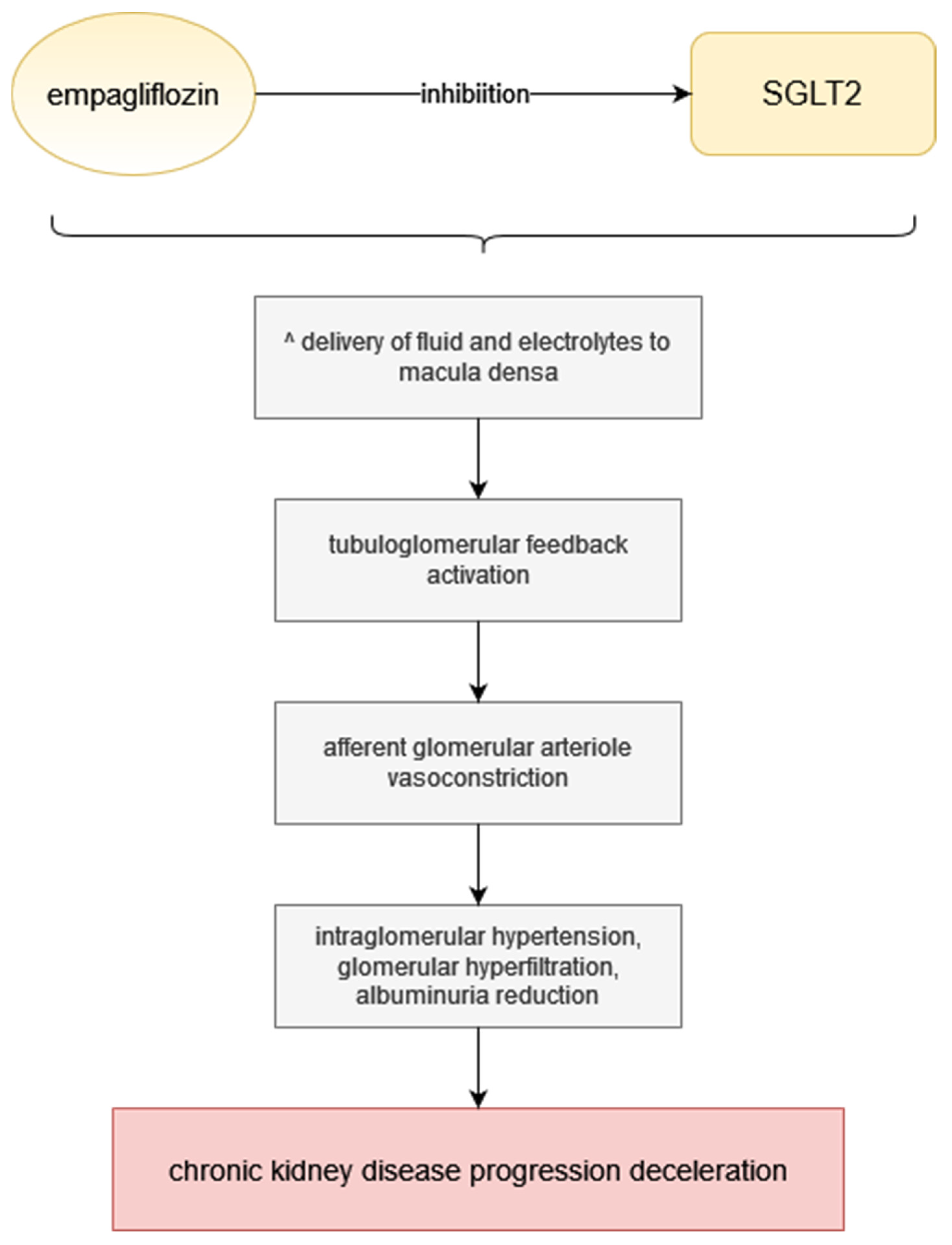
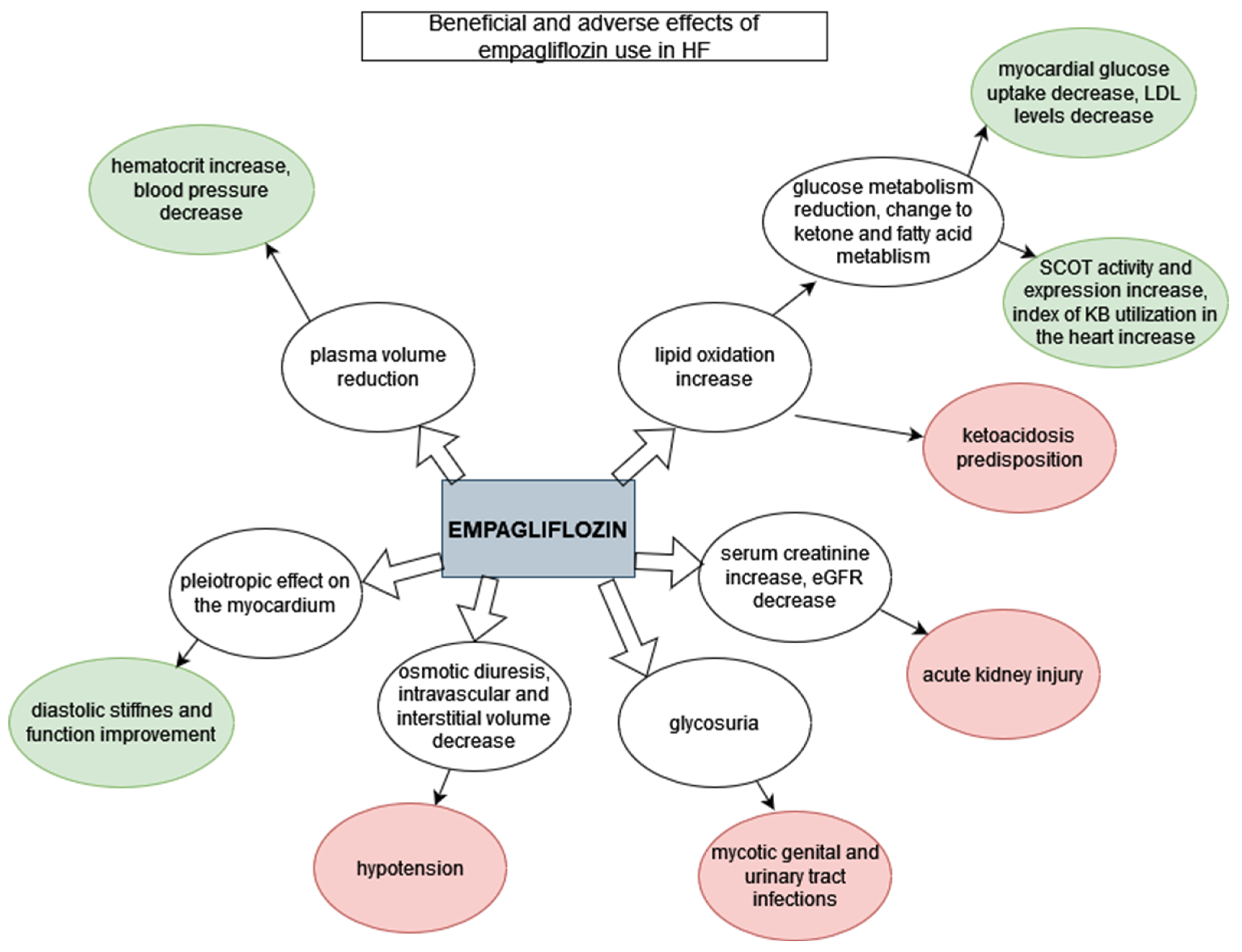
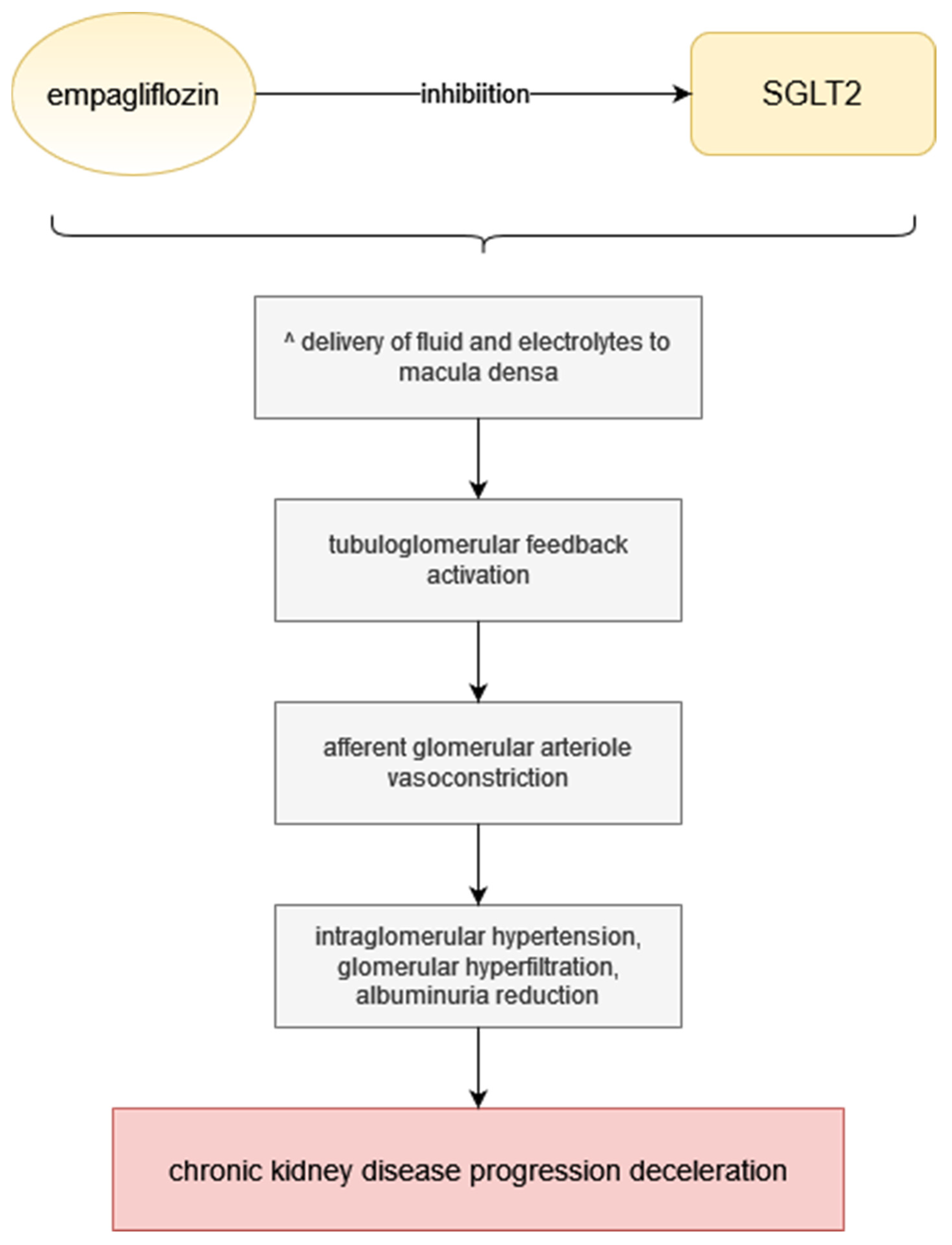
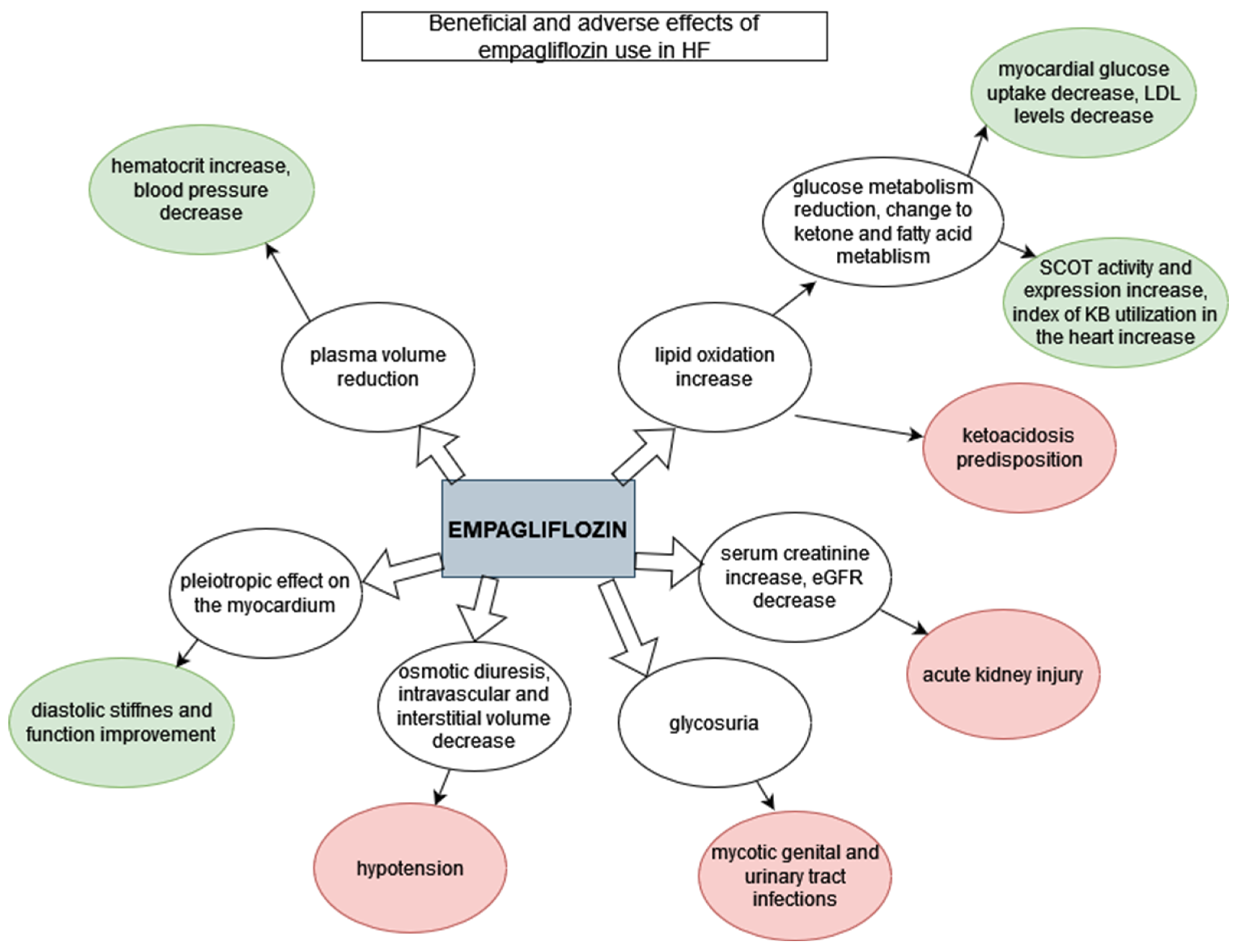
4. The Underlying Mechanism of the Beneficial Effect of Empagliflozin in HF Treatment
5. Limitations of Empagliflozin Use in Patients with HF
6. Empagliflozin versus Dapagliflozin in HF Treatment

{kind=link}
{kind=link}
| Selected Clinical Trials on SGLT-2 Inhibitors in Heart Failure | ||||
|---|---|---|---|---|
| FLOZIN | DAPAGLIFLOZIN | EMPAGLIFLOZIN | ||
| STUDY | DAPA-HF [47] | DELIEVER [48] | EMPEROR-Reduced [44] | EMPEROR-Preserved [49] |
| INCLUSION CRITERIA | Patients of an age of at least 18 years, an ejection fraction of 40% or less, NYHA class II, III, or IV. Patients were required to have a plasma level of N-terminal pro–B-type natriuretic peptide (NT-proBNP) of at least 600 pg per millilitre (or ≥400 pg per millilitre if they had been hospitalized for heart failure within the previous 12 months). Patients with atrial fibrillation or atrial flutter on baseline electrocardiography were required to have an NT-proBNP level of at least 900 pg per millilitre. | Patients at 40 years of age or older, with an LVEF > 40%, evidence of structural heart disease and elevation in natriuretic peptides [N-terminal pro B-type natriuretic peptide (NT-proBNP) ≥300 pg/mL (≥600 pg/mL for patients in atrial fibrillation or flutter). | Adults (≥18 years of age) who had chronic heart failure (functional class II, III, or IV) and
| Patients with LVEF >40%, elevated N-terminal pro B-type natriuretic peptide (NT-proBNP) concentrations (i.e., >300 pg/mL in patients without and >900 pg/mL in patients with atrial fibrillation) along with evidence of structural changes in the heart or documented history of heart failure hospitalization. NYHA II-IV. |
| NUMBER OF PATIENTS | 4744 | 6263 | 3730 | 5988 |
| DIABETIC STATUS | Both diabetic and non-diabetic patients. | Both diabetic and non-diabetic patients. | Both diabetic and non-diabetic patients. | Both diabetic and non-diabetic patients. |
| MEAN FOLLOW-UP TIME | 18.2 months. | Ongoing trial. | 16 months. | 26.2 months |
| PRIMARY ENDPOINT | Worsening heart failure (urgent hospitalization or intravenous therapy) or death from cardiovascular causes. | Cardiovascular death or worsening heart failure event (heart failure hospitalization or urgent HF visit). | Adjudicated cardiovascular death or hospitalization for heart failure, analysed as the time to the first event. | A composite of adjudicated cardiovascular (CV) death or hospitalization for HF. |
| PRIMARY ENDPOINT OCCURENCE | The primary outcome occurred in 386 of 2368 patients (16.3%) in the dapagliflozin group and in 502 of 2375 patients (21.2%) in the placebo group (HR: 0.74). | Ongoing trial | Primary outcome event occurred in 361 of 1863 patients (19.4%) in the empagliflozin group and in 462 of 1867 patients (24.7%) in the placebo group (hazard ratio for cardiovascular death or hospitalization for heart failure: 0.75). | A primary composite outcome event occurred in 415 patients (13.8%) in the empagliflozin group and in 511 patients (17.1%) in the placebo group, HR: 0.79. |
| DIABETIC VS. NON-DIABETIC GROUP | Findings in patients with diabetes were similar to those in patients without diabetes. | Ongoing trial | The effect of empagliflozin on the primary outcome was consistent in patients regardless of the presence or absence of diabetes. | The effects were consistent across prespecified subgroups, including in the presence or absence of diabetes at baseline. |
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef]
- Wasywich, C.A.; Gamble, G.D.; Whalley, G.A.; Doughty, R.N. Understanding changing patterns of survival and hospitalization for heart failure over two decades in New Zealand: Utility of ‘days alive and out of hospital’ from epidemiological data. Eur. J. Heart Fail. 2010, 12, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Anker, S.D.; AlHabib, K.F.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death worldwide. ESC Heart Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Larson, M.G.; Leip, E.P.; Beiser, A.; D’Agostino, R.B.; Kannel, W.B.; Murabito, J.M.; Vasan, R.S.; Benjamin, E.J.; Levy, D. Framingham Heart Study. Lifetime risk for developing congestive heart failure: The Framingham Heart Study. Circulation 2002, 106, 3068–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komorowska, A.; Lelonek, M. Heart failure with preserved ejection fraction: The challenge for modern cardiology. Folia Cardiol. 2020, 15, 407–412. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [Green Version]
- Stewart, S.; Jenkins, A.; Buchan, S.; McGuire, A.; Capewell, S.; McMurray, J.J. The current cost of heart failure to the National Health Service in the UK. Eur. J. Heart Fail. 2002, 4, 361–371. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. Corrigendum to: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Nashawi, M.; Sheikh, O.; Battisha, A.; Mir, M.; Chilton, R. Beyond the myocardium? SGLT2 inhibitors target peripheral components of reduced oxygen flux in the diabetic patient with heart failure with preserved ejection fraction. Heart Fail. Rev. 2020, 1–16. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Coronel, R.; de Groot, J.R.; van Lieshout, J.J. Defining heart failure. Cardiovasc. Res. 2001, 50, 419–422. [Google Scholar] [CrossRef] [Green Version]
- Hummel, A.; Empe, K.; Dörr, M.; Felix, S.B. De novo acute heart failure and acutely decompensated chronic heart failure. Dtsch. Ärztebl. Int. 2015, 112, 298–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokos, G.G.; Raina, A. Understanding the early mortality benefit observed in the PARADIGM-HF trial: Considerations for the management of heart failure with sacubitril/valsartan. Vasc. Health Risk Manag. 2020, 16, 41. [Google Scholar] [CrossRef] [Green Version]
- Mosterd, A.; Hoes, A.W. Clinical epidemiology of heart failure. Heart 2007, 93, 1137–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrzypek, A.; Mostowik, M.; Szeliga, M.; Wilczyńska-Golonka, M.; Dębicka-Dąbrowska, D.; Nessler, J. Chronic heart failure in the elderly: Still a current medical problem. Folia Med. Cracov. 2018, 58, 47–56. [Google Scholar] [PubMed]
- Elgendy, I.Y.; Mahtta, D.; Pepine, C.J. Medical Therapy for Heart Failure Caused by Ischemic Heart Disease. Circ. Res. 2019, 124, 1520–1535. [Google Scholar] [CrossRef] [PubMed]
- Iyngkaran, P.; Liew, D.; Neil, C.; Driscoll, A.; Marwick, T.H.; Hare, D.L. Moving From Heart Failure Guidelines to Clinical Practice: Gaps Contributing to Readmissions in Patients With Multiple Comorbidities and Older Age. Clin. Med. Insights Cardiol. 2018, 12, 1179546818809358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badu-Boateng, C.; Jennings, R.; Hammersley, D. The therapeutic role of ivabradine in heart failure. Ther. Adv. Chronic. Dis. 2018, 9, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Książczyk, M.; Lelonek, M. Angiotensin receptor/neprilysin inhibitor-a breakthrough in chronic heart failure therapy: Summary of subanalysis on PARADIGM-HF trial findings. Heart Fail. Rev. 2020, 25, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Braunwald, E. Heart failure. JACC Heart Fail. 2013, 1, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Levesque, V.; et al. CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.R.; Ades, P.A.; Thompson, P.D. The role of cardiac rehabilitation in patients with heart disease. Trends Cardiovasc. Med. 2017, 27, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Sagar, V.A.; Davies, E.J.; Briscoe, S.; Coats, A.J.; Dalal, H.; Lough, F.; Rees, K.; Singh, S. Exercise-based rehabilitation for heart failure. Cochrane Database Syst. Rev. 2014, 2014, CD003331. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Fernandez, B.; Sarafidis, P.; Kanbay, M.; Navarro-González, J.F.; Soler, M.J.; Górriz, J.L.; Ortiz, A. SGLT2 inhibitors for non-diabetic kidney disease: Drugs to treat CKD that also improve glycaemia. Clin. Kidney J. 2020, 13, 728–733. [Google Scholar] [CrossRef]
- Announcement of the Minister of Health of 21 December 2020 on the List of Reimbursed Medicines, Foodstuffs for Special Nutritional Purposes and Medical Devices for 1 January 2021. Available online: https://www.gov.pl/web/zdrowie/obwieszczenie-ministra-zdrowia-z-dnia-21-grudnia-2020-r-w-sprawie-wykazu-refundowanych-lekow-srodkow-spozywczych-specjalnego-przeznaczenia-zywieniowego-oraz-wyrobow-medycznych-na-1-stycznia-2021-r (accessed on 22 December 2020).
- Kohler, S.; Zeller, C.; Iliev, H.; Kaspers, S. Safety and Tolerability of Empagliflozin in Patients with Type 2 Diabetes: Pooled Analysis of Phase I-III Clinical Trials. Adv. Ther. 2017, 34, 1707–1726. [Google Scholar] [CrossRef] [Green Version]
- Michel, M.C.; Mayoux, E.; Vallon, V. A comprehensive review of the pharmacodynamics of the SGLT2 inhibitor empagliflozin in animals and humans. Naunyn Schmiedebergs Arch. Pharmacol. 2015, 388, 801–816. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E.; Zinman, B.; Fitchett, D.; Wanner, C.; Ferrannini, E.; Schumacher, M.; Schmoor, C.; Ohneberg, K.; Johansen, O.E.; George, J.T.; et al. How Does Empagliflozin Reduce Cardiovascular Mortality? Insights from a Mediation Analysis of the EMPA-REG OUTCOME Trial. Diabetes Care 2018, 41, 356–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pabel, S.; Wagner, S.; Bollenberg, H.; Bengel, P.; Kovács, Á.; Schach, C.; Tirilomis, P.; Mustroph, J.; Renner, A.; Gummert, J.; et al. Empagliflozin directly improves diastolic function in human heart failure. Eur. J. Heart Fail. 2018, 20, 1690–1700. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Marx, N. SGLT2 inhibitors: The future for treatment of type 2 diabetes mellitus and other chronic diseases. Diabetologia 2018, 61, 2134–2139. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, D.E.; Foresto, R.D.; Ribeiro, A.B. SGLT-2 inhibitors in diabetes: A focus on renoprotection. Rev. Assoc. Med. Bras. 2020, 66, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Vallon, V.; Thomson, S.C. Targeting renal glucose reabsorption to treat hyperglycaemia: The pleiotropic effects of SGLT2 inhibition. Diabetologia 2017, 60, 215–225. [Google Scholar] [CrossRef]
- Wanner, C.; Heerspink, H.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; Hantel, S.; Woerle, H.J.; Broedl, U.C.; von Eynatten, M.; et al. EMPA-REG OUTCOME Investigators. Empagliflozin and Kidney Function Decline in Patients with Type 2 Diabetes: A Slope Analysis from the EMPA-REG OUTCOME Trial. J. Am. Soc. Nephrol. 2018, 29, 2755–2769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacIsaac, R.J.; Jerums, G.; Ekinci, E.I. Cardio-renal protection with empagliflozin. Ann. Transl. Med. 2016, 4, 409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Requena-Ibanez, J.A.; San Antonio, R.; Ishikawa, K.; Watanabe, S.; Picatoste, B.; Flores, E.; Garcia-Ropero, A.; Sanz, J.; Hajjar, R.J.; et al. Empagliflozin Ameliorates Adverse Left Ventricular Remodeling in Nondiabetic Heart Failure by Enhancing Myocardial Energetics. J. Am. Coll. Cardiol. 2019, 73, 1931–1944. [Google Scholar] [CrossRef]
- Patorno, E.; Pawar, A.; Franklin, J.M.; Najafzadeh, M.; Déruaz-Luyet, A.; Brodovicz, K.G.; Sambevski, S.; Bessette, L.G.; Santiago Ortiz, A.J.; Kulldorff, M.; et al. Empagliflozin and the Risk of Heart Failure Hospitalization in Routine Clinical Care. Circulation 2019, 139, 2822–2830. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J. Cardiovascular Effects of New Oral Glucose-Lowering Agents: DPP-4 and SGLT-2 Inhibitors. Circ. Res. 2018, 122, 1439–1459. [Google Scholar] [CrossRef] [PubMed]
- Sizar, O.; Podder, V.; Talati, R. Empagliflozin. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Scheen, A.J. SGLT2 Inhibitors: Benefit/Risk Balance. Curr. Diab. Rep. 2016, 16, 92. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 413–1424. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]
- Verma, S.; McGuire, D.K.; Kosiborod, M.N. Two Tales: One Story: EMPEROR-Reduced and DAPA-HF. Circulation 2020, 142, 2201–2204. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; Shah, S.J.; Lindholm, D.; et al. Dapagliflozin in heart failure with preserved and mildly reduced ejection fraction: Rationale and design of the DELIVER trial. Eur. J. Heart Fail. 2021, 23, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Patrono, C. The EMPEROR-Preserved study: End of the search for the “Phoenix” or beginning of a new season for trials in heart failure with preserved ejection fraction. Eur. Heart J. 2021, 42, 4621–4623. [Google Scholar] [CrossRef] [PubMed]
| HFrEF | HFmrEF | HFpEF | |
|---|---|---|---|
| Criterion number 1 | Symptoms and signs | Symptoms and signs | Symptoms and signs |
| Criterion number 2: LVEF | <40% | 40–49% | >50% |
| Criterion number 3 | - | - | Objective evidence of cardiac structural and/or functional anomalies |
| Adverse Effect | Anker SD et al. [44] | Zinman et al. [43] | ||
|---|---|---|---|---|
| Empagliflozin Group | Placebo | Empagliflozin Group | Placebo | |
| Hypotension | 176/1863 | 163/1863 | - | - |
| 9.45% | 8.75% | |||
| Confirmed hypoglycemia | 33/1863 | 35/1863 | 1303/4684 | 650/2333 |
| 1.77% | 1.88% | 27.80% | 27.80% | |
| Urinary tract infection | 91/1863 | 83/1863 | 842/4684 | 423/2333 |
| 4.88% | 4.46% | 17.97% | 18.12% | |
| Acute renal failure | 175/1863 | 192/1863 | 246/4684 | 155/2333 |
| 9.39% | 10.3% | 5.25% | 6.64% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalska, K.; Walczak, J.; Femlak, J.; Młynarska, E.; Franczyk, B.; Rysz, J. Empagliflozin—A New Chance for Patients with Chronic Heart Failure. Pharmaceuticals 2022, 15, 47. https://doi.org/10.3390/ph15010047
Kowalska K, Walczak J, Femlak J, Młynarska E, Franczyk B, Rysz J. Empagliflozin—A New Chance for Patients with Chronic Heart Failure. Pharmaceuticals. 2022; 15(1):47. https://doi.org/10.3390/ph15010047
Chicago/Turabian StyleKowalska, Klaudia, Justyna Walczak, Joanna Femlak, Ewelina Młynarska, Beata Franczyk, and Jacek Rysz. 2022. "Empagliflozin—A New Chance for Patients with Chronic Heart Failure" Pharmaceuticals 15, no. 1: 47. https://doi.org/10.3390/ph15010047
APA StyleKowalska, K., Walczak, J., Femlak, J., Młynarska, E., Franczyk, B., & Rysz, J. (2022). Empagliflozin—A New Chance for Patients with Chronic Heart Failure. Pharmaceuticals, 15(1), 47. https://doi.org/10.3390/ph15010047