
Framework Using Multicriteria Analysis for Evaluating the Risk of Musculoskeletal Disorders



Abstract
1. Introduction
2. Materials and Methods
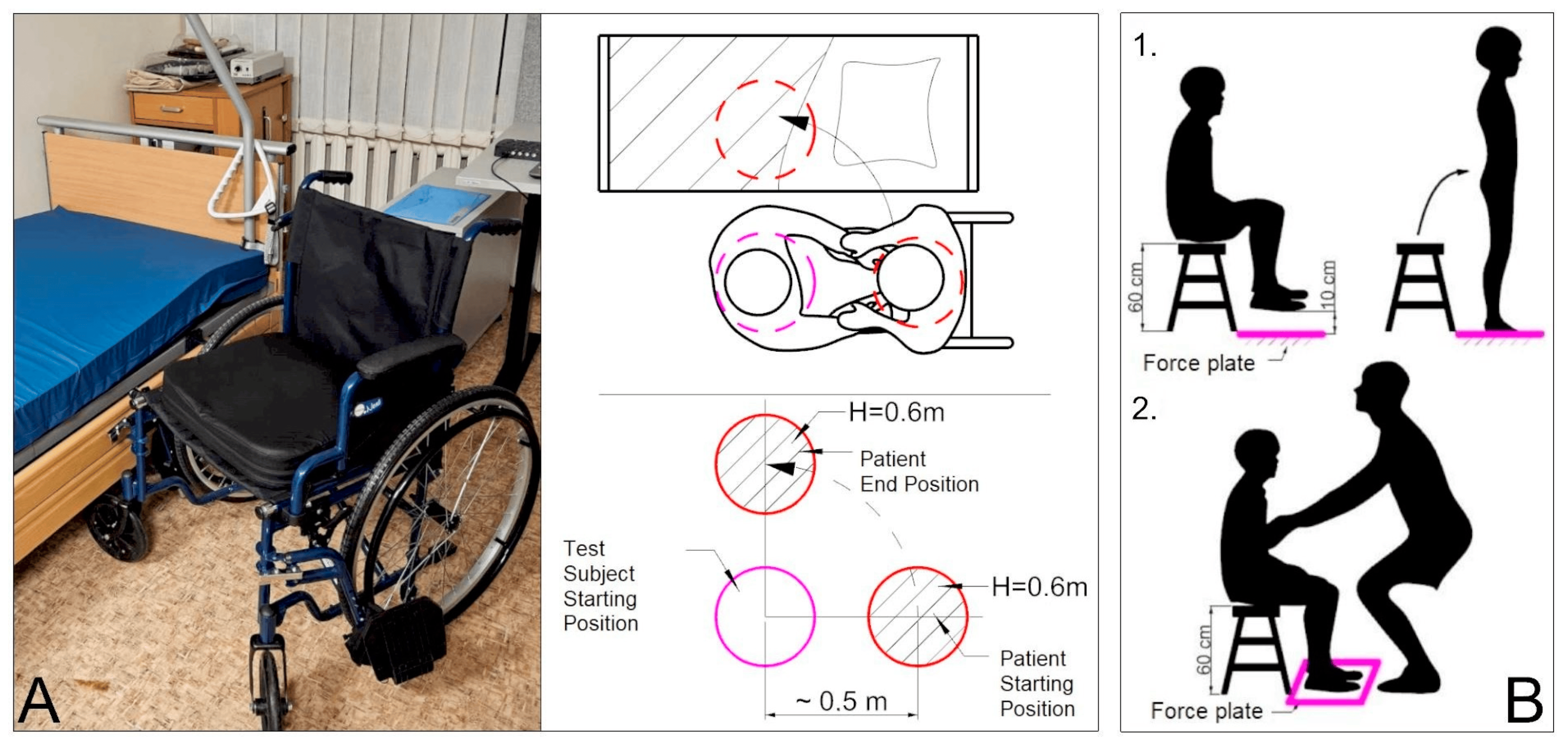
2.1. Research Procedure
2.2. Research Experimental and Statistical Data
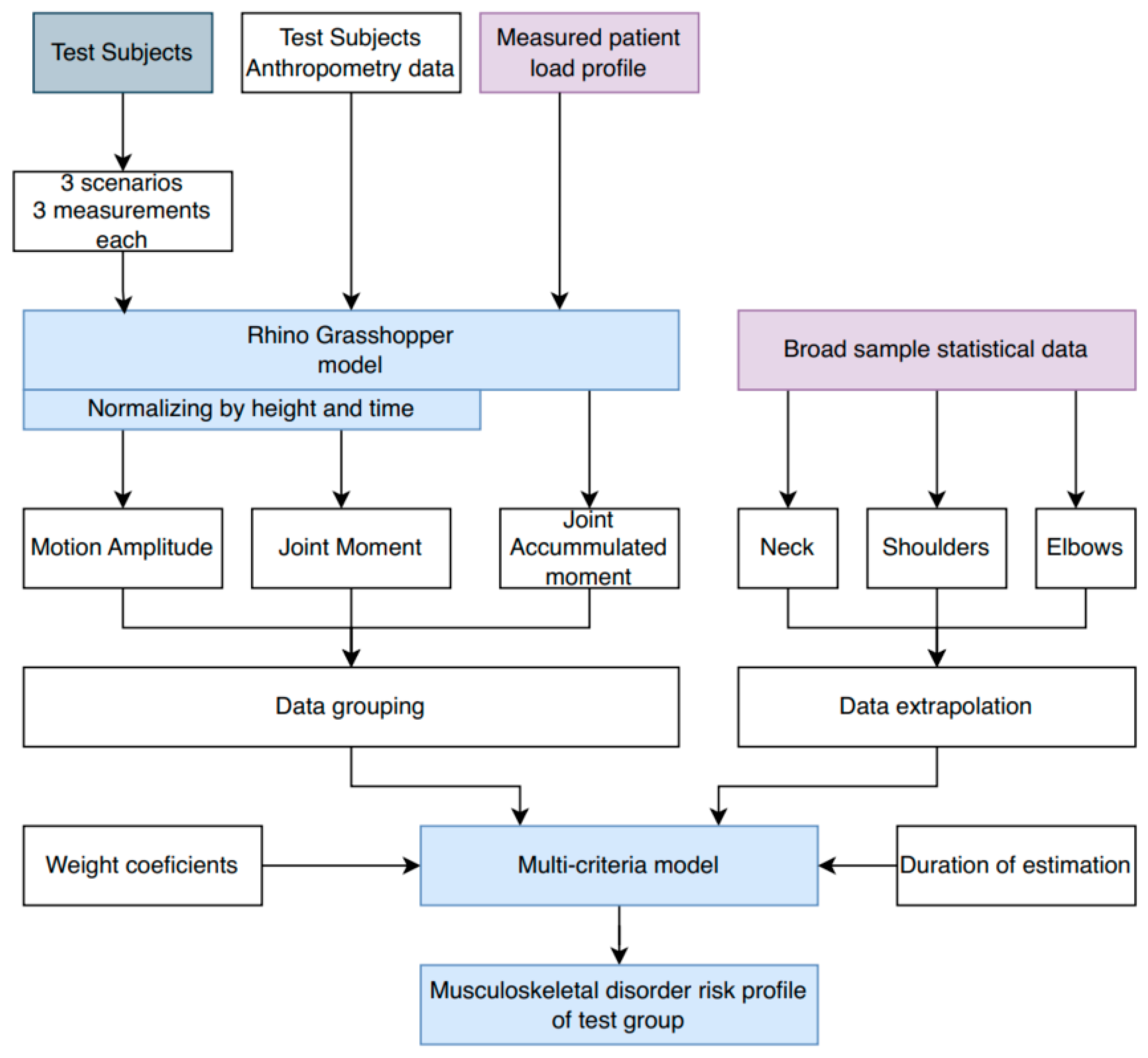
2.3. Matchematical Method
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knudsen, M.L.; Ludewig, P.M.; Braman, J.P. Musculoskeletal pain in resident orthopedic surgeons: Results of a novel survey. Iowa Orthop. J. 2014, 34, 190–196. [Google Scholar]
- Yunus, M.; Jaafar, M.; Mohamed, A.S.A.; Azraai, N. Implementation of Kinetic and Kinematic Variables in Ergonomic Risk Assessment Using Motion Capture Simulation: A Review. Int. J. Environ. Res. Public Health 2021, 18, 8342. [Google Scholar] [CrossRef] [PubMed]
- Czaja, S.J.; Nair, S.N. Human Factors Engineering and Systems Design; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Xiang, X.; Yamada, Y.; Akiyama, Y.; Nakamura, H.; Kudo, N. Effect of Parameters on Lumbar Compressive Force During Patient Transfer. Appl. Sci. 2021, 11, 11622. [Google Scholar] [CrossRef]
- Legal Act of the Republic of Lithuania. Order of the Minister of Social Protection and Labor of the Republic of Lithuania. On the Approval of Methodological Instructions for the Research of Ergonomic Occupational Risk Factors, Original Language Dėl Ergonominių Rizikos Veiksnių Tyrimo Metodinių Nurodymų Patvirtinimo, Valstybės Žinios, 2005-08-06, Nr. 95-3536, Vilnius. Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/TAIS.260443/asr (accessed on 12 January 2025).
- Buckley, J.P.; Hedge, A.; Yates, T.; Copeland, R.J.; Loosemore, M.; Hamer, M.; Bradley, G.; Dunstan, D.W. The sedentary office: An expert statement on the growing case for change towards better health and productivity. Br. J. Sports Med. 2015, 49, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Jokela, M.; Nyberg, S.T.; Singh-Manoux, A.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 2015, 386, 1739–1746. [Google Scholar] [CrossRef]
- Farì, G.; Santagati, D.; Macchiarola, D.; Ricci, V.; Di Paolo, S.; Caforio, L.; Invernizzi, M.; Notarnicola, A.; Megna, M.; Ranieri, M. Musculoskeletal pain related to surfing practice: Which role for sports rehabilitation strategies? A cross-sectional study. J. Back Musculoskelet. Rehabil. 2022, 35, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Sheskin, D.J. Handbook of Parametric and Nonparametric Statistical Procedures, 5th ed.; Chapman and Hall/CRC: New York, NY, USA, 2020. [Google Scholar]
- Senvaitis, K.; Daunoravičienė, K. Skeletal Modeling in Rhino Grasshopper—A Confirmed Kinematic Model. Machines 2023, 11, 556. [Google Scholar] [CrossRef]
- Senvaitis, K.; Adomavičienė, A.; Tomaševič, A.; Kernagytė, R.; Petrauskaitė, A.; Daunoravičienė, K. Ergonomic Assessment of Key Biomechanical Factors in Patient Lifting: Results from a Cross-Sectional Study. Appl. Sci. 2024, 14, 8076. [Google Scholar] [CrossRef]
- Kim, W.; Sung, J.; Saakes, D.; Huang, C.; Xiong, S. Ergonomic postural assessment using a new open-source human pose estimation technology (OpenPose). Int. J. Ind. Ergon. 2021, 84, 103164. [Google Scholar] [CrossRef]
- Senvaitis, K.; Daunoravičienė, K.; Adomavičienė, A. Biomechanical Assessment of Critical Factors during Patient Lifting: Shoulder Girdle and Cumulative Moment Ergonomic Evaluation. Acta Mech. Autom. 2024, 18, 323–332. [Google Scholar] [CrossRef]
- Ribeiro, T.; Serranheira, F.; Loureiro, H. Work-related musculoskeletal disorders in primary health care nurses. Appl. Nurs. Res. 2017, 33, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Anap, D.B.; Iyer, C.; Rao, K. Work-related musculoskeletal disorders among hospital nurses in rural Maharashtra, India: A multi-centre survey. Int. J. Res. Med. Sci. 2017, 1, 101–107. [Google Scholar] [CrossRef]
- Ryu, E.; Ye, B.; Yi, Y.; Kim, J. Risk factors of musculoskeletal symptoms in university hospital nurses. Ann. Occup. Environ. Med. 2014, 26, 47. [Google Scholar] [CrossRef]
- Chung, Y.C.; Hung, C.T.; Li, S.F.; Lee, H.M.; Wang, S.G.; Chang, S.C.; Pai, L.W.; Huang, C.N.; Yang, J.H. Risk of musculoskeletal disorder among Taiwanese nurses cohort: A nationwide population-based study. BMC Musculoskelet. Disord. 2013, 14, 144. [Google Scholar] [CrossRef]
- Arvidsson, I.; Gremark Simonsen, J.; Dahlqvist, C.; Axmon, A.; Karlson, B.; Björk, J.; Nordander, C. Cross-sectional associations between occupational factors and musculoskeletal pain in women teachers, nurses and sonographers. BMC Musculoskelet. Disord. 2016, 17, 35. [Google Scholar] [CrossRef]
- Zheng, M.; Teng, H.; Wang, Y. A simple approach for multi-criteria decision-making on basis of probability theory. Eng. Struct. Technol. 2023, 13, 26–30. [Google Scholar] [CrossRef]
- Tapanya, W.; Puntumetakul, R.; Swangnetr Neubert, M.; Boucaut, R. Influence of neck flexion angle on gravitational moment and neck muscle activity when using a smartphone while standing. Ergonomics 2021, 64, 900–911. [Google Scholar] [CrossRef]
- Kleijnen, J.P. Validation of Models: Statistical Techniques and Data Availability. In Proceedings of the 31st Conference on Winter Simulation: Simulation—A Bridge to the Future, Phoenix, AZ, USA, 5–8 December 1999. [Google Scholar] [CrossRef]
- Luger, T.; Maher, G.C.H.; Rieger, A.M.; Steinhilber, B. Work-break schedules for preventing musculoskeletal symptoms and disorders in healthy workers. Cochrane Database Syst. Rev. 2019, 7, CD012886. [Google Scholar] [CrossRef]
- Sasikumar, V.; Binoosh, S.C.A.B. A model for predicting the risk of musculoskeletal disorders among computer professionals. Int. J. Occup. Saf. Ergon. 2020, 26, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Darvishi, E.; Ghasemi, F.; Sadeghi, F.; Abedi, K.; Rahmati, S.; Sadeghzade, G. Risk assessment of the work-related musculoskeletal disorders based on individual characteristics using path analysis models. BMC Musculoskelet. Disord. 2022, 23, 616. [Google Scholar] [CrossRef]
- Das, S.K.; Patyal, V.S.; Ambekar, S. Modeling of risk factors leading to work related musculoskeletal disorders in medical practitioners. Saf. Sci. 2024, 172, 106427. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
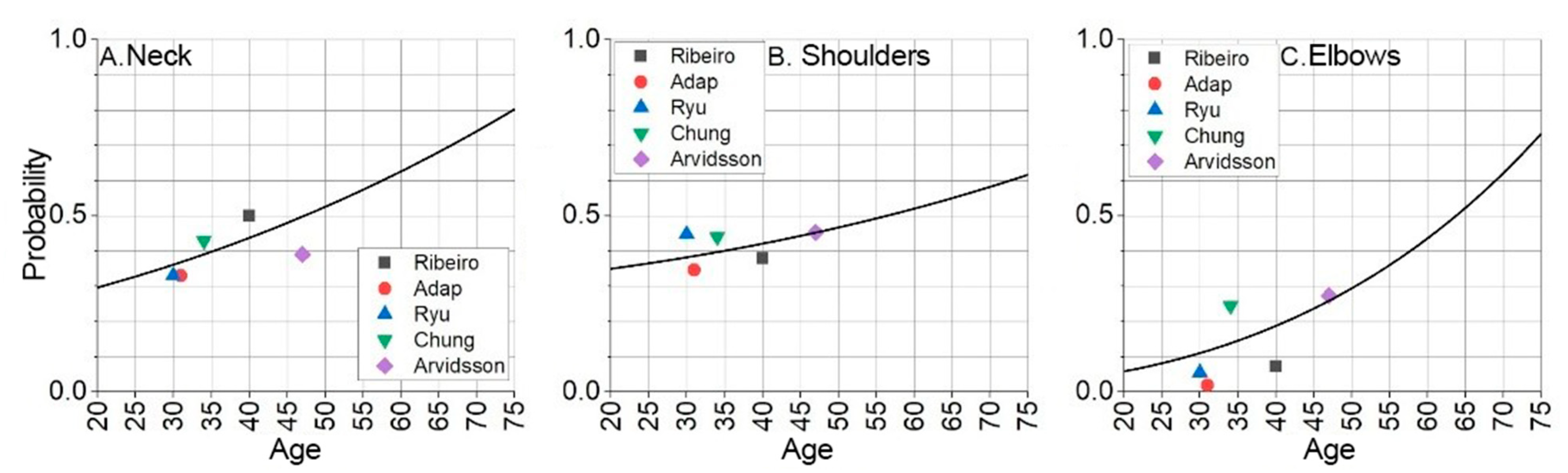
| Reference | Ribeiro et al., 2016 [14] | Adap et al., 2017 [15] | Ryu et al., 2014 [16] | Chung et al., 2013 [17] | Arvidsson et al., 2016 [18] |
|---|---|---|---|---|---|
| Research Country | Portugal | India | USA | Taiwan | Sweden |
| Sample Size | 409 | 212 | 531 | 1914 | 925 |
| Sample average age (±SD) | 40 ± 9 | 31 ± 6 | 30 ± 7 | 34 ± 8 | 47 ± 10 |
| Base risk of musculoskeletal disorder | |||||
| Neck | 0.501 | 0.331 | 0.333 | 0.434 | 0.390 |
| Shoulders | 0.378 | 0.346 | 0.448 | 0.440 | 0.453 |
| Elbows | 0.072 | 0.019 | 0.055 | 0.245 | 0.273 |
| Criteria | Physical Readiness | Sex | Technique Scenario | Amplitude | Moment | Cumulative Moment | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Weight score (B) | 1 | 1 | 1 | 1 | 1 | 2 | ||||
| Weight coefficient (q) | 0.143 | 0.143 | 0.143 | 0.143 | 0.143 | 0.285 | ||||
| Element title | Low | Medium | High | Male | Female | w/o Belt | w Belt | — | — | — |
| Element likelihood (a) | 1.018 | 0.901 | 0.161 | 1.120 | 0.930 | 0.952 | 1.024 | — | — | — |
| Element factor (X) | 0.146 | 0.129 | 0.023 | 0.160 | 0.133 | 0.136 | 0.146 | a · q | a · q | a · q |
| Criteria | Physical Readiness | Sex | Technique Scenario | Symmetry | Amplitude | Moment | Cumulative Moment | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight score (B) | 1 | 1 | 1 | 2 | 1 | 1 | 2 | |||||
| Weight coefficient (q) | 0.111 | 0.111 | 0.111 | 0.222 | 0.111 | 0.111 | 0.223 | |||||
| Element title | Low | Medium | High | Male | Female | w/o Belt | w Belt | Left | Right | — | — | — |
| Element likelihood (a) | 1.009 | 0.997 | 1.030 | 1.016 | 0.991 | 0.919 | 1.041 | 1.009 | 0.998 | — | — | — |
| Element factor (X) | 0.112 | 0.110 | 0.114 | 0.113 | 0.110 | 0.102 | 0.116 | 0.224 | 0.222 | a · q | a · q | a · q |
| Criteria | Physical Readiness | Sex | Technique Scenario | Symmetry | Amplitude | Moment | Cumulative Moment | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight score (B) | 1 | 1 | 1 | 2 | 1 | 1 | 2 | |||||
| Weight coefficient (q) | 0.111 | 0.111 | 0.111 | 0.222 | 0.111 | 0.111 | 0.222 | |||||
| Element title | Low | Medium | High | Male | Female | w/o Belt | w Belt | Left | Right | — | — | — |
| Element likelihood (a) | 1.008 | 0.998 | 1.029 | 1.019 | 0.989 | 0.976 | 1.017 | 1.005 | 0.999 | — | — | — |
| Element factor (X) | 0.112 | 0.109 | 0.114 | 0.114 | 0.110 | 0.108 | 0.113 | 0.223 | 0.222 | a · q | a · q | a · q |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senvaitis, K.; Adomavičienė, A.; Daunoravičienė, K. Framework Using Multicriteria Analysis for Evaluating the Risk of Musculoskeletal Disorders. Sensors 2025, 25, 444. https://doi.org/10.3390/s25020444
Senvaitis K, Adomavičienė A, Daunoravičienė K. Framework Using Multicriteria Analysis for Evaluating the Risk of Musculoskeletal Disorders. Sensors. 2025; 25(2):444. https://doi.org/10.3390/s25020444
Chicago/Turabian StyleSenvaitis, Karolis, Aušra Adomavičienė, and Kristina Daunoravičienė. 2025. "Framework Using Multicriteria Analysis for Evaluating the Risk of Musculoskeletal Disorders" Sensors 25, no. 2: 444. https://doi.org/10.3390/s25020444
APA StyleSenvaitis, K., Adomavičienė, A., & Daunoravičienė, K. (2025). Framework Using Multicriteria Analysis for Evaluating the Risk of Musculoskeletal Disorders. Sensors, 25(2), 444. https://doi.org/10.3390/s25020444