
Recent Advances in Biosensors for Diagnosis of Autoimmune Diseases



Abstract
1. Introduction
2. Autoimmune Diseases and Their Biomarkers
2.1. Celiac Disease
2.2. Multiple Sclerosis
2.3. Rheumatoid Arthritis
2.4. Psoriatic Arthritis
2.5. Systemic Lupus Erythematosus
2.6. Clinical Concentrations of Some AD Biomarkers
2.7. Other Diseases
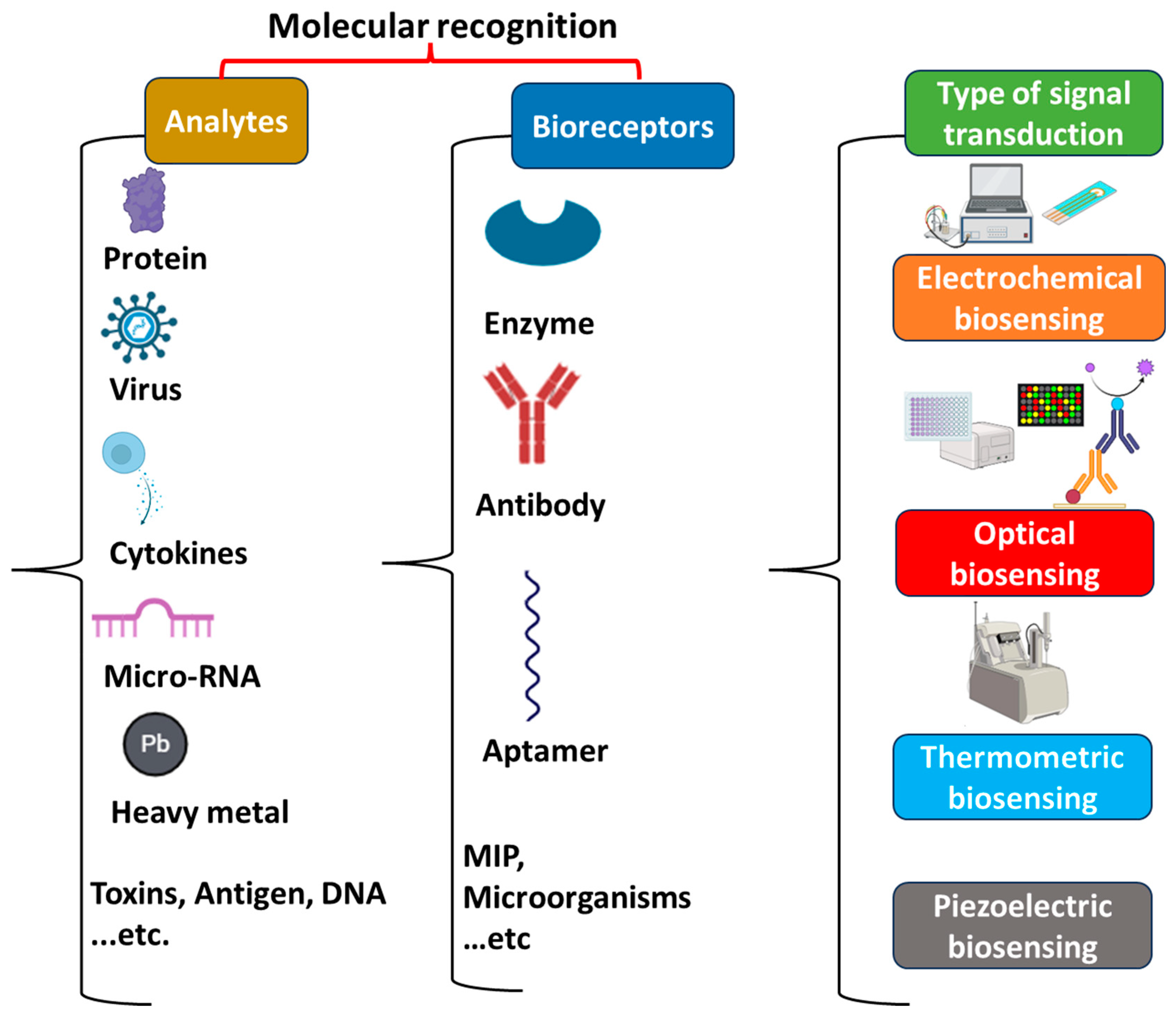
3. Key Components of Biosensors
3.1. Bioreceptors
3.2. Transducers
3.2.1. Optical Biosensors
3.2.2. Electrochemical Biosensors
3.2.3. Piezoelectric Biosensors
3.2.4. Thermometric Biosensors
4. Autoimmune Disease Biosensing
4.1. Celiac Disease Sensing Strategies
4.2. Multiple Sclerosis Sensing Strategies
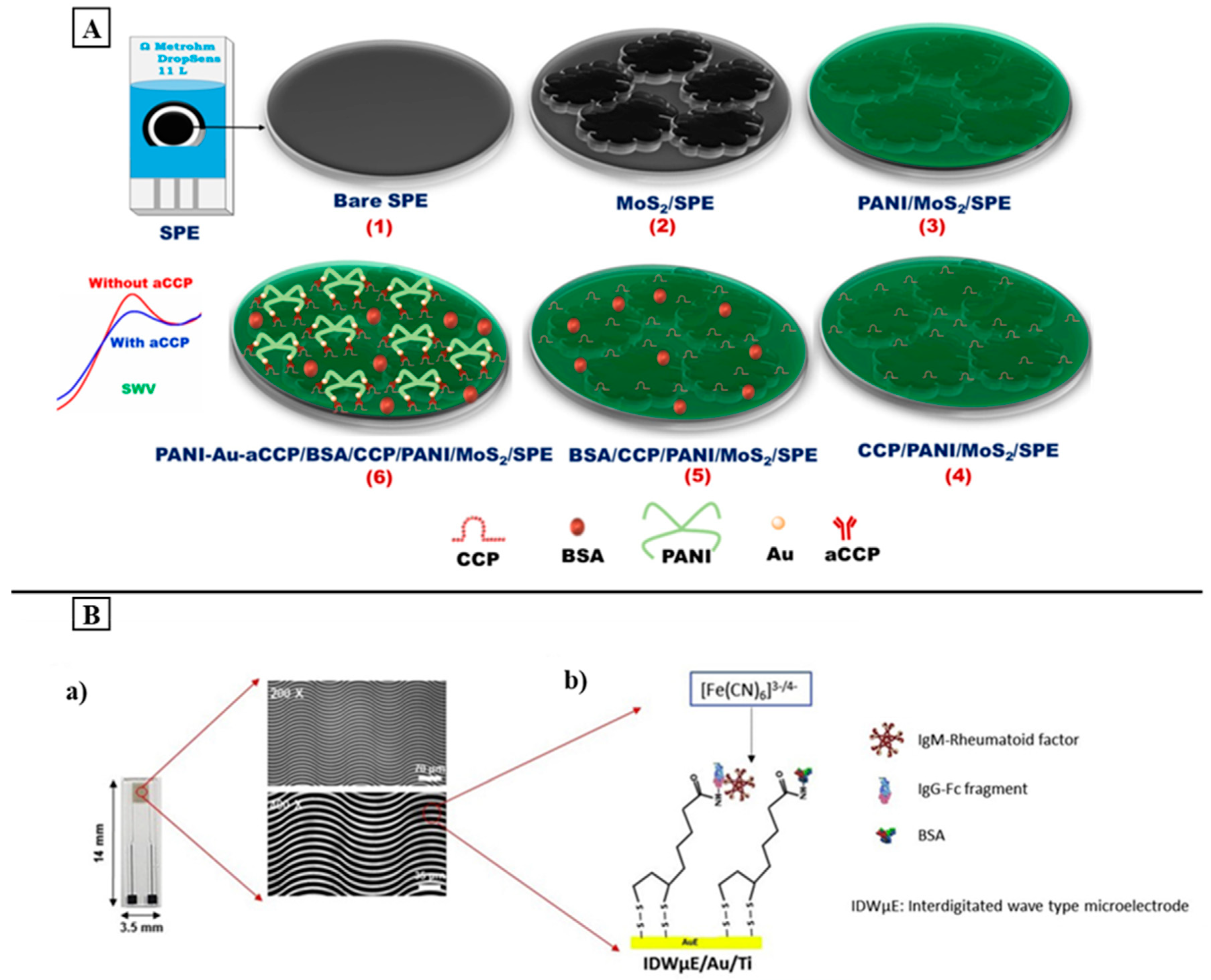
4.3. Rheumatoid Arthritis Sensing Strategies
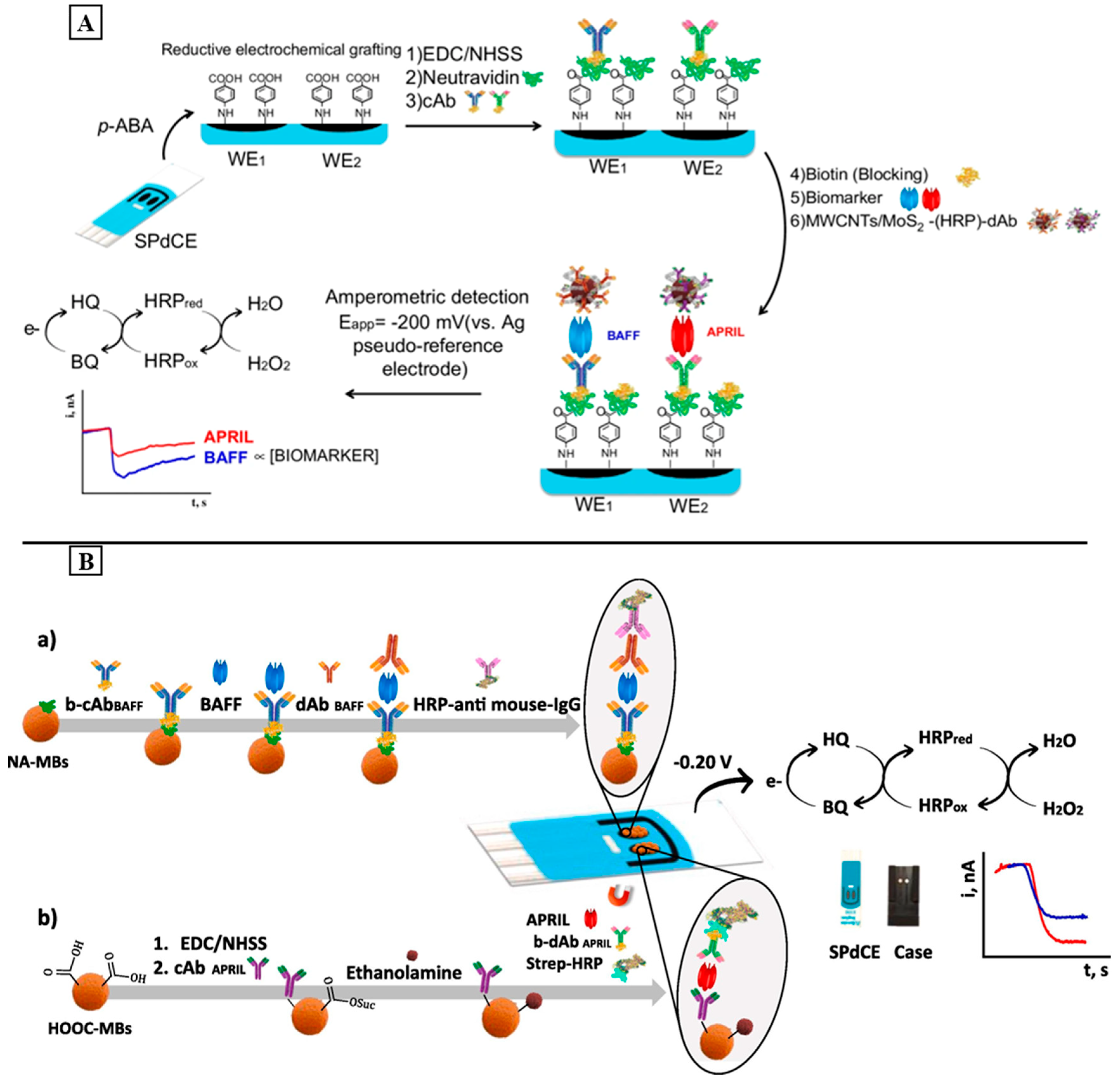
4.4. Systemic Lupus Erythematous Sensing Strategies
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidson, A.; Diamond, B. Autoimmune diseases. N. Engl. J. Med. 2001, 345, 340–350. [Google Scholar] [CrossRef]
- Chwastiak, L.; Ehde, D.M.; Gibbons, L.E.; Sullivan, M.; Bowen, J.D.; Kraft, G.H. Depressive symptoms and severity of illness in multiple sclerosis: Epidemiologic study of a large community sample. Am. J. Psychiatry 2002, 159, 1862–1868. [Google Scholar] [CrossRef]
- Alegria, G.C.; Guellec, D.; Mariette, X.; Gottenberg, J.E.; Dernis, E.; Dubost, J.J.; Trouvin, A.P.; Hachulla, E.; Larroche, C.; Le Guern, V.; et al. Epidemiology of neurological manifestations in Sjögren’s syndrome: Data from the French ASSESS Cohort. RMD Open 2016, 2, e000179. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sørensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Rook, G.A. Hygiene hypothesis and autoimmune diseases. Clin. Rev. Allergy Immunol. 2012, 42, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Javierre, B.M.; Hernando, H.; Ballestar, E. Environmental triggers and epigenetic deregulation in autoimmune disease. Discov. Med. 2011, 12, 535–545. [Google Scholar] [PubMed]
- Davidson, A.; Diamond, B. General features of autoimmune disease. In The Autoimmune Diseases; Academic Press: Cambridge, MA, USA, 2020; pp. 17–44. [Google Scholar]
- Shoenfeld, Y.; Tincani, A.; Gershwin, M.E. Sex gender and autoimmunity. J. Autoimmun. 2012, 38, J71–J73. [Google Scholar] [CrossRef] [PubMed]
- Hayter, S.M.; Cook, M.C. Updated assessment of the prevalence, spectrum and case definition of autoimmune disease. Autoimmun. Rev. 2012, 11, 754–765. [Google Scholar] [CrossRef] [PubMed]
- Amador-Patarroyo, M.J.; Rodriguez-Rodriguez, A.; Montoya-Ortiz, G. How does age at onset influence the outcome of autoimmune diseases? Autoimmune Dis. 2012, 2012, 251730. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zambrano, A.; Lin, Z.-T.; Xing, Y.; Rippy, J.; Wu, T. Immunosensors for biomarker detection in autoimmune diseases. Arch. Immunol. Ther. Exp. 2017, 65, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Campuzano, S.; Pedrero, M.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J.M. Electrochemical biosensors for autoantibodies in autoimmune and cancer diseases. Anal. Methods 2019, 11, 871–887. [Google Scholar] [CrossRef]
- Tan, E.M. Autoantibodies, autoimmune disease, and the birth of immune diagnostics. J. Clin. Investig. 2012, 122, 3835–3836. [Google Scholar] [CrossRef]
- Yang, F.; Ma, Y.; Stanciu, S.G.; Wu, A. Transduction process-based classification of biosensors. In Nanobiosensors: From Design to Applications; Wiley: Hoboken, NJ, USA, 2020; pp. 23–44. [Google Scholar]
- Mascini, M.; Tombelli, S. Biosensors for biomarkers in medical diagnostics. Biomarkers 2008, 13, 637–657. [Google Scholar] [CrossRef] [PubMed]
- Burbelo, P.D.; O’Hanlon, T.P. New autoantibody detection technologies yield novel insights into autoimmune disease. Curr. Opin. Rheumatol. 2014, 26, 717. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R. Predictors of autoimmune disease: Autoantibodies and beyond. Autoimmunity 2008, 41, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani, F.; Abbaszadeh, H.; Mehdizadeh, A.; Ebrahimi-Warkiani, M.; Rashidi, M.-R.; Yousefi, M. Biosensors and nanobiosensors for rapid detection of autoimmune diseases: A review. Microchim. Acta 2019, 186, 838. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Orbai, A.M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Jeremias, P.; Matthias, T. The world incidence and prevalence of autoimmune diseases is increasing. Int. J. Celiac Dis. 2015, 3, 151–155. [Google Scholar] [CrossRef]
- Rubio–Tapia, A.; Kyle, R.A.; Kaplan, E.L.; Johnson, D.R.; Page, W.; Erdtmann, F.; Brantner, T.L.; Kim, W.R.; Phelps, T.K.; Lahr, B.D. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology 2009, 137, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Rubio-Tapia, A.; Van Dyke, C.T.; Melton, L.J., III; Zinsmeister, A.R.; Lahr, B.D.; Murray, J.A. Increasing incidence of celiac disease in a North American population. Am. J. Gastroenterol. 2013, 108, 818. [Google Scholar] [CrossRef]
- Leffler, D.A.; Schuppan, D. Update on serologic testing in celiac disease. Off. J. Am. Coll. Gastroenterol. ACG 2010, 105, 2520–2524. [Google Scholar] [CrossRef]
- Hill, I.D. What are the sensitivity and specificity of serologic tests for celiac disease? Do sensitivity and specificity vary in different populations? Gastroenterology 2005, 128, S25–S32. [Google Scholar] [CrossRef]
- Spijkerman, M.; Tan, I.L.; Kolkman, J.J.; Withoff, S.; Wijmenga, C.; Visschedijk, M.C.; Weersma, R.K. A large variety of clinical features and concomitant disorders in celiac disease–a cohort study in the Netherlands. Dig. Liver Dis. 2016, 48, 499–505. [Google Scholar] [CrossRef]
- Meresse, B.; Ripoche, J.; Heyman, M.; Cerf-Bensussan, N. Celiac disease: From oral tolerance to intestinal inflammation, autoimmunity and lymphomagenesis. Mucosal Immunol. 2009, 2, 8–23. [Google Scholar] [CrossRef]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G. European Society Paediatric Gastroenterology, Hepatology and Nutrition guidelines for diagnosing coeliac disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef]
- Monzani, A.; Rapa, A.; Fonio, P.; Tognato, E.; Panigati, L.; Oderda, G. Use of deamidated gliadin peptide antibodies to monitor diet compliance in childhood celiac disease. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 55–60. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Mäki, M.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Diagnostic accuracy of point of care tests for diagnosing celiac disease. J. Clin. Gastroenterol. 2019, 53, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Planas, R.; Pujol-Autonell, I.; Ruiz, E.; Montraveta, M.; Cabre, E.; Lucas-Martin, A.; Pujol-Borrell, R.; Martinez-Caceres, E.; Vives-Pi, M. Regenerating gene Iα is a biomarker for diagnosis and monitoring of celiac disease: A preliminary study. Transl. Res. 2011, 158, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Alaedini, A.; Green, P.H. Autoantibodies in celiac disease. Autoimmunity 2008, 41, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Manavalan, J.S.; Hernandez, L.; Shah, J.G.; Konikkara, J.; Naiyer, A.J.; Lee, A.R.; Ciaccio, E.; Minaya, M.T.; Green, P.H.; Bhagat, G. Serum cytokine elevations in celiac disease: Association with disease presentation. Hum. Immunol. 2010, 71, 50–57. [Google Scholar] [CrossRef]
- Iervasi, E.; Auricchio, R.; Strangio, A.; Greco, L.; Saverino, D. Serum IL-21 levels from celiac disease patients correlates with anti-tTG IgA autoantibodies and mucosal damage. Autoimmunity 2020, 53, 225–230. [Google Scholar] [CrossRef]
- Jabri, B.; Sollid, L.M. T cells in celiac disease. J. Immunol. 2017, 198, 3005–3014. [Google Scholar] [CrossRef]
- Serin, M.; Kara, P. Biosensing strategies (approaches) for diagnosis and monitoring of multiple sclerosis. Talanta 2023, 252, 123794. [Google Scholar] [CrossRef]
- Housley, W.J.; Pitt, D.; Hafler, D.A. Biomarkers in multiple sclerosis. Clin. Immunol. 2015, 161, 51–58. [Google Scholar] [CrossRef]
- Ascherio, A. Environmental factors in multiple sclerosis. Expert Rev. Neurother. 2013, 13 (Suppl. S2), 3–9. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and treatment of multiple sclerosis: A review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, W.J.; Hardy, T.A.; Fazekas, F.; Miller, D.H. Diagnosis of multiple sclerosis: Progress and challenges. Lancet 2017, 389, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Caudle, W.M.; Zhang, J. Biomarker discovery in neurodegenerative diseases: A proteomic approach. Neurobiol. Dis. 2009, 35, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Pachner, A.R.; DiSano, K.; Royce, D.B.; Gilli, F. Clinical utility of a molecular signature in inflammatory demyelinating disease. Neurol.-Neuroimmunol. Neuroinflamm. 2019, 6, e520. [Google Scholar] [CrossRef] [PubMed]
- Martinsen, V.; Kursula, P. Multiple sclerosis and myelin basic protein: Insights into protein disorder and disease. Amino Acids 2022, 54, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Belogurov, A.A.; Kurkova, I.N.; Friboulet, A.; Thomas, D.; Misikov, V.K.; Zakharova, M.Y.; Suchkov, S.V.; Kotov, S.V.; Alehin, A.I.; Avalle, B. Recognition and degradation of myelin basic protein peptides by serum autoantibodies: Novel biomarker for multiple sclerosis. J. Immunol. 2008, 180, 1258–1267. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hamade, M.; Wu, Q.; Wang, Q.; Axtell, R.; Giri, S.; Mao-Draayer, Y. Current and Future Biomarkers in Multiple Sclerosis. Int. J. Mol. Sci. 2022, 23, 5877. [Google Scholar] [CrossRef] [PubMed]
- Kuhle, J.; Malmeström, C.; Axelsson, M.; Plattner, K.; Yaldizli, Ö.; Derfuss, T.; Giovannoni, G.; Kappos, L.; Lycke, J. Neurofilament light and heavy subunits compared as therapeutic biomarkers in multiple sclerosis. Acta Neurol. Scand. 2013, 128, e33–e36. [Google Scholar] [CrossRef] [PubMed]
- Disanto, G.; Adiutori, R.; Dobson, R.; Martinelli, V.; Dalla Costa, G.; Runia, T.; Evdoshenko, E.; Thouvenot, E.; Trojano, M.; Norgren, N. Serum neurofilament light chain levels are increased in patients with a clinically isolated syndrome. J. Neurol. Neurosurg. Psychiatry 2016, 87, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Salzer, J.; Svenningsson, A.; Sundström, P. Neurofilament light as a prognostic marker in multiple sclerosis. Mult. Scler. J. 2010, 16, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, M.; Malmeström, C.; Axelsson, M.; Sundström, P.; Dahle, C.; Vrethem, M.; Olsson, T.; Piehl, F.; Norgren, N.; Rosengren, L. Axonal damage in relapsing multiple sclerosis is markedly reduced by natalizumab. Ann. Neurol. 2011, 69, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.R.; Ratzer, R.; Börnsen, L.; Lyksborg, M.; Garde, E.; Dyrby, T.B.; Siebner, H.R.; Sorensen, P.S.; Sellebjerg, F. Natalizumab in progressive MS: Results of an open-label, phase 2A, proof-of-concept trial. Neurology 2014, 82, 1499–1507. [Google Scholar] [CrossRef]
- Kuhle, J.; Disanto, G.; Lorscheider, J.; Stites, T.; Chen, Y.; Dahlke, F.; Francis, G.; Shrinivasan, A.; Radue, E.-W.; Giovannoni, G. Fingolimod and CSF neurofilament light chain levels in relapsing-remitting multiple sclerosis. Neurology 2015, 84, 1639–1643. [Google Scholar] [CrossRef]
- Håkansson, I.; Tisell, A.; Cassel, P.; Blennow, K.; Zetterberg, H.; Lundberg, P.; Dahle, C.; Vrethem, M.; Ernerudh, J. Neurofilament levels, disease activity and brain volume during follow-up in multiple sclerosis. J. Neuroinflamm. 2018, 15, 209. [Google Scholar] [CrossRef]
- Burman, J.; Zetterberg, H.; Fransson, M.; Loskog, A.S.; Raininko, R.; Fagius, J. Assessing tissue damage in multiple sclerosis: A biomarker approach. Acta Neurol. Scand. 2014, 130, 81–89. [Google Scholar] [CrossRef]
- Ziemssen, T.; Ziemssen, F. The role of the humoral immune system in multiple sclerosis (MS) and its animal model experimental autoimmune encephalomyelitis (EAE). Autoimmun. Rev. 2005, 4, 460–467. [Google Scholar] [CrossRef]
- Link, H.; Huang, Y.-M. Oligoclonal bands in multiple sclerosis cerebrospinal fluid: An update on methodology and clinical usefulness. J. Neuroimmunol. 2006, 180, 17–28. [Google Scholar] [CrossRef]
- Chu, A.B.; Sever, J.L.; Madden, D.L.; Iivanainen, M.; Leon, M.; Wallen, W.; Brooks, B.R.; Lee, Y.J.; Houff, S. Oligoclonal IgG bands in cerebrospinal fluid in various neurological diseases. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 1983, 13, 434–439. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Arrambide, G.; Tintore, M.; Montalban, X. Oligoclonal bands do not represent dissemination in time in the 2017 revisions to the McDonald criteria. Mult. Scler. J. 2019, 25, 1690–1691. [Google Scholar] [CrossRef] [PubMed]
- Trojano, M.; Tintore, M.; Montalban, X.; Hillert, J.; Kalincik, T.; Iaffaldano, P.; Spelman, T.; Sormani, M.P.; Butzkueven, H. Treatment decisions in multiple sclerosis—Insights from real-world observational studies. Nat. Rev. Neurol. 2017, 13, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Akgün, K.; Brück, W. Molecular biomarkers in multiple sclerosis. J. Neuroinflamm. 2019, 16, 272. [Google Scholar] [CrossRef] [PubMed]
- Lefvert, A.K.; Link, H. IgG production within the central nervous system: A critical review of proposed formulae. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 1985, 17, 13–20. [Google Scholar]
- Comabella, M.; Montalban, X. Body fluid biomarkers in multiple sclerosis. Lancet Neurol. 2014, 13, 113–126. [Google Scholar] [CrossRef]
- Malmeström, C.; Haghighi, S.; Rosengren, L.; Andersen, O.; Lycke, J. Neurofilament light protein and glial fibrillary acidic protein as biological markers in MS. Neurology 2003, 61, 1720–1725. [Google Scholar] [CrossRef]
- Norgren, N.; Sundström, P.; Svenningsson, A.; Rosengren, L.; Stigbrand, T.; Gunnarsson, M. Neurofilament and glial fibrillary acidic protein in multiple sclerosis. Neurology 2004, 63, 1586–1590. [Google Scholar] [CrossRef]
- Rosengren, L.; Lycke, J.; Andersen, O. Glial fibrillary acidic protein in CSF of multiple sclerosis patients: Relation to neurological deficit. J. Neurol. Sci. 1995, 133, 61–65. [Google Scholar] [CrossRef]
- Barateiro, A.; Afonso, V.; Santos, G.; Cerqueira, J.J.; Brites, D.; van Horssen, J.; Fernandes, A. S100B as a potential biomarker and therapeutic target in multiple sclerosis. Mol. Neurobiol. 2016, 53, 3976–3991. [Google Scholar] [CrossRef] [PubMed]
- Islas-Hernandez, A.; Aguilar-Talamantes, H.S.; Bertado-Cortes, B.; Mejia-delCastillo, G.d.J.; Carrera-Pineda, R.; Cuevas-Garcia, C.F.; Garcia-delaTorre, P. BDNF and Tau as biomarkers of severity in multiple sclerosis. Biomark. Med. 2018, 12, 717–726. [Google Scholar] [CrossRef]
- Mancuso, R.; Hernis, A.; Agostini, S.; Rovaris, M.; Caputo, D.; Clerici, M. MicroRNA-572 expression in multiple sclerosis patients with different patterns of clinical progression. J. Transl. Med. 2015, 13, 148. [Google Scholar] [CrossRef] [PubMed]
- Bahmani, E.; Hoseini, R.; Amiri, E. Home-based aerobic training and vitamin D improve neurotrophins and inflammatory biomarkers in MS patients. Mult. Scler. Relat. Disord. 2022, 60, 103693. [Google Scholar] [CrossRef] [PubMed]
- Mathur, D.; Rout, S.; Mishra, B.K.; Rodas, G.L.; Vallamkondu, J.; Kandimalla, R.; Casanova, B. Potential Pathological Biomarkers in Multiple Sclerosis. Preprints 2020. [Google Scholar] [CrossRef]
- Smolen, J.S.; Burmester, G.-R.; Combe, B.; Curtis, J.R.; Hall, S.; Haraoui, B.; van Vollenhoven, R.; Cioffi, C.; Ecoffet, C.; Gervitz, L. Head-to-head comparison of certolizumab pegol versus adalimumab in rheumatoid arthritis: 2-year efficacy and safety results from the randomised EXXELERATE study. Lancet 2016, 388, 2763–2774. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Smolen, J.S. Diagnosis and management of rheumatoid arthritis: A review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef] [PubMed]
- Gavrilă, B.; Ciofu, C.; Stoica, V. Biomarkers in rheumatoid arthritis, what is new? J. Med. Life 2016, 9, 144. [Google Scholar]
- Luime, J.; Colin, E.; Hazes, J.; Lubberts, E. Does anti-mutated citrullinated vimentin have additional value as a serological marker in the diagnostic and prognostic investigation of patients with rheumatoid arthritis? A systematic review. Ann. Rheum. Dis. 2010, 69, 337–344. [Google Scholar] [CrossRef]
- Nielsen, S.F.; Bojesen, S.E.; Schnohr, P.; Nordestgaard, B.G. Elevated rheumatoid factor and long term risk of rheumatoid arthritis: A prospective cohort study. BMJ 2012, 345, e5244. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, T.; Arinbjarnarson, S.; Thorsteinsson, J.; Steinsson, K.; Geirsson, A.; Jonsson, H.; Valdimarsson, H. Raised IgA rheumatoid factor (RF) but not IgM RF or IgG RF is associated with extra-articular manifestations in rheumatoid arthritis. Scand. J. Rheumatol. 1995, 24, 372–375. [Google Scholar] [CrossRef]
- Westwood, O.M.R.; Nelson, P.N.; Hay, F.C. Rheumatoid factors: What’s new? Rheumatology 2006, 45, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.; Gourley, M. Diagnostic testing and interpretation of tests for autoimmunity. J. Allergy Clin. Immunol. 2010, 125, S238–S247. [Google Scholar] [CrossRef] [PubMed]
- Valesini, G.; Gerardi, M.C.; Iannuccelli, C.; Pacucci, V.A.; Pendolino, M.; Shoenfeld, Y. Citrullination and autoimmunity. Autoimmun. Rev. 2015, 14, 490–497. [Google Scholar] [CrossRef]
- Shi, J.; van Steenbergen, H.W.; van Nies, J.A.; Levarht, E.; Huizinga, T.W.; van der Helm-van Mil, A.; Toes, R.E.; Trouw, L.A. The specificity of anti-carbamylated protein antibodies for rheumatoid arthritis in a setting of early arthritis. Arthritis Res. Ther. 2015, 17, 339. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Smidt, N.; Sterne, J.A.C.; Harbord, R.; Burton, A.; Burke, M.; Beynon, R.; Ben-Shlomo, Y.; Axford, J.; Dieppe, P. Systematic Review: Accuracy of Anti–Citrullinated Peptide Antibodies for Diagnosing Rheumatoid Arthritis. Ann. Intern. Med. 2010, 152, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Bae, S.C.; Song, G.G. Diagnostic accuracy of anti-MCV and anti-CCP antibodies in rheumatoid arthritis. Z. Rheumatol. 2015, 74, 911–918. [Google Scholar] [CrossRef]
- Emery, P.; Gabay, C.; Kraan, M.; Gomez-Reino, J. Evidence-based review of biologic markers as indicators of disease progression and remission in rheumatoid arthritis. Rheumatol. Int. 2007, 27, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Dixey, J.; Solymossy, C.; Young, A. Is it possible to predict radiological damage in early rheumatoid arthritis (RA)? A report on the occurrence, progression, and prognostic factors of radiological erosions over the first 3 years in 866 patients from the Early RA Study (ERAS). J. Rheumatol. Suppl. 2004, 69, 48–54. [Google Scholar] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham III, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein*. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [PubMed]
- Sokka, T.; Pincus, T. Erythrocyte sedimentation rate, C-reactive protein, or rheumatoid factor are normal at presentation in 35%–45% of patients with rheumatoid arthritis seen between 1980 and 2004: Analyses from Finland and the United States. J. Rheumatol. 2009, 36, 1387–1390. [Google Scholar] [CrossRef]
- Shapiro, S.C. Biomarkers in rheumatoid arthritis. Cureus 2021, 13, e15063. [Google Scholar] [CrossRef]
- Generali, E.; Scire, C.A.; Favalli, E.G.; Selmi, C. Biomarkers in psoriatic arthritis: A systematic literature review. Expert Rev. Clin. Immunol. 2016, 12, 651–660. [Google Scholar] [CrossRef]
- Strand, V.; Sharp, V.; Koenig, A.S.; Park, G.; Shi, Y.; Wang, B.; Zack, D.J.; Fiorentino, D. Comparison of health-related quality of life in rheumatoid arthritis, psoriatic arthritis and psoriasis and effects of etanercept treatment. Ann. Rheum. Dis. 2012, 71, 1143–1150. [Google Scholar] [CrossRef]
- O’Rielly, D.D.; Rahman, P. Genetics of susceptibility and treatment response in psoriatic arthritis. Nat. Rev. Rheumatol. 2011, 7, 718–732. [Google Scholar] [CrossRef]
- Tsoi, L.C.; Spain, S.L.; Knight, J.; Ellinghaus, E.; Stuart, P.E.; Capon, F.; Ding, J.; Li, Y.; Tejasvi, T.; Gudjonsson, J.E. Identification of 15 new psoriasis susceptibility loci highlights the role of innate immunity. Nat. Genet. 2012, 44, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; FitzGerald, O.; Helliwell, P.S.; Paul, C. Psoriasis, psoriatic arthritis, and rheumatoid arthritis: Is all inflammation the same? Semin. Arthritis Rheum. 2016, 46, 291–304. [Google Scholar] [CrossRef]
- Boehncke, S.; Salgo, R.; Garbaraviciene, J.; Beschmann, H.; Hardt, K.; Diehl, S.; Fichtlscherer, S.; Thaçi, D.; Boehncke, W.H. Effective continuous systemic therapy of severe plaque-type psoriasis is accompanied by amelioration of biomarkers of cardiovascular risk: Results of a prospective longitudinal observational study. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1187–1193. [Google Scholar] [CrossRef]
- Mease, P.; Goffe, B.S. Diagnosis and treatment of psoriatic arthritis. J. Am. Acad. Dermatol. 2005, 52, 1–19. [Google Scholar] [CrossRef]
- Villanova, F.; Di Meglio, P.; Nestle, F.O. Biomarkers in psoriasis and psoriatic arthritis. Ann. Rheum. Dis. 2013, 72 (Suppl. 2), ii104–ii110. [Google Scholar] [CrossRef]
- Waszczykowski, M.; Bednarski, I.; Lesiak, A.; Waszczykowska, E.; Narbutt, J.; Fabiś, J. The influence of tumour necrosis factor α inhibitors treatment–etanercept on serum concentration of biomarkers of inflammation and cartilage turnover in psoriatic arthritis patients. Adv. Dermatol. Allergol./Postępy Dermatol. Alergol. 2020, 37, 995–1000. [Google Scholar] [CrossRef]
- Johnson, C.; Fitch, K.; Merola, J.; Han, J.; Qureshi, A.; Li, W.Q. Plasma levels of tumour necrosis factor-α and adiponectin can differentiate patients with psoriatic arthritis from those with psoriasis. Br. J. Dermatol. 2019, 181, 379–380. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Boehncke, S. Cardiovascular mortality in psoriasis and psoriatic arthritis: Epidemiology, pathomechanisms, therapeutic implications, and perspectives. Curr. Rheumatol. Rep. 2012, 14, 343–348. [Google Scholar] [CrossRef]
- Chandran, V.; Scher, J.U. Biomarkers in psoriatic arthritis: Recent progress. Curr. Rheumatol. Rep. 2014, 16, 453. [Google Scholar] [CrossRef] [PubMed]
- Strober, B.; Teller, C.; Yamauchi, P.; Miller, J.; Hooper, M.; Yang, Y.C.; Dann, F. Effects of etanercept on C-reactive protein levels in psoriasis and psoriatic arthritis. Br. J. Dermatol. 2008, 159, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Bosè, F.; Capsoni, F.; Molteni, S.; Raeli, L.; Diani, M.; Altomare, A.; Garavaglia, M.; Garutti, C.; Frigerio, E.; Banfi, G. Differential expression of interleukin-2 by anti-CD3-stimulated peripheral blood mononuclear cells in patients with psoriatic arthritis and patients with cutaneous psoriasis. Clin. Exp. Dermatol. 2014, 39, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Fava, A.; Petri, M. Systemic lupus erythematosus: Diagnosis and clinical management. J. Autoimmun. 2019, 96, 1–13. [Google Scholar] [CrossRef]
- Arriens, C.; Wren, J.D.; Munroe, M.E.; Mohan, C. Systemic lupus erythematosus biomarkers: The challenging quest. Rheumatology 2016, 56 (Suppl. 1), i32–i45. [Google Scholar] [CrossRef]
- Cojocaru, M.; Cojocaru, I.M.; Silosi, I.; Vrabie, C.D. Manifestations of systemic lupus erythematosus. Maedica 2011, 6, 330. [Google Scholar] [PubMed]
- Kuhn, A.; Bonsmann, G.; Anders, H.-J.; Herzer, P.; Tenbrock, K.; Schneider, M. The diagnosis and treatment of systemic lupus erythematosus. Dtsch. Ärzteblatt Int. 2015, 112, 423. [Google Scholar] [CrossRef] [PubMed]
- Seligman, V.A.; Lum, R.F.; Olson, J.L.; Li, H.; Criswell, L.A. Demographic differences in the development of lupus nephritis: A retrospective analysis. Am. J. Med. 2002, 112, 726–729. [Google Scholar] [CrossRef]
- Abbas, A.H.; Melconian, A.K.; Ad’hiah, A.H. Autoantibody Profile in Systemic Lupus Erythematosus Patients. J. Phys. Conf. Ser. 2019, 1294, 062006. [Google Scholar] [CrossRef]
- Akhil, A.; Bansal, R.; Anupam, K.; Tandon, A.; Bhatnagar, A. Systemic lupus erythematosus: Latest insight into etiopathogenesis. Rheumatol. Int. 2023, 43, 1381–1393. [Google Scholar] [CrossRef]
- Dima, A.; Opris, D.; Jurcut, C.; Baicus, C. Is there still a place for erythrocyte sedimentation rate and C-reactive protein in systemic lupus erythematosus? Lupus 2016, 25, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Firooz, N.; Albert, D.; Wallace, D.; Ishimori, M.; Berel, D.; Weisman, M. High-sensitivity C-reactive protein and erythrocyte sedimentation rate in systemic lupus erythematosus. Lupus 2011, 20, 588–597. [Google Scholar] [CrossRef]
- Habtamu, H.B.; Not, T.; De Leo, L.; Longo, S.; Moretto, L.M.; Ugo, P. Electrochemical immunosensor based on nanoelectrode ensembles for the serological analysis of IgG-type tissue transglutaminase. Sensors 2019, 19, 1233. [Google Scholar] [CrossRef]
- Mubarak, A.; Wolters, V.M.; Gmelig-Meyling, F.H.; Ten Kate, F.J.; Houwen, R.H. Tissue transglutaminase levels above 100 U/mL and celiac disease: A prospective study. World J. Gastroenterol. 2012, 18, 4399–4403. [Google Scholar] [CrossRef]
- Hafler, D.A.; Weiner, H.L. Immunologic mechanisms and therapy in multiple sclerosis. Immunol. Rev. 1995, 144, 75–107. [Google Scholar] [CrossRef]
- Cao, Y.; Chen, D.; Chen, W.; Yu, J.; Chen, Z.; Li, G. Aptamer-based homogeneous protein detection using cucurbit[7]uril functionalized electrode. Anal. Chim. Acta 2014, 812, 45–49. [Google Scholar] [CrossRef]
- Paimela, L.; Palosuo, T.; Leirisalo-Repo, M.; Helve, T.; Aho, K. Prognostic value of quantitative measurement of rheumatoid factor in early rheumatoid arthritis. Rheumatology 1995, 34, 1146–1150. [Google Scholar] [CrossRef]
- Trisnawati, E.; Nontji, W.; Nurasni, S. Tumour necrosis factor-α (TNF-α) serum levels in preeclampsia pregnant women and pregnant women at risk with preeclampsia. Enferm. Clín. 2020, 30, 27–30. [Google Scholar] [CrossRef]
- Chinnadayyala, S.R.; Cho, S. Electrochemical immunosensor for the early detection of rheumatoid arthritis biomarker: Anti-cyclic citrullinated peptide antibody in human serum based on avidin-biotin system. Sensors 2020, 21, 124. [Google Scholar] [CrossRef] [PubMed]
- Sabio, J.M.; Sánchez-Berná, I.; Martinez-Bordonado, J.; Vargas-Hitos, J.A.; Navarrete-Navarrete, N.; Expósito Ruíz, M.; Jiménez-Alonso, J. Prevalence of and factors associated with increased arterial stiffness in patients with primary Sjögren’s syndrome. Arthritis Care Res. 2015, 67, 554–562. [Google Scholar] [CrossRef]
- Pasoto, S.G.; Chakkour, H.P.; Natalino, R.R.; Viana, V.S.; Bueno, C.; Lianza, A.C.; de Andrade, J.L.; Neto, M.L.; Fuller, R.; Bonfa, E. Lupus anticoagulant: A marker for stroke and venous thrombosis in primary Sjögren’s syndrome. Clin. Rheumatol. 2012, 31, 1331–1338. [Google Scholar] [CrossRef]
- Amaya-Amaya, J.; Montoya-Sánchez, L.; Rojas-Villarraga, A. Cardiovascular involvement in autoimmune diseases. BioMed Res. Int. 2014, 2014, 367359. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef]
- Caprilli, R. Why does Crohn’s disease usually occur in terminal ileum? J. Crohn’s Colitis 2008, 2, 352–356. [Google Scholar] [CrossRef]
- Porter, A.C.; Aubrecht, J.; Birch, C.; Braun, J.; Cuff, C.; Dasgupta, S.; Gale, J.D.; Hinton, R.; Hoffmann, S.C.; Honig, G.; et al. Biomarkers of Crohn’s Disease to Support the Development of New Therapeutic Interventions. Inflamm. Bowel Dis. 2020, 26, 1498–1508. [Google Scholar] [CrossRef]
- Smith, T.J.; Hegedüs, L. Graves’ disease. N. Engl. J. Med. 2016, 375, 1552–1565. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Masetti, G.; Colucci, G.; Salvi, M.; Covelli, D.; Eckstein, A.; Kaiser, U.; Draman, M.S.; Muller, I.; Ludgate, M.; et al. Combining micro-RNA and protein sequencing to detect robust biomarkers for Graves’ disease and orbitopathy. Sci. Rep. 2018, 8, 8386. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Hou, Q.; Huang, S.; Ou, Q.; Huo, D.; Vázquez-Baeza, Y.; Cen, C.; Cantu, V.; Estaki, M.; Chang, H.; et al. Compositional and genetic alterations in Graves’ disease gut microbiome reveal specific diagnostic biomarkers. ISME J. 2021, 15, 3399–3411. [Google Scholar] [CrossRef] [PubMed]
- Luong, J.H.; Male, K.B.; Glennon, J.D. Biosensor technology: Technology push versus market pull. Biotechnol. Adv. 2008, 26, 492–500. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, Q.; Cui, D. Recent advances in nanotechnology applied to biosensors. Sensors 2009, 9, 1033–1053. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.H.; Lee, S.H.; Lee, U.J.; Fermin, C.D.; Kim, M. Immobilized enzymes in biosensor applications. Materials 2019, 12, 121. [Google Scholar] [CrossRef]
- Wang, J. Glucose biosensors: 40 years of advances and challenges. Electroanal. Int. J. Devoted Fundam. Pract. Asp. Electroanal. 2001, 13, 983–988. [Google Scholar] [CrossRef]
- Shukla, S.; Govender, P.; Tiwari, A. Polymeric micellar structures for biosensor technology. In Advances in Biomembranes and Lipid Self-Assembly; Elsevier: Amsterdam, The Netherlands, 2016; pp. 143–161. [Google Scholar]
- Karunakaran, C.; Rajkumar, R.; Bhargava, K. Introduction to biosensors. In Biosensors and Bioelectronics; Elsevier: Amsterdam, The Netherlands, 2015; pp. 1–68. [Google Scholar]
- Monk, D.J.; Walt, D.R. Optical fiber-based biosensors. Anal. Bioanal. Chem. 2004, 379, 931–945. [Google Scholar] [CrossRef]
- Morrison, D.W.; Dokmeci, M.R.; Demirci, U.; Khademhosseini, A. Clinical applications of micro-and nanoscale biosensors. Biomed. Nanostruct. 2008, 1, 433–458. [Google Scholar]
- Warsinke, A.; Benkert, A.; Scheller, F. Electrochemical immunoassays. Fresenius’ J. Anal. Chem. 2000, 366, 622–634. [Google Scholar] [CrossRef]
- Schroeder, H.W., Jr.; Cavacini, L. Structure and function of immunoglobulins. J. Allergy Clin. Immunol. 2010, 125, S41–S52. [Google Scholar] [CrossRef]
- Kubik, T.; Bogunia-Kubik, K.; Sugisaka, M. Nanotechnology on duty in medical applications. Curr. Pharm. Biotechnol. 2005, 6, 17–33. [Google Scholar] [CrossRef]
- Haupt, K. Molecularly imprinted polymers in analytical chemistry. Analyst 2001, 126, 747–756. [Google Scholar] [CrossRef]
- Ashley, J.; Shahbazi, M.-A.; Kant, K.; Chidambara, V.A.; Wolff, A.; Bang, D.D.; Sun, Y. Molecularly imprinted polymers for sample preparation and biosensing in food analysis: Progress and perspectives. Biosens. Bioelectron. 2017, 91, 606–615. [Google Scholar] [CrossRef]
- Stoltenburg, R.; Reinemann, C.; Strehlitz, B. SELEX—A (r) evolutionary method to generate high-affinity nucleic acid ligands. Biomol. Eng. 2007, 24, 381–403. [Google Scholar] [CrossRef] [PubMed]
- Onoa, B.; Tinoco, I., Jr. RNA folding and unfolding. Curr. Opin. Struct. Biol. 2004, 14, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, A.; Kalra, P.; Bansal, V.; Bruno, J.G.; Sharma, T.K. Aptamer-based point-of-care diagnostic platforms. Sens. Actuators B Chem. 2017, 246, 535–553. [Google Scholar] [CrossRef]
- Sun, H.; Zu, Y. A highlight of recent advances in aptamer technology and its application. Molecules 2015, 20, 11959–11980. [Google Scholar] [CrossRef]
- Naresh, V.; Lee, N. A review on biosensors and recent development of nanostructured materials-enabled biosensors. Sensors 2021, 21, 1109. [Google Scholar] [CrossRef]
- Polat, E.O.; Cetin, M.M.; Tabak, A.F.; Bilget Güven, E.; Uysal, B.Ö.; Arsan, T.; Kabbani, A.; Hamed, H.; Gül, S.B. Transducer technologies for biosensors and their wearable applications. Biosensors 2022, 12, 385. [Google Scholar] [CrossRef] [PubMed]
- Bosch, M.E.; Sánchez, A.J.R.; Rojas, F.S.; Ojeda, C.B. Recent development in optical fiber biosensors. Sensors 2007, 7, 797–859. [Google Scholar] [CrossRef]
- Chen, C.; Wang, J. Optical biosensors: An exhaustive and comprehensive review. Analyst 2020, 145, 1605–1628. [Google Scholar] [CrossRef] [PubMed]
- Chun, L.; Kim, S.-E.; Cho, M.; Choe, W.-s.; Nam, J.; Lee, D.W.; Lee, Y. Electrochemical detection of HER2 using single stranded DNA aptamer modified gold nanoparticles electrode. Sens. Actuators B Chem. 2013, 186, 446–450. [Google Scholar] [CrossRef]
- Kucherenko, I.; Soldatkin, O.; Dzyadevych, S.; Soldatkin, A. Electrochemical biosensors based on multienzyme systems: Main groups, advantages and limitations–a review. Anal. Chim. Acta 2020, 1111, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, B.D.; Ali, M.A. Nanomaterials in biosensors: Fundamentals and applications. In Nanomaterials for Biosensors; William Andrew: Norwich, NY, USA, 2018; pp. 1–74. [Google Scholar]
- Elshafey, R.; Tavares, A.C.; Siaj, M.; Zourob, M. Electrochemical impedance immunosensor based on gold nanoparticles–protein G for the detection of cancer marker epidermal growth factor receptor in human plasma and brain tissue. Biosens. Bioelectron. 2013, 50, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Alam, Z.; Zhang, C.; Samali, B. Influence of seismic incident angle on response uncertainty and structural performance of tall asymmetric structure. Struct. Des. Tall Spec. Build. 2020, 29, e1750. [Google Scholar] [CrossRef]
- Wang, A.; Feng, J.; Li, Y.; Zou, P. Beyond fluorescent proteins: Hybrid and bioluminescent indicators for imaging neural activities. ACS Chem. Neurosci. 2018, 9, 639–650. [Google Scholar] [CrossRef]
- Kaur, H.; Shorie, M. Nanomaterial based aptasensors for clinical and environmental diagnostic applications. Nanoscale Adv. 2019, 1, 2123–2138. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.-H.; Zhou, Y.-H.; Wu, J.-J.; Cao, J.-T.; Li, L.-L.; Liu, H.-Y.; Zhu, J.-J. Microwave-assisted synthesis of nitrogen and boron co-doped graphene and its application for enhanced electrochemical detection of hydrogen peroxide. Rsc Adv. 2013, 3, 22597–22604. [Google Scholar] [CrossRef]
- Skládal, P. Piezoelectric biosensors. TrAC Trends Anal. Chem. 2016, 79, 127–133. [Google Scholar] [CrossRef]
- Lakshmipriya, T.; Gopinath, S.C. An introduction to biosensors and biomolecules. In Nanobiosensors for Biomolecular Targeting; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–21. [Google Scholar]
- Vasuki, S.; Varsha, V.; Mithra, R.; Dharshni, R.; Abinaya, S.; Dharshini, R.; Sivarajasekar, N. Thermal biosensors and their applications. Am. Int. J. Res. Sci. Technol. Eng. Math. 2019, 1, 262–264. [Google Scholar]
- Ramanathan, K.; Danielsson, B. Principles and applications of thermal biosensors. Biosens. Bioelectron. 2001, 16, 417–423. [Google Scholar] [CrossRef]
- Lenti, M.V.; Rossi, C.M.; Melazzini, F.; Gastaldi, M.; Bugatti, S.; Rotondi, M.; Bianchi, P.I.; Gentile, A.; Chiovato, L.; Montecucco, C. Seronegative autoimmune diseases: A challenging diagnosis. Autoimmun. Rev. 2022, 21, 103143. [Google Scholar] [CrossRef]
- Scherf, K.A.; Koehler, P.; Wieser, H. Electrochemical immunosensors for the diagnosis of celiac disease. Adv. Chem. Eng. Sci. 2014, 5, 83. [Google Scholar] [CrossRef]
- Karachaliou, C.-E.; Livaniou, E. Immunosensors for Autoimmune-Disease-Related Biomarkers: A Literature Review. Sensors 2023, 23, 6770. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.; Kelly, C.; Calderwood, A.; Murray, J. American College of Gastroenterology clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef]
- Scherf, K.A.; Ciccocioppo, R.; Pohanka, M.; Rimarova, K.; Opatrilova, R.; Rodrigo, L.; Kruzliak, P. Biosensors for the diagnosis of celiac disease: Current status and future perspectives. Mol. Biotechnol. 2016, 58, 381–392. [Google Scholar] [CrossRef]
- Nguyen, A.B.N.; Maldonado, M.; Poch, D.; Sodia, T.; Smith, A.; Rowland, T.J.; Bonham, A.J. Electrochemical DNA Biosensor That Detects Early Celiac Disease Autoantibodies. Sensors 2021, 21, 2671. [Google Scholar] [CrossRef]
- Dulay, S.; Lozano-Sánchez, P.; Iwuoha, E.; Katakis, I.; O’Sullivan, C.K. Electrochemical detection of celiac disease-related anti-tissue transglutaminase antibodies using thiol based surface chemistry. Biosens. Bioelectron. 2011, 26, 3852–3856. [Google Scholar] [CrossRef]
- Kergaravat, S.V.; Beltramino, L.; Garnero, N.; Trotta, L.; Wagener, M.; Pividori, M.I.; Hernandez, S.R. Electrochemical magneto immunosensor for the detection of anti-TG2 antibody in celiac disease. Biosens. Bioelectron. 2013, 48, 203–209. [Google Scholar] [CrossRef]
- Rosales-Rivera, L.; Acero-Sánchez, J.; Lozano-Sánchez, P.; Katakis, I.; O’Sullivan, C. Electrochemical immunosensor detection of antigliadin antibodies from real human serum. Biosens. Bioelectron. 2011, 26, 4471–4476. [Google Scholar] [CrossRef]
- Rosales-Rivera, L.C.; Dulay, S.; Lozano-Sánchez, P.; Katakis, I.; Acero-Sánchez, J.L.; O’Sullivan, C.K. Disulfide-modified antigen for detection of celiac disease-associated anti-tissue transglutaminase autoantibodies. Anal. Bioanal. Chem. 2017, 409, 3799–3806. [Google Scholar] [CrossRef]
- Wajs, E.; Fernández, N.; Fragoso, A. Supramolecular biosensors based on electropolymerised pyrrole–cyclodextrin modified surfaces for antibody detection. Analyst 2016, 141, 3274–3279. [Google Scholar] [CrossRef]
- Giannetto, M.; Bianchi, V.; Gentili, S.; Fortunati, S.; De Munari, I.; Careri, M. An integrated IoT-Wi-Fi board for remote data acquisition and sharing from innovative immunosensors. Case of study: Diagnosis of celiac disease. Sens. Actuators B Chem. 2018, 273, 1395–1403. [Google Scholar] [CrossRef]
- Longo, S.; De Leo, L.; Not, T.; Ugo, P. Nanoelectrode ensemble immunosensor platform for the anodic detection of anti-tissue transglutaminase isotype IgA. J. Electroanal. Chem. 2022, 906, 115984. [Google Scholar] [CrossRef]
- Neves, M.M.P.S.; González-García, M.B.; Delerue-Matos, C.; Costa-García, A. Multiplexed electrochemical immunosensor for detection of celiac disease serological markers. Sens. Actuators B Chem. 2013, 187, 33–39. [Google Scholar] [CrossRef]
- Habtamu, H.B.; Sentic, M.; Silvestrini, M.; De Leo, L.; Not, T.; Arbault, S.; Manojlovic, D.; Sojic, N.; Ugo, P. A sensitive electrochemiluminescence immunosensor for celiac disease diagnosis based on nanoelectrode ensembles. Anal. Chem. 2015, 87, 12080–12087. [Google Scholar] [CrossRef]
- Neves, M.M.; González-García, M.B.; Nouws, H.P.; Costa-García, A. An electrochemical deamidated gliadin antibody immunosensor for celiac disease clinical diagnosis. Analyst 2013, 138, 1956–1958. [Google Scholar] [CrossRef]
- Gupta, S.; Kaushal, A.; Kumar, A.; Kumar, D. Ultrasensitive transglutaminase based nanosensor for early detection of celiac disease in human. Int. J. Biol. Macromol. 2017, 105, 905–911. [Google Scholar] [CrossRef]
- La Belle, J.T.; Bhavsar, K.; Fairchild, A.; Das, A.; Sweeney, J.; Alford, T.L.; Wang, J.; Bhavanandan, V.P.; Joshi, L. A cytokine immunosensor for multiple sclerosis detection based upon label-free electrochemical impedance spectroscopy. Biosens. Bioelectron. 2007, 23, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Bhavsar, K.; Fairchild, A.; Alonas, E.; Bishop, D.K.; La Belle, J.T.; Sweeney, J.; Alford, T.; Joshi, L. A cytokine immunosensor for Multiple Sclerosis detection based upon label-free electrochemical impedance spectroscopy using electroplated printed circuit board electrodes. Biosens. Bioelectron. 2009, 25, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Derkus, B.; Emregul, E.; Emregul, K.C.; Yucesan, C. Alginate and alginate-titanium dioxide nanocomposite as electrode materials for anti-myelin basic protein immunosensing. Sens. Actuators B Chem. 2014, 192, 294–302. [Google Scholar] [CrossRef]
- Guerrero, S.; Sánchez-Tirado, E.; Agüí, L.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J. Monitoring autoimmune diseases by bioelectrochemical detection of autoantibodies. Application to the determination of anti-myelin basic protein autoantibodies in serum of multiple sclerosis patients. Talanta 2022, 243, 123304. [Google Scholar] [CrossRef] [PubMed]
- Mukama, O.; Wu, W.; Wu, J.; Lu, X.; Liu, Y.; Liu, Y.; Liu, J.; Zeng, L. A highly sensitive and specific lateral flow aptasensor for the detection of human osteopontin. Talanta 2020, 210, 120624. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, J.; Ambrosio, R.; Carrillo, A. Design of a Myelin Basic Protein Biosensor based on EnFET Technology. In Biodevices; SciTePress: Setúbal, Portugal, 2015; pp. 78–82. [Google Scholar]
- Song, J.; Dailey, J.; Li, H.; Jang, H.J.; Russell, L.; Zhang, P.; Searson, P.C.; Wang, J.T.H.; Everett, A.D.; Katz, H.E. Influence of bioreceptor layer structure on myelin basic protein detection using organic field effect transistor-based biosensors. Adv. Funct. Mater. 2018, 28, 1802605. [Google Scholar] [CrossRef]
- Krasitskaya, V.V.; Chaukina, V.V.; Abroskina, M.V.; Vorobyeva, M.A.; Ilminskaya, A.A.; Kabilov, M.R.; Prokopenko, S.V.; Nevinsky, G.A.; Venyaminova, A.G.; Frank, L.A. Bioluminescent aptamer-based sandwich-type assay of anti-myelin basic protein autoantibodies associated with multiple sclerosis. Anal. Chim. Acta 2019, 1064, 112–118. [Google Scholar] [CrossRef]
- Sadeghzadeh, J.; Shahabi, P.; Farhoudi, M.; Ebrahimi-Kalan, A.; Mobed, A.; Shahpasand, K. Tau Protein Biosensors in the Diagnosis of Neurodegenerative Diseases. Adv. Pharm. Bull. 2023, 13, 502. [Google Scholar] [CrossRef]
- Derkus, B.; Acar Bozkurt, P.; Tulu, M.; Emregul, K.C.; Yucesan, C.; Emregul, E. Simultaneous quantification of Myelin Basic Protein and Tau proteins in cerebrospinal fluid and serum of Multiple Sclerosis patients using nanoimmunosensor. Biosens. Bioelectron. 2017, 89, 781–788. [Google Scholar] [CrossRef]
- Zhou, S.; Gu, C.; Li, Z.; Yang, L.; He, L.; Wang, M.; Huang, X.; Zhou, N.; Zhang, Z. Ti3C2Tx MXene and polyoxometalate nanohybrid embedded with polypyrrole: Ultra-sensitive platform for the detection of osteopontin. Appl. Surf. Sci. 2019, 498, 143889. [Google Scholar] [CrossRef]
- Shariati, S.; Ghaffarinejad, A.; Omidinia, E. Early detection of multiple sclerosis (MS) as a neurodegenerative disease using electrochemical nano-aptasensor. Microchem. J. 2022, 178, 107358. [Google Scholar] [CrossRef]
- Ayankojo, A.G.; Boroznjak, R.; Reut, J.; Tuvikene, J.; Timmusk, T.; Syritski, V. Electrochemical sensor based on molecularly imprinted polymer for rapid quantitative detection of brain-derived neurotrophic factor. Sens. Actuators B Chem. 2023, 397, 134656. [Google Scholar] [CrossRef]
- van Delft, M.A.; Huizinga, T.W. An overview of autoantibodies in rheumatoid arthritis. J. Autoimmun. 2020, 110, 102392. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, Y.; Li, X.; Wang, H.; Zhang, Y.; Ma, H.; Wei, Q. Label-free ECL immunosensor for the early diagnosis of rheumatoid arthritis based on asymmetric heterogeneous polyaniline-gold nanomaterial. Sens. Actuators B Chem. 2018, 257, 354–361. [Google Scholar] [CrossRef]
- Selvam, S.P.; Chinnadayyala, S.R.; Cho, S. Electrochemical nanobiosensor for early detection of rheumatoid arthritis biomarker: Anti-cyclic citrullinated peptide antibodies based on polyaniline (PANI)/MoS2-modified screen-printed electrode with PANI-Au nanomatrix-based signal amplification. Sens. Actuators B Chem. 2021, 333, 129570. [Google Scholar] [CrossRef]
- Chinnadayyala, S.R.; Park, J.; Abbasi, M.A.; Cho, S. Label-free electrochemical impedimetric immunosensor for sensitive detection of IgM rheumatoid factor in human serum. Biosens. Bioelectron. 2019, 143, 111642. [Google Scholar] [CrossRef]
- Veigas, B.; Matias, A.; Calmeiro, T.; Fortunato, E.; Fernandes, A.R.; Baptista, P.V. Antibody modified gold nanoparticles for fast colorimetric screening of rheumatoid arthritis. Analyst 2019, 144, 3613–3619. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Yan, Y.; Xie, J.; Huang, H.; Wang, H.; Gopinath, S.C.B.; Anbu, P.; He, S.; Zhang, L. Immunosensing the rheumatoid arthritis biomarker through bifunctional aldehyde-amine linkers on an iron oxide nanoparticle seeded voltammetry sensor. Nanomater. Nanotechnol. 2022, 12, 18479804221085103. [Google Scholar] [CrossRef]
- Guerrero, S.; Sánchez-Tirado, E.; Martínez-García, G.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J.M. Electrochemical biosensor for the simultaneous determination of rheumatoid factor and anti-cyclic citrullinated peptide antibodies in human serum. Analyst 2020, 145, 4680–4687. [Google Scholar] [CrossRef]
- Arya, S.K.; Estrela, P. Electrochemical immunosensor for tumor necrosis factor-alpha detection in undiluted serum. Methods 2017, 116, 125–131. [Google Scholar] [CrossRef]
- Baydemir, G.; Bettazzi, F.; Palchetti, I.; Voccia, D. Strategies for the development of an electrochemical bioassay for TNF-alpha detection by using a non-immunoglobulin bioreceptor. Talanta 2016, 151, 141–147. [Google Scholar] [CrossRef]
- Bellagambi, F.G.; Baraket, A.; Longo, A.; Vatteroni, M.; Zine, N.; Bausells, J.; Fuoco, R.; Di Francesco, F.; Salvo, P.; Karanasiou, G.S. Electrochemical biosensor platform for TNF-α cytokines detection in both artificial and human saliva: Heart failure. Sens. Actuators B Chem. 2017, 251, 1026–1033. [Google Scholar] [CrossRef]
- Yagati, A.K.; Lee, M.-H.; Min, J. Electrochemical immunosensor for highly sensitive and quantitative detection of tumor necrosis factor-α in human serum. Bioelectrochemistry 2018, 122, 93–102. [Google Scholar] [CrossRef]
- Tertiş, M.; Ciui, B.; Suciu, M.; Săndulescu, R.; Cristea, C. Label-free electrochemical aptasensor based on gold and polypyrrole nanoparticles for interleukin 6 detection. Electrochim. Acta 2017, 258, 1208–1218. [Google Scholar] [CrossRef]
- Hosseini Ghalehno, M.; Mirzaei, M.; Torkzadeh-Mahani, M. Electrochemical aptasensor for tumor necrosis factor α using aptamer–antibody sandwich structure and cobalt hexacyanoferrate for signal amplification. J. Iran. Chem. Soc. 2019, 16, 1783–1791. [Google Scholar] [CrossRef]
- Zhang, C.; Shi, D.; Li, X.; Yuan, J. Microfluidic electrochemical magnetoimmunosensor for ultrasensitive detection of interleukin-6 based on hybrid of AuNPs and graphene. Talanta 2022, 240, 123173. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed]
- do Nascimento, N.M.; Juste-Dolz, A.; Grau-García, E.; Román-Ivorra, J.A.; Puchades, R.; Maquieira, A.; Morais, S.; Gimenez-Romero, D. Label-free piezoelectric biosensor for prognosis and diagnosis of Systemic Lupus Erythematosus. Biosens. Bioelectron. 2017, 90, 166–173. [Google Scholar] [CrossRef]
- Fagúndez, P.; Brañas, G.; Cairoli, E.; Laíz, J.; Tosar, J.P. An electrochemical biosensor for rapid detection of anti-dsDNA antibodies in absolute scale. Analyst 2018, 143, 3874–3882. [Google Scholar] [CrossRef]
- Vincent, F.B.; Morand, E.F.; Schneider, P.; Mackay, F. The BAFF/APRIL system in SLE pathogenesis. Nat. Rev. Rheumatol. 2014, 10, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Arévalo, B.; Blázquez-García, M.; Valverde, A.; Serafín, V.; Montero-Calle, A.; Solis-Fernandez, G.; Barderas, R.; Campuzano, S.; Yáñez-Sedeño, P.; Pingarrón, J.M. Binary MoS2 nanostructures as nanocarriers for amplification in multiplexed electrochemical immunosensing: Simultaneous determination of B cell activation factor and proliferation-induced signal immunity-related cytokines. Microchim. Acta 2022, 189, 143. [Google Scholar] [CrossRef]
- Arévalo, B.; Blázquez-García, M.; Valverde, A.; Serafín, V.; Montero-Calle, A.; Solís-Fernández, G.; Barderas, R.; Yáñez-Sedeño, P.; Campuzano, S.; Pingarrón, J. Simultaneous electrochemical immunosensing of relevant cytokines to diagnose and track cancer and autoimmune diseases. Bioelectrochemistry 2022, 146, 108157. [Google Scholar] [CrossRef] [PubMed]
- Puiu, M.; Idili, A.; Moscone, D.; Ricci, F.; Bala, C. A modular electrochemical peptide-based sensor for antibody detection. Chem. Commun. 2014, 50, 8962–8965. [Google Scholar] [CrossRef]
- González-López, A.; Blanco-López, M.C.; Fernández-Abedul, M.T. Micropipette tip-based immunoassay with electrochemical detection of antitissue transglutaminase to diagnose celiac disease using staples and a paper-based platform. ACS Sens. 2019, 4, 2679–2687. [Google Scholar] [CrossRef]
- Martín-Yerga, D.; Costa-García, A. Towards a blocking-free electrochemical immunosensing strategy for anti-transglutaminase antibodies using screen-printed electrodes. Bioelectrochemistry 2015, 105, 88–94. [Google Scholar] [CrossRef]
- Manfredi, A.; Mattarozzi, M.; Giannetto, M.; Careri, M. Piezoelectric immunosensor based on antibody recognition of immobilized open-tissue transglutaminase: An innovative perspective on diagnostic devices for celiac disease. Sens. Actuators B Chem. 2014, 201, 300–307. [Google Scholar] [CrossRef]
- Martín-Yerga, D.; Fanjul-Bolado, P.; Hernández-Santos, D.; Costa-García, A. Enhanced detection of quantum dots by the magnetohydrodynamic effect for electrochemical biosensing. Analyst 2017, 142, 1591–1600. [Google Scholar] [CrossRef]
- Nanni, P.I.; González-López, A.; Nunez-Bajo, E.; Madrid, R.E.; Fernández-Abedul, M.T. Staple-Based Paper Electrochemical Platform for Celiac Disease Diagnosis. ChemElectroChem 2018, 5, 4036–4045. [Google Scholar] [CrossRef]
- Cennamo, N.; Varriale, A.; Pennacchio, A.; Staiano, M.; Massarotti, D.; Zeni, L.; D’Auria, S. An innovative plastic optical fiber-based biosensor for new bio/applications. The case of celiac disease. Sens. Actuators B Chem. 2013, 176, 1008–1014. [Google Scholar] [CrossRef]
- Derkus, B.; Emregul, E.; Yucesan, C.; Emregul, K.C. Myelin basic protein immunosensor for multiple sclerosis detection based upon label-free electrochemical impedance spectroscopy. Biosens. Bioelectron. 2013, 46, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Mansourian, N.; Rahaie, M.; Hosseini, M. A Nanobiosensor Based on Fluorescent DNA-Hosted Silver Nanocluster and HCR Amplification for Detection of MicroRNA Involved in Progression of Multiple Sclerosis. J. Fluoresc. 2017, 27, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Chon, H.; Lee, S.; Wang, R.; Bang, S.Y.; Lee, H.S.; Bae, S.C.; Hong, S.H.; Yoon, Y.H.; Lim, D.; Choo, J. Highly sensitive immunoassay of anti-cyclic citrullinated peptide marker using surface-enhanced Raman scattering detection. In Proceedings of the International Conference on Nano-Bio Sensing, Imaging, and Spectroscopy, Jeju, Republic of Korea, 25–27 February 2015. [Google Scholar]
- Ma, J.; Li, D.; Sun, B.; Hou, X.; Zhang-Peng, X.; Li, W.; Zhang, Y.; Hu, F.; Shi, X. Label-free Electrochemical Immunosensor for Sensitive Detection of Rheumatoid Arthritis Biomarker Anti-CCP-ab. Electroanalysis 2022, 34, 761–771. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Biomarkers | Clinical Concentration Levels | References |
|---|---|---|---|
| Celiac disease | Anti-tTG antibodies | <7.0 U/mL: normal range Between 7.0 and 9.0 U/mL: weakly positive >9.0 U/mL: positive | [112,113] |
| Multiple sclerosis | IgG index | 0.7: the cut-off value of the IgG index >0.7: positive | [60] |
| MBP | <4 ng/mL: normal range of the MBP in CSF Between 4 and 8 ng/mL: chronic myelin disruption or recovery from a relapse >9 ng/mL: myelin damage at the moment | [36] | |
| IL-12 | 0–5.0 pg/mL normal range Between 5.5 and 18.6 pg/mL: positive | [36,114] | |
| Osteopontin | 63.74 ng/mL: normal value >63.74 ng/mL: positive | [115] | |
| Rheumatoid arthritis | RF | 0–20 IU/mL: normal range >20 IU/mL: positive | [116] |
| TNF-alpha | 24.47 pg/mL: normal value >24.47 pg/mL: positive | [117] | |
| Anti-CCP-ab | <20 IU/mL: normal value >20 IU/mL: positive | [118] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teniou, A.; Rhouati, A.; Marty, J.-L. Recent Advances in Biosensors for Diagnosis of Autoimmune Diseases. Sensors 2024, 24, 1510. https://doi.org/10.3390/s24051510
Teniou A, Rhouati A, Marty J-L. Recent Advances in Biosensors for Diagnosis of Autoimmune Diseases. Sensors. 2024; 24(5):1510. https://doi.org/10.3390/s24051510
Chicago/Turabian StyleTeniou, Ahlem, Amina Rhouati, and Jean-Louis Marty. 2024. "Recent Advances in Biosensors for Diagnosis of Autoimmune Diseases" Sensors 24, no. 5: 1510. https://doi.org/10.3390/s24051510
APA StyleTeniou, A., Rhouati, A., & Marty, J.-L. (2024). Recent Advances in Biosensors for Diagnosis of Autoimmune Diseases. Sensors, 24(5), 1510. https://doi.org/10.3390/s24051510