
Immersive Virtual Reality Reaction Time Test and Relationship with the Risk of Falling in Parkinson’s Disease




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
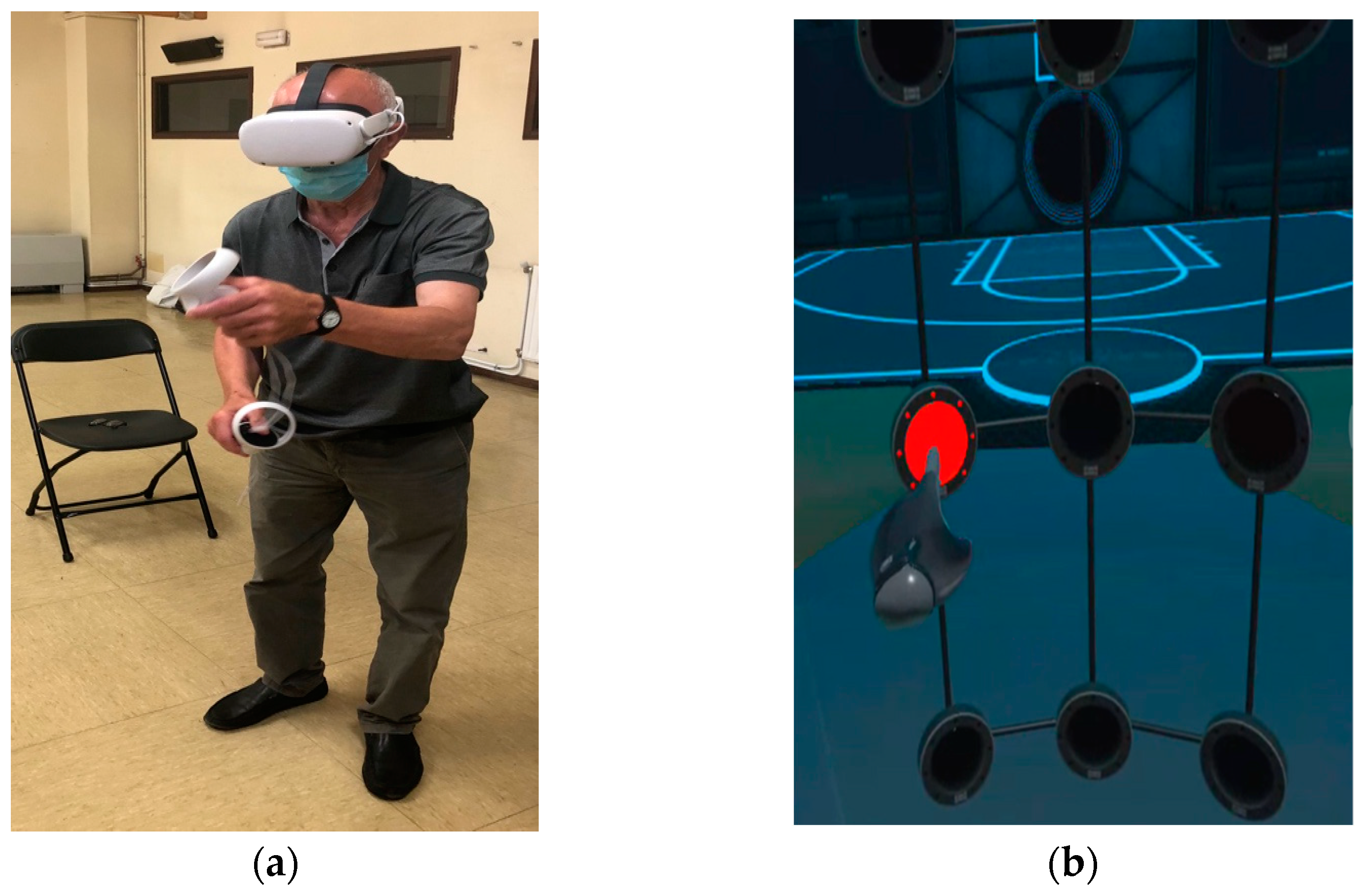
2.2. Virtual Reality Device
2.3. Virtual Reality Software and Procedure
2.4. Assessments
- Level of cognitive impairment. Cognitive ability was assessed with the mini-mental state examination (MMSE) scale [46]. The MMSE is a written test with a maximum score of 30, in which lower scores indicate more severe cognitive problems. The cut-off point established for the MMSE defines “normal” cognitive function is generally set at 24 and has been shown to be useful for the detection of dementia in older people [47].
- Functionality and functionality in dual tasks. These were evaluated with the classic timed up and go (TUG) test and a version of the same test with a cognitive component: the TUG-Cognitive task. All the participants completed both tests once. The TUG test was created and validated by Podsiadlo and Richardson [17] to assess functional mobility in the elderly. The test procedure consists of standing up from a seated position in a chair, walking a distance of 3 m, performing a 180 degree turn around a cone, then returning to the chair and sitting down again. The time taken to complete this task is recorded in seconds (taken by an evaluator using a stopwatch). The TUG-Cognitive task test is based on the dual-task paradigm, aims to quantify the influence of the cognitive sphere on a common functional task [19] and has already been used successfully in PD [20]. In our study, it was performed in the same way as the classic TUG test is, but this time the participants had to count down in threes from 51 while simultaneously performing the physical task (errors in the dual TUG answers were not considered a penalizing element in the test result).
- Risk of falling. This was evaluated with an ad hoc questionnaire about clinical characteristics (falls in the last three months) and according to the TUG test values following Podsiadlo and Richardson [17].
- Reaction time. This was evaluated with the Rezzil player software in the Micro wall mode available in the Oculus store (https://www.oculus.com, accessed on 15 November 2022). Participants had to react as quickly as possible to the random appearance of a red light on the presented grid. Participants made several attempts, and the best reaction time was recorded.
- The safety of the immersive experience was evaluated by the Simulator Sickness Questionnaire (SSQ), adapted and translated into Spanish [48]. The SSQ is an assessment tool used for recording the perceived severity of IVR simulator symptoms [49,50]. It comprises 16 items (e.g., nausea, headache, blurred vision, etc.) which are then divided into three subscales based on the type of symptoms experienced (nausea, oculomotor, and disorientation subscales). For each item, the severity of experienced discomfort is evaluated by the participant using a 4-point scale (1 for none, and 4 for severe).
2.5. Statistical Analysis
3. Results
4. Discussion
- Reaction times and cognitive impairment: these were moderately negatively correlated with MMSE scores (rho = −0.576; p = 0.002) and as could be expected, people with greater cognitive impairment showed slower response times, in line with the findings of other studies [36].
- Reaction times and functionality: these were moderately positively correlated in both tests, with the classic TUG (rho = 0.537; p = 0.005) and with the cognitive TUG (rho = 0.454; p = 0.020). As already mentioned, balance and the risk of falling seem to be related to the ability to respond quickly to a stimulus. This fact coincides with that expressed in the study by Arroyo-Ferrer et al. [55], in which they found that balance measured through limits of stability (LOS) was related simply to reaction time as measured by a computer. In our study, a slower reaction time conditioned lower levels of functionality and a higher risk of falls in patients with PD. This fact reinforces the idea of introducing cognitive strategies into programs based on physical exercise as has been carried in other studies aimed at treatments for cognitive impairment [56], PD [57] and atypical Parkinson’s [58] in order to strengthen their therapeutic effects.
- Reaction times and disease progression: there was a positive moderate correlation of (rho = 0.456; p = 0.019) with the non-faller vs. faller condition and a positive weak correlation with the age of the patients (rho = 0.399; p = 0.043), although not with the first symptom or the stage of the disease. These results might seem contradictory since, under normal conditions, older age could lead to worse performance in the reaction time test due simply to aging, or due to aging in conjunction with a degenerative disease. However, it is the stage of the disease that to a greater extent conditions disability and the severity of involvement, and in this case, there was no relationship. There was also no relationship with the first symptom, although a previous study with RVI tasks in PD has shown that if the first symptom was postural instability, the performance of virtual tasks was less well-executed [54]. In our case, and probably due to the short duration of the virtual tasks, this fact had no influence, although a certain relationship was found in the non-faller vs. faller condition, which was normally linked to the progression of the disease. More studies are needed to clarify this topic.
4.1. Practical Implications
4.2. Future Research
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Bloem, B.R. The Parkinson Pandemic—A Call to Action. JAMA Neurol. 2018, 75, 9. [Google Scholar] [CrossRef] [PubMed]
- Opara, J.; Małecki, A.; Małecka, E.; Socha, T. Motor Assessment in Parkinson’s Disease. Ann. Agric. Environ. Med. 2017, 24, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Park. Relat. Disord. 2016, 22 (Suppl. S1), S119–S122. [Google Scholar] [CrossRef]
- Shipley, B.A.; Deary, I.J.; Tan, J.; Christie, G.; Starr, J.M. Efficiency of Temporal Order Discrimination as an Indicator of Brady-phrenia in Parkinson’s Disease: The Inspection Time Loop Task. Neuropsychologia 2002, 40, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.K.; Langford, Z.; Garnier-Villarreal, M.; Morris, J.C.; Galvin, J.E. Onset of Mild Cognitive Impairment in Parkinson Disease. Alzheimer Dis. Assoc. Disord. 2016, 30, 127–133. [Google Scholar] [CrossRef]
- Allcock, L.; Rowan, E.; Steen, I.; Wesnes, K.; Kenny, R.; Burn, D. Impaired Attention Predicts Falling in Parkinson’s Disease. Park. Relat. Disord. 2009, 15, 110–115. [Google Scholar] [CrossRef]
- Stack, E.L.; Ashburn, A.M.G.; Jupp, K.E. Strategies used by people with Parkinson’s disease who report difficulty turning. Park. Relat. Disord. 2006, 12, 87–92. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.M.; Cramer, M.; Willemsen, M.; Zwinderman, A.H. Prospective assessment of falls in Parkinson’s disease. J. Neurol. 2001, 248, 950–958. [Google Scholar] [CrossRef]
- Paul, S.S.; Sherrington, C.; Canning, C.G.; Fung, V.S.C.; Close, J.C.T.; Lord, S.R. The relative contribution of physical and cognitive fall risk factors in people with Parkinson’s disease: A large prospective cohort study. Neurorehabilit. Neural Repair. 2014, 28, 282–290. [Google Scholar] [CrossRef]
- Nguyen, K.; Rui JG, M.; Nguyen, B.P.; Chua MC, H.; Yang, Y.O. Classification of Parkinson’s disease-associated gait patterns. In Research in Intelligent and Computing in Enginneering; Springer Nature: Singapore, 2021; ISBN 9811575274. [Google Scholar]
- Nguyen, K.; Chee, J.; Soh, C.W.; Hoang, N.S.; Lim, J.H.; Nguyen, B.P.; Chui, C.K.; Heng Chua, M.C. Classification of gait patterns using overlapping time displacement of batchwise video subclips. In Research in Intelligent and Computing in Enginneering; Springer Nature: Singapore, 2021; ISBN 9811575274. [Google Scholar]
- Varalta, V.; Picelli, A.; Fonte, C.; Amato, S.; Melotti, C.; Zatezalo, V.; Saltuari, L.; Smania, N. Relationship between Cognitive Performance and Motor Dysfunction in Patients with Parkinson’s Disease: A Pilot Cross-Sectional Study. BioMed Res. Int. 2015, 2015, 365959. [Google Scholar] [CrossRef]
- Smith-Ray, R.L.; Hughes, S.L.; Prohaska, T.R.; Little, D.M.; Jurivich, D.A.; Hedeker, D. Impact of Cognitive Training on Balance and Gait in Older Adults. J. Gerontol. Ser. B 2015, 70, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Fan, Y.; Zhuang, X.; Feng, D.; Chen, Y.; Chan, P.; Du, Y. Postural sway in patients with early Parkinson’s disease performing cognitive tasks while standing. Neurol. Res. 2018, 40, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Plotnik, M.; Giladi, N.; Dagan, Y.; Hausdorff, J.M. Postural instability and fall risk in Parkinson’s disease: Impaired dual tasking, pacing, and bilateral coordination of gait during the “ON” medication state. Exp. Brain Res. 2011, 210, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Pal, G.; O’keefe, J.; Robertson-Dick, E.; Bernard, B.; Anderson, S.; Hall, D. Global cognitive function and processing speed are associated with gait and balance dysfunction in Parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Mollinedo, I.; Cancela, J.M. Evaluation of the psychometric properties and clinical applications of the Timed Up and Go test in Parkinson disease: A systematic review. J. Exerc. Rehabil. 2020, 16, 302–312. [Google Scholar] [CrossRef]
- Theill, N.; Martin, M.; Schumacher, V.; Bridenbaugh, S.A.; Kressig, R.W. Simultaneously measuring gait and cognitive performance in cognitively healthy and cognitively impaired older adults: The Basel motor-cognition dual-task paradigm. J. Am. Geriatr. Soc. 2011, 59, 1012–1018. [Google Scholar] [CrossRef]
- Vance, R.C.; Healy, D.G.; Galvin, R.; French, H.P. Dual tasking with the timed “up & go” test improves detection of risk of falls in people with Parkinson disease. Phys. Ther. 2015, 95, 95–102. [Google Scholar] [CrossRef]
- Godefroy, O.; Lhullier, C.; Rousseaux, M. Reliability of reaction time measurements in brain-damaged patients. J. Neurol. Sci. 1994, 126, 168–171. [Google Scholar] [CrossRef]
- Jensen, A.R. Clocking the Mind: Mental Chronometry and Individual Differences; Elsevier: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Hocherman, S.; Moont, R.; Schwartz, M. Response selection and execution in patients with Parkinson’s disease. Cogn. Brain Res. 2004, 19, 40–51. [Google Scholar] [CrossRef]
- Evarts, E.V.; Teräväinen, H.; Calne, D.B. Reaction time in Parkinson’s disease. Brain 1981, 104 Pt 1, 167–186. [Google Scholar] [CrossRef]
- Sheridan, M.R.; Flowers, K.A.; Hurrell, J. Programming and execution of movement in Parkinson’s disease. Brain 1987, 110, 1247–1271. [Google Scholar] [CrossRef] [PubMed]
- Berry, E. Slowing of reaction time in Parkinson’s disease: The involvement of the frontal lobes. Neuropsychologia 1999, 37, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.A.; Tidswell, P.; Jordan, N.; Sagar, H.J. Slowed central processing in simple and go/no-go reaction time tasks in Parkinson’s disease. Brain 1994, 117 Pt 3, 517–529. [Google Scholar] [CrossRef]
- Gauntlett-Gilbert, J.; Brown, V.J. Reaction time deficits and Parkinson’s disease. Neurosci. Biobehav. Rev. 1998, 22, 865–881. [Google Scholar] [CrossRef] [PubMed]
- Sawamoto, N.; Honda, M.; Hanakawa, T.; Fukuyama, H.; Shibasaki, H. Cognitive slowing in Parkinson’s disease: A behavioral evaluation independent of motor slowing. J. Neurosci. 2002, 22, 5198–5203. [Google Scholar] [CrossRef] [PubMed]
- Vlagsma, T.T.; Koerts, J.; Tucha, O.; Dijkstra, H.T.; Duits, A.A.; van Laar, T.; Spikman, J.M. Mental slowness in patients with Parkinson’s disease: Associations with cognitive functions? J. Clin. Exp. Neuropsychol. 2016, 38, 844–852. [Google Scholar] [CrossRef]
- Taylor Tavares, A.L.; Jefferis, G.S.; Koop, M.; Hill, B.C.; Hastie, T.; Heit, G.; Bronte-Stewart, H.M. Quantitative measurements of alternating finger tapping in Parkinson’s disease correlate with UPDRS motor disability and reveal the improvement in fine motor control from medication and deep brain stimulation. Mov. Disord. 2005, 20, 1286–1298. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Vincos, G.B.; Kern, D.S.; Fox, S.H.; Lang, A.E.; Fasano, A. Learning more from finger tapping in Parkinson’s disease: Up and down from Dyskinesia to Bradykinesia. Mov. Disord. Clin. Pr. 2015, 3, 184–187. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Tosco, V.; Vitiello, F.; Orilisi, G.; Fraccastoro, F.; Putignano, A.; Orsini, G. Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges. Appl. Sci. 2022, 12, 877. [Google Scholar] [CrossRef]
- Mujber, T.; Szecsi, T.; Hashmi, M. Virtual reality applications in manufacturing process simulation. J. Mater. Process. Technol. 2004, 155–156, 1834–1838. [Google Scholar] [CrossRef]
- Traversoni, L. Delaunay’s tetrahedronalization: An efficient algorithm for 3-D triangulation. In SC-DL Tentative; SPIE: Santa Clara, CA, USA, 1990; pp. 56–61. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Can Immersive Virtual Reality Videogames Help Parkinson’s Disease Patients? A Case Study. Sensors 2021, 21, 4825. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Brandín-De la Cruz, N.; Secorro, N.; Calvo, S.; Benyoucef, Y.; Herrero, P.; Bellosta-López, P. Immersive virtual reality and antigravity treadmill training for gait rehabilitation in Parkinson’s disease: A pilot and feasibility study. Rev. Neurol. 2020, 71, 447–454. [Google Scholar] [PubMed]
- Campo-Prieto, P.; Santos-García, D.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Current status of immersive virtual reality as a tool for physical and functional rehabilitation in patients with Parkinson’s disease: Systematic review. Rev. Neurol. 2021, 73, 358–367. [Google Scholar]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors 2022, 22, 3302. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Immersive Virtual Reality Exergame Promotes the Practice of Physical Activity in Older People: An Opportunity during COVID-19. Multimodal Technol. Interact. 2021, 5, 52. [Google Scholar] [CrossRef]
- Robles-García, V.; Arias, P.; Sanmartín, G.; Espinosa, N.; Flores, J.; Grieve, K.L.; Cudeiro, J. Motor facilitation during real-time movement imitation in Parkinson’s disease: A virtual reality study. Park. Relat. Disord. 2013, 19, 1123–1129. [Google Scholar] [CrossRef]
- Chen, W.; Bang, M.; Krivonos, D.; Schimek, H.; Naval, A. An immersive virtual reality exergame for people with Parkinson’s disease. Lect. Notes Comput. Sci. 2020, 12376, 138–145. [Google Scholar] [CrossRef]
- Polechoński, J.; Langer, A. Assessment of the Relevance and Reliability of Reaction Time Tests Performed in Immersive Virtual Reality by Mixed Martial Arts Fighters. Sensors 2022, 22, 4762. [Google Scholar] [CrossRef]
- Bagatin, R.T.; Fonseca, A.; Garganta, J.; Williams, A.M.; Dias, C. The Effects of Competitive Pressure on Scanning Activity and Passing Accuracy in a VR-based Soccer Test. In Proceedings of the 3th World Congress of Performance Analysis of Sport 2022 & 13th International Symposium on Computer Science in Sport, Vienna, Austria, 10–13 September 2022. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 13, CD011145. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Carral, J.M.C. Translation and cross-cultural adaptation to Spanish of the Simulator Sickness Questionnaire. Retos 2021, 43, 503–509. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Drexler, J. Research in visually induced motion sickness. Appl. Ergon. 2010, 41, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef]
- Bloxham, C.A.; Dick, D.J.; Moore, M. Reaction times and attention in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1987, 50, 1178–1183. [Google Scholar] [CrossRef]
- Goodrich, S.; Henderson, L.; Kennard, C. On the existence of an attention-demanding process peculiar to simple reaction time: Converging evidence from Parkinson’s disease. Cogn. Neuropsychol. 1989, 6, 309–331. [Google Scholar] [CrossRef]
- Arroyo, A.; Periáñez, J.A.; Ríos-Lago, M.; Lubrini, G.; Andreo, J.; Benito-León, J.; Louis, E.D.; Romero, J.P. Components determining the slowness of information processing in parkinson’s disease. Brain Behav. 2021, 11, e02031. [Google Scholar] [CrossRef]
- Arroyo-Ferrer, A.; Sánchez-Cuesta, F.J.; González-Zamorano, Y.; del Castillo, M.D.; Sastre-Barrios, C.; Ríos-Lago, M.; Romero, J.P. Validation of Cognitive Rehabilitation as a Balance Rehabilitation Strategy in Patients with Parkinson’s Disease: Study Protocol for a Randomized Controlled Trial. Medicina 2021, 57, 314. [Google Scholar] [CrossRef]
- Thapa, N.; Park, H.J.; Yang, J.-G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- King, L.A.; Horak, F.B. Delaying mobility disability in people with Parkinson disease using a sensorimotor agility exercise program. Phys. Ther. 2009, 89, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Aplicación de un programa de ejercicios con atención focaliza-da en 2 pacientes afectados por síndrome de Parkinson-plus. Fisioterapia 2020, 42, 51–55. [Google Scholar] [CrossRef]
- Pham, H.N.; Do, T.T.T.; Chan, K.Y.J.; Sen, G.; Han, A.Y.K.; Lim, P.; Cheng, T.S.L.; Nguyen, Q.H.; Nguyen, B.P.; Chua, M.C.H. Multimodal Detection of Parkinson Disease based on Vocal and Improved Spiral Test. In Proceedings of the 2019 International Conference on System Science and Engineering (ICSSE), Dong Hoi, Vietnam, 20–21 July 2019; pp. 279–284. [Google Scholar] [CrossRef]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef]
- Lima, L.C.A.; Ansai, J.H.; Andrade, L.P.; Takahashi, A.C.M. The relationship between dual-task and cognitive performance among elderly participants who exercise regularly. Braz. J. Phys. Ther. 2015, 19, 159–166. [Google Scholar] [CrossRef]
- Borges, S.D.M.; Radanovic, M.; Forlenza, O.V. Correlation between functional mobility and cognitive performance in older adults with cognitive impairment. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2018, 25, 23–32. [Google Scholar] [CrossRef]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Davis, J.C.; Nagamatsu, L.S.; Hsu, C.L.; Katarynych, L.A.; Khan, K.M. Changes in executive functions and self-efficacy are independently associated with improved usual gait speed in older women. BMC Geriatr. 2010, 10, 25. [Google Scholar] [CrossRef]
- Yogev, G.; Giladi, N.; Peretz, C.; Springer, S.; Simon, E.S.; Hausdorff, J.M. Dual tasking, gait rhythmicity, and Parkinson’s disease: Which aspects of gait are attention demanding? Eur. J. Neurosci. 2005, 22, 1248–1256. [Google Scholar] [CrossRef]
- Plotnik, M.; Giladi, N.; Hausdorff, J.M. Bilateral coordination of gait and Parkinson’s disease: The effects of dual tasking. J. Neurol. Neurosurg. Psychiatry 2009, 80, 347–350. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, P.L.; Hausdorff, J.M. The role of higher-level cognitive function in gait: Executive dysfunction contributes to fall risk in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2007, 24, 125–137. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients diagnosed with PD | An inability to respond to the assessment protocol correctly, as judged by the observing clinician. |
| Age: 60–80 years | The presence of cardiovascular, pulmonary, or musculoskeletal conditions that would affect the patient’s ability to safely participate in the study, according to the physiotherapist’s judgement. |
| H&Y: I–III | Severe visual loss, vertigo, epilepsy, psychosis or severe diskinesias that could interfere with the ability to see and perform the IVR test and parkinsonism diagnosis. |
| All Participants n = 26 %/Mean ± SD | Fallers n = 10 %/Mean ± SD | Non-Fallers n = 16 %/Mean ± SD | Mean Difference (95% CI) | p | ||
|---|---|---|---|---|---|---|
| Age (years) | 69.73 ± 6.32 | 68.40 ± 7.79 | 70.56 ± 5.33 | −3.13–7.45 | 0.408 | |
| Gender (Male) | 79.2% | 68.8% | 70.0% | - | 0.946 | |
| H&Y Scale | 1.54 ± 0.90 | 1.80 ± 0.79 | 1.38 ± 0.96 | −1.17–0.32 | 0.252 | |
| MMSE Score | 26.92 ± 2.64 | 25.90 ± 2.42 | 27.56 ± 2.63 | −0.46–3.78 | 0.120 | |
| DBS surgical (No) | 96.2% | 100% | 93.8% | - | 0.420 | |
| First Symptom | Tremor | 46.2% | 60.0% | 37.5% | - | 0.728 |
| Bradykinesia Rigidity | 15.4% | 10.0% | 18.8% | - | ||
| Postural Instability | 11.5% | 20.0% | 12.5% | - | ||
| Others | 26.9% | 10.0% | 31.3% | - | ||
| Variable (Cut-Off Times, s) | AUC (95% CI) | % Sensitivity (95% CI) | % Specificity (95% CI) | Positive LR (95% CI) | Negative LR (95% CI) |
|---|---|---|---|---|---|
| Reaction time (0.574) | 0.74 (0.54, 0.95) | 70 (80, 60) | 75 (69, 82) | 2.80 (2.4, 3.3) | 0.36 (0.2, 0.4) |
| TUG Test (10.47) | 0.80 (0.57, 0.99) | 80 (90, 70) | 87.5 (81, 94) | 6.40 (3.7, 15) | 0.15 (0.1, 0.2) |
| TUG-Cognitive Test (14.23) | 0.85 (0.62, 0.99) | 85 (90, 80) | 90.5 (92, 89) | 8.95 (7.27, 11.2) | 0.11 (0.1, 0.14) |
| Non-Fallers | Fallers | p | |||||
|---|---|---|---|---|---|---|---|
| Median | Min | Max | Median | Min | Max | ||
| Reaction time (s) | 0.48 | 0.33 | 0.846 | 0.63 | 0.442 | 1.13 | 0.019 |
| TUG test (s) | 9.40 | 6.77 | 11.06 | 12.09 | 7.39 | 26.00 | 0.014 |
| TUG-Cognitive test (s) | 12.30 | 8.43 | 13.86 | 17.68 | 14.13 | 37.17 | 0.007 |
| MMSE Score | TUG Test (s) | TUG Cognitive Test (s) | Age (Years) | Non-Fallers (0) vs. Fallers (1) | ||
|---|---|---|---|---|---|---|
| Reaction time (s) | Spearman’s correlation (rho) | −0.576 | 0.537 | 0.454 | 0.399 | 0.456 |
| p-value | 0.002 | 0.005 | 0.020 | 0.043 | 0.019 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Immersive Virtual Reality Reaction Time Test and Relationship with the Risk of Falling in Parkinson’s Disease. Sensors 2023, 23, 4529. https://doi.org/10.3390/s23094529
Campo-Prieto P, Cancela-Carral JM, Rodríguez-Fuentes G. Immersive Virtual Reality Reaction Time Test and Relationship with the Risk of Falling in Parkinson’s Disease. Sensors. 2023; 23(9):4529. https://doi.org/10.3390/s23094529
Chicago/Turabian StyleCampo-Prieto, Pablo, José Mª Cancela-Carral, and Gustavo Rodríguez-Fuentes. 2023. "Immersive Virtual Reality Reaction Time Test and Relationship with the Risk of Falling in Parkinson’s Disease" Sensors 23, no. 9: 4529. https://doi.org/10.3390/s23094529
APA StyleCampo-Prieto, P., Cancela-Carral, J. M., & Rodríguez-Fuentes, G. (2023). Immersive Virtual Reality Reaction Time Test and Relationship with the Risk of Falling in Parkinson’s Disease. Sensors, 23(9), 4529. https://doi.org/10.3390/s23094529