Oxidative Stress in Preterm Infants: Overview of Current Evidence and Future Prospects

 , ,
, , 
Abstract
1. Introduction
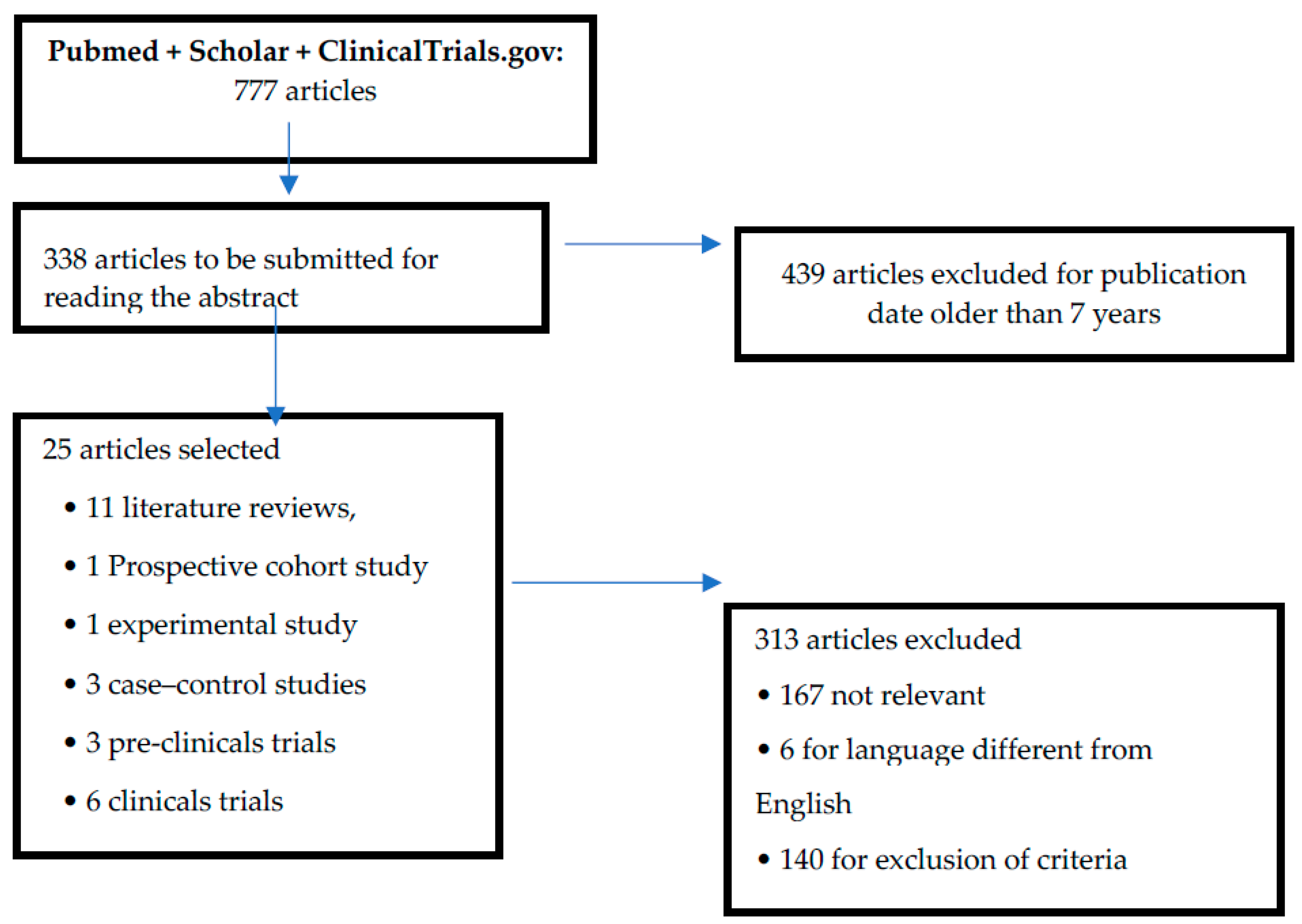
2. Search Strategy
3. Results
4. Discussion
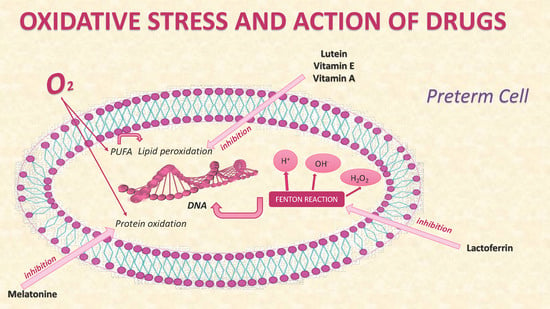
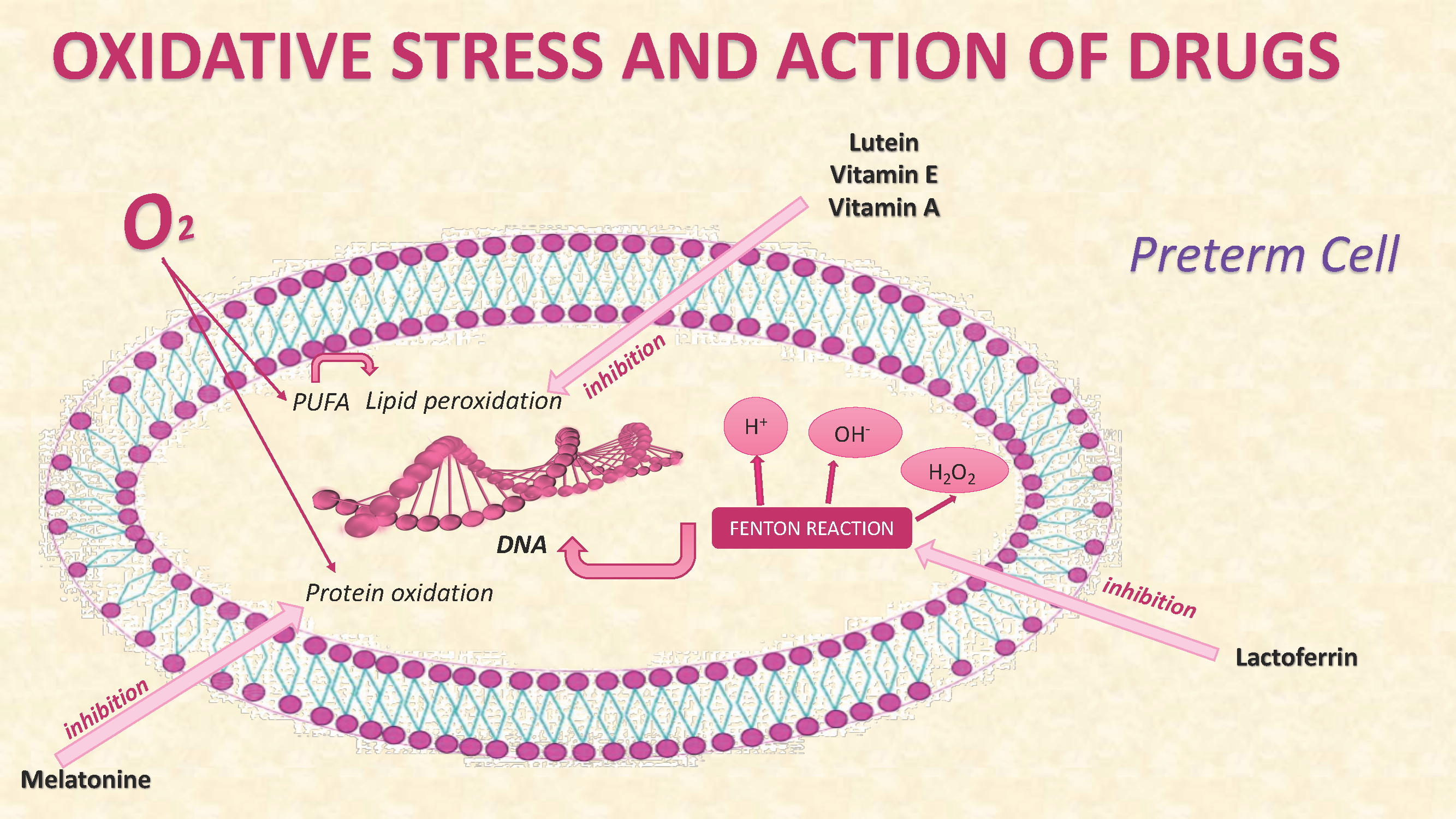
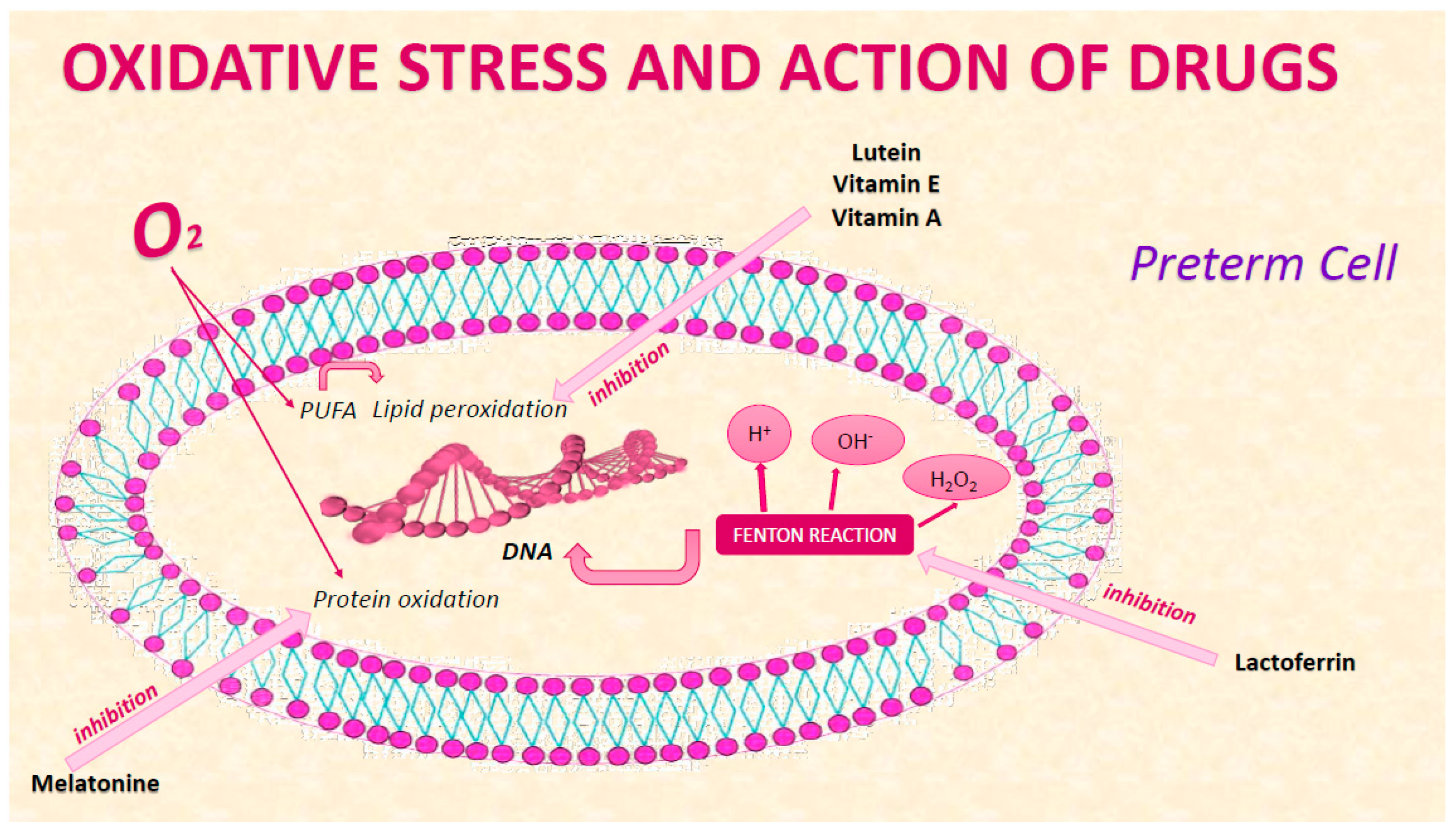
4.1. Molecules that Suffer Damage from FR
4.1.1. Proteins
4.1.2. Lipids
4.1.3. Nucleic Acids
4.2. Therapeutical View from Experimental to Clinical Evidence
4.2.1. Pre-Clinical Trials
4.2.2. Clinical Trials
4.3. Future Prospects
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Althabe, F.; Bhutta, Z.; Blencowe, H.; Chandra-mouli, V.; Chou, D.; Costello, A.; Cousens, S.; Davidge, R.; De Graft Johnson, J.; Dean, S.; et al. Born Too Soon: The Global Action Report on Preterm Birth; World Health Organization: Geneva, Switzerland, 2012; ISBN 9789241503433. [Google Scholar]
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.K.; Curtin, S.C.; Matthews, T.J. Births: Final Data for 2014. Natl. Vit. Stat. Rep. 2015, 64, 1–64. [Google Scholar]
- March of Dimes. The March of Dimes Data Book for Policy Makers: Maternal, Infant, and Health in the United States; March of Dimes: Washington, DC, USA, 2012. [Google Scholar]
- Requejo, J.; Merialdi, M.; Althabe, F.; Keller, M.; Katz, J.; Menon, R. Born Too Soon: Care during pregnancy and childbirth to reduce preterm deliveries and improve health outcomes of the preterm baby. Reprod. Health 2013, 10 (Suppl. 1), S4. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Zhang, Z.; Morales, M.; Wang, Y.; Khafipour, E.; Friel, J. Feeding practice influences gut microbiome composition in very low birth weight preterm infants and the association with oxidative stress: A prospective cohort study. Free Radic. Biol. Med. 2019, 142, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Peña-Bautista, C.; Durand, T.; Vigor, C.; Oger, C.; Galano, J.-M.; Cháfer-Pericás, C. Non-invasive assessment of oxidative stress in preterm infants. Free Radic. Biol. Med. 2019, 142, 73–81. [Google Scholar] [CrossRef]
- Stefanovic, V.; Andersson, S.; Vento, M. Oxidative stress - Related spontaneous preterm delivery challenges in causality determination, prevention and novel strategies in reduction of the sequelae. Free Radic. Biol. Med. 2019, 142, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Betteridge, D.J. What is oxidative stress? Metabolism 2000, 49, 3–8. [Google Scholar] [CrossRef]
- Distefano, G.; Sciacca, P.; Mattia, C.; Betta, P.; Falsaperla, R.; Romeo, M.; Amato, M. Troponin I as a Biomarker of Cardiac Injury in Neonates with Idiopathic Respiratory Distress. Am. J. Perinatol. 2006, 23, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Panfoli, I.; Candiano, G.; Malova, M.; De Angelis, L.; Cardiello, V.; Buonocore, G.; Ramenghi, L.A. Oxidative Stress as a Primary Risk Factor for Brain Damage in Preterm Newborns. Front. Pediatr. 2018, 6, 369. [Google Scholar] [CrossRef]
- Perrone, S.; Tataranno, M.L.; Negro, S.; Longini, M.; Marzocchi, B.; Proietti, F.; Iacoponi, F.; Capitani, S.; Buonocore, G. Early identification of the risk for free radical-related diseases in preterm newborns. Early Hum. Dev. 2010, 86, 241–244. [Google Scholar] [CrossRef]
- Sies, H.; Jones, D.P. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef]
- Dizdaroglu, M.; Jaruga, P. Mechanisms of free radical-induced damage to DNA. Free Radic. Res. 2012, 46, 382–419. [Google Scholar] [CrossRef] [PubMed]
- Mut-Salud, N.; Alvarez, P.; Garrido, J.M.; Carrasco, E.; Aránega, A.; Rodríguez-Serrano, F. Antioxidant Intake and Antitumor Therapy: Toward Nutritional Recommendations for Optimal Results. Oxidative Med. Cell. Longev. 2016, 2016, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Martorell, M.; Arbiser, J.L.; Sureda, A.; Martins, N.; Maurya, P.K.; Sharifi-Rad, J.; Kumar, P.; Sharifi-Rad, J. Antioxidants: Positive or Negative Actors? Biomolecules 2018, 8, 124. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.A.; Ahmad, I.; Zimmerman, M.C. Oxidative Stress and Preterm Birth: An Integrative Review. Biol. Res. Nurs. 2018, 20, 497–512. [Google Scholar] [CrossRef]
- Forde, D.; Deming, D.D.; Tan, J.C.; Phillips, R.M.; Fry-Bowers, E.K.; Barger, M.K.; Bahjri, K.; Angeles, D.M.; Boskovic, D.S. Oxidative Stress Biomarker Decreased in Preterm Neonates Treated with Kangaroo Mother Care. Biol. Res. Nurs. 2020, 22, 188–196. [Google Scholar] [CrossRef]
- Lawenda, B.D.; Kelly, K.M.; Ladas, E.J.; Sagar, S.M.; Vickers, A.J.; Blumberg, J.B. Should Supplemental Antioxidant Administration Be Avoided During Chemotherapy and Radiation Therapy? J. Natl. Cancer Inst. 2008, 100, 773–783. [Google Scholar] [CrossRef]
- Perkins, A.; Nelson, K.J.; Parsonage, D.; Poole, L.B.; Karplus, P. Peroxiredoxins: Guardians against oxidative stress and modulators of peroxide signaling. Trends Biochem. Sci. 2015, 40, 435–445. [Google Scholar] [CrossRef]
- Valero, Y.; Martínez-Morcillo, F.J.; Esteban, M.; Chaves-Pozo, E.; Cuesta, A. Fish Peroxiredoxins and Their Role in Immunity. Biology 2015, 4, 860–880. [Google Scholar] [CrossRef]
- Marseglia, L.; D’Angelo, G.; Granese, R.; Falsaperla, R.; Reiter, R.J.; Corsello, G.; Gitto, E. Role of oxidative stress in neonatal respiratory distress syndrome. Free Radic. Biol. Med. 2019, 142, 132–137. [Google Scholar] [CrossRef]
- Garofoli, F. Oral Melatonin as Neuroprotectant in Preterm Infants. Available online: https://clinicaltrials.gov/ct2/show/NCT04235673 (accessed on 22 January 2020).
- Ain Shams University. Effect of Melatonin on Feeding Intolerance and Incidence of Necrotizing Enterocolitis in Preterm Infants. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04304807 (accessed on 22 January 2020).
- Di Fiore, J.M.; Vento, M. Intermittent hypoxemia and oxidative stress in preterm infants. Respir. Physiol. Neurobiol. 2019, 266, 121–129. [Google Scholar] [CrossRef]
- Lavu, N.; Richardson, L.S.; Radnaa, E.; Kechichian, T.; Urrabaz-Garza, R.; Sheller-Miller, S.; Bonney, E.; Menon, R. Oxidative stress-induced downregulation of glycogen synthase kinase 3 beta in fetal membranes promotes cellular senescence†. Biol. Reprod. 2019, 101, 1018–1030. [Google Scholar] [CrossRef] [PubMed]
- Endesfelder, S.; Strauß, E.; Scheuer, T.; Schmitz, T.; Bührer, C. Antioxidative effects of caffeine in a hyperoxia-based rat model of bronchopulmonary dysplasia. Respir. Res. 2019, 20, 88. [Google Scholar] [CrossRef] [PubMed]
- Romantsik, O.; Agyemang, A.A.; Sveinsdóttir, S.; Rutardóttir, S.; Holmqvist, B.; Cinthio, M.; Mörgelin, M.; Gumus, H.G.; Karlsson, H.; Hansson, S.R.; et al. The heme and radical scavenger α1-microglobulin (A1M) confers early protection of the immature brain following preterm intraventricular hemorrhage. J. Neuroinflammation 2019, 16, 122. [Google Scholar] [CrossRef] [PubMed]
- Büyüktiryaki, M.; Tayman, C.; Koyuncu, I.; Cakir, U.; Turkmenoglu, T.T.; Cakir, E.; Okur, N. Therapeutic and preventative effects of ankaferd blood stopper in an experimental necrotizing enterocolitis model. Biomed. Pharmacother. 2019, 110, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Millán, I.; Piñero-Ramos, J.D.; Lara, I.; Parra-Llorca, A.; Torres-Cuevas, I.; Vento, M. Oxidative Stress in the Newborn Period: Useful Biomarkers in the Clinical Setting. Antioxidants 2018, 7, 193. [Google Scholar] [CrossRef]
- Aceti, A.; Beghetti, I.; Martini, S.; Faldella, G.; Corvaglia, L. Oxidative Stress and Necrotizing Enterocolitis: Pathogenetic Mechanisms, Opportunities for Intervention, and Role of Human Milk. Oxidative Med. Cell. Longev. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Martin, A.; Faës, C.; Debevec, T.; Rytz, C.; Millet, G.; Pialoux, V. Preterm birth and oxidative stress: Effects of acute physical exercise and hypoxia physiological responses. Redox Biol. 2018, 17, 315–322. [Google Scholar] [CrossRef]
- Sun, H. Effects of Early Vitamin A Supplementation on the Risk for Retinopathy of Prematurity in Extremely Preterm Infants. Available online: https://clinicaltrials.gov/ct2/show/NCT03154723 (accessed on 22 January 2020).
- Torres-Cuevas, I.; Parra-Llorca, A.; Sánchez-Illana, Á.; Nuñez-Ramiro, A.; Kuligowski, J.; Cháfer-Pericás, C.; Cernada, M.; Escobar, J.; Vento, M. Oxygen and oxidative stress in the perinatal period. Redox Biol. 2017, 12, 674–681. [Google Scholar] [CrossRef]
- Norishadkam, M.; Andishmand, S.; Reza, J.Z.; Sakhvidi, M.J.Z.; Hachesoo, V.R. Oxidative stress and DNA damage in the cord blood of preterm infants. Mutat. Res. Toxicol. Environ. Mutagen. 2017, 824, 20–24. [Google Scholar] [CrossRef]
- Dutta, E.H.; Behnia, F.; Boldogh, I.; Saade, G.; Taylor, B.D.; Kacerovsky, M.; Menon, R. Oxidative stress damage-associated molecular signaling pathways differentiate spontaneous preterm birth and preterm premature rupture of the membranes. Mol. Hum. Reprod. 2015, 22, 143–157. [Google Scholar] [CrossRef]
- Yzydorczyk, C.; Mitanchez, D.; Buffat, C.; Ligi, I.; Grandvuillemin, I.; Boubred, F.; Simeoni, U. Stress oxydant chez l’enfant prématuré: Causes, biomarqueurs et possibilités thérapeutiques. Arch. Pédiatrie 2015, 22, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- NICHD Neonatal Research Network. Vitamin E for Extremely Preterm Infants. Available online: https://clinicaltrials.gov/ct2/show/NCT01193270?term=Vitamin+E+for+Extremely+Preterm+Infants (accessed on 22 January 2020).
- University of Siena. Evaluation of Antioxidant Activity of Oral Lutein in Preterm and Term Newborn. Available online: https://clinicaltrials.gov/ct2/show/NCT02068807?term=%2C+Evaluation+of+Antioxidant+Activity+of+Oral+Lutein+in+Preterm+and+Term+Newborn (accessed on 22 January 2020).
- University of Siena. Upplementation with Lactoferrin in Preterm Newborns (lactoprenew). Available online: https://clinicaltrials.gov/ct2/show/record/NCT01172236 (accessed on 22 January 2020).
- Tao, E.-F.; Yuan, T.-M. Vitamin A level and diseases of premature infants. Zhongguo Dang Dai Er Ke Za Zhi 2016, 18, 177–182. [Google Scholar]
- Aydemir, C.; Dilli, D.; Uras, N.; Ulu, H.O.; Oguz, S.S.; Erdeve, O.; Dilmen, U. Total oxidant status and oxidative stress are increased in infants with necrotizing enterocolitis. J. Pediatr. Surg. 2011, 46, 2096–2100. [Google Scholar] [CrossRef] [PubMed]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Harma, M.; Harma, M.; Erel, O. Measurement of the total antioxidant response in preeclampsia with a novel automated method. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 118, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M. Short- and Long-Term Outcomes for Extremely Preterm Infants. Am. J. Perinatol. 2016, 33, 318–328. [Google Scholar] [CrossRef]
- Ozdemir, V. Microbiome Special Issue: Food, Drugs, Diagnostics, and Built Environments. OMICS J. Integr. Biol. 2018, 22, 89. [Google Scholar] [CrossRef]
- Perrone, S.; Laschi, E.; Buonocore, G. Oxidative stress biomarkers in the perinatal period: Diagnostic and prognostic value. Semin. Fetal Neonatal Med. 2020, 25, 101087. [Google Scholar] [CrossRef]
- Yang, J. The expanding landscape of the thiol redox proteome. Toxicol. Lett. 2016, 258, S43. [Google Scholar] [CrossRef]
- McDonagh, B. Detection of ROS Induced Proteomic Signatures by Mass Spectrometry. Front. Physiol. 2017, 8, 1–7. [Google Scholar] [CrossRef]
- Gould, N.S.; Evans, P.; Martínez-Acedo, P.; Marino, S.M.; Gladyshev, V.N.; Carroll, K.S.; Ischiropoulos, H. Site-Specific Proteomic Mapping Identifies Selectively Modified Regulatory Cysteine Residues in Functionally Distinct Protein Networks. Chem. Biol. 2015, 22, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Leichert, L.I.O.; Gehrke, F.; Gudiseva, H.V.; Blackwell, T.; Ilbert, M.; Walker, A.K.; Strahler, J.R.; Andrews, P.; Jakob, U. Quantifying changes in the thiol redox proteome upon oxidative stress in vivo. Proc. Natl. Acad. Sci. USA 2008, 105, 8197–8202. [Google Scholar] [CrossRef] [PubMed]
- Go, Y.-M.; Roede, J.R.; Walker, D.I.; Duong, D.M.; Seyfried, N.T.; Orr, M.; Liang, Y.; Pennell, K.D.; Jones, D.P. Selective Targeting of the Cysteine Proteome by Thioredoxin and Glutathione Redox Systems. Mol. Cell. Proteom. 2013, 12, 3285–3296. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Ha, S.; Lee, H.Y.; Lee, K.-J. ROSics: Chemistry and proteomics of cysteine modifications in redox biology. Mass Spectrom. Rev. 2015, 34, 184–208. [Google Scholar] [CrossRef] [PubMed]
- Held, J.M. Redox Systems Biology: Harnessing the Sentinels of the Cysteine Redoxome. Antioxid. Redox Signal. 2019, 32, 659–676. [Google Scholar] [CrossRef] [PubMed]
- Cobley, J.N.; Husi, H. Immunological Techniques to Assess Protein Thiol Redox State: Opportunities, Challenges and Solutions. Antioxidants 2020, 9, 315. [Google Scholar] [CrossRef]
- Perrone, S.; Tataranno, M.L.; Stazzoni, G.; Buonocore, G. Biomarkers of oxidative stress in fetal and neonatal diseases. J. Matern. Neonatal Med. 2012, 25, 2575–2578. [Google Scholar] [CrossRef]
- Frijhoff, J.; Winyard, P.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef]
- Tsikas, D. Analytical methods for 3-nitrotyrosine quantification in biological samples: The unique role of tandem mass spectrometry. Amino Acids 2010, 42, 45–63. [Google Scholar] [CrossRef]
- Franco, M.C.; Estevez, A.G. Tyrosine nitration as mediator of cell death. Cell. Mol. Life Sci. 2014, 71, 3939–3950. [Google Scholar] [CrossRef]
- Sánchez-Illana, Á.; Parra-Llorca, A.; Escuder, D.; Pallás-Alonso, C.; Cernada, M.; Gormáz, M.; Vento, M.; Kuligowski, J. Biomarkers of oxidative stress derived damage to proteins and DNA in human breast milk. Anal. Chim. Acta 2018, 1016, 78–85. [Google Scholar] [CrossRef]
- Torres-Cuevas, I.; Kuligowski, J.; Cárcel, M.; Cháfer-Pericás, C.; Asensi, M.; Solberg, R.; Cubells, E.; Nunez, A.; Saugstad, O.D.; Vento, M.; et al. Protein-bound tyrosine oxidation, nitration and chlorination by-products assessed by ultraperformance liquid chromatography coupled to tandem mass spectrometry. Anal. Chim. Acta 2016, 913, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Solberg, R.; Andresen, J.H.; Escrig, R.; Vento, M.; Saugstad, O.D. Resuscitation of Hypoxic Newborn Piglets With Oxygen Induces a Dose-Dependent Increase in Markers of Oxidation. Pediatr. Res. 2007, 62, 559–563. [Google Scholar] [CrossRef]
- Ledo, A.; Arduini, A.; Asensi, A.M.; Sastre, J.; Escrig, R.; Brugada, M.; Aguar, M.; Saenz, P.; Vento, M. Human milk enhances antioxidant defenses against hydroxyl radical aggression in preterm infants. Am. J. Clin. Nutr. 2008, 89, 210–215. [Google Scholar] [CrossRef]
- Escobar, J.; Teramo, K.; Stefanovic, V.; Andersson, S.; Asensi, M.A.; Arduini, A.; Cubells, E.; Sastre, J.; Vento, M. Amniotic Fluid Oxidative and Nitrosative Stress Biomarkers Correlate with Fetal Chronic Hypoxia in Diabetic Pregnancies. Neonatology 2013, 103, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Dalli, J.; Colas, R.A.; Winkler, J.W.; Chiang, N. Protectins and maresins: New pro-resolving families of mediators in acute inflammation and resolution bioactive metabolome. Biochim. Biophys. Acta (BBA)—Bioenerg. 2014, 1851, 397–413. [Google Scholar] [CrossRef]
- Musiek, E.S.; Yin, H.; Milne, G.L.; Morrow, J.D. Recent advances in the biochemistry and clinical relevance of the isoprostane pathway. Lipids 2005, 40, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, G.; Rakshasbhuvankar, A.; Simmer, K.; Mori, T.; Croft, K.; Currie, A. Efficacy and safety of a novel fish oil-based emulsion (SMOFlipid®) compared with olive oil-based lipid emulsion (Cli-nOleic®) in term and near-term (>34 weeks) surgical neonates—A randomised controlled trial. In Proceedings of the Pediatric Academic Societies (PAS) Annual Meeting, Washington, DC, USA, 4–7 May 2013. Abstract 3838.626. [Google Scholar]
- Deshpande, G.C.; Simmer, K.; Mori, T.; Croft, K. Parenteral lipid emulsions based on olive oil compared with soybean oil in preterm (<28 weeks’gestation) neonates: A randomized controlled trial. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 619–625. [Google Scholar] [PubMed]
- Deshpande, G.C.; Cai, W. Use of Lipids in Neonates Requiring Parenteral Nutrition. J. Parenter. Enter. Nutr. 2020, 44 (Suppl. 1), S45–S54. [Google Scholar] [CrossRef]
- Chavez-Valdez, R.; Ahlawat, R.; Wills-Karp, M.; Nathan, A.; Ezell, T.; Gauda, E.B. Correlation between Serum Caffeine Levels and Changes in Cytokine Profile in a Cohort of Preterm Infants. J. Pediatr. 2011, 158, 57–64. [Google Scholar] [CrossRef]
- Manning, F.A.; Morrison, I.; Lange, I.R.; Harman, C.R.; Chamberlain, P.F. Fetal assessment based on fetal biophysical profile scoring: Experience in 12,620 referred high-risk pregnancies. Am. J. Obstet. Gynecol. 1985, 151, 343–350. [Google Scholar] [CrossRef]
- Grosso, L.M.; Triche, E.W.; Belanger, K.; Benowitz, N.L.; Holford, T.R.; Bracken, M.B. Caffeine Metabolites in Umbilical Cord Blood, Cytochrome P-450 1A2 Activity, and Intrauterine Growth Restriction. Am. J. Epidemiol. 2006, 163, 1035–1041. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ambalavanan, N.; Carlo, W.A.; D’Angio, C.T.; McDonald, S.A.; Das, A.; Schendel, D.; Thorsen, P.; Higgings, R.D.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Cytokines associated with bronchopulmonary dysplasia or death in extremely low birth weight infants. Pediatrics 2009, 123, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Goker, H.; Haznedaroglu, I.C.; Ercetin, S.; Kirazli, S.; Akman, U.; Ozturk, Y.; Firat, H.C. Haemostatic actions of the folkloric medicinal plant extract Ankaferd Blood Stopper. J. Int. Med. Res. 2008, 36, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Beyazit, Y.; Kurtm, M.; Kekilli, M.; Goker, H.; Haznedaroglu, I.C. Evaluation of hemostatic effects of Ankaferd as an alternative medicine. Altern. Med. Rev. 2010, 15, 329–336. [Google Scholar]
- Haznedaroglu, B.Z.; Beyazit, Y.; Walker, S.L.; Haznedaroğlu, I.C. Pleiotropic cellular, hemostatic, and biological actions of Ankaferd hemostat. Crit. Rev. Oncol. 2012, 83, 21–34. [Google Scholar] [CrossRef]
- Belizy, S.; Nasarova, I.N.; Procof’Ev, V.N.; Sorokina, I.A.; Puschkina, N.V.; Lukach, A.I. Changes in antioxidative properties of lactoferrin from women’s milk during deamidation. Biochestry (Moscow) 2001, 66, 576–580. [Google Scholar] [CrossRef]
- Raghuveer, T.S.; McGuire, E.M.; Martin, S.M.; Wagner, B.A.; Rebouche, C.J.; Buetter, G.R.; Widness, J.A. Lactoferrin in the preterm infants’ diet attenuates iron-induced oxidation products. Pediatr. Res. 2002, 52, 964–972. [Google Scholar] [CrossRef]
- Van De Looij, Y.; Ginet, V.; Chatagner, A.; Toulotte, A.; Somm, E.; Hüppi, P.S.; Sizonenko, S.V. Lactoferrin during lactation protects the immature hypoxic-ischemic rat brain. Ann. Clin. Transl. Neurol. 2014, 1, 955–967. [Google Scholar] [CrossRef]
- Perrone, S.; Tei, M.; Longini, M.; Santacroce, A.; Turrisi, G.; Proietti, F.; Felici, C.; Picardi, A.; Bazzini, F.; Vasarri, P.; et al. Lipid and Protein Oxidation in Newborn Infants after Lutein Administration. Oxidative Med. Cell. Longev. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Ramani, M.; Van Groen, T.; Kadish, I.; Ambalavanan, N.; McMahon, L.L. Vitamin A and retinoic acid combination attenuates neonatal hyperoxia-induced neurobehavioral impairment in adult mice. Neurobiol. Learn. Mem. 2017, 141, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Yawno, T.; Mahen, M.; Li, J.; Fahey, M.C.; Jenkin, G.; Miller, S.L. The Beneficial Effects of Melatonin Administration Following Hypoxia-Ischemia in Preterm Fetal Sheep. Front. Cell. Neurosci. 2017, 11, 296. [Google Scholar] [CrossRef] [PubMed]
- Acuna-Castroviejo, D.; Martin, M.; Macias, M.; Escames, G.; Leon, J.; Reiter, R.J. Melatonin, mitochondria, and cellular bioenergetics. J. Pineal Res. 2001, 30, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Pandi-Perumal, S.R.; Bahammam, A.S.; Brown, G.M.; Spence, D.W.; Bharti, V.K.; Kaur, C.; Hardeland, R.; Cardinali, D.; Pandi-Perumal, S.R. Melatonin Antioxidative Defense: Therapeutical Implications for Aging and Neurodegenerative Processes. Neurotox. Res. 2012, 23, 267–300. [Google Scholar] [CrossRef]
- Fu, J.; Zhao, S.-D.; Liu, H.-J.; Yuan, Q.-H.; Liu, S.-M.; Zhang, Y.; Ling, E.-A.; Hao, A. Melatonin promotes proliferation and differentiation of neural stem cells subjected to hypoxia in vitro. J. Pineal Res. 2011, 51, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Villapol, S.; Fau, S.; Renolleau, S.; Biran, V.; Charriaut-Marlangue, C.; Baud, O. Melatonin Promotes Myelination by Decreasing White Matter Inflammation After Neonatal Stroke. Pediatr. Res. 2011, 69, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Hardeland, R.; Tan, D.-X.; Reiter, R.J. Kynuramines, metabolites of melatonin and other indoles: The resurrection of an almost forgotten class of biogenic amines. J. Pineal Res. 2009, 47, 109–126. [Google Scholar] [CrossRef]
- Tan, D.-X.; Manchester, L.C.; Terron, M.P.; Flores, L.J.; Reiter, R. One molecule, many derivatives: A never-ending interaction of melatonin with reactive oxygen and nitrogen species? J. Pineal Res. 2007, 42, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Hassell, K.J.; Ezzati, M.; Alonso-Alconada, D.; Hausenloy, D.J.; Robertson, N.J. New horizons for newborn brain protection: Enhancing endogenous neuroprotection. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F541–F552. [Google Scholar] [CrossRef]
- Gollwitzer, E.S.; Saglani, S.; Trompette, A.; Yadava, K.; Sherburn, R.; McCoy, K.D.; Nicod, L.P.; Lloyd, C.M.; Marsland, B.J. Lung microbiota promotes tolerance to allergens in neonates via PD-L1. Nat. Med. 2014, 20, 642–647. [Google Scholar] [CrossRef]
- Nardiello, C.; Mižíková, I.; Silva, D.M.; Ruiz-Camp, J.; Mayer, K.; Vadász, I.; Herold, S.; Seeger, W.; Morty, R.E. Standardisation of oxygen exposure in the development of mouse models for bronchopulmonary dysplasia. Dis. Model. Mech. 2016, 10, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Berkelhamer, S.K.; Kim, G.A.; Radder, J.E.; Wedgwood, S.; Czech, L.; Steinhorn, R.H.; Schumacker, P.T. Developmental differences in hyperoxia-induced oxidative stress and cellular responses in the murine lung. Free Radic. Biol. Med. 2013, 61, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Segal, L.; Clemente, J.C.; Wu, B.; Wikoff, W.R.; Gao, Z.; Li, Y.; Ko, J.P.; Rom, W.N.; Blaser, M.J.; Weiden, M.D. Randomised, double-blind, placebo-controlled trial with azithromycin selects for anti-inflammatory microbial metabolites in the emphysematous lung. Thorax 2016, 72, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Pellaton, C.; Nutten, S.; Thierry, A.-C.; Boudousquie, C.; Barbier, N.; Blanchard, C.; Corthésy, B.; Mercenier, A.; Spertini, F. Intragastric and Intranasal Administration of Lactobacillus paracasei NCC2461 Modulates Allergic Airway Inflammation in Mice. Int. J. Inflamm. 2012, 2012, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.; Srinivas, G.; Kuenzel, S.; Linnenbrink, M.; Alnahas, S.; Bruce, K.D.; Steinhoff, U.; Baines, J.F.; Schaible, U.E. Environmentally Determined Differences in the Murine Lung Microbiota and Their Relation to Alveolar Architecture. PLoS ONE 2014, 9, e113466. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.; Tibboel, D.; De Kleer, I.M.; Reiss, I.K.M.; Rottier, R.J. The Future of Bronchopulmonary Dysplasia: Emerging Pathophysiological Concepts and Potential New Avenues of Treatment. Front. Med. 2017, 4, 61. [Google Scholar] [CrossRef]
- Capasso, L.; Vento, G.; Loddo, C.; Tirone, C.; Iavarone, F.; Raimondi, F.; Dani, C.; Fanos, V. Oxidative Stress and Bronchopulmonary Dysplasia: Evidences from Microbiomics, Metabolomics, and Proteomics. Front. Pediatr. 2019, 7, 30. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Type of Study | Review Article | Experimental Study | Preclinical trial | Clinical trial |
|---|---|---|---|---|
| 2020 | DOI: 10.1177/1099800419900231 [17] DOI: 10.1016/j.freeradbiomed.2019.02.032 [5] | ClinicalTrials.gov Identifier: NCT04235673 [22] ClinicalTrials.gov Identifier: NCT04304807 [23] | ||
| 2019 | DOI: 10.1016/j.freeradbiomed.2019.02.019 [6] DOI: 10.1016/j.resp.2019.05.006 [24] DOI: 10.1016/j.freeradbiomed.2019.06.008 [7] DOI: 10.1016/j.freeradbiomed.2019.04.029 [21] | DOI: 10.1093/biolre/ioz119 [25] | DOI: 10.1186/s12931-019-1063-5 [26] DOI: 10.1186/s12974-019-1486-4. [27] DOI: 10.1016/j.biopha.2018.11.023 [28] | |
| 2018 | DOI: 10.3389/fped.2018.00369 [10] DOI: 10.3390/antiox7120193 [29] DOI: 10.1155/2018/7397659 [30] DOI: 10.1177/1099800418791028 [16] DOI: 10.1016/j.redox.2018.04.022 [31] | ClinicalTrials.gov Identifier: NCT03154723 [32] | ||
| 2017 | DOI: 10.1016/j.redox.2017.03.011 [33] | DOI: 10.1016/j.mrgentox.2017.10.003 [34] | ||
| 2016 | DOI: 10.1093/molehr/gav074 [35] | |||
| 2015 | DOI: 10.1016/j.arcped.2015.05.019 [36] | ClinicalTrials.gov Identifier: NCT01193270 [37] | ||
| 2014 | ClinicalTrials.gov Identifier: NCT02068807 [38] | |||
| 2013 | ClinicalTrials.gov Identifier: NCT01172236 [39] |
| Substances under Study | α1-Microglobulin | Caffeine | Ankaferd Blood Stopper® |
|---|---|---|---|
| Preclinical trials | The heme and A1M confers early protection of the immature brain following preterm intraventricular hemorrhage J Neuroinflammation | Antioxidative effects of caffeine in a hyperoxia-based rat model of bronchopulmonary dysplasia | Therapeutic and preventative effects of ankaferd blood stopper in an experimental necrotizing enterocolitis model |
| Authors | Olga Romantsik, et al. [27] | Stefanie Endesfelder, et al. [26] | Mehmet Buyuktiryaki, et al. [28] |
| Year of publication | 2019 | 2019 | 2019 |
| Cavy (animal) | Rabbits pups | Rats pups | Rats pups |
| Molecule | Protein | Methylxanthine | Protein |
| Mechanisms of action | -Heme binding -Reductase activity -Radical scavenging -Binding to mitochondria | -Reduced oxidative DNA damage -Protective interference with the oxidative stress response -Antagonism of adenosine receptors -Full blocking of hyperoxia-induced oxidative | -Significantly reduced apoptosis -Reduction intestinal lesion -Antioxidant, antinflammatory, and antiapoptotic properties |
| Distribution | Periventricular cerebellar regions with high plasticity (white matter, subventricular zone, corpus callosum, corona radiata, thalamocortical projection) | Pulmonary | Intestinal |
| Administration | Intracerebroventricular | Intravenous | Intraperitoneal |
| Posology | 25 μL | 10 mg/kg every 48 h beginning on the day of birth | 2 mL/kg by diluting 2 mL with saline at a ratio of 1:3 |
| Protective role | neuroprotective against brain damage following preterm IVH | BPD | NEC |
| Drugs | Lactoferrin | Lutein | Vitamin E | Vitamin A | Studies of | Melatonin |
|---|---|---|---|---|---|---|
| Clinical trials | Supplementation with Lactoferrin in Preterm Newborns (lactoprenew) | Evaluation of Antioxidant Activity of Oral Lutein in Preterm and Term Newborn | Vitamin E for Extremely Preterm Infants | Effects of Early Vitamin A Supplementation on the Risk for Retinopathy of Prematurity in Extremely Preterm Infants | Oral Melatonin as Neuroprotectant in Preterm Infants | Effect of Melatonin on Feeding Intolerance and Incidence of Necrotizing Enterocolitis in Preterm Infants |
| Date | January 2013 | February 2014 | November 2015 | September 2018 | January 2020 | March 2020 |
| Study phase | 4 | 2 | 1 | Not Applicable | Not Applicable | 4 |
| Population | Birthweight ≤ 1500 grand/or gestational age ≤ 32 weeks | Preterm born neonates with gestational age <30 weeks | Preterm infants < 27 weeks’ gestation and < 1000 g birth weight | Premature infants weighing less than 1500 g | Neonates born before 29 + 6-week gestation | Preterm infants < 37 week |
| Total Population | 1300 | 100 | 93 | 262 | 60 | 90 |
| Mechanisms of action | Binds iron with high affinity and its structure is unusually resistant to proteolytic degradation. Antioxidant sequestering free ions of Fe2+ and thus preventing lipid peroxidation and subsequent milk oxidation | Activity of inhibition of peroxidation of membrane lipids is peculiarly important for the photoreceptors and neurons | Effective lipid membrane antioxidant | Effective lipid membrane antioxidant | Potent antioxidant/-inflammatory effect | potent antioxidant/-inflammatory effect |
| Posology | 100 mg/day | 0.28 mg of lutein in two doses: within 6 h | α-tocopheryl acetate 50 IU/kg. 1 dose | 1500 IU/day for 28 day | 3 mg/kg/day for 15 days | 20 mg/day in two doses of 10 mg each with a 1-h interval in between |
| Administration | Enteral | Enteral | Intragastrical | Enteral | Enteral | Enteral |
| Protective role | Neuroprotective | Neuroprotective ROP | Reduce the incidence of death or development of neural impairment | ROP | Neuroprotectant for cerebral ischemia | NEC |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falsaperla, R.; Lombardo, F.; Filosco, F.; Romano, C.; Saporito, M.A.N.; Puglisi, F.; Piro, E.; Ruggieri, M.; Pavone, P. Oxidative Stress in Preterm Infants: Overview of Current Evidence and Future Prospects. Pharmaceuticals 2020, 13, 145. https://doi.org/10.3390/ph13070145
Falsaperla R, Lombardo F, Filosco F, Romano C, Saporito MAN, Puglisi F, Piro E, Ruggieri M, Pavone P. Oxidative Stress in Preterm Infants: Overview of Current Evidence and Future Prospects. Pharmaceuticals. 2020; 13(7):145. https://doi.org/10.3390/ph13070145
Chicago/Turabian StyleFalsaperla, Raffaele, Filadelfo Lombardo, Federica Filosco, Catia Romano, Marco Andrea Nicola Saporito, Federica Puglisi, Ettore Piro, Martino Ruggieri, and Piero Pavone. 2020. "Oxidative Stress in Preterm Infants: Overview of Current Evidence and Future Prospects" Pharmaceuticals 13, no. 7: 145. https://doi.org/10.3390/ph13070145
APA StyleFalsaperla, R., Lombardo, F., Filosco, F., Romano, C., Saporito, M. A. N., Puglisi, F., Piro, E., Ruggieri, M., & Pavone, P. (2020). Oxidative Stress in Preterm Infants: Overview of Current Evidence and Future Prospects. Pharmaceuticals, 13(7), 145. https://doi.org/10.3390/ph13070145