

Neuroimaging Technology in Exercise Neurorehabilitation Research in Persons with MS: A Scoping Review



Abstract
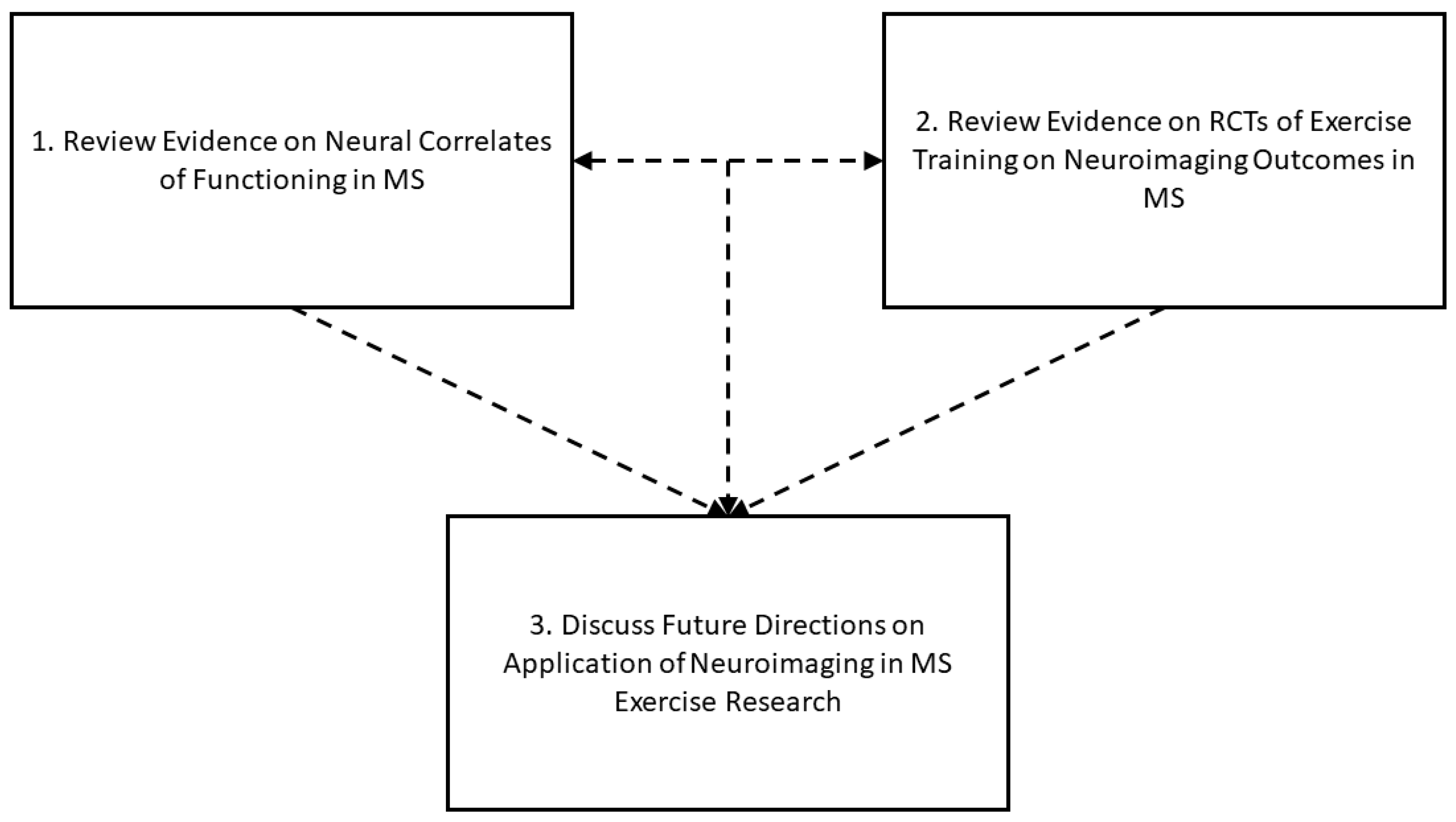
1. Introduction
2. Neural Correlates of Functions Targeted in Exercise Training Research in MS
3. Neuroimaging Outcomes from Exercise Training RCTs in MS
4. Discussion/Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wallin, M.T.; Culpepper, W.J.; Campbell, J.D.; Nelson, L.M.; Langer-Gould, A.; Marrie, R.A.; Cutter, G.R.; Kaye, W.E.; Wagner, L.; Tremlett, H.; et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology 2019, 92, e1029–e1040. [Google Scholar] [CrossRef] [PubMed]
- Trapp, B.D.; Nave, K.-A. Multiple sclerosis: An immune or neurodegenerative disorder. Ann. Rev. Neurosci. 2008, 31, 247–269. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Bross, M.; Hackett, M.; Bernitsas, E. Approved and emerging disease modifying therapies on neurodegeneration in multiple sclerosis. Int. J. Mol. Sci. 2020, 21, 4312. [Google Scholar] [CrossRef]
- Kraft, G.H. Rehabilitation still the only way to improve function in multiple sclerosis. Lancet 1999, 354, 2016. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Sandroff, B.M.; Kwakkel, G.; Dalgas, U.; Feinstein, A.; Heesen, C.; Feys, P.; Thompson, A.J. Exercise in patients with multiple sclerosis. Lancet Neurol. 2017, 16, 848–856. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Motl, R.W.; Yong, V.W.; Cutter, G.R.; Giovannoni, G. Exercise training in multiple sclerosis. Lancet Neurol. 2022, 21, 313. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M. Physical exercise in multiple sclerosis is not just a symptomatic therapy, it has a disease-modifying effect—Yes. Mult. Scler. J. 2021; in press. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Richardson, E.V.; Motl, R.W. The neurologist as an agent of exercise rehabilitation in multiple sclerosis. Exerc. Sport Sci. Rev. 2021, 49, 260–266. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Lai, B.; Young, H.-J.; Bickel, C.S.; Motl, R.W.; Rimmer, J.H. Current trends in exercise intervention research, technology, and behavioral change strategies for people with disabilities: A scoping review. Am. J. Phys. Med. Rehabil. 2017, 96, 748–761. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Motl, R.W.; Scudder, M.R.; DeLuca, J. Systematic, evidence-based review of exercise, physical activity, and physical fitness effects on cognition in persons with multiple sclerosis. Neuropsychol. Rev. 2016, 26, 271–294. [Google Scholar] [CrossRef]
- DeLuca, J.; Chiaravalloti, N.D.; Sandroff, B.M. Treatment and management of cognitive dysfunction in patients with multiple sclerosis. Nat. Rev. Neurol. 2020, 16, 319–332. [Google Scholar] [CrossRef]
- Filippi, M.; Rocca, M.A.; Benedict, R.H.B.; DeLuca, J.; Geurts, J.J.G.; Rombouts, S.A.R.B.; Ron, M.; Comi, G. The contribution of MRI in assessing cognitive impairment in multiple sclerosis. Neurology 2010, 75, 2121–2128. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Amato, M.P.; DeLuca, J.; Geurts, J.J.G. Cognitive impairment in multiple sclerosis: Clinical management, MRI, and therapeutic avenues. Lancet Neurol. 2020, 19, 860–871. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Motl, R.W.; Reed, W.R.; Barbey, A.K.; Benedict, R.H.B.; DeLuca, J. Integrative CNS plasticity with exercise in MS: The PRIMERS (PRocessing, Integration of Multisensory Exercise-Related Stimuli) conceptual framework. Neurorehabil. Neural Repair 2018, 32, 847–862. [Google Scholar] [CrossRef]
- Brummer, T.; Muthuraman, M.; Steffen, F.; Uphaus, T.; Minch, L.; Person, M.; Zipp, F.; Groppa, S.; Bittner, S.; Fleischer, V. Improved prediction of early cognitive impairment in multiple sclerosis combining blood and imaging biomarkers. Brain Commun. 2022, 4, fcac153. [Google Scholar] [CrossRef]
- Dziadkowiak, E.; Wieczorek, M.; Zagrajek, M.; Chojdak-Lukasiewicz, J.; Gruszka, E.; Budrewicz, S.; Pokryszko-Dragan, A. Multimodal evoked potentials as potential biomarkers of disease activity in patients with clinically isolated syndrome. Front. Neurol. 2022, 12, 678035. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M. Current perspectives on exercise training in the management of multiple sclerosis. Exp. Rev. Neurother. 2020, 20, 855–865. [Google Scholar] [CrossRef]
- Prakash, R.S.; Snook, E.M.; Erickson, K.I.; Colcombe, S.J.; Voss, M.W.; Motl, R.W.; Kramer, A.F. Cardiorespiratory fitness: A predictor of cortical plasticity in multiple sclerosis. Neuroimage 2007, 34, 1238–1244. [Google Scholar] [CrossRef]
- Prakash, R.S.; Snook, E.M.; Motl, R.W.; Kramer, A.F. Aerobic fitness is associated with gray matter volume and white matter integrity in multiple sclerosis. Brain Res. 2010, 1341C, 41–51. [Google Scholar] [CrossRef]
- Motl, R.W.; Pilutti, L.A.; Hubbard, E.A.; Wetter, N.C.; Sosnoff, J.J.; Sutton, B.P. Cardiorespiratory fitness and its association with thalamic, hippocampal, and basal ganglia volumes in multiple sclerosis. Neuroimage Clin. 2015, 7, 661–666. [Google Scholar] [CrossRef]
- Albergoni, M.; Storelli, L.; Preziosa, P.; Rocca, M.A.; Filippi, M. The insula modulates the effects of aerobic training on cardiovascular function and ambulation in multiple sclerosis. J. Neurol. 2023, 270, 1672–1681. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; Benedict, R.H.B.; Hubbard, E.A.; Pilutti, L.A.; Sutton, B.P. Do subcortical gray matter volumes and aerobic capacity account for cognitive-motor coupling in multiple sclerosis? Mult. Scler. 2021, 27, 401–409. [Google Scholar] [CrossRef]
- Romano, F.; Motl, R.W.; Valsasina, P.; Amato, M.P.; Brichetto, G.; Bruschi, N.; Chataway, J.; Chiaravalloti, N.D.; Cutter, G.; Dalgas, U.; et al. Abnormal thalamic functional connectivity correlates with cardiorespiratory fitness and physical activity in progressive multiple sclerosis. J. Neurol. 2023; in press. [Google Scholar] [CrossRef]
- Baird, J.F.; Hubbard, E.A.; Sutton, B.P.; Motl, R.W. The relationship between corticospinal tract integrity and lower-extremity strength is attenuated when controlling for age and sex in multiple sclerosis. Brain Res. 2018, 1701, 171–176. [Google Scholar] [CrossRef]
- Fritz, N.E.; Keller, J.; Calabresi, P.A.; Zackowski, K.M. Quantitative measures of walking and strength provide insight into brain corticospinal tract pathology in multiple sclerosis. Neuroimage Clin. 2017, 14, 490–498. [Google Scholar] [CrossRef]
- Klaren, R.E.; Hubbard, E.A.; Motl, R.W.; Pilutti, L.A.; Wetter, N.C.; Sutton, B.P. Objectively measured physical activity is associated with brain volumetric measurements in multiple sclerosis. Behav. Neurol. 2015, 2015, 482536. [Google Scholar] [CrossRef]
- Kalron, A.; Menascu, S.; Hoffmann, C.; Achiron, A. The importance of physical activity to preserve hippocampal volume in people with multiple sclerosis: A structural MRI study. J. Neurol. 2020, 267, 3723–3730. [Google Scholar] [CrossRef]
- Block, V.J.; Cheng, S.; Juwono, J.; Cuneo, R.; Kirkish, G.; Alexander, A.M.; Khan, M.; Akula, A.; Caverzasi, E.; Papinutto, N.; et al. Association of daily physical activity with brain volumes and cervical spinal cord areas in multiple sclerosis. Mult. Scler. 2023, 29, 363–373. [Google Scholar] [CrossRef]
- Prakash, R.S.; Patterson, B.; Janssen, A.; Abduljalil, A.; Boster, A. Physical activity associated with increased resting-state functional connectivity in multiple sclerosis. J. Int. Neuropsychol. Soc. 2011, 17, 986–997. [Google Scholar] [CrossRef]
- Mokhtarzade, M.; Shamsi, M.M.; Abolhasani, M.; Bakshi, B.; Sahraian, M.A.; Shalamzari, M.H.; Soudi, S. Lifetime physical activity is associated with gut bacteria and brain health in people with multiple sclerosis: Focus on physical activity intensity. Mult. Scler. Relat. Disord. 2022, 59, 103639. [Google Scholar] [CrossRef] [PubMed]
- Negaresh, R.; Gharakhanlou, R.; Ali Sahraian, M.; Abolhasani, M.; Motl, R.W.; Zimmer, P. Physical activity may contribute to brain health in multiple sclerosis: An MR volumetric and spectroscopy study. J. Neuroimaging 2021, 31, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.A.; Aubert-Broche, B.; Fetco, D.; Collins, D.L.; Arnold, D.L.; Finlayson, M.; Banwell, B.L.; Motl, R.W.; Yeh, E.A. Lower physical activity is associated with higher disease burden in pediatric multiple sclerosis. Neurology 2015, 85, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, E.A.; Wetter, N.C.; Sutton, B.P.; Pilutti, L.A.; Motl, R.W. Diffusion tensor imaging of the corticospinal tract and walking performance in multiple sclerosis. J. Neurol. Sci. 2016, 363, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Baird, J.F.; Cutter, G.R.; Motl, R.W. Do physical activity, cardiorespiratory fitness, and subcortical brain structures explain reduced walking performance in older adults with multiple sclerosis? Mult. Scler. Relat. Disord. 2022, 60, 103702. [Google Scholar] [CrossRef]
- Baird, J.F.; Motl, R.W. Cognitive function and whole-brain MRI metrics are not associated with mobility in older adults with multiple sclerosis. Int. J. Environ. Res. Public Health 2021, 18, 4232. [Google Scholar] [CrossRef]
- Mueller, C.; Baird, J.F.; Motl, R.W. Whole-brain metabolic abnormalities are associated with mobility in older adults with multiple sclerosis. Neurorehabil. Neural Repair 2022, 36, 286–297. [Google Scholar] [CrossRef]
- Preziosa, P.; Rocca, M.A.; Pagani, E.; Valsasina, P.; Amato, M.P.; Brichetto, G.; Bruschi, N.; Chataway, J.; Chiaravalloti, N.D.; Cutter, D.; et al. Structural and functional magnetic resonance imaging correlates of fatigue and dual-task performance in progressive multiple sclerosis. J. Neurol. 2022; in press. [Google Scholar] [CrossRef]
- Bollaert, R.E.; Poe, K.; Hubbard, E.A.; Motl, R.W.; Pilutti, L.A.; Johnson, C.L.; Sutton, B.P. Associations of functional connectivity and walking performance in multiple sclerosis. Neuropsychologia 2018, 117, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Hattori, T.; Tomisato, H.; Ohara, M.; Hirata, K.; Yokota, T.; Alzheimer’s Disease Neuroimaging Initiative. Turning and multitask gait unmask gait disturbance in mild-to-moderate multiple sclerosis: Underlying specific cortical thinning and connecting fibers damage. Hum. Brain Mapp. 2023, 44, 1193–1208. [Google Scholar] [CrossRef]
- Cofre Lizama, L.E.; Strik, M.; Van der Walt, A.; Kilpatrick, T.J.; Colbe, S.C.; Galea, M.P. Gait stability reflects motor tracts damage at early stages of multiple sclerosis. Mult. Scler. 2022, 28, 1773–1782. [Google Scholar] [CrossRef]
- Nygaard, M.K.E.; Langeskov-Christensen, M.; Dalgas, U.; Eskildsen, S.F. Cortical diffusion kurtosis imaging and thalamic volume are associated with cognitive and walking performance in relapsing-remitting multiple sclerosis. J. Neurol. 2021, 268, 3861–3870. [Google Scholar] [CrossRef]
- Mistri, D.; Cacciaguerra, L.; Storelli, L.; Meani, A.; Cordani, F.; Rocca, M.A.; Filippi, M. The association between cognition and motor performance is beyond structural damage in relapsing-remitting multiple sclerosis. J. Neurol. 2022, 269, 4213–4221. [Google Scholar] [CrossRef] [PubMed]
- Mamoei, S.; Jensen, H.B.; Dalgas, U.; Zijdewind, I.; Pederson, A.K.; Nygaard, M.K.E.; Eskildsen, S.F.; Stenager, E. A cross-sectional comparison of performance, neurophysiological and MRI outcomes of responders and non-responders to fampridine treatment in multiple sclerosis—An explorative study. J. Clin. Neurosci. 2020, 82, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, G.; Balto, J.M.; Sandroff, B.M.; Holtzer, R.; Izzetoglu, M.; Motl, R.W.; Hernandez, M.E. Frontal brain activation changes due to dual-tasking under partial body wight support conditions in older adults with multiple sclerosis. J. Neuroeng. Rehabil. 2017, 14, 65. [Google Scholar] [CrossRef]
- Hernandez, M.E.; Holtzer, R.; Chaparro, G.; Jean, K.; Balto, J.M.; Sandroff, B.M.; Izzetoglu, M.; Motl, R.W. Brain activation changes during locomotion in middle-aged to older adults with multiple sclerosis. J. Neurol. Sci. 2016, 370, 277–283. [Google Scholar] [CrossRef]
- Saleh, S.; Sandroff, B.M.; Vitiello, T.; Owoeye, O.; Hoxha, A.; Hake, P.; Goverover, Y.; Wylie, G.R.; Yue, G.H.; DeLuca, J. The role of premotor areas in dual tasking in healthy controls and persons with multiple sclerosis: An fNIRS imaging study. Front. Behav. Neurosci. 2018, 12, 296. [Google Scholar] [CrossRef]
- De Sanctis, P.; Malcolm, B.R.; Mabie, P.C.; Francisco, A.A.; Mowrey, W.B.; Joshi, S.; Molholm, S.; Foxe, J.J. Mobility brain/body imaging of cognitive-motor impairment in multiple sclerosis: Deriving EEG-based neuro-markers during a dual-task walking study. Clin. Neurophysiol. 2020, 131, 1119–1128. [Google Scholar] [CrossRef]
- Kalron, A.; Allali, G.; Achiron, A. Neural correlates of gait variability in people with multiple sclerosis with fall history. Eur. J. Neurol. 2018, 25, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Kloos, A.E.; Kegelmeyer, D.A.; Kaur, P.; Nichols-Larsen, D.S. Supplementary motor area connectivity and dual-task walking variability in multiple sclerosis. J. Neurol. Sci. 2019, 396, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Kalron, A.; Menascu, S.; Givon, U.; Dolev, M.; Achiron, A. Is the walk ratio a window to the cerebellum in multiple sclerosis? A structural magnetic resonance imaging study. Eur. J. Neurol. 2020, 27, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Grothe, M.; Lotze, M.; Langner, S.; Dressel, A. Impairments in walking ability, dexterity, and cognitive function in multiple sclerosis are associated with different regional cerebellar gray matter loss. Cerebellum 2017, 16, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Nourbakhsh, B.; Azevedo, C.; Maghzi, A.-H.; Spain, R.; Pelletier, D.; Waubant, E. Subcortical grey matter volumes predict subsequent walking function in early multiple sclerosis. J. Neurol. Sci. 2016, 366, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Zivadinov, R.; Bergsland, N.; Benedict, R.H.B. Thalamus volume and ambulation in multiple sclerosis: A cross-sectional study. Neurodegen. Dis. Manag. 2016, 6, 23–29. [Google Scholar] [CrossRef]
- Motl, R.W.; Hubbard, E.A.; Sreekumar, N.; Wetter, N.C.; Sutton, B.P.; Pilutti, L.A.; Sosnoff, J.J.; Benedict, R.H.B. Pallidal and caudate volumes correlate with walking function in multiple sclerosis. J. Neurol. Sci. 2015, 354, 33–36. [Google Scholar] [CrossRef]
- Zackowski, K.M.; Smith, S.A.; Reich, D.S.; Gordon-Lipkin, E.; Chodkowski, B.A.; Sambandan, D.R.; Shteyman, M.; Bastian, A.J.; van Zijl, P.C.; Calabresi, P.A. Sensorimotor dysfunction in multiple sclerosis and column-specific magnetization transfer-imaging abnormalities in the spinal cord. Brain 2009, 132, 1200–1209. [Google Scholar] [CrossRef]
- Richmond, S.B.; Peterson, D.S.; Fling, B.W. Bridging the callosal gap in gait: Corpus callosum white matter integrity’s role in lower limb coordination. Brain Imaging Behav. 2022, 16, 1552–1562. [Google Scholar] [CrossRef]
- Fritz, N.E.; Edwards, E.M.; Ye, C.; Prince, J.; Yang, Z.; Gressett, T.; Keller, J.; Myers, E.; Calabresi, P.A.; Zackowski, K.M. Cerebellar contributions to motor and cognitive control in multiple sclerosis. Arch. Phys. Med. Rehabil. 2022, 103, 1592–1599. [Google Scholar] [CrossRef]
- Ruggieri, S.; Bharti, K.; Prosperini, L.; Gianni, C.; Petsas, N.; Tommasin, S.; De Giglio, L.; Pozzilli, C.; Pantano, P. A comprehensive approach to disentangle the effect of cerebellar damage on physical disability in multiple sclerosis. Front. Neurol. 2020, 11, 529. [Google Scholar] [CrossRef]
- Sbardella, E.; Tona, F.; Petsas, N.; Upadhyay, N.; Piattella, M.C.; Filippini, N.; Prosperini, L.; Pozzilli, C.; Pantano, P. Functional connectivity changes and their relationship with clinical disability and white matter integrity in patients with relapsing-remitting multiple sclerosis. Mult. Scler. 2015, 21, 1681–1692. [Google Scholar] [CrossRef] [PubMed]
- Richmond, S.B.; Whittier, T.T.; Peterson, D.S.; Fling, B.W. Advanced characterization of static postural control dysfunction in persons with multiple sclerosis and associated neural mechanisms. Gait Posture 2021, 83, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Odom, A.D.; Richmond, S.B.; Fling, B.W. White matter microstructure of the cerebellar peduncles is associated with balance performance during sensory re-weighting in people with multiple sclerosis. Cerebellum 2021, 20, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Gera, G.; Fling, B.W.; Horak, F.B. Cerebellar white matter damage is associated with postural sway deficits in people with multiple sclerosis. Arch. Phys. Med. Rehabil. 2020, 101, 258–264. [Google Scholar] [CrossRef]
- Capone, F.; Capone, G.; Motolese, F.; Voci, A.; Caminiti, M.L.; Musumeci, G.; Di Lazzaro, V. Spinal cord dysfunction contributes to balance impairment in multiple sclerosis patients. Clin. Neurol. Neurosurg. 2019, 184, 105451. [Google Scholar] [CrossRef]
- Tona, F.; De Giglio, L.; Petsas, N.; Sbardella, E.; Prosperini, L.; Upadhyay, N.; Gianni, C.; Pozzilli, C.; Pantano, P. Role of cerebellar dentate functional connectivity in balance deficits in patients with multiple sclerosis. Radiology 2018, 287, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.S.; Gera, G.; Horak, F.B.; Fling, B.W. Corpus callosum structural integrity is associated with postural control improvement in persons with MS who have minimal disability. Neurorehabil. Neural Repair 2017, 31, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Prosperini, L.; Petsas, N.; Raz, E.; Sbardella, E.; Tona, F.; Mancinelli, C.R.; Pozzilli, C.; Pantano, P. Balance deficit with opened or closed eyes reveals involvement of different structures of the central nervous system in multiple sclerosis. Mult. Scler. 2014, 20, 81–90. [Google Scholar] [CrossRef]
- Prosperini, L.; Sbardella, E.; Raz, E.; Cercignani, M.; Tona, F.; Bozzali, M.; Petsas, N.; Pozzilli, C.; Pantano, P. Multiple sclerosis: White and gray matter damage associated with balance deficit detected at static posturography. Radiology 2013, 268, 181–189. [Google Scholar] [CrossRef]
- Fling, B.W.; Dutta, G.G.; Horak, F. Functional connectivity underlying postural motor adaptation in people with multiple sclerosis. Neuroimage Clin. 2015, 8, 281–289. [Google Scholar] [CrossRef]
- Prosperini, L.; Kouleridou, A.; Petsas, N.; Leonardi, L.; Tona, F.; Pantano, P.; Pozzilli, C. The relationship between infratentorial lesions, balance deficit and accidental falls in multiple sclerosis. J. Neurol. Sci. 2011, 304, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Schoonheim, M.M.; Broeders, T.A.A.; Geurts, J.J.G. The network collapse in multiple sclerosis: An overview of novel concepts to address disease dynamics. Neuroimage Clin. 2022, 35, 103108. [Google Scholar] [CrossRef] [PubMed]
- Prosperini, L.; Fanelli, F.; Petsas, N.; Sbardella, E.; Tona, F.; Raz, E.; Fortuna, D.; De Angelis, F.; Pozzilli, C.; Pantano, P. Multiple sclerosis: Changes in microarchitecture of white matter tracts after training with a video game balance board. Radiology 2014, 273, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Johnson, C.L.; Motl, R.W. Exercise training effects on memory and hippocampal viscoelasticity in multiple sclerosis: A novel application of magnetic resonance elastography. Neuroradiology 2017, 59, 61–67. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Wylie, G.R.; Sutton, B.P.; Johnson, C.L.; DeLuca, J.; Motl, R.W. Treadmill walking exercise training and brain function in multiple sclerosis: Preliminary evidence setting the stage for a network-based approach to rehabilitation. Mult. Scler. J. Exp. Transl. Clin. 2018, 4, 2055217318760641. [Google Scholar] [CrossRef]
- Kjølhede, T.; Siemonsen, S.; Wenzel, D.; Stellman, J.-P.; Ringgaard, S.; Pederson, B.G.; Stenager, E.; Peterson, T.; Vissing, K.; Heesen, C.; et al. Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult. Scler. 2018, 24, 1356–1365. [Google Scholar] [CrossRef]
- Tavazzi, E.; Bergsland, N.; Cattaneo, D.; Gervasoni, E.; Lagana, M.M.; Dipasquale, O.; Grosso, C.; Salbene, F.L.; Baglio, F.; Rovaris, M. Effects of motor rehabilitation on mobility and brain plasticity in multiple sclerosis: A structural and functional MRI study. J. Neurol. 2018, 265, 1393–1401. [Google Scholar] [CrossRef]
- Feys, P.; Moumdjian, L.; Van Halewyck, F.; Wens, I.; Eijnde, B.O.; Van Wijmeersch, B.V.; Popescu, V.; Van Asch, P. Effects of an individual 12-week community-located “start-to-run” program on physical capacity, walking, fatigue, cognitive function, brain volumes, and structures in persons with multiple sclerosis. Mult. Scler. 2019, 25, 92–103. [Google Scholar] [CrossRef]
- Huiskamp, M.; Moumdjian, L.; van Asch, P.; Popescu, V.; Schoonheim, M.M.; Steenwijk, M.D.; Vanzeir, E.; van Wijmeersch, B.; Geurts, J.J.G.; Feys, P.; et al. A pilot study of the effects of running training on visuospatial memory in MS: A stronger functional embedding of the hippocampus in the default-mode network? Mult. Scler. 2019, 26, 1594–1598. [Google Scholar] [CrossRef]
- Stellmann, J.-P.; Maarouf, A.; Schulz, K.-H.; Baquet, L.; Pottgen, J.; Patra, S.; Penner, I.-K.; Gelliben, S.; Ketels, G.; Besson, P.; et al. Aerobic exercise induces functional and structural reorganization of CNS networks in multiple sclerosis: A randomized controlled trial. Front. Hum. Neurosci. 2020, 14, 255. [Google Scholar] [CrossRef]
- Savsek, L.; Stergar, T.; Strojnik, V.; Ihan, A.; Koren, A.; Spiclin, Z.; Sega Jazbec, S. Impact of aerobic exercise on clinical and magnetic resonance imaging biomarkers in persons with multiple sclerosis: An exploratory randomized controlled trial. J. Rehabil. Med. 2021, 53, 2772. [Google Scholar] [CrossRef] [PubMed]
- Langeskov-Christensen, M.; Hvid, L.G.; Nygaard, M.K.E.; Ringgaard, S.; Jensen, H.B.; Nielsen, H.H.; Peterson, T.; Stenager, E.; Eskildsen, S.F.; Dalgas, U. Efficacy of high-intensity aerobic exercise on brain MRI measures in multiple sclerosis. Neurology 2021, 96, e203–e213. [Google Scholar] [CrossRef] [PubMed]
- Androwis, G.J.; Sandroff, B.M.; Niewrzol, P.; Fakhoury, F.; Wylie, G.R.; Yue, G.; DeLuca, J. A pilot randomized controlled trial of robotic exoskeleton-assisted exercise rehabilitation in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 51, 102936. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Wylie, G.R.; Baird, J.F.; Jones, C.D.; Diggs, M.D.; Genova, H.; Bamman, M.M.; Cutter, G.R.; DeLuca, J.; Motl, R.W. Effects of walking exercise training on learning and memory and hippocampal neuroimaging outcomes in MS: A targeted, pilot randomized controlled trial. Contemp. Clin. Trials 2021, 110, 106563. [Google Scholar] [CrossRef] [PubMed]
- Riemenschneider, M.; Hvid, L.G.; Ringgaard, S.; Nygaard, M.K.E.; Eskildsen, S.F.; Gaemelke, T.; Magyari, M.; Jensen, H.B.; Nielsen, H.H.; Kant, M.; et al. Investigating the potential disease-modifying and neuroprotective efficacy of exercise therapy early in the disease course of multiple sclerosis: The Early Multiple Sclerosis Exercise Study (EMSES). Mult. Scler. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Leavitt, V.M.; Cirnigliaro, C.; Cohen, A.; Farag, A.; Brooks, M.; Wecht, J.M.; Wylie, G.R.; Chiaravalloti, N.D.; DeLuca, J.; Sumowski, J.F. Aerobic exercise increases hippocampal volume and improves memory in multiple sclerosis: Preliminary findings. Neurocase 2014, 20, 695–697. [Google Scholar] [CrossRef] [PubMed]
- Orban, A.; Garg, B.; Sammi, M.K.; Bourdette, D.N.; Rooney, W.D.; Kuehl, K.; Spain, R.I. Effect of high-intensity exercise on multiple sclerosis function and phosphorus magnetic resonance spectroscopy outcomes. Med. Sci. Sports Exerc. 2019, 51, 1380–1386. [Google Scholar] [CrossRef]
- Akbar, N.; Sandroff, B.M.; Wylie, G.R.; Strober, L.B.; Smith, A.; Goverover, Y.; Motl, R.W.; DeLuca, J.; Genova, H. Progressive resistance exercise training and changes in resting-state functional connectivity of the caudate in persons with multiple sclerosis and severe fatigue: A proof-of-concept study. Neuropsychol. Rehabil. 2018, 30, 54–66. [Google Scholar] [CrossRef]
- Mayo, C.D.; Harrison, L.; Attwell-Pope, K.; Stuart-Hill, L.; Gawryluk, J.R. A pilot study of the impact of an exercise intervention on brain structure, cognition, and psychosocial symptoms in individuals with relapsing-remitting multiple sclerosis. Pilot Feasibility Stud. 2021, 7, 65. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Jones, C.D.; Baird, J.F.; Motl, R.W. Systematic review on exercise training as a neuroplasticity-inducing behavior in multiple sclerosis. Neurorehabil. Neural Repair 2020, 34, 575–588. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Bouchard, C.; Shephard, R.J. Physical Activity, Fitness, and Health: International Proceedings and Consensus Statement; Human Kinetics: Champaign, IL, USA, 1994. [Google Scholar]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of physical activity on neurocognitive function: A review at multiple levels of analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Hejazi, S.; Karwowski, W.; Farahani, F.V.; Marek, T.; Hancock, P.A. Graph-based analysis of brain connectivity in multiple sclerosis using functional MRI: A systematic review. Brain Sci. 2023, 13, 246. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.J.; Kramer, A.F.; Erickson, K.I.; Scalf, P.; McAuley, E.; Cohen, N.J.; Webb, A.; Jerome, G.J.; Marquez, D.X.; Elavsky, S. Cardiovascular fitness, cortical plasticity, and aging. Proc. Natl. Acad. Sci. USA 2004, 101, 3316–3321. [Google Scholar] [CrossRef]
- Pesce, C. An integrated approach to the effect of acute and chronic exercise on cognition: The linked role of individual and task constraints. In Exercise and Cognitive Function; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Kaur, J.; Ghosh, S.; Singh, P.; Dwivedi, A.K.; Sahani, A.K.; Sinha, J.K. Cervical spinal lesion, completeness of injury, stress, and depression reduce the efficiency of mental imagery in people with spinal cord. Am. J. Phys. Med. Rehabil. 2022, 101, 513–519. [Google Scholar] [CrossRef]
- Kelly, C.; Castellanos, F.X. Strengthening connections: Functional connectivity and brain plasticity. Neuropsychol. Rev. 2014, 24, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Rocca, M.A.; Preziosa, P.; Filippi, M. Application of advanced MRI techniques to monitor pharmacologic and rehabilitative treatment in multiple sclerosis: Current status and future perspectives. Exp. Rev. Neurother. 2019, 19, 835–866. [Google Scholar] [CrossRef]


{kind=link}
| Construct | Paper | Imaging Modality | n | MS Clinical Course | Disability Status | Functional Outcomes | Imaging Outcomes/ROI | Primary Results |
|---|---|---|---|---|---|---|---|---|
| Physical Fitness | Prakash et al., 2007 [20] | fMRI | 24 | RRMS | EDSS Mean: 2.6 Range: 0–6 | Cardiorespiratory Fitness: VO2peak | Imaging Outcomes: Cortical activation during PVSAT ROI: N/A | Higher cardiorespiratory fitness associated with greater recruitment of right IFG/MFG and reduced activation of ACC during PVSAT. |
| Prakash et al., 2010 [21] | MRI DTI | 21 | RRMS | EDSS Mean: 2.2 Range: 0–6 | Cardiorespiratory Fitness: VO2peak | Imaging Outcomes: Volumetrics WM lesion burden Structural connectivity (FA) ROI: N/A | After controlling for covariates, better cardiorespiratory fitness was associated with lower lesion load. Better fitness was associated with larger grey matter volumes in the right postcentral gyrus and the midline cortical structures (i.e., MFG, ACC, the precuneus. Better fitness was associated with higher FA in left thalamic radiation and right anterior corona radiata. | |
| Motl et al., 2015 [22] | MRI | 35 | RRMS PMS | EDSS Median: 5.0 IQR: 3.5 | Cardiorespiratory Fitness: VO2peak | Imaging Outcomes: Volumetrics ROI: Hippocampus Thalamus Basal ganglia | Better cardiorespiratory fitness was significantly associated with larger caudate, putamen, pallidum, and hippocampus volumes when controlling for covariates. No association between cardiorespiratory fitness and thalamic volume when controlling for covariates. | |
| Albergoni et al., 2023 [23] | MRI | 61 | RRMS PMS | EDSS Median: 3.0 Range: 0–6.5 | Cardiorespiratory Fitness: VO2peak HRR | Imaging Outcomes: Volumetrics WM lesion burden ROI: Insula | Higher HRR was associated with greater lesion volume in left insula. | |
| Motl et al., 2021 [24] | MRI | 62 | RRMS PMS | EDSS median: 5.0 IQR: 3.5 | Cardiorespiratory Fitness: Peak power output | Imaging Outcomes: Volumetrics ROI: Basal ganglia Thalamus | Higher peak power output significantly associated with larger thalamic, caudate, putamen, and pallidum volume. | |
| Romano et al., in press [25] | MRI fMRI | 91 | PMS | EDSS median: 6.0 IQR: 2.5 | Cardiorespiratory Fitness: VO2peak Peak power output Physical Activity: Device-measured MVPA, LPA, SB | Imaging Outcomes: Volumetrics WM lesion burden RSFC ROI: Thalamus Hippocampus Caudate Pallidum Putamen Amygdala Nucleus accumbens | Worse cardiorespiratory fitness was significantly associated with lower normal WM volume, decreased thalamic RSFC with the left ACC, and increased thalamic RSFC with the left calcarine cortex and right lingual gyrus. No association between device-measured physical activity and structural MRI outcomes. Engaging in less MVPA associated with decreased inter-thalamic RSFC. Engaging in less LPA was associated with increased thalamic RSFC with right hippocampus, left lingual gyrus. | |
| Baird et al., 2018 [26] | MRI DTI | 36 | NR | PDDS median: 4.0 IQR: 2.5 | Muscular Strength: KE and KF strength (isokinetic dynamometry) | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: CST | When controlling for covariates, larger CST FA was significantly associated with summed strength measures. | |
| Fritz et al., 2017 [27] | MRI MTI DTI | 29 | RRMS | EDSS Median: 4.0 Range: 1.0–6.5 | Muscular Strength: MVC of hip flexion, extension, abduction based on manual muscle testing | Imaging Outcomes: MTR ROI: CST Brainstem | Quantitative measures of strength and walking were associated with brain CST pathology. Walk velocity was a significant contributor to MTR and FA. | |
| Physical Activity | Klaren et al., 2015 [28] | MRI | 39 | RRMS PMS | EDSS Median: 4.5 IQR: 2.5 | Physical Activity: Device-measured MVPA, LPA, SB | Imaging Outcomes: Volumetrics ROI: Thalamus Basal ganglia Hippocampus | When controlling for covariates, engaging in more MVPA was significantly associated with larger normal GM, normal WM, thalamus, caudate, pallidum, putamen, and hippocampus volumes. No significant associations between LPA, SB, and MRI outcomes. |
| Kalron et al., 2020 [29] | MRI | 153 | RRMS PMS | EDSS Median: 2.0 Range: 0–6.5 | Physical Activity: GLTEQ | Imaging Outcomes: Volumetrics ROI: Hippocampus Amygdala Brain stem Thalamus Nucleus accumbens Caudate | Physically active persons with MS demonstrated significantly larger hippocampal volume than inactive persons with MS. No other differences between groups for other subcortical volumes when controlling for age, biological sex, total cranial volume. | |
| Block et al., 2023 [30] | MRI | 50 | RRMS PMS | EDSS Median: 4.0 Range: 2.5–6.5 | Physical Activity: Device-measured steps per day from wrist-worn Fitbit | Imaging Outcomes: Volumetrics ROI: Spinal cord | Engaging in more steps per day was significantly associated with greater spinal cord GM area, total cord area, and cortical volume fraction. | |
| Prakash et al., 2011 [31] | fMRI | 45 | RRMS PMS | EDSS Mean: 4.1 Range: 2–6 | Physical Activity: Device-measured activity counts per day | Imaging Outcomes: RSFC ROI: Hippocampus | When controlling for covariates, engaging in more physical activity was associated with greater RSFC between the hippocampus and posteromedial cortex. No associations between physical activity and hippocampal RSFC with other regions. | |
| Mokhtarzade et al., 2022 [32] | MRI | 45 | RRMS PMS | EDSS Median: 2.0 Range: 0–5 | Physical Activity: Adapted version of historical activity questionnaire | Imaging Outcomes: Volumetrics WM lesion burden ROI: N/A | No significant differences in brain volume, lesion volume, and lesion number between high- and low-active groups. When controlling for covariates, engaging in more physical activity (total energy expenditure) was associated with larger brain volume, less lesion burden (similar relationship for moderate and vigorous physical activity). | |
| Negaresh et al., 2021 [33] | MRI MRS | 52 | RRMS PMS | EDSS Mean: 2.1 SD: 1.1 | Physical Activity: Adapted form of historical activity questionnaire Device-measured MVPA, LPA, SB | Imaging Outcomes: Volumetrics Metabolite (NAA, MI, Cho) ratios on Cr ROI: Hippocampus Thalamus | Whole-brain and hippocampal volumes were significantly larger in highly active vs. inactive/moderately active groups; thalamic volume not significantly different between groups. After controlling for covariates, engaging in more device-measured MVPA, but not LPA, associated with larger thalamic and hippocampal volume, and higher thalamic and hippocampal NAA/Cr ratio; similar pattern of results for self-reported physical activity. | |
| Grover et al., 2015 [34] | MRI | 31 | Pediatric MS | EDSS Median: 1.5 Range: 0–3 | Physical Activity: GLTEQ | Imaging Outcomes: Volumetrics WM lesion burden ROI: N/A | Engaging in more strenuous physical activity was significantly associated with lower T2 lesion volume. |
| Construct | Paper | Imaging Modality | n | MS Clinical Course | Disability Status | Functional Outcomes | Imaging Outcomes/ROI | Primary Results |
|---|---|---|---|---|---|---|---|---|
| Mobility | Hubbard et al., 2016 [35] | MRI DTI | 69 | RRMS PMS | EDSS Median: 5.5 IQR: 3.4 | Mobility: T25FW 6MW Gait parameters | Imaging Outcomes: Volumetrics Structural connectivity (FA, MD, RD, AD) ROI: N/A | AD was significantly correlated with step length. MD was significantly associated with 6MW, T25FW, gait velocity, step time, and step length. FA was not significantly correlated with any of the walking parameters. |
| Motl et al., 2021 [24] | MRI | 62 | RRMS PMS | EDSS Median: 5.0 IQR: 3.0 | Mobility: T25FW 6MW | Imaging Outcomes: Volumetrics ROI: Thalamus Caudate Putamen Pallidum | T25FW and 6MW performance were significantly associated with larger thalamic, caudate, putamen, and pallidum volumes. | |
| Baird et al., 2022 [36] | MRI | 29 | RRMS PMS | EDSS Median: 4.0 IQR: 1.5 | Mobility: T25FW 6MW | Imaging Outcomes: Volumetrics ROI: Thalamus Basal ganglia | Among persons with MS, participants’ larger pallidum volume was associated with faster walking speed. | |
| Albergoni et al., 2023 [23] | MRI | 61 | RRMS PMS | EDSS Median: 3.0 IQR: 6.5 | Mobility: T25FW 6MW | Imaging Outcomes: Volumetrics WM lesion burden ROI: Insula | No significant associations among 6MW, T25FW performance and MRI outcomes. | |
| Baird and Motl, 2021 [37] | MRI | 31 | RRMS PMS | EDSS Median: 4.0 IQR: 1.5 | Mobility: SPPB | Imaging Outcomes: Volumetrics ROI: N/A | No significant associations among SPPB performance, NGMV, NWMV, and CSF volume in persons with MS. | |
| Mueller et al., 2022 [38] | MRI MRS | 15 | RRMS | EDSS Median: 4.0 IQR: 1.0 | Mobility: T25FW 6MW | Imaging Outcomes: Metabolites (NAA, MI, Cho) Brain thermometry ROI: N/A | MI in eleven regions correlated with walking speed and MI in twelve regions correlated with walking endurance. Brain temperature did not correlate with mobility measures. | |
| Preziosa et al., 2022 [39] | MRI fMRI DTI | 57 | PMS | EDSS Median: 6.0 Range: 4.5–6.5 | Mobility: Dual-task walking (reciting alternating letters while walking at self-selected speed) | Imaging Outcomes: Volumetrics WM lesion burden Structural connectivity (FA, MD, RD, AD) RSEC ROI: N/A | Higher lesion volume, MD of the WM tracts connecting the left caudate with left thalamus, and left thalamus with the left DLPFC, and lower FA of the WM tract connecting the right caudate with right DLPFC predicted higher dual-task walking speed. No significant MRI, fMRI, or DTI predictors of dual-task cost of walking speed. | |
| Bollaert et al., 2018 [40] | fMRI | 29 | RRMS PMS | EDSS Median: 6.0 Range: 2.0–6.5 | Mobility: T25FW | Imaging Outcomes: Volumetrics RSFC ROI: N/A | When controlling for covariates, faster T25FW speed was associated with higher RSFC of the left parahippocampal gyrus, left transverse temporal gyrus, right fusiform gyrus, right inferior temporal gyrus, right lingual gyrus, right pericalcarine cortex, right superior temporal gyrus, and right transverse temporal gyrus. | |
| Chen et al., 2023, [41] | MRI DTI | 25 | NR | EDSS Median: 2.0 Range: 1.0–2.5 | Mobility: Gait parameters assessed during several different tasks, including straight-line walking, circular walking, dual-task walking, triple-task walking TUG | Imaging Outcomes: Cortical thickness WM lesion burden Structural connectivity (FA) ROI: N/A | Worse TUG performance and slower stride velocity during dual-tasking was significantly associated with thinner cortex in left precuneus and left temporoparietal junction. Worse TUG performance, but not stride velocity, during dual-tasking, was associated with lower FA in corpus callosum, cingulum, bilateral corticospinal tract, and bilateral superior longitudinal fasciculus. | |
| Cofré Lizama et al., 2022 [42] | MRI | 25 | NR | EDSS Mean: 1.0 IQR: 2.0 | Mobility: Local divergence exponent (i.e., local dynamic stability across multiple planes) | Imaging Outcomes: Volumetrics WM lesion burden WM fiber tractography ROI: CST Interhemispheric sensorimotor tracts Cerebellothalamic tracts | Worse local dynamic stability at the sacrum, shoulder, and cervical vertebrae was associated with lower fiber density in the CST. Worse local dynamic stability at the cervical vertebrae was associated with lower fiber density in the interhemispheric sensorimotor tracts. | |
| Nygaard et al., 2021 [43] | MRI DKI | 67 | RRMS | EDSS Median: 2.5 IQR: 5.5 | Mobility: 6MW SSST | Imaging Outcomes: Volumetrics Structural connectivity (MD) ROI: N/A | Worse performance on the SSST and 6MW was associated with higher MD in the bilateral parietal lobes, cingulate gyri, precuneus, cuneus, SFG, MFG, and unilateral occipital gyrus, and inferior parietal lobule, postcentral gyrus, inferior parietal sulcus, and bilateral superior frontal gyrus, and MFG, respectively. Worse SSST and 6MW performance was associated with lower thalamic volume. | |
| Mistri et al., 2022 [44] | MRI | 106 | RRMS | EDSS Median: 1.5 Range: 1.0–2.0 | Mobility: T25FW | Imaging Outcomes: Volumetrics WM lesion burden ROI: N/A | Better T25FW performance was associated with lower lesion burden, higher normalized brain volume, higher NGMV, NWMV, and NDGMV. | |
| Mamoei et al., 2020 [45] | MRI TMS | 49 | RRMS PMS | EDSS: N/A | Mobility: T25FW SSST 5-STS MSWS-12 | Imaging Outcomes: Volumetrics WM lesion burden MEP (Central motor conduction time; peripheral motor conduction time) ROI: N/A | Central motor conduction time was associated with MSWS-12 scores, and T25FW, SSST performance, but not 5-STS. MRI outcomes not associated with MSWS-12, T25FW, SSST, or 5-STS. | |
| Chaparro et al., 2017 [46] | fNIRS | 10 | NR | EDSS Mean: 3.9 SD: 1.6 | Mobility: SPPB Over ground gait speed | Imaging Outcomes: PFC activation HbO2 ROI: PFC | For older adults with MS, activation levels were significantly higher during dual task conditions when compared with single task relative to age-matched controls. SPPB performance did not predict walking-related increases in activation. | |
| Hernandez et al., 2016 [47] | fNIRS | 8 | RRMS | EDSS Mean: NR Range: 1.0–6.0 | Mobility: Dual-task walking (walking at self-selected speed and reciting alternate letters of the alphabet) | Imaging Outcomes: PFC activation HbO2 ROI: PFC | Persons with MS demonstrated larger increases in PFC oxygenation during dual-task walking relative to single-task walking compared with controls. | |
| Saleh et al., 2018 [48] | fNIRS | 14 | RRMS | EDSS: NR | Mobility: Dual-task walking (walking at a self-selected speed and subtracting serial 7 s) | Imaging Outcomes: Cortical activation HbO2 HbR ROI: PMC SMA | Persons with MS demonstrated smaller PMC activation during dual-task walking relative to single task walking compared with controls. Within persons with MS, slower walking speed was associated with increased SMA activation. | |
| De Sanctis et al., 2020 [49] | EEG | 13 | RRMS | PDDS Mean: 1.6 | Mobility: Dual-task walking (walking on treadmill and completing visual Go/No-Go task) | Imaging Outcomes: ERP ROI: N/A | Within persons with MS, N2 differentiation associated with Go/No-Go performance was not significantly different between single- and dual-task walking trials. | |
| Kalron et al., 2020 [50] | MRI | 343 | RRMS PMS | EDSS Median: 2.5 IQR: 6.5 | Mobility: Walk ratio (calculated based on spatiotemporal gait parameters during self-selected walking) | Imaging Outcomes: Volumetrics ROI: Hippocampus Amygdala Putamen Caudate Pallidum Thalamus Cerebellum Corpus callosum | Better walk ratio was significantly and selectively associated with cerebellum volume, but not volumes of other brain ROI. | |
| Fritz et al., 2019 [51] | MRI fMRI DTI | 18 | RRMS | EDSS Median: 2.25 Range: 1.5–4 | Mobility: Spatiotemporal gait parameters during single- and dual-task walking (self-selected walking and subtracting serial 3 s) Dual-task TUG (TUG and subtracting serial 3 s) Dual-task walking (walking at self-selected speed and reciting alternating letters of the alphabet) | Imaging Outcomes: Volumetrics BOLD activation during ankle flexion/extension WM lesion burden Structural connectivity (FA, MD, RD, AD) ROI: SMA V4 | Lower SMA activation was associated with slower TUG-cognitive times. Structural imaging measures of SMA interhemispheric connectivity (AD, RD, MD, but not FA) were significantly related to dual-task walking variability. No association between V4 interhemispheric tract diffusivity and dual-task mobility measures. | |
| Kalron et al., 2018 [52] | MRI | 225 | RRMS PMS | EDSS Mean: 2.6 SD: 1.8 | Mobility: Spatiotemporal gait parameters during self-selected walking | Imaging Outcomes: Volumetrics Cortical thickness ROI: Hippocampus Putamen Caudate Pallidum Thalamus Cerebellum Cerebral cortex | Gait coefficient of variation was significantly associated with left hippocampus volume and left putamen volume among fallers with MS; no associations between MRI outcomes and gait variability in non-fallers with MS. | |
| Grothe et al., 2017 [53] | MRI | 45 | RRMS SPMS | EDSS Median: 1.5 IQR: 7.5 | Mobility: T25FW | Imaging Outcomes: Volumetrics ROI: N/A | Worse T25FW performance was associated with lower GM volume in Larsell’s lobule VI. | |
| Fritz et al., 2017 [27] | MRI MTI DTI | 29 | RRMS | EDSS Median: 4.0 Range: 1.0–6.5 | Mobility: Walk velocity TUG T25FW 2MW | Imaging Outcomes: MTR ROI: CST Brainstem | When controlling for covariates, higher walk velocity and 2MW performance were associated with higher MTR and FA of the CST. When controlling for covariates, better T25FW performance was associated with higher FA of the CST. | |
| Nourbakhsh et al., 2016 [54] | MRI | 42 | RRMS | EDSS Median: 2.0 IQR: 5.5 | Mobility: T25FW | Imaging Outcomes: Volumetrics ROI: Thalamus Caudate Putamen Pallidum Cerebellar cortex | No significant cross-sectional associations between T25FW performance and GM volumes. Higher baseline thalamic volume predicted less worsening in T25FW performance over 24 months. | |
| Motl et al., 2016 [55] | MRI | 79 | RRMS PMS | EDSS Median: 3.5 IQR: 3.6 | Mobility: T25FW | Imaging Outcomes: Volumetrics WM lesion burden ROI: Thalamus Basal ganglia | Faster T25FW speed significantly was associated with larger thalamic, caudate, putamen, and pallidum volumes and smaller WM lesion burden. Thalamic and caudate volume partially explained differences in T25FW speed between persons with MS and healthy controls. | |
| Motl et al., 2015 [56] | MRI | 61 | RRMS PMS | EDSS Median: 5.5 IQR: 3.0 | Mobility: T25FW 6MW | Imaging Outcomes: Volumetrics ROI: Thalamus Caudate Putamen Pallidum | When controlling for covariates, larger pallidum and caudate volumes were associated with better T25FW and 6MW performance. Pallidum volume was identified as the strongest correlate of T25FW and 6MW performance. | |
| Zackowski et al., 2009 [57] | MRI | 42 | RRMS PMS | EDSS Mean: 3.7 SD: 2.0 | Mobility: Walking speed based on fastest walking speed over 20 feet | Imaging Outcomes: Volumetrics MTR of CSF WM lesion burden ROI: Cervical spinal cord | Faster walking velocity was associated with lower lateral column MTR of CSF. | |
| Richmond et al., 2022 [58] | MRI DTI | 27 | RRMS | EDSS Median: 3.5 Range: 0–4.0 | Mobility: Spatiotemporal gait parameters based on walking at self-selected speed over 2 min | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: Transcallosal sensorimotor fiber tracts | Better phase coordination index based on gait parameters was associated with better RD and FA of the cingulate motor area, pre-supplementary motor area, dorsal premotor cortex, and primary sensory area. Better phase coordination index was associated with better RD in supplementary motor area and anterior primary motor cortex. Better phase coordination index was associated with better FA in posterior primary motor cortex. | |
| Fritz et al., 2022 [59] | MRI DTI | 29 | RRMS | EDSS Median: 4.0 Range: 1.0–6.5 | Mobility: Walking velocity SSST T25FW TUG 2MW | Imaging Outcomes: Volumetrics Structural connectivity (FA, MD, RD, AD) ROI: Cerebellar peduncles Cerebellar lobules I–VIII | Larger cerebellar peduncle and lobular volumes were associated with better T25FW, TUG, and 2MW performance, faster walking velocity. Lower MD and RD of the superior cerebellar peduncles were associated with faster T25FW speed and walking velocity. Lower MD, AD, and RD of the superior cerebellar peduncles were associated with better TUG, SSST, and 2MW performance. | |
| Ruggieri et al., 2020 [60] | MRI DTI | 49 | RRMS PMS | EDSS Median: 2.5 Range: 1.0–5.5 | Mobility: T25FW | Imaging Outcomes: Volumetrics WM lesion burden Structural connectivity (FA, MD, RD, AD) ROI: Cerebellar peduncles Cerebellar lobules I–X | When controlling for covariates, worse T25FW performance was associated with global atrophy and atrophy of cerebellar lobule VIIIIb. | |
| Sbardella et al., 2015 [61] | fMRI DTI | 30 | RRMS | EDSS Median: 2.5 Range: 0–4.0 | Mobility: T25FW | Imaging Outcomes: RSFC Structural connectivity (FA, MD, RD, AD) ROI: Cerebellum Basal ganglia Corpus callosum | No reported associations among DTI and RSFC outcomes with T25FW performance. |
| Construct | Paper | Imaging Modality | n | MS Clinical Course | Disability Status | Functional Outcomes | Imaging Outcomes/ROI | Primary Results |
|---|---|---|---|---|---|---|---|---|
| Balance | Richmond et al., 2021 [62] | MRI DTI | 27 | RRMS | EDSS Median: 3.5 Range: 0–4.0 | Balance: Time-to-boundary based on imCTSIB performance | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: Cortical sensorimotor pathway | Lower RD of sensorimotor pathway was associated with shorter time-to-boundary during eyes open imCTSIB conditions on a compliant surface. |
| Odom et al., 2021 [63] | MRI DTI | 27 | RRMS | EDSS Median: 3.75 IQR: 3.1–4.0 | Balance: Path length and root mean square of sway based on mCTSIB performance | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: Cerebellar peduncles | Higher FA in inferior cerebellar peduncles was associated with shorter path length during the proprioceptive-based mCTSIB condition. Higher middle cerebellar peduncle RD was associated with longer path length and smaller root mean square of sway during the visual-based balance condition of mCTSIB. Higher inferior cerebellar peduncle RD was associated with longer path length in the vestibular-based balance condition. | |
| Gera et al., 2020 [64] | MRI DTI | 29 | RRMS PMS | EDSS Mean: 3.1 (mild ataxia) EDSS Mean: 3.9 (moderate ataxia) | Balance: International Cooperative Ataxia Rating Scale Mini-BESTest | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: Cerebellar peduncles | RD of the inferior cerebellar peduncles was related to postural sway measures during both eyes open and closed. RD of the of the superior cerebellar peduncle was related to postural sway only in stance with eyes open. | |
| Ruggieri et al., 2020 [60] | MRI DTI | 49 | RRMS PMS | EDSS Median: 2.5 Range: 1.0–5.5 | Balance: Postural sway during static posturography | Imaging Outcomes: Volumetrics Structural connectivity (FA, MD, RD, AD) ROI: Cerebellar peduncles Cerebellar lobules I–X | Greater postural sway during eyes open conditions was associated with smaller volumes of cerebellar lobules I–IV, smaller total WM volume, and greater WM lesion burden. Greater postural sway during eyes closed conditions was associated with smaller volumes of cerebellar lobules I–IV and greater WM lesion burden. | |
| Capone et al., 2019 [65] | MRI SEP MEP | 38 | RRMS PMS | EDSS Median: 2.5 Range: 0–6.5 | Balance: Tinetti Scale | Imaging Outcomes: Spinal cord functionality (SEP, MEP) WM lesion burden ROI: Spinal cord | Higher Tinetti Scale scores were associated with lower cervical WM lesion burden and shorter central somatosensory conduction time. | |
| Tona et al., 2018 [66] | MRI fMRI | 25 | RRMS | EDSS Median: 3.0 Range: 2.0–4.0 | Balance: COP sway during static posturography | Imaging Outcomes: RSFC WM lesion burden ROI: Basal ganglia Cerebellar dentate nuclei | Higher RSFC in the left caudate nucleus was associated with shorter COP path. | |
| Peterson et al., 2017 [67] | MRI DTI | 29 | RRMS PMS | EDSS Mean: 3.5 Range: 2.0–4.0 | Balance: Postural performance in response to multiple trials of balance testing while standing on a hydraulically controlled platform that oscillated in forward and backwards directions | Imaging Outcomes: Structural connectivity (FA, MD, RD, AD) ROI: Corpus callosum Sensorimotor cortical regions | Temporal improvement in postural performance was associated with RD changes in the corpus callosum and MD changes in the left superior frontal lobe and arcuate fasciculus. | |
| Prosperini et al., 2014 [68] | MRI | 50 | RRMS PMS | EDSS Median: 2.5 Range: 1.0–5.5 | Balance: COP sway during static posturography | Imaging Outcomes: Volumetrics WM lesion burden ROI: Cerebellum Spinal cord | When controlling for covariates, greater COP sway during eyes open and eyes closed conditions was associated with lower cerebellar and upper cervical spinal cord volume, worse brainstem and spinal cord lesion burden, but not whole-brain or cerebellar WM lesion burden. | |
| Prosperini et al., 2013 [69] | MRI DTI | 45 | RRMS PMS | EDSS Median: 2.5 Range: 1.0–5.0 | Balance: COP sway during static posturography | Imaging Outcomes: Volumetrics WM lesion burden Structural connectivity (FA, MD, RD, AD) ROI: Cerebellum Spinal cord | When controlling for covariates, higher infratentorial WM lesion burden, lower whole-brain FA, and lower total WM volume significantly predicted greater COP sway. When controlling for covariates, worse balance control was associated with lower regional cerebellar volumes. | |
| Fling et al., 2015 [70] | fMRI | 24 | RRMS | EDSS Median: 4.0 Range: 2.0–4.0 | Balance: Postural performance in response to multiple trials of balance testing while standing on a hydraulically controlled platform that oscillated in forward and backwards directions | Imaging Outcomes: RSFC ROI: Cerebellum Basal ganglia | Higher RSFC within the corticocerebellar circuit was associated with better baseline postural control. Lower RSFC within the right cortico-striatal loop was associated with better short-term balance adaptation. | |
| Sbardella et al., 2015 [61] | fMRI DTI | 30 | RRMS | EDSS Median: 2.5 Range: 0–4.0 | Balance: COP sway during static posturography | Imaging Outcomes: RSFC Structural connectivity (FA, MD, RD, AD) ROI: Cerebellum Basal ganglia Corpus callosum | No reported associations among DTI and RSFC outcomes with COP sway. | |
| Prosperini et al., 2011 [71] | MRI | 31 | RRMS PMS | EDSS Median: 3.5 Range: 2.0–5.0 | Balance: COP sway during static posturography | Imaging Outcomes: WM lesion burden ROI: Cerebellum Brainstem Cerebellar peduncles | Worse brainstem WM lesion burden was associated with greater COP sway under eyes open conditions. | |
| Zackowski et al., 2009 [57] | MRI | 42 | RRMS PMS | EDSS Mean: 3.7 SD: 2.0 | Balance: COP sway during static posturography | Imaging Outcomes: Volumetrics MTR of CSF WM lesion burden ROI: Cervical spinal cord | Greater COP sway was associated with greater dorsal column MTR of CSF. |
| Paper | Imaging Modality | n | MS Clinical Course | Disability Status | Exercise Prescription | Imaging Outcomes/ROI | Functional Outcomes | Primary Results |
|---|---|---|---|---|---|---|---|---|
| Prosperini et al., 2014 [73] | MRI DTI | 27 | RRMS PMS | EDSS median: 3.0 Range: 1.5–5.0 | Modality: Home-based, high intensity, task-oriented feedback balance exercise (WBBS) Duration: 12 weeks Frequency: 5×/week Time: 30 min/session Intensity: WBBS games automatically progressed in difficulty based on achievement of criterion scores | Imaging Outcomes: Structural connectivity (FA, MD, RD) ROI: Cerebellar peduncles | Balance: COP sway during static posturography | Exercise training was associated with increased FA, decreased RD of cerebellar peduncles relative to waitlist control condition. Exercise training was associated with reduced postural sway under eyes open conditions relative to control. Reductions in postural sway were associated with improvements in structural connectivity. |
| Sandroff et al., 2017 [74] Sandroff et al., 2018 [75] | MRI MRE fMRI | 8 | RRMS | EDSS median: 3.0 Range: 1.5–4.0 | Modality: Supervised aerobic treadmill walking exercise Duration: 12 weeks Frequency: 3×/week Time: Progressive (15–40 min/session) Intensity: Progressive (40–80% HRR) | Imaging Outcomes: Viscoelasticity based on MRE RSFC ROI: Hippocampus (MRE) Thalamocortical circuit (RSFC) | Cardiorespiratory fitness: VO2peak Cognition: CVLT-II SDMT | Exercise training was associated with improved hippocampal viscoelasticity, increased thalamocortical RSFC relative to waitlist control condition. |
| Kjølhede et al., 2018 [76] | MRI | 35 | Not reported | EDSS mean: 2.9 Range: 2–4.0 | Modality: Supervised progressive resistance training of lower and upper extremities Duration: 24 weeks Frequency: 2×/week Time: Not reported Intensity: Progressive (3–4 sets of 6–12 reps between 6 and 15 repetition maximum) | Imaging Outcomes: Volumetrics Cortical thickness ROI: Exploratory | Lower extremity muscular strength: MVC of knee extensors and flexors 5-STS Mobility: T25FW 2MW Cognition: PASAT | No exercise-related changes in whole-brain PBVC, white/grey matter volume, volumes of subcortical structures relative to waitlist control condition. Exercise was associated with improvements in cortical thickness in 19/74 exploratory ROI relative to waitlist control. Exercise was associated with improvements in lower extremity muscular strength, T25FW performance relative to control. Exercise-related increases in cortical thickness of anterior cingular sulcus and gyrus associated with improvements in lower extremity muscular strength. |
| Tavazzi et al., 2018 [77] | DTI fMRI | 26 | RRMS PMS | EDSS median: 6.0 Range: 4.5–6.5 | Modality: Supervised aerobic treadmill endurance training Supervised progressive resistance training of the lower extremity Duration: 4 weeks Frequency: 10×/week Time: 30–45 min/session Intensity: Endurance training: Moderate (below 16–17 on Borg RPE) Progressive resistance training: Progressive (2–3 sets of 10–15 reps) | Imaging Outcomes: Structural connectivity (FA, MD, RD) RSFC BOLD signal during plantar dorsiflexion ROI: Sensorimotor network (RSFC) | Balance: BBS Mobility: T25FW 2MW Dynamic Gait Index | No change in any DTI measures for exercise and control conditions. Both groups demonstrated changes in RSFC, activation during dorsiflexion task, and improvements in 2MW and BBS performance, but between-group differences were not reported. No association among changes in task-related activation and functional outcomes; other correlations among changes not reported. |
| Feys et al., 2019 [78] Huiskamp et al., 2019 [79] | MRI fMRI DTI | 29 | Not reported | Not reported | Modality: Community-based aerobic running training Duration: 12 weeks Frequency: 3×/week Time: Not reported, distance-based Intensity: Progressive (1 minute running bouts through running 5 km without interruption) | Imaging Outcomes: Volumetrics Structural connectivity (specific measures not reported) RSFC ROI: Subcortical deep grey matter structures (volumetrics) DMN (RSFC) | Cardiorespiratory fitness: VO2peak Lower extremity muscular strength: 5-STS Mobility: T25FW 6MW Cognition: PASAT DSST WLG SRT 10/36 SPART | Exercise training was associated with increased left pallidum volume relative to waitlist control. No other between-group differences in whole-brain volume, subcortical volumes, structural connectivity outcomes, or hippocampal/DMN RSFC. Exercise training was associated with improved cardiorespiratory fitness, lower extremity muscular strength, and 10/36 SPART performance relative to control. Improvements in 10/36 SPART performance was associated with increased hippocampal-DMN RSFC in the exercise condition. |
| Stellmann et al., 2020 [80] | MRI DTI fMRI | 57 | RRMS | EDSS median: 1.5 Range: 0–3.5 | Modality: Aerobic cycle ergometer training (intervals) Duration: 12 weeks Frequency: 2–3×/week Time: Up to 60 min Intensity: Progressive (tailored based on numerous variables associated with baseline CPET) | Imaging Outcomes: Volumetrics WM lesion burden RSFC Structural connectivity (FA) Node connectivity metrics (i.e., hub disruption index) ROI: N/A | Functional outcomes data reported in a larger sample in primary analysis paper | No between-group changes in total brain volume, WM lesion burden, or clustering coefficient and node path length. Exercise training was associated with topology-independent (i.e., no significant effect based on hub/non-hub) increases in functional and structural connectivity metrics. No associations among exercise-related changes in functional and structural connectivity outcomes. |
| Savsek et al., 2021 [81] | MRI | 25 | RRMS | EDSS median: 2.5–3.0 Range: 1.0–6.5 | Modality: Choreographed aerobics Duration: 12 weeks Frequency: 2×/week Time: 60 min/session Intensity: 60–70% HRR | Imaging Outcomes: Volumetrics WM lesion burden ROI: N/A | Mobility: T25FW Cognition: SDMT CVLT-II BVMT-R | Overall negligible effects of exercise on MRI outcomes and cognitive performance. Weak effect of exercise training on T25FW speed. Mixed results regarding effects of exercise training vs. control on specific brain volumetrics. |
| Langeskov-Christensen et al., 2021 [82] | MRI DKI | 86 | RRMS PMS | EDSS mean: Intervention (2.7) Waitlist (2.8) | Modality: Aerobic cycling/rowing/cross-training (continuous) Aerobic cycling (intervals) Duration: 24 weeks Frequency: 2×/week (1× continuous and 1× interval) Time: 30–60 min/session Intensity: Progressive 65–95% HRmax | Imaging Outcomes: Volumetrics Cortical thickness WM + black hole lesion burden Structural connectivity (FA, kurtosis FA, MD, mean kurtosis tensor) ROI: Whole-brain Hippocampus Thalamus Corpus callosum Basal ganglia nuclei Upper spinal cord Cortex (DKI) Hippocampus (DKI) Thalamus (DKI) Basal Ganglia (DKI) Corpus callosum (DKI) | Cardiorespiratory fitness: VO2peak Peak work rate Mobility: 6MW Other outcomes reported in a secondary paper | No difference in percent brain volume change. Exercise-related improvements in cardiorespiratory fitness. No significant changes in MRI, cortical thickness, or DKI variables after Bonferroni correction. |
| Androwis et al., 2021 [83] | fMRI | 10 | RRMS PMS | Ambulation Index median: 4.0 Range: 2–5 | Modality: Robotic exoskeleton-assisted walking exercise Duration: 4 weeks Frequency: 2×/week Time: 30–45 min/session Intensity: Progressive (reduced assistance from robot from session-to-session) | Imaging Outcomes: RSFC ROI: Thalamus | Mobility: TUG 6MW Cognition: SDMT | Statistically significant time x group interaction on RSFC between thalamus and ventromedial prefrontal cortex; exercise was associated with increased RSFC compared with control. Exercise was associated with improvements in TUG and SDMT relative to control. Changes in RSFC were moderately associated with changes in TUG, 6MW, and SDMT. |
| Sandroff et al., 2021 [84] | MRI fMRI | 11 | RRMS | EDSS median: 3.5 Range: 2–4.0 | Modality: Aerobic treadmill walking exercise Duration: 12 weeks Frequency: 3×/week Time: 15–40 min/session Intensity: Progressive 40–80% HRR | Imaging Outcomes: Volumetrics RSFC ROI: Hippocampus | Cardiorespiratory fitness: VO2peak Time to exhaustion Cognition: CVLT-II OT-SRT BVMT-R 10/36 SPART SDMT | Significant time x condition interaction on normalized hippocampal volume; exercise was associated with preservation, stretching and toning associated with atrophy. Non-significant interaction on hippocampal RSFC using seed-based approach. Large, time x condition interaction on hippocampal-DMN RSFC using independent components analysis approach; exercise associated with reduced RSFC relative to control condition. |
| Riemenschneider et al., 2022 [85] | MRI DKI | 84 | Newly diagnosed RRMS | EDSS mean: Exercise 1.4 Health education control 1.8 | Modality: Aerobic cycling, rowing, cross-training, treadmill (unclear) Duration: 48 weeks Frequency: 2×/week Time: 30–60 min/session Intensity: Progressive based on mesocycles; 65–95% HRmax | Imaging Outcomes: Volumetrics Structural connectivity (MD, mean kurtosis tensor, FA, kurtosis FA) ROI: Whole-brain (volumetrics) Hippocampus (volumetrics, DKI) Thalamus (volumetrics, DKI) Corpus callosum (volumetrics, DKI) Caudate (volumetrics, DKI) Putamen (volumetrics, DKI) Pallidum (volumetrics, DKI) CST (DKI) Cingulate gyrus (DKI) | Cardiorespiratory fitness: VO2peak Other outcomes reported in a secondary paper | Exercise training associated with increase in VO2peak. No between-group difference for PBVC or BPF or any regional volumes. Exercise was associated with decreased MD in the thalamus, pallidum, CST, and cingulate gyrus relative to control. |
| Albergoni et al., 2023 [23] | MRI | 61 | RRMS PMS | EDSS median: 4.5 IQR: 3.0–6.5 | Modality: Aerobic, specific modality not reported Duration: 2–3 months Frequency: 2×–3×/week Time: 30–40 min/session Intensity: Between 55% and 75% HRmax | Imaging Outcomes: Volumetrics WM lesion burden ROI: Insula | Cardiorespiratory fitness: VO2peak HRR Mobility: T25FW 6MW | Aerobic exercise training was associated with improved 6MW distance relative to active control. PBVC, WM lesion burden, and insula volume did not differ between conditions. Aerobic exercise training was associated with increases in grey matter volume in frontotemporal regions and decreased grey matter volume in parieto-occipital regions compared with active control. Within the exercise condition, greater 6MW improvements were associated with less left anterior insula volume loss. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandroff, B.M.; Rafizadeh, C.M.; Motl, R.W. Neuroimaging Technology in Exercise Neurorehabilitation Research in Persons with MS: A Scoping Review. Sensors 2023, 23, 4530. https://doi.org/10.3390/s23094530
Sandroff BM, Rafizadeh CM, Motl RW. Neuroimaging Technology in Exercise Neurorehabilitation Research in Persons with MS: A Scoping Review. Sensors. 2023; 23(9):4530. https://doi.org/10.3390/s23094530
Chicago/Turabian StyleSandroff, Brian M., Caroline M. Rafizadeh, and Robert W. Motl. 2023. "Neuroimaging Technology in Exercise Neurorehabilitation Research in Persons with MS: A Scoping Review" Sensors 23, no. 9: 4530. https://doi.org/10.3390/s23094530
APA StyleSandroff, B. M., Rafizadeh, C. M., & Motl, R. W. (2023). Neuroimaging Technology in Exercise Neurorehabilitation Research in Persons with MS: A Scoping Review. Sensors, 23(9), 4530. https://doi.org/10.3390/s23094530