Creatinine-Based Renal Function Estimates and Dosage of Postoperative Pain Management for Elderly Acute Hip Fracture Patients

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Estimated Glomerular Filtration Rate
2.2. CKD Re-Classification Compared with the CKD-EPI
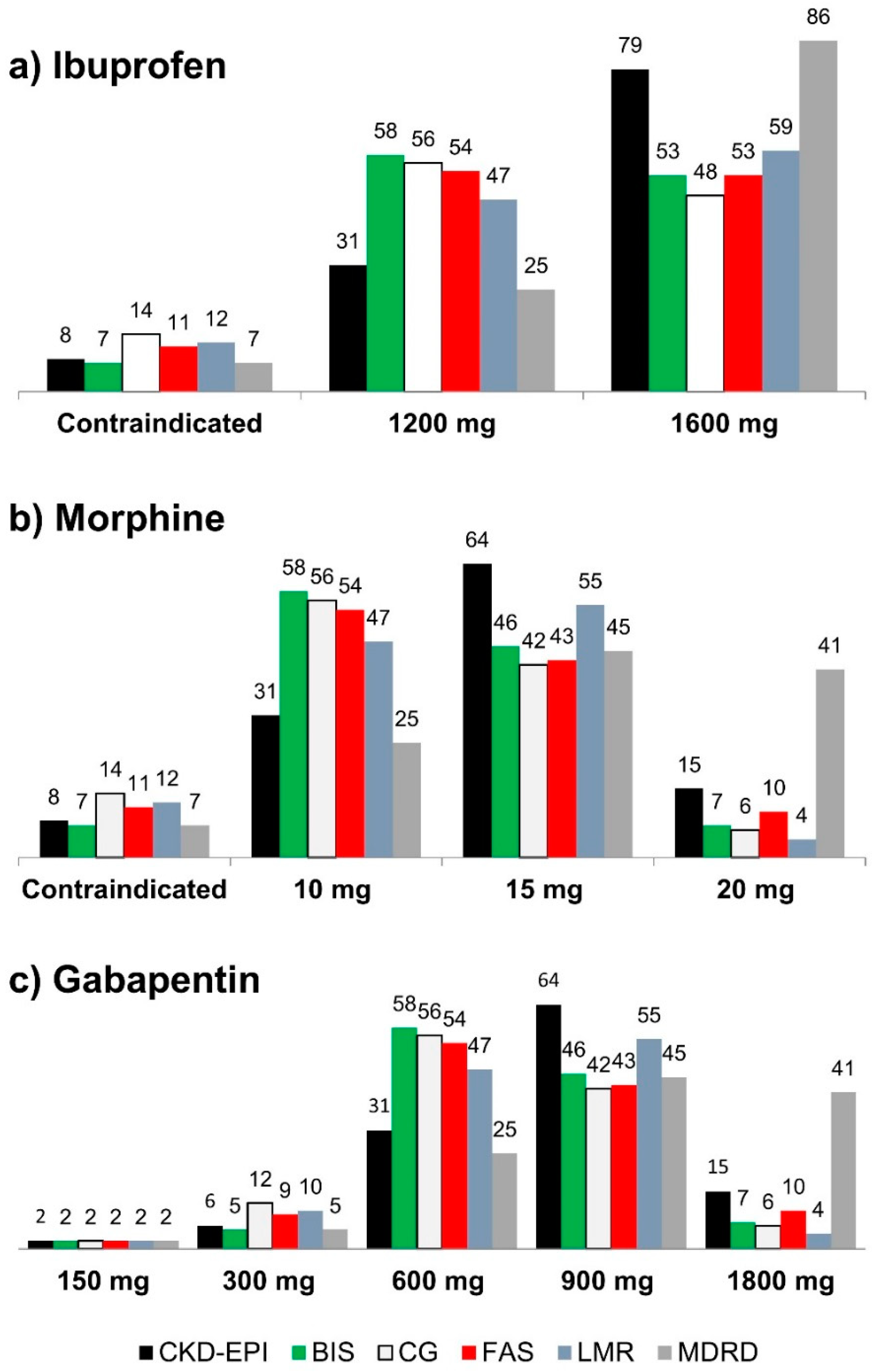
2.3. Shift in Recommended Prescription Dose of Ibuprofen, Morphine, and Gabapentin
3. Discussion
3.1. eGFR Equations Based on Creatinine and Elderly
3.2. Renal Risk Medications and How to Meet the Challenge Clinical Practice
3.3. Strengths and Limitations
4. Materials and Methods
4.1. Ethics Approval
4.2. Design and Setting
4.3. Study Data and Measurement
4.4. Acute Kidney Injury (AKI)
4.5. Medications
4.6. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- White, P.F.; Kehlet, H. Improving postoperative pain management: What are the unresolved issues? Anesthesiology 2010, 112, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Southerland, W.; Catalani, B. The Importance of Optimizing Acute Pain in the Orthopedic Trauma Patient. Orthop. Clin. USA 2017, 48, 445–465. [Google Scholar] [CrossRef] [PubMed]
- Garimella, V.; Cellini, C. Postoperative Pain Control. Clin. Colon Rectal Surg. 2013, 26, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of Postoperative Pain: A Clinical Practice Guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Tawfic, Q.A.; Bellingham, G. Postoperative pain management in patients with chronic kidney disease. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.S.; Parmar, K.S. Management of acute and post-operative pain in chronic kidney disease. F1000Research 2013, 2. [Google Scholar] [CrossRef]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and functional changes with the aging kidney. Adv. Chronic Kidney Dis. 2016, 23, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.J.; Rakheja, D.; Yu, X.; Saxena, R.; Vaziri, N.D.; Silva, F.G. The aging kidney. Kidney Int. 2008, 74, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Mallappallil, M.; Friedman, E.A.; Delano, B.G.; McFarlane, S.I.; Salifu, M.O. Chronic kidney disease in the elderly: Evaluation and management. Clin. Pract. 2014, 11, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Leung, F.; Blauth, M.; Bavonratanavech, S. Surgery for fragility hip fracture—Streamlining the process. Osteoporos. Int. 2010, 21, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Kronborg, L.; Bandholm, T.; Palm, H.; Kehlet, H.; Kristensen, M.T. Feasibility of Progressive Strength Training Implemented in the Acute Ward after Hip Fracture Surgery. PLoS ONE 2014, 9, e93332. [Google Scholar] [CrossRef] [PubMed]
- Nitsch, D.; Mylne, A.; Roderick, P.J.; Smeeth, L.; Hubbard, R.; Fletcher, A. Chronic kidney disease and hip fracture-related mortality in older people in the UK. Nephrol. Dial. Transplant. 2009, 24, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.F.; Biggs, M.L.; Shlipak, M.G.; Seliger, S.; Kestenbaum, B.; Stehman-Breen, C.; Sarnak, M.; Siscovick, D.; Harris, T.; Cauley, J.; et al. Association of kidney function with incident hip fracture in older adults. J. Am. Soc. Nephrol. 2007, 18, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Nickolas, T.L.; McMahon, D.J.; Shane, E. Relationship between Moderate to Severe Kidney Disease and Hip Fracture in the United States. J. Am. Soc. Nephrol. 2006, 17, 3223–3232. [Google Scholar] [CrossRef] [PubMed]
- Marsh, D.; Palm, H. Rising to the challenge of fragility fractures. Injury 2018, 49, 1392. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, J.T.; Schmader, K.E. The Medication Appropriateness Index at 20: Where it Started, Where it has been and Where it May be Going. Drugs Aging 2013, 30, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Dean, M. Opioids in renal failure and dialysis patients. J. Pain Symptom Manag. 2004, 28, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Hörl, W.H. Nonsteroidal Anti-Inflammatory Drugs and the Kidney. Pharmaceuticals 2010, 3, 2291–2321. [Google Scholar] [CrossRef] [PubMed]
- Raouf, M.; Atkinson, T.J.; Crumb, M.W.; Fudin, J. Rational dosing of gabapentin and pregabalin in chronic kidney disease. J. Pain Res. 2017, 10, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Age-Associated General Pharmacological Aspects, Drug Therapy for the Elderly; Martin, W., Ed.; Springer: Berlin, Germany, 2013. [Google Scholar]
- Macedo, E.; Mehta, R.L. Measuring renal function in critically ill patients: Tools and strategies for assessing glomerular filtration rate. Curr. Opin. Crit. Care 2013, 19, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Coresh, J.; Schmid, C.H.; Feldman, H.I.; Froissart, M.; Kusek, J.; Rossert, J.; Van Lente, F.; Bruce, R.D.; Zhang, Y.; et al. Estimating GFR using Serum Cystatin C Alone and in Combination with Serum Creatinine: A Pooled Analysis of 3418 Individuals with CKD. Am. J. Kidney Dis. 2008, 51, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- KDIGO. 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Int. Soc. Nephrol. 2013, 3. [Google Scholar]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Chronic Kidney Disease Epidemiology Collaboration Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Jones, I.; Nyman, U.; Sjöström, P. Validation of the Lund–Malmö, Chronic Kidney Disease Epidemiology (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) equations to estimate glomerular filtration rate in a large Swedish clinical population. Scand. J. Urol. Nephrol. 2012, 46, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Schaeffner, E.S.; Ebert, N.; Delanaye, P.; Frei, U.; Gaedeke, J.; Jakob, O.; Kuhlmann, M.K.; Schuchardt, M.; Tölle, M.; Ziebig, R.; et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann. Intern. Med. 2012, 157, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Dowling, T.C.; Wang, E.-S.; Ferrucci, L.; Sorkin, J.D. Glomerular filtration rate equations overestimate creatinine clearance in older individuals enrolled in the Baltimore Longitudinal Study on Aging: Impact on renal drug dosing. Pharmacotherapy 2013, 33, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Péquignot, R.; Belmin, J.; Chauvelier, S.; Gaubert, J.-Y.; Konrat, C.; Duron, E.; Hanon, O. Renal function in older hospital patients is more accurately estimated using the Cockcroft-Gault formula than the modification diet in renal disease formula. J. Am. Geriatr. Soc. 2009, 57, 1638–1643. [Google Scholar] [CrossRef] [PubMed]
- Michels, W.M.; Grootendorst, D.C.; Verduijn, M.; Elliott, E.G.; Dekker, F.W.; Krediet, R.T. Performance of the Cockcroft-Gault, MDRD, and New CKD-EPI Formulas in Relation to GFR, Age, and Body Size. Clin. J. Am. Soc. Nephrol. 2010, 5, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Pottel, H.; Hoste, L.; Dubourg, L.; Ebert, N.; Schaeffner, E.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; et al. An estimated glomerular filtration rate equation for the full age spectrum. Nephrol. Dial. Transplant. 2016, 31, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Grubb, A.; Sterner, G.; Nyman, U. Revised equations for estimating glomerular filtration rate based on the Lund-Malmö Study cohort. Scand. J. Clin. Lab. Investig. 2011, 71, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Werner, K.; Pihlsgård, M.; Elmståhl, S.; Legrand, H.; Nyman, U.; Christensson, A. Combining Cystatin C and Creatinine Yields a Reliable Glomerular Filtration Rate Estimation in Older Adults in Contrast to β-Trace Protein and β2-Microglobulin. Nephron 2017, 137, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Grubb, A.; Gudnason, V.; Indridason, O.S.; Levey, A.S.; Palsson, R.; Nyman, U. Comparison of glomerular filtration rate estimating equations derived from creatinine and cystatin C: Validation in the Age, Gene/Environment Susceptibility-Reykjavik elderly cohort. Nephrol. Dial. Transplant. 2017, 33, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Fan, L. Comparing GFR estimating equations using cystatin C and creatinine in elderly individuals. J. Am. Soc. Nephrol. 2015, 26, 1982–1989. [Google Scholar] [CrossRef] [PubMed]
- Heldal, K.; Midtvedt, K.; Hartmann, A.; Reisæter, A.V.; Heldal, T.F.; Bergan, S.; Salvador, C.L.; Åsberg, A. Estimated glomerular filtration rate in stable older kidney transplant recipients—Are present algorithms valid? A national cross-sectional cohort study. Transplant Int. 2018, 31, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Raman, M.; Middleton, R.J.; Kalra, P.A.; Green, D. Estimating renal function in old people: An in-depth review. Int. Urol. Nephrol. 2017, 49, 1979–1988. [Google Scholar] [CrossRef] [PubMed]
- Oscanoa, T.J.; Amado, J.P.; Romero-Ortuno, R.; Hidalgo, J.A. Estimation of the glomerular filtration rate in older individuals with serum creatinine-based equations: A systematic comparison between CKD-EPI and BIS1. Arch. Gerontol. Geriatr. 2018, 75, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Levey, A.S.; Coresh, J. Estimated Glomerular Filtration Rate From a Panel of Filtration Markers-Hope for Increased Accuracy Beyond Measured Glomerular Filtration Rate? Adv. Chronic Kidney Dis. 2018, 25, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Hornum, M.; Feldt-Rasmussen, B. Drug Dosing and Estimated Renal Function—Any Step Forward from Effersoe? Nephron 2017, 136, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Segarra, A.; de la Torre, J.; Ramos, N.; Quiroz, A.; Garjau, M.; Torres, I.; Azancot, M.A.; López, M.; Sobrado, A. Assessing glomerular filtration rate in hospitalized patients: A comparison between CKD-EPI and four cystatin C-based equations. Clin. J. Am. Soc. Nephrol. 2011, 6, 2411–2420. [Google Scholar] [CrossRef] [PubMed]
- Helldén, A.; Bergman, U.; von Euler, M.; Hentschke, M.; Odar-Cederlöf, I.; Ohlén, G. Adverse drug reactions and impaired renal function in elderly patients admitted to the emergency department: A retrospective study. Drugs Aging 2009, 26, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Gheewala, P.A.; Peterson, G.M.; Curtain, C.M.; Nishtala, P.S.; Hannan, P.J.; Castelino, R.L. Impact of the pharmacist medication review services on drug-related problems and potentially inappropriate prescribing of renally cleared medications in residents of aged care facilities. Drugs Aging 2014, 31, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Sönnerstam, E.; Sjölander, M.; Gustafsson, M. Inappropriate Prescription and Renal Function Among Older Patients with Cognitive Impairment. Drugs Aging 2016, 33, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.L.; Henriksen, D.P.; Marinakis, C.; Hellebek, A.; Birn, H.; Nybo, M.; Søndergaard, J.; Nymark, A.; Pedersen, C. Drug dosing in patients with renal insufficiency in a hospital setting using electronic prescribing and automated reporting of estimated glomerular filtration rate. Basic Clin. Pharmacol. Toxicol. 2014, 114, 407–413. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, P.K.; Mathur, R.; Hull, S.A.; Saja, K.; Green, L.; Morris, J.K.; Ashman, N. Patient safety and estimation of renal function in patients prescribed new oral anticoagulants for stroke prevention in atrial fibrillation: A cross-sectional study. BMJ Open 2013, 3, e003343. [Google Scholar] [CrossRef] [PubMed]
- Helldén, A.; Odar-Cederlöf, I.; Nilsson, G.; Sjöviker, S.; Söderström, A.; von Euler, M.; Öhlén, G.; Bergman, U. Renal function estimations and dose recommendations for dabigatran, gabapentin and valaciclovir: A data simulation study focused on the elderly. BMJ Open 2013, 3, e002686. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.G.; Hawkins, N.M.; Fordyce, C.B.; Deyell, M.W.; Er, L.; Djurdjev, O.; Macle, L.; Virani, S.A.; Levin, A. Variability in Non-Vitamin K Antagonist Oral Anticoagulants Dose Adjustment in Atrial Fibrillation Patients With Renal Dysfunction: The Influence of Renal Function Estimation Formulae. Can. J. Cardiol. 2018, 34, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, T.N.; Klepstad, P.; Davies, A.; Bjordal, K.; Lundström, S.; Kaasa, S.; Dale, O. Influences on the pharmacokinetics of oxycodone: A multicentre cross-sectional study in 439 adult cancer patients. Eur. J. Clin. Pharmacol. 2011, 67, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Pöyhiä, R.; Seppälä, T.; Olkkola, K.T.; Kalso, E. The pharmacokinetics and metabolism of oxycodone after intramuscular and oral administration to healthy subjects. Br. J. Clin. Pharmacol. 1992, 33, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Kummer, O.; Hammann, F.; Moser, C.; Schaller, O.; Drewe, J.; Krähenbühl, S. Effect of the inhibition of CYP3A4 or CYP2D6 on the pharmacokinetics and pharmacodynamics of oxycodone. Eur. J. Clin. Pharmacol. 2011, 67, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.S. Opioid Metabolism. Mayo Clin. Proc. 2009, 84, 613–624. [Google Scholar] [CrossRef]
- Davis, M.P.; Homsi, J. The importance of cytochrome P450 monooxygenase CYP2D6 in palliative medicine. Support. Care Cancer 2001, 9, 442–451. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2014, 44, 213–218. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Guidance for Industry: Pharmacokinetics in Patients with Impaired Renal Function—Study Design, Data Analysis and Impact on Dosing and Labeling, Revision 1; US Food and Drug Administration: Silver Spring, MD, USA, 2010. Available online: https://www.fda.gov/downloads/drugs/guidances/ucm204959.pdf (accessed on 12 September 2018).
- European Medicines Agency. Guideline on the Evaluation of the Pharmacokinetics of Medicinal Products in Patients with Decreased Renal Function; European Medicines Agency: London, UK, 2014; Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2016/02/WC500200841.pdf (accessed on 12 September 2018).
- KDIGO. Clinical Practice Guideline for Acute Kidney Injury. Int. Soc. Nephrol. 2012, 2, 8. [Google Scholar]
- The Danish Council on Ethics Research with Health Data and Biological Material in Denmark Statement. Available online: http://www.etiskraad.dk/~/media/Etisk-Raad/en/Publications/Research-with-health-data-and-biological-material-in-Denmark-Statement-2015.pdf?la=da (accessed on 12 September 2018).
- Du Bois, D.; Du Bois, E.F. A formula to estimate the approximate surface area if height and weight be known, 1916. Nutrition 1989, 5, 303–311. [Google Scholar] [PubMed]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National Kidney Foundation National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Medbase, Ltd. Renbase—Drug Dosing in Renal Failure; Medbase, Ltd.: Turku, Finland, 2018. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Value |
|---|---|
| Female sex, n (%) | 80 (67.8) |
| Age (years) | 82.6 (70.1–100.8) |
| Actual body weight (kg) | 63.0 (32.0–98.0) |
| Height (cm) | 167 (144–191) |
| Body Mass Index (kg/m2) | 22.4 (14.2–33.3) |
| Body Mass Index (kg/m2) ≤ 18.5, n (%) | 14 (11.9) |
| Body Mass Index (kg/m2) > 30.0, n (%) | 3 (2.50) |
| Body surface area (m2) | 1.71 (1.19–2.19) |
| Body surface area > 1.9 m2, n (%) | 25 (21.2) |
| Body surface area < 1.6 m2, n (%) | 40 (33.9) |
| Serum creatinine (µmol/L) | 71.0 (25.0–430) |
| Comorbidities and medication | |
| Hypertension, n (%) | 56 (47.5) |
| Osteoporosis, n (%) | 34 (28.8) |
| Dementia, n (%) | 21 (17.8) |
| Ischemic heart disease, n (%) | 19 (16.1) |
| Diabetes, n (%) | 18 (15.2) |
| Number of medication at admission | 6 (0–21) |
| Source of Equation | eGFR (Mean ± SD) | Estimated Difference in eGFR | 95% Cl | p-Value |
|---|---|---|---|---|
| CKD-EPI | 67.3 ± 22.3 | - | - | - |
| BIS | 59.1 ± 21.3 | −8.2 | −10.0–−6.4 | <0.0001 |
| CG | 56.9 ± 25.7 | −10.4 | −12.2–−8.6 | <0.0001 |
| FAS | 60.3 ± 24.6 | −7.0 | −8.8–−5.2 | <0.0001 |
| LMR | 58.9 ± 20.1 | −8.4 | −10.2–−6.6 | <0.0001 |
| MDRD | 79.1 ± 33.6 | +11.8 | 10.0–13.6 | <0.0001 |
| Source of Equation | CKD I eGFR ≥ 90 | CKD II eGFR 60–89 | CKD III eGFR 30–59 | CKD IV eGFR 15–29 | CKD V eGFR < 15 |
|---|---|---|---|---|---|
| CKD-EPI | 15 (12.7) | 64 (54.2) | 31 (26.3) | 6 (5.1) | 2 (1.7) |
| BIS | 7 (5.9) | 46 (39.0) | 58 (49.2) | 5 (4.2) | 2 (1.7) |
| CG | 6 (5.1) | 42 (35.6) | 56 (47.4) | 12 (10.2) | 2 (1.7) |
| FAS | 10 (8.5) | 43 (36.4) | 54 (45.8) | 9 (7.6) | 2 (1.7) |
| LMR | 4 (3.4) | 55 (46.6) | 47 (39.8) | 10 (8.5) | 2 (1.7) |
| MDRD | 41 (34.8) | 45 (38.1) | 25 (21.2) | 5 (4.2) | 2 (1.7) |
| BIS | CG | FAS | LMR | MDRD | |
|---|---|---|---|---|---|
| CKD-EPI | 0.65 (0.54–0.76) (83; 70.4%) | 0.57 (0.46–0.68) (75; 63.6%) | 0.68 (0.57–0.78) (84; 71.2%) | 0.65 (0.54–0.75) (83; 70.4%) | 0.70 (0.60–0.79) (84; 71.2%) |
| BIS | 0.78 (0.68–0.87) (97; 76.2%) | 0.93 (0.87–0.98) (111; 94.0%) | 0.85 (0.77–0.92) (104; 88.1%) | 0.45 (0.34–0.56) (59; 50.0%) | |
| CG | 0.82 (0.74–0.90) (100; 84.7%) | 0.80 (0.71–0.89) (100; 84.7%) | 0.38 (0.28–0.49) (60; 50.8%) | ||
| FAS | 0.87 (0.80–0.94) (105; 89.0%) | 0.46 (0.36–0.56) (50; 42.4%) | |||
| LMR | 0.44 (0.34–0.54) (49; 41.5%) |
| BIS | CG | FAS | LMR | MDRD | |
|---|---|---|---|---|---|
| CKD-EPI | 91 (26/1) 83 (34/1) | 81 (37/0) 72 (46/0) | 89 (29/0) 84 (34/0) | 94 (24/0) 83 (35/0) | 110 (0/8) 84 (0/34) |
| BIS | 100 (15/3) 97 (17/4) | 114 (4/0) 111 (4/3) | 107 (5/6) 104 (6/8) | 85 (0/33) 51 (0/67) | |
| CG | 104 (3/11) 100 (3/15) | 101 (2/15) 99 (4/15) | 73 (0/45) 41 (0/77) | ||
| FAS | 111 (1/6) 105 (7/6) | 81 (0/37) 50 (0/68) | |||
| LMR | 86 (0/32) 49 (0/69) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Houlind, M.B.; Petersen, K.K.; Palm, H.; Jørgensen, L.M.; Aakjær, M.; Christrup, L.L.; Petersen, J.; Andersen, O.; Treldal, C. Creatinine-Based Renal Function Estimates and Dosage of Postoperative Pain Management for Elderly Acute Hip Fracture Patients. Pharmaceuticals 2018, 11, 88. https://doi.org/10.3390/ph11030088
Houlind MB, Petersen KK, Palm H, Jørgensen LM, Aakjær M, Christrup LL, Petersen J, Andersen O, Treldal C. Creatinine-Based Renal Function Estimates and Dosage of Postoperative Pain Management for Elderly Acute Hip Fracture Patients. Pharmaceuticals. 2018; 11(3):88. https://doi.org/10.3390/ph11030088
Chicago/Turabian StyleHoulind, Morten Baltzer, Kristian Kjær Petersen, Henrik Palm, Lillian Mørch Jørgensen, Mia Aakjær, Lona Louring Christrup, Janne Petersen, Ove Andersen, and Charlotte Treldal. 2018. "Creatinine-Based Renal Function Estimates and Dosage of Postoperative Pain Management for Elderly Acute Hip Fracture Patients" Pharmaceuticals 11, no. 3: 88. https://doi.org/10.3390/ph11030088
APA StyleHoulind, M. B., Petersen, K. K., Palm, H., Jørgensen, L. M., Aakjær, M., Christrup, L. L., Petersen, J., Andersen, O., & Treldal, C. (2018). Creatinine-Based Renal Function Estimates and Dosage of Postoperative Pain Management for Elderly Acute Hip Fracture Patients. Pharmaceuticals, 11(3), 88. https://doi.org/10.3390/ph11030088