

Daily Variability in Sedentary Behaviour and Physical Activity Responsiveness in Older Women


Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Physical Behaviour Interventions
2.3. Physical Behaviour Assessment
2.4. Physical Behaviour Classification
2.5. Inter-Day Variability Assessment
2.6. Threshold Determination
2.7. Statistical Analyses
- (1)
- Changes in the inter-day variability (CV% and individualized variance) in each physical behaviour across time (from baseline to week 8), and the effect of the intervention group (SBF, LIPA, or control). Baseline (raw data and variability) group differences were examined with a one-way analysis of variance (ANOVA) or a Kruskal–Wallis ANOVA (where data were non-normal) given the 3-group design, with post hoc pairwise unpaired student t-test comparisons conducted using the Bonferroni adjustment the or Mann–Whitney U test (for the Kruskal–Wallis ANOVA), respectively. The effects of the interventions were determined using a 2 × 3 split-plot ANOVA [given the study design of 2 time phases (pre- and post-intervention) and 3 intervention groups (SBF, LIPA, and control)] with Bonferroni-corrected post hoc comparisons. In cases of non-normally distributed data, first, within-group comparisons were made using the Wilcoxon signed-rank test, and then between-group pairwise differences were analyzed through a Kruskal–Wallis ANOVA of the relative changes from the baseline [(post-pre)/pre-], with post hoc pairwise comparisons examined by the Mann–Whitney U test. In cases where groups were unmatched at baseline (i.e., significantly different), the baseline values were accounted for in the statistical analysis model as a covariate (ANCOVA analysis).
- (2)
- The link between the change in a given physical behaviour metric (e.g., absolute SB time), and its baseline inter-day variability. Here, participants were classified as either high- or low-regularity, and the change (from baseline to week 8) in their absolute physical behaviour outcomes was quantified. The complete set of all baseline classifications can be seen in Table 1. When analysing the PB change by baseline regularity classification, all participants were grouped together regardless of experimental condition (SBF, LIPA, and control). A chi-squared test was used to compare the distribution of inter-day variability classifications (high vs. low regularity) between experimental groups (SBF, LIPA, and CON), sedentary classification groups (ambulatory and couch potato), and activity classification groups (active and inactive) at baseline. These classifications were applied within each group and/or across all participants to ensure balanced comparisons and avoid bias. For a chi-squared test to be appropriate, the expected frequency count for each cell should generally be at least 5. We ensured this assumption was met by verifying that the number of participants in each classification category (e.g., high vs. low regularity) was sufficient for comparison. Specifically, all high-regularity groups had n = 8, meaning comparisons were made against a frequency of n ≥ 8.
3. Results
3.1. Baseline Differences
3.2. Intervention Outcomes Pertaining to PA Amount
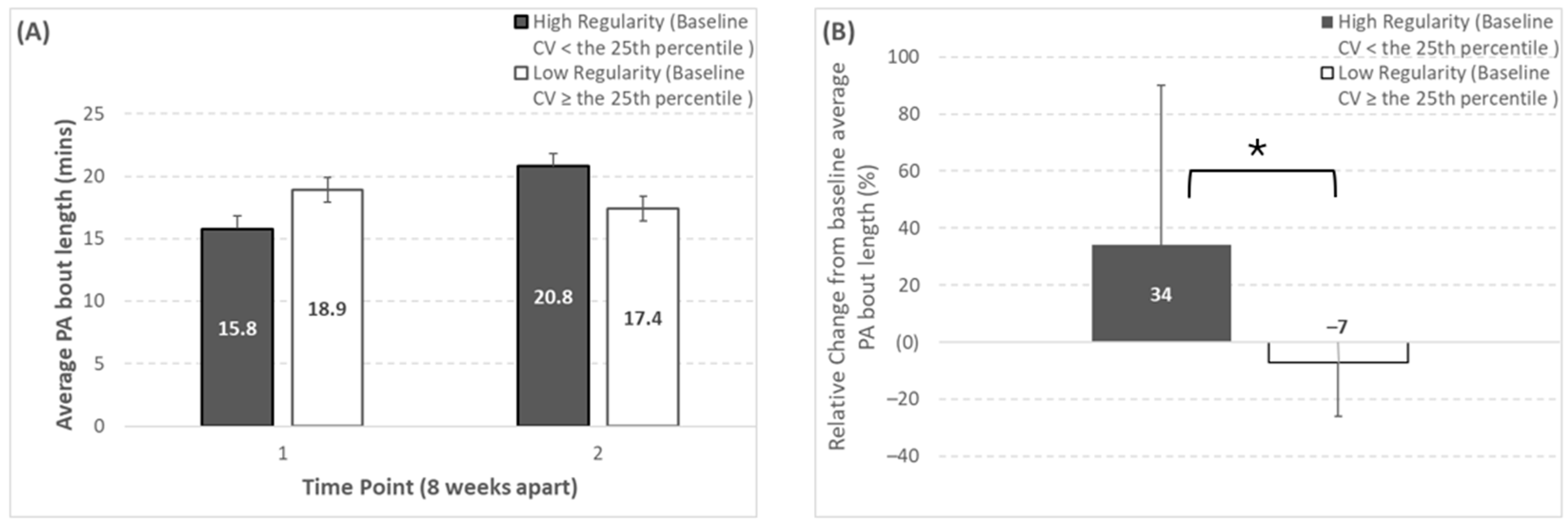
3.3. Intervention Outcomes Pertaining to PA Pattern
3.4. Intervention Outcomes Pertaining to SB Amount
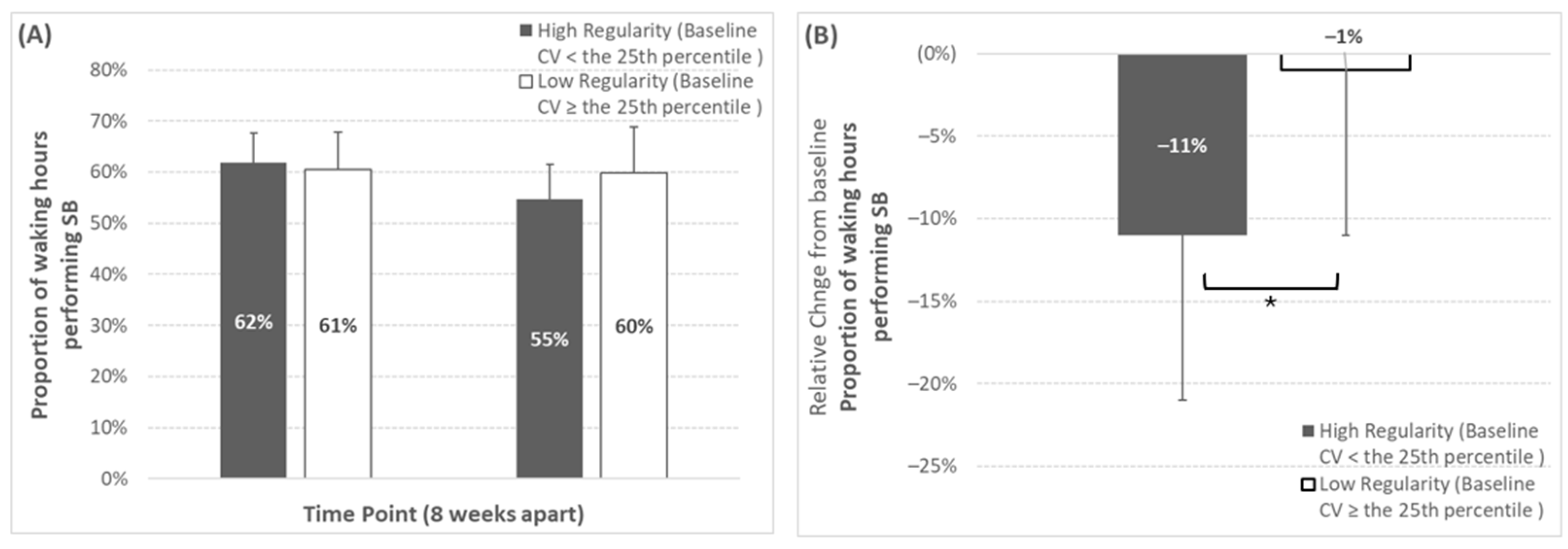
3.5. Intervention Results Pertaining to SB Pattern
4. Discussion
4.1. Study Strengths and Limitations
4.2. Recommendations for Future Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [PubMed]
- Stamatakis, E.; Ekelund, U.; Ding, D.; Hamer, M.; Bauman, A.E.; Lee, I.M. Is the time right for quantitative public health guidelines on sitting? A narrative review of sedentary behaviour research paradigms and findings. Br. J. Sports Med. 2019, 53, 377–382. [Google Scholar] [PubMed]
- Silveira, E.A.; Mendonça, C.R.; Delpino, F.M.; Souza, G.V.E.; de Souza Rosa, L.P.; de Oliveira, C.; Noll, M. Sedentary behavior, physical inactivity, abdominal obesity and obesity in adults and older adults: A systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 50, 63–73. [Google Scholar] [CrossRef]
- Reid, N.; Healy, G.N.; Gianoudis, J.; Formica, M.; Gardiner, P.A.; Eakin, E.E.; Nowson, C.A.; Daly, R.M. Association of sitting time and breaks in sitting with muscle mass, strength, function, and inflammation in community-dwelling older adults. Osteoporos. Int. 2018, 29, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- de Rezende, L.F.M.; Rey-López, J.P.; Matsudo, V.K.R.; Luiz, O.D.C. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health 2014, 14, 333. [Google Scholar] [CrossRef]
- da Silva, V.D.; Tribess, S.; Meneguci, J.; Sasaki, J.E.; Garcia-Meneguci, C.A.; Carneiro, J.A.O.; Virtuoso, J.S. Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health 2019, 19, 709. [Google Scholar]
- Maasakkers, C.M.; Claassen, J.A.; Gardiner, P.A.; Olde Rikkert, M.G.; Lipnicki, D.M.; Scarmeas, N.; Dardiotis, E.; Yannakoulia, M.; Anstey, K.J.; Cherbuin, N.; et al. The Association of Sedentary Behaviour and Cognitive Function in People Without Dementia: A Coordinated Analysis Across Five Cohort Studies from COSMIC. Sports Med. 2020, 50, 403–413. [Google Scholar] [PubMed]
- Moreira, P.D.; Matos, S.M.A.D.; Pitanga, F.J.G.; Giatti, L.; Barreto, S.M.; Harter Griep, R.; Santos, C.A.D.S.T. Association between Sedentary Behavior and Cognitive Performance in Middle-Aged and Elderly Adults: Cross-Sectional Results from ELSA-Brasil. Int. J. Environ. Res. Public Health 2022, 19, 14234. [Google Scholar] [CrossRef]
- Matthews, C.E.; George, S.M.; Moore, S.C.; Bowles, H.R.; Park, Y.; Blair, A.; Troiano, R.P.; Hollenbeck, A.; Schatzkin, A. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. Am. J. Clin. Nutr. 2012, 95, 437–445. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar]
- Stamatakis, E.; Rogers, K.; Ding, D.; Berrigan, D.; Chau, J.; Hamer, M.; Bauman, A. All-cause mortality effects of replacing sedentary time with physical activity and sleeping using an isotemporal substitution model: A prospective study of 201,129 mid-aged and older adults. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 121. [Google Scholar]
- Mansoubi, M.; Pearson, N.; Biddle, S.J.; Clemes, S. The relationship between sedentary behaviour and physical activity in adults: A systematic review. Prev. Med. 2014, 69, 28–35. [Google Scholar] [PubMed]
- Jefferis, B.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Whincup, P.H. Validity of questionnaire-based assessment of sedentary behaviour and physical activity in a population-based cohort of older men; comparisons with objectively measured physical activity data. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 14. [Google Scholar] [PubMed]
- Fuezeki, E.; Engeroff, T.; Banzer, W. Health benefits of light-intensity physical activity: A systematic review of accelerometer data of the National Health and Nutrition Examination Survey (NHANES). Sports Med. 2017, 47, 1769–1793. [Google Scholar]
- Chastin, S.F.; De Craemer, M.; De Cocker, K.; Powell, L.; Van Cauwenberg, J.; Dall, P.; Hamer, M.; Stamatakis, E. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br. J. Sports Med. 2019, 53, 370–376. [Google Scholar] [CrossRef]
- Gennuso, K.P.; Thraen-Borowski, K.M.; Gangnon, R.E.; Colbert, L.H. Patterns of sedentary behavior and physical function in older adults. Aging Clin. Exp. Res. 2016, 28, 943–950. [Google Scholar] [CrossRef]
- Diaz, K.M.; Howard, V.J.; Hutto, B.; Colabianchi, N.; Vena, J.E.; Safford, M.M.; Blair, S.N.; Hooker, S.P. Patterns of sedentary behavior and mortality in US middle-aged and older adults: A national cohort study. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar]
- Dempsey, P.C.; Strain, T.; Winkler, E.A.; Westgate, K.; Rennie, K.L.; Wareham, N.J.; Brage, S.; Wijndaele, K. Association of Accelerometer-Measured Sedentary Accumulation Patterns With Incident Cardiovascular Disease, Cancer, and All-Cause Mortality. J. Am. Heart Assoc. 2022, 11, e023845. [Google Scholar]
- El Fatouhi, D.; Delrieu, L.; Goetzinger, C.; Malisoux, L.; Affret, A.; Campo, D.; Fagherazzi, G. Associations of physical activity level and variability with 6-month weight change among 26,935 users of connected devices: Observational real-life study. JMIR mHealth uHealth 2021, 9, e25385. [Google Scholar]
- Hunter, R.F.; Tully, M.A.; Donnelly, P.; Stevenson, M.; Kee, F. Knowledge of UK physical activity guidelines: Implications for better targeted health promotion. Prev. Med. 2014, 65, 33–39. [Google Scholar] [PubMed]
- Nobles, J.; Thomas, C.; Banks Gross, Z.; Hamilton, M.; Trinder-Widdess, Z.; Speed, C.; Gibson, A.; Davies, R.; Farr, M.; Jago, R.; et al. “Let’s talk about physical activity”: Understanding the preferences of under-served communities when messaging physical activity guidelines to the public. Int. J. Environ. Res. Public Health 2020, 17, 2782. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.H.; Lahart, I.; Carlin, A.; Murtagh, E. The effects of continuous compared to accumulated exercise on health: A meta-analytic review. Sports Med. 2019, 49, 1585–1607. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Kraus, W.E.; Powell, K.E.; Campbell, W.W.; Janz, K.F.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L.; 2018 Physical Activity Guidelines Advisory Committee. Association between bout duration of physical activity and health: Systematic review. Med. Sci. Sports Exerc. 2019, 51, 1213. [Google Scholar]
- Clemente, F.M.; Owen, A.; Serra-Olivares, J.; Nikolaidis, P.T.; Van Der Linden, C.M.; Mendes, B. Characterization of the weekly external load profile of professional soccer teams from portugal and the Netherlands. J. Hum. Kinet. 2019, 66, 155. [Google Scholar] [CrossRef]
- Matos, S.; Clemente, F.M.; Brandão, A.; Pereira, J.; Rosemann, T.; Nikolaidis, P.T.; Knechtle, B. Training Load, Aerobic Capacity and Their Relationship With Wellness Status in Recreational Trail Runners. Front. Physiol. 2019, 10, 1189. [Google Scholar] [CrossRef]
- Silva, D.; Vázquez, J.O.S.É.; Ramos, J.O.Ã.O.; Clemente, F.M.; Camões, M.I.G.U.E.L.; Lima, R.F. Intra-week variations and associations between internal and external load measures in a elite volleyball team. J. Hum. Sport Exerc. 2019, 14, 1286–1289. [Google Scholar]
- Schwendinger, F.; Wagner, J.; Infanger, D.; Schmidt-Trucksäss, A.; Knaier, R. Methodological aspects for accelerometer-based assessment of physical activity in heart failure and health. BMC Med. Res. Methodol. 2021, 21, 251. [Google Scholar]
- Abel, B.; Pomiersky, R.; Werner, C.; Lacroix, A.; Schaeufele, M.; Hauer, K. Day-to-day variability of multiple sensor-based physical activity parameters in older persons with dementia. Arch. Gerontol. Geriatr. 2019, 85, 103911. [Google Scholar]
- Tono-oka, T.; Kaneko, I. The estimation of daily physical activity with the coefficient of variation (cv) of heart rates continuously recorded. Hokkaido Igaku Zasshi Hokkaido J. Med. Sci. 1993, 68, 431–434. [Google Scholar]
- O’Conor, R.; Benavente, J.Y.; Kwasny, M.J.; Eldeirawi, K.; Hasnain-Wynia, R.; Federman, A.D.; Hebert-Beirne, J.; Wolf, M.S. Daily routine: Associations with health status and urgent health care utilization among older adults. Gerontologist 2019, 59, 947–955. [Google Scholar] [CrossRef]
- Loyen, A.; Clarke-Cornwell, A.M.; Anderssen, S.A.; Hagströmer, M.; Sardinha, L.B.; Sundquist, K.; Ekelund, U.; Steene-Johannessen, J.; Baptista, F.; Hansen, B.H.; et al. Sedentary time and physical activity surveillance through accelerometer pooling in four European countries. Sports Med. 2017, 47, 1421–1435. [Google Scholar] [CrossRef] [PubMed]
- Wickel, E.E.; Eisenmann, J.C. Within-and between-individual variability in estimated energy expenditure and habitual physical activity among young adults. Eur. J. Clin. Nutr. 2006, 60, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Ridley, K.; Olds, T.; Hands, B.; Larkin, D.; Parker, H. Intra-individual variation in children’s physical activity patterns: Implications for measurement. J. Sci. Med. Sport 2009, 12, 568–572. [Google Scholar] [CrossRef]
- Compernolle, S.; DeSmet, A.; Poppe, L.; Crombez, G.; De Bourdeaudhuij, I.; Cardon, G.; Van Der Ploeg, H.P.; Van Dyck, D. Effectiveness of interventions using self-monitoring to reduce sedentary behavior in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 63. [Google Scholar] [CrossRef]
- Ryan, D.J.; Wullems, J.A.; Stebbings, G.K.; Morse, C.I.; Stewart, C.E.; Onambele-Pearson, G.L. Reliability and validity of the international physical activity questionnaire compared to calibrated accelerometer cut-off points in the quantification of sedentary behaviour and physical activity in older adults. PLoS ONE 2018, 13, e0195712. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1· 9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Barone Gibbs, B.; Brach, J.S.; Byard, T.; Creasy, S.; Davis, K.K.; McCoy, S.; Peluso, A.; Rogers, R.J.; Rupp, K.; Jakicic, J.M. Reducing Sedentary Behavior Versus Increasing Moderate-to-Vigorous Intensity Physical Activity in Older Adults. J. Aging Health 2017, 29, 247–267. [Google Scholar] [CrossRef]
- Harvey, J.A.; Chastin, S.F.M.; Skelton, D.A. Breaking sedentary behaviour has the potential to increase / maintain function in frail older adults. J. Frailty Sarcopenia Falls 2018, 3, 26–34. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Gell, N.M.; Jones, S.M.; Renz, A.; Kerr, J.; Gardiner, P.A.; Arterburn, D. The feasibility of reducing sitting time in overweight and obese older adults. Health Educ. Behav. 2015, 42, 669–676. [Google Scholar] [CrossRef]
- Holm, S. Declaration of helsinki. In The International Encyclopedia of Ethics; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Grant, D.; Tomlinson, D.; Tsintzas, K.; Kolic, P.; Onambele-Pearson, G. Displacing Sedentary Behaviour with Light Intensity Physical Activity Spontaneously Alters Habitual Macronutrient Intake and Enhances Dietary Quality in Older Females. Nutrients 2020, 12, 2431. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Han, H.; Aguiar, E.J.; Barreira, T.V.; Schuna, J.M., Jr.; Kang, M.; Rowe, D.A. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: A narrative review. Br. J. Sports Med. 2018, 52, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Esliger, D.W.; Rowlands, A.V.; Hurst, T.L.; Catt, M.; Murray, P.; Eston, R.G. Validation of the GENEA Accelerometer. Med. Sci. Sports Exerc. 2011, 43, 1085–1093. [Google Scholar]
- Rowlands, A.V.; Olds, T.S.; Hillsdon, M.; Pulsford, R.; Hurst, T.L.; Eston, R.G.; Gomersall, S.R.; Johnston, K.; Langford, J. Assessing sedentary behavior with the GENEActiv: Introducing the sedentary sphere. Med. Sci. Sports Exerc. 2014, 46, 1235–1247. [Google Scholar]
- Pavey, T.G.; Gomersall, S.R.; Clark, B.K.; Brown, W.J. The validity of the GENEActiv wrist-worn accelerometer for measuring adult sedentary time in free living. J. Sci. Med. Sport 2016, 19, 395–399. [Google Scholar] [PubMed]
- Wullems, J.A.; Verschueren, S.M.; Degens, H.; Morse, C.I.; Onambele, G.L. Performance of thigh-mounted triaxial accelerometer algorithms in objective quantification of sedentary behaviour and physical activity in older adults. PLoS ONE 2017, 12, e0188215. [Google Scholar]
- Wullems, J.A.; Verschueren, S.M.; Degens, H.; Morse, C.I.; Onambélé-Pearson, G.L. Concurrent Validity of Four Activity Monitors in Older Adults. Sensors 2024, 24, 895. [Google Scholar] [CrossRef]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.G. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar]
- Ayabe, M.; Kumahara, H.; Morimura, K.; Tanaka, H. Epoch length and the physical activity bout analysis: An accelerometry research issue. BMC Res. Notes 2013, 6, 20. [Google Scholar]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J. Methods of measurement in epidemiology: Sedentary behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar]
- Baumann, S.; Groß, S.; Voigt, L.; Ullrich, A.; Weymar, F.; Schwaneberg, T.; Dörr, M.; Meyer, C.; John, U.; Ulbricht, S. Pitfalls in accelerometer-based measurement of physical activity: The presence of reactivity in an adult population. Scand. J. Med. Sci. Sports 2018, 28, 1056–1063. [Google Scholar] [CrossRef]
- Sasaki, J.E.; Júnior, J.H.; Meneguci, J.; Tribess, S.; Marocolo Júnior, M.; Stabelini Neto, A.; Virtuoso Júnior, J.S. Number of days required for reliably estimating physical activity and sedentary behaviour from accelerometer data in older adults. J. Sports Sci. 2018, 36, 1572–1577. [Google Scholar] [PubMed]
- Chastin, S.F.; Winkler, E.A.; Eakin, E.G.; Gardiner, P.A.; Dunstan, D.W.; Owen, N.; Healy, G.N. Sensitivity to change of objectively-derived measures of sedentary behavior. Meas. Phys. Educ. Exerc. Sci. 2015, 19, 138–147. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Thiese, M.S.; Ronna, B.; Ott, U. P value interpretations and considerations. J. Thorac. Dis. 2016, 8, E928. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; Dontje, M.L.; Skelton, D.A.; Čukić, I.; Shaw, R.J.; Gill, J.M.R.; Greig, C.A.; Gale, C.R.; Deary, I.J.; Der, G.; et al. Systematic comparative validation of self-report measures of sedentary time against an objective measure of postural sitting (activPAL). Int. J. Behav. Nutr. Phys. Act. 2018, 15, 21. [Google Scholar]
- Strath, S.J.; Holleman, R.G.; Richardson, C.R.; Ronis, D.L.; Swartz, A.M. Objective physical activity accumulation in bouts and nonbouts and relation to markers of obesity in US adults. Prev. Chronic Dis. 2008, 5, A131. [Google Scholar] [PubMed]
- Hall, K.S.; Howe, C.A.; Rana, S.R.; Martin, C.L.; Morey, M.C. METs and accelerometry of walking in older adults: Standard versus measured energy cost. Med. Sci. Sports Exerc. 2013, 45, 574. [Google Scholar]
- Grant, D.; Tomlinson, D.; Tsintzas, K.; Kolić, P.; Onambele-Pearson, G.L. The Effects of Displacing Sedentary Behavior With Two Distinct Patterns of Light Activity on Health Outcomes in Older Adults (Implications for COVID-19 Quarantine). Front. Physiol. 2020, 11, 574595. [Google Scholar]
- Brawner, C.A.; Churilla, J.R.; Keteyian, S.J. Prevalence of physical activity is lower among individuals with chronic disease. Med. Sci. Sports Exerc. 2016, 48, 1062–1067. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Schlaff, R.A.; Baruth, M.; Boggs, A.; Hutto, B. Patterns of sedentary behavior in older adults. Am. J. Health Behav. 2017, 41, 411–418. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Physical Behaviour Category | Average Baseline Absolute PB Outcome | Average Baseline Inter-Day Variability Expressed as Coefficient of Variation (%) | Low Regularity Threshold Value (≥25th Percentile Value) | Average Baseline Inter-Day Variability Expressed as Individualized Variance |
|---|---|---|---|---|
| PA amounts | ||||
| Standing Time (hours) | 1.3 ± 0.5 | 28 ± 8% | ≥23% | 0.1 ± 0.1 |
| Light-intensity physical activity time (hours) | 2.1 ± 0.4 | 21 ± 10% | ≥17% | 0.2 ± 0.2 |
| Moderate-to-vigorous physical activity time (hours) | 2.7 ± 0.8 | 20 ± 6% | ≥17% | 0.2 ± 0.3 |
| MVPA in bouts ≥ 10 min duration (minutes) | 8.5 ± 11.9 | 139 ± 145% | ≥55% | 139.3 ± 184.6 |
| MVPA in bouts of <10 min duration (minutes) | 150 ± 44 | 21 ± 8% | ≥18% | 658 ± 870 |
| Daily sum of PA bout time (minutes) | 361 ± 73 | 19 ± 7% | ≥15% | 3400 ± 3333 |
| PA patterns | ||||
| Bouts of PA (number) | 21 ± 5 | 18 ± 10% | ≥15% | 13 ± 10 |
| Average Daily PA bout length (minutes) | 18.1 ± 4.2 | 25 ± 17% | ≥17% | 16 ± 38 |
| SB amounts | ||||
| Sedentary Behaviour Time (hours) | 9.5 ± 1.1 | 12 ± 8% | ≥9% | 1.2 ± 1.4 |
| Sedentary Behaviour Time (% of waking hours) | 60.8 ± 7.0 | 11 ± 5% | ≥8% | 38.2 ± 30.8 |
| SB patterns | ||||
| SB in bouts of <5 min (number) | 6 ± 2 | 43 ± 20% | ≥14% | 5 ± 5 |
| Average Daily Sedentary Behaviour Bout Length (Minutes) | 32.9 ± 9.2 | 27 ± 17% | ≥20% | 70.7 ± 158.2 |
| SBF (n = 12) | LIPA (n = 13) | Control (n = 6) | ANOVA (or * Kruskal–Wallis) | |
|---|---|---|---|---|
| Age (y) | 74 ± 5 | 73 ± 5 | 70 ± 3 (67, 73) | p = n.s. |
| Weight (kg) | 68.6 ± 11.3 | 65.5 ± 8.6 | 65.4 ± 9.7 | p = n.s. |
| BMI (kg·m2) | 26.9 ± 3.6 | 25.3 ± 3.6 | 26.2 ± 3.7 | p = n.s. |
| FRAT responses (n) | 1.0 ± 0.9 (0.4, 1.6) | 0.7 ± 0.8 (0.2, 1.1) | 0.5 ± 0.8 (−0.4, 1.4) | p = n.s. |
| Polypharmacy (n) | 2.0 ± 2.0 (0.8, 3.2) | 0.7 ± 1.1 (0.2, 1.4) | 1.7 ± 2.0 | p = n.s. |
| PA amounts | ||||
| Standing time (hours) | 1.16 ± 0.57 | 1.42 ± 0.57 | 1.25 ± 0.39 | |
| Light-intensity physical activity time (hours) | 2.19 ± 0.48 | 2.08 ± 0.35 | 2.23 ± 0.7 | p = n.s. |
| Moderate-to-vigorous physical activity time (hours) | 2.95 ± 0.96 | 2.5 ± 0.78 | 3.6 ± 1.09 | p = n.s. |
| MVPA in bouts ≥ 10 min duration (minutes) | 21.4 ± 25.5 (6.7, 36.1) | 7.8 ± 5.5 (4.7, 11.0) | 15.9 ± 13.8 (1.4, 30.5) | p = n.s. |
| MVPA in bouts of <10 min duration (minutes) | 145 ± 34 | 140 ± 47 | 181 ± 49 | p = n.s. |
| Daily sum of PA bout time (minutes) | 369.77 ± 68.26 | 351.9 ± 77.04 | 416.03 ± 120.64 | p = n.s. |
| Standing (%waking hours) | 7.28 ± 3.66 | 9.04 ± 3.51 | 8.13 ± 2.5 | p = n.s. |
| LIPA (%waking hours) | 13.76 ± 2.93 | 13.32 ± 2.06 | 14.45 ± 4.04 | p = n.s. |
| MVPA (%waking hours) | 18.53 ± 5.96 | 15.93 ± 4.53 | 23.44 ± 6.92 | p = n.s. |
| PA Patterns | ||||
| Bouts of PA (number) | 21.47 ± 4.9 (18.6, 24.3) | 21.24 ± 3.3 (19.3, 23.1) | 21.41 ± 3.68 (16.5, 25.0) | p = n.s. |
| Average daily PA bout length (minutes) | 18.65 ± 4.73 | 17.12 ± 3.59 | 20.77 ± 6.67 | p = n.s. |
| SBPAtime (mins) | 1.46 ± 0.55 | 1.23 ± 0.53 | 1.57 ± 0.46 | p = n.s. |
| STDPAtime (mins) | 18.84 ± 9.08 | 23.55 ± 6.85 | 17.62 ± 3.8 | p = n.s. |
| LIPAPAtime (mins) | 35.01 ± 5.99 | 35.27 ± 5.12 | 31.13 ± 3.99 | p = n.s. |
| MVPAPAtime (mins) | 44.68 ± 10.11 | 39.95 ± 7.03 | 49.68 ± 6.19 | p = n.s. |
| >10 MINSMVPABOUTS (n is count) | 1.06 ± 1.19 | 0.54 ± 0.36 | 0.77 ± 0.66 | p = n.s. |
| SPMVPA (mins) | 155.78 ± 42.52 | 142.41 ± 46.28 | 202.56 ± 71.51 | p = n.s. |
| SB Amounts | ||||
| Sedentary behaviour time (hours) | 9.64 ± 1.24 | 9.63 ± 1.05 | 8.3 ± 1.77 | p = n.s. |
| Sedentary behaviour time (% of waking hours) | 60.43 ± 7.01 | 61.71 ± 7.3 | 53.98 ± 12.06 | p = n.s. |
| Sleep (hrs) | 8.06 ± 0.87 | 8.37 ± 0.65 | 8.62 ± 0.78 | p = n.s. |
| >5 MinSB (mins) | 16.17 ± 3.13 | 15.87 ± 1.55 | 15.62 ± 2.86 | p = n.s. |
| MeanSB (mins) | 32.6 ± 10.16 | 32.97 ± 8.23 | 27.61 ± 10.29 | p = n.s. |
| SB Patterns | ||||
| SB in bouts of <5 min (number) | 6.12 ± 2.2 (4.9, 7.4) | 6.2 ± 2.43 (4.8, 7.6) | 6.56 ± 2.56 (3.2, 9.4) | p = n.s. |
| Average daily sedentary behaviour Bout length (minutes) | 32.2 (27.7–34.6) | 31.9 (27.4–39.4) | 28.2 (21.4–36.8) | p = n.s. |
| SBBreak (n is count) | 21.47 ± 4.9 | 21.25 ± 3.31 | 21.41 ± 3.68 | p = n.s. |
| Alpha-scaling parameter sedentary bout length distribution | 1.44 ± 0.04 | 1.45 ± 0.04 | 1.47 ± 0.06 | p = n.s. |
| W50 (%)-half of total SB is accumulated in SB bouts ≤ this duration | 59.64 ± 15.35 | 58.6 ± 13.07 | 45.96 ± 13.68 | p = n.s. |
| Participants Categorisation | ||||
| Proportion meeting 150 min/week MVPA (%) | 16% | 0% | 0% | p = n.s. (chi-square test) |
| Proportion classified as sedentary (%) | 100% | 100% | 84% | p = n.s. (chi-square test) |
| (A) Proportion of High Regularity at Baseline | SBF | LIPA | Control | ANOVA (* Kruskal–Wallis) | Whole Sample |
| PA amounts | |||||
| Standing time (hours) | 42% | 46% (24%, 37%) | 17% | * p = n.s. | 39% |
| Light-intensity physical activity -LIPA time (hours) | 75% | 46% | 67% | p = n.s. | 61% |
| Moderate-to-vigorous physical activity -MVPA time (hours) | 83% | 77% (19%, 28%) | 100% | * p = n.s. | 84% |
| Standing (%waking hours) | 42% | 38% | 17% | p = n.s. | 35% |
| LIPA (%waking hours) | 75% | 46% | 67% | p = n.s. | 61% |
| MVPA (%waking hours) | 83% | 69% | 100% | p = n.s. | 81% |
| MVPA in bouts ≥ 10 min duration (minutes) | 33% | 15% | 0% | p = n.s. | 19% |
| PA patterns | |||||
| Bouts of physical activity -PA (number) | 83% | 85% | 67% | p = n.s. | 81% |
| Physical activity bouts (Mins) | 67% | 77% | 100% | p = n.s. | 77% |
| Average daily PA bout length (minutes) | 58% | 54% | 33% | p = n.s. | 52% |
| PASTD%_BL | 83% | 69% | 83% | p = n.s. | 77% |
| PAMVPA%_BL | 100% | 100% | 100% | p = 0.041 | 100% |
| SB amounts | |||||
| Sedentary behaviour time (hours) | 100% (9%, 16%) | 100% | 100% | * p = n.s. | 100% |
| Sedentary behaviour time (% of waking hours) | 100% | 100% | 100% | p = n.s. | 100% |
| SB shorter than 5 min (mins) | 8% | 15% | 17% | p = n.s. | 13% |
| SB longer than 5 min (mins) | 75% | 85% | 100% (15%, 25%) | * p = n.s. | 84% |
| Mean SB bout duration (Mins) | 42% | 31% | 83% (17%, 31%) | * p = n.s. | 45% |
| SB patterns | |||||
| Breaks in sedentary behaviour | 83% | 85% | 67% | p = n.s. | 81% |
| Alfa-scaling parameter sedentary bout length distribution | 100% | 100% | 100% (3%, 5%) | * p = n.s. | 100% |
| W50%-half of total SB is accumulated in SB bouts ≤ this duration | 42% | 15% | 17% | p = n.s. | 26% |
| (B) Proportion of high regularity at Week 8 | SBF | LIPA | Control | Kruskal–Wallis | Whole Sample |
| PA amounts | |||||
| Standing time (hours) | 50% | 69% | 67% | p = n.s. | 61% |
| Light-intensity physical activity -LIPA time (hours) | 75% | 54% | 50% | p = n.s. | 61% |
| Moderate-to-vigorous physical activity-MVPA time (hours) | 67% | 46% | 67% | p = n.s. | 58% |
| Standing (%waking hours) | 50% | 69% | 50% | p = n.s. | 58% |
| LIPA (%waking hours) | 75% | 62% | 50% | p = n.s. | 65% |
| MVPA (%waking hours) | 67% | 46% | 67% | p = n.s. | 58% |
| MVPA in bouts ≥10 min duration (minutes) | 58% | 8% | 17% | p = n.s. | 29% |
| PA patterns | |||||
| Bouts of physical activity-PA (number) | 83% | 62% | 83% | p = n.s. | 74% |
| Physical activity bouts (Mins) | 83% | 69% | 67% | p = n.s. | 74% |
| Average daily PA bout length (minutes) | 50% | 62% | 50% | p = n.s. | 55% |
| PASTD%_BL | 83% | 77% | 83% | p = n.s. | 81% |
| PAMVPA%_BL | 92% | 100% | 100% | p = n.s. | 97% |
| SB amounts | |||||
| Sedentary behaviour time (hours) | 83% | 92% | 100% | p = n.s. | 90% |
| Sedentary behaviour time (% of waking hours) | 83% | 92% | 100% | p = n.s. | 90% |
| SB shorter than 5 min (mins) | 8% | 0% | 17% | p = n.s. | 6% |
| SB longer than 5 min (mins) | 50% | 92% | 67% | p = n.s. | 71% |
| Mean SB bout duration (Mins) | 42% | 8% | 50% | p = n.s. | 29% |
| SB patterns | |||||
| Breaks in sedentary behaviour | 83% | 62% | 83% | p = n.s. | 74% |
| Alfa-scaling parameter sedentary bout length distribution | 100% | 100% | 100% | p = n.s. | 100% |
| W50%-half of total SB is accumulated in SB bouts ≤ this duration | 25% | 31% | 33% | p = n.s. | 29% |
| (C) Change in participants’ variability at baseline vs. week 8 | SBF | LIPA | Control | Whole Sample | |
| PA amounts | |||||
| Standing time (hours) | p = n.s. | p = 0.084 | p = n.s. | p = 0.091 | |
| Light-intensity physical activity-LIPA time (hours) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Moderate-to-vigorous physical activity -MVPA time (hours) | p = n.s. | p = n.s. | p = n.s. | p = 0.079 | |
| Standing (%waking hours) | p = n.s. | p = 0.064 | p = n.s. | p = 0.079 | |
| LIPA (%waking hours) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| MVPA (%waking hours) | p = 0.055 | p = 0.073 | p = n.s. | p = 0.029 | |
| MVPA in bouts ≥10 min duration (minutes) | p = n.s. | p = n.s. | p = 0.031 | p = n.s. | |
| PA patterns | |||||
| Bouts of physical activity-PA (number) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Physical activity bouts (Mins) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Average daily PA bout length (minutes) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| PASTD%_BL | p = n.s. | p = 0.020 | p = n.s. | p = n.s. | |
| PAMVPA%_BL | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| SB amounts | |||||
| Sedentary behaviour time (hours) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Sedentary behaviour time (% of waking hours) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| SB shorter than 5 min (mins) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| SB longer than 5 min (mins) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Mean SB bout duration (Mins) | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| SB Patterns | |||||
| Breaks in sedentary behaviour | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| Alfa-scaling parameter sedentary bout length distribution | p = n.s. | p = n.s. | p = n.s. | p = n.s. | |
| W50%_half of total SB is accumulated in SB bouts ≤ this duration | p = 0.055 | p = n.s. | p = n.s. | p = n.s. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grant, D.M.; Tomlinson, D.J.; Tsintzas, K.; Onambele-Pearson, G.L. Daily Variability in Sedentary Behaviour and Physical Activity Responsiveness in Older Women. Sensors 2025, 25, 2194. https://doi.org/10.3390/s25072194
Grant DM, Tomlinson DJ, Tsintzas K, Onambele-Pearson GL. Daily Variability in Sedentary Behaviour and Physical Activity Responsiveness in Older Women. Sensors. 2025; 25(7):2194. https://doi.org/10.3390/s25072194
Chicago/Turabian StyleGrant, Dale M., David J. Tomlinson, Kostas Tsintzas, and Gladys L. Onambele-Pearson. 2025. "Daily Variability in Sedentary Behaviour and Physical Activity Responsiveness in Older Women" Sensors 25, no. 7: 2194. https://doi.org/10.3390/s25072194
APA StyleGrant, D. M., Tomlinson, D. J., Tsintzas, K., & Onambele-Pearson, G. L. (2025). Daily Variability in Sedentary Behaviour and Physical Activity Responsiveness in Older Women. Sensors, 25(7), 2194. https://doi.org/10.3390/s25072194