
Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment



Abstract
1. Introduction
2. General Definitions
- −
- low-level disinfection, which consists of reducing the vegetative forms of bacteria (except Mycobacterium tuberculosis), enveloped viruses and fungi. This category of disinfectant includes 3% hydrogen peroxide, quaternary ammonium compounds, diluted phenolics and glutaraldehyde.
- −
- Intermediate-level disinfection is the process of reducing all species of bacteria in the vegetative form (including Tbc), viruses (enveloped and non-enveloped) and fungi. Disinfectants belonging to this category include phenolics, iodophor, alcohols, and chlorinated compounds.
- −
3. Antiseptics
3.1. The Difference between an Antiseptic and a Disinfectant
3.2. The Use of Antiseptics
3.3. Features of Antiseptics
3.4. Old Antiseptics
4. Antisepsis of Wounds
4.1. Octenidine Dihydrochloride
4.1.1. Application
4.1.2. Safety
4.2. Povidone-Iodine (Polyvinylpyrrolidone-Iodine; PVP-Iodine)
4.2.1. Application
4.2.2. Safety
4.3. Polihexanide
4.3.1. Application
4.3.2. Safety
4.4. Sodium Hypochlorite (NaOCl)
4.4.1. Application
4.4.2. Safety
4.5. Nanosilver
4.5.1. Application
4.5.2. Safety
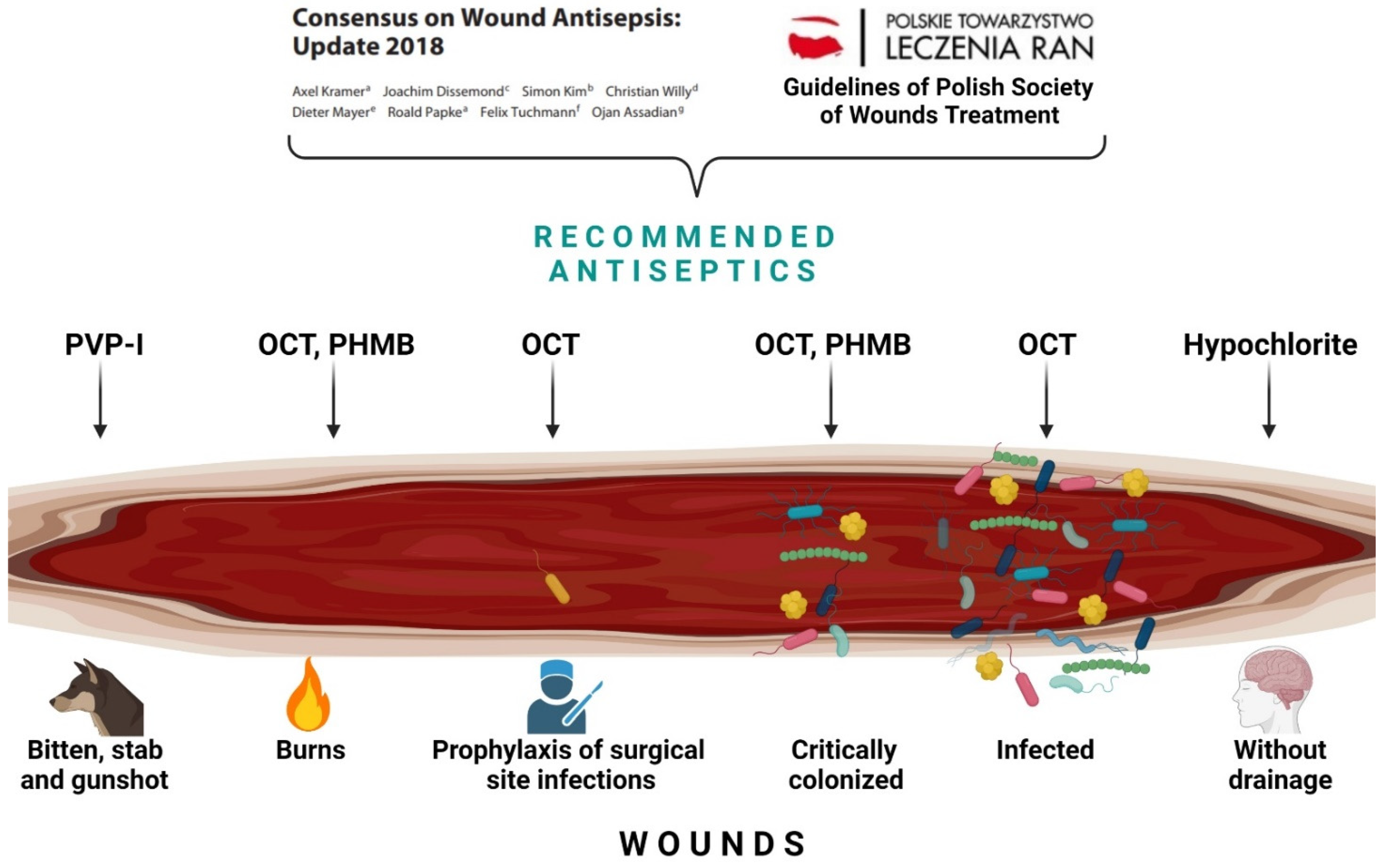
5. Guidelines for the Use of Wound Antiseptics
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakayama, D.K. Antisepsis and Asepsis and How They Shaped Modern Surgery. Am. Surg. 2018, 84, 766–771. [Google Scholar] [CrossRef]
- Jones, A. Bare below the Elbows: A Brief History of Surgeon Attire and Infection. BJU Int. 2008, 102, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, T.M. The Use of Antiseptics in the Treatment of Wounds. Chir. Dyplomie 2021, 16, 14–18. [Google Scholar]
- Karpiński, T.; Sopata, M.; Mańkowski, B. The Antimicrobial Effectiveness of Antiseptics as a Challenge in Hard to Heal Wounds. Leczenie Ran 2020, 17, 88–94. [Google Scholar] [CrossRef]
- Makhayeva, D.N.; Irmukhametova, G.S.; Khutoryanskiy, V.V. Polymeric Iodophors: Preparation, Properties, and Biomedical Applications. Rev. J. Chem. 2020, 10, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Best, M.; Neuhauser, D. Ignaz Semmelweis and the Birth of Infection Control. Qual. Saf. Health Care 2004, 13, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Pitt, D.; Aubin, J.-M. Joseph Lister: Father of Modern Surgery. Can. J. Surg. 2012, 55, E8–E9. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.; Rosenthal, K.; Pfaller, M. Medical Microbiology, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Rutala, W.A.; Weber, D.J. Healthcare Infection Control Practices Advisory Committee (HICPAC). In Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008; CDC: Atlanta, GA, USA, 2008. [Google Scholar]
- Junka, A.; Bartoszewicz, M.; Smutnicka, D.; Secewicz, A.; Szymczyk, P. Efficacy of Antiseptics Containing Povidone-Iodine, Octenidine Dihydrochloride and Ethacridine Lactate against Biofilm Formed by Pseudomonas Aeruginosa and Staphylococcus Aureus Measured with the Novel Biofilm-Oriented Antiseptics Test. Int. Wound J. 2014, 11, 730–734. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, G.; Russell, A.D. Antiseptics and Disinfectants: Activity, Action, and Resistance. Clin. Microbiol. Rev. 1999, 12, 147–179. [Google Scholar] [CrossRef]
- Müller, G.; Kramer, A. Biocompatibility Index of Antiseptic Agents by Parallel Assessment of Antimicrobial Activity and Cellular Cytotoxicity. J. Antimicrob. Chemother. 2008, 61, 1281–1287. [Google Scholar] [CrossRef] [PubMed]
- Hübner, N.-O.; Siebert, J.; Kramer, A. Octenidine Dihydrochloride, a Modern Antiseptic for Skin, Mucous Membranes and Wounds. Skin Pharmacol. Physiol. 2010, 23, 244–258. [Google Scholar] [CrossRef]
- Pitten, F.-A.; Werner, H.-P.; Kramer, A. A Standardized Test to Assess the Impact of Different Organic Challenges on the Antimicrobial Activity of Antiseptics. J. Hosp. Infect. 2003, 55, 108–115. [Google Scholar] [CrossRef]
- Kujath, P.; Michelsen, A. Wounds—From Physiology to Wound Dressing. Dtsch. Arztebl. Int. 2008, 105, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Maillard, J.-Y.; Kampf, G.; Cooper, R. Antimicrobial Stewardship of Antiseptics That Are Pertinent to Wounds: The Need for a United Approach. JAC Antimicrob. Resist. 2021, 3, dlab027. [Google Scholar] [CrossRef]
- Petel, R.; Moskovitz, M.; Tickotsky, N.; Halabi, A.; Goldstein, J.; Houri-Haddad, Y. Cytotoxicity and Proliferative Effects of Iodoform-Containing Root Canal-Filling Material on RAW 264.7 Macrophage and RKO Epithelial Cell Lines. Arch. Oral. Biol. 2013, 58, 75–81. [Google Scholar] [CrossRef]
- Cifuentes-Mendiola, S.; Barrera-Francisco, M.; Garcia-Navarro, M.; Llamosas-Hernandez, E.; Perez-Martinez, I.; Garcia-Hernandez, A. Endoflas FS Decreases the Viability and Mineralisation Process in Human Alveolar Osteoblastic Cells. J. Clin. Diagn. Res. 2018, 12, ZC30–ZC33. [Google Scholar] [CrossRef]
- Lee, J.; Lorenzo, D.; Rawlins, T.; Cardo, V.A. Sodium Hypochlorite Extrusion: An Atypical Case of Massive Soft Tissue Necrosis. J. Oral Maxillofac. Surg. 2011, 69, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Basumatary, B.; Basumatary, R.; Ramchiary, A.; Konwar, D. Evaluation of Ag@TiO2/WO3 Heterojunction Photocatalyst for Enhanced Photocatalytic Activity towards Methylene Blue Degradation. Chemosphere 2022, 286, 131848. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, F.; Tsutsui, T. Cell-Transforming Activity of Fourteen Chemical Agents Used in Dental Practice in Syrian Hamster Embryo Cells. J. Pharmacol. Sci. 2003, 93, 497–500. [Google Scholar] [CrossRef][Green Version]
- Oplatowska, M.; Donnelly, R.F.; Majithiya, R.J.; Glenn Kennedy, D.; Elliott, C.T. The Potential for Human Exposure, Direct and Indirect, to the Suspected Carcinogenic Triphenylmethane Dye Brilliant Green from Green Paper Towels. Food Chem. Toxicol. 2011, 49, 1870–1876. [Google Scholar] [CrossRef] [PubMed]
- IARC Monographs Vol 129 Group. Carcinogenicity of Gentian Violet, Leucogentian Violet, Malachite Green, Leucomalachite Green, and CI Direct Blue 218. Lancet Oncol. 2021, 22, 585–586. [Google Scholar] [CrossRef]
- Xiao, X.; Chen, C.; Deng, J.; Wu, J.; He, K.; Xiang, Z.; Yang, Y. Analysis of Trace Malachite Green, Crystal Violet, and Their Metabolites in Zebrafish by Surface-Coated Probe Nanoelectrospray Ionization Mass Spectrometry. Talanta 2020, 217, 121064. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, T.M. Efficacy of Octenidine against Pseudomonas Aeruginosa Strains. Eur. J. Biol. Res. 2019, 9, 135–140. [Google Scholar]
- Koburger, T.; Hübner, N.-O.; Braun, M.; Siebert, J.; Kramer, A. Standardized Comparison of Antiseptic Efficacy of Triclosan, PVP–Iodine, Octenidine Dihydrochloride, Polyhexanide and Chlorhexidine Digluconate. J. Antimicrob. Chemother. 2010, 65, 1712–1719. [Google Scholar] [CrossRef]
- Al-Doori, Z.; Goroncy-Bermes, P.; Gemmell, C.G.; Morrison, D. Low-Level Exposure of MRSA to Octenidine Dihydrochloride Does Not Select for Resistance. J. Antimicrob. Chemother. 2007, 59, 1280–1281. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on Wound Antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef]
- Sopata, M.; Banasiewicz, T.; Gabriel, M.; Jawień, A.; Mańkowski, B.; Mańkowski, P.; Mościcka, P.; Szewczyk, M.; Szoka, P.; Zieliński, M. Review of Antimicrobial Substances Used in Wound Treatment Based on the German Consensus and Polish Guidelines (2018 State of Knowledge); Karger: Basel, Switzerland, 2018. [Google Scholar]
- Sopata, M.; Jawień, A.; Mrozikiewicz-Rakowska, B.; Augusewicz, Z.; Bakowska, M.; Samson, I.; Gabriel, M.; Grzela, T.; Karpiński, T.; Kuberka, I.; et al. Guidelines for local management of uninfected wounds, wounds at risk of infection and infected wounds—An overview of the available antimicrobial substances used in the treatment of wounds. Recommendations of the Polish Wound Treatment Society. Leczenie Ran 2020, 17, 1–21. [Google Scholar] [CrossRef]
- Dettenkofer, M.; Wilson, C.; Gratwohl, A.; Schmoor, C.; Bertz, H.; Frei, R.; Heim, D.; Luft, D.; Schulz, S.; Widmer, A.F. Skin Disinfection with Octenidine Dihydrochloride for Central Venous Catheter Site Care: A Double-Blind, Randomized, Controlled Trial. Clin. Microbiol. Infect. 2010, 16, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Novakov Mikić, A.; Stojic, S. Study Results on the Use of Different Therapies for the Treatment of Vaginitis in Hospitalised Pregnant Women. Arch. Gynecol. Obstet. 2015, 292, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Zumtobel, M.; Assadian, O.; Leonhard, M.; Stadler, M.; Schneider, B. The Antimicrobial Effect of Octenidine-Dihydrochloride Coated Polymer Tracheotomy Tubes on Staphylococcus Aureus and Pseudomonas Aeruginosa Colonisation. BMC Microbiol. 2009, 9, 150. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, A.; Schneider, J.; Föhr, P.; Wehner, S.; Kühn, K.-D.; Stemberger, A.; Schieker, M.; Burgkart, R. In Vitro Evaluation of Novel Antimicrobial Coatings for Surgical Sutures Using Octenidine. BMC Microbiol. 2015, 15, 186. [Google Scholar] [CrossRef]
- Kampf, G. Antiseptic Stewardship; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2018. [Google Scholar]
- Vanscheidt, W.; Harding, K.; Téot, L.; Siebert, J. Effectiveness and Tissue Compatibility of a 12-Week Treatment of Chronic Venous Leg Ulcers with an Octenidine Based Antiseptic--a Randomized, Double-Blind Controlled Study. Int. Wound J. 2012, 9, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Bührer, C.; Bahr, S.; Siebert, J.; Wettstein, R.; Geffers, C.; Obladen, M. Use of 2% 2-Phenoxyethanol and 0.1% Octenidine as Antiseptic in Premature Newborn Infants of 23–26 Weeks Gestation. J. Hosp. Infect. 2002, 51, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Zyba, V.; Jung, K.; Rinke, S.; Haak, R.; Mausberg, R.F.; Ziebolz, D. Cytotoxic Effects of Octenidine Mouth Rinse on Human Fibroblasts and Epithelial Cells—An In Vitro Study. Drug Chem. Toxicol. 2016, 39, 322–330. [Google Scholar] [CrossRef]
- Chhabra, N. Povidone-Iodine in Dermatology: A Reappraisal. CSDM 2021, 1, 51. [Google Scholar] [CrossRef]
- Bigliardi, P.; Langer, S.; Cruz, J.J.; Kim, S.W.; Nair, H.; Srisawasdi, G. An Asian Perspective on Povidone Iodine in Wound Healing. Dermatology 2017, 233, 223–233. [Google Scholar] [CrossRef]
- Sauerbrei, A. Bactericidal and Virucidal Activity of Ethanol and Povidone-Iodine. Microbiologyopen 2020, 9, e1097. [Google Scholar] [CrossRef]
- Gorman, S.P.; Scott, E.M.; Hutchinson, E.P. Effects of Aqueous and Alcoholic Povidone-Iodine on Spores of Bacillus Subtilis. J. Appl. Bacteriol. 1985, 59, 99–105. [Google Scholar] [CrossRef]
- Bigliardi, P.L.; Alsagoff, S.A.L.; El-Kafrawi, H.Y.; Pyon, J.-K.; Wa, C.T.C.; Villa, M.A. Povidone Iodine in Wound Healing: A Review of Current Concepts and Practices. Int. J. Surg. 2017, 44, 260–268. [Google Scholar] [CrossRef]
- Gmur, M.K.; Karpiński, T.M. Povidone-Iodine in Wound Healing and Prevention of Wound Infections. Eur. J. Biol. Res. 2020, 10, 232–239. [Google Scholar]
- Majidipour, N.; Abdeyazdan, Z.; Zargham-Boroujeni, A. Chlorhexidine or Povidone-Iodine: Which Solution Is More Effective on Skin Colonization in Neonates? Iran J. Nurs. Midwifery Res. 2013, 18, 54–58. [Google Scholar] [PubMed]
- Cheng, M.-T.; Chang, M.-C.; Wang, S.-T.; Yu, W.-K.; Liu, C.-L.; Chen, T.-H. Efficacy of Dilute Betadine Solution Irrigation in the Prevention of Postoperative Infection of Spinal Surgery. Spine 2005, 30, 1689–1693. [Google Scholar] [CrossRef]
- Giordano, S.; Peltoniemi, H.; Lilius, P.; Salmi, A. Povidone-Iodine Combined with Antibiotic Topical Irrigation to Reduce Capsular Contracture in Cosmetic Breast Augmentation: A Comparative Study. Aesthet. Surg. J. 2013, 33, 675–680. [Google Scholar] [CrossRef]
- Eason, E.; Wells, G.; Garber, G.; Hemmings, R.; Luskey, G.; Gillett, P.; Martin, M. Vaginal Antisepsis For Abdominal Hysterectomy Study Group Antisepsis for Abdominal Hysterectomy: A Randomised Controlled Trial of Povidone-Iodine Gel. BJOG 2004, 111, 695–699. [Google Scholar] [CrossRef]
- Brown, N.M.; Cipriano, C.A.; Moric, M.; Sporer, S.M.; Della Valle, C.J. Dilute Betadine Lavage before Closure for the Prevention of Acute Postoperative Deep Periprosthetic Joint Infection. J. Arthroplasty 2012, 27, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Johani, K.; Malone, M.; Jensen, S.O.; Dickson, H.G.; Gosbell, I.B.; Hu, H.; Yang, Q.; Schultz, G.; Vickery, K. Evaluation of Short Exposure Times of Antimicrobial Wound Solutions against Microbial Biofilms: From In Vitro to In Vivo. J. Antimicrob. Chemother. 2018, 73, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Müller, G.; Hai, D.N.; Kramer, A. Lack of in Vitro Genotoxicity of Povidone-Iodine in Solution, in Ointment or in a Liposomal Formulation (Repithel). Dermatology 2006, 212 (Suppl. 1), 94–97. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.H.; Nahm, W.K.; Badiavas, E.; Yufit, T.; Falanga, V. Slow Release Iodine Preparation and Wound Healing: In Vitro Effects Consistent with Lack of in Vivo Toxicity in Human Chronic Wounds. Br. J. Dermatol. 2002, 146, 365–374. [Google Scholar] [CrossRef]
- Freise, J.; Kohaus, S.; Korber, A.; Hillen, U.; Kroger, K.; Grabbe, S.; Dissemond, J. Contact Sensitization in Patients with Chronic Wounds: Results of a Prospective Investigation. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1203–1207. [Google Scholar] [CrossRef]
- Bruyère, F.; Laine, P.; Saint-Jalmes, G.; Malavaud, S.; Pradere, B. Mucosal Impact of Alcoholic Povidone-Iodine Indicated in Preoperative Disinfection. J. Hosp. Infect. 2020, 104, 302–304. [Google Scholar] [CrossRef] [PubMed]
- Kaehn, K. Polihexanide: A Safe and Highly Effective Biocide. Skin Pharmacol. Physiol. 2010, 23 (Suppl. 1), 7–16. [Google Scholar] [CrossRef]
- O’Malley, L.P.; Shaw, C.H.; Collins, A.N. Microbial Degradation of the Biocide Polyhexamethylene Biguanide: Isolation and Characterization of Enrichment Consortia and Determination of Degradation by Measurement of Stable Isotope Incorporation into DNA. J. Appl. Microbiol. 2007, 103, 1158–1169. [Google Scholar] [CrossRef] [PubMed]
- Roth, B.; Brill, F.H.H. Polihexanide for Wound Treatment—How It Began. Skin Pharmacol. Physiol. 2010, 23 (Suppl. 1), 4–6. [Google Scholar] [CrossRef]
- Eberlein, T.; Assadian, O. Clinical Use of Polihexanide on Acute and Chronic Wounds for Antisepsis and Decontamination. Skin Pharmacol. Physiol. 2010, 23 (Suppl. 1), 45–51. [Google Scholar] [CrossRef]
- Szkołuda, P.; Karpiński, T.M. Polyhexanide (PHMB)—Properties and Applications in Medicine. Eur. J. Biol. Res. 2020, 10, 225–231. [Google Scholar]
- Daeschlein, G.; Assadian, O.; Bruck, J.C.; Meinl, C.; Kramer, A.; Koch, S. Feasibility and Clinical Applicability of Polihexanide for Treatment of Second-Degree Burn Wounds. Skin Pharmacol. Physiol. 2007, 20, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Gerli, S.; Rossetti, D.; Di Renzo, G.C. A New Approach for the Treatment of Bacterial Vaginosis: Use of Polyhexamethylene Biguanide. A Prospective, Randomized Study. Eur. Rev. Med. Pharmacol. Sci. 2003, 7, 127–130. [Google Scholar] [PubMed]
- Opinion on Polyaminopropyl Biguanide (PHMB)—Submission III. 90. Available online: https://hal.archives-ouvertes.fr/hal-01493478 (accessed on 10 November 2021).
- Schnuch, A.; Geier, J.; Uter, W.; Basketter, D.A.; Jowsey, I.R. The Biocide Polyhexamethylene Biguanide Remains an Uncommon Contact Allergen. Contact Dermatitis 2007, 56, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Guastalli, A.R.; Clarkson, R.M.; Rossi-Fedele, G. The Effect of Surfactants on the Stability of Sodium Hypochlorite Preparations. J. Endod. 2015, 41, 1344–1348. [Google Scholar] [CrossRef]
- Pişkin, B.; Türkün, M. Stability of Various Sodium Hypochlorite Solutions. J. Endod. 1995, 21, 253–255. [Google Scholar] [CrossRef]
- Narui, K.; Takano, M.; Noguchi, N.; Sasatsu, M. Susceptibilities of Methicillin-Resistant Staphylococcus Aureus Isolates to Seven Biocides. Biol. Pharm. Bull. 2007, 30, 585–587. [Google Scholar] [CrossRef]
- Spencer, H.R.; Ike, V.; Brennan, P.A. Review: The Use of Sodium Hypochlorite in Endodontics--Potential Complications and Their Management. Br. Dent. J. 2007, 202, 555–559. [Google Scholar] [CrossRef]
- Gruye, L.E.; McCunney, R.J.; Buchheit, K.M.; Goldminz, A.M. Allergic Contact Dermatitis in a Wastewater Treatment Worker: The Role of Sodium Hypochlorite. Contact Dermat. 2020, 83, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Chia Shi Zhe, G.; Green, A.; Fong, Y.T.; Lee, H.Y.; Ho, S.F. Rare Case of Type I Hypersensitivity Reaction to Sodium Hypochlorite Solution in a Healthcare Setting. BMJ Case Rep. 2016, 2016, bcr2016217228. [Google Scholar] [CrossRef] [PubMed]
- Guivarc’h, M.; Ordioni, U.; Ahmed, H.M.A.; Cohen, S.; Catherine, J.-H.; Bukiet, F. Sodium Hypochlorite Accident: A Systematic Review. J. Endod. 2017, 43, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Dandakis, C.; Lambrianidis, T.; Boura, P. Immunologic Evaluation of Dental Patient with History of Hypersensitivity Reaction to Sodium Hypochlorite. Endod. Dent. Traumatol. 2000, 16, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Syed, M.; Chopra, R.; Sachdev, V. Allergic Reactions to Dental Materials-A Systematic Review. J. Clin. Diagn Res. 2015, 9, ZE04–ZE09. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, R.J.; Watts, M.; Vale, J.A.; Grieve, J.R.; Schep, L.J. The Clinical Toxicology of Sodium Hypochlorite. Clin. Toxicol. (Phila) 2019, 57, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Pontes, F.; Pontes, H.; Adachi, P.; Rodini, C.; Almeida, D.; Pinto, D. Gingival and Bone Necrosis Caused by Accidental Sodium Hypochlorite Injection Instead of Anaesthetic Solution. Int. Endod. J. 2008, 41, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Klasen, H.J. Historical Review of the Use of Silver in the Treatment of Burns. I. Early Uses. Burns 2000, 26, 117–130. [Google Scholar] [CrossRef]
- Dibrov, P.; Dzioba, J.; Gosink, K.K.; Häse, C.C. Chemiosmotic Mechanism of Antimicrobial Activity of Ag(+) in Vibrio Cholerae. Antimicrob. Agents Chemother. 2002, 46, 2668–2670. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Jiang, Y.; Fang, Y. Spectroscopy Property of Ag Nanoparticles. Spectrochim Acta A Mol. Biomol. Spectrosc. 2006, 65, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Morones, J.R.; Elechiguerra, J.L.; Camacho, A.; Holt, K.; Kouri, J.B.; Ramírez, J.T.; Yacaman, M.J. The Bactericidal Effect of Silver Nanoparticles. Nanotechnology 2005, 16, 2346–2353. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.; Tak, Y.K.; Song, J.M. Does the Antibacterial Activity of Silver Nanoparticles Depend on the Shape of the Nanoparticle? A Study of the Gram-Negative Bacterium Escherichia Coli. Appl. Environ. Microbiol. 2007, 73, 1712–1720. [Google Scholar] [CrossRef]
- Rai, M.; Yadav, A.; Gade, A. Silver Nanoparticles as a New Generation of Antimicrobials. Biotechnol. Adv. 2009, 27, 76–83. [Google Scholar] [CrossRef]
- Sondi, I.; Salopek-Sondi, B. Silver Nanoparticles as Antimicrobial Agent: A Case Study on E. Coli as a Model for Gram-Negative Bacteria. J. Colloid. Interface Sci. 2004, 275, 177–182. [Google Scholar] [CrossRef]
- Riley, D.K.; Classen, D.C.; Stevens, L.E.; Burke, J.P. A Large Randomized Clinical Trial of a Silver-Impregnated Urinary Catheter: Lack of Efficacy and Staphylococcal Superinfection. Am. J. Med. 1995, 98, 349–356. [Google Scholar] [CrossRef]
- Morgan-Jones, R.; Bishay, M.; Hernández-Hermoso, J.; Lantis, J.; Murray, J.; Pajamaki, J.; Pellegrini, A.; Tarabichi, S.; Willy, C. Incision Care and Dressing Selection in Surgical Wounds Findings from an International Meeting of Surgeons. Wounds Int. 2019, 1–4. [Google Scholar]
- Murphy, C.; Atkin, L.; Swanson, T.; Tachi, M.; Tan, Y.K.; de Ceniga, M.V.; Weir, D.; Wolcott, R.; Ĉernohorská, J.; Ciprandi, G.; et al. Defying Hard-to-Heal Wounds with an Early Antibiofilm Intervention Strategy: Wound Hygiene. J. Wound Care 2020, 29, S1–S26. [Google Scholar] [CrossRef]
- Furno, F.; Morley, K.S.; Wong, B.; Sharp, B.L.; Arnold, P.L.; Howdle, S.M.; Bayston, R.; Brown, P.D.; Winship, P.D.; Reid, H.J. Silver Nanoparticles and Polymeric Medical Devices: A New Approach to Prevention of Infection? J. Antimicrob. Chemother. 2004, 54, 1019–1024. [Google Scholar] [CrossRef]
- Li, Y.; Leung, P.; Yao, L.; Song, Q.W.; Newton, E. Antimicrobial Effect of Surgical Masks Coated with Nanoparticles. J. Hosp. Infect. 2006, 62, 58–63. [Google Scholar] [CrossRef]
- Leaper, D.J. Silver Dressings: Their Role in Wound Management. Int. Wound J. 2006, 3, 282–294. [Google Scholar] [CrossRef]
- Tian, J.; Wong, K.K.Y.; Ho, C.-M.; Lok, C.-N.; Yu, W.-Y.; Che, C.-M.; Chiu, J.-F.; Tam, P.K.H. Topical Delivery of Silver Nanoparticles Promotes Wound Healing. ChemMedChem 2007, 2, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Gong, P.; Li, H.; He, X.; Wang, K.; Hu, J.; Tan, W.; Zhang, S.; Yang, X. Preparation and Antibacterial Activity of Fe3O4@Ag Nanoparticles. Nanotechnology 2007, 18, 285604. [Google Scholar] [CrossRef]
- Chen, X.; Schluesener, H.J. Nanosilver: A Nanoproduct in Medical Application. Toxicol. Lett. 2008, 176, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lansdown, A.B.G.; Williams, A. How Safe Is Silver in Wound Care? J. Wound Care 2004, 13, 131–136. [Google Scholar] [CrossRef]
- Liu, W.; Wu, Y.; Wang, C.; Li, H.C.; Wang, T.; Liao, C.Y.; Cui, L.; Zhou, Q.F.; Yan, B.; Jiang, G.B. Impact of Silver Nanoparticles on Human Cells: Effect of Particle Size. Nanotoxicology 2010, 4, 319–330. [Google Scholar] [CrossRef]
- Connolly, M.; Fernandez-Cruz, M.-L.; Quesada-Garcia, A.; Alte, L.; Segner, H.; Navas, J.M. Comparative Cytotoxicity Study of Silver Nanoparticles (AgNPs) in a Variety of Rainbow Trout Cell Lines (RTL-W1, RTH-149, RTG-2) and Primary Hepatocytes. Int. J. Environ. Res. Public Health 2015, 12, 5386–5405. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, C.A.; Seckler, M.M.; Ingle, A.P.; Gupta, I.; Galdiero, S.; Galdiero, M.; Gade, A.; Rai, M. Silver Nanoparticles: Therapeutical Uses, Toxicity, and Safety Issues. J. Pharm. Sci. 2014, 103, 1931–1944. [Google Scholar] [CrossRef]
- Powers, C.M.; Slotkin, T.A.; Seidler, F.J.; Badireddy, A.R.; Padilla, S. Silver Nanoparticles Alter Zebrafish Development and Larval Behavior: Distinct Roles for Particle Size, Coating and Composition. Neurotoxicol. Teratol. 2011, 33, 708–714. [Google Scholar] [CrossRef]
- de Lima, R.; Seabra, A.B.; Durán, N. Silver Nanoparticles: A Brief Review of Cytotoxicity and Genotoxicity of Chemically and Biogenically Synthesized Nanoparticles. J. Appl. Toxicol. 2012, 32, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Munger, M.A.; Radwanski, P.; Hadlock, G.C.; Stoddard, G.; Shaaban, A.; Falconer, J.; Grainger, D.W.; Deering-Rice, C.E. In Vivo Human Time-Exposure Study of Orally Dosed Commercial Silver Nanoparticles. Nanomedicine 2014, 10, 1–9. [Google Scholar] [CrossRef]
- Gaillet, S.; Rouanet, J.-M. Silver Nanoparticles: Their Potential Toxic Effects after Oral Exposure and Underlying Mechanisms—A Review. Food Chem. Toxicol. 2015, 77, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Antony, J.J.; Sivalingam, P.; Chen, B. Toxicological Effects of Silver Nanoparticles. Environ. Toxicol. Pharmacol. 2015, 40, 729–732. [Google Scholar] [CrossRef]
- Bock, L.J.; Hind, C.K.; Sutton, J.M.; Wand, M.E. Growth Media and Assay Plate Material Can Impact on the Effectiveness of Cationic Biocides and Antibiotics against Different Bacterial Species. Lett. Appl. Microbiol. 2018, 66, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Takami, T.; Matsumura, R.; Dorofeev, A.; Hirata, Y.; Nagamune, H. In Vitro Evaluation of the Biocompatibility of Newly Synthesized Bis-Quaternary Ammonium Compounds with Spacer Structures Derived from Pentaerythritol or Hydroquinone. Biocontrol. Sci. 2016, 21, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.L.; Karpanen, T.J.; Nightingale, P.; Conway, B.R.; Elliott, T.S.J. Antimicrobial Activity and Skin Permeation of Iodine Present in an Iodine-Impregnated Surgical Incise Drape. J. Antimicrob. Chemother. 2015, 70, 2255–2260. [Google Scholar] [CrossRef]
- Chen, L.; Lü, X.; Cao, W.; Zhang, C.; Xu, R.; Meng, X.; Chen, K. An Investigation and Evaluation on Species and Characteristics of Pathogenic Microorganisms in Chinese Local Hospital Settings. Microb. Pathog. 2015, 89, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Zisi, A.P.; Exindari, M.K.; Siska, E.K.; Koliakos, G.G. Iodine-Lithium-Alpha-Dextrin (ILαD) against Staphylococcus Aureus Skin Infections: A Comparative Study of in-Vitro Bactericidal Activity and Cytotoxicity between ILαD and Povidone-Iodine. J. Hosp. Infect. 2018, 98, 134–140. [Google Scholar] [CrossRef]
- Beier, R.C.; Foley, S.L.; Davidson, M.K.; White, D.G.; McDermott, P.F.; Bodeis-Jones, S.; Zhao, S.; Andrews, K.; Crippen, T.L.; Sheffield, C.L.; et al. Characterization of Antibiotic and Disinfectant Susceptibility Profiles among Pseudomonas Aeruginosa Veterinary Isolates Recovered during 1994-2003. J. Appl. Microbiol. 2015, 118, 326–342. [Google Scholar] [CrossRef] [PubMed]
- Jeng, D.K.; Severin, J.E. Povidone Iodine Gel Alcohol: A 30-Second, Onetime Application Preoperative Skin Preparation. Am. J. Infect. Control 1998, 26, 488–494. [Google Scholar] [CrossRef]
- Witney, A.A.; Gould, K.A.; Pope, C.F.; Bolt, F.; Stoker, N.G.; Cubbon, M.D.; Bradley, C.R.; Fraise, A.; Breathnach, A.S.; Butcher, P.D.; et al. Genome Sequencing and Characterization of an Extensively Drug-Resistant Sequence Type 111 Serotype O12 Hospital Outbreak Strain of Pseudomonas Aeruginosa. Clin. Microbiol. Infect. 2014, 20, O609–O618. [Google Scholar] [CrossRef] [PubMed]
- Helal, Z.H.; Hafez, H.M.; Khan, M.I. Susceptibility of Multidrug Resistant Pseudomonas Aeruginosa to Commonly Used Biocides and Its Association with Qac Efflux Pump Genes. Egypt. J. Med Microbiol. 2015, 38, 1–10. [Google Scholar] [CrossRef]
- Assadian, O.; Wehse, K.; Hübner, N.-O.; Koburger, T.; Bagel, S.; Jethon, F.; Kramer, A. Minimum Inhibitory (MIC) and Minimum Microbicidal Concentration (MMC) of Polihexanide and Triclosan against Antibiotic Sensitive and Resistant Staphylococcus Aureus and Escherichia Coli Strains. GMS Krankenhhyg Interdiszip 2011, 6, Doc06. [Google Scholar] [CrossRef]
- Fabry, W.; Kock, H.-J. In-Vitro Activity of Polyhexanide Alone and in Combination with Antibiotics against Staphylococcus Aureus. J. Hosp. Infect. 2014, 86, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Fabry, W.; Reimer, C.; Azem, T.; Aepinus, C.; Kock, H.J.; Vahlensieck, W. Activity of the Antiseptic Polyhexanide against Meticillin-Susceptible and Meticillin-Resistant Staphylococcus Aureus. J. Glob. Antimicrob. Resist. 2013, 1, 195–199. [Google Scholar] [CrossRef]
- Kamaruzzaman, N.F.; Firdessa, R.; Good, L. Bactericidal Effects of Polyhexamethylene Biguanide against Intracellular Staphylococcus Aureus EMRSA-15 and USA 300. J. Antimicrob. Chemother. 2016, 71, 1252–1259. [Google Scholar] [CrossRef]
- Forbes, S.; Dobson, C.B.; Humphreys, G.J.; McBain, A.J. Transient and Sustained Bacterial Adaptation Following Repeated Sublethal Exposure to Microbicides and a Novel Human Antimicrobial Peptide. Antimicrob. Agents Chemother. 2014, 58, 5809–5817. [Google Scholar] [CrossRef]
- Fabry, W.H.K.; Kock, H.-J.; Vahlensieck, W. Activity of the Antiseptic Polyhexanide against Gram-Negative Bacteria. Microb. Drug Resist. 2014, 20, 138–143. [Google Scholar] [CrossRef]
- Almatroudi, A.; Gosbell, I.B.; Hu, H.; Jensen, S.O.; Espedido, B.A.; Tahir, S.; Glasbey, T.O.; Legge, P.; Whiteley, G.; Deva, A.; et al. Staphylococcus Aureus Dry-Surface Biofilms Are Not Killed by Sodium Hypochlorite: Implications for Infection Control. J. Hosp. Infect. 2016, 93, 263–270. [Google Scholar] [CrossRef]
- Jaglic, Z.; Červinková, D.; Vlková, H.; Michu, E.; Kunová, G.; Babák, V. Bacterial Biofilms Resist Oxidising Agents Due to the Presence of Organic Matter. Czech J. Food Sci. 2012, 30, 178–187. [Google Scholar] [CrossRef]
- Estrela, C.R.A.; Estrela, C.; Reis, C.; Bammann, L.L.; Pécora, J.D. Control of Microorganisms in Vitro by Endodontic Irrigants. Braz Dent. J. 2003, 14, 187–192. [Google Scholar] [CrossRef][Green Version]
- Locker, J.; Fitzgerald, P.; Sharp, D. Antibacterial Validation of Electrogenerated Hypochlorite Using Carbon-Based Electrodes. Lett. Appl. Microbiol. 2014, 59, 636–641. [Google Scholar] [CrossRef]
- Ayala-Núñez, N.V.; Lara Villegas, H.H.; del Carmen Ixtepan Turrent, L.; Rodríguez Padilla, C. Silver Nanoparticles Toxicity and Bactericidal Effect Against Methicillin-Resistant Staphylococcus Aureus: Nanoscale Does Matter. Nanobiotechnology 2009, 5, 2–9. [Google Scholar] [CrossRef]
- Iñiguez-Moreno, M.; Avila-Novoa, M.G.; Iñiguez-Moreno, E.; Guerrero-Medina, P.J.; Gutiérrez-Lomelí, M. Antimicrobial Activity of Disinfectants Commonly Used in the Food Industry in Mexico. J. Glob. Antimicrob. Resist. 2017, 10, 143–147. [Google Scholar] [CrossRef]
- Vieira, C.D.; de Macêdo Farias, L.; Diniz, C.G.; Alvarez-Leite, M.E.; da Silva Camargo, E.R.; de Carvalho, M.A.R. New Methods in the Evaluation of Chemical Disinfectants Used in Health Care Services. Am. J. Infect. Control 2005, 33, 162–169. [Google Scholar] [CrossRef]
- Kora, A.J.; Arunachalam, J. Assessment of Antibacterial Activity of Silver Nanoparticles on Pseudomonas Aeruginosa and Its Mechanism of Action. World J. Microbiol. Biotechnol. 2011, 27, 1209–1216. [Google Scholar] [CrossRef]
- Mirzajani, F.; Ghassempour, A.; Aliahmadi, A.; Esmaeili, M.A. Antibacterial Effect of Silver Nanoparticles on Staphylococcus Aureus. Res. Microbiol. 2011, 162, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, B.; Garmaroudi, F.S.; Hashemi, M.; Nezhad, H.R.; Nasrollahi, A.; Ardalan, S.; Ardalan, S. Comparison of the Anti-Bacterial Activity on the Nanosilver Shapes: Nanoparticles, Nanorods and Nanoplates. Adv. Powder Technol. 2012, 23, 22–26. [Google Scholar] [CrossRef]
- Panacek, A.; Kvítek, L.; Prucek, R.; Kolar, M.; Vecerova, R.; Pizúrova, N.; Sharma, V.K.; Nevecna, T.; Zboril, R. Silver Colloid Nanoparticles: Synthesis, Characterization, and Their Antibacterial Activity. J. Phys. Chem. B 2006, 110, 16248–16253. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.-C.; Wu, K.-H.; Liu, M.-J.; Lin, W.-P.; Hu, M.-K. Evaluation of the Antibacterial Efficacy of Bamboo Charcoal/Silver Biological Protective Material. Mater. Chem. Phys. 2009, 113, 474–479. [Google Scholar] [CrossRef]


{kind=link}
| Antiseptic | S. aureus | References | P. aeruginosa | References |
|---|---|---|---|---|
| MIC (µg/mL) | MIC (µg/mL) | |||
| OCT | 0.25–4 | [26,31,100,101] | 1–8 | [25,26,100,101] |
| PVP-I | 7.8–512 | [26,102,103,104] | 2048–50,000 | [105,106,107,108] |
| PHMB | 0.25–8 | [26,101,109,110,111,112] | 2–32 | [26,101,113,114] |
| NaClO | 250–4063 | [115,116,117,118] | 1000–8192 | [119,120,121] |
| Nano-silver | 5–1350 | [122,123,124] | 0.3–27 | [125,126] |
| Indication | Anti-Bacterial Substance | |
|---|---|---|
| First Choice | Second Choice | |
| Wounds without drainage | Hypochlorite | - |
| Critically colonized wounds, wounds at risk of infection | PHMB (0.02%, 0.04%, 0.1%), OCT 0.05% | OCT/hypochlorite, silver |
| Bitten, stab and gunshot wounds | PVP-I | Hypochlorite |
| Wounds colonized or infected by MDRO | OCT | OCT 0.05%, PHMB, silver |
| Decontamination of acute and chronic wounds | PHMB, hypochlorite | - |
| Burns | PHMB, OCT 0.05% | OCT/hypochlorite |
| Rinsing the peritoneal cavity | Hypochlorite | - |
| Risk of PNS exposure | Hypochlorite | PVP-I |
| SSI prophylaxis | OCT | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babalska, Z.Ł.; Korbecka-Paczkowska, M.; Karpiński, T.M. Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment. Pharmaceuticals 2021, 14, 1253. https://doi.org/10.3390/ph14121253
Babalska ZŁ, Korbecka-Paczkowska M, Karpiński TM. Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment. Pharmaceuticals. 2021; 14(12):1253. https://doi.org/10.3390/ph14121253
Chicago/Turabian StyleBabalska, Zuzanna Łucja, Marzena Korbecka-Paczkowska, and Tomasz M. Karpiński. 2021. "Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment" Pharmaceuticals 14, no. 12: 1253. https://doi.org/10.3390/ph14121253
APA StyleBabalska, Z. Ł., Korbecka-Paczkowska, M., & Karpiński, T. M. (2021). Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment. Pharmaceuticals, 14(12), 1253. https://doi.org/10.3390/ph14121253