
The Use of Electrocardiogram Smartwatches in Patients with Cardiac Implantable Electrical Devices

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
3. Safety and Precautions for Use
4. Automatic Diagnosis of AF
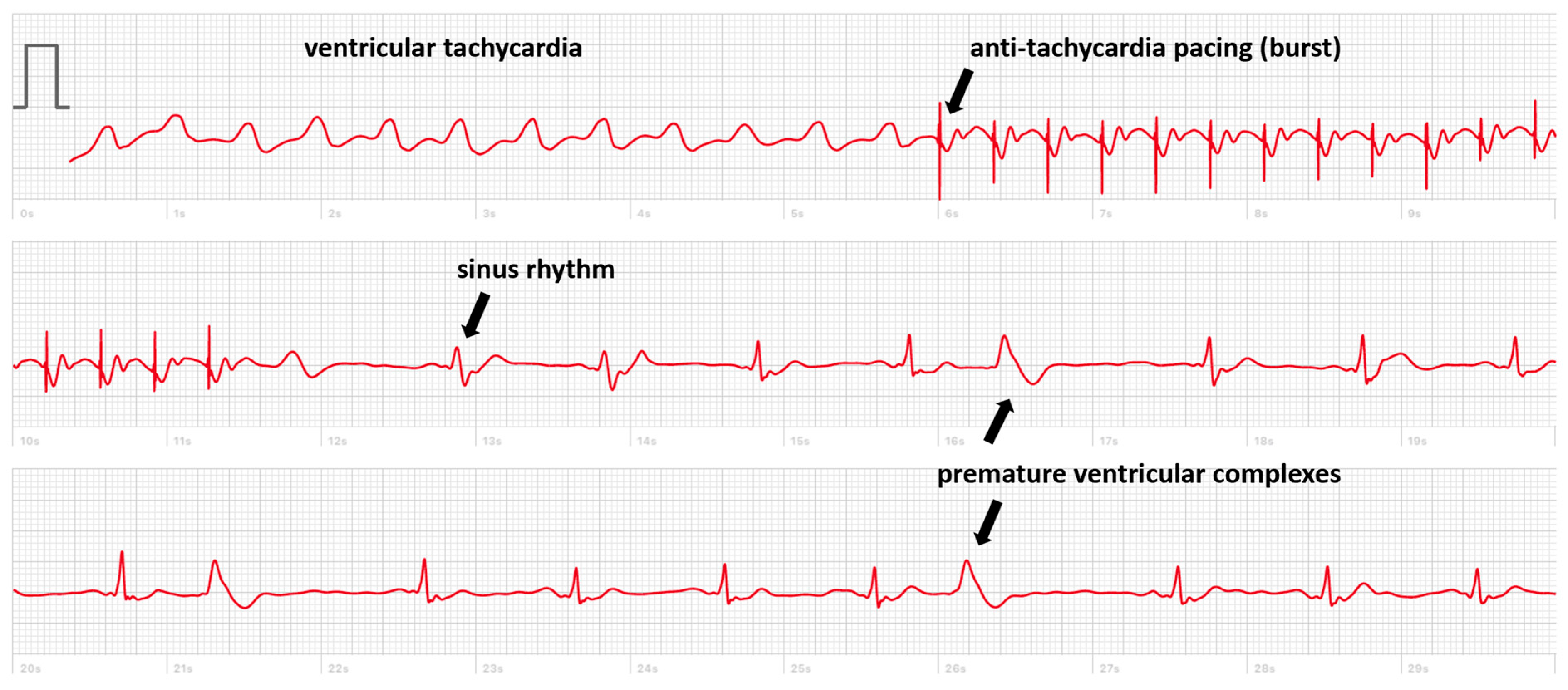
5. Diagnosis of Palpitations or Pre-Syncope
6. Smartwatches in Patients Implanted with a Leadless Pacemaker
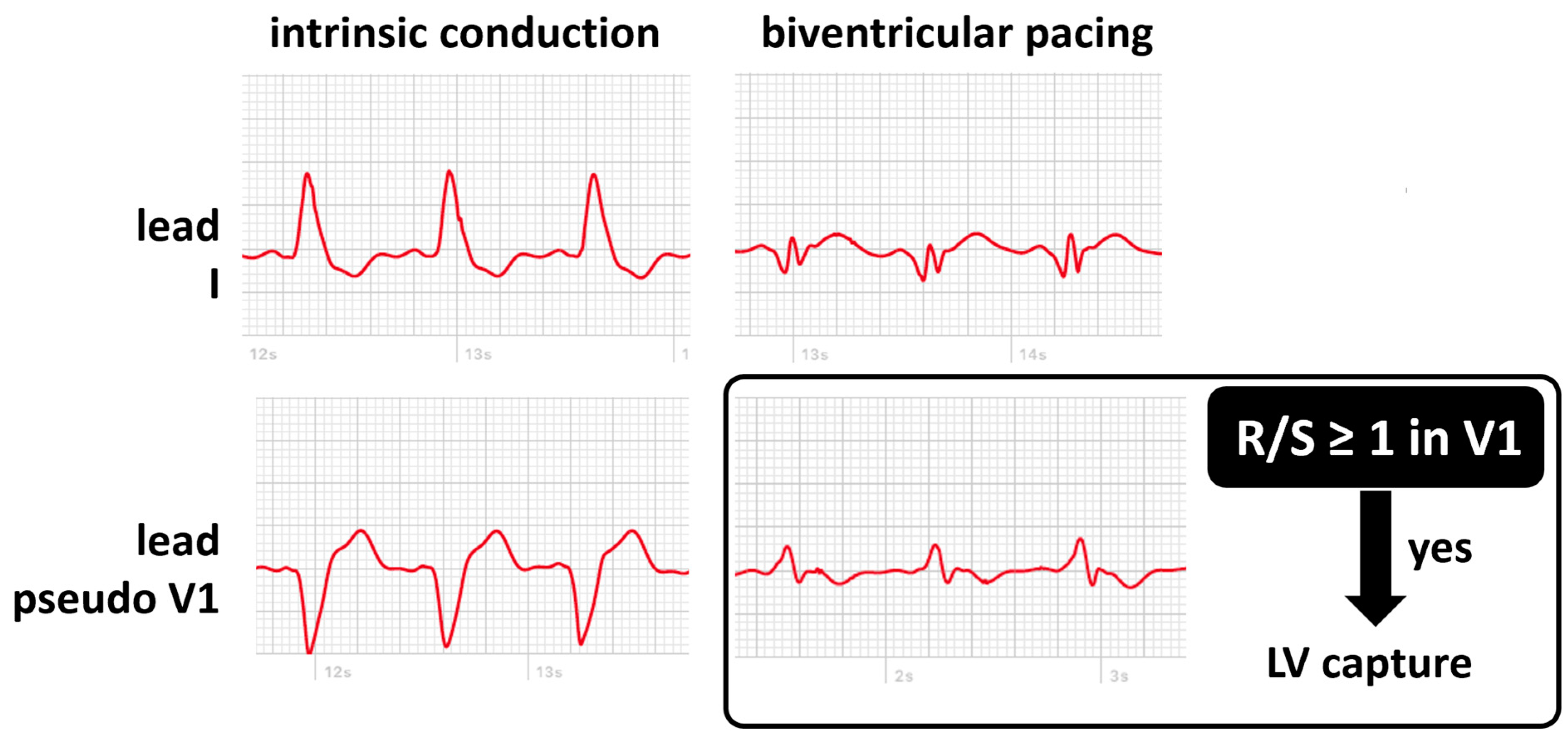
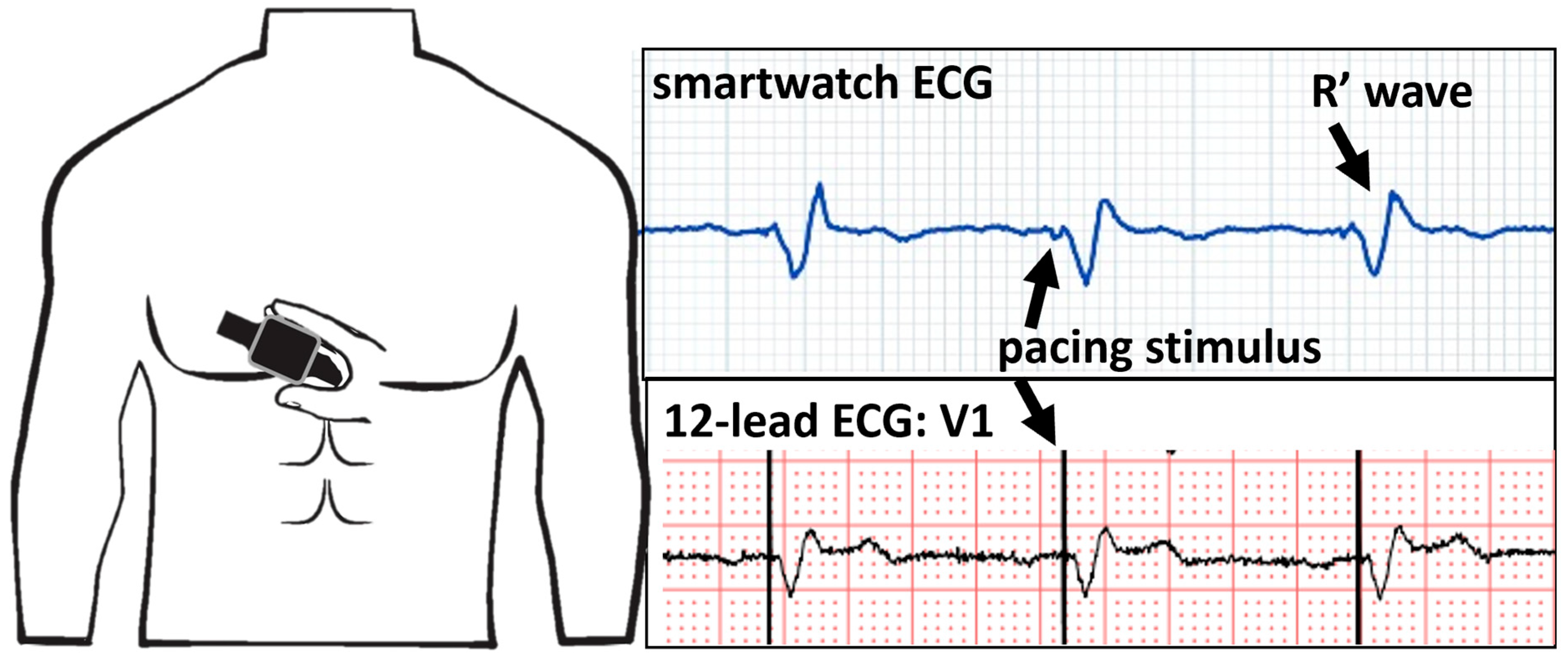
7. Using Smartwatches to Monitor Left Ventricular Capture
8. Smartwatches in Patients with Left Bundle Branch Area Pacing
9. Opportunities for CIED Remote Follow-Up
- Leadless pacemaker with atrial tracking (Micra AV, Medtronic or Aveir DR, Abbott): while the device interrogation reports the amount of ventricular pacing that is synchronized to the atrium, this figure may be incorrect and needs ECG verification. This holds true certainly in cases where atrioventricular synchrony is suboptimal.
- New pacing technologies such as left bundle branch area pacing are used more and more, but it is not clear whether automatic algorithms such as auto-threshold are reliable. The recording of a smartwatch ECG confirms capture.
- Single-chamber ICDs and subcutaneous ICDs now register an EGM when there is suspicion of atrial fibrillation. At the moment, these algorithms are only based on irregularity, which makes them unreliable with the occurrence of many false positives. The registration of the cardiac rhythm using a smartwatch ECG can aid in rejecting the diagnosis, avoiding unnecessary in-clinic investigation and inappropriate treatment (e.g., anticoagulation).
10. Smartwatch Applications beyond the ECG
- Heart rate monitoring: Most smartwatches come equipped with heart rate sensors that continuously monitor the heart rate using photoplethysmography. This can be useful for patients with pacemakers to ensure that their heart rate is within the desired range set by their healthcare provider. This is especially true in the case of patients with active rate modulation, in whom it is often difficult to find the correct settings for sensor sensitivity and rate-responsive aggressiveness. It is possible to obtain reliable heart rate curves with the use of photoplethysmography. Displayed heart rate at peak activity or even increases and decreases in the heart rate can provide very helpful information. Heart rate notifications: Some smartwatches can notify users if their heart rate goes above or below a certain threshold. This feature can be configured to alert patients if their heart rate exceeds safe limits, allowing them to seek medical attention if necessary.
- Activity tracking: Smartwatches can track daily activity levels, including steps taken, distance walked, and calories burned. Most PM and ICDs also have activity trackers based on the activation of the sensor, but this information is not readily available to the patient. Patients can use this data to monitor their overall physical health and ensure they are staying active within the limits recommended by their healthcare provider.
- Fall detection and emergency alerts: Many smartwatches include fall detection features that can automatically alert emergency services or a designated contact in case of a fall. This can be especially important for elderly patients with pacemakers who may be at a higher risk of falls.
- Medication and appointment reminders: Smartwatches can be used to set reminders for taking medications and attending medical appointments. This can help patients with pacemakers and ICDs adhere to their treatment plans.
- Sleep tracking: Monitoring sleep patterns can be important for overall health. Some smartwatches offer sleep-tracking features that can provide insights into sleep quality, which can indirectly impact cardiac health.
11. Future Directions
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strik, M.; Ploux, S.; Ramirez, F.D.; Abu-Alrub, S.; Jais, P.; Haïssaguerre, M.; Bordachar, P. Smartwatch-based detection of cardiac arrhythmias Beyond the differentiation between sinus rhythm and atrial fibrillation. Heart Rhythm 2021, 18, 1524–1532. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Ploux, S.; Weigel, D.; van der Zande, J.; Velraeds, A.; Racine, H.-P.; Ramirez, F.D.; Haïssaguerre, M.; Bordachar, P. The use of smartwatch electrocardiogram beyond arrhythmia detection. Trends Cardiovasc. Med. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- van der Zande, J.; Strik, M.; Dubois, R.; Ploux, S.; Alrub, S.A.; Caillol, T.; Nasarre, M.; Donker, D.W.; Oppersma, E.; Bordachar, P. Using a Smartwatch to Record Precordial Electrocardiograms: A Validation Study. Sensors 2023, 23, 2555. [Google Scholar] [CrossRef]
- Nasarre, M.; Strik, M.; Daniel Ramirez, F.; Buliard, S.; Marchand, H.; Abu-Alrub, S.; Ploux, S.; Haïssaguerre, M.; Bordachar, P. Using a smartwatch electrocardiogram to detect abnormalities associated with sudden cardiac arrest in young adults. Europace 2021, 24, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Welte, N.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Validating QT-Interval Measurement Using the Apple Watch ECG to Enable Remote Monitoring During the COVID-19 Pandemic. Circulation 2020, 142, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Zepeda-Echavarria, A.; Van De Leur, R.R.; Van Sleuwen, M.; Hassink, R.J.; Wildbergh, T.X.; Doevendans, P.A.; Jaspers, J.; Van Es, R. Electrocardiographic Devices for Home Use: A Technological and Clinical Scoping Review. JMIR Cardio 2023, 7, e44003. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Nadeem, F.; Tran, C.T.; Torbey, E.; Philbin, D.; Morales, C.; Wu, M. Interference by Modern Smartphones and Accessories with Cardiac Pacemakers and Defibrillators. Curr. Cardiol. Rep. 2022, 24, 347–353. [Google Scholar] [CrossRef]
- Hayes, D.L.; Wang, P.J.; Reynolds, D.W.; Estes, N.A.M.; Griffith, J.L.; Steffens, R.A.; Carlo, G.L.; Findlay, G.K.; Johnson, C.M. Interference with Cardiac Pacemakers by Cellular Telephones. N. Engl. J. Med. 1997, 336, 1473–1479. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Magnets in Cell Phones and Smart Watches May Affect Pacemakers and Other Implanted Medical Devices; FDA: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/radiation-emitting-products/cell-phones/magnets-cell-phones-and-smart-watches-may-affect-pacemakers-and-other-implanted-medical-devices (accessed on 1 December 2023).
- Burri, H.; Mondouagne Engkolo, L.P.; Dayal, N.; Etemadi, A.; Makhlouf, A.-M.; Stettler, C.; Trentaz, F. Low risk of electromagnetic interference between smartphones and contemporary implantable cardioverter defibrillators. Europace 2016, 18, 726–731. [Google Scholar] [CrossRef]
- Lacour, P.; Parwani, A.S.; Schuessler, F.; Hohendanner, F.; Heinzel, F.R.; Trippel, T.D.; Boldt, L.-H.; Pieske, B.; Blaschke, F. Are Contemporary Smartwatches and Mobile Phones Safe for Patients With Cardiovascular Implantable Electronic Devices? JACC Clin. Electrophysiol. 2020, 6, 1158–1166. [Google Scholar] [CrossRef]
- Tzeis, S.; Asvestas, D.; Moraitis, N.; Vardas, E.P.; Mililis, P.; Letsas, K.; Kouvelas, K.; Nikita, K.S.; Vardas, P. Safety of smartwatches and their chargers in patients with cardiac implantable electronic devices. Europace 2021, 23, 99–103. [Google Scholar] [CrossRef]
- Badertscher, P.; Vergne, C.; Féry, C.; Mannhart, D.; Quirin, T.; Osswald, S.; Kühne, M.; Sticherling, C.; Knecht, S.; Pascal, J. Magnetic field interactions of smartwatches and portable electronic devices with CIEDs—Did we open a Pandora’s box? Int. J. Cardiol. Heart Vasc. 2022, 43, 101122. [Google Scholar] [CrossRef] [PubMed]
- Ha, G.-B.; Steinberg, B.A.; Freedman, R.; Bayés-Genís, A.; Sanchez, B. Safety evaluation of smart scales, smart watches, and smart rings with bioimpedance technology shows evidence of potential interference in cardiac implantable electronic devices. Heart Rhythm 2023, 20, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Lapsa, D.; Janeliukstis, R.; Elsts, A. Adaptive Signal-to-Noise Ratio Indicator for Wearable Bioimpedance Monitoring. Sensors 2023, 23, 8532. [Google Scholar] [CrossRef]
- Reitan, R.; Mouchawar, G.; Stadnik, P.; Kippola, J.; Seidman, S.; Peltier, J.; Shein, M.; Stevenson, R. To the Editor—Safety of wearable bioimpedance monitors for CIED patients remains unknown. Heart Rhythm 2023, 20, 1341–1342. [Google Scholar] [CrossRef]
- Greenberg, J.C.; Altawil, M.R.; Singh, G. Letter to the Editor—Lifesaving therapy inhibition by phones containing magnets. Heart Rhythm 2021, 18, 1040–1041. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, F.; Nunez Garcia, A.; Thach Tran, C.; Wu, M. Magnetic Interference on Cardiac Implantable Electronic Devices From Apple iPhone MagSafe Technology. J. Am. Heart Assoc. 2021, 10, e020818. [Google Scholar] [CrossRef]
- Apple Support [Internet]. About Potential Magnetic Interference with Medical Devices. Available online: https://support.apple.com/en-us/HT211900 (accessed on 29 September 2023).
- Patel, H.; Whitler, C.; Foster, N.; Bradley, C.; Shah, D.; Machado, C. Implantable Cardioverter-defibrillator Magnetic Interference by the iPhone 12: Is It Clinically Significant? J. Innov. Card. Rhythm Manag. 2022, 13, 5070–5072. [Google Scholar] [CrossRef]
- Asher, E.B.; Panda, N.; Tran, C.T.; Wu, M. Smart wearable device accessories may interfere with implantable cardiac devices. Hear. Case Rep. 2021, 7, 167–169. [Google Scholar] [CrossRef]
- Wolber, T.; Ryf, S.; Binggeli, C.; Holzmeister, J.; Brunckhorst, C.; Luechinger, R.; Duru, F. Potential interference of small neodymium magnets with cardiac pacemakers and implantable cardioverter-defibrillators. Heart Rhythm 2007, 4, 1–4. [Google Scholar] [CrossRef]
- Abu-Alrub, S.; Strik, M.; Ramirez, F.D.; Moussaoui, N.; Racine, H.P.; Marchand, H.; Buliard, S.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Smartwatch Electrocardiograms for Automated and Manual Diagnosis of Atrial Fibrillation: A Comparative Analysis of Three Models. Front. Cardiovasc. Med. 2022, 9, 836375. [Google Scholar] [CrossRef]
- Wasserlauf, J.; You, C.; Patel, R.; Valys, A.; Albert, D.; Passman, R. Smartwatch Performance for the Detection and Quantification of Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2019, 12, e006834. [Google Scholar] [CrossRef] [PubMed]
- Wasserlauf, J.; Vogel, K.; Whisler, C.; Benjamin, E.; Helm, R.; Steinhaus, D.A.; Yousuf, O.; Passman, R.S. Accuracy of the Apple watch for detection of AF: A multicenter experience. J. Cardiovasc. Electrophysiol. 2023, 34, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Doshi, A.M.; Ebert, R.M.; Grinnell, J.D.; Saxon, L.A. Consumer-facing Diagnostic Sensors in a Patient with Implantable Cardioverter-Defibrillator. J. Innov. Card. Rhythm Manag. 2019, 10, 3822–3825. [Google Scholar] [CrossRef] [PubMed]
- Racine, H.-P.; Strik, M.; van der Zande, J.; Alrub, S.A.; Caillol, T.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Role of Coexisting ECG Anomalies in the Accuracy of Smartwatch ECG Detection of Atrial Fibrillation. Can. J. Cardiol. 2022, 38, 1709–1712. [Google Scholar] [CrossRef] [PubMed]
- Dilaveris, P.E.; Antoniou, C.K.; Caiani, E.G.; Casado-Arroyo, R.; Climent, A.Μ.; Cluitmans, M.; Cowie, M.R.; Doehner, W.; Guerra, F.; Jensen, M.T.; et al. ESC Working Group on e-Cardiology Position Paper: Accuracy and reliability of electrocardiogram monitoring in the detection of atrial fibrillation in cryptogenic stroke patients: In collaboration with the Council on Stroke, the European Heart Rhythm Association, and the Digital Health Committee. Eur. Heart J. Digit. Health 2022, 3, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Take an ECG with the ECG App on Apple Watch—Apple Support. Available online: https://support.apple.com/en-us/HT208955 (accessed on 23 November 2023).
- Measure Your ECG with the Galaxy Watch Series|Samsung Caribbean. Available online: https://www.samsung.com/latin_en/support/mobile-devices/measure-your-ecg-with-the-galaxy-watch-series/ (accessed on 23 November 2023).
- What Is the Fitbit ECG App? Available online: https://help.fitbit.com/articles/en_US/Help_article/2457.htm (accessed on 23 November 2023).
- ECG App|Health Science|Garmin Technology|Garmin. Available online: https://www.garmin.com/en-US/garmin-technology/health-science/ecg/ (accessed on 23 November 2023).
- ScanWatch—Understanding My ECG Recordings—Withings|Support. Available online: https://support.withings.com/hc/en-us/articles/360009959537-ScanWatch-Understanding-my-ECG-recordings (accessed on 23 November 2023).
- Gu, K.; Marshall, K.; Robertson-Stovel, Q.; Zieroth, S. Polymorphic Ventricular Tachycardia Detected With a Smartwatch. CJC Open 2022, 4, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Fan, J.; Guo, Y.; Dai, H.; Xu, J.; Wang, L.; Hu, P.; Lin, X.; Li, C.; Zhou, D.; et al. Wearable Smartwatch Facilitated Remote Health Management for Patients Undergoing Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2022, 11, e023219. [Google Scholar] [CrossRef]
- Fan, J.; Liu, X.; Xu, Y.; Xu, J.; Wang, J. Smartwatch detected high-degree atrioventricular block requiring pacemaker implantation after transcatheter aortic valve replacement during COVID-19. Eur. Heart J. Digit. Health 2021, 2, 545–546. [Google Scholar] [CrossRef]
- Lee, A.; Moss, J.D. Device rounds: Pacemaker 2:1 upper rate behavior—Two causes, one patient. Pacing Clin. Electrophysiol. 2018, 41, 1665–1668. [Google Scholar] [CrossRef]
- Strik, M.; Nicolas, C.; Mondoly, P.; Eschalier, R.; Ramirez, F.D.; Hugo-Pierre, R.; Haïssaguerre, M.; Ritter, P.; Ploux, S.; Pierre, B. Implantation of a leadless pacemaker in young adults. J. Cardiovasc. Electrophysiol. 2023, 34, 412–417. [Google Scholar] [CrossRef]
- Chinitz, L.; Ritter, P.; Khelae, S.K.; Iacopino, S.; Garweg, C.; Grazia-Bongiorni, M.; Neuzil, P.; Johansen, J.B.; Mont, L.; Gonzalez, E.; et al. Accelerometer-based atrioventricular synchronous pacing with a ventricular leadless pacemaker: Results from the Micra atrioventricular feasibility studies. Heart Rhythm 2018, 15, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Lenormand, T.; Abou Khalil, K.; Bodin, A.; Babuty, D.; Bisson, A.; Clementy, N. Comparison of first- and second-generation leadless pacemakers in patients with sinus rhythm and complete atrioventricular block. J. Cardiovasc. Electrophysiol. 2023, 34, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Ammann, P.; Sticherling, C.; Kalusche, D.; Eckstein, J.; Bernheim, A.; Schaer, B.; Osswald, S. An electrocardiogram-based algorithm to detect loss of left ventricular capture during cardiac resynchronization therapy. Ann. Intern. Med. 2005, 142, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Mannhart, D.; Badertscher, P.; Serban, T.; Kühne, M.; Ammann, P.; Sticherling, C. Using a smartwatch for the detection of loss of left ventricular capture in patients receiving cardiac resynchronization therapy. Heart Rhythm 2023, 20, 146–148. [Google Scholar] [CrossRef]
- Wan, E.Y.; Ghanbari, H.; Akoum, N.; Itzhak Attia, Z.; Asirvatham, S.J.; Chung, E.H.; Dagher, L.; Al-Khatib, S.M.; Stuart Mendenhall, G.; McManus, D.D.; et al. HRS White Paper on Clinical Utilization of Digital Health Technology. Cardiovasc. Digit. Health J. 2021, 2, 196–211. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspect | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
|---|---|---|---|---|---|---|
| Price range | USD 399–USD 799 [30] | USD 249–USD 329 [31] | USD 199–USD 249 [32] | USD 349 [33] | USD 349 [32] | USD 299–USD 499 [34] |
| Sensitivity/specificity for diagnosing AF [24,25] | 85–87%/75–86% | 85–88%/75–81% | 66%/79% | Not available | Not available | 58–78%/75–80% |
| Limit of heart rate for interpretation | 50–150 beats/min | 50–120 beats/min | 50–120 beats/min | 50–120 beats/min | 50–120 beats/min | 50–100 beats/min |
| Battery life | 18 h | 45 h | 144 h | 9 days | 24 h | 30 days |
| Water resistance | 50 m–100 m | 50 m | 50 m | 50 m | 50 m | 50 m |
| Health features | ECG, SpO2, fitness rings, fall detection | ECG, SpO2, stress tracking | ECG, SpO2, stress tracking | ECG, SpO2, body energy | ECG, SpO2, stress tracking | ECG, SpO2, breathing, temperature |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strik, M.; Ploux, S.; Zande, J.v.d.; Velraeds, A.; Fontagne, L.; Haïssaguerre, M.; Bordachar, P. The Use of Electrocardiogram Smartwatches in Patients with Cardiac Implantable Electrical Devices. Sensors 2024, 24, 527. https://doi.org/10.3390/s24020527
Strik M, Ploux S, Zande Jvd, Velraeds A, Fontagne L, Haïssaguerre M, Bordachar P. The Use of Electrocardiogram Smartwatches in Patients with Cardiac Implantable Electrical Devices. Sensors. 2024; 24(2):527. https://doi.org/10.3390/s24020527
Chicago/Turabian StyleStrik, Marc, Sylvain Ploux, Joske van der Zande, Anouk Velraeds, Leslie Fontagne, Michel Haïssaguerre, and Pierre Bordachar. 2024. "The Use of Electrocardiogram Smartwatches in Patients with Cardiac Implantable Electrical Devices" Sensors 24, no. 2: 527. https://doi.org/10.3390/s24020527
APA StyleStrik, M., Ploux, S., Zande, J. v. d., Velraeds, A., Fontagne, L., Haïssaguerre, M., & Bordachar, P. (2024). The Use of Electrocardiogram Smartwatches in Patients with Cardiac Implantable Electrical Devices. Sensors, 24(2), 527. https://doi.org/10.3390/s24020527