

Investigation of Optimal Light Source Wavelength for Cuffless Blood Pressure Estimation Using a Single Photoplethysmography Sensor


Abstract
1. Introduction
2. Materials and Methods
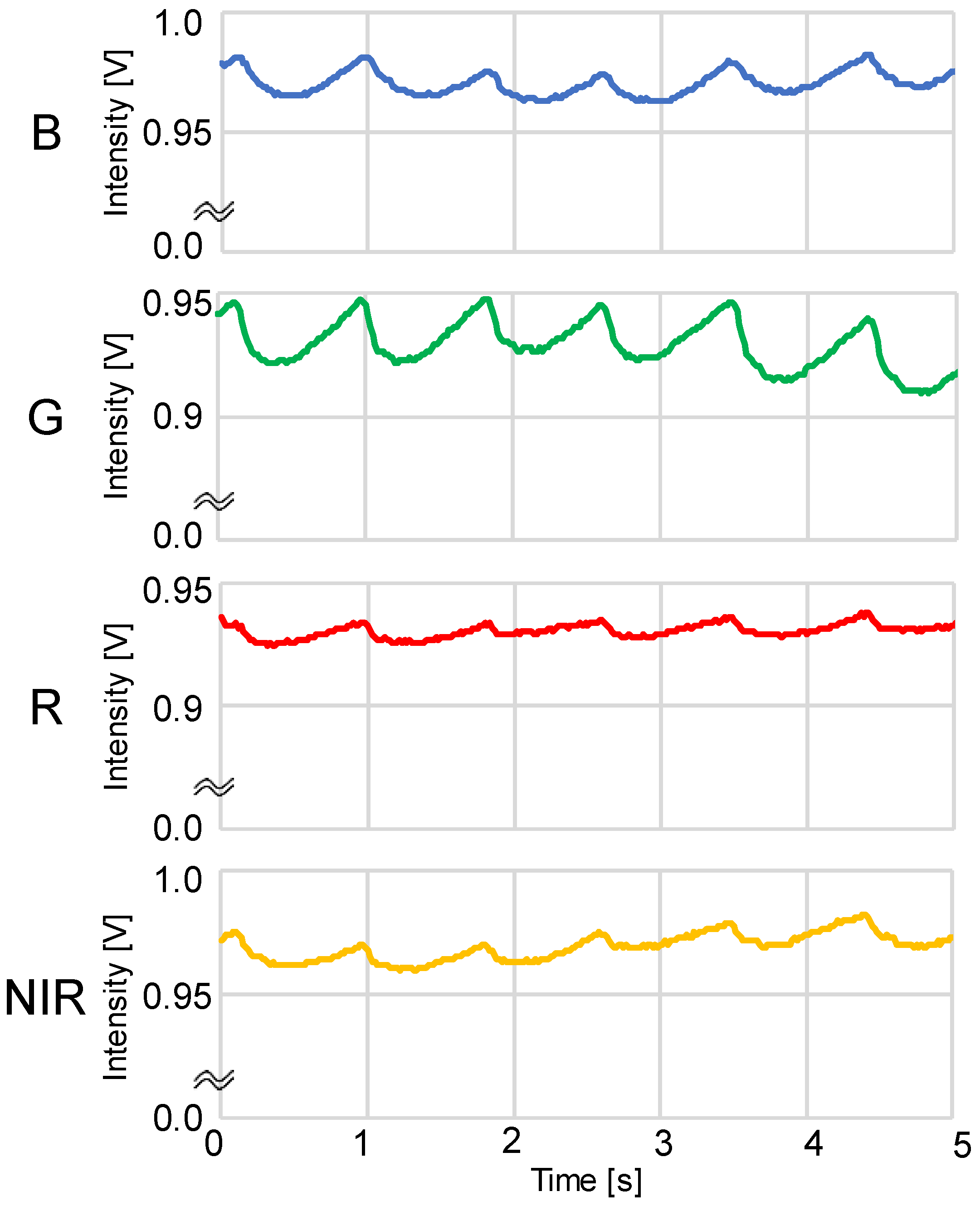
2.1. PPG Measurement
2.2. Cuffless BP Estimation Method
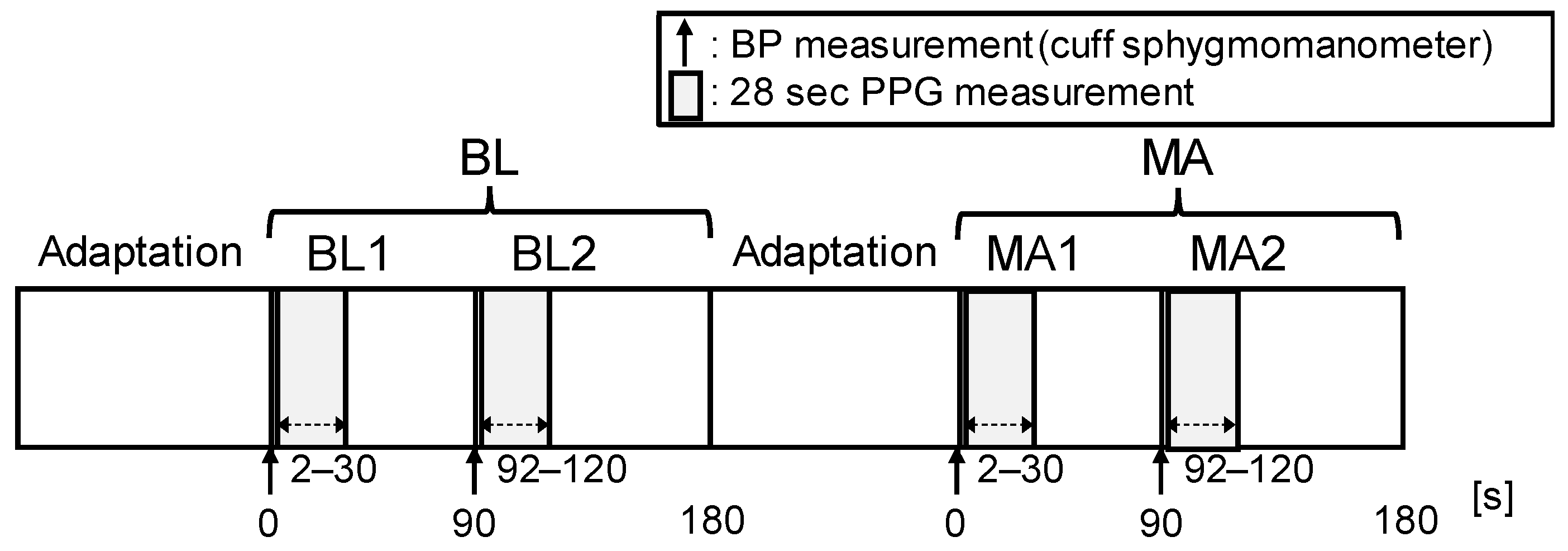
2.3. Experimental Protocol
2.4. Participants
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef]
- Parati, G.; Ochoa, J.E.; Lombardi, C.; Bilo, G. Assessment and management of blood-pressure variability. Nat. Rev. Cardiol. 2013, 10, 143–155. [Google Scholar] [CrossRef]
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Johansson, J.K.; Niiranen, T.J.; Puukka, P.J.; Jula, A.M. Prognostic value of the variability in home-measured blood pressure and heart rate: The Finn-Home Study. Hypertension 2012, 59, 212–218. [Google Scholar] [CrossRef]
- Hansen, T.W.; Thijs, L.; Li, Y.; Boggia, J.; Kikuya, M.; Björklund-Bodegård, K.; Richart, T.; Ohkubo, T.; Jeppesen, J.; Torp-Pedersen, C.; et al. Prognostic value of reading-to-reading blood pressure variability over 24 hours in 8938 subjects from 11 populations. Hypertension 2010, 55, 1049–1057. [Google Scholar] [CrossRef]
- Yamakoshi, K.; Shimazu, H.; Shibata, M.; Kamiya, A. New oscillometric method for indirect measurement of systolic and mean arterial pressure in the human finger. Part 1: Model experiment. Med. Biol. Eng. Comput. 1982, 20, 307–313. [Google Scholar] [CrossRef]
- Kaplan, N.M.; Victor, R.G. Chapter 2 Measurement of Blood Pressure. In Kaplan’s Clinical Hypertension, 11th ed.; LWW: Philadelphia, PA, USA, 2014; pp. 18–39. [Google Scholar]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Töreyin, H.; Kyal, S. Toward Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Theory and Practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef]
- Sharma, M.; Barbosa, K.; Ho, V.; Griggs, D.; Ghirmai, T.; Krishnan, S.K.; Hsiai, T.K.; Chiao, J.-C.; Cao, H. Cuff-less and continuous blood pressure monitoring: A methodological review. Technologies 2017, 5, 21. [Google Scholar] [CrossRef]
- Wibmer, T.; Doering, K.; Kropf-Sanchen, C.; Rüdiger, S.; Blanta, I.; Stoiber, K.M.; Rottbauer, W.; Schumann, C. Pulse transit time and blood pressure during cardiopulmonary exercise tests. Physiol. Res. 2014, 63, 287–296. [Google Scholar] [CrossRef]
- Proença, J.; Muehlsteff, J.; Aubert, X.; Carvalho, P. Is pulse transit time a good indicator of blood pressure changes during short physical exercise in a young population? Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2010, 2010, 598–601. [Google Scholar] [CrossRef]
- Fung, P.; Dumont, G.; Ries, C.; Mott, C.; Ansermino, M. Continuous noninvasive blood pressure measurement by pulse transit time. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2004, 2006, 738–741. [Google Scholar] [CrossRef]
- Choi, Y.; Zhang, Q.; Ko, S. Noninvasive cuffless blood pressure estimation using pulse transit time and Hilbert–Huang transform. Comput. Electr. Eng. 2013, 39, 103–111. [Google Scholar] [CrossRef]
- Kumar, N.; Agrawal, A.; Deb, S. Cuffless BP measurement using a correlation study of pulse transient time and heart rate. In Proceedings of the 2014 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Delhi, India, 24–27 September 2014; IEEE: Piscataway, NJ, USA; pp. 1538–1541. [Google Scholar] [CrossRef]
- Payne, R.A.; Symeonides, C.N.; Webb, D.J.; Maxwell, S.R. Pulse transit time measured from the ECG: An unreliable marker of beat-to-beat blood pressure. J. Appl. Physiol. (1985) 2006, 100, 136–141. [Google Scholar] [CrossRef]
- Patzak, A.; Mendoza, Y.; Gesche, H.; Konermann, M. Continuous blood pressure measurement using the pulse transit time: Comparison to intra-arterial measurement. Blood Press 2015, 24, 217–221. [Google Scholar] [CrossRef]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef]
- Barvik, D.; Cerny, M.; Penhaker, M.; Noury, N. Noninvasive Continuous Blood Pressure Estimation From Pulse Transit Time: A Review of the Calibration Models. IEEE Rev. Biomed Eng. 2022, 15, 138–151. [Google Scholar] [CrossRef]
- Chua, C.P.; Heneghan, C. Continuous blood pressure monitoring using ECG and finger photoplethysmogram. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 2006, 5117–5120. [Google Scholar] [CrossRef]
- Samria, R.; Jain, R.; Jha, A.; Saini, S.; Chowdhury, S.R. Noninvasive cuff’less estimation of blood pressure using Photoplethysmography without electrocardiograph measurement. In 2014 IEEE Region 10 Symposium; IEEE: Piscataway, NJ, USA, 2014; pp. 254–257. [Google Scholar] [CrossRef]
- Li, Z.; He, W. A Continuous Blood Pressure Estimation Method Using Photoplethysmography by GRNN-Based Model. Sensor 2021, 21, 7207. [Google Scholar] [CrossRef]
- Maher, N.; Elsheikh, G.; Anis, W.R.; Emara, T. Non-invasive calibration-free blood pressure estimation based on artificial neural network. In International Conference on Advanced Machine Learning Technologies and Applications; Springer: Berlin/Heidelberg, Germany, 2019; pp. 701–711. [Google Scholar] [CrossRef]
- Chandrasekhar, A.; Kim, C.S.; Naji, M.; Natarajan, K.; Hahn, J.O.; Mukkamala, R. Smartphone-based blood pressure monitoring via the oscillometric finger-pressing method. Sci. Transl. Med. 2018, 10, eaap8674. [Google Scholar] [CrossRef]
- Yamakoshi, T.; Rolfe, P.; Yamakoshi, K.I. Cuffless blood pressure estimation based on haemodynamic principles: Progress towards mobile healthcare. PeerJ 2021, 9, e11479. [Google Scholar] [CrossRef]
- Matsumura, K.; Rolfe, P.; Toda, S.; Yamakoshi, T. Cuffless blood pressure estimation using only a smartphone. Sci. Rep. 2018, 8, 7298. [Google Scholar] [CrossRef] [PubMed]
- Geddes, L.A.; Voelz, M.H.; Babbs, C.F.; Bourland, J.D.; Tacker, W.A. Pulse transit time as an indicator of arterial blood pressure. Psychophysiology 1981, 18, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Guyton, A.C.; Hall, J.E. Human Physiology and Mechanisms of Disease, 6th ed.; Saunders: Philadelphia, PA, USA, 1986. [Google Scholar]
- Gregg, M.E.; Matyas, T.A.; James, J.E. A new model of individual differences in hemodynamic profile and blood pressure reactivity. Psychophysiology 2002, 39, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, A.; Dolan, C.A.; Light, K.C. Hemodynamics of blood pressure responses during active and passive coping. Psychophysiology 1990, 27, 656–668. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Matsumura, K.; Yamakoshi, T.; Rolfe, P.; Tanaka, N.; Kim, K.; Yamakoshi, K. Validation of normalized pulse volume in the outer ear as a simple measure of sympathetic activity using warm and cold pressor tests: Towards applications in ambulatory monitoring. Physiol. Meas. 2013, 34, 359–375. [Google Scholar] [CrossRef]
- Matsumura, K.; Shimizu, K.; Rolfe, P.; Kakimoto, M.; Yamakoshi, T. Inter-method reliability of pulse volume related measures derived using finger-photoplethysmography: Across sensor positions and light intensities. J. Psychophysiol. 2018, 32, 182. [Google Scholar] [CrossRef]
- Sawada, Y.; Tanaka, G.; Yamakoshi, K.I. Normalized pulse volume (NPV) derived photo-plethysmographically as a more valid measure of the finger vascular tone. Int. J. Psychophysiol. 2001, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.R.; Parrish, J.A. The optics of human skin. J. Investig. Derm. 1981, 77, 13–19. [Google Scholar] [CrossRef]
- Roggan, A.; Friebel, M.; Do Rschel, K.; Hahn, A.; Mu Ller, G. Optical Properties of Circulating Human Blood in the Wavelength Range 400–2500 nm. J. Biomed. Opt. 1999, 4, 36–46. [Google Scholar] [CrossRef]
- Bashkatov, A.N.; Genina, E.; Kochubey, V.; Tuchin, V. Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. J. Phys. D Appl. Phys. 2005, 38, 2543. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Harness, J.; Irving, G.; Mearns, A. Skin photoplethysmography—A review. Comput. Methods Programs Biomed. 1989, 28, 257–269. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e484–e594. [Google Scholar] [CrossRef] [PubMed]
- Protogerou, A.D.; Safar, M.E.; Iaria, P.; Safar, H.; Le Dudal, K.; Filipovsky, J.; Henry, O.; Ducimetière, P.; Blacher, J. Diastolic blood pressure and mortality in the elderly with cardiovascular disease. Hypertension 2007, 50, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Light, K.C. Young Psychophysiologist Award address, 1980. Cardiovascular responses to effortful active coping: Implications for the role of stress in hypertension development. Psychophysiology 1981, 18, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Obrist, P.A.; Gaebelein, C.J.; Teller, E.S.; Langer, A.W.; Grignolo, A.; Light, K.C.; McCubbin, J.A. The relationship among heart rate, caratid dP/dt, and blood pressure in humans as a function of the type of stress. Psychophysiology 1978, 15, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, K.; Toda, S.; Kato, Y. RGB and near-infrared light reflectance/transmittance photoplethysmography for measuring heart rate during motion. IEEE Access 2020, 8, 80233–80242. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | SBP [mmHg] | DBP [mmHg] | MAP [mmHg] | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| BL | 112.3 | 12.3 | 68.5 | 6.3 | 83.1 | 7.2 |
| MA | 121.6 | 14.2 | 77.9 | 8.7 | 92.5 | 9.4 |
| Property | LED Color | Condition | Paired t-Test between BL and MA | ||||
|---|---|---|---|---|---|---|---|
| BL | MA | ||||||
| Mean | SD | Mean | SD | t | p | ||
| HR [bpm] | Blue | 72.8 | 12.7 | 89.8 | 15.8 | −7.55 | <0.001 |
| Green | 72.8 | 12.7 | 89.5 | 15.7 | −7.31 | <0.001 | |
| Red | 72.7 | 12.5 | 88.6 | 15.2 | −7.40 | <0.001 | |
| NIR | 72.9 | 12.8 | 88.0 | 15.2 | −6.45 | <0.001 | |
| mNPV [a.u.] | Blue | 0.0378 | 0.0179 | 0.0203 | 0.0074 | 6.28 | <0.001 |
| Green | 0.0364 | 0.0208 | 0.0193 | 0.0086 | 5.62 | <0.001 | |
| Red | 0.0206 | 0.0104 | 0.0111 | 0.0041 | 4.80 | <0.001 | |
| NIR | 0.0247 | 0.0115 | 0.0126 | 0.0047 | 5.84 | <0.001 | |
| BP | LED Color | HR (a) | mNPV (b) | c | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 | p | Β | std. β | p | β | std. β | p | β | p | ||
| Δln SBP | Blue | 0.612 | <0.001 | 0.288 | 0.572 | <0.001 | −0.045 | −0.262 | 0.079 | −0.003 | 0.771 |
| Green | 0.549 | <0.001 | 0.337 | 0.661 | <0.001 | −0.022 | −0.129 | 0.329 | −0.003 | 0.816 | |
| Red | 0.592 | <0.001 | 0.330 | 0.620 | <0.001 | −0.030 | −0.209 | 0.122 | −0.001 | 0.923 | |
| NIR | 0.634 | <0.001 | 0.373 | 0.736 | <0.001 | −0.012 | −0.086 | 0.520 | 0.001 | 0.914 | |
| Δln DBP | Blue | 0.497 | <0.001 | 0.203 | 0.280 | 0.097 | −0.117 | −0.475 | 0.006 | 0.024 | 0.168 |
| Green | 0.406 | <0.001 | 0.405 | 0.552 | <0.001 | −0.032 | −0.134 | 0.375 | 0.021 | 0.267 | |
| Red | 0.48 | <0.001 | 0.273 | 0.355 | 0.022 | −0.084 | −0.411 | 0.009 | 0.031 | 0.090 | |
| NIR | 0.47 | <0.001 | 0.205 | 0.281 | 0.085 | −0.097 | −0.463 | 0.006 | 0.036 | 0.035 | |
| Δln MAP | Blue | 0.630 | <0.001 | 0.245 | 0.424 | 0.005 | −0.084 | −0.431 | 0.004 | 0.011 | 0.329 |
| Green | 0.541 | <0.001 | 0.377 | 0.646 | <0.001 | −0.028 | −0.143 | 0.282 | 0.010 | 0.442 | |
| Red | 0.607 | <0.001 | 0.303 | 0.497 | <0.001 | −0.059 | −0.362 | 0.008 | 0.016 | 0.197 | |
| NIR | 0.598 | <0.001 | 0.286 | 0.493 | 0.001 | −0.058 | −0.349 | 0.016 | 0.020 | 0.089 | |
| SBP | DBP | MAP | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | G | R | NIR | B | G | R | NIR | B | G | R | NIR | |
| Mean (mmHg) | 4.84 | 5.27 | 4.90 | 4.67 | 4.68 | 5.13 | 5.00 | 5.01 | 3.57 | 4.09 | 3.98 | 3.97 |
| SD (mmHg) | 3.83 | 4.20 | 4.06 | 3.79 | 4.60 | 4.84 | 4.25 | 4.42 | 4.01 | 4.28 | 3.71 | 3.86 |
| 0–5 mmHg | 24 | 22 | 25 | 26 | 27 | 26 | 27 | 27 | 32 | 29 | 31 | 32 |
| 5–10 mmHg | 12 | 15 | 13 | 13 | 10 | 11 | 8 | 10 | 6 | 8 | 7 | 6 |
| 10–15 mmHg | 6 | 3 | 2 | 2 | 3 | 2 | 6 | 4 | 3 | 3 | 3 | 3 |
| >15 mmHg | 0 | 2 | 2 | 1 | 2 | 3 | 1 | 1 | 1 | 2 | 1 | 1 |
| Property | LED Color | Condition | Paired t-Test between BL and MA | ||||
|---|---|---|---|---|---|---|---|
| BL | MA | ||||||
| Mean | SD | Mean | SD | t | p | ||
| SBP [mmHg] | Blue | 111.6 | 13.2 | 122.3 | 14.4 | −7.85 | <0.001 |
| Green | 112.0 | 13.4 | 122.1 | 14.3 | −8.16 | <0.001 | |
| Red | 111.9 | 13.2 | 122.2 | 13.9 | −7.69 | <0.001 | |
| NIR | 112.2 | 13.2 | 122.0 | 14.0 | −6.85 | <0.001 | |
| DBP [mmHg] | Blue | 69.3 | 6.5 | 78.0 | 7.8 | −7.22 | <0.001 |
| Green | 69.8 | 6.6 | 77.8 | 8.2 | −7.89 | <0.001 | |
| Red | 69.4 | 6.1 | 77.9 | 7.5 | −7.38 | <0.001 | |
| NIR | 69.3 | 6.2 | 77.9 | 7.3 | −8.21 | <0.001 | |
| MAP [mmHg] | Blue | 83.4 | 7.6 | 92.7 | 8.9 | −7.62 | <0.001 |
| Green | 83.9 | 7.7 | 92.6 | 9.0 | −8.07 | <0.001 | |
| Red | 83.5 | 7.3 | 92.7 | 8.3 | −7.67 | <0.001 | |
| NIR | 83.6 | 7.6 | 92.6 | 8.5 | −8.16 | <0.001 | |
| LED Color | Results of Statistical Tests | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| B | G | R | NIR | ANOVA | Tukey’s HSD Multiple Comparison | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F(3,6) | p | ||
| R2 | 0.580 | 0.059 | 0.499 | 0.066 | 0.560 | 0.057 | 0.567 | 0.070 | 18.74 | 0.002 | G < B, R, NIR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toda, S.; Matsumura, K. Investigation of Optimal Light Source Wavelength for Cuffless Blood Pressure Estimation Using a Single Photoplethysmography Sensor. Sensors 2023, 23, 3689. https://doi.org/10.3390/s23073689
Toda S, Matsumura K. Investigation of Optimal Light Source Wavelength for Cuffless Blood Pressure Estimation Using a Single Photoplethysmography Sensor. Sensors. 2023; 23(7):3689. https://doi.org/10.3390/s23073689
Chicago/Turabian StyleToda, Sogo, and Kenta Matsumura. 2023. "Investigation of Optimal Light Source Wavelength for Cuffless Blood Pressure Estimation Using a Single Photoplethysmography Sensor" Sensors 23, no. 7: 3689. https://doi.org/10.3390/s23073689
APA StyleToda, S., & Matsumura, K. (2023). Investigation of Optimal Light Source Wavelength for Cuffless Blood Pressure Estimation Using a Single Photoplethysmography Sensor. Sensors, 23(7), 3689. https://doi.org/10.3390/s23073689