
Reducing Driving Risk Factors in Adolescents with Attention Deficit Hyperactivity Disorder (ADHD): Insights from EEG and Eye-Tracking Analysis



Abstract
1. Introduction
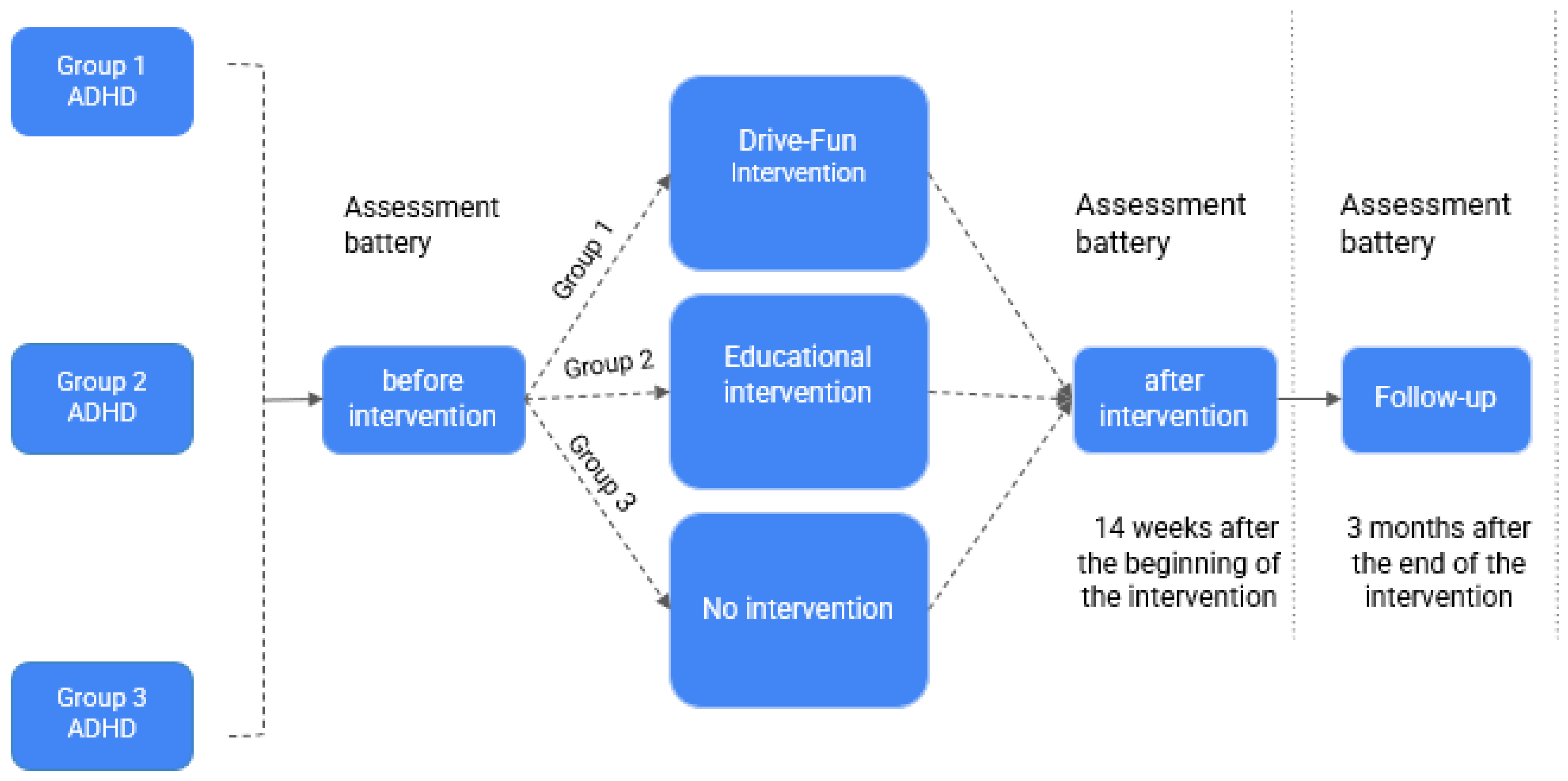
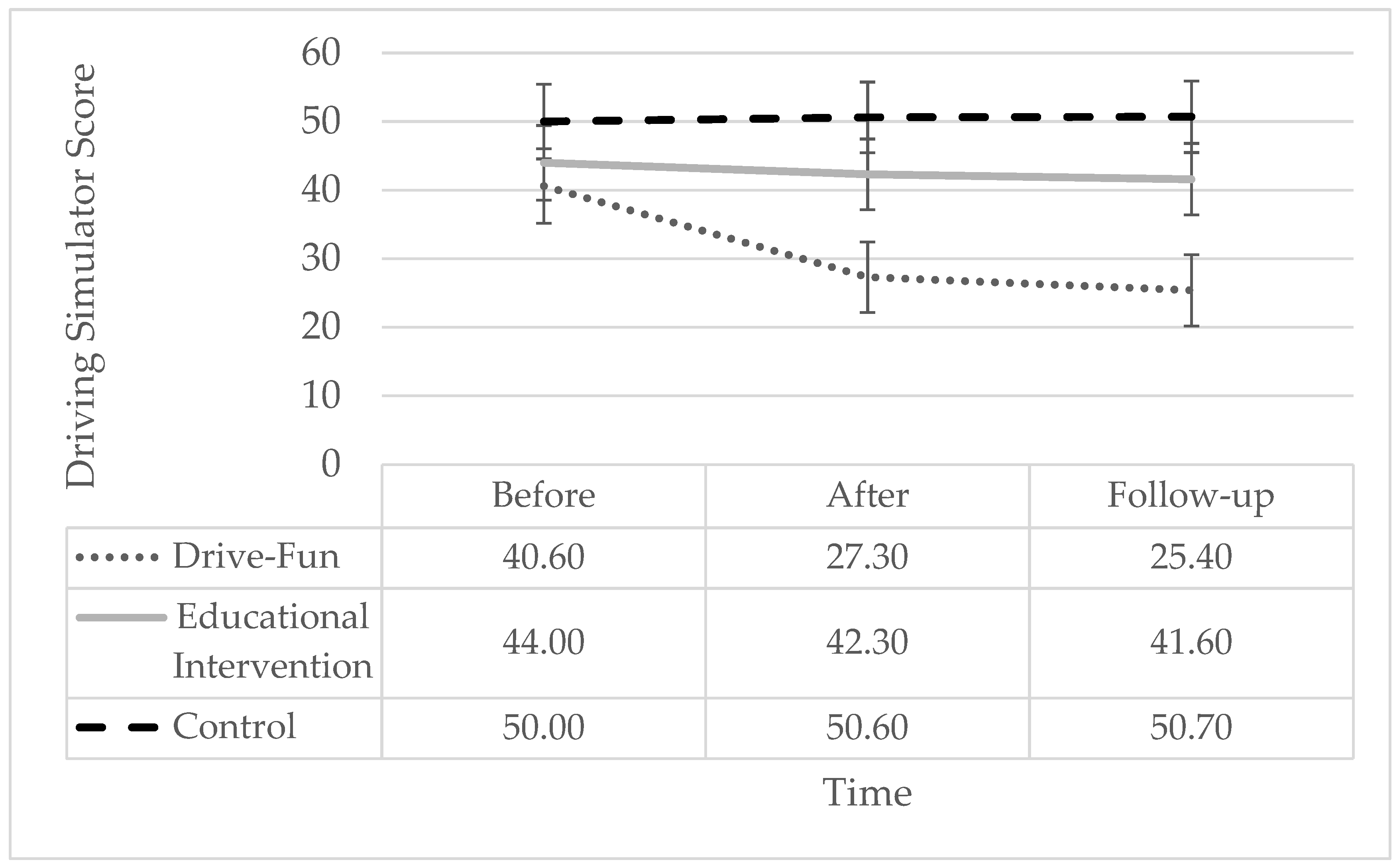
- There will be a statistically significant difference in simulator driving grades between the Drive-Fun participants and the control groups, as measured by the 3D-Fahrschule simulator, after the 14-week intervention and again at a three-month follow-up;
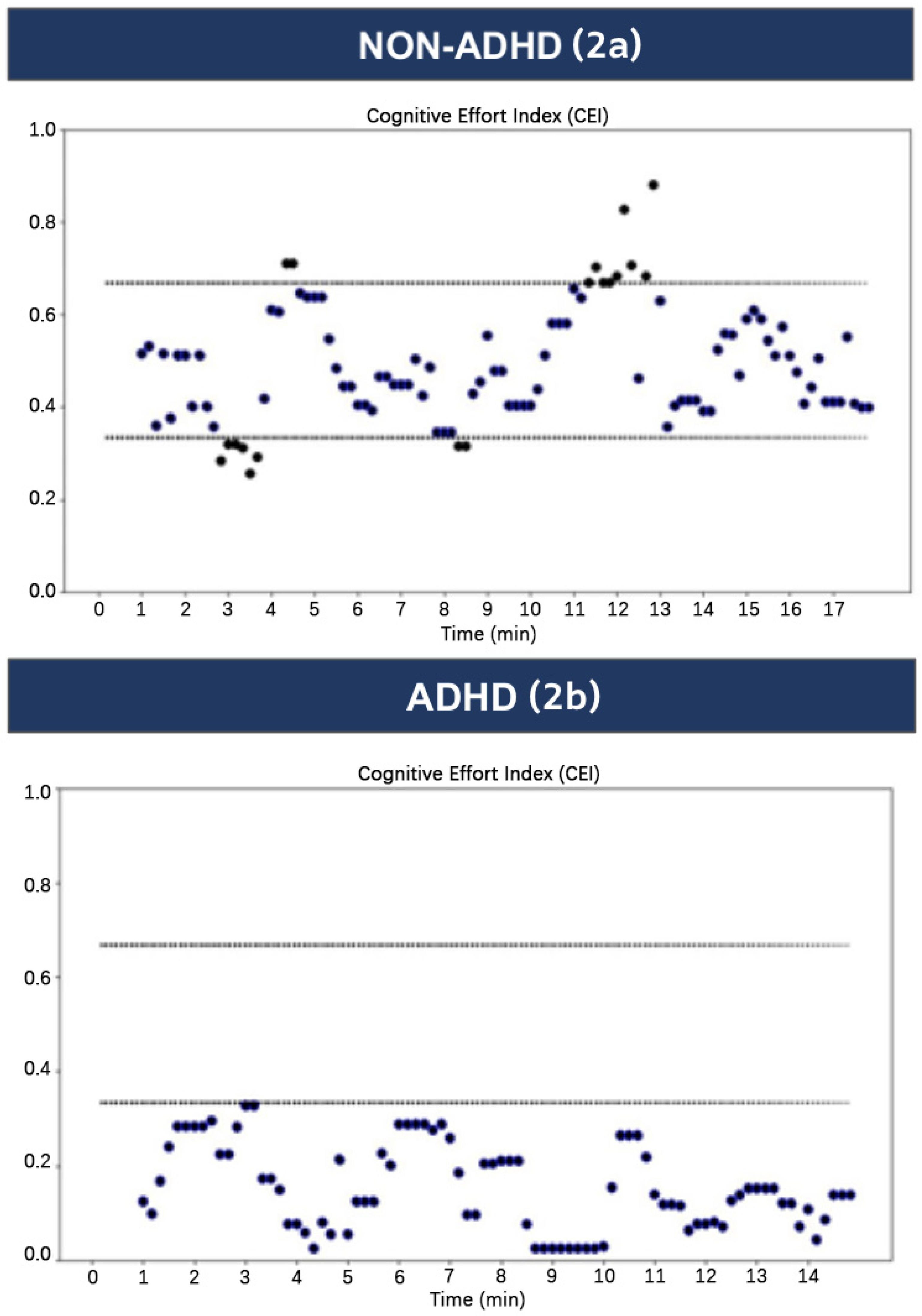
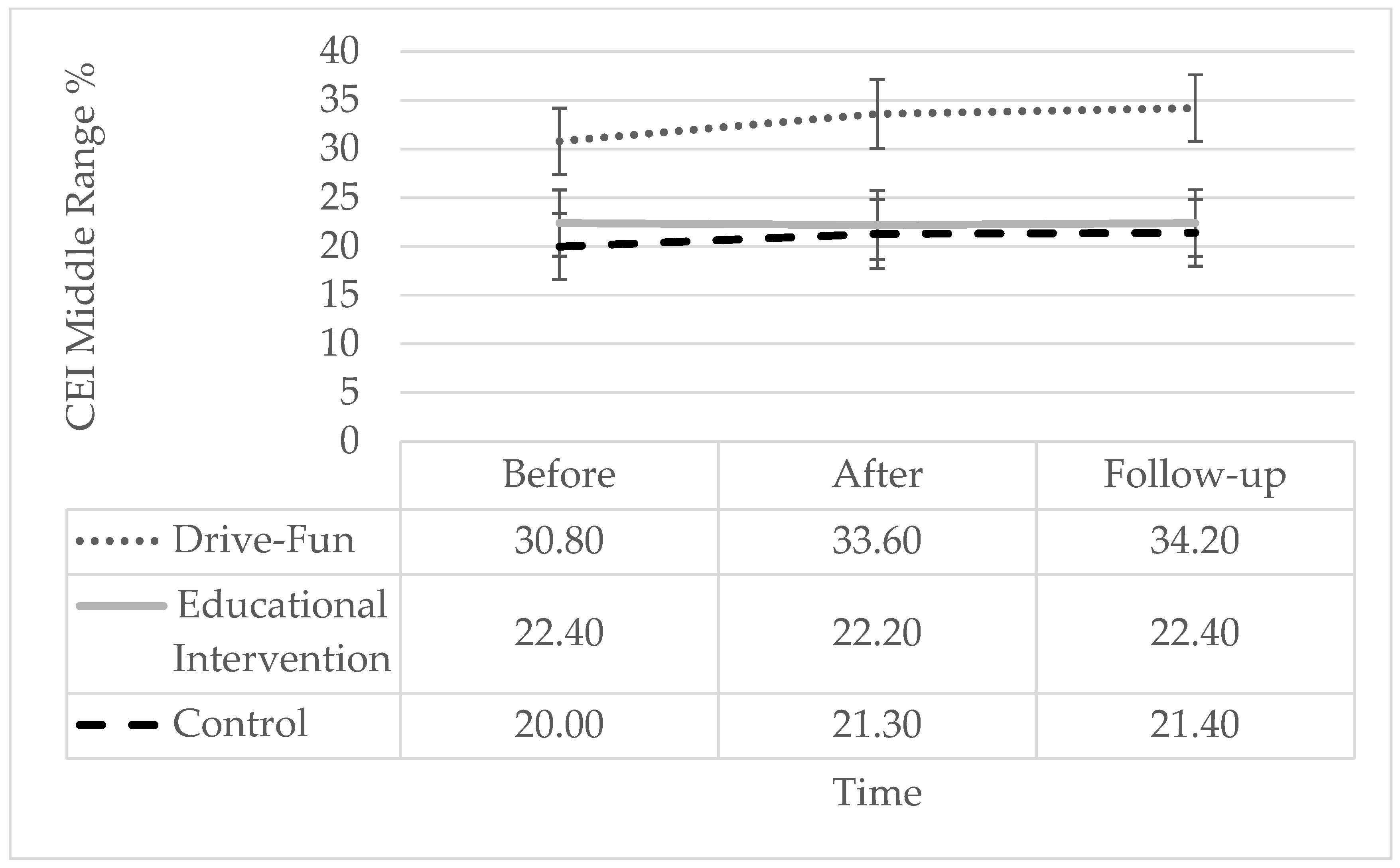
- There will be a statistically significant difference in the middle-range CEI score percentages, as measured by the CEI index, between the Drive-Fun participants and the control groups while driving on a simulator. This difference will be assessed after the 14-week intervention and again at a three-month follow-up;
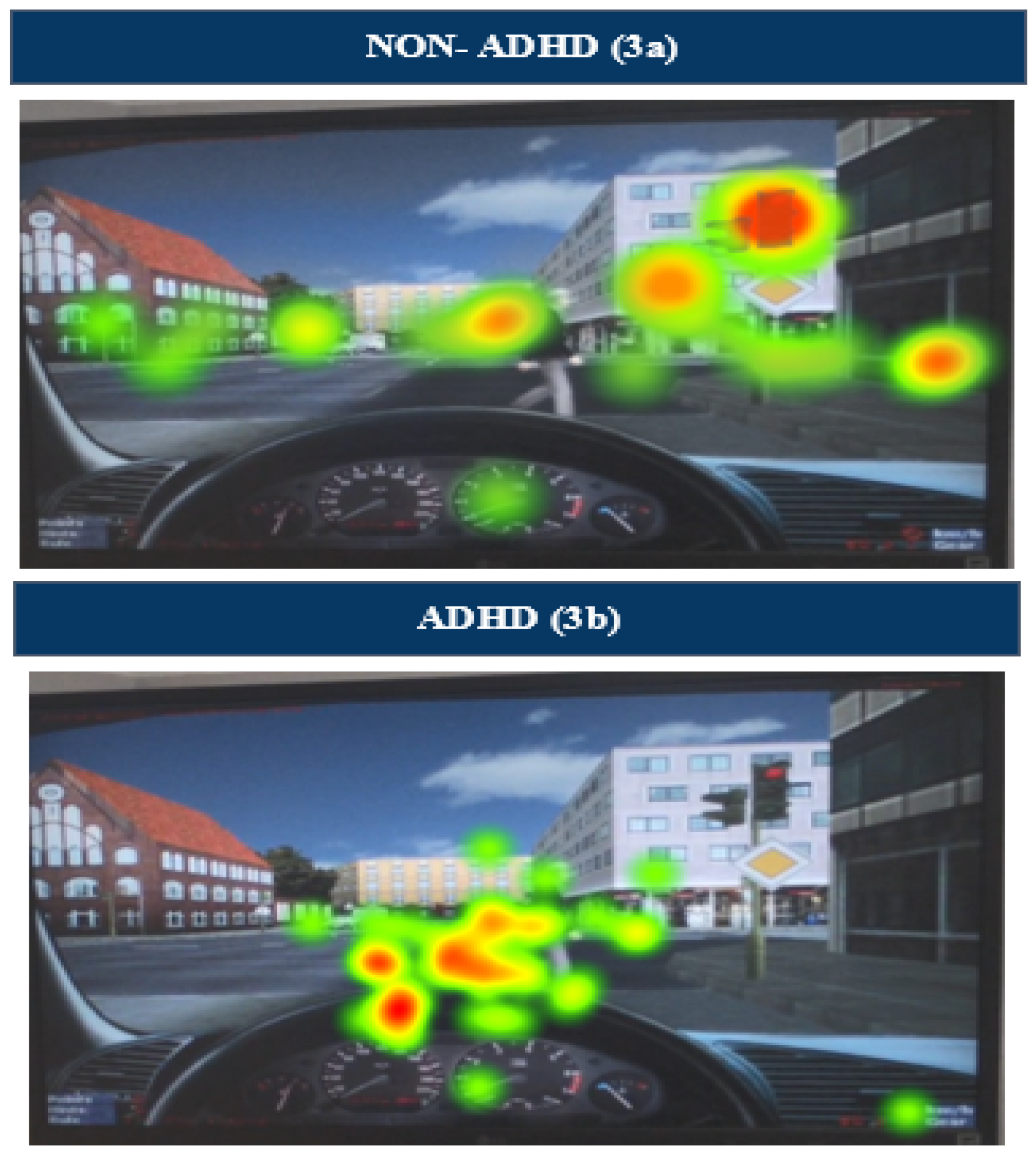
- There will be a statistically significant difference in the focused gaze time on the dashboard between the Drive-Fun participants and the control groups, as measured by the Tobii Pro Glasses 2 eye-tracking device. This difference will be assessed after the 14-week intervention and again at a three-month follow-up.
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolraich, M.; Hagan, J.; Allan, C. Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deicit/Hyperactivity Disorder in Children and Adolescents. Pediatrics 2019, 144, e20192528, Erratum in Pediatrics 2020, 145, e20193997. https://doi.org/10.1542/peds.2019-3997. [Google Scholar] [CrossRef]
- Lambez, B.; Harwood-Gross, A.; Golumbic, E.Z.; Rassovsky, Y. Non-Pharmacological Interventions for Cognitive Difficulties in ADHD: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2020, 120, 40–55. [Google Scholar] [CrossRef]
- Shalev, L.; Mevorach, C.; Tsal, Y. The Various Attention Deficits in Adult-ADHD and Their Relation to Driving Behavior. J. Vis. 2010, 8, 778. [Google Scholar] [CrossRef]
- Fuermaier, A.B.M.; Tucha, L.; Koerts, J.; Aschenbrenner, S.; Weisbrod, M.; Lange, K.W.; Tucha, O. Cognitive Complaints of Adults with Attention Deficit Hyperactivity Disorder. Clin. Neuropsychol. 2014, 28, 1104–1122. [Google Scholar] [CrossRef]
- Goldstick, J.E.; Cunningham, R.M.; Carter, P.M. Current Causes of Death in Children and Adolescents in the United States. N. Engl. J. Med. 2022, 386, 1955–1956. [Google Scholar] [CrossRef]
- Vaa, T. ADHD and Relative Risk of Accidents in Road Traffic: A Meta-Analysis. Accid. Anal. Prev. 2014, 62, 415–425. [Google Scholar] [CrossRef]
- Stavrinos, D.; Yang, G.; Kerwin, T.; McManus, B.; Bell, T.R.; Newton, A.; Singichetti, B. Driving Simulator Performance in the Acute Post-Injury Phase Following a Mild Traumatic Brain Injury Among Young Drivers. In Proceedings of the 10th International Driving Symposium on Human Factors in Driver Assessment, Training and Vehicle Design: Driving Assessment 2019, University of Iowa, Santa Fe, NM, USA, 26 June 2019; pp. 168–174. [Google Scholar]
- Lucidi, F.; Girelli, L.; Chirico, A.; Alivernini, F.; Cozzolino, M.; Violani, C.; Mallia, L. Personality Traits and Attitudes Toward Traffic Safety Predict Risky Behavior Across Young, Adult, and Older Drivers. Front. Psychol. 2019, 10, 536. [Google Scholar] [CrossRef]
- Road Traffic Injuries. Available online: https://www.who.int/news-room/fact-sheets/detail/road-traffic-injuries (accessed on 8 April 2024).
- Zamani Sani, S.H.; Fathirezaie, Z.; Sadeghi-Bazargani, H.; Badicu, G.; Ebrahimi, S.; Grosz, R.W.; Sadeghi Bahmani, D.; Brand, S. Driving Accidents, Driving Violations, Symptoms of Attention-Deficit-Hyperactivity (ADHD) and Attentional Network Tasks. Int. J. Environ. Res. Public Health 2020, 17, 5238. [Google Scholar] [CrossRef]
- Sahebi, S.; Nassiri, H.; Naderi, H. A Study of the Factors Affecting Driving Risk Perception Using the Bivariate Ordered Probit Model. Int. J. Inj. Control Saf. Promot. 2023, 30, 172–184. [Google Scholar] [CrossRef]
- Albright, M.G. Trajectories of Teen Driver Self-Regulation: Role of Learner Phase Practice and Executive Function. Master’s Thesis, The University of Alabama at Birmingham, Birmingham, AL, USA, 2020. [Google Scholar]
- Depestele, S.; Ross, V.; Verstraelen, S.; Brijs, K.; Brijs, T.; Van Dun, K.; Meesen, R. The Impact of Cognitive Functioning on Driving Performance of Older Persons in Comparison to Younger Age Groups: A Systematic Review. Transp. Res. Part F Traffic Psychol. Behav. 2020, 73, 433–452. [Google Scholar] [CrossRef]
- Brunkhorst-Kanaan, N.; Libutzki, B.; Reif, A.; Larsson, H.; McNeill, R.V.; Kittel-Schneider, S. ADHD and Accidents over the Life Span—A Systematic Review. Neurosci. Biobehav. Rev. 2021, 125, 582–591. [Google Scholar] [CrossRef]
- Lengenfelder, J.; Schultheis, M.T.; Al-Shihabi, T.M.; Mourant, R.; DeLuca, J. Divided Attention and Driving: A Pilot Study Using Virtual Reality Technology. J. Head Trauma Rehabil. 2002, 17, 26–37. [Google Scholar] [CrossRef]
- Pollak, Y.; Dekkers, T.J.; Shoham, R.; Huizenga, H.M. Risk-Taking Behavior in Attention Deficit/Hyperactivity Disorder (ADHD): A Review of Potential Underlying Mechanisms and of Interventions. Curr. Psychiatry Rep. 2019, 21, 33. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.L.; Molina, B.S.G.; Pelham, W.; Gnagy, E.M. Risky Driving in Adolescents and Young Adults with Childhood ADHD. J. Pediatr. Psychol. 2007, 32, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Jerome, L.; Segal, A.; Habinski, L. What We Know about ADHD and Driving Risk: A Literature Review, Meta-Analysis and Critique. J. Can. Acad. Child Adolesc. Psychiatry 2006, 15, 105–125. [Google Scholar] [PubMed]
- Barkley, R.A.; Cox, D. A Review of Driving Risks and Impairments Associated with Attention-Deficit/Hyperactivity Disorder and the Effects of Stimulant Medication on Driving Performance. J. Saf. Res. 2007, 38, 113–128. [Google Scholar] [CrossRef]
- Boland, H.; DiSalvo, M.; Fried, R.; Woodworth, K.Y.; Wilens, T.; Faraone, S.V.; Biederman, J. A Literature Review and Meta-Analysis on the Effects of ADHD Medications on Functional Outcomes. J. Psychiatr. Res. 2020, 123, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Olesen, A.V.; Madsen, T.K.O.; Lahrmann, H.; Nielsen, J. Use of Psychotropic Medication and Risk of Road Traffic Crashes: A Registry-Based Case–Control Study in Denmark, 1996–2018. Psychopharmacology 2022, 239, 2537–2546. [Google Scholar] [CrossRef]
- Romo, L.; Julien Sweerts, S.; Ordonneau, P.; Blot, E.; Gicquel, L. Road Accidents in Young Adults with ADHD: Which Factors Can Explain the Occurrence of Injuries in Drivers with ADHD and How to Prevent It? Appl. Neuropsychol. Adult 2021, 28, 372–377. [Google Scholar] [CrossRef]
- Bednarz, H.M.; Stavrinos, D.; Svancara, A.M.; Sherrod, G.M.; McManus, B.; Deshpande, H.D.; Kana, R.K. Executive Function Brain Network Activation Predicts Driving Hazard Detection in ADHD. Brain Topogr. 2022, 35, 251–267. [Google Scholar] [CrossRef]
- Cutello, C.A.; Hellier, E.; Stander, J.; Hanoch, Y. Evaluating the Effectiveness of a Young Driver-Education Intervention: Learn2Live. Transp. Res. Part F Traffic Psychol. Behav. 2020, 69, 375–384. [Google Scholar] [CrossRef]
- Evans, S.W.; Owens, J.S.; Wymbs, B.T.; Ray, A.R. Evidence-Based Psychosocial Treatments for Children and Adolescents with Attention Deficit/Hyperactivity Disorder. J. Clin. Child Adolesc. Psychol. 2018, 47, 157–198. [Google Scholar] [CrossRef] [PubMed]
- Pelham, W.E.; Fabiano, G.A. Evidence-Based Psychosocial Treatments for Attention-Deficit/Hyperactivity Disorder. J. Clin. Child Adolesc. Psychol. 2008, 37, 184–214. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Waschbusch, D.A.; Willoughby, M.T.; Evans, S. The Efficacy, Safety, and Practicality of Treatments for Adolescents with Attention-Deficit/Hyperactivity Disorder (ADHD). Clin. Child Fam. Psychol. Rev. 2000, 3, 243–267. [Google Scholar] [CrossRef] [PubMed]
- Surman, C.B.H.; Fried, R.; Rhodewalt, L.; Boland, H. Do Pharmaceuticals Improve Driving in Individuals with ADHD? A Review of the Literature and Evidence for Clinical Practice. CNS Drugs 2017, 31, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, G.A.; Hulme, K.; Linke, S.; Nelson-Tuttle, C.; Pariseau, M.; Gangloff, B.; Lewis, K.; Pelham, W.E.; Waschbusch, D.A.; Waxmonsky, J.G.; et al. The Supporting a Teen’s Effective Entry to the Roadway (STEER) Program: Feasibility and Preliminary Support for a Psychosocial Intervention for Teenage Drivers With ADHD. Cogn. Behav. Pract. 2011, 18, 267–280. [Google Scholar] [CrossRef]
- French, B.; Sayal, K.; Daley, D. Barriers and Facilitators to Understanding of ADHD in Primary Care: A Mixed-Method Systematic Review. Eur. Child Adolesc. Psychiatry 2019, 28, 1037–1064. [Google Scholar] [CrossRef]
- Levanon-Erez, N.; Kampf-Sherf, O.; Maeir, A. Occupational Therapy Metacognitive Intervention for Adolescents with ADHD: Teen Cognitive-Functional (Cog-Fun) Feasibility Study. Br. J. Occup. Ther. 2019, 82, 618–629. [Google Scholar] [CrossRef]
- Levanon-Erez, N.; Maeir, A. The Teen Cog-Fun Model of Intervention for Adolescents with ADHD. In ADHD: A Transparent Impairment, Clinical, Daily-Life and Research Aspects in Diverse Populations; Berger, I., Maeir, A., Eds.; Nova Publishers: New York, NY, USA, 2014; pp. 17–34. ISBN 978-1-63321-047-9. [Google Scholar]
- Maeir, A.; Traub-Bar Ilan, R.; Kastner, L.; Fisher, O.; Levanon-Erez, N.; Hahn-Markowitz, J. An Integrative Cognitive-Functional (Cog-Fun) Intervention Model for Children’adolescents and Adults with ADHD. In Cognition, Occupation, and Participation across the Lifespan: Neuroscience, Neurorehabilitation, and Models of Intervention; AOTA Press: Philadelphia, PA, USA, 2018; pp. 335–351. [Google Scholar]
- Taylor, R.R. The Intentional Relationship: Occupational Therapy and Use of Self, 2nd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2020; ISBN 978-1-71964-177-7. [Google Scholar]
- Yuval-Greenberg, S.; Keren, A.; Hilo, R.; Paz, A.; Ratzon, N. Gaze Control During Simulator Driving in Adolescents with and Without Attention Deficit Hyperactivity Disorder. Am. J. Occup. Ther. 2019, 73, 7303345030p1–7303345030p8. [Google Scholar] [CrossRef]
- Shahaf, G.; Kuperman, P.; Bloch, Y.; Yariv, S.; Granovsky, Y. Monitoring Migraine Cycle Dynamics with an Easy-to-Use Electrophysiological Marker—A Pilot Study. Sensors 2018, 18, 3918. [Google Scholar] [CrossRef]
- Gvion, A.; Shahaf, G. Real-Time Monitoring of Barriers to Patient Engagement for Improved Rehabilitation: A Protocol and Representative Case Reports. Disabil. Rehabil. Assist. Technol. 2023, 18, 849–861. [Google Scholar] [CrossRef]
- Bartur, G.; Joubran, K.; Peleg-Shani, S.; Vatine, J.-J.; Shahaf, G. An EEG Tool for Monitoring Patient Engagement during Stroke Rehabilitation: A Feasibility Study. BioMed Res. Int. 2017, 2017, 9071568. [Google Scholar] [CrossRef]
- Karpin, H.; Misha, T.; Herling, N.T.; Bartur, G.; Shahaf, G. Bedside Patient Engagement Monitor for Rehabilitation in Disorders of Consciousness—Demonstrative Case-Reports. Disabil. Rehabil. Assist. Technol. 2022, 17, 539–548. [Google Scholar] [CrossRef]
- Shahaf, G.; Nitzan, U.; Erez, G.; Mendelovic, S.; Bloch, Y. Monitoring Attention in ADHD with an Easy-to-Use Electrophysiological Index. Front. Hum. Neurosci. 2018, 12, 32. [Google Scholar] [CrossRef]
- Wu, W.; Sun, W.; Wu, Q.M.J.; Zhang, C.; Yang, Y.; Yu, H.; Lu, B.-L. Faster Single Model Vigilance Detection Based on Deep Learning. IEEE Trans. Cogn. Dev. Syst. 2021, 13, 621–630. [Google Scholar] [CrossRef]
- Eye Tracking Software for Behavior Research. Available online: https://www.tobii.com/products/software/behavior-research-software/tobii-pro-lab/ (accessed on 13 May 2024).
- Goh, D.H.; Ang, R.P.; Tan, H.C. Strategies for Designing Effective Psychotherapeutic Gaming Interventions for Children and Adolescents. Comput. Hum. Behav. 2008, 24, 2217–2235. [Google Scholar] [CrossRef]
- Ozment, D.K. The Effectiveness of Using an Interactive Driving Simulator to Improve Driving Skills and Abilities for Teens and Young Adults with Autism Spectrum Disorder within the Context of a Driving Bootcamp. Master’s Thesis, East Carolina University, Greenville, NC, USA, 2016. [Google Scholar]
- Williams, R.M.; Alikhademi, K.; Gilbert, J.E. Design of a Toolkit for Real-Time Executive Function Assessment in Custom-Made Virtual Experiences and Interventions. Int. J. Hum. Comput. Stud. 2022, 158, 102734. [Google Scholar] [CrossRef]
- Hayes, S.C.; Hofmann, S.G. “Third-wave” Cognitive and Behavioral Therapies and the Emergence of a Process-Based Approach to Intervention in Psychiatry. World Psychiatry 2021, 20, 363–375. [Google Scholar] [CrossRef]
- Gonzalez, A.J.; Wong, J.M.; Thomas, E.M.; Kerrigan, A.; Hastings, L.; Posadas, A.; Negy, K.; Wu, A.S.; Ontañon, S.; Lee, Y.-C.; et al. Detection of Driver Health Condition by Monitoring Driving Behavior through Machine Learning from Observation. Expert Syst. Appl. 2022, 199, 117167. [Google Scholar] [CrossRef]
- Krueger, R.A. Designing and Conducting Focus Group Interviews. 2002. Available online: https://www.eiu.edu/ihec/Krueger-FocusGroupInterviews.pdf (accessed on 15 August 2023).
- Movsisyan, A.; Arnold, L.; Evans, R.; Hallingberg, B.; Moore, G.; O’Cathain, A.; Pfadenhauer, L.M.; Segrott, J.; Rehfuess, E. Adapting Evidence-Informed Complex Population Health Interventions for New Contexts: A Systematic Review of Guidance. Implement. Sci. 2019, 14, 105. [Google Scholar] [CrossRef]
- Zhao, X.; Wu, Y.; Rong, J.; Zhang, Y. Development of a Driving Simulator Based Eco-Driving Support System. Transp. Res. Part C Emerg. Technol. 2015, 58, 631–641. [Google Scholar] [CrossRef]
- Ratzon, N.Z.; Lunievsky, E.K.; Ashkenasi, A.; Laks, J.; Cohen, H.A. Simulated Driving Skills Evaluation of Teenagers with Attention Deficit Hyperactivity Disorder Before Driving Lessons. Am. J. Occup. Ther. 2017, 71, 7103220010p1. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Gandolfi, F.; Marchesi, G.; Bellitto, A.; Basteris, A.; Canessa, A.; Massone, A.; Casadio, M. ADRIS: The New Open-Source Accessible Driving Simulator for Training and Evaluation of Driving Abilities. Comput. Methods Programs Biomed. 2022, 221, 106857. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.N.; Garner, A.A.; Kiefer, A.W.; Peugh, J.; Tamm, L.; MacPherson, R.P.; Simon, J.O.; Fisher, D.L. Trial of Training to Reduce Driver Inattention in Teens with ADHD. N. Engl. J. Med. 2022, 387, 2056–2066. [Google Scholar] [CrossRef] [PubMed]
- Shichrur, R.; Ratzon, N.Z. Convergent Validity of Vision Based Technology (VBT) among Professional Bus Drivers. J. Saf. Res. 2022, 82, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Mitsea, E.; Drigas, A.; Skianis, C. VR Gaming for Meta-Skills Training in Special Education: The Role of Metacognition, Motivations, and Emotional Intelligence. Educ. Sci. 2023, 13, 639. [Google Scholar] [CrossRef]
- Rief, S.F. How to Reach and Teach Children and Teens with ADD/ADHD; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016. [Google Scholar]
- Scott-Parker, B. Emotions, Behaviour, and the Adolescent Driver: A Literature Review. Transp. Res. Part F Traffic Psychol. Behav. 2017, 50, 1–37. [Google Scholar] [CrossRef]
- Bishop, H.; Boe, L.; Stavrinos, D.; Mirman, J. Driving among Adolescents with Autism Spectrum Disorder and Attention-Deficit Hyperactivity Disorder. Safety 2018, 4, 40. [Google Scholar] [CrossRef]
- Hulme, K.F.; Estes, A.; Schmid, M.; Torres, E.; Hendrick, C.; Sivashangaran, S. Game-Based Proving-Grounds Simulation to Assess Driving & Learning Preferences. In Proceedings of the Interservice/Industry Training, Simulation and Education Conference (I/ITSEC), Orlando, FL, USA, 26–30 November 2018; Volume 2. [Google Scholar]
- Parsons, T.D. Virtual Reality for Enhanced Ecological Validity and Experimental Control in the Clinical, Affective and Social Neurosciences. Front. Hum. Neurosci. 2015, 9, 660. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F | Df | p | Cohen | Power | ||
|---|---|---|---|---|---|---|
| Driving simulator score | Time | 12.02 | 2.26 | <0.001 | 0.48 | 0.99 |
| Group | 3.56 | 2.27 | 0.043 | 0.21 | 0.61 | |
| Time × Group | 7.28 | 4.52 | <0.001 | 0.36 | 0.99 | |
| CEI middle range value (%) | Time | 5.32 | 2.26 | 0.012 | 0.29 | 0.79 |
| Group | 3.63 | 2.27 | 0.040 | 0.21 | 0.62 | |
| Time × Group | 1.93 | 4.52 | 0.119 | 0.13 | 0.54 | |
| Focused gaze time on dashboard (%) | Time | 5.26 | 2.26 | 0.012 | 0.29 | 0.79 |
| Group | 2.66 | 2.27 | 0.088 | 0.17 | 0.48 | |
| Time × Group | 3.07 | 4.52 | 0.024 | 0.19 | 0.77 | |
| Focused gaze time on traffic light (%) | Time | 1.89 | 2.26 | 0.172 | 0.13 | 0.36 |
| Group | 1.46 | 2.27 | 0.251 | 0.10 | 0.28 | |
| Time × Group | 2.70 | 4.52 | 0.040 | 0.17 | 0.71 | |
| Focused gaze time on pedestrian (%) | Time | 3.17 | 2.26 | 0.059 | 0.20 | 0.56 |
| Group | 2.90 | 2.27 | 0.072 | 0.18 | 0.52 | |
| Time × Group | 1.93 | 4.52 | 0.120 | 0.13 | 0.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keren, A.; Fisher, O.; Hamde, A.; Tsafrir, S.; Ratzon, N.Z. Reducing Driving Risk Factors in Adolescents with Attention Deficit Hyperactivity Disorder (ADHD): Insights from EEG and Eye-Tracking Analysis. Sensors 2024, 24, 3319. https://doi.org/10.3390/s24113319
Keren A, Fisher O, Hamde A, Tsafrir S, Ratzon NZ. Reducing Driving Risk Factors in Adolescents with Attention Deficit Hyperactivity Disorder (ADHD): Insights from EEG and Eye-Tracking Analysis. Sensors. 2024; 24(11):3319. https://doi.org/10.3390/s24113319
Chicago/Turabian StyleKeren, Anat, Orit Fisher, Anwar Hamde, Shlomit Tsafrir, and Navah Z. Ratzon. 2024. "Reducing Driving Risk Factors in Adolescents with Attention Deficit Hyperactivity Disorder (ADHD): Insights from EEG and Eye-Tracking Analysis" Sensors 24, no. 11: 3319. https://doi.org/10.3390/s24113319
APA StyleKeren, A., Fisher, O., Hamde, A., Tsafrir, S., & Ratzon, N. Z. (2024). Reducing Driving Risk Factors in Adolescents with Attention Deficit Hyperactivity Disorder (ADHD): Insights from EEG and Eye-Tracking Analysis. Sensors, 24(11), 3319. https://doi.org/10.3390/s24113319