
Thermography Sensor to Assess Motor and Sensitive Neuromuscular Sequels of Brain Damage


Abstract
1. Introduction
2. Methodology
2.1. Study Design
2.2. Participants
2.3. Procedures
2.4. Familiarization and Clinical Exam
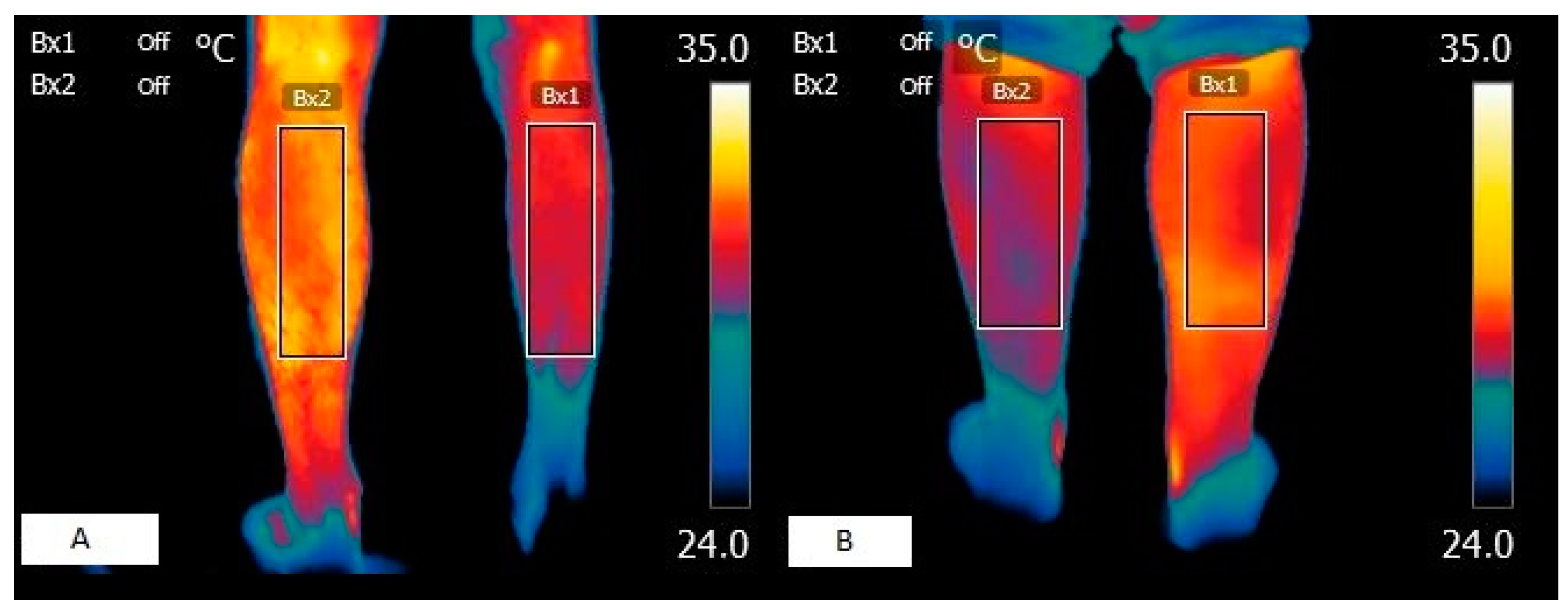
2.5. Thermography
2.6. Statistical Analysis
3. Results
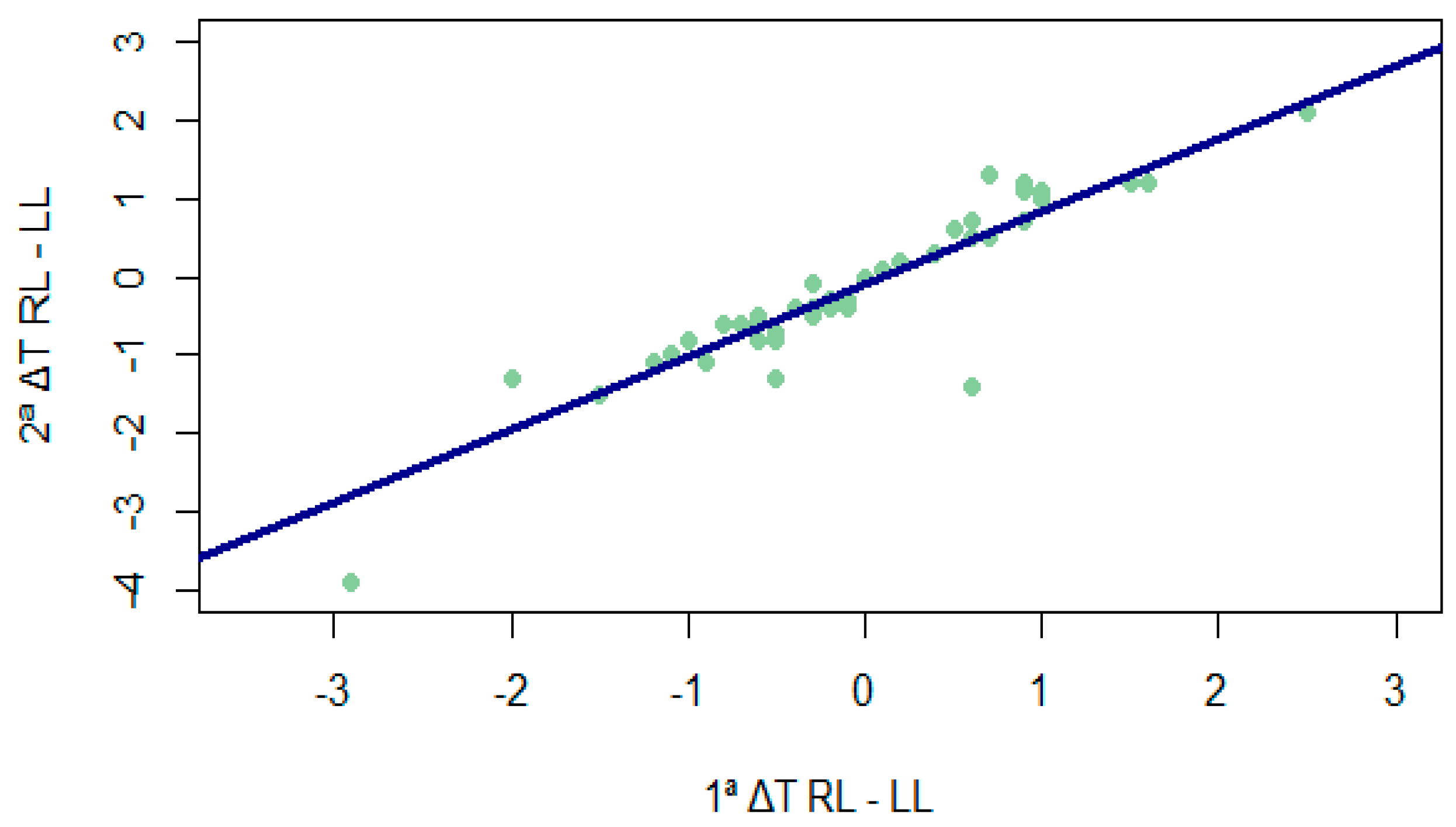
3.1. Concurrent Validity of Thermography, Diagnostic Capacity, and Reliability of Thermography
3.1.1. Significant and Descriptive Inferiority of all Temperatures with Respect to 32 °C
3.1.2. Differences between Times of Temperature Differences between Legs
3.1.3. Temperature Differences between Times for Each Leg
3.2. Convergent Validity with Other Instruments
3.2.1. Relationship between Temperature and Ashworth Scale
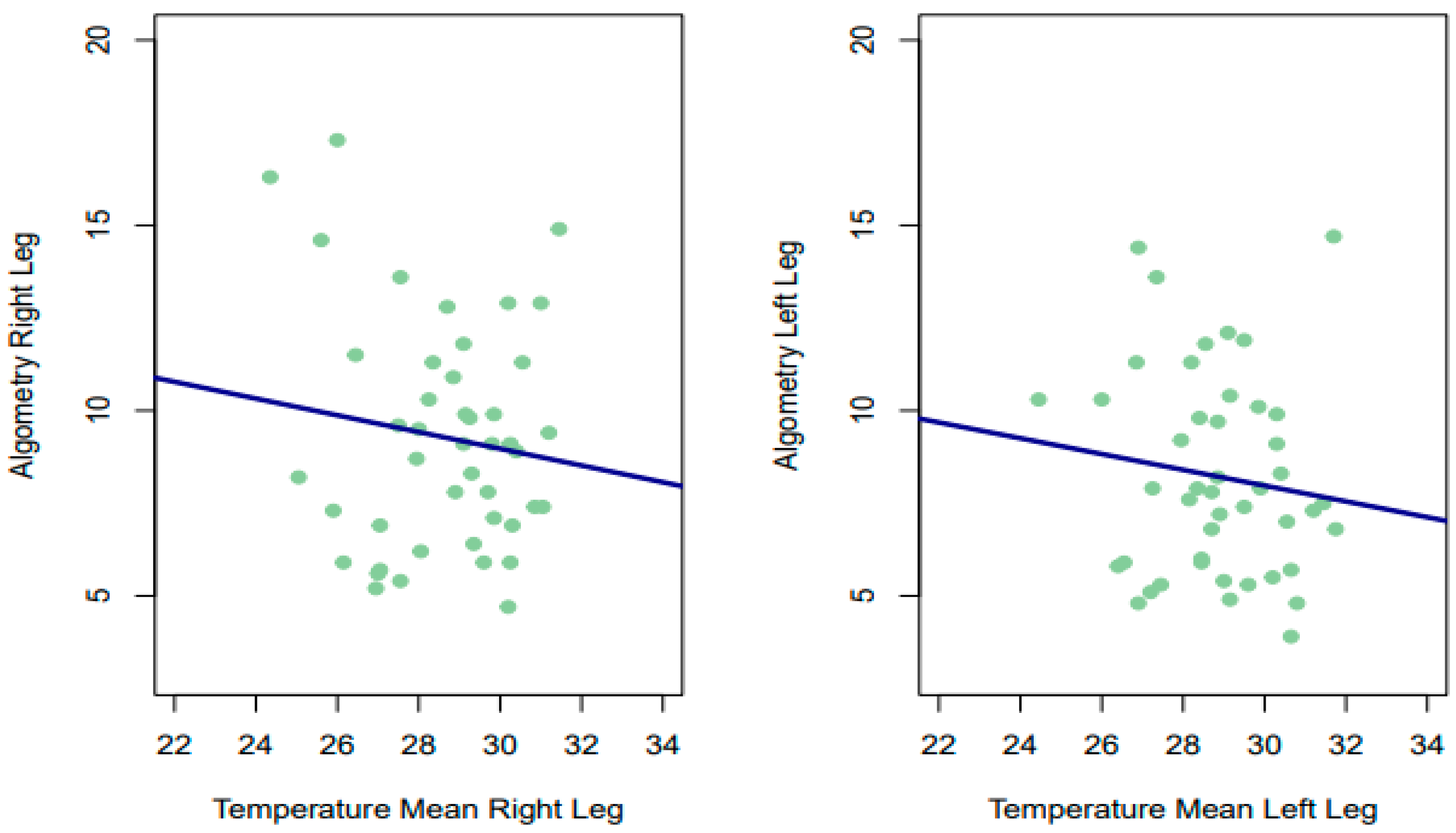
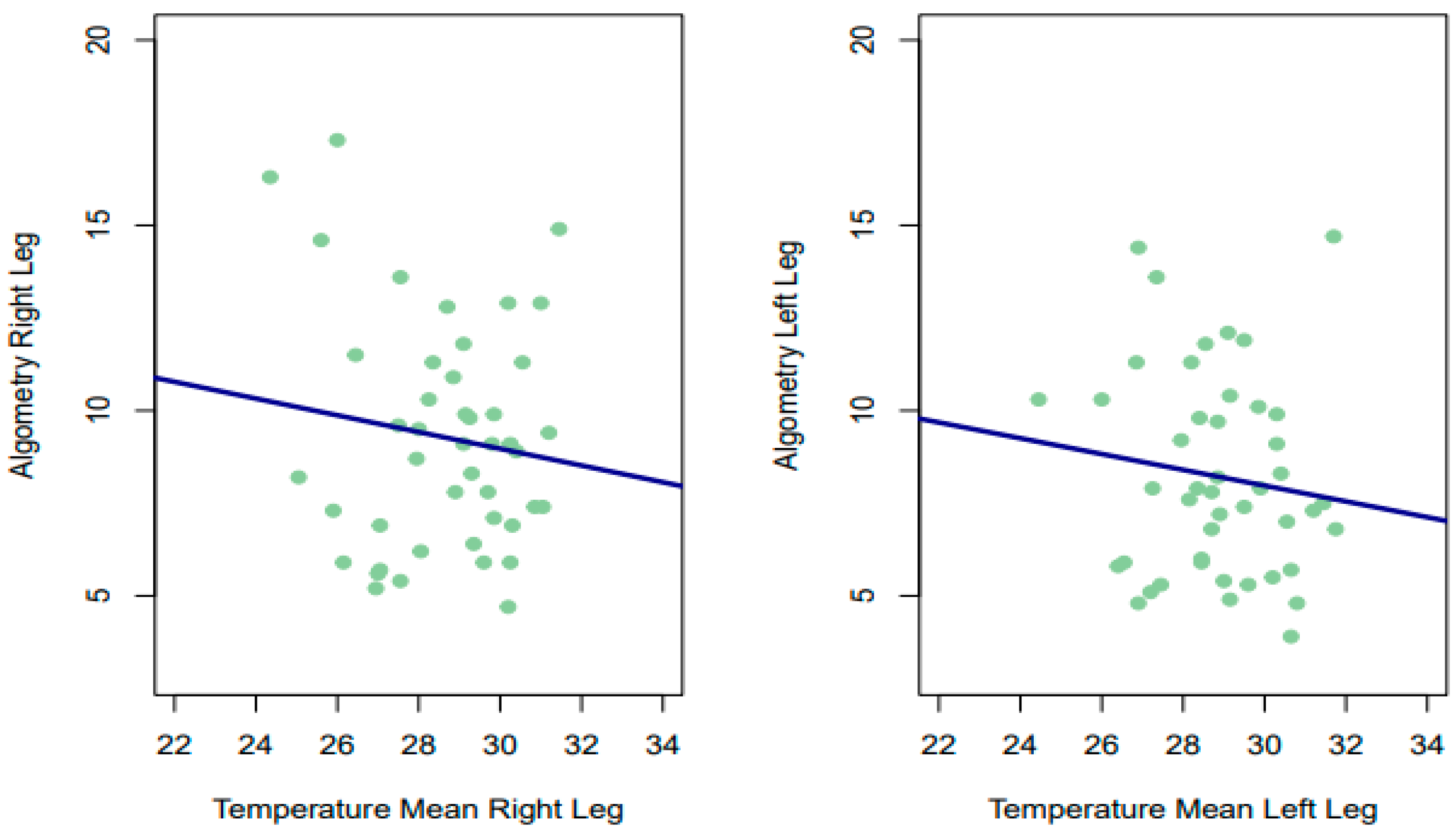
3.2.2. Relationship between Temperature and PPT
4. Discussion
4.1. Thermographic Validity, Diagnostic Capacity, and Reliability
4.2. Thermography Validity in Relation to Motor Ability
4.3. Thermography Validity in Relation to Sensitive Ability
5. Conclusions
6. Limitation of the Study
7. Future Direction
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATM | Atmosphere |
| BMI | Body mass index |
| DITI | Digital infrared thermal imaging |
| ΔT | Difference of temperature |
| HYP | Hypotonia |
| ICC | Interclass correlation coefficient |
| LH | Left hemiplegia |
| LL | Left leg |
| MAS | Modified Ashworth scale |
| MRI | Magnetic resonance Imaging |
| PMI | Psycomotor impairment |
| PPT | Pressure pain threshold |
| RL | Right leg |
| RH | Right hemiplegia |
| ROI | Region of interest |
| SD | Spastic diplegia |
| TE | Tetraplegia |
| T1 | Time 1 of measurement |
| T2 | Time 2 of measurement |
| TISEM | Thermographic imaging in sports and exercise medicine |
References
- Ring, E.F.J.; Ammer, K. Infrared Thermal Imaging in Medicine. Physiol. Meas. 2012, 33, R33–R46. [Google Scholar] [CrossRef]
- Wu, T.; Luo, Y.; Wei, L. Mid-Infrared Sensing of Molecular Vibrational Modes with Tunable Graphene Plasmons. Opt. Lett. 2017, 42, 2066–2069. [Google Scholar] [CrossRef] [PubMed]
- Ring, E.F. Quantitative Thermal Imaging. Clin. Phys. Physiol. Meas. 1990, 11, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Amson, H.; Vacheron, C.-H.; Thiolliere, F.; Piriou, V.; Magnin, M.; Allaouchiche, B. Core-to-Skin Temperature Gradient Measured by Thermography Predicts Day-8 Mortality in Septic Shock: A Prospective Observational Study. J. Crit. Care 2020, 60, 294–299. [Google Scholar] [CrossRef]
- Magalhaes, C.; Vardasca, R.; Mendes, J. Recent Use of Medical Infrared Thermography in Skin Neoplasms. Skin Res. Technol. 2018, 24, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.D.; Leggett, S.A.; Marjanovic, E.J.; Moore, T.L.; Allen, J.; Anderson, M.E.; Britton, J.; Buch, M.H.; Del Galdo, F.; Denton, C.P.; et al. A Multicenter Study of the Validity and Reliability of Responses to Hand Cold Challenge as Measured by Laser Speckle Contrast Imaging and Thermography: Outcome Measures for Systemic Sclerosis-Related Raynaud’s Phenomenon. Arthritis Rheumatol. 2018, 70, 903–911. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Berentson-Shaw, J. Thermography as a Screening and Diagnostic Tool: A Systematic Review. N. Z. Med. J. 2012, 125, 80–91. [Google Scholar]
- Ring, E.F.J. The Historical Development of Thermometry and Thermal Imaging in Medicine. J. Med. Eng. Technol. 2006, 30, 192–198. [Google Scholar] [CrossRef]
- Tattersall, G.J. Infrared Thermography: A Non-Invasive Window into Thermal Physiology. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2016, 202, 78–98. [Google Scholar] [CrossRef]
- Tansey, E.A.; Johnson, C.D. Recent Advances in Thermoregulation. Adv. Physiol. Educ. 2015, 39, 139–148. [Google Scholar] [CrossRef]
- Rustemeyer, J.; Radtke, J.; Bremerich, A. Thermography and Thermoregulation of the Face. Head Face Med. 2007, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Sanz, D.; Losa-Iglesias, M.E.; Becerro-de-Bengoa-Vallejo, R.; Dorgham, H.A.A.; Benito-de-Pedro, M.; San-Antolín, M.; Mazoteras-Pardo, V.; Calvo-Lobo, C. Thermography Related to Electromyography in Runners with Functional Equinus Condition after Running. Phys. Ther. Sport 2019, 40, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Anzengruber, F.; Alotaibi, F.; Kaufmann, L.S.; Ghosh, A.; Oswald, M.R.; Maul, J.-T.; Meier, B.; French, L.E.; Bonmarin, M.; Navarini, A.A. Thermography: High Sensitivity and Specificity Diagnosing Contact Dermatitis in Patch Testing. Allergol. Int. 2019, 68, 254–258. [Google Scholar] [CrossRef]
- Modrzejewska, A.; Cieszyński, Ł.; Zaborski, D.; Parafiniuk, M. Thermography in Clinical Ophthalmic Oncology. Arq. Bras. Oftalmol. 2021, 84, 22–30. [Google Scholar]
- Tan, Y.K.; Hong, C.; Li, H.; Allen, J.C.; Thumboo, J. Thermography in Rheumatoid Arthritis: A Comparison with Ultrasonography and Clinical Joint Assessment. Clin. Radiol. 2020, 75, 963.e17–963.e22. [Google Scholar] [CrossRef]
- da Silva Dias, C.; Alfieri, F.M.; Dos Santos, A.C.A.; Battistella, L.R. Body Temperature and Esthesia in Individuals with Stroke. Sci. Rep. 2021, 11, 10106. [Google Scholar] [CrossRef]
- Hegedűs, B. The Potential Role of Thermography in Determining the Efficacy of Stroke Rehabilitation. J. Stroke Cerebrovasc. Dis. 2018, 27, 309–314. [Google Scholar] [CrossRef]
- Cabizosu, A.; Carboni, N.; Figus, A.; Vegara-Meseguer, J.M.; Casu, G.; Hernández Jiménez, P.; Martinez-Almagro Andreo, A. Is Infrared Thermography (IRT) a Possible Tool for the Evaluation and Follow up of Emery-Dreifuss Muscular Dystrophy? A Preliminary Study. Med. Hypotheses 2019, 127, 91–96. [Google Scholar] [CrossRef]
- Cabizosu, A.; Carboni, N.; Martínez-Almagro Andreo, A.; Casu, G.; Ramón Sánchez, C.; Vegara-Meseguer, J.M. Relationship between Infrared Skin Radiation and Muscular Strength Tests in Patients Affected by Emery-Dreifuss Muscular Dystrophy. Med. Hypotheses 2020, 138, 109592. [Google Scholar] [CrossRef]
- de Freitas Zanona, A.; de Souza, R.F.; Aidar, F.J.; de Matos, D.G.; Santos, K.M.B.; da Conceição Paixão, M.; Sampaio, P.Y.S.; Almeida Junior, H.; Monte-Silva, K.K. Use of Virtual Rehabilitation to Improve the Symmetry of Body Temperature, Balance, and Functionality of Patients with Stroke Sequelae. Ann. Neurosci. 2019, 25, 166–173. [Google Scholar] [CrossRef]
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S. Stroke: A Global Response Is Needed. Bull. World Health Organ 2016, 94, 634–634A. [Google Scholar] [CrossRef]
- GBD 2016 Neurology Collaborators Global, Regional, and National Burden of Neurological Disorders, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [CrossRef]
- Moreira, D.G.; Costello, J.T.; Brito, C.J.; Adamczyk, J.G.; Ammer, K.; Bach, A.J.E.; Costa, C.M.A.; Eglin, C.; Fernandes, A.A.; Fernández-Cuevas, I.; et al. Thermographic Imaging in Sports and Exercise Medicine: A Delphi Study and Consensus Statement on the Measurement of Human Skin Temperature. J. Therm. Biol. 2017, 69, 155–162. [Google Scholar] [CrossRef]
- Cabizosu, A.; Grotto, D.; Lopez Esteban, M.J.; Castañeda Vozmediano, R. The assessment of neuromuscular sequels post brain damage by thermography. A pilot study. Cuest. Fisioter. 2024, 53, 93–106. [Google Scholar]
- Harb, A.; Kishner, S. Modified Ashworth Scale. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Barbachan Mansur, N.S.; Pereira, V.F.; Cunha, H.C.M.; Nunes, C.G.; Ferreira, D.S.; Sato, V.N.; Yamada, A.F.; Matsunaga, F.T.; Belloti, J.C.; Tamaoki, M.J.S. Diagnosis of Achilles Insertional Tendinopathies by Algometry. Pain Med. 2021, 22, 2670–2675. [Google Scholar] [CrossRef]
- Avellanal, M.; Riquelme, I.; Díaz-Regañón, G. Quantitative Sensory Testing in Pain Assesment and Treatment. Brief Review and Algorithmic Management Proposal. Rev. Esp. Anestesiol. Reanim. 2020, 67, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M.; Stanley, S.A.; Whitman, Z.; Wenn, V.; Coats, T.J.; Sims, M.; Thompson, J.P. The Effect of Constitutive Pigmentation on the Measured Emissivity of Human Skin. PLoS ONE 2020, 15, e0241843. [Google Scholar] [CrossRef]
- Bouzas Marins, J.C.; de Andrade Fernandes, A.; Gomes Moreira, D.; Souza Silva, F.; Magno, A.; Costa, C.; Pimenta, E.M.; Sillero-Quintana, M. Thermographic profile of soccer players’ lower limbs. Rev. Andal. Med. Deporte 2014, 7, 1–6. [Google Scholar] [CrossRef]
- FLIR Systems|Sistemas de Cámaras Termográficas, de Visión Nocturna e Infrarrojas|Teledyne FLIR. Available online: https://www.flir.es/ (accessed on 23 October 2023).
- Côrte, A.C.; Pedrinelli, A.; Marttos, A.; Souza, I.F.G.; Grava, J.; José Hernandez, A. Infrared Thermography Study as a Complementary Method of Screening and Prevention of Muscle Injuries: Pilot Study. BMJ Open Sport Exerc. Med. 2019, 5, e000431. [Google Scholar] [CrossRef]
- Carrière, M.E.; de Haas, L.E.M.; Pijpe, A.; Meij-de Vries, A.; Gardien, K.L.M.; van Zuijlen, P.P.M.; Jaspers, M.E.H. Validity of Thermography for Measuring Burn Wound Healing Potential. Wound Repair. Regen. 2020, 28, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Reprint; Psychology Press: New York, NY, USA, 2009; ISBN 978-0-8058-0283-2. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropract. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Kolosovas-Machuca, E.S.; González, F.J. Distribution of Skin Temperature in Mexican Children. Skin Res. Technol. 2011, 17, 326–331. [Google Scholar] [CrossRef]
- Sousa, N.T.A.D.; Guirro, E.C.D.O.; Calió, J.G.; Queluz, M.C.D.; Guirro, R.R.D.J. Application of Shortwave Diathermy to Lower Limb Increases Arterial Blood Flow Velocity and Skin Temperature in Women: A Randomized Controlled Trial. Braz. J. Phys. Ther. 2017, 21, 127–137. [Google Scholar] [CrossRef]
- Nowak, I.; Mraz, M.; Mraz, M. Thermography Assessment of Spastic Lower Limb in Patients after Cerebral Stroke Undergoing Rehabilitation. J. Therm. Anal. Calorim. 2020, 140, 755–762. [Google Scholar] [CrossRef]
- Alfieri, F.M.; Battistella, L.R. Body Temperature of Healthy Men Evaluated by Thermography: A Study of Reproducibility. Technol. Health Care 2018, 26, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Noguera, F.J.; Cabizosu, A.; Marín-Pagán, C.; Alcaraz, P.E. Body Surface Profile in Ambient and Hot Temperatures during a Rectangular Test in Race Walker Champions of the World Cup in Oman 2022. J. Therm. Biol. 2023, 114, 103548. [Google Scholar] [CrossRef]
- Ekhart, D.; Wicht, H.; Kersken, T.; Ackermann, H.; Kaczmarczyk, M.; Pretzsch, G.; Alexander, H.; Korf, H.W. Dynamics of Core Body Temperature Cycles in Long-Term Measurements under Real Life Conditions in Women. Chronobiol. Int. 2018, 35, 8–23. [Google Scholar] [CrossRef]
- Harding, C.; Pompei, F.; Bordonaro, S.F.; McGillicuddy, D.C.; Burmistrov, D.; Sanchez, L.D. The Daily, Weekly, and Seasonal Cycles of Body Temperature Analyzed at Large Scale. Chronobiol. Int. 2019, 36, 1646–1657. [Google Scholar] [CrossRef]
- Uematsu, S.; Edwin, D.H.; Jankel, W.R.; Kozikowski, J.; Trattner, M. Quantification of Thermal Asymmetry. Part 1: Normal Values and Reproducibility. J. Neurosurg. 1988, 69, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Cabizosu, A.; Berenguer-Vidal, R.; Vegara-Meseguer, J.M.; Martínez-Almagro Andreo, A.; Maiquez Mojica, V.; Casu, G.; Carboni, N. Relationship between Infrared Skin Radiation and Functional Tests in Patients Affected by Emery-Dreifuss Muscular Dystrophy: Part 2. Med. Hypotheses 2021, 146, 110348. [Google Scholar] [CrossRef]
- Zhu, C.; Qiu, L.; Sun, W.; Yang, C.; Cong, D.; Wang, Y.; Ji, G. Effect of TCM Rehabilitation Program on Activities of Daily Living in Patients with Post-Stroke Limb Spasticity: An Observational Study. Medicine 2023, 102, e36079. [Google Scholar] [CrossRef]
- Finegan, E.; Li Hi Shing, S.; Siah, W.F.; Chipika, R.H.; Chang, K.M.; McKenna, M.C.; Doherty, M.A.; Hengeveld, J.C.; Vajda, A.; Donaghy, C.; et al. Evolving Diagnostic Criteria in Primary Lateral Sclerosis: The Clinical and Radiological Basis of “Probable PLS”. J. Neurol. Sci. 2020, 417, 117052. [Google Scholar] [CrossRef]
- Kim, M.S.; Seo, D.H.; Lim, M.H.; Kim, T.U.; Lee, S.J.; Hyun, J.K. Skin Temperature Changes Following Sciatic Nerve Injury in Rats. J. Neurotrauma 2012, 29, 2738–2747. [Google Scholar] [CrossRef]
- Ra, J.Y.; An, S.; Lee, G.-H.; Kim, T.U.; Lee, S.J.; Hyun, J.K. Skin Temperature Changes in Patients with Unilateral Lumbosacral Radiculopathy. Ann. Rehabil. Med. 2013, 37, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Wagatsuma, A.; Osawa, T. Time Course of Changes in Angiogenesis-Related Factors in Denervated Muscle. Acta Physiol. 2006, 187, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Whitney, D.G.; Singh, H.; Miller, F.; Barbe, M.F.; Slade, J.M.; Pohlig, R.T.; Modlesky, C.M. Cortical Bone Deficit and Fat Infiltration of Bone Marrow and Skeletal Muscle in Ambulatory Children with Mild Spastic Cerebral Palsy. Bone 2017, 94, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Gomes, G.G.C.; Palinkas, M.; da Silva, G.P.; Gonçalves, C.R.; Lopes, R.F.T.; Verri, E.D.; Fabrin, S.C.V.; Fioco, E.M.; Siéssere, S.; Regalo, S.C.H. Bite Force, Thickness, and Thermographic Patterns of Masticatory Muscles Post-Hemorrhagic Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106173. [Google Scholar] [CrossRef] [PubMed]
- Candelario-Jalil, E.; Dijkhuizen, R.M.; Magnus, T. Neuroinflammation, Stroke, Blood-Brain Barrier Dysfunction, and Imaging Modalities. Stroke 2022, 53, 1473–1486. [Google Scholar] [CrossRef]
- Karaszewski, B.; Carpenter, T.K.; Thomas, R.G.R.; Armitage, P.A.; Lymer, G.K.S.; Marshall, I.; Dennis, M.S.; Wardlaw, J.M. Relationships between Brain and Body Temperature, Clinical and Imaging Outcomes after Ischemic Stroke. J. Cereb. Blood Flow Metab. 2013, 33, 1083–1089. [Google Scholar] [CrossRef]
- Naito, E.; Nakashima, T.; Kito, T.; Aramaki, Y.; Okada, T.; Sadato, N. Human Limb-Specific and Non-Limb-Specific Brain Representations during Kinesthetic Illusory Movements of the Upper and Lower Extremities. Eur. J. Neurosci. 2007, 25, 3476–3487. [Google Scholar] [CrossRef]
- Pontén, E.M.; Stål, P.S. Decreased Capillarization and a Shift to Fast Myosin Heavy Chain IIx in the Biceps Brachii Muscle from Young Adults with Spastic Paresis. J. Neurol. Sci. 2007, 253, 25–33. [Google Scholar] [CrossRef]
- Salom-Moreno, J.; Sánchez-Mila, Z.; Ortega-Santiago, R.; Palacios-Ceña, M.; Truyol-Domínguez, S.; Fernández-de-las-Peñas, C. Changes in Spasticity, Widespread Pressure Pain Sensitivity, and Baropodometry after the Application of Dry Needling in Patients Who Have Had a Stroke: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2014, 37, 569–579. [Google Scholar] [CrossRef]
- Dibai Filho, A.V.; de Oliveira, A.K.; Oliveira, M.P.; Bevilaqua-Grossi, D.; de Jesus Guirro, R.R. Relationship between Pressure and Thermal Pain Threshold, Pain Intensity, Catastrophizing, Disability, and Skin Temperature over Myofascial Trigger Point in Individuals with Neck Pain. Rev. Assoc. Med. Bras. 2021, 67, 1798–1803. [Google Scholar] [CrossRef]
- Alfieri, F.M.; Lima, A.R.S.; Battistella, L.R.; de Oliveira Vargas e Silva, N.C. Superficial Temperature and Pain Tolerance in Patients with Chronic Low Back Pain. J. Bodyw. Mov. Ther. 2019, 23, 583–587. [Google Scholar] [CrossRef]
- Haddad, D.S.; Brioschi, M.L.; Arita, E.S. Thermographic and Clinical Correlation of Myofascial Trigger Points in the Masticatory Muscles. Dentomaxillofac. Radiol. 2012, 41, 621–629. [Google Scholar] [CrossRef]
- Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Inglés, M.; Izquierdo-Alventosa, R.; Serra-Añó, P. Thermal Imaging Ruled out as a Supplementary Assessment in Patients with Fibromyalgia: A Cross-Sectional Study. PLoS ONE 2021, 16, e0253281. [Google Scholar] [CrossRef]
- Zhang, Y.-H.; Xu, H.-R.; Wang, Y.-C.; Hu, G.-W.; Ding, X.-Q.; Shen, X.-H.; Yang, H.; Rong, J.-F.; Wang, X.-Q. Pressure Pain Threshold and Somatosensory Abnormalities in Different Ages and Functional Conditions of Post-Stroke Elderly. BMC Geriatrics 2022, 22, 830. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N = 45) |
|---|---|
| Sex | |
| Woman | 24 (53.4%) |
| Man | 21 (46.6%) |
| Age | |
| Mean ± SD | 33.8 ± 7.4 |
| IMC | |
| Mean ± SD | 26.5 ± 5.3 |
| Right MAS | |
| Mean ± SD | 1.4 ± 1.2 |
| Left MAS | |
| Mean ± SD | 1.2 ± 1.2 |
| Right PPT | |
| Mean ± SD | 9.3 ± 3.1 |
| Left PPT | |
| Mean ± SD | 8.2 ± 2.7 |
| RL1° | LL 1° | RL 2° | LL 2° | |
|---|---|---|---|---|
| N = 45 | N = 42 a | N = 38 b | N = 42 a | N = 38 b |
| Mean ± SD | 29.1 ± 1.8 | 29.1 ± 1.5 | 28.2 ± 2.2 | 28.3 ± 2.1 |
| Median IQR [25–75%] | 29.4 [28.3–30.4] | 29.1 [28.0–30.4] | 28.8 [26.0–29.8] | 28.7 [26.3–29.8] |
| Range | 23.9, 31.4 | 24.5, 31.6 | 23.9, 31.5 | 24.3, 32.3 |
| p value | <0.001 * | <0.001 ** | <0.001 * | <0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabizosu, A.; Grotto, D.; López López, A.; Castañeda Vozmediano, R. Thermography Sensor to Assess Motor and Sensitive Neuromuscular Sequels of Brain Damage. Sensors 2024, 24, 1723. https://doi.org/10.3390/s24061723
Cabizosu A, Grotto D, López López A, Castañeda Vozmediano R. Thermography Sensor to Assess Motor and Sensitive Neuromuscular Sequels of Brain Damage. Sensors. 2024; 24(6):1723. https://doi.org/10.3390/s24061723
Chicago/Turabian StyleCabizosu, Alessio, Daniele Grotto, Alberto López López, and Raúl Castañeda Vozmediano. 2024. "Thermography Sensor to Assess Motor and Sensitive Neuromuscular Sequels of Brain Damage" Sensors 24, no. 6: 1723. https://doi.org/10.3390/s24061723
APA StyleCabizosu, A., Grotto, D., López López, A., & Castañeda Vozmediano, R. (2024). Thermography Sensor to Assess Motor and Sensitive Neuromuscular Sequels of Brain Damage. Sensors, 24(6), 1723. https://doi.org/10.3390/s24061723