
Physical Activity in Pre-Ambulatory Children with Cerebral Palsy: An Exploratory Validation Study to Distinguish Active vs. Sedentary Time Using Wearable Sensors

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
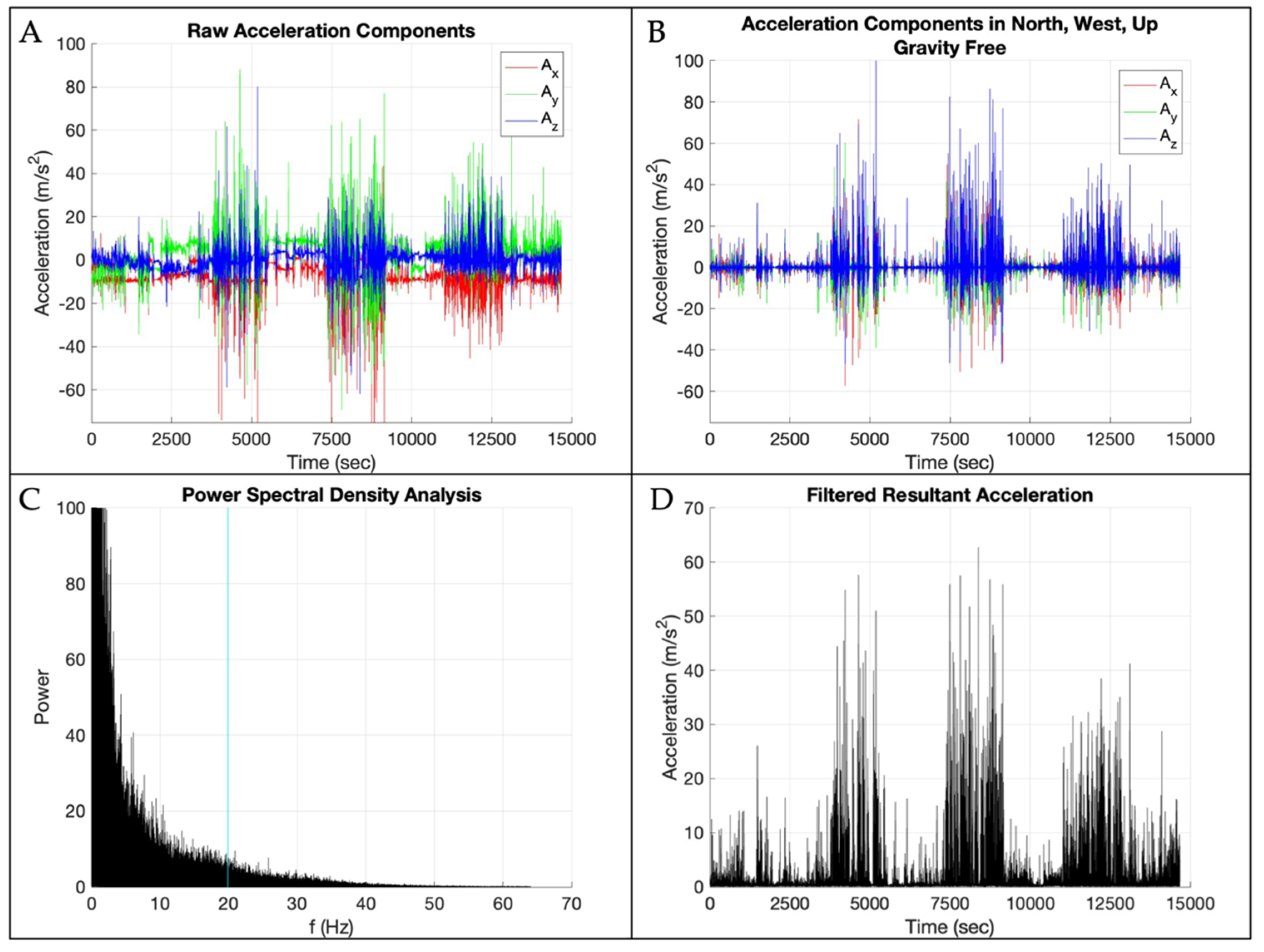
2.3. Data Processing
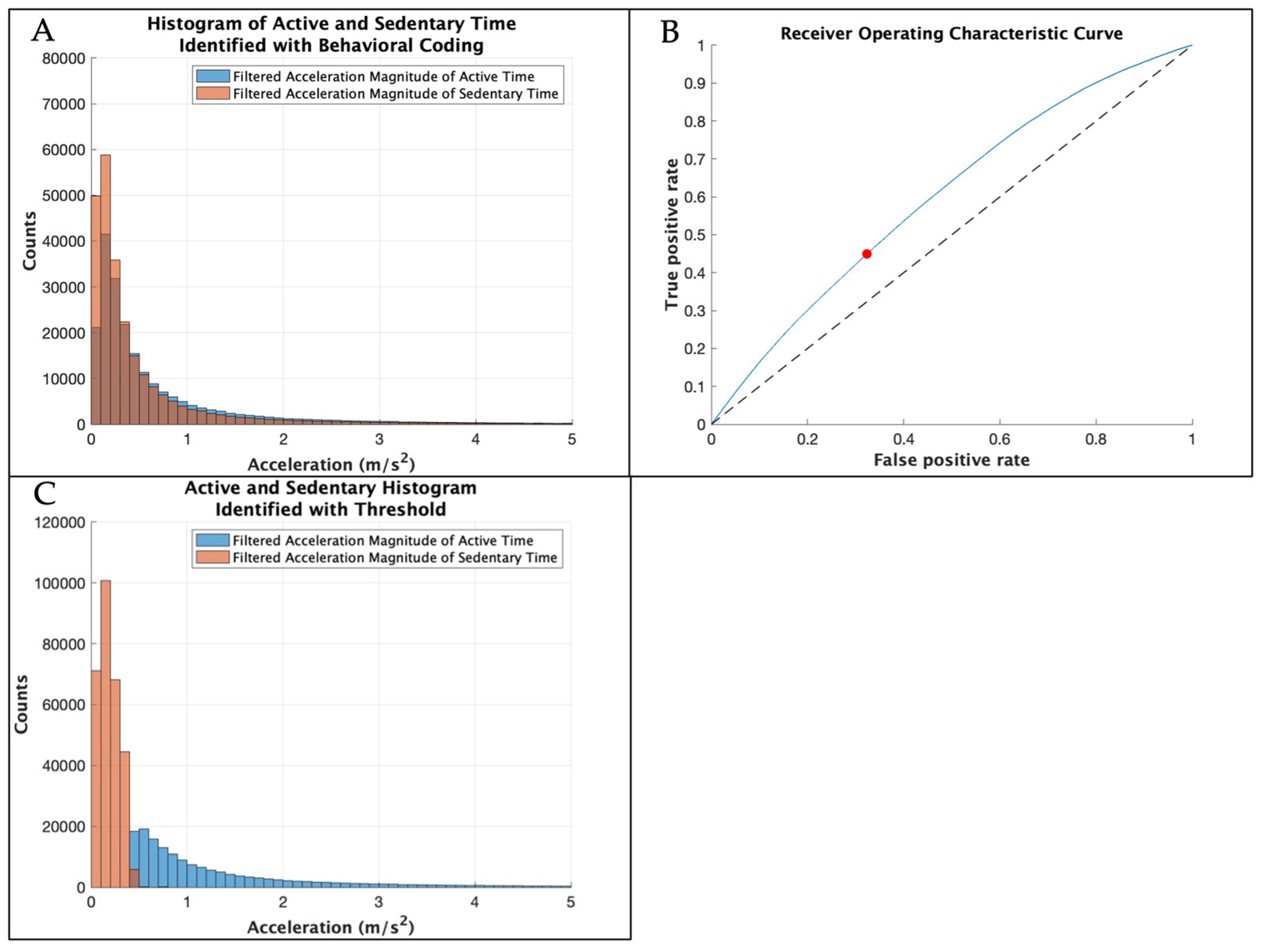
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CP | Cerebral palsy |
| GMFCS | Gross Motor Function Classification System |
| ROC | Receiver operating characteristic |
| EMA | Ecological momentary assessment |
References
- Franchak, J.M.; Kretch, K.S.; Adolph, K.E. See and be seen: Infant-caregiver social looking during locomotor free play. Dev. Sci. 2018, 21, e12626. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.J. Exploratory-Behavior In The Development Of Perceiving, Acting, And The Acquiring Of Knowledge. Annu. Rev. Psychol. 1988, 39, 1–41. [Google Scholar] [CrossRef]
- Belsky, J.; Most, R.K. From Exploration to Play—A Cross-Sectional Study of Infant Free Play-Behavior. Dev. Psychol. 1981, 17, 630–639. [Google Scholar] [CrossRef]
- Babik, I.; Galloway, J.C.; Lobo, M.A. Early Exploration of One’s Own Body, Exploration of Objects, and Motor, Language, and Cognitive Development Relate Dynamically Across the First Two Years of Life. Dev. Psychol. 2022, 58, 222–235. [Google Scholar] [CrossRef] [PubMed]
- James, K.H.; Swain, S.N. Only self-generated actions create sensori-motor systems in the developing brain. Dev. Sci. 2011, 14, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Soska, K.C.; Adolph, K.E. Postural Position Constrains Multimodal Object Exploration in Infants. Infancy 2014, 19, 138–161. [Google Scholar] [CrossRef] [PubMed]
- Alamoudi, N.A.; Algabbani, M.F.; Al-Heizan, M.O.; Alhusaini, A.A. Physical activity and sedentary behavior among ambulatory children with cerebral palsy using accelerometer: A cross-sectional study. Front. Pediatr. 2024, 12, 1463288. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child. Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Keawutan, P.; Bell, K.L.; Oftedal, S.; Ware, R.S.; Stevenson, R.D.; Davies, P.S.W.; Boyd, R.N. Longitudinal physical activity and sedentary behaviour in preschool-aged children with cerebral palsy across all functional levels. Dev. Med. Child. Neurol. 2017, 59, 852–857. [Google Scholar] [CrossRef]
- Oftedal, S.; Bell, K.L.; Davies, P.S.W.; Ware, R.S.; Boyd, R.N. Sedentary and Active Time in Toddlers with and without Cerebral Palsy. Med. Sci. Sports Exerc. 2015, 47, 2076–2083. [Google Scholar] [CrossRef]
- Abbruzzese, L.D.; Yamane, N.; Fein, D.; Naigles, L.; Goldman, S. Assessing Child Postural Variability: Development, Feasibility, and Reliability of a Video Coding System. Phys. Occup. Ther. Pediatr. 2020, 41, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Bril, B.; Sabatier, C. The Cultural-Context of Motor Development—Postural Manipulations in the Daily Life of Bambara Babies (MALI). Int. J. Behav. Dev. 1986, 9, 439–453. [Google Scholar] [CrossRef]
- Ahmadi, M.N.; O’Neil, M.E.; Baque, E.; Boyd, R.N.; Trost, S.G. Machine Learning to Quantify Physical Activity in Children with Cerebral Palsy: Comparison of Group, Group-Personalized, and Fully-Personalized Activity Classification Models. Sensors 2020, 20, 3976. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.V.; Sugianto, A.; Nickele, K.; Zavos, P.; Sindu, P.; Ali, M.; Kwon, S. Hidden Markov model-based activity recognition for toddlers. Physiol. Meas. 2020, 41, 025003. [Google Scholar] [CrossRef]
- Kwon, S.; Sindu, P.; Nickele, K.; Zavos, P.; Sugianto, A.; Albert, M.V. Accelerometer-Based Activity Classification Algorithm for Toddlers: Machine Learning Approach. Med. Sci. Sports Exerc. 2019, 51, 363–364. [Google Scholar] [CrossRef]
- Kwon, S.; Zavos, P.; Nickele, K.; Sugianto, A.; Albert, M.V. Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities. Int. J. Environ. Res. Public Health 2019, 16, 2598. [Google Scholar] [CrossRef]
- Welch, S.B.; Honegger, K.; O’Brien, M.; Capan, S.; Kwon, S.; Welch, S.B.; Honegger, K.; O’Brien, M.; Capan, S.; Kwon, S. Examination of physical activity development in early childhood: Protocol for a longitudinal cohort study of mother-toddler dyads. BMC Pediatrics 2023, 23, 129. [Google Scholar] [CrossRef]
- Bennetts, S.K.; Mensah, F.K.; Green, J.; Hackworth, N.J.; Westrupp, E.M.; Reilly, S. Mothers’ Experiences of Parent-Reported and Video-Recorded Observational Assessments. J. Child. Fam. Stud. 2017, 26, 3312–3326. [Google Scholar] [CrossRef]
- Friesen, K.B.; Zhang, Z.T.; Monaghan, P.G.; Oliver, G.D.; Roper, J.A. All eyes on you: How researcher presence changes the way you walk. Sci. Rep. 2020, 10, 17159. [Google Scholar] [CrossRef] [PubMed]
- Hager, E.R.; Gormley, C.E.; Latta, L.W.; Treuth, M.S.; Caulfield, L.E.; Black, M.M. Toddler physical activity study: Laboratory and community studies to evaluate accelerometer validity and correlates. BMC Public Health 2016, 16, 936. [Google Scholar] [CrossRef]
- O’Neil, M.E.; Fragala-Pinkham, M.A.; Forman, J.L.; Trost, S.G. Measuring reliability and validity of the ActiGraph GT3X accelerometer for children with cerebral palsy: A feasibility study. J. Pediatr. Rehabil. Med. 2014, 7, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Cauwenberghe, E.; Gubbels, J.; De Bourdeaudhuij, I.; Cardon, G. Feasibility and validity of accelerometer measurements to assess physical activity in toddlers. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Oftedal, S.; Bell, K.L.; Davies, P.S.W.; Ware, R.S.; Boyd, R.N. Validation of Accelerometer Cut Points in Toddlers with and without Cerebral Palsy. Med. Sci. Sports Exerc. 2014, 46, 1808–1815. [Google Scholar] [CrossRef] [PubMed]
- Alhassan, S.; Sirard, J.R.; Kurdziel, L.B.F.; Merrigan, S.; Greever, C.; Spencer, R.M.C. Cross-Validation of Two Accelerometers for Assessment of Physical Activity and Sedentary Time in Preschool Children. Pediatr. Exerc. Sci. 2017, 29, 268–277. [Google Scholar] [CrossRef]
- Greever, C.J.; Sirard, J.; Alhassan, S. Objective Analysis of Preschoolers’ Physical Activity Patterns During Free Playtime. J. Phys. Act. Health 2015, 12, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Thelen, E.; Fisher, D.M. Newborn stepping: An explanation for a “disappearing” reflex. Dev. Psychol. 1982, 18, 760–775. [Google Scholar] [CrossRef]
- Prioreschi, A.; Micklesfield, L.K. A scoping review examining physical activity measurement and levels in the first 2 years of life. Child. Care Health Dev. 2016, 42, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Reedman, S.E.; Kho, M.E.; Timmons, B.W.; Verschuren, O.; Gorter, J.W. Operationalization, measurement, and health indicators of sedentary behavior in individuals with cerebral palsy: A scoping review. Disabil. Rehabil. 2021, 44, 6070–6081. [Google Scholar] [CrossRef] [PubMed]
- Hurter, L.; Fairclough, S.J.; Knowles, Z.R.; Porcellato, L.A.; Cooper-Ryan, A.M.; Boddy, L.M. Establishing Raw Acceleration Thresholds to Classify Sedentary and Stationary Behaviour in Children. Children 2018, 5, 172. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Cliff, D.P.; Ahmadi, M.N.; Tuc, N.V.; Hagenbuchner, M. Sensor-enabled Activity Class Recognition in Preschoolers: Hip versus Wrist Data. Med. Sci. Sports Exerc. 2018, 50, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Fees, B.S.; Haar, S.J.; Murray, A.D.; Crowe, L.K. Identification and Validity of Accelerometer Cut-Points for Toddlers. Obesity 2012, 20, 2317–2319. [Google Scholar] [CrossRef]
- Bruijns, B.A.; Truelove, S.; Johnson, A.M.; Gilliland, J.; Tucker, P. Infants’ and toddlers’ physical activity and sedentary time as measured by accelerometry: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, B.; Cunha, A.B.; Lobo, M.A. Design and validation of a smart garment to measure positioning practices of parents with young infants. Infant. Behav. Dev. 2021, 62, 101530. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M.; Rasanen, O.; Ilen, E.; Hayrinen, T.; Kivi, A.; Marchi, V.; Gallen, A.; Blom, S.; Varhe, A.; Kaartinen, N.; et al. Automatic Posture and Movement Tracking of Infants with Wearable Movement Sensors. Sci. Rep. 2020, 10, 169. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M.; Taylor, E.; Gallen, A.; Ilén, E.; Saari, A.; Sankilampi, U.; Räsänen, O.; Haataja, L.M.; Vanhatalo, S. Charting infants’ motor development at home using a wearable system: Validation and comparison to physical growth charts. eBioMedicine 2023, 92, 104591. [Google Scholar] [CrossRef]
- Trujillo-Priego, I.A.; Smith, B.A. Kinematic characteristics of infant leg movements produced across a full day. J. Rehabil. Assist. Technol. Eng. 2017, 4, 2055668317717461. [Google Scholar] [CrossRef]
- Smith, B.A.; Trujillo-Priego, I.A.; Lane, C.J.; Finley, J.M.; Horak, F.B. Daily Quantity of Infant Leg Movement: Wearable Sensor Algorithm and Relationship to Walking Onset. Sensors 2015, 15, 19006–19020. [Google Scholar] [CrossRef]
- Ghazi, M.A.; Zhou, J.; Havens, K.L.; Smith, B.A. Accelerometer Thresholds for Estimating Physical Activity Intensity Levels in Infants: A Preliminary Study. Sensors 2024, 24, 4436. [Google Scholar] [CrossRef]
- Prosser, L.A.; Skorup, J.; Pierce, S.R.; Jawad, A.F.; Fagg, A.H.; Kolobe, T.H.A.; Smith, B.A. Locomotor learning in infants at high risk for cerebral palsy: A study protocol. Front. Pediatr. 2023, 11, 891633. [Google Scholar] [CrossRef] [PubMed]
- Prosser, L.A.; Pierce, S.R.; Dillingham, T.R.; Bernbaum, J.C.; Jawad, A.F. iMOVE: Intensive Mobility training with Variability and Error compared to conventional rehabilitation for young children with cerebral palsy: The protocol for a single blind randomized controlled trial. BMC Pediatr. 2018, 18, 329. [Google Scholar] [CrossRef] [PubMed]
- Datavyu Team. Datavyu: A Video Coding Tool. 2014. Available online: http://datavyu.org (accessed on 16 February 2025).
- Holmstrom, L. Using Orientation Estimates to Convert from Sensor Frame to Earth Frame of Reference. Available online: https://support.apdm.com/hc/en-us/articles/214504186-Using-orientation-estimates-to-convert-from-sensor-frame-to-Earth-frame-of-refernce (accessed on 30 September 2021).
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Zhou, J.D.; Schaefer, S.Y.; Smith, B.A. Quantifying Caregiver Movement when Measuring Infant Movement across a Full Day: A Case Report. Sensors 2019, 19, 2886. [Google Scholar] [CrossRef] [PubMed]
- Worobey, J.; Vetrini, N.R.; Rozo, E.M. Mechanical measurement of infant activity: A cautionary note. Infant. Behav. Dev. 2009, 32, 167–172. [Google Scholar] [CrossRef]
- Airaksinen, M.; Vaaras, E.; Haataja, L.; Räsänen, O.; Vanhatalo, S. Automatic assessment of infant carrying and holding using at-home wearable recordings. Sci. Rep. 2024, 14, 4852. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J. Using accelerometers to measure physical activity in large-scale epidemiological studies: Issues and challenges. Br. J. Sports Med. 2014, 48, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Franchak, J.M.; Scott, V.; Luo, C. A Contactless Method for Measuring Full-Day, Naturalistic Motor Behavior Using Wearable Inertial Sensors. Front. Psychol. 2021, 12, 701343. [Google Scholar] [CrossRef]
- Franchak, J.M. Changing Opportunities for Learning in Everyday Life: Infant Body Position Over the First Year. Infancy 2019, 24, 187–209. [Google Scholar] [CrossRef] [PubMed]
- Rosales, M.R.; Rohloff, P.; Vanderbilt, D.L.; Tripathi, T.; Valentini, N.C.; Dusing, S.; Smith, B.A. Collecting Infant Environmental and Experiential Data Using Smartphone Surveys. Pediatr. Phys. Ther. 2021, 33, 47–49. [Google Scholar] [CrossRef]
- Nam, Y.; Park, J.W. Child Activity Recognition Based on Cooperative Fusion Model of a Triaxial Accelerometer and a Barometric Pressure Sensor. IEEE J. Biomed. Health Inform. 2013, 17, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Hagenbuchner, M.; Cliff, D.P.; Trost, S.G.; Tuc, N.V.; Peoples, G.E. Prediction of activity type in preschool children using machine learning techniques. J. Sci. Med. Sport. 2015, 18, 426–431. [Google Scholar] [CrossRef]
- Zhao, W.; Adolph, A.L.; Puyau, M.R.; Vohra, F.A.; Butte, N.F.; Zakeri, I.F. Support vector machines classifiers of physical activities in preschoolers. Physiol. Rep. 2013, 1, e00006. [Google Scholar] [CrossRef]
- Kang, L.J.; Hsieh, M.C.; Liao, H.F.; Hwang, A.W. Environmental Barriers to Participation of Preschool Children with and without Physical Disabilities. Int. J. Environ. Res. Public. Health 2017, 14, 518. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.S.; Kwon, J.Y. Effects of Modified Constraint-Induced Movement Therapy in Real-World Arm Use in Young Children with Unilateral Cerebral Palsy: A Single-Blind Randomized Trial. Neuropediatrics 2020, 51, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Trujillo-Priego, I.A.; Lane, C.J.; Vanderbilt, D.L.; Deng, W.Y.; Loeb, G.E.; Shida, J.; Smith, B.A. Development of a Wearable Sensor Algorithm to Detect the Quantity and Kinematic Characteristics of Infant Arm Movement Bouts Produced across a Full Day in the Natural Environment. Technologies 2017, 5, 39. [Google Scholar] [CrossRef] [PubMed]
- Orlando, J.M.; Pierce, S.; Mohan, M.; Skorup, J.; Paremski, A.; Bochnak, M.; Prosser, L.A. Physical activity in non-ambulatory toddlers with cerebral palsy. Res. Dev. Disabil. 2019, 90, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Rachwani, J.; Santamaria, V.; Saavedra, S.L.; Woollacott, M.H. The development of trunk control and its relation to reaching in infancy: A longitudinal study. Front. Hum. Neurosci. 2015, 9, 94. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Sex | Age (Months) | GMFCS ^ |
|---|---|---|---|
| 1 | F | 21.9 | III |
| 2 | M | 16.9 | V |
| 3 | F | 15.9 | I |
| 4 | F | 16.0 | III |
| 5 | F | 11.6 | I |
| 6 | M | 9.4 | V |
| 7 | M | 16.3 | IV |
| 8 | F | 16.6 | II |
| 9 | F | 13.8 | I |
| 10 | M | 12.8 | I |
| Study ID | Optimal Threshold (m/s/s) | Area Under the Curve | Sum of True Positives and True Negatives + | True Positives + (%) | True Negatives + (%) | False Positives + (%) | False Negatives + (%) |
|---|---|---|---|---|---|---|---|
| 1–8 | 0.417 | 0.60 | 75.1 | 27.9 | 47.2 | 6.9 | 17.9 |
| Study ID | Sum of True Positives and True Negatives + | True Positives + (%) | True Negatives + (%) | False Positives + (%) | False Negatives + (%) | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| 9 | 92.2 | 75.2 | 17.0 | 2.0 | 5.8 | 0.93 | 0.90 |
| 10 | 89.7 | 53.8 | 35.9 | 4.3 | 6.1 | 0.90 | 0.89 |
| Mean | 90.9 | 64.5 | 26.5 | 3.1 | 5.9 | 0.91 | 0.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlando, J.M.; Smith, B.A.; Hafer, J.F.; Paremski, A.; Amodeo, M.; Lobo, M.A.; Prosser, L.A. Physical Activity in Pre-Ambulatory Children with Cerebral Palsy: An Exploratory Validation Study to Distinguish Active vs. Sedentary Time Using Wearable Sensors. Sensors 2025, 25, 1261. https://doi.org/10.3390/s25041261
Orlando JM, Smith BA, Hafer JF, Paremski A, Amodeo M, Lobo MA, Prosser LA. Physical Activity in Pre-Ambulatory Children with Cerebral Palsy: An Exploratory Validation Study to Distinguish Active vs. Sedentary Time Using Wearable Sensors. Sensors. 2025; 25(4):1261. https://doi.org/10.3390/s25041261
Chicago/Turabian StyleOrlando, Julie M., Beth A. Smith, Jocelyn F. Hafer, Athylia Paremski, Matthew Amodeo, Michele A. Lobo, and Laura A. Prosser. 2025. "Physical Activity in Pre-Ambulatory Children with Cerebral Palsy: An Exploratory Validation Study to Distinguish Active vs. Sedentary Time Using Wearable Sensors" Sensors 25, no. 4: 1261. https://doi.org/10.3390/s25041261
APA StyleOrlando, J. M., Smith, B. A., Hafer, J. F., Paremski, A., Amodeo, M., Lobo, M. A., & Prosser, L. A. (2025). Physical Activity in Pre-Ambulatory Children with Cerebral Palsy: An Exploratory Validation Study to Distinguish Active vs. Sedentary Time Using Wearable Sensors. Sensors, 25(4), 1261. https://doi.org/10.3390/s25041261