
Investigation and Validation of New Heart Rate Measurement Sites for Wearable Technologies



Abstract
1. Introduction
2. Materials and Methods
2.1. Sensor Location
2.2. Photoplethysmography (PPG) Sensor
2.3. Microcontroller
2.4. Bluetooth Module
2.5. Mobile Application
2.6. Data Acquisition
2.7. Testing
2.8. Data Analysis
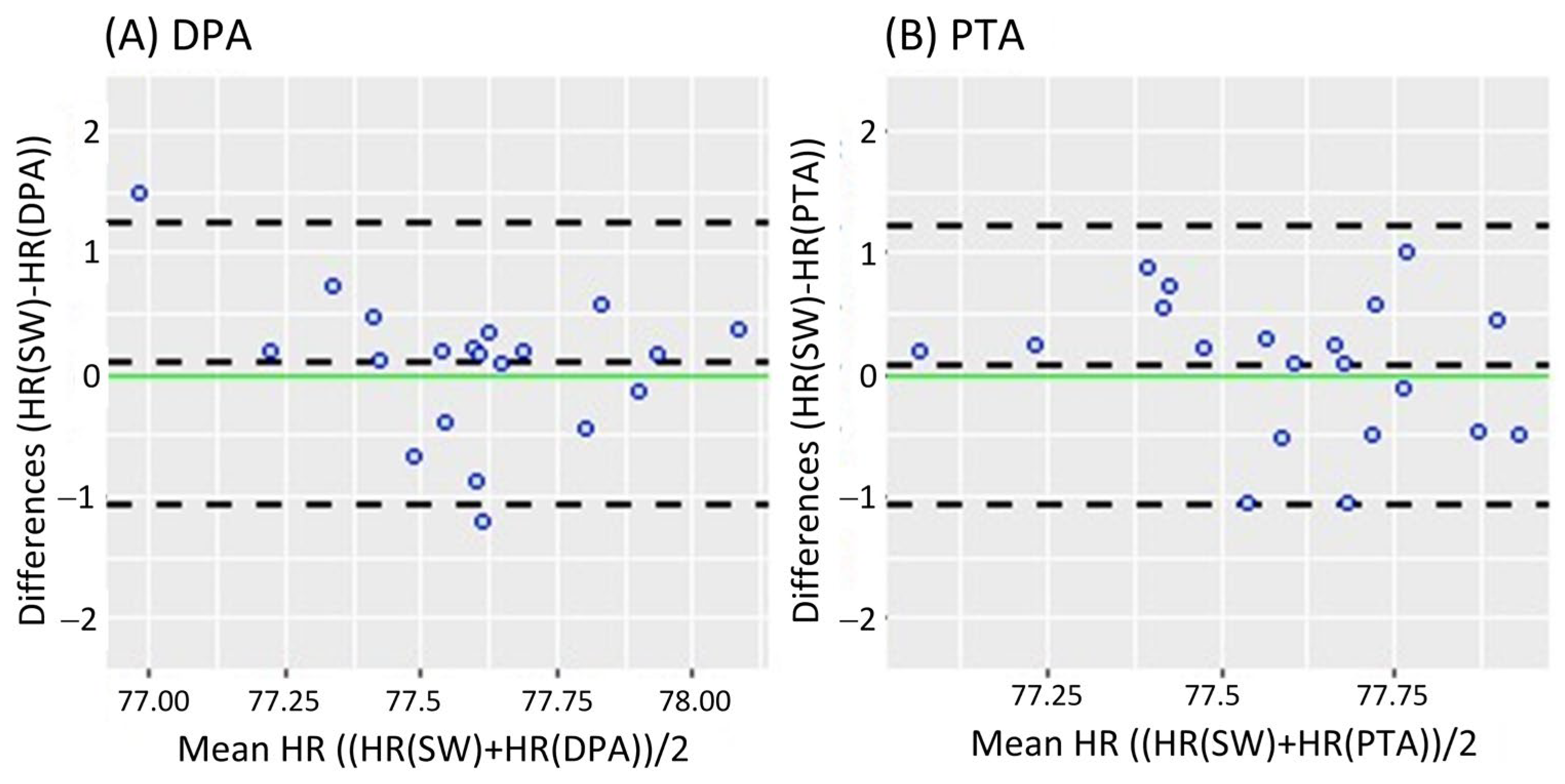
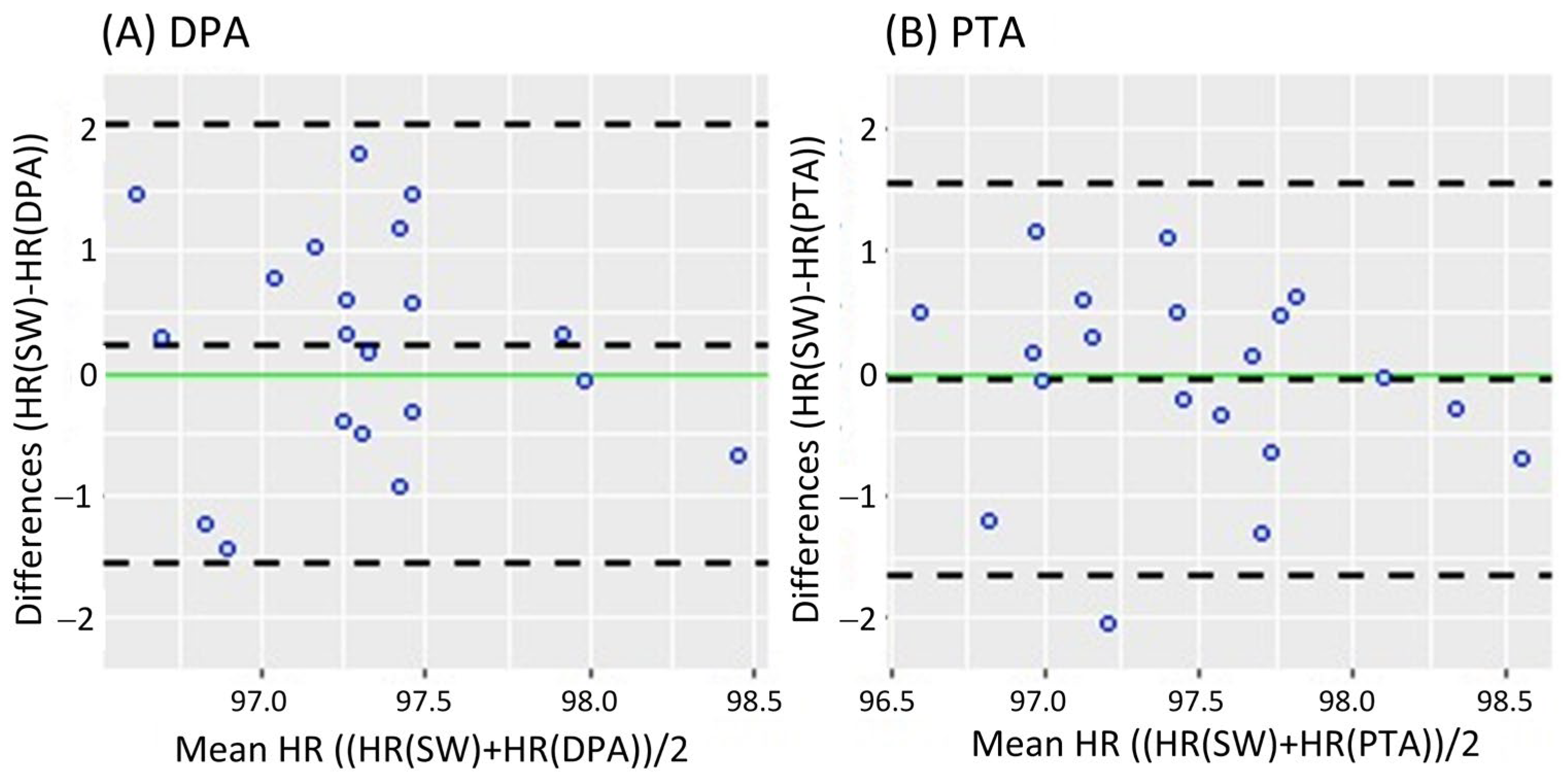
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheong, S.H.R.; Ng, Y.J.X.; Lau, Y.; Lau, S.T. Wearable technology for early detection of COVID-19: A systematic scoping review. Prev. Med. 2022, 162, 107170. [Google Scholar] [CrossRef] [PubMed]
- Henson, C.; Rambaldini, B.; Freedman, B.; Carlson, B.; Parter, C.; Christie, V.; Skinner, J.; Meharg, D.; Kirwan, M.; Ward, K.; et al. Wearables for early detection of atrial fibrillation and timely referral for Indigenous people ≥55 years: Mixed-methods protocol. BMJ Open 2024, 14, e077820. [Google Scholar] [CrossRef] [PubMed]
- Wearable Technology Market Size & Trends. Available online: https://www.grandviewresearch.com/industry-analysis/wearable-technology-market (accessed on 20 March 2025).
- ACSM Fitness Trends, ACSM_CMS. Available online: https://www.acsm.org/education-resources/trending-topics-resources/acsm-fitness-trends (accessed on 11 August 2024).
- Subramaniam, S.; Majumder, S.; Faisal, A.I.; Deen, M.J. Insole-Based Systems for Health Monitoring: Current Solutions and Research Challenges. Sensors 2022, 22, 438. [Google Scholar] [CrossRef]
- Sun, X.; Qiu, L.; Wu, Y.; Tang, Y.; Cao, G. SleepMonitor: Monitoring Respiratory Rate and Body Position During Sleep Using Smartwatch. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 1–22. [Google Scholar] [CrossRef]
- Artese, A.L.; Rawat, R.; Sung, A.D. The use of commercial wrist-worn technology to track physiological outcomes in behavioral interventions. Curr. Opin. Clin. Nutr. Metab. Care 2023, 26, 534–540. [Google Scholar] [CrossRef]
- Bonato, P. Wearable Sensors and Systems. IEEE Eng. Med. Biol. Mag. 2010, 29, 25–36. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhu, Z.; Bazor, B.; Lee, S.; Ding, Z.; Pan, T. FeetBeat: A Flexible Iontronic Sensing Wearable Detects Pedal Pulses and Muscular Activities. IEEE Trans. Biomed. Eng. 2019, 66, 3072–3079. [Google Scholar] [CrossRef]
- Han, H.; Kim, G.; Choi, S.; Basu, A.; Yoon, S.W. Human Activity and Correlated Posture Monitoring Using Earlobe-Worn Wearable Sensor System and Deep Learning Algorithm. IEEE Sensors J. 2023, 24, 533–542. [Google Scholar] [CrossRef]
- Hegde, N.; Bries, M.; Sazonov, E. A Comparative Review of Footwear-Based Wearable Systems. Electronics 2016, 5, 48. [Google Scholar] [CrossRef]
- Celik, Y.; Stuart, S.; Woo, W.; Godfrey, A. Gait analysis in neurological populations: Progression in the use of wearables. Med. Eng. Phys. 2021, 87, 9–29. [Google Scholar] [CrossRef]
- Panahi, M.; Masihi, S.; Hanson, A.; Rodriguez-Labra, J.R.; Masihi, A.; Maddipatla, D.; Narakathu, B.B.; Lawson, D.; Atashbar, M.Z. A Smart Wearable Oximeter Insole for Monitoring SpO2 Levels of Diabetics’ Foot Ulcer. In Proceedings of the IEEE International Conference on Flexible and Printable Sensors and Systems (FLEPS), Vienna, Austria, 10–13 July 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Moulaei, K.; Malek, M.; Sheikhtaheri, A. A smart wearable device for monitoring and self-management of diabetic foot: A proof of concept study. Int. J. Med. Inform. 2021, 146, 104343. [Google Scholar] [CrossRef]
- Hong, S.; Park, K.S. Unobtrusive Photoplethysmographic Monitoring Under the Foot Sole while in a Standing Posture. Sensors 2018, 18, 3239. [Google Scholar] [CrossRef]
- Datcu, M.; Luca, C.; Corciova, C. Smart Wearable SpO2 Monitor for Newborns. In Proceedings of the 6th International Conference on Advancements of Medicine and Health Care through Technology, Cluj-Napoca, Romania, 17–20 October 2018; Vlad, S., Roman, N.M., Eds.; IFMBE Proceedings. Springer: Singapore, 2019; Volume 71, pp. 41–44. [Google Scholar] [CrossRef]
- Jarchi, D.; Casson, A.J. Estimation of heart rate from foot worn photoplethysmography sensors during fast bike exercise. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3155–3158. [Google Scholar] [CrossRef]
- Liu, M.; Jiang, F.; Jiang, H.; Ye, S.; Chen, H. Low-power, noninvasive measurement system for wearable ballistocardiography in sitting and standing positions. Comput. Ind. 2017, 91, 24–32. [Google Scholar] [CrossRef]
- Eom, H.; Roh, J.; Hariyani, Y.S.; Baek, S.; Lee, S.; Kim, S.; Park, C. Deep Learning-Based Optimal Smart Shoes Sensor Selection for Energy Expenditure and Heart Rate Estimation. Sensors 2021, 21, 7058. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.; Eom, H.; Hariyani, Y.S.; Kim, G.; Roh, J.; Kim, S.; Park, C. Deep Learning Based Heart Rate Estimation Using Smart Shoes Sensor. In Proceedings of the 2020 IEEE International Conference on Consumer Electronics—Asia (ICCE-Asia), Seoul, Republic of Korea, 1–3 November 2020; pp. 1–4. [Google Scholar] [CrossRef]
- Health—United Nations Sustainable Development. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 13 August 2024).
- Moran, J.F. Pulse. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworth Publisher: Boston, MA, USA, 1990. [Google Scholar]
- Kim, J.; Chou, E.-F.; Le, J.; Wong, S.; Chu, M.; Khine, M. Soft Wearable Pressure Sensors for Beat-to-Beat Blood Pressure Monitoring. Adv. Healthc. Mater. 2019, 8, 1900109. [Google Scholar] [CrossRef] [PubMed]
- Maddury, J. Arterial Pulse. Indian J. Cardiovasc. Dis. Women WINCARS 2017, 02, 099–110. [Google Scholar] [CrossRef]
- Gogalniceanu, P.; Lancaster, R.T.; Patel, V.I. Clinical Assessment of Peripheral Arterial Disease of the Lower Limbs. N. Engl. J. Med. 2018, 378, e24. [Google Scholar] [CrossRef]
- MAX30100 Datasheet and Product Info|Analog Devices. Available online: https://www.analog.com/en/products/max30100.html#documentation (accessed on 11 June 2024).
- Wang, C.; Li, Z.; Wei, X. Monitoring heart and respiratory rates at radial artery based on PPG. Optik 2013, 124, 3954–3956. [Google Scholar] [CrossRef]
- Matouq, J.; AlSaaideh, I.; Hatahet, O. Validation of Heart Rate Monitoring Using PPG Sensor at Dorsalis Pedis Artery. In Proceedings of the 22nd International Conference on Research and Education in Mechatronics (REM), Amman, Jordan, 24–26 September 2024; pp. 1–4. [Google Scholar] [CrossRef]
- Karnadi, J.; Roihan, I.; Ekadiyanto, A.; A Koestoera, R. Development of a Low-cost Arduino-based Patient Monitoring System for Heartrate, Oxygen Saturation and Body Temperature Parameters. J. Appl. Sci. Eng. Technol. 2022, 1, 26. [Google Scholar] [CrossRef]
- MIT App Inventor. Available online: https://appinventor.mit.edu/ (accessed on 12 August 2024).
- Spaccarotella, C.; Polimeni, A.; Mancuso, C.; Pelaia, G.; Esposito, G.; Indolfi, C. Assessment of Non-Invasive Measurements of Oxygen Saturation and Heart Rate with an Apple Smartwatch: Comparison with a Standard Pulse Oximeter. J. Clin. Med. 2022, 11, 1467. [Google Scholar] [CrossRef]
- Alkalthem, D.; Alenazi, S.; Alsowinea, M.; Al Fagih, A.; Alnasser, S.K.; Alanzai, N. The Reliability of the Apple Watch’s Electrocardiogram. Cureus 2023, 15, e49786. [Google Scholar] [CrossRef]
- Bent, B.; Goldstein, B.A.; Kibbe, W.A.; Dunn, J.P. Investigating sources of inaccuracy in wearable optical heart rate sensors. npj Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Khushhal, A.; Nichols, S.; Evans, W.; Gleadall-Siddall, D.O.; Page, R.; O’Doherty, A.F.; Carroll, S.; Ingle, L.; Abt, G. Validity and Reliability of the Apple Watch for Measuring Heart Rate During Exercise. Sports Med. Int. Open 2017, 1, E206–E211. [Google Scholar] [CrossRef]
- Falter, M.; Budts, W.; Goetschalckx, K.; Cornelissen, V.; Buys, R. Accuracy of Apple Watch Measurements for Heart Rate and Energy Expenditure in Patients with Cardiovascular Disease: Cross-Sectional Study. JMIR mHealth uHealth 2019, 7, e11889. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Bunce, C. Correlation, Agreement, and Bland–Altman Analysis: Statistical Analysis of Method Comparison Studies. Arch. Ophthalmol. 2009, 148, 4–6. [Google Scholar] [CrossRef]
- Saçan, K.B.; Ertaş, G. Performance assessment of MAX30100 SpO2/heartrate sensor. In Proceedings of the 2017 Medical Technologies National Congress (TIPTEKNO), Trabzon, Turkey, 12–14 October 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Sari, N.N.; Gani, M.N.; Yusuf, R.A.M.; Firmando, R. Telemedicine for silent hypoxia: Improving the reliability and accuracy of Max30100-based system. Indones. J. Electr. Eng. Comput. Sci. 2021, 22, 1419–1426. [Google Scholar] [CrossRef]
- Islam, R.; Kabir, M.; Mridha, M.F.; Alfarhood, S.; Safran, M.; Che, D. Deep Learning-Based IoT System for Remote Monitoring and Early Detection of Health Issues in Real-Time. Sensors 2023, 23, 5204. [Google Scholar] [CrossRef]
- Ganesh, K.V.S.S.; Jeyanth, S.S.; Bevi, A.R. IOT based portable heart rate and SpO2 pulse oximeter. HardwareX 2022, 11, e00309. [Google Scholar] [CrossRef]
- ANSI/AAMI EC13-2002; Cardiac Monitors, Heart Rate Meters, and Alarms. Association for the Advancement of Medical Instrumentation (AAMI): Arlington, VA, USA, 2002.
- Shaffer, F.; Meehan, Z.M.; Zerr, C.L. A Critical Review of Ultra-Short-Term Heart Rate Variability Norms Research. Front. Neurosci. 2020, 14, e594880. [Google Scholar] [CrossRef]
- Brearley, S.; Shearman, C.P.; Simms, M.H. Peripheral pulse palpation: An unreliable physical sign. Ann. R. Coll. Surg. Eng. 1992, 74, 169–171. [Google Scholar]
- Hill, R.D.; Smith, R.B. Examination of the Extremities: Pulses, Bruits, and Phlebitis. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworth Publisher: Boston, MA, USA, 1990. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variable | n = 20 (10 Females, 10 Males) |
|---|---|
| Mean (SD) | |
| Age (years) | 21.5 (2.4) |
| Weight (kg) | 63.4 (8.2) |
| Height (cm) | 170.5 (6.7) |
| BMI | 21.778 (2.3) |
| Standing Mean (SD) | Walking Mean (SD) | |
|---|---|---|
| Apple Smartwatch (bpm) * | 77.6 (0.3) | 97.4 (0.6) |
| Dorsalis Pedis Artery (DPA) (bpm) * | 77.6 (0.4) | 97.2 (0.6) |
| Posterior Tibial Artery (TPA) (bpm) * | 77.6 (0.4) | 97.5 (0.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matouq, J.; AlSaaideh, I.; Hatahet, O.; Pott, P.P. Investigation and Validation of New Heart Rate Measurement Sites for Wearable Technologies. Sensors 2025, 25, 2069. https://doi.org/10.3390/s25072069
Matouq J, AlSaaideh I, Hatahet O, Pott PP. Investigation and Validation of New Heart Rate Measurement Sites for Wearable Technologies. Sensors. 2025; 25(7):2069. https://doi.org/10.3390/s25072069
Chicago/Turabian StyleMatouq, Jumana, Ibrahim AlSaaideh, Oula Hatahet, and Peter P. Pott. 2025. "Investigation and Validation of New Heart Rate Measurement Sites for Wearable Technologies" Sensors 25, no. 7: 2069. https://doi.org/10.3390/s25072069
APA StyleMatouq, J., AlSaaideh, I., Hatahet, O., & Pott, P. P. (2025). Investigation and Validation of New Heart Rate Measurement Sites for Wearable Technologies. Sensors, 25(7), 2069. https://doi.org/10.3390/s25072069