
Differential Effect of Three Macrolide Antibiotics on Cardiac Pathology and Electrophysiology in a Myocardial Infarction Rat Model: Influence on Sodium Nav1.5 Channel Expression


 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
2.1. The Effect of Azithromycin, Clarithromycin, and Erythromycin on Serum Lactate Dehydrogenase and CK-MB in Healthy Rats and AMI Rats
2.2. ECG Parameters in Normal and AMI raTs Received Azithromycin, Clarithromycin, and Erythromycin
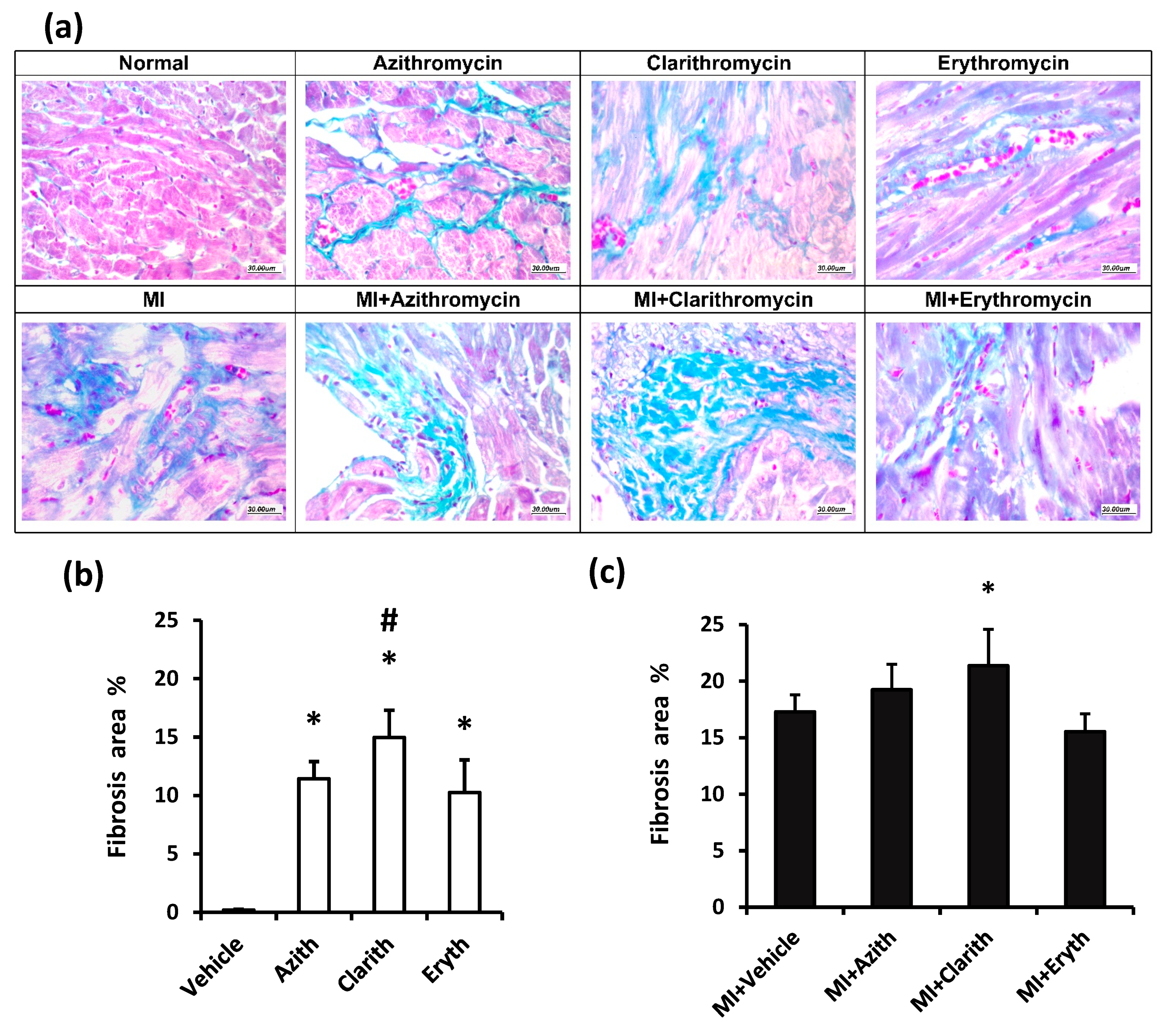
2.3. Effect of Azithromycin, Clarithromycin, and Erythromycin on Myocardial Histopathologic Findings
2.4. The Survival Percent in Experimental Groups
2.5. The Effect of Azithromycin, Clarithromycin, and Erythromycin on Cardiac Nav1.5 Channel Gene Expression
3. Discussion
4. Materials and Methods
4.1. Antibiotic Preparations
4.2. Experimental Animals
4.3. Induction of Experimental Myocardial Infarction by Isoproterenol
4.4. Dose Justification for Macrolide Antibiotics
4.5. Study Design
4.6. Electrocardiography
4.7. Animal Scarification and Specimen Collection
4.8. Determination of Serum LDH and CK-MB
4.9. Quantitative Real-Time Reverse Transcription-Polymerase Chain Reaction (RT-PCR) Analysis of Cardiac Sodium Nav1.5 Ion Channel Gene Expression
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abugharbieh, E.; Vasina, V.; Poluzzi, E.; Deponti, F. Antibacterial macrolides: A drug class with a complex pharmacological profile. Pharmacol. Res. 2004, 50, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Swadron, S. Preventing Sudden Death in Acute Myocardial Infarction: The ‘Mortality Plateau’; BMJ Publishing Group Ltd. and British Cardiovascular Society: London, UK, 2014. [Google Scholar]
- Sieira, J.; Dendramis, G.; Brugada, P. Pathogenesis and management of Brugada syndrome. Nat. Rev. Cardiol. 2016, 13, 744. [Google Scholar] [CrossRef]
- Lane, J.C.E.; Weaver, J.; Kostka, K.; Duarte-Salles, T.; Abrahao, M.T.F.; Alghoul, H.; Alser, O.; Alshammari, T.M.; Biedermann, P.; Burn, E.; et al. Safety of hydroxychloroquine, alone and in combination with azithromycin, in light of rapid wide-spread use for COVID-19: A multinational, network cohort and self-controlled case series study. medRXiv 2020. [Google Scholar] [CrossRef]
- Moran, A.E.; Tzong, K.Y.; Forouzanfar, M.H.; Roth, G.A.; Mensah, G.A.; Ezzati, M.; Murray, C.J.L.; Naghavi, M. Variations in ischemic heart disease burden by age, country, and income: The Global Burden of Diseases, Injuries, and Risk Factors 2010 study. Glob. Heart 2014, 9, 91–99. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. 2013. Available online: https://apps.who.int/iris/bitstream/handle/10665/94384/9789244506233_rus.pdf (accessed on 10 February 2021).
- Nattel, S.; Maguy, A.; Le Bouter, S.; Yeh, Y.-H. Arrhythmogenic ion-channel remodeling in the heart: Heart failure, myocardial infarction, and atrial fibrillation. Physiol. Rev. 2007, 87, 425–456. [Google Scholar] [CrossRef] [PubMed]
- León-Ariza, H.H.; Valenzuela-Faccini, N.; Rojas-Ortega, A.C.; Botero-Rosas, D.A. Nav1. 5 cardiac sodium channels, regulation and clinical implications. Rev. Fac. Med. 2014, 62, 587–592. [Google Scholar] [CrossRef]
- Reinhard, K.; Rougier, J.-S.; Ogrodnik, J.; Abriel, H. Electrophysiological properties of mouse and epitope-tagged human cardiac sodium channel Na v1. 5 expressed in HEK293 cells. F1000Research 2013, 2, 48. [Google Scholar] [CrossRef]
- Isbister, G.K. Risk assessment of drug-induced QT prolongation. Aust. Prescr. 2015, 38, 20–24. [Google Scholar] [CrossRef]
- Iannini, P.B. Cardiotoxicity of macrolides, ketolides and fluoroquinolones that prolong the QTc interval. Expert Opin. Drug Saf. 2002, 1, 121–128. [Google Scholar] [CrossRef]
- Albert, R.K.; Schuller, J.L.; Network, C.C.R. Macrolide antibiotics and the risk of cardiac arrhythmias. Am. J. Respir. Crit. Care Med. 2014, 189, 1173–1180. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Ray, W.A.; Murray, K.T.; Hall, K.; Arbogast, P.G.; Stein, C.M. Azithromycin and the risk of cardiovascular death. New Engl. J. Med. 2012, 366, 1881–1890. [Google Scholar] [CrossRef]
- Kezerashvili, A.; Khattak, H.; Barsky, A.; Nazari, R.; Fisher, J.D. Azithromycin as a cause of QT-interval prolongation and torsade de pointes in the absence of other known precipitating factors. J. Interv. Card. Electrophysiol. 2007, 18, 243–246. [Google Scholar] [CrossRef]
- Matsunaga, N.; Oki, Y.; Prigollini, A. A case of QT-interval prolongation precipitated by azithromycin. N. Z. Med. J. (Online) 2003, 116, 1185. [Google Scholar]
- Nishida, K.; Michael, G.; Dobrev, D.; Nattel, S. Animal models for atrial fibrillation: Clinical insights and scientific opportunities. Europace 2010, 12, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Abdelrady, A.M.; Zaitone, S.A.; Farag, N.E.; Fawzy, M.S.; Moustafa, Y.M. Cardiotoxic effect of levofloxacin and ciprofloxacin in rats with/without acute myocardial infarction: Impact on cardiac rhythm and cardiac expression of Kv4. 3, Kv1. 2 and Nav1. 5 channels. Biomed. Pharmacother. 2017, 92, 196–206. [Google Scholar] [CrossRef]
- Ohtani, H.; Taninaka, C.; Hanada, E.; Kotaki, H.; Sato, H.; Sawada, Y.; Iga, T. Comparative pharmacodynamic analysis of QT interval prolongation induced by the macrolides clarithromycin, roxithromycin, and azithromycin in rats. Antimicrob. Agents Chemother. 2000, 44, 2630–2637. [Google Scholar] [CrossRef] [PubMed]
- Milberg, P.; Eckardt, L.; Bruns, H.-J.; Biertz, J.; Ramtin, S.; Reinsch, N.; Fleischer, D.; Kirchhof, P.; Fabritz, L.; Breithardt, G. Divergent proarrhythmic potential of macrolide antibiotics despite similar QT prolongation: Fast phase 3 repolarization prevents early afterdepolarizations and torsade de pointes. J. Pharmacol. Exp. Ther. 2002, 303, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Fujikawa, K.; Harada, S.; Ohura, K.; Sasaki, T.; Takayama, S. Reproductive toxicity of the new quinolone antibacterial agent levofloxacin in rats and rabbits. Arzneimittel-Forschung 1992, 43, 374–377. [Google Scholar] [PubMed]
- Yue, L.; Melnyk, P.; Gaspo, R.; Wang, Z.; Nattel, S. Molecular mechanisms underlying ionic remodeling in a dog model of atrial fibrillation. Circ. Res. 1999, 84, 776–784. [Google Scholar] [CrossRef]
- Bennett, P.B.; Yazawa, K.; Makita, N.; George, A.L. Molecular mechanism for an inherited cardiac arrhythmia. Nature 1995, 376, 683–685. [Google Scholar] [CrossRef]
- Bezzina, C.; Veldkamp, M.W.; van den Berg, M.P.; Postma, A.V.; Rook, M.B.; Viersma, J.-W.; van Langen, I.M.; Tan-Sindhunata, G.; Bink-Boelkens, M.T.E.; van der Hout, A.H. A single Na+ channel mutation causing both long-QT and Brugada syndromes. Circ. Res. 1999, 85, 1206–1213. [Google Scholar] [CrossRef]
- Fredj, S.; Sampson, K.J.; Liu, H.; Kass, R.S. Molecular basis of ranolazine block of LQT-3 mutant sodium channels: Evidence for site of action. Br. J. Pharmacol. 2006, 148, 16–24. [Google Scholar] [CrossRef]
- Kim, M.H.; Berkowitz, C.; Trohman, R.G. Polymorphic ventricular tachycardia with a normal QT interval following azithromycin. Pacing Clin. Electrophysiol. PACE 2005, 28, 1221–1222. [Google Scholar] [CrossRef]
- Yang, Z.; Prinsen, J.K.; Bersell, K.R.; Shen, W.; Yermalitskaya, L.; Sidorova, T.; Luis, P.B.; Hall, L.; Zhang, W.; Du, L. Azithromycin causes a novel proarrhythmic syndrome. Circ. Arrhythmia Electrophysiol. 2017, 10, e003560. [Google Scholar] [CrossRef]
- Fujikawa, H.; Kawakami, T.; Nakashima, R.; Nasu, A.; Kamei, S.; Nohara, H.; Eto, Y.; Ueno-Shuto, K.; Takeo, T.; Nakagata, N. Azithromycin inhibits constitutive airway epithelial sodium channel activation in vitro and modulates downstream pathogenesis in vivo. Biol. Pharm. Bull. 2020, b19-01091. [Google Scholar] [CrossRef]
- Adsit, G.S.; Vaidyanathan, R.; Galler, C.M.; Kyle, J.W.; Makielski, J.C. Channelopathies from mutations in the cardiac sodium channel protein complex. J. Mol. Cell. Cardiol. 2013, 61, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.E.; Chen-Izu, Y.; Bers, D.M.; Belardinelli, L.; Boyden, P.A.; Csernoch, L.; Despa, S.; Fermini, B.; Hool, L.C.; Izu, L. Deranged sodium to sudden death. J. Physiol. 2015, 593, 1331–1345. [Google Scholar] [CrossRef] [PubMed]
- Araujo, F.G.; Shepard, R.M.; Remington, J.S. In vivo activity of the macrolide antibiotics azithromycin, roxithromycin and spiramycin against Toxoplasma gondii. Eur. J. Clin. Microbiol. Infect. Dis. 1991, 10, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Foulds, G.; Shepard, R.M.; Johnson, R.B. The pharmacokinetics of azithromycin in human serum and tissues. J. Antimicrob. Chemother. 1990, 25, 73–82. [Google Scholar] [CrossRef]
- Banerjee, S.K.; Sood, S.; Dinda, A.K.; Das, T.K.; Maulik, S.K. Chronic oral administration of raw garlic protects against isoproterenol-induced myocardial necrosis in rat. Comp. Biochem. Physiol. Part C Toxicol. Pharmacol. 2003, 136, 377–386. [Google Scholar] [CrossRef]
- Zaitone, S.A.; Abo-Gresha, N.M. Rosuvastatin promotes angiogenesis and reverses isoproterenol-induced acute myocardial infarction in rats: Role of iNOS and VEGF. Eur. J. Pharmacol. 2012, 691, 134–142. [Google Scholar] [CrossRef]
- Khodeer, D.M.; Zaitone, S.A.; Farag, N.E.; Moustafa, Y.M. Cardioprotective effect of pioglitazone in diabetic and non-diabetic rats subjected to acute myocardial infarction involves suppression of AGE-RAGE axis and inhibition of apoptosis. Can. J. Physiol. Pharmacol. 2016, 94, 463–476. [Google Scholar] [CrossRef]
- Rehg, J.E. Activity of azithromycin against cryptosporidia in immunosuppressed rats. J. Infect. Dis. 1991, 163, 1293–1296. [Google Scholar] [CrossRef]
- Sassa, K.; Mizushima, Y.; Fujishita, T.; Oosaki, R.; Kobayashi, M. Therapeutic effect of clarithromycin on a transplanted tumor in rats. Antimicrob. Agents Chemother. 1999, 43, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Kmecova, J.; Klimas, J. Heart rate correction of the QT duration in rats. Eur. J. Pharmacol. 2010, 641, 187–192. [Google Scholar] [CrossRef]
- Banchroft, J.D.; Stevens, A.; Turner, D.R. Theory and Practice of Histological Techniques, 4th ed.; Churchil Living Stone: New York, NY, USA; London, UK; San Francisco, CA, USA; Tokyo, Japan, 1996. [Google Scholar]
- Saito, T.; Tamura, K.; Uchida, D.; Saito, T.; Togashi, M.; Nitta, T.; Sugisaki, Y. Histopathological features of the resected left atrial appendage as predictors of recurrence after surgery for atrial fibrillation in valvular heart disease. Circ. J. 2007, 71, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, H.J. Drug-induced chronic hepatic disease. Med. Clin. N. Am. 1979, 63, 567–582. [Google Scholar] [CrossRef]
- Ibrahiem, A.T.; Fawzy, M.S.; Abu AlSel, B.T.; Toraih, E.A. Prognostic value of BRAF/MIR-17 signature and B-Raf protein expression in patients with colorectal cancer: A pilot study. J. Clin. Lab. Anal. 2021, 35, e23679. [Google Scholar] [CrossRef]
- Kattan, S.W.; Hobani, Y.H.; Shaheen, S.; Mokhtar, S.H.; Hussein, M.H.; Toraih, E.A.; Fawzy, M.S.; Abdalla, H.A. Association of cyclin-dependent kinase inhibitor 2B antisense RNA 1 gene expression and rs2383207 variant with breast cancer risk and survival. Cell. Mol. Biol. Lett. 2021, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | PR Interval (ms) | QT Interval (ms) | HR (Beat/min) |
|---|---|---|---|
| Vehicle | 40.1 ± 1.79 | 88.6 ± 2.37 | 369.3 ± 8.65 |
| Azith | 44.3 ± 1.50 * | 93.8 ± 1.05 * | 379.3 ± 2.56 * |
| Clarith | 43.9 ± 2.2 * | 93.6 ± 137 * | 375.3 ± 1.44 * |
| Eryth | 44.2 ± 1.89 * | 94.6 ± 1.65 * | 381.1 ± 2.34 * |
| MI+ Vehicle | 46.4 ± 1.90 | 94.2 ± 2.15 | 388.1 ± 8.21 |
| MI + Azith | 48.8 ± 5.22 | 95.6 ± 3.37 | 389.9 ± 80.69 |
| MI + Clarith | 49.6 ± 2.32 a | 99.3 ± 2.91 a | 425.5 ± 45.63 a |
| MI + Eryth | 50.1 ± 3.3 a | 98.2 ± 1.71 a | 426.6 ± 36.33 a |
| Weeks | 1 | 2 | 9 | 10 |
|---|---|---|---|---|
| Healthy | Vehicle or Oral Macrolides | Functional assessment | Blood tests & Histology | |
| MI | Vehicle or Oral Macrolides | Functional assessment | Blood tests & Histology |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farag, N.E.; El-Kherbetawy, M.K.; Ismail, H.M.; Abdelrady, A.M.; Toraih, E.A.; Abdelbasset, W.K.; Lashine, R.M.; EL-dosoky, M.; Abed, S.Y.; Ibraheem, K.M.; et al. Differential Effect of Three Macrolide Antibiotics on Cardiac Pathology and Electrophysiology in a Myocardial Infarction Rat Model: Influence on Sodium Nav1.5 Channel Expression. Pharmaceuticals 2021, 14, 597. https://doi.org/10.3390/ph14070597
Farag NE, El-Kherbetawy MK, Ismail HM, Abdelrady AM, Toraih EA, Abdelbasset WK, Lashine RM, EL-dosoky M, Abed SY, Ibraheem KM, et al. Differential Effect of Three Macrolide Antibiotics on Cardiac Pathology and Electrophysiology in a Myocardial Infarction Rat Model: Influence on Sodium Nav1.5 Channel Expression. Pharmaceuticals. 2021; 14(7):597. https://doi.org/10.3390/ph14070597
Chicago/Turabian StyleFarag, Noha E., Mohamed K. El-Kherbetawy, Hussein M. Ismail, Ahmed M. Abdelrady, Eman A. Toraih, Walid Kamal Abdelbasset, Rehab M. Lashine, Mohammed EL-dosoky, Sally Yussef Abed, Khalid M. Ibraheem, and et al. 2021. "Differential Effect of Three Macrolide Antibiotics on Cardiac Pathology and Electrophysiology in a Myocardial Infarction Rat Model: Influence on Sodium Nav1.5 Channel Expression" Pharmaceuticals 14, no. 7: 597. https://doi.org/10.3390/ph14070597
APA StyleFarag, N. E., El-Kherbetawy, M. K., Ismail, H. M., Abdelrady, A. M., Toraih, E. A., Abdelbasset, W. K., Lashine, R. M., EL-dosoky, M., Abed, S. Y., Ibraheem, K. M., Fawzy, M. S., & Zaitone, S. A. (2021). Differential Effect of Three Macrolide Antibiotics on Cardiac Pathology and Electrophysiology in a Myocardial Infarction Rat Model: Influence on Sodium Nav1.5 Channel Expression. Pharmaceuticals, 14(7), 597. https://doi.org/10.3390/ph14070597