
Clinical Management of COVID-19: A Review of Pharmacological Treatment Options





Abstract
1. Introduction
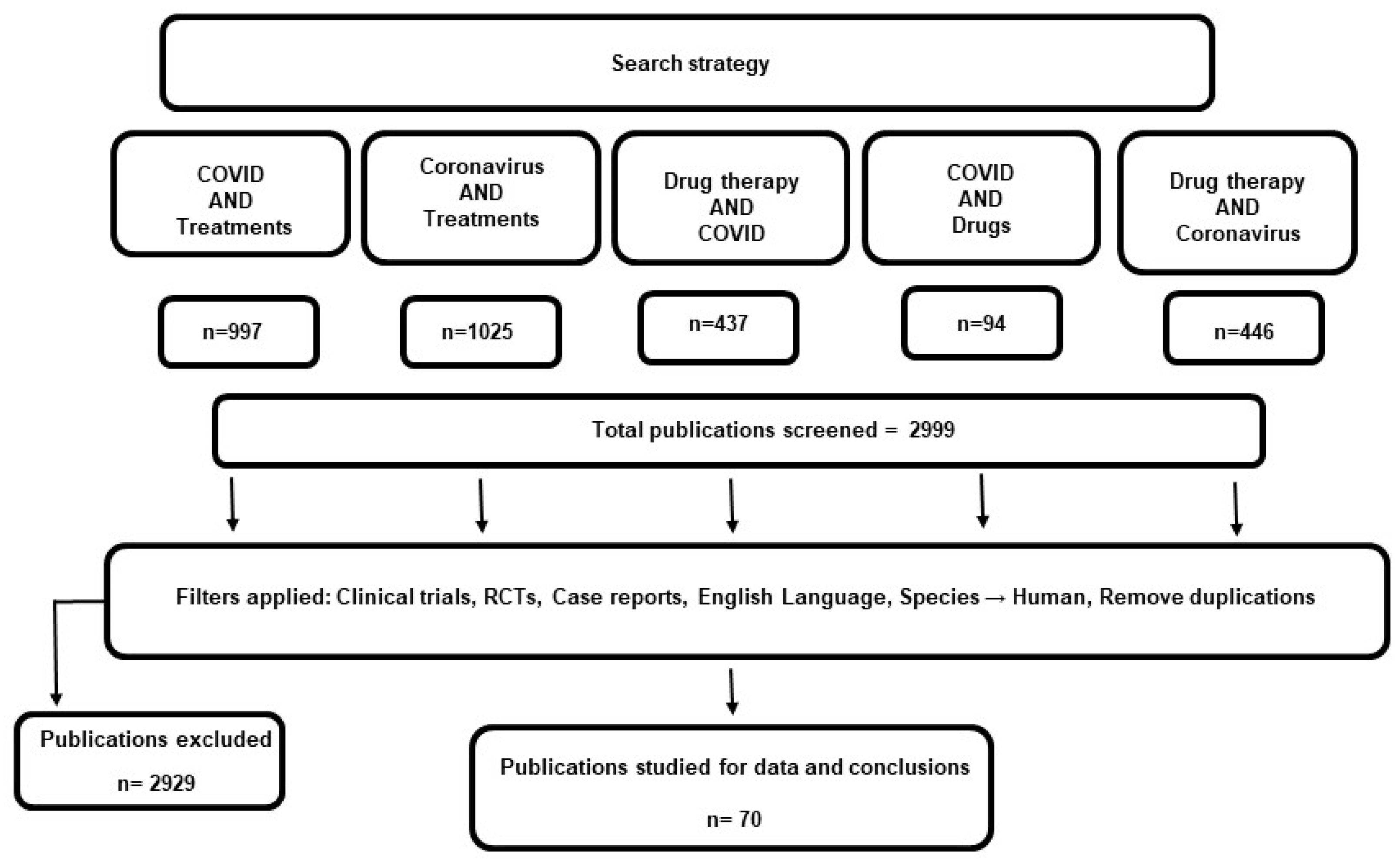
2. Methodology
3. Results
3.1. Approved Therapeutics
3.1.1. Convalescent Plasma
3.1.2. Remdesivir
3.1.3. Casirivimab/Imdevimab
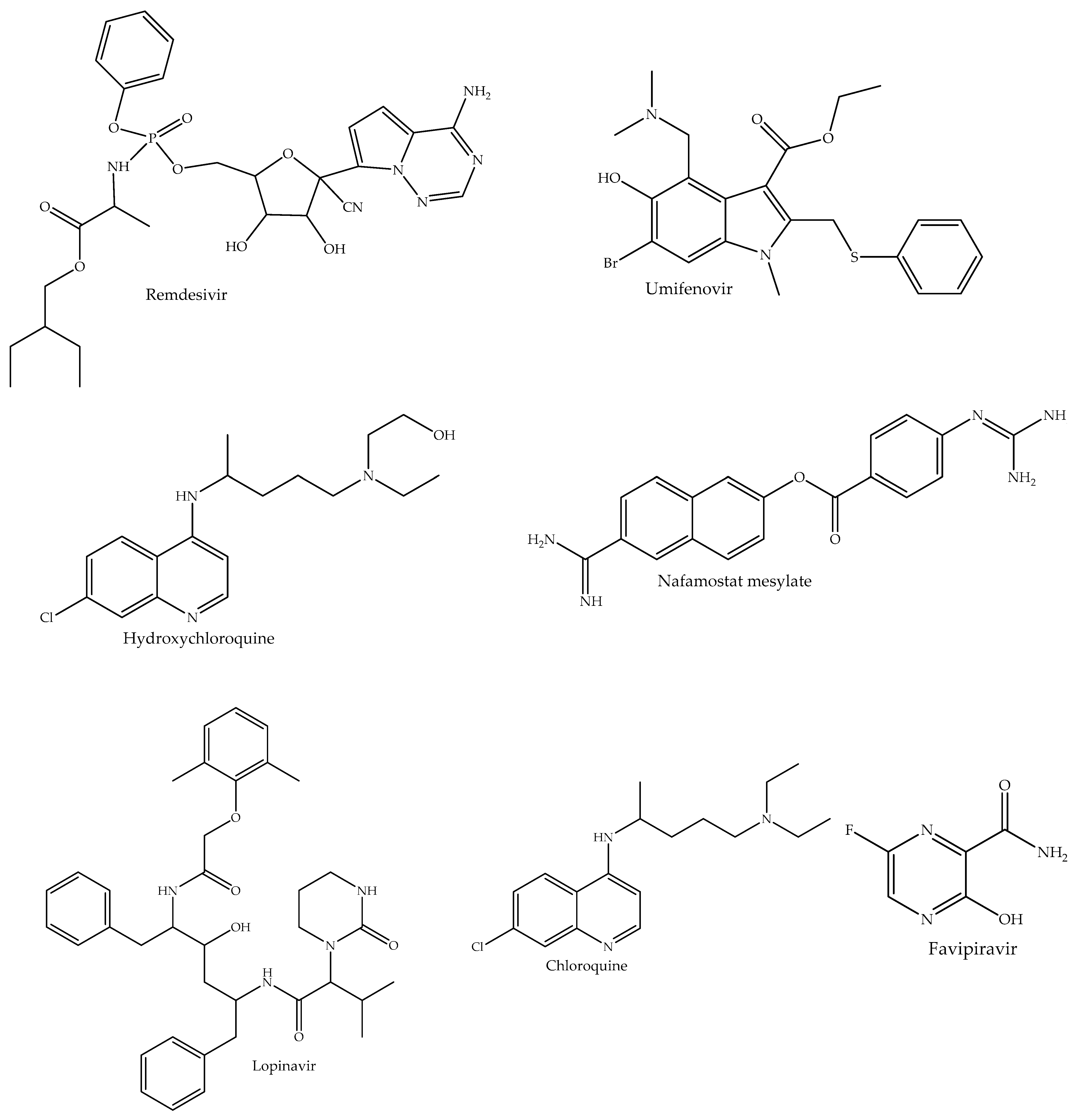
3.2. Repurposed and Off-Label Anti-Infective Drugs
3.2.1. Lopinavir–Ritonavir
3.2.2. Umifenovir
3.2.3. Favipiravir
3.2.4. Chloroquine and Hydroxychloroquine
3.3. Biologics, Immunomodulators and Other Supportive Treatments
3.3.1. Anakinra
3.3.2. Corticosteroids
3.3.3. Tocilizumab
3.3.4. Interferons
3.3.5. Tissue Plasminogen Activator
3.3.6. Intravenous Immunoglobulin
3.3.7. Nafamostat
3.3.8. Vaccines
3.3.9. Adjunctive and Supplementary Medicines
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 24 May 2021).
- WHO. COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 5 May 2021).
- Guarner, J. Three emerging coronaviruses in two decades: The story of SARS, MERS, and now COVID-19. Am. J. Clin. Pathol. 2020, 153, 420–421. [Google Scholar] [CrossRef]
- Goldsmith, C.S.; Tatti, K.M.; Ksiazek, T.G.; Rollin, P.E.; Comer, J.A.; Lee, W.W.; Rota, P.A.; Bankamp, B.; Bellini, W.J.; Zaki, S.R. Ultrastructural characterization of SARS coronavirus. Emerg. Infect. Dis. 2004, 10, 320–326. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.W.; Yuan, S.; Yuen, K.S.; Fung, S.Y.; Chan, C.P.; Jin, D.Y. Zoonotic origins of human coronaviruses. Int. J. Biol. Sci. 2020, 16, 1686. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef]
- Woo, P.C.; Wang, M.; Lau, S.K.; Xu, H.; Poon, R.W.; Guo, R.; Wong, B.H.; Gao, K.; Tsoi, H.W.; Huang, Y.; et al. Comparative analysis of twelve genomes of three novel group 2c and group 2d coronaviruses reveals unique group and subgroup features. J. Virol. 2007, 81, 1574–1585. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.K.; Woo, P.C.; Yip, C.C.; Fan, R.Y.; Huang, Y.; Wang, M.; Guo, R.; Lam, C.S.; Tsang, A.K.; Lai, K.K.; et al. Isolation and characterization of a novel Betacoronavirus subgroup A coronavirus, rabbit coronavirus HKU14, from domestic rabbits. J. Virol. 2012, 86, 5481–5496. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.K.; Poon, R.W.; Wong, B.H.; Wang, M.; Huang, Y.; Xu, H.; Guo, R.; Li, K.S.; Gao, K.; Chan, K.H.; et al. Coexistence of different genotypes in the same bat and serological characterization of Rousettus bat coronavirus HKU9 belonging to a novel Betacoronavirus subgroup. J. Virol. 2010, 84, 11385–11394. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Lam, T.T.Y.; Jia, N.; Zhang, Y.W.; Shum, M.H.H.; Jiang, J.F.; Zhu, H.C.; Tong, Y.G.; Shi, Y.X.; Ni, X.B.; Liao, Y.S.; et al. Identifying SARS-CoV-2-related coronaviruses in Malayan pangolins. Nature 2020, 583, 282–285. [Google Scholar] [CrossRef]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a neutralizing antibody cocktail, in outpatients with Covid-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef]
- Siu, Y.L.; Teoh, K.T.; Lo, J.; Chan, C.M.; Kien, F.; Escriou, N.; Tsao, S.W.; Nicholls, J.M.; Altmeyer, R.; Peiris, J.S.M.; et al. The M, E, and N structural proteins of the severe acute respiratory syndrome coronavirus are required for efficient assembly, trafficking, and release of virus-like particles. J. Virol. 2008, 82, 11318–11330. [Google Scholar] [CrossRef]
- Schoeman, D.; Fielding, B.C. Coronavirus envelope protein: Current knowledge. Virol. J. 2019, 16, 69. [Google Scholar] [CrossRef]
- Hartenian, E.; Nandakumar, D.; Lari, A.; Ly, M.; Tucker, J.M.; Glaunsinger, B.A. The molecular virology of coronaviruses. J. Biol. Chem. 2020, 295, 12910–12934. [Google Scholar] [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 18, 271–280. [Google Scholar] [CrossRef]
- Wadman, M.; Couzin-Frankel, J.; Kaiser, J.; Matacic, C. A rampage through the body. Science 2020, 368, 356–360. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2019, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Mao, R.; Qiu, Y.; He, J.S.; Tan, J.Y.; Li, X.H.; Liang, J.; Shen, J.; Zhu, L.R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatology 2020, 5, 667–678. [Google Scholar]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Spinato, G.; Fabbris, C.; Polesel, J.; Cazzador, D.; Borsetto, D.; Hopkins, C.; Boscolo-Rizzo, P. Alterations in smell or taste in mildly symptomatic outpatients with SARS-CoV-2 infection. JAMA 2020, 323, 2089–2209. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the cytokine Storm’in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- US Center for Disease Control and Prevntion. Available online: https://www.cdc.gov/vaccines/covid-19/index.html (accessed on 4 May 2021).
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Antinori, S.; Cossu, M.V.; Ridolfo, A.L.; Rech, R.; Bonazzetti, C.; Pagani, G.; Gubertini, G.; Coen, M.; Magni, C.; Castelli, A.; et al. Compassionate remdesivir treatment of severe Covid-19 pneumonia in intensive care unit (ICU) and Non-ICU patients: Clinical outcome and differences in post-treatment hospitalisation status. Pharmacol. Res. 2020, 158, 104899. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.X.; et al. Compassionate use of remdesivir for patients with severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Maldarelli, G.A.; Savage, M.; Mazur, S.; Oxford-Horrey, C.; Salvatore, M.; Marks, K.M. Remdesivir treatment for severe COVID-19 in third-trimester pregnancy: Case report and management discussion. Open Forum Infect. Dis. 2020, 7, ofaa345. [Google Scholar] [CrossRef] [PubMed]
- Dubert, M.; Visseaux, B.; Isernia, V.; Bouadma, L.; Deconinck, L.; Patrier, J.; Wicky, P.H.; Le Pluart, D.; Kramer, L.; Rioux, C.; et al. Case report study of the first five COVID-19 patients treated with remdesivir in France. Int. J. Infect. Dis. 2020, 98, 290–293. [Google Scholar] [CrossRef]
- Helleberg, M.; Niemann, C.U.; Moestrup, K.S.; Kirk, O.; Lebech, A.M.; Lane, C.; Lundgren, J. Persistent COVID-19 in an immunocompromised patient temporarily responsive to two courses of remdesivir therapy. J Infect. Dis. 2020, 222, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. ACTT-1 Study Group Members. Remdesivir for the Treatment of Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 days in patients with severe Covid-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Jafari, R.; Jonaidi-Jafari, N.; Dehghanpoor, F.; Saburi, A. Convalescent plasma therapy in a pregnant COVID-19 patient with a dramatic clinical and imaging response: A case report. World J. Radiol. 2020, 12, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Figlerowicz, M.; Mania, A.; Lubarski, K.; Lewandowska, Z.; Służewski, W.; Derwich, K.; Wachowiak, J.; Mazur-Melewska, K. First case of convalescent plasma transfusion in a child with COVID-19-associated severe aplastic anemia Transfus. Apher. Sci. 2020, 59, 102866. [Google Scholar] [CrossRef]
- Im, J.H.; Nahm, C.H.; Baek, J.H.; Kwon, H.Y.; Lee, J.S. Convalescent plasma therapy in coronavirus disease 2019: A case report and suggestions to overcome obstacles. J. Korean Med. Sci. 2020, 35, e239. [Google Scholar] [CrossRef]
- Xu, T.M.; Lin, B.; Chen, C.; Liu, L.G.; Xue, Y. Non-optimal effectiveness of convalescent plasma transfusion and hydroxychloroquine in treating COVID-19: A case report. Virol. J. 2020, 17, 80. [Google Scholar] [CrossRef]
- Ye, M.; Fu, D.; Ren, Y.; Wang, F.; Wang, D.; Zhang, F.; Xia, X.; Lv, T. Treatment with convalescent plasma for COVID-19 patients in Wuhan, China. J. Med. Virol. 2020, 92, 1890–1901. [Google Scholar] [CrossRef]
- Abdullah, H.M.; Hama-Ali, H.H.; Ahmed, S.N.; Ali, K.M.; Karadakhy, K.A.; Mahmood, S.O.; Mahmood, Z.H.; Amin, K.Q.H.; Atta, P.M.; Nuradeen, B.E.; et al. Severe refractory COVID-19 patients responding to convalescent plasma; A case series. Ann. Med. Surg. 2020, 56, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef]
- Fung, M.; Nambiar, A.; Pandey, S.; Aldrich, J.M.; Teraoka, J.; Freise, C.; Roberts, J.; Chandran, S.; Hays, S.R.; Bainbridge, E.; et al. Treatment of immunocompromised COVID-19 patients with convalescent plasma. Transpl. Infect. Dis. 2020, e13477. [Google Scholar] [CrossRef]
- Wang, M.; Yang, X.; Yang, F.; Zhu, X.; Sun, Z.; Bao, P.; Yan, Y. Convalescent plasma therapy in critically ill coronavirus disease 2019 patients with persistently positive nucleic acid test, case series report. Medicine 2020, 99, e21596. [Google Scholar] [CrossRef] [PubMed]
- Olivares-Gazca, J.C.; Priesca-Marín, J.M.; Ojeda-Laguna, M.; Garces-Eisele, J.; Soto-Olvera, S.; Palacios-Alonso, A.; Izquierdo-Vega, J.; Chacon-Cano, R.; Arizpe-Bravo, D.; López-Trujillo, M.A.; et al. Infusion of convalescent plasma is associated with clinical improvement in critically ill patients with COVID-19: A pilot study. Rev. Invest. Clin. 2020, 72, 159–164. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Ahn, J.Y.; Sohn, Y.; Lee, S.H.; Cho, Y.; Hyun, J.H.; Baek, Y.J.; Jeong, S.J.; Kim, J.H.; Ku, N.S.; Yeom, J.S.; et al. Use of convalescent plasma therapy in two COVID-19 patients with acute respiratory distress syndrome in Korea. J. Korean Med. Sci. 2020, 35, e149. [Google Scholar] [CrossRef]
- Zeng, Q.L.; Yu, Z.J.; Gou, J.J.; Li, G.M.; Ma, S.H.; Zhang, G.F.; Xu, J.H.; Lin, W.B.; Cui, G.L.; Zhang, M.M.; et al. Effect of convalescent plasma therapy on viral shedding and survival in patients with coronavirus disease 2019. J. Infect. Dis. 2020, 222, 38–43. [Google Scholar] [CrossRef]
- Salazar, E.; Perez, K.K.; Ashraf, M.; Chen, J.; Castillo, B.; Christensen, P.A.; Eubank, T.; Bernard, D.W.; Eagar, T.N.; Long, S.W.; et al. Treatment of coronavirus disease 2019 (COVID-19) patients with convalescent plasma. Am. J. Pathol. 2020, 190, 1680–1690. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of convalescent plasma therapy on time to clinical improvement in patients with severe and life-threatening COVID-19: A randomized clinical trial. JAMA 2020, 324, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wong, R.; Soo, Y.O.Y.; Wong, W.S.; Lee, C.K.; Ng, M.H.L.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 24, 44–46. [Google Scholar] [CrossRef]
- Park, W.H. Therapeutic use of antipoliomyelitits serum in preparalytic cases of poliomyelitis. JAMA 1932, 99, 1050–1053. [Google Scholar] [CrossRef]
- Park, W.H.; Freeman, R.G. The prophylactic use of measles convalescent serum. JAMA 1926, 87, 556–558. [Google Scholar] [CrossRef]
- Rambar, A.C. Mumps: Use of convalescent serum in the treatment and prophylaxis of orchitis. Am. J. Dis. Child. 1946, 71, 1–13. [Google Scholar] [CrossRef]
- Stinebaugh, B.J.; Schloeder, F.X.; Johnson, K.M.; Mackenzie, R.B.; Entwisle, G.; De Alba, E. Bolivian hemorrhagic fever: A report of four cases. Am. J. Med. 1966, 40, 217–230. [Google Scholar] [CrossRef]
- Frame, J.D.; Verbrugge, G.P.; Gill, R.G.; Pinneo, L. The use of Lassa fever convalescent plasma in Nigeria. Trans. R. Soc. Trop. Med. Hyg. 1984, 78, 319–324. [Google Scholar] [CrossRef]
- Ruggiero, H.A.; Milani, H.A.; Barri, A.; Val, A.; Maglio, F.; Astarloa, L.; Milani, H.L.; Tallone, J.C. Treatment of Argentine hemorrhagic fever with convalescent’s plasma. 4433 cases. Presse Med. 1986, 15, 2239–2242. (In French) [Google Scholar]
- Mupapa, K.; Massamba, M.; Kibadi, K.; Kuvula, K.; Bwaka, A.; Kipasa, M.; Colebunders, R.; Muyembe-Tamfum, J.J. Treatment of Ebola hemorrhagic fever with blood transfusions from convalescent patients. J. Infect. Dis. 1999, 179 (Suppl. 1), 18–23. [Google Scholar] [CrossRef]
- Luke, T.C.; Casadevall, A.; Watowich, S.J.; Hoffman, S.L.; Beigel, J.H.; Burgess, T.H. Hark back: Passive immunotherapy for influenza and other serious infections. Crit. Care Med. 2010, 38, 66–73. [Google Scholar] [CrossRef]
- Zhou, B.; Zhong, N.; Guan, Y. Treatment with convalescent plasma for influenza A (H5N1) infection. N. Engl. J. Med. 2007, 357, 1450–1451. [Google Scholar] [CrossRef]
- Hung, I.F.; To, K.K.; Lee, C.K.; Lee, K.L.; Chan, K.; Yan, W.W.; Liu, R.; Watt, C.L.; Chan, W.M.; Lai, K.Y.; et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin. Infect. Dis. 2011, 52, 447–456. [Google Scholar] [CrossRef]
- Zhang, B.; Liu, S.; Tan, T.; Huang, W.; Dong, Y.; Chen, L.; Chen, Q.; Zhang, L.; Zhong, Q.; Zhang, X.; et al. Treatment with convalescent plasma for critically ill patients with severe acute respiratory syndrome coronavirus 2 infection. Chest. 2020, 158, e9–e13. [Google Scholar] [CrossRef]
- Agostini, M.L.; Andres, E.L.; Sims, A.C.; Graham, R.L.; Sheahan, T.P.; Lu, X.; Smith, E.C.; Case, J.B.; Feng, J.Y.; Jordan, R.; et al. Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease. Mbio 2018, 9, e00221-18. [Google Scholar] [CrossRef]
- Warren, T.; Jordan, R.; Lo, M.; Soloveva, V.; Ray, A.; Bannister, R.; Mackman, R.; Perron, M.; Stray, K.; Feng, J.; et al. Nucleotide prodrug GS-5734 is a broad-spectrum filovirus inhibitor that provides complete therapeutic protection against the development of Ebola virus disease (EVD) in infected non-human primates. Open Forum Infect. Dis. 2015, 2 (Suppl. 1), LB-2. [Google Scholar] [CrossRef]
- Warren, T.K.; Jordan, R.; Lo, M.K.; Ray, A.S.; Mackman, R.L.; Soloveva, V.; Siegel, D.; Perron, M.; Bannister, R.; Hui, H.C.; et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016, 531, 381–385. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O.; et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat. Comm. 2020, 11, 1–4. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Baum, A.; Fulton, B.O.; Wloga, E.; Copin, R.; Pascal, K.E.; Russo, V.; Giordano, S.; Lanza, K.; Negron, N.; Ni, M.; et al. Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies. Science 2020, 369, 1014–1018. [Google Scholar] [CrossRef]
- Hansen, J.; Baum, A.; Pascal, K.E.; Russo, V.; Giordano, S.; Wloga, E.; Fulton, B.O.; Yan, Y.; Koon, K.; Patel, K.; et al. Studies in humanized mice and convalescent humans yield a SARS-CoV-2 antibody cocktail. Science 2020, 369, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Baum, A.; Ajithdoss, D.; Copin, R.; Zhou, A.; Lanza, K.; Negron, N.; Ni, M.; Wei, Y.; Mohammadi, K.; Musser, B.; et al. REGN-COV2 antibodies prevent and treat SARS-CoV-2 infection in rhesus macaques and hamsters. Science 2020, 370, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.M.; Cheng, V.C.C.; Hung, I.F.N.; Wong, M.M.L.; Chan, K.H.; Chan, K.S.; Kao, R.Y.T.; Poon, L.L.M.; Wong, C.L.P.; Guan, Y.; et al. Role of lopinavir/ritonavir in the treatment of SARS: Initial virological and clinical findings. Thorax 2004, 59, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.; Lai, S.T.; Chu, C.M.; Tsui, E.; Tam, C.Y.; Wong, M.M.L.; Tse, M.W.; Que, T.L.; Peiris, J.S.M.; Sung, J.; et al. Treatment of severe acute respiratory syndrome with lopinavir/ritonavir: A multicentre retrospective matched cohort study. Hong Kong Med. J. 2003, 9, 399–406. [Google Scholar] [PubMed]
- Ye, X.T.; Luo, Y.L.; Xia, S.C.; Sun, Q.F.; Ding, J.G.; Zhou, Y.; Chen, W.; Wang, X.F.; Zhang, W.W.; Du, W.J.; et al. Clinical efficacy of lopinavir/ritonavir in the treatment of Coronavirus disease 2019. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3390–3396. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Boriskin, Y.S.; Leneva, I.A.; Pecheur, E.I.; Polyak, S.J. Arbidol: A broad-spectrum antiviral compound that blocks viral fusion. Curr. Med. Chem. 2008, 15, 997–1005. [Google Scholar] [CrossRef]
- Pécheur, E.I.; Borisevich, V.; Halfmann, P.; Morrey, J.D.; Smee, D.F.; Prichard, M.; Mire, C.E.; Kawaoka, Y.; Geisbert, T.W.; Polyak, S.J. The synthetic antiviral drug arbidol inhibits globally prevalent pathogenic viruses. J. Virol. 2016, 90, 3086–3092. [Google Scholar] [CrossRef]
- Blaising, J.; Polyak, S.J.; Pécheur, E.I. Arbidol as a broad-spectrum antiviral: An update. Antivir. Res. 2014, 107, 84–94. [Google Scholar] [CrossRef]
- Dong, L.; Hu, S.; Gao, J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov. Ther. 2020, 14, 58–60. [Google Scholar] [CrossRef]
- Deng, L.; Li, C.; Zeng, Q.; Liu, X.; Li, X.; Zhang, H.; Hong, Z.; Xia, J. Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study. J. Infect. 2020, 81, e1–e5. [Google Scholar] [CrossRef]
- Zhu, Z.; Lu, Z.; Xu, T.; Chen, C.; Yang, G.; Zha, T.; Lu, J.; Xue, Y. Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19. J. Infect. 2020, 81, e21–e23. [Google Scholar] [CrossRef]
- Chen, W.; Yao, M.; Fang, Z.; Lv, X.; Deng, M.; Wu, Z. A study on clinical effect of Arbidol combined with adjuvant therapy on COVID-19. J. Med. Virol. 2020, 92, 2702–2708. [Google Scholar] [CrossRef]
- Li, Y.; Xie, Z.; Lin, W.; Cai, W.; Wen, C.; Guan, Y.; Mo, X.; Wang, J.; Wang, Y.; Peng, P.; et al. Efficacy and safety of lopinavir/ritonavir or arbidol in adult patients with mild/moderate COVID-19: An exploratory randomized controlled trial. Med 2020, 1, 105–113. [Google Scholar] [CrossRef]
- Lian, N.; Xie, H.; Lin, S.; Huang, J.; Zhao, J.; Lin, Q. Umifenovir treatment is not associated with improved outcomes in patients with coronavirus disease 2019: A retrospective study. Clin. Microbiol. Infect. 2020, 26, 917–921. [Google Scholar] [CrossRef]
- Chen, C.; Huang, J.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; Luo, Y.; Zhang, J.; et al. Favipiravir versus arbidol for COVID-19: A randomized clinical trial. MedRxiv 2020. [Google Scholar] [CrossRef]
- Oestereich, L.; Lüdtke, A.; Wurr, S.; Rieger, T.; Muñoz-Fontela, C.; Günther, S. Successful treatment of advanced Ebola virus infection with T-705 (favipiravir) in a small animal model. Antiviral. Res. 2014, 105, 17–21. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef]
- Li, X.; Burton, E.M.; Bhaduri-McIntosh, S. Chloroquine triggers Epstein-Barr virus replication through phosphorylation of KAP1/TRIM28 in Burkitt lymphoma cells. PLoS Pathog. 2017, 13, e1006249. [Google Scholar] [CrossRef]
- Li, C.; Zhu, X.; Ji, X.; Quanquin, N.; Deng, Y.Q.; Tian, M. Chloroquine, a FDA-approved drug, prevents Zika virus infection and its associated congenital microcephaly in mice. EBioMedicine 2017, 24, 189–194. [Google Scholar] [CrossRef]
- Moellgaard, H. The theoretical basis of the sanocrysin treatment of tuberculosis. Br. Med. J. 1925, 1, 643–647. [Google Scholar] [CrossRef][Green Version]
- Falzarano, D.; Safronetz, D.; Prescott, J.; Marzi, A.; Feldmann, F.; Feldmann, H. Lack of protection against ebola virus from chloroquine in mice and hamsters. Emerg. Infect. Dis. 2015, 21, 1065–1067. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.C.; Castro, L.A.; Fonseca, B.A. Chloroquine use improves dengue-related symptoms. Mem. Inst. Oswaldo Cruz. 2013, 108, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.F.; Lin, Y.S.; Huang, N.C.; Yu, C.Y.; Tsai, W.L.; Chen, J.J.; Kubota, T.; Matsuoka, M.; Chen, S.R.; Yang, C.S.; et al. Hydroxychloroquine-inhibited dengue virus is associated with host defense machinery. J. Interferon Cytokine Res. 2015, 35, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discov. 2020, 6, 16. [Google Scholar] [CrossRef]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends 2020, 14, 72–73. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; Dupont, H.T.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical tria. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, R.G.; et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A randomized trial of hydroxychloroquine as postexposure prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: Open label, randomised controlled trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Borba, M.G.S.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Brito, M.; Mourão, M.P.G.; Brito-Sousa, J.D.; Baía-da-Silva, D.; Guerra, M.V.F.; et al. Effect of high vs low doses of chloroquine diphosphate as adjunctive therapy for patients hospitalized with severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection: A randomized clinical trial. JAMA Netw. Open 2020, 3, e208857. [Google Scholar] [CrossRef]
- FDA. Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Chloroquine and Hydroxychloroquine. 2020. Available online: https://www.fda.gov/media/138945/download (accessed on 18 April 2021).
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef] [PubMed]
- Filocamo, G.; Mangioni, D.; Tagliabue, P.; Aliberti, S.; Costantino, G.; Minoia, F.; Bandera, A. Use of anakinra in severe COVID-19: A case report. Int. J. Infect. Dis. 2020, 96, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Day, J.W.; Fox, T.A.; Halsey, R.; Carpenter, B.; Kottaridis, P.D. Interleukin-1 blockade with anakinra in acute leukaemia patients with severe COVID-19 pneumonia appears safe and may result in clinical improvement. Br. J. Haematol. 2020, 190, e80–e83. [Google Scholar] [CrossRef]
- Franzetti, M.; Pozzetti, U.; Carugati, M.; Pandolfo, A.; Molteni, C.; Faccioli, P.; Castaldo, G.; Longoni, E.; Ormas, V.; Iemoli, E.; et al. Interleukin-1 receptor antagonist anakinra in association with remdesivir in severe COVID-19: A case report. Int. J. Infect. Dis. 2020, 97, 215–218. [Google Scholar] [CrossRef]
- Karadeniz, H.; Yamak, B.A.; Özger, H.S.; Sezenöz, B.; Tufan, A.; Emmi, G. Anakinra for the treatment of COVID-19-associated pericarditis: A case report. Cardiovasc. Drugs Ther. 2020, 34, 883–885. [Google Scholar] [CrossRef]
- Nemchand, P.; Tahir, H.; Mediwake, R.; Lee, J. Cytokine storm and use of anakinra in a patient with COVID-19. BMJ Case Rep. 2020, 13, e237525. [Google Scholar] [CrossRef]
- Navarro-Millán, I.; Sattui, S.E.; Lakhanpal, A.; Zisa, D.; Siegel, C.H.; Crow, M.K. Use of anakinra to prevent mechanical ventilation in severe COVID-19: A case series. Arthritis Rheumatol. 2020, 72, 1990–1997. [Google Scholar] [CrossRef]
- Haigh, K.; Syrimi, Z.J.; Irvine, S.; Blanchard, T.J.; Pervaiz, M.S.; Toth, A.G.; Ratcliffe, L. Hyperinflammation with COVID-19: The key to patient deterioration? Clin. Infect. Pract. 2020, 100033. [Google Scholar] [CrossRef]
- Bozzi, G.; Mangioni, D.; Minoia, F.; Aliberti, S.; Grasselli, G.; Barbetta, L.; Castelli, V.; Palomba, E.; Alagna, L.; Lombardi, A.; et al. Anakinra combined with methylprednisolone in patients with severe COVID-19 pneumonia and hyperinflammation: An observational cohort study. J. Allergy Clin. Immunol. 2021, 147, 561–566. [Google Scholar] [CrossRef]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Din, C.T.; Boffini, N.; et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e325–e331. [Google Scholar] [CrossRef]
- Kooistra, E.J.; Waalders, N.J.; Grondman, I.; Janssen, N.A.; de Nooijer, A.H.; Netea, M.G.; van de Veerdonk, F.L.; Ewalds, E.; van der Hoeven, J.G.; Kox, M.; et al. Anakinra treatment in critically ill COVID-19 patients: A prospective cohort study. Crit. Care. 2020, 24, 688. [Google Scholar] [CrossRef]
- Balkhair, A.; Al-Zakwani, I.; Al Busaidi, M.; Al-Khirbash, A.; Al Mubaihsi, S.; BaTaher, H.; Al Aghbari, J.; Al Busaidi, I.; Al Kindi, M.; Baawain, S.; et al. Anakinra in hospitalized patients with severe COVID-19 pneumonia requiring oxygen therapy: Results of a prospective, open-label, interventional study. Int. J. Infect. Dis. 2021, 103, 288–296. [Google Scholar] [CrossRef]
- So, C.; Ro, S.; Murakami, M.; Imai, R.; Jinta, T. High-dose, short-term corticosteroids for ARDS caused by COVID-19: A case series. Respirol. Case Rep. 2020, 8, e00596. [Google Scholar] [CrossRef]
- Nelson, B.C.; Laracy, J.; Shoucri, S.; Dietz, D.; Zucker, J.; Patel, N.; Sobieszczyk, M.E.; Kubin, C.J.; Gomez-Simmonds, A. Clinical outcomes associated with methylprednisolone in mechanically ventilated patients with COVID-19. Clin. Infect. Dis. 2020, ciaa1163. [Google Scholar] [CrossRef]
- Liu, J.; Zheng, X.; Huang, Y.; Shan, H.; Huang, J. Successful use of methylprednisolone for treating severe COVID-19. J. Allergy Clin. Immunol. 2020, 146, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Murohashi, K.; Hagiwara, E.; Kitayama, T.; Yamaya, T.; Higa, K.; Sato, Y.; Otoshi, R.; Shintani, R.; Okabayashi, H.; Ikeda, S.; et al. Outcome of early-stage combination treatment with favipiravir and methylprednisolone for severe COVID-19 pneumonia: A report of 11 cases. Respir. Investig. 2020, 58, 430–434. [Google Scholar] [CrossRef]
- Hassan, M.E.; Hasan, H.M.; Sridharan, K.; Elkady, A.; ElSeirafi, M.M. Dexamethasone in severe COVID-19 infection: A case series. Resp. Med. Case Rep. 2020, 31, 101205. [Google Scholar] [CrossRef] [PubMed]
- Edalatifard, M.; Akhtari, M.; Salehi, M.; Naderi, Z.; Jamshidi, A.; Mostafaei, S.; Najafizadeh, S.R.; Farhadi, E.; Jalili, N.; Esfahani, M.; et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: Results from a randomised controlled clinical trial. Eur. Respir. J. 2020, 56, 2002808. [Google Scholar] [CrossRef] [PubMed]
- Jeronimo, C.M.P.; Farias, M.E.L.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Safe, I.P.; Borba, M.G.S.; Netto, R.L.A.; Maciel, A.B.S.; et al. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized With Coronavirus Disease 2019 (COVID-19; Metcovid): A Randomized, Double-blind, Phase IIb, Placebo-controlled Trial. Clin. Infect. Dis. 2020, ciaa1177. [Google Scholar] [CrossRef]
- Selvaraj, V.; Dapaah-Afriyie, K.; Finn, A.; Flanigan, T.P. Short-term dexamethasone in Sars-CoV-2 patients. RI Med. J. 2020, 103, 39–43. [Google Scholar]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Cano, E.J.; Fuentes, X.F.; Campioli, C.C.; O’Horo, J.C.; Saleh, O.A.; Odeyemi, Y.; Yadav, H.; Temesgen, Z. Impact of corticosteroids in COVID-19 outcomes: Systematic review and meta-analysis. Chest 2021, 159, 1019–1040. [Google Scholar] [CrossRef]
- Michot, J.M.; Albiges, L.; Chaput, N.; Saada, V.; Pommeret, F.; Griscelli, F.; Balleyguier, C.; Besse, B.; Marabelle, A.; Netzer, F.; et al. Tocilizumab, an anti-IL-6 receptor antibody, to treat COVID-19-related respiratory failure: A case report. Ann. Oncol. 2020, 31, 961–964. [Google Scholar] [CrossRef]
- Wang, L.; Peng, X.; Wang, Z.H.; Cai, J.; Zhou, F.C. Tocilizumab in the treatment of a critical COVID-19 patient: A case report. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 5783–5787. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Mauro, I.; De Blasio, E.; Crispo, A.; Del Gaudio, A.; Bimonte, S.; Cuomo, A.; Ascierto, P.A. Rapid and impressive response to a combined treatment with single-dose tocilizumab and niv in a patient with COVID-19 pneumonia/ARDS. Medicina 2020, 56, 377. [Google Scholar] [CrossRef]
- Dastan, F.; Nadji, S.A.; Saffaei, A.; Tabarsi, P. Tocilizumab administration in a refractory case of COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106043. [Google Scholar] [CrossRef] [PubMed]
- Dastan, F.; Saffaei, A.; Haseli, S.; Marjani, M.; Moniri, A.; Abtahian, Z.; Abedini, A.; Kiani, A.; Seifi, S.; Jammati, H.; et al. Promising effects of tocilizumab in COVID-19: A non-controlled, prospective clinical trial. Int. Immunopharmacol. 2020, 88, 106869. [Google Scholar] [CrossRef]
- Douedi, S.; Chaudhri, M.; Miskoff, J. Anti-interleukin-6 monoclonal antibody for cytokine storm in COVID-19. Ann. Thorac. Med. 2020, 15, 171–173. [Google Scholar] [CrossRef] [PubMed]
- ElSeirafi, M.M.; Hasan, H.M.; Sridharan, K.; Zamoori, A.; Alkhawaja, S.; Pasha, S.A.A. Efficacy and safety of tocilizumab in critically ill adults with COVID-19 infection in Bahrain: A report of 5 cases. Respir. Med. Case Rep. 2020, 30, 101139. [Google Scholar] [CrossRef]
- Radbel, J.; Narayanan, N.; Bhatt, P.J. Use of tocilizumab for COVID-19-induced cytokine release syndrome: A cautionary case report. Chest. 2020, 158, e15–e19. [Google Scholar] [CrossRef]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab treatment in COVID-19: A single center experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef]
- West, T.A.; Malik, S.; Nalpantidis, A.; Tran, T.; Cannon, C.; Bhonagiri, D.; Chan, K.; Cheong, E.; Wan Sai Cheong, J.; Cheung, W.; et al. Tocilizumab for severe COVID-19 pneumonia: Case series of 5 Australian patients. Int. J. Rheum. Dis. 2020, 23, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Hitawala, A.; Kumar, S.; Gopalakrishna, K.V. Early Use of Tocilizumab May Prevent Clinical Deterioration in Select COVID-19 Patients: A Case Series. Cureus 2020, 12, e9187. [Google Scholar] [CrossRef]
- Tadepalli, S.; Vanjarapu, J.M.R.; De Dona, A.; Cheriyath, P.; Nookala, V. The role of interleukin-6 inhibitors in the treatment of COVID-19 infections: A case series. Cureus 2020, 12, e8631. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Chen, V.; Shannon, C.P.; Wei, X.S.; Xiang, X.; Wang, X.; Wang, Z.H.; Tebbutt, S.J.; Kollmann, T.R.; Fish, E.N. Interferon-α2b Treatment for COVID-19. Front. Immunol. 2020, 11, 1061. [Google Scholar] [CrossRef]
- Dastan, F.; Nadji, S.A.; Saffaei, A.; Marjani, M.; Moniri, A.; Jamaati, H.; Hashemian, S.M.; Baghaei, P.; Abedini, A.; Varahram, M.; et al. Subcutaneous administration of interferon beta-1a for COVID-19: A non-controlled prospective trial. Int. Immunopharmacol. 2020, 85, 106688. [Google Scholar] [CrossRef]
- Davoudi-Monfared, E.; Rahmani, H.; Khalili, H.; Hajiabdolbaghi, M.; Salehi, M.; Abbasian, L.; Kazemzadeh, H.; Yekaninejad, M.S. A randomized clinical trial of the efficacy and safety of interferon β-1a in treatment of severe COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01061-20. [Google Scholar] [CrossRef]
- Rahmani, H.; Davoudi-Monfared, E.; Nourian, A.; Khalili, H.; Hajizadeh, N.; Jalalabadi, N.Z.; Fazeli, M.R.; Ghazaeian, M.; Yekaninejad, M.S. Interferon β-1b in treatment of severe COVID-19: A randomized clinical trial. Int. Immunopharmacol. 2020, 88, 106903. [Google Scholar] [CrossRef] [PubMed]
- Ghia, S.; Bhatt, H.; Lazar, M. Role of Tissue Plasminogen Activator for Diffuse Pulmonary Microemboli in Coronavirus Disease 2019 Patient. J Cardiothorac. Vasc. Anesth. 2020, 35, 2137–2139. [Google Scholar] [CrossRef]
- Wang, J.; Hajizadeh, N.; Moore, E.E.; McIntyre, R.C.; Moore, P.K.; Veress, L.A. Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): A case series. J. Thromb. Haemost. 2020, 18, 1752–1755. [Google Scholar] [CrossRef] [PubMed]
- Barrett, C.D.; Oren-Grinberg, A.; Chao, E.; Moraco, A.H.; Martin, M.J.; Reddy, S.H.; Ilg, A.M.; Jhunjhunwala, R.; Uribe, M.; Moore, H.B.; et al. Rescue therapy for severe COVID-19 associated acute respiratory distress syndrome (ARDS) with tissue plasminogen activator (tPA): A case series Rescue therapy for severe COVID-19-associated acute respiratory distress syndrome with tissue plasminogen activator: A case series. J. Trauma. Acute Care Surg. 2020, 89, 453–457. [Google Scholar] [CrossRef]
- LeVine, S.; Dhakal, G.P.; Penjor, T.; Chuki, P.; Namgyal, K.; Watts, M. Case report: The first case of COVID-19 in Bhutan. Am. J. Trop. Med. Hyg. 2020, 102, 1205–1207. [Google Scholar] [CrossRef]
- Mohtadi, N.; Ghaysouri, A.; Shirazi, S.; Shafiee, E.; Bastani, E.; Kokhazadeh, T.; Tavan, H. Recovery of severely ill COVID-19 patients by intravenous immunoglobulin (IVIG) treatment: A case series. Virology 2020, 548, 1–5. [Google Scholar] [CrossRef]
- Cao, W.; Liu, X.; Bai, T.; Fan, H.; Hong, K.; Song, H.; Han, Y.; Lin, L.; Ruan, L.; Li, T. High-dose intravenous immunoglobulin as a therapeutic option for deteriorating patients with coronavirus disease 2019. Open Forum Infect. Dis. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Zhou, C.; He, P.; Huang, S.; Duan, Y.; Wang, X.; Lin, K.; Zhou, C.; Zhang, X.; Zha, Y. Successful treatment with plasma exchange followed by intravenous immunoglobulin in a critically ill patient with COVID-19. Int. J. Antimicrob. Agents 2020, 56, 105974. [Google Scholar] [CrossRef]
- Yamamoto, M.; Matsuyama, S.; Li, X.; Takeda, M.; Kawaguchi, Y.; Inoue, J.I.; Matsuda, Z. Identification of nafamostat as a potent inhibitor of Middle East respiratory syndrome coronavirus S protein-mediated membrane fusion using the split-protein-based cell-cell fusion assay. Antimicrob. Agents Chemother. 2016, 60, 6532–6539. [Google Scholar] [CrossRef]
- Inoue, J.; Yamamoto, M. Identification of an Existing Japanese Pancreatitis Drug, Nafamostat, which is Expected to Prevent the Transmission of New Coronavirus Infection (COVID-19). BioRxiv 2020. Available online: https://www.u-tokyo.ac.jp/focus/en/articles/z0508_00083.html (accessed on 26 May 2021).
- Jang, S.; Rhee, J.Y. Three cases of treatment with nafamostat in elderly patients with COVID-19 pneumonia who need oxygen therapy. Int. J. Infect. Dis. 2020, 96, 500–502. [Google Scholar] [CrossRef]
- Doi, K.; Ikeda, M.; Hayase, N.; Moriya, K.; Morimura, N. Nafamostat mesylate treatment in combination with favipiravir for patients critically ill with Covid-19: A case series. Crit Care. 2020, 24, 392. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Jeon, S.; Shin, H.Y.; Kim, M.J.; Seong, Y.M.; Lee, W.J.; Choe, K.W.; Kang, Y.M.; Lee, B.; Park, S.J. Case of the Index Patient Who Caused Tertiary Transmission of COVID-19 Infection in Korea: The Application of Lopinavir/Ritonavir for the Treatment of COVID-19 Infected Pneumonia Monitored by Quantitative RT-PCR. J. Korean Med. Sci. 2020, 35, e79. [Google Scholar] [CrossRef] [PubMed]
- Joumaa, H.; Regard, L.; Carlier, N.; Chassagnon, G.; Alabadan, E.; Canouï, E.; L’honneur, A.; Rozenberg, F.; Burgel, P.R.; Roche, N. A severe COVID-19 despite ongoing treatment with Lopinavir-Ritonavir. Respir. Med. Res. 2020, 78, 100780. [Google Scholar] [CrossRef] [PubMed]
- Mazan, P.; Lesiak, A.; Skibiñska, M.; Kamerys, J.; Czajkowski, R.; Owczarek, W.; Narbutt, J. Maculopapular rash in COVID-19 patient treated with lopinavir/ritonavir. Postepy. Dermatol. Alergol. 2020, 37, 435–437. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Lee, Y.L.; Chen, C.P.; Lin, Y.C.; Liu, C.E.; Liao, C.H.; Cheng, S.H. Lopinavir/ritonavir did not shorten the duration of SARS CoV-2 shedding in patients with mild pneumonia in Taiwan. J. Microbiol. Immunol. Infect. 2020, 53, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Shimode, K.; Hoshiyama, T.; Takayama, Y.; Yamaoka, K. Three novel COVID-19 pneumonia cases successfully treated with lopinavir/ritonavir. Front. Med. 2020, 7, 241. [Google Scholar] [CrossRef]
- Kim, Y.; Kwon, O.; Paek, J.H.; Park, W.Y.; Jin, K.; Hyun, M.; Lee, J.Y.; Lee, J.Y.; Kim, H.A.; Han, S. Two distinct cases with COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 2269–2275. [Google Scholar] [CrossRef]
- Iancu, G.M.; Solomon, A.; Birlutiu, V. Viral exanthema as manifestation of SARS-CoV-2 infection: A case report. Medicine 2020, 99, e21810. [Google Scholar] [CrossRef]
- Hong, S.I.; Ryu, B.H.; Chong, Y.P.; Lee, S.; Kim, S.; Kim, H.C.; Hong, K.W.; Bae, I.G.; Cho, O.H. Five severe COVID-19 pneumonia patients treated with triple combination therapy with lopinavir/ritonavir, hydroxychloroquine, and interferon β-1b. Int. J. Antimicrob. Agents 2020, 56, 106052. [Google Scholar] [CrossRef]
- Hung, I.F.N.; Lung, K.C.; Tso, E.Y.K.; Liu, R.; Chung, T.W.H.; Chu, M.Y.; Ng, Y.Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet. 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Ahn, B.Y.; Kang, C.K.; Do Seo, J.; Choe, P.G.; Song, S.H.; Park, W.B.; Park, S.W.; Kim, N.J.; Oh, M.D. A case of breakthrough COVID-19 during hydroxychloroquine maintenance. J. Korean. Med. Sci. 2020, 35, e231. [Google Scholar] [CrossRef]
- Fontana, F.; Alfano, G.; Mori, G.; Amurri, A.; Tei, L.; Ballestri, M.; Leonelli, M.; Facchini, F.; Damiano, F.; Magistroni, R.; et al. Covid-19 pneumonia in a kidney transplant recipient successfully treated with tocilizumab and hydroxychloroquine. Am. J. Transplant. 2020, 20, 1902–1906. [Google Scholar] [CrossRef]
- Ng, K.K.; Ng, M.K.; Zhyvotovska, A.; Singh, S.; Shevde, K. Acute respiratory failure secondary to COVID-19 viral pneumonia managed with hydroxychloroquine/azithromycin treatment. Cureus 2020, 12, e8268. [Google Scholar] [CrossRef] [PubMed]
- Albani, F.; Fusina, F.; Giovannini, A.; Ferretti, P.; Granato, A.; Prezioso, C.; Divizia, D.; Sabaini, A.; Marri, M.; Malpetti, E.; et al. Impact of azithromycin and/or hydroxychloroquine on hospital mortality in COVID-19. J. Clin. Med. 2020, 9, E2800. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.K.; Purdy, A.G.; Ender, P.T. COVID-19 Pneumonia in Patients on Chronic Hydroxychloroquine Therapy: Three Cases of COVID-19 Pneumonia. Case Rep. Infect. Dis. 2020, 8822753. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.Y.; Lu, S.D.; Ye, X.; Cao, M.Y.; Xu, G.D.; Yu, Q.; Qian, J.X.; Zeng, G. Combined treatment of tocilizumab and chloroquine on severe COVID-19: A case report. QJM Int. J. Med. 2020, 113, 569–572. [Google Scholar] [CrossRef]
- Furtado, R.H.; Berwanger, O.; Fonseca, H.A.; Corrêa, T.D.; Ferraz, L.R.; Lapa, M.G.; Zampieri, F.G.; Veiga, V.C.; Azevedo, L.C.; Rosa, R.G.; et al. Azithromycin in addition to standard of care versus standard of care alone in the treatment of patients admitted to the hospital with severe COVID-19 in Brazil (COALITION II): A randomised clinical trial. Lancet 2020, 396, 959–967. [Google Scholar] [CrossRef]
- Cala-García, J.D.; Sierra-Bretón, J.D.; Cavelier-Baiz, J.E.; Faccini-Martínez, Á.A.; Pérez-Díaz, C.E. Recovery of COVID-19 acute respiratory distress syndrome with tocilizumab: Successful outcome in two critically ill patients. Immunotherapy 2020, 12, 1127–1132. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- WHO. Available online: https://extranet.who.int/pqweb/vaccines/covid-19-vaccines (accessed on 23 May 2021).
- Dehghani-Samani, A.; Kamali, M.; Hoseinzadeh-Chahkandak, F. The Role of vitamins on the prevention and/or treatment of COVID-19 infection; A Systematic Review. Modern Care J. 2020, 17. [Google Scholar] [CrossRef]
- Ren, J.L.; Zhang, A.H.; Wang, X.J. Traditional Chinese medicine for COVID-19 treatment. Pharmacol. Res. 2020, 155, 104743. [Google Scholar] [CrossRef]
- Waqas Khan, H.M.; Parikh, N.; Megala, S.M.; Predeteanu, G.S. Unusual Early Recovery of a Critical COVID-19 Patient After Administration of Intravenous Vitamin C. Am. J. Case Rep. 2020, 21, e925521. [Google Scholar] [CrossRef]
- Kumari, P.; Dembra, S.; Dembra, P.; Bhawna, F.; Gul, A.; Ali, B.; Sohail, H.; Kumar, B.; Memon, M.K.; Rizwan, A. The Role of Vitamin C as Adjuvant Therapy in COVID-19. Cureus 2020, 12, e11779. [Google Scholar] [CrossRef]
- Hiedra, R.; Lo, K.B.; Elbashabsheh, M.; Gul, F.; Wright, R.M.; Albano, J.; Azmaiparashvili, Z.; Patarroyo Aponte, G. The use of IV vitamin C for patients with COVID-19: A case series. Expert Rev. Anti-Infect. Ther. 2020, 18, 1259–1261. [Google Scholar] [CrossRef]
- Gao, D.; Xu, M.; Wang, G.; Lv, J.; Ma, X.; Guo, Y.; Zhang, D.; Yang, H.; Jiang, W.; Deng, F.; et al. The efficiency and safety of high-dose vitamin C in patients with COVID-19: A retrospective cohort study. Aging 2021, 13, 7020. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Rao, X.; Li, Y.; Zhu, Y.; Liu, F.; Guo, G.; Luo, G.; Meng, Z.; De Backer, D.; Xiang, H.; et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 2021, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Creagan, E.T.; Moertel, C.G.; O’Fallon, J.R.; Schutt, A.J.; O’Connell, M.J.; Rubin, J.; Frytak, S. Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer: A controlled trial. N. Engl. J. Med. 1979, 301, 687–690. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C.G.; Fleming, T.R.; Creagan, E.T.; Rubin, J.; O’Connell, M.J.; Ames, M.M. High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy: A randomized double-blind comparison. N. Engl. J. Med. 1985, 312, 137–141. [Google Scholar] [CrossRef]
- JamaliMoghadamSiahkali, S.; Zarezade, B.; Koolaji, S.; SeyedAlinaghi, S.; Zendehdel, A.; Tabarestani, M.; Moghadam, E.S.; Abbasian, L.; Manshadi, S.A.D.; Salehi, M.; et al. Safety and effectiveness of high-dose vitamin C in patients with COVID-19: A randomized open-label clinical trial. Eur. J. Med. Res. 2021, 26, 1–9. [Google Scholar] [CrossRef]
- Smolders, J.; van den Ouweland, J.; Geven, C.; Pickkers, P.; Kox, M. Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence. Metabolism 2021, 115, 154434. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Study Design | Description | Findings |
|---|---|---|---|
| Remdesivir | |||
| Wang et al., 2020 [31] | Randomized, double-blind, placebo-controlled, multicenter clinical trial | Total of 237 patients enrolled (158 and 79 randomized to remdesivir and placebo group, respectively) with concurrent use of other antivirals and corticosteroids | Although patients taking remdesivir had faster clinical improvement, differences in time to clinical improvement in the two groups were not statistically significant. |
| Antinori et al., 2020 [32] | Prospective open-label study | Total of 35 critically ill COVID-19 patients (18 ICU, 17 IDW) enrolled | At day 28, 6 and 14 patients were discharged from the ICU and IDW, respectively. Remdesivir was believed to enhance clinical improvement. |
| Grein et al., 2020 [33] | Case series | 53 patients received remdesivir on compassionate use grounds. | At follow-up (median of 18 days), significant clinical improvement was observed in 36 patients, including 17 out of 30 extubated, and 25 patients discharged. |
| Maldarelli et al., 2020 [34] | Case report | 39-year-old pregnant woman in the ICU for COVID-19 was given remdesivir on compassionate use grounds. | Patient discharged on day 9 after completing 8 out of the planned 10-day remdesivir therapy. Emergency delivery was not required. |
| Dubert et al., 2020 [35] | Case series | First cases of five (5) patients hospitalized with COVID-19 and treated with remdesivir based on compassionate use in France. | Despite significant decrease in viral load in all patients, remdesivir use had to be interrupted in 4 patients (2 because of elevated liver enzymes and 2 because of nephrotoxicity). Two patients died. |
| Helleberg et al., 2021 [36] | Case report | Immunocompromised patient in his 50s treated for COVID-19 with two 10-day courses of remdesivir at 24 and 45 days after onset of symptoms. No adjunctive corticosteroid was used. | Symptoms improved. Patient tested negative by day 38 and was discharged by day 65. |
| Beigel et al., 2020 [37] | Randomized, double-blind, placebo-controlled trial | Total of 1062 patients randomized with 541 receiving remdesivir (200 mg day 1, and 100 mg daily for 7 days) and 521 receiving placebos. | Median recovery time with remdesivir was 10 days compared to 15 days in placebo group. Incidence of serious adverse event was lower in the remdesivir group. |
| Goldman et al., 2020 [38] | Randomized, open-label, phase 3 trial | Total of 397 COVID-19 patients randomized into 200 and 197 receiving intravenous remdesivir for 5 or 10 days, respectively (200 mg day 1, then 100 mg daily subsequently). | Clinical improvement by day 14 was similar in both groups. |
| Casirivimab/Imdevimab (Regeneron) | |||
| Weinreich et al., 2020 [15] | Double-blind, phases 1–3 | Total of 275 patients randomized equally into 3 groups: placebo and 2.4 g or 8.0 g of casirivimab/imdevimab combination. | Safety profiles was similar in tests and placebo. Significant reduction in viral load was associated with the drug compared to the placebo. |
| Convalescent Plasma | |||
| Jafari et al., 2020 [39] | Case report | 26-year-old COVID-19 patient pregnant with twins delivered via caesarean section, and then was treated with meropenem, azithromycin, and hydroxychloroquine. CP was given on day 6 of hospitalization. | Significant clinical response was observed, and patient was discharged after 2 weeks. |
| Figlerowicz et al., 2020 [40] | Case report | 6-year-old diagnosed with severe COVID-19 whose treatment did not respond to antiviral and immunomodulatory drugs. | Viral elimination after the initiation of CP |
| Im et al., 2020 [41] | Case report | 68-year-old with severe COVID-19 treated with hydroxychloroquine and antiviral drugs; later transfused with CP. | Patient was discharged after 12 days. Showed significant improvement within 3 days after CP infusion. |
| Xu et al., 2020 [42] | Case report | Critically ill 65-yer-old patient with COVID-19 treated with 2 rounds of CP infusion and 7-day course of oral HCQ. | Patient remained positive after 11 days of treatment with minimal symptom improvement. Response to the combination was not optimal. |
| Ye et al., 2020 [43] | Case series | Six COVID-19 patients received between 1 and 3 cycles of CP infusion. | Significant symptom resolution and viral cure in all patients with no major side effects: 5 discharged; 1 stable and under clinical monitoring. |
| Abdullah et al., 2020 [44] | Case series | Two patients with severe COVID-19 that was refractory to antiviral and supportive treatment. | Initiation of CP was accompanied by significant improvement with resultant cure and negative virology tests |
| Duan et al., 2020 [45] | Case series | Ten patients with severe cases who received 250 mL single-dose infusion of CP. | Rapid clinical improvements and viral cure within 7 days. |
| Fung et al., 2020 [46] | Case series | Four immunocompromised patients (3 transplant recipients, and one with chronic myelogenous leukemia) who contracted COVID-19 and were treated with CP. | Clinical improvement in all 4 patients with 2 fully recovered and the other 2 discharged to skilled nursing facilities. |
| Wang et al., 2020 [47] | Case series | Five patients with severe COVID-19 associated with severe respiratory failure who required mechanical ventilation and were treated with CP. | Two patients were cured, while 3 died due to multiple organ failure. CP was initiated late (median time from symptom onset was 37 days. |
| Olivares-Gazca et al., 2020 [48] | Case series | Ten patients with severe COVID-19 were treated with CP and adjunctive therapies | Significant improvement in the measures of organ damage in all patients; improved chest X-ray and CT scans in 7 and 6 patients, respectively; 3 out of 5 removed from mechanical ventilation, 6 cured and discharged, and 2 died. |
| Shen et al., 2020 [49] | Case series | Five patients who developed critical illness including acute respiratory distress from COVID-19. All were on mechanical ventilation and received antiviral and corticosteroid therapy while being treated with CP. | Symptoms improved significantly after CP infusion. By day 37, 3 patients had been discharged home while the other 2 were in stable condition. |
| Ahn et al., 2020 [50] | Case series | Two severely ill patients with COVID-19 whose conditions did not improve by mechanical intubation, antiviral and supportive therapies. Both were treated with CP. | Symptoms improved. Patients were extubated and tested negative (after 20 and 26 days) with one discharged and the other stable. |
| Zeng et al., 2020 [51] | Case series | Six severely ill patients with respiratory failure due to COVID-19 were treated with CP (21.5 median days after testing positive). | All 6 had viral clearance (testing negative within 3 days after CP infusion). CP did not reduce mortality (5 patients died) probably because of late initiation, and patients were critically ill. |
| Salazar et al., 2020 [52] | Case series | Total of 25 patients with severe COVID-19 illness enrolled. Patients were transfused with CP with outcomes of safety and clinical status 14 days post-infusion. CP administered in addition to antiviral and other supportive treatments. | No adverse event reported in any of the patients; 19 patients showed clinical improvements by day 14, and 11 were discharged. At the time of publication, 20 of the 25 patients had been discharged. |
| Li et al., 2020 [53] | Open-label, multicenter, randomized clinical trial | A total of 103 COVID-19 patients with severe or life-threatening symptoms enrolled and randomized to evaluate the efficacy of add-on CP to standard therapy. | CP did not cause any significant difference in 28-day mortality compared to standard therapy. Differences in time to discharge were not significant. Study was terminated early, without reaching the planned 200 recruits. |
| Drug and Study Type | Description | Findings | References |
|---|---|---|---|
| LPV/r, case report | Index (54-year-old) patient in a Korean hospital treated with LPV/r 10 days after disease onset. | Significant decrease in viral load after LPV/r administration. LPV might have played a role. | [155] |
| LPV/r, case report | 65-year-old HIV/AIDS patient being treated with LPV/r who contracted SARS-CoV-2. Support treatment was added. | Patient improved and was discharged after 34 days. LPV/r was thought to play a role in recovery. | [156] |
| LPV/r, case report | 35-year-old patient treated with LPV/r for 10 days, along with supportive therapies. | Virological cure was confirmed, and patient was discharged. | [157] |
| LPV/r, case series | 5 cases of COVID-19 with 2 patients treated with LPV/r while 3 patients served as controls for the analysis. | The rate and duration of SARS CoV-2 shedding was not different with or without LPV/r. | [158] |
| LPV/r, case series | 3 patients received LPV/r for 3, 10, and 12 days, several days after the onset of illness. | All patients recovered, tested negative, and were discharged. | [159] |
| LPV/r, azithromycin, HCQ; case series | Two cases of immunosuppressed patients who were managed with drug combinations. | Despite being recipients of kidney transplants, both patients recovered after drug treatments. | [160] |
| LPV/r, AZM and HCQ combination; case report | Severe COVID-19 case in a 41-year-old who was treated with the combination therapy. | Most multi-organ symptoms resolved within 10 days and patient was discharged after 2 weeks of hospitalization. | [161] |
| LPV/r, controlled open-label | 47 hospitalized COVID-19 patients were grouped to either receiving or not receiving LPV/r in addition to their adjuvant therapies. | LPV/r was associated with faster clinical response and a shorter disease course. | [77] |
| LPV/r, randomized, controlled, open-label trial | 199 hospitalized severe COVID-19 patients were randomized to receive either a 14-day course of LPV/ritonavir in addition to standard care or standard care alone. | LPV/r neither shortened the time to clinical improvement nor reduced mortality at 28 days. Virological response was similar in both groups. | [78] |
| LPV/r, HCQ, and interferon β-1b combination; case series | 5 patients with severe cases of COVID-19 treated with the combination therapy, in addition to corticosteroids for associated inflammation. | Clinical improvement and resolution of symptoms were observed. All 5 patients were discharged. | [162] |
| LPV/r, ribavirin and interferon combination; open-label, randomized, phase 2 trial | 127 patients were randomized 86:41 to receive a 14-day course of either the combination or the control LPV/r only. | The combination therapy was associated with shorter duration of viral shedding and hospitalization. | [163] |
| Umifenovir, case control | Retrospective analysis of 50 cases of COVID-19 patients treated with LPV/r (34 cases) or umifenovir (16 cases). | Disease progression was halted in both groups. Viral cure at day 14 was 100% and 56%in umifenovir and LPV/r groups, respectively. | [84] |
| Umifenovir, case control | 62 hospitalized COVID-19 patients were analyzed based on whether they received adjuvant therapy alone (20, control) or with umifenovir (test, 42). | The use of umifenovir was associated with a shorter course of disease and reduced duration of hospitalization. | [85] |
| Umifenovir; retrospective cohort study | Analysis of patients treated with umifenovir-LPV/r combination (16 patients) compared to LPV/r only (17 patients). | By day 7 of treatment, negative conversion occurred in 75% of the patients in the combination group compared to 35% in LPV/r group. There was better chest CT scan improvement with the combination. | [83] |
| Umifenovir, case control | A retrospective analysis of 81 hospitalized patients treated for COVID-19 (45 umifenovir and 36 control). | Clinical outcomes were not better with umifenovir. | [87] |
| Umifenovir, randomized controlled trial | 86 patients randomized as follows: 34 LPV/r, 35 to umifenovir, and 17 control, no antiviral medication. | Viral cure rate and clinical responses were not significantly different in the groups. | [86] |
| Umifenovir; randomized open-label controlled trial | 240 patients were randomized (1:1) in a multicenter study to receive conventional COVID-19 therapy plus either umifenovir or favipiravir. | Clinical recovery by day 7 was not significantly different between the groups, but umifenovir was inferior to favipiravir in shortening the duration of symptoms. | [88] |
| HCQ; case report | 60-year-old who was taking HCQ for 6 months for Sjogren’s syndrome contracted SARS-CoV-2 and had illness. | Chronic use of HCQ did not prevent COVID-19. | [164] |
| HCQ, tocilizumab; case report | 61-year-old immunocompromised transplant recipient diagnosed with COVID-19 and treated with HCQ and tocilizumab. | Patient experienced significant clinical improvement and was discharged 13 days after diagnosis. | [165] |
| HCQ, AZM; case report | 74-year-old COVID-19 patient with significant comorbidities was managed in the ICU with HCQ and AZM. | Patient recorded significant clinical improvement and was extubated by day 5 and moved to the floor. | [166] |
| HCQ, AZM; open-label | Analysis of 1376 hospitalized patients treated with one or a combination of HCQ and AZM | AZM alone was associated with reduced mortality compared to no treatment. HCQ did not affect mortality. | [167] |
| HCQ; case series | 3 cases of chronic HCQ users who contracted SARS-CoV-2 and had serious symptoms. | Chronic HCQ use did not prevent COVID-19. | [168] |
| HCQ observational study | Analysis of 1446 patients to establish association between HCQ use and intubation or death. | HCQ did not reduce or increase the need for intubation or incidence of death. | [100] |
| HCQ, AZM; Open label, non-randomized study | 20 hospitalized COVID-19 patients treated with HCQ (and AZM when necessary) with outcome of viral load suppression compared to untreated patients. | HCQ and AZM were associated with significantly reduced viral load by day 6 of treatment compared to untreated control. | [99] |
| HCQ; randomized, double-blind, placebo-controlled trial | 821 participants who had been exposed to COVID-19 but were asymptomatic were randomized to receive either HCQ or placebo for post-exposure prophylaxis. | HCQ did not reduce the incidence of illness, but rather was associated with a higher incidence of side effects. | [101] |
| HCQ; randomized open-label, multicenter, controlled trial | 150 hospitalized COVID-19 patients randomized (1:1) to receive HCQ or not, in addition to standard care. | The use of HCQ was not associated with a higher rate of negative conversion of SARS-CoV-2. HCQ was associated with higher incidence of side effects | [102] |
| CQ and tocilizumab, case report | 63-year-old hospitalized for COVID-19 and treated with a 7-day course of CQ and single IV tocilizumab. | Patient experienced significant clinical improvement, recovered, and was discharged. | [169] |
| CQ, randomized phase II trial | Patients were enrolled in a study to compare the efficacy and safety of high-dose (81 patients) vs. low-dose (40 patients) CQ as adjunct therapy for severe COVID-19. | High CQ dose was associated with higher incidence of side effects. High-dose CQ did not have a better effect on viral load than low CQ dose. | [103] |
| AZM; open-label, randomized multicenter | Study of randomized 397 hospitalized patients with severe COVID-19 to either receive (214) or not (183) receive AZM in addition to standard treatment which included HCQ. | AZM was not associated with significant clinical improvement. | [170] |
| TCZ, case report | 42-year-old cancer patient who had respiratory failure as a complication of COVID-19 despite treatment with LPV/r. He was treated with two infusions of TCZ. | Patient experienced rapid clinical improvement and was fully discontinued on oxygen 5 days after TCZ infusions. Patient later fully recovered. | [128] |
| TCZ; case report | Critically ill 57-year-old with COVID-19 who was refractory to standard treatment and treated with TCZ to inhibit cytokine storm. | Significant and progressive clinical response was observed in response to TCZ. | [129] |
| TCZ; case report | 54-year-old with severe respiratory symptoms from COVID-19 who did not respond to antiviral drugs and was infused with TCZ. | Remarkable clinical improvement was observed only 4 days after TCZ administration. | [130] |
| TCZ; case report | 36-year-old severe COVID-19 patient whose symptoms did not improve with HCQ and antiviral drugs. A single-dose TCZ was infused. | Progressive improvement was observed after TZC use, with subsequent negative conversion and recovery. | [131] |
| TCZ; case report | 46-year-old patient in ICU whose COVID-19 illness was refractory to HCQ, and other supportive therapy was treated with TCZ. | Patient experienced remarkable recovery and was discharged to home 5 days after TCZ use. | [133] |
| TCZ; case series | 5 critically ill COVID-19 patients whose illness was refractory to standardized treatment. | Marked clinical improvement was observed in all patients except one. Recovery and negative conversion were reported. | [134] |
| TCZ; case series | Two patients whose COVID-19 was complicated by cytokine release syndrome were treated with TCZ. | Progression to secondary hemophagocytic lymphohistiocytosis was observed in both patients, with viral myocarditis in one, despite the treatment. | [135] |
| TCZ, case series | A retrospective analysis of 15 COVID-19 patients treated with TCZ with or without adjunct corticosteroids. | TCZ was associated with significant clinical improvement and the amelioration of cytokine storms in COVID-19 patients. | [136] |
| TCZ, case series | A retrospective analysis of 5 patients with severe COVID-19 illness requiring ICU admissions who were treated with TCZ. | All patients had significant improvement and were discharged from ICU after 13–26 days, with 2 discharged home. | [137] |
| TCZ; case series | 3 patients admitted and treated with HCQ and AZT with no significant clinical improvement. All 3 received doses of TCZ. | Patients had sufficient clinical improvement to avoid intubation, and ultimately recovered. | [138] |
| TCZ; case series | 2 patients whose symptoms worsened after treatment with HCQ, AZM and other supportive therapies were administered with TCZ. | Drastic improvement in respiratory symptoms and markers of inflammation were observed following TCZ use. Both patients recovered and were discharged. | [139] |
| TCZ, case series | 2 patients with severe COVID-19 illness refractory to standard therapy including HCQ, AZM, and antiviral drugs | Remarkable clinical resolution of septic shock and respiratory symptoms within 72 h. | [171] |
| TCZ, non-controlled, prospective | 42 patients with severe COVID-19 were treated with single 400 mg TCZ infusion. Primary outcome was a reduction in the need for invasive mechanical ventilation and death. | Only 6 patients required invasive mechanical ventilation. Total of 7 patients died by day 8. | [132] |
| IFN-α2b; prospective cohort study | Hospitalized patients were treated with nebulized IFN-α2b (n = 7), umifenovir (n = 24), or IFN-α2b–umifenovir combination (standard of care; n = 46) | The use of IFN-α2b alone or in combination was associated with significantly higher viral clearance and reduction in circulating biomarkers (IL-2 and CRP) of inflammation. | [140] |
| IFN-β-1a; prospective non-controlled study | Observation and analysis of 20 patients treated with IFN-β-1a in addition to conventional treatment (HCQ and LPV/r). | Significant clinical response including viral clearance and symptom relief. Recovery after 14 days, with no serious adverse events in any patient. | [141] |
| IFN-β-1a; randomized controlled trial | Patients (n = 44) were treated with IFN-β-1a in addition to standard treatment and compared with controls (39) who received standard treatment only. | Mortality at day 28 was significantly lower in patients treated with IFN-β-1a compared to control (19% vs. 43.6%). IFN-β-1a did not shorten the time to clinical response. | [142] |
| IFN-β-1b, randomized, open-label trial | Patients received IFN-β-1b in addition to standard treatment (n = 33) and were compared to controls who received only the standard treatment (n = 33). | IFN-β-1b shortened the time to clinical improvement (9 vs. 11 days); enhanced recovery and 14-day discharge (78.79% vs. 54.55%); reduced ICU admission (42.42% vs. 66.66%) and all-cause 28-day mortality (6.06% vs. 18.18%). | [143] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heustess, A.M.; Allard, M.A.; Thompson, D.K.; Fasinu, P.S. Clinical Management of COVID-19: A Review of Pharmacological Treatment Options. Pharmaceuticals 2021, 14, 520. https://doi.org/10.3390/ph14060520
Heustess AM, Allard MA, Thompson DK, Fasinu PS. Clinical Management of COVID-19: A Review of Pharmacological Treatment Options. Pharmaceuticals. 2021; 14(6):520. https://doi.org/10.3390/ph14060520
Chicago/Turabian StyleHeustess, Ashli M., Melissa A. Allard, Dorothea K. Thompson, and Pius S. Fasinu. 2021. "Clinical Management of COVID-19: A Review of Pharmacological Treatment Options" Pharmaceuticals 14, no. 6: 520. https://doi.org/10.3390/ph14060520
APA StyleHeustess, A. M., Allard, M. A., Thompson, D. K., & Fasinu, P. S. (2021). Clinical Management of COVID-19: A Review of Pharmacological Treatment Options. Pharmaceuticals, 14(6), 520. https://doi.org/10.3390/ph14060520