
Endoscope Automation Framework with Hierarchical Control and Interactive Perception for Multi-Tool Tracking in Minimally Invasive Surgery

 , , ,
, , , 
Abstract
1. Introduction
1.1. Background
1.2. Related Works
1.2.1. Instrument Segmentation and Tracking
1.2.2. RCM Constraint
1.2.3. FOV Control in MIS
1.3. Contributions
- Integration of HQP for Autonomous FOV Control: We introduce a hierarchical framework that exploits Hierarchical Quadratic Programming (HQP) to autonomously control the endoscope’s FOV. This approach manages the multiple objectives inherent in surgical scenarios, ensuring an unobstructed view of the surgical field amidst the dynamic nature of multi-instrument manipulation.
- Development of an Interactive Segmentation Module: Central to our framework is what we refer to as the "Interactive Segmentation and Tracking Module." This provides surgeons flexibility in real-time during surgeries, allowing the selection and robust tracking of various objects within the surgical field. This module is instrumental for adapting to the dynamic and unpredictable conditions presented by multi-user surgical procedure.
- Implementation Availability: We provide a simulation environment and the corresponding codebase. Our contributions include the HQP-based control framework and the interactive segmentation and tracking modules, specifically designed for integration with robotic control systems. These resources aim to facilitate the integration of our system for practical applications in the future.
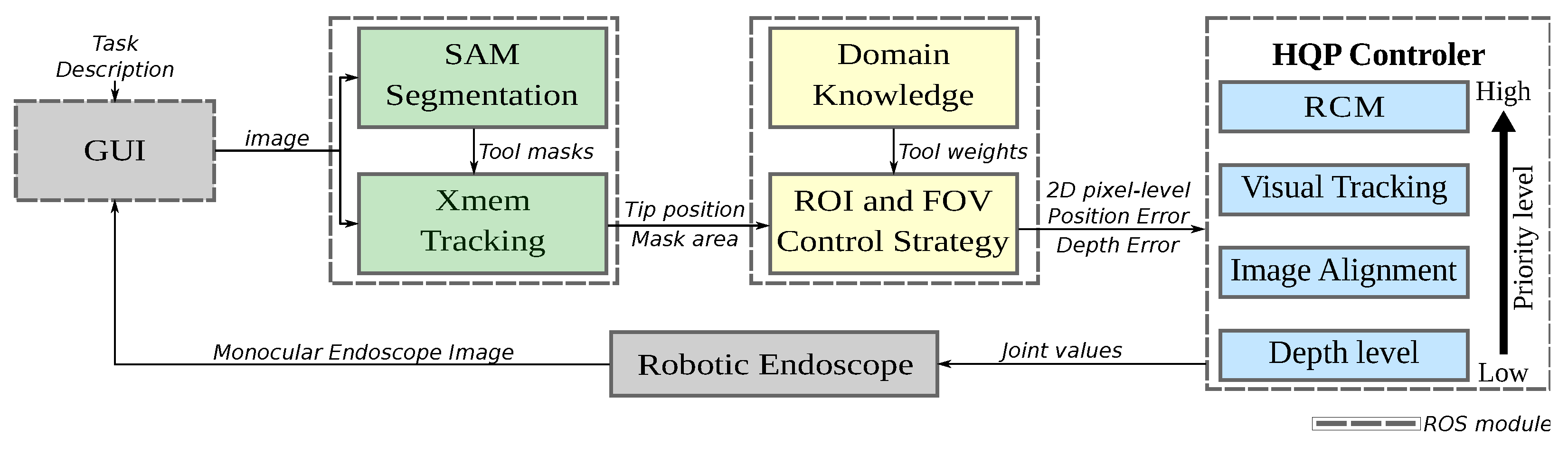
2. Proposed System Overview
3. Perception Methods
3.1. Interactive Segmentation and Tracking
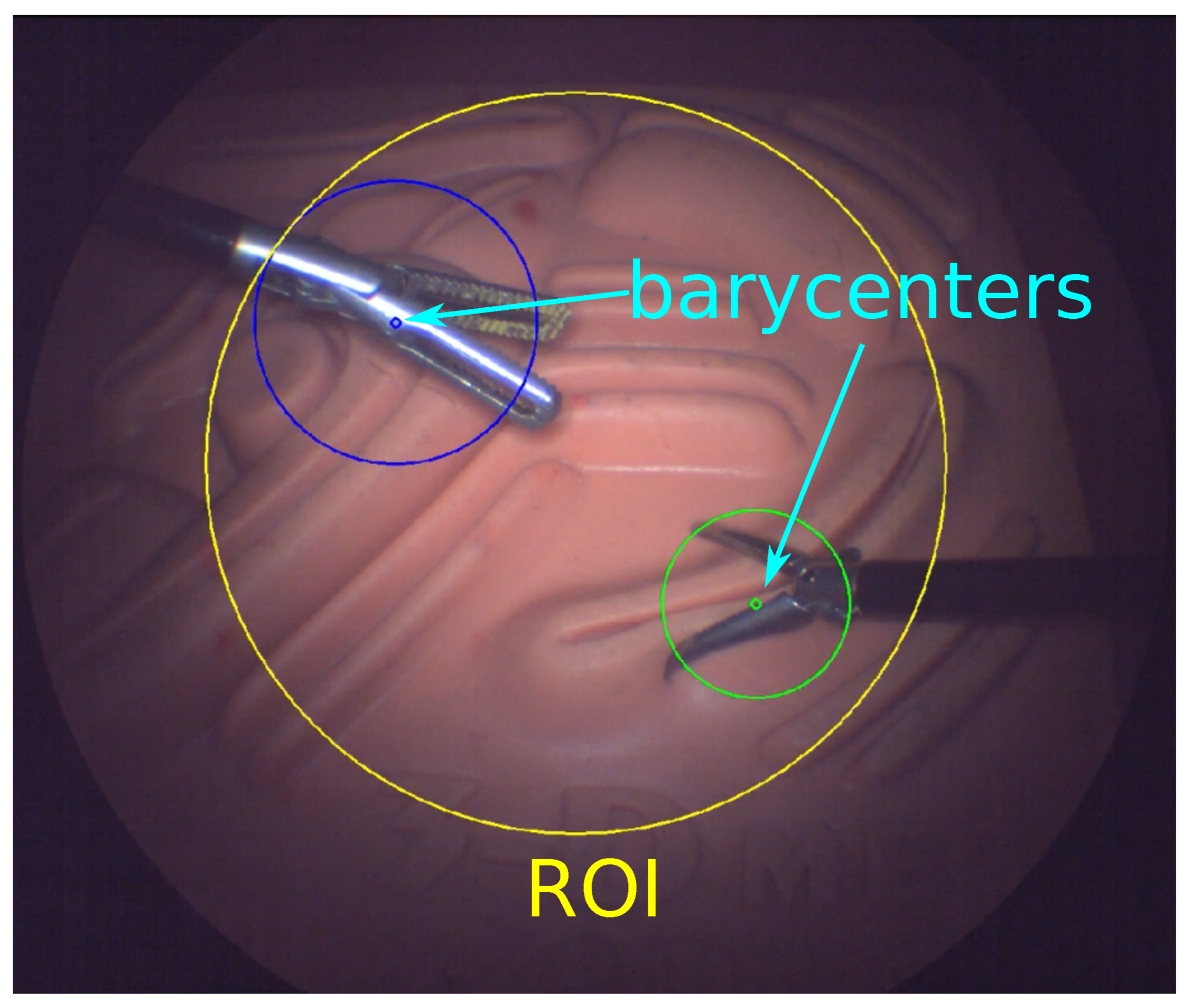
3.2. Determining the ROI
4. Hierarchical Framework for Surgical Robot Motion Planning
4.1. HQP Controller
4.2. Tasks Hierarchy
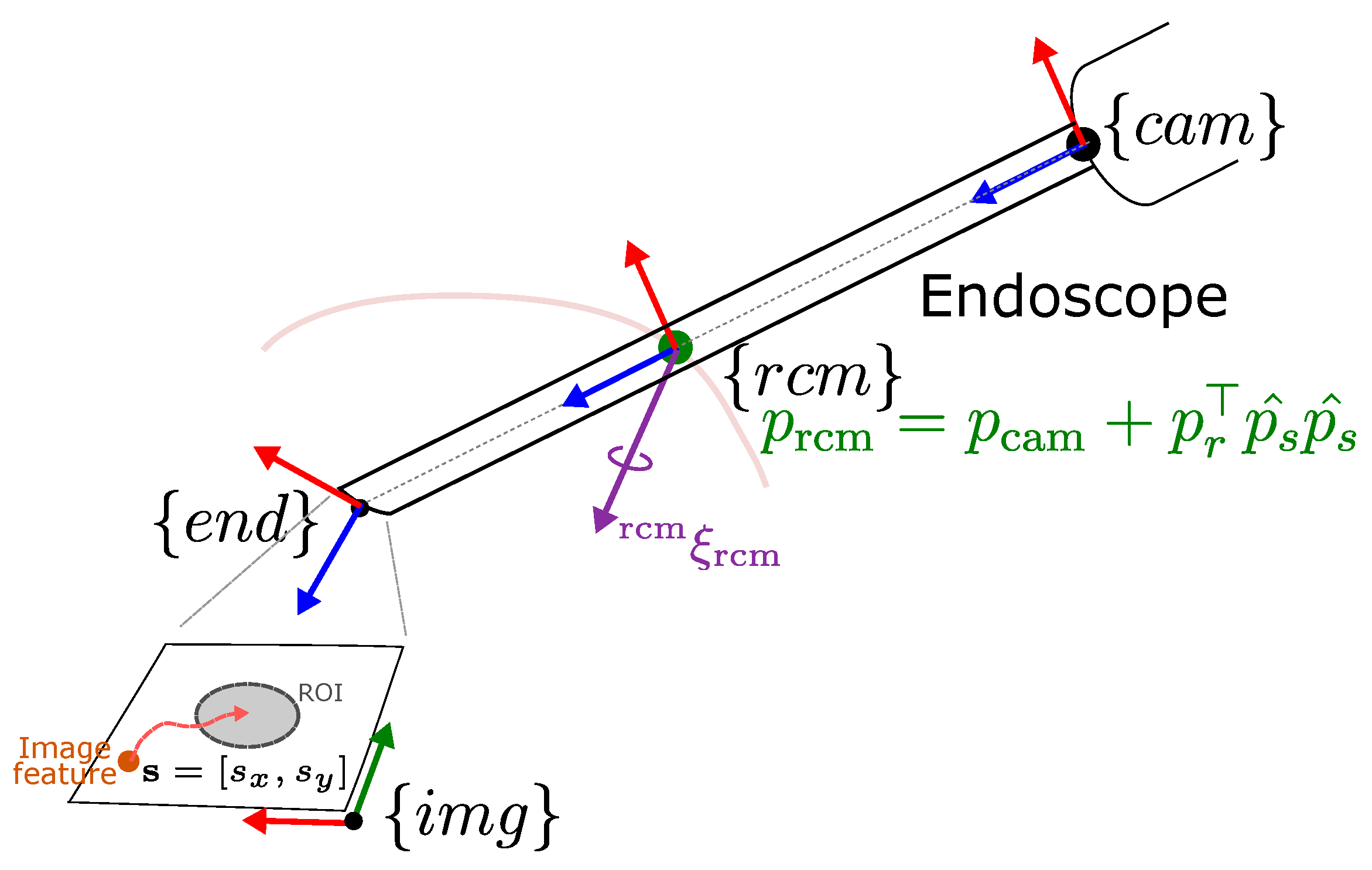
4.2.1. Remote Center of Motion
4.2.2. Visual Servoing
4.2.3. Misalignment
- is the vector representing the sine component of the angle.
- is the vector representing the cosine component of the angle.
- ensures that the angle is measured in the correct direction.
4.2.4. Depth
4.3. Inverse Kinematics
5. Experiments
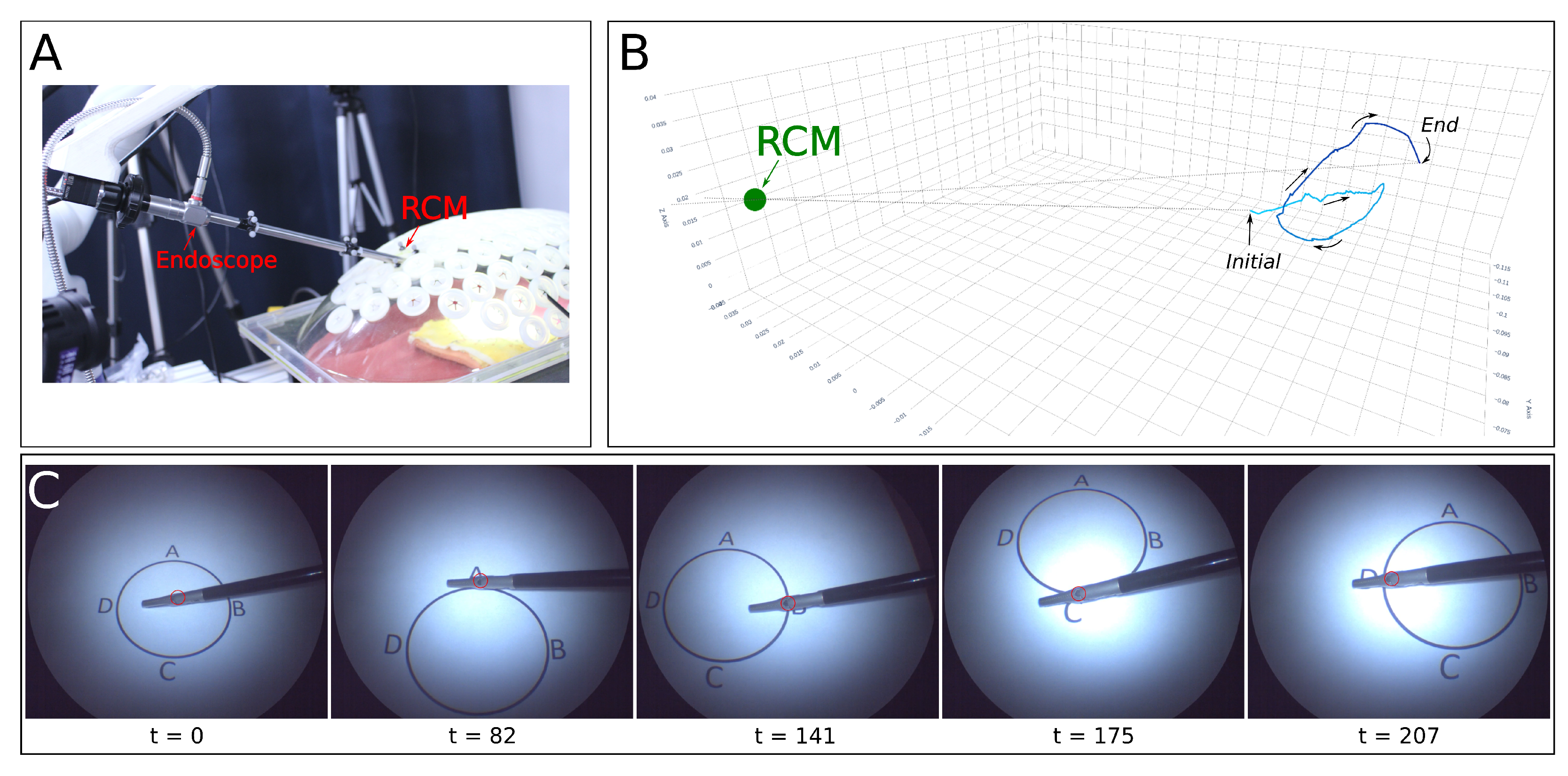
5.1. Experimental Setup
5.2. Single Tool Tracking
5.3. User Studies
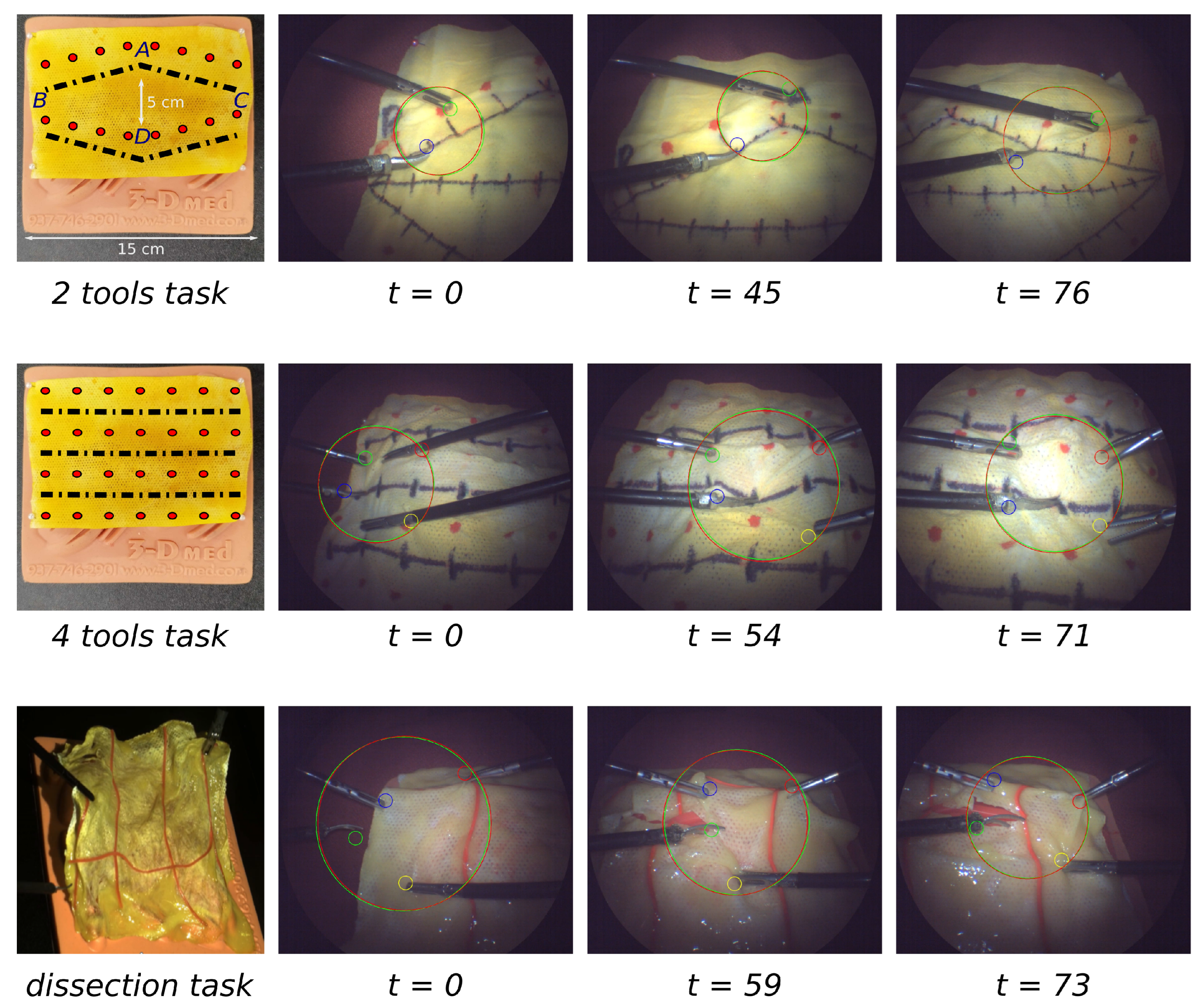
5.3.1. Task Scenarios
5.3.2. Participants for User Studies
- Each User 1 completes a 30-min training session with the tools on the day before the experiment.
- During the main study, User 1 performs the assigned task, interacting with a GUI to position the tools and initiate tracking.
- Upon selecting a path, User 1 manipulates the tissue with visual assistance from the endoscope robot until the task is completed. This is done five times, with the endoscope returning to its initial position after each iteration.
- Following the tasks, User 1 completes a survey designed to capture their subjective experience.
- For medical professionals only, additional insights are gathered through informal post-task interviews.
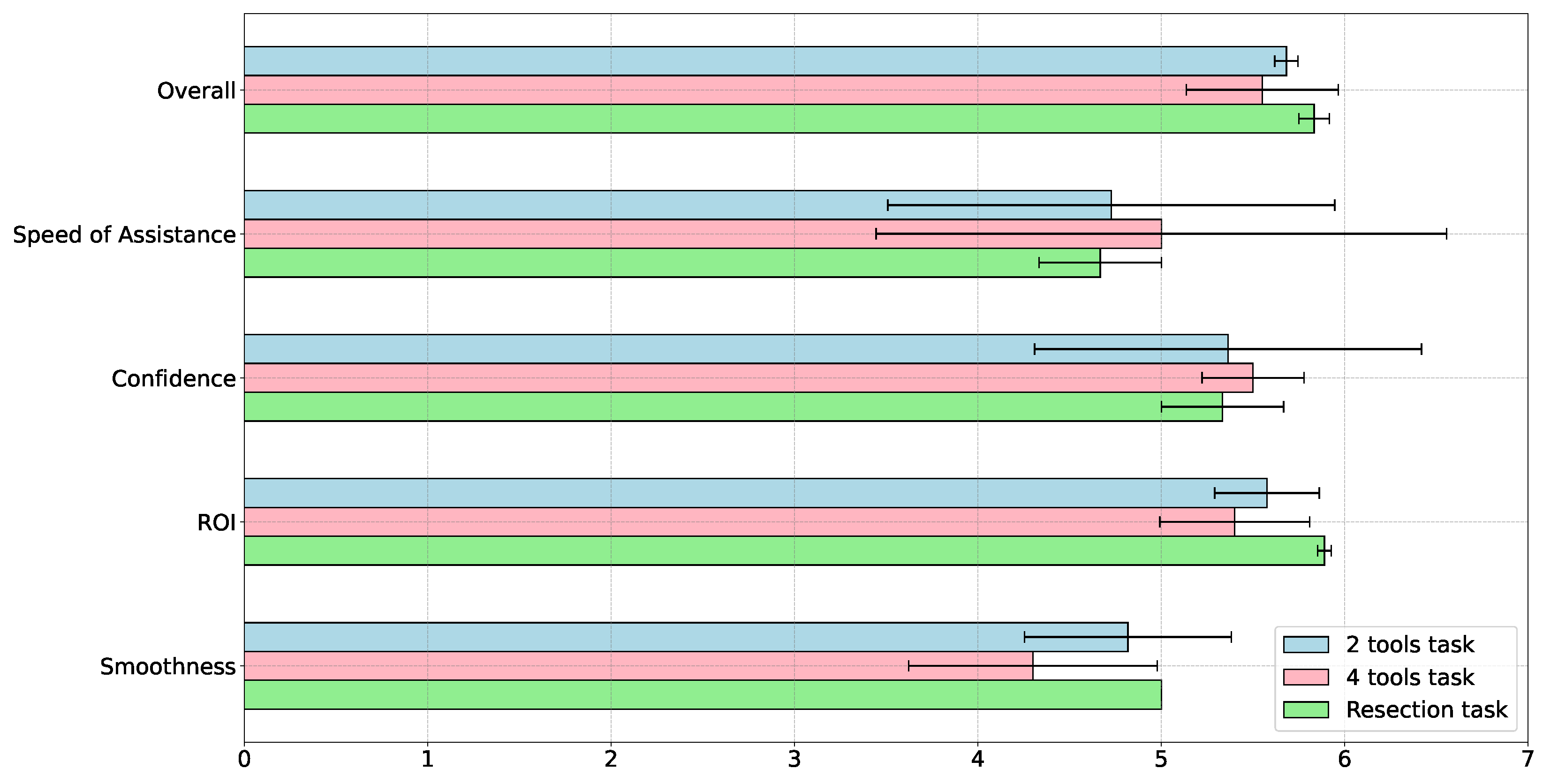
5.3.3. Experiment Questionnaires
5.3.4. Results on Users’ Case Studies
6. Conclusions and Future Works
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DOF | Degrees of Freedom |
| FOV | Field of View |
| GUI | Graphical User Interface |
| IK | Inverse Kinematics |
| IVP | Intuitive Virtual Plane |
| MIS | Minimally Invasive Surgery |
| QP | Quadratic Programming |
| RAMIS | Robot-Assisted Minimally Invasive Surgery |
| RCM | Remote Center of Motion |
| ROI | Region of Interest |
References
- Zelhart, M.; Kaiser, A.M. Robotic versus laparoscopic versus open colorectal surgery: Towards defining criteria to the right choice. Surg. Endosc. 2018, 32, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Su, P.; Li, J.; Yue, C.; Liu, T.; Liu, B.; Li, J. Preoperative positioning planning for a robot-assisted minimally invasive surgical system based on accuracy and safety. Int. J. Med. Robot. Comput. Assist. Surg. 2022, 18, e2405. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Luo, Y.; Wang, J.; Wang, X.; Song, H. Robotic-Assisted Laparoscopic Adjustment: A Meta-Analysis and Review. IEEE Trans. Instrum. Meas. 2023, 72, 5022019. [Google Scholar] [CrossRef]
- Nakawala, H.; De Momi, E.; Tzemanaki, A.; Dogramadzi, S.; Russo, A.; Catellani, M.; Bianchi, R.; Cobelli, O.D.; Sideridis, A.; Papacostas, E.; et al. Corrigendum to Requirements elicitation for robotic and computer-assisted minimally invasive surgery. Int. J. Adv. Robot. Syst. 2020, 17, 1729881420912871. [Google Scholar] [CrossRef]
- Aiono, S.; Gilbert, J.; Soin, B.; Finlay, P.; Gordan, A. Controlled trial of the introduction of a robotic camera assistant (Endo Assist) for laparoscopic cholecystectomy. Surg. Endosc. Other Interv. Tech. 2002, 16, 1267–1270. [Google Scholar] [CrossRef]
- Col, T.D.; Caccianiga, G.; Catellani, M.; Mariani, A.; Ferro, M.; Cordima, G.; Momi, E.D.; Ferrigno, G.; de Cobelli, O. Automating Endoscope Motion in Robotic Surgery: A Usability Study on da Vinci-Assisted Ex Vivo Neobladder Reconstruction. Front. Robot. AI 2021, 8, 707704. [Google Scholar] [CrossRef]
- Fujii, K.; Gras, G.; Salerno, A.; Yang, G.Z. Gaze gesture based human robot interaction for laparoscopic surgery. Med. Image Anal. 2018, 44, 196–214. [Google Scholar] [CrossRef]
- Zinchenko, K.; Song, K.T. Autonomous endoscope robot positioning using instrument segmentation with virtual reality visualization. IEEE Access 2021, 9, 72614–72623. [Google Scholar] [CrossRef]
- Qian, L.; Deguet, A.; Wang, Z.; Liu, Y.H.; Kazanzides, P. Augmented reality assisted instrument insertion and tool manipulation for the first assistant in robotic surgery. In Proceedings of the 2019 International Conference on Robotics and Automation (ICRA), Montreal, QC, Canada, 20–24 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 5173–5179. [Google Scholar]
- Attanasio, A.; Scaglioni, B.; De Momi, E.; Fiorini, P.; Valdastri, P. Autonomy in Surgical Robotics. Annu. Rev. Control Robot. Auton. Syst. 2021, 4, 651–679. [Google Scholar] [CrossRef]
- Fozilov, K.; Colan, J.; Sekiyama, K.; Hasegawa, Y. Toward Autonomous Robotic Minimally Invasive Surgery: A Hybrid Framework Combining Task-Motion Planning and Dynamic Behavior Trees. IEEE Access 2023, 11, 91206–91224. [Google Scholar] [CrossRef]
- Holden, J.G.; Flach, J.M.; Donchin, Y. Perceptual-motor coordination in an endoscopic surgery simulation. Surg. Endosc. 1999, 13, 127–132. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wentink, B. Eye-hand coordination in laparoscopy-an overview of experiments and supporting aids. Minim. Invasive Ther. Allied Technol. 2001, 10, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chen, W.; Wang, Z.; Lu, Y.; Mao, J.; Wang, H.; Liu, Y.H. Adaptive fov control of laparoscopes with programmable composed constraints. IEEE Trans. Med. Robot. Bionics 2019, 1, 206–217. [Google Scholar] [CrossRef]
- Yang, S.; Wang, Y.; Zhao, H.; Cheng, H.; Ding, H. Autonomous Laparoscope Control for Minimally Invasive Surgery with Intuition and RCM Constraints. IEEE Robot. Autom. Lett. 2022, 7, 7934–7941. [Google Scholar] [CrossRef]
- Qureshi, R.; Ragab, M.G.; Abdulkader, S.J.; Muneer, A.; Alqushaib, A.; Sumiea, E.H.; Alhussian, H. A Comprehensive Systematic Review of YOLO for Medical Object Detection (2018 to 2023). TechRxiv 2023. [Google Scholar] [CrossRef]
- Peng, J.; Chen, Q.; Kang, L.; Jie, H.; Han, Y. Autonomous Recognition of Multiple Surgical Instruments Tips Based on Arrow OBB-YOLO Network. IEEE Trans. Instrum. Meas. 2022, 71, 5007913. [Google Scholar] [CrossRef]
- Gruijthuijsen, C.; Garcia-Peraza-Herrera, L.C.; Borghesan, G.; Reynaerts, D.; Deprest, J.; Ourselin, S.; Vercauteren, T.; Vander Poorten, E. Robotic endoscope control via autonomous instrument tracking. Front. Robot. AI 2022, 9, 832208. [Google Scholar] [CrossRef]
- Li, L.; Li, X.; Ouyang, B.; Ding, S.; Yang, S.; Qu, Y. Autonomous multiple instruments tracking for robot-assisted laparoscopic surgery with visual tracking space vector method. IEEE/ASME Trans. Mechatron. 2021, 27, 733–743. [Google Scholar] [CrossRef]
- Kuo, C.H.; Dai, J.S.; Dasgupta, P. Kinematic design considerations for minimally invasive surgical robots: An overview. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 127–145. [Google Scholar] [CrossRef]
- Sadeghian, H.; Zokaei, F.; Hadian Jazi, S. Constrained kinematic control in minimally invasive robotic surgery subject to remote center of motion constraint. J. Intell. Robot. Syst. 2019, 95, 901–913. [Google Scholar] [CrossRef]
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. Optimization-based constrained trajectory generation for robot-assisted stitching in endonasal surgery. Robotics 2021, 10, 27. [Google Scholar] [CrossRef]
- Colan, J.; Davila, A.; Fozilov, K.; Hasegawa, Y. A Concurrent Framework for Constrained Inverse Kinematics of Minimally Invasive Surgical Robots. Sensors 2023, 23, 3328. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Lu, B.; Lu, Y.; Dou, Q.; Liu, Y.H. Data-driven holistic framework for automated laparoscope optimal view control with learning-based depth perception. In Proceedings of the 2021 IEEE International Conference on Robotics and Automation (ICRA), Xi’an, China, 30 May–5 June 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 12366–12372. [Google Scholar]
- Peng, J.; Zhang, C.; Kang, L.; Feng, G. Endoscope FOV Autonomous Tracking Method for Robot-Assisted Surgery Considering Pose Control, Hand–Eye Coordination, and Image Definition. IEEE Trans. Instrum. Meas. 2022, 71, 3522916. [Google Scholar] [CrossRef]
- Zhang, C.; Zhu, W.; Peng, J.; Han, Y.; Liu, W. Visual servo control of endoscope-holding robot based on multi-objective optimization: System modeling and instrument tracking. Measurement 2023, 211, 112658. [Google Scholar] [CrossRef]
- Cui, Z.; Li, W.; Zhang, X.; Chiu, P.W.Y.; Li, Z. Accelerated Dual Neural Network Controller for Visual Servoing of Flexible Endoscopic Robot with Tracking Error, Joint Motion, and RCM Constraints. IEEE Trans. Ind. Electron. 2022, 69, 9246–9257. [Google Scholar] [CrossRef]
- Huang, Y.; Li, J.; Zhang, X.; Xie, K.; Li, J.; Liu, Y.; Ng, C.S.H.; Chiu, P.W.Y.; Li, Z. A Surgeon Preference-Guided Autonomous Instrument Tracking Method with a Robotic Flexible Endoscope Based on dVRK Platform. IEEE Robot. Autom. Lett. 2022, 7, 2250–2257. [Google Scholar] [CrossRef]
- Ma, X.; Song, C.; Qian, L.; Liu, W.; Chiu, P.W.; Li, Z. Augmented Reality-Assisted Autonomous View Adjustment of a 6-DOF Robotic Stereo Flexible Endoscope. IEEE Trans. Med. Robot. Bionics 2022, 4, 356–367. [Google Scholar] [CrossRef]
- Huang, Y.; Li, W.; Zhang, X.; Li, J.; Li, Y.; Sun, Y.; Chiu, P.W.Y.; Li, Z. 4-DOF Visual Servoing of a Robotic Flexible Endoscope with a Predefined-Time Convergent and Noise-Immune Adaptive Neural Network. IEEE/ASME Trans. Mechatron. 2023, 1–12. [Google Scholar] [CrossRef]
- Kirillov, A.; Mintun, E.; Ravi, N.; Mao, H.; Rolland, C.; Gustafson, L.; Xiao, T.; Whitehead, S.; Berg, A.C.; Lo, W.Y.; et al. Segment anything. arXiv 2023, arXiv:2304.02643. [Google Scholar]
- Cheng, H.K.; Schwing, A.G. Xmem: Long-term video object segmentation with an atkinson-shiffrin memory model. In European Conference on Computer Vision; Springer: Cham, Switzerland, 2022; pp. 640–658. [Google Scholar]
- Quigley, M.; Conley, K.; Gerkey, B.; Faust, J.; Foote, T.; Leibs, J.; Wheeler, R.; Ng, A.Y.; Berger, E. ROS: An open-source Robot Operating System. In Proceedings of the ICRA Workshop on Open Source Software, Kobe, Japan, 12 May 2009; Volume 3, p. 5. [Google Scholar]
- Mazurowski, M.A.; Dong, H.; Gu, H.; Yang, J.; Konz, N.; Zhang, Y. Segment anything model for medical image analysis: An experimental study. Med. Image Anal. 2023, 89, 102918. [Google Scholar] [CrossRef]
- Colan, J.; Davila, A.; Hasegawa, Y. Constrained Motion Planning for a Robotic Endoscope Holder Based on Hierarchical Quadratic Programming. In Proceedings of the 2023 8th International Conference on Control and Robotics Engineering (ICCRE), Niigata, Japan, 21–23 April 2023; pp. 198–203. [Google Scholar] [CrossRef]
- Chiaverini, S. Singularity-robust task-priority redundancy resolution for real-time kinematic control of robot manipulators. IEEE Trans. Robot. Autom. 1997, 13, 398–410. [Google Scholar] [CrossRef]
- Kanoun, O.; Lamiraux, F.; Wieber, P.B. Kinematic Control of Redundant Manipulators: Generalizing the Task-Priority Framework to Inequality Task. IEEE Trans. Robot. 2011, 27, 785–792. [Google Scholar] [CrossRef]
- Hutchinson, S.; Hager, G.; Corke, P. A tutorial on visual servo control. IEEE Trans. Robot. Autom. 1996, 12, 651–670. [Google Scholar] [CrossRef]
- Solà, J.; Deray, J.; Atchuthan, D. A micro Lie theory for state estimation in robotics. arXiv 2018, arXiv:1812.01537. [Google Scholar] [CrossRef]
- Carpentier, J.; Saurel, G.; Buondonno, G.; Mirabel, J.; Lamiraux, F.; Stasse, O.; Mansard, N. The Pinocchio C++ library: A fast and flexible implementation of rigid body dynamics algorithms and their analytical derivatives. In Proceedings of the 2019 IEEE/SICE International Symposium on System Integration (SII), Paris, France, 14–16 January 2019; pp. 614–619. [Google Scholar] [CrossRef]
- Andersson, J.A.; Gillis, J.; Horn, G.; Rawlings, J.B.; Diehl, M. CasADi: A software framework for nonlinear optimization and optimal control. Math. Program. Comput. 2019, 11, 1–36. [Google Scholar] [CrossRef]
- Stellato, B.; Banjac, G.; Goulart, P.; Bemporad, A.; Boyd, S. OSQP: An operator splitting solver for quadratic programs. Math. Program. Comput. 2020, 12, 637–672. [Google Scholar] [CrossRef]
- Hart, S.G. NASA-task load index (NASA-TLX); 20 years later. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, San Francisco, CA, USA, 16–20 October 2006; Sage Publications: Los Angeles, CA, USA, 2006; Volume 50, pp. 904–908. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metrics | 2 Tools | 4 Tools | Resection |
|---|---|---|---|
| Manipulation Time (s) | 96.73 ± 10.34 | 164.27 ± 27.71 | 186.67 ± 21.59 |
| Following Rate (%) | 81.4 ± 21.7 | 76.1 ± 11.2 | 78.4 ± 22.9 |
| Tracking Error (pixels) | 113.30 ± 27.86 | 90.74 ± 38.48 | 91.68 ± 67.25 |
| Angle Error (deg) | 0.02522 ± 0.013196 | 0.01504 ± 0.01982 | 0.013599 ± 0.018781 |
| Depth Error (m) | 0.01108 ± 0.00439 | 0.00781 ± 0.00722 | 0.00974 ± 0.00799 |
| RCM Error (m) | 0.00279 ± 0.00181 | 0.00350 ± 0.00271 | 0.00431 ± 0.00311 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fozilov, K.; Colan, J.; Davila, A.; Misawa, K.; Qiu, J.; Hayashi, Y.; Mori, K.; Hasegawa, Y. Endoscope Automation Framework with Hierarchical Control and Interactive Perception for Multi-Tool Tracking in Minimally Invasive Surgery. Sensors 2023, 23, 9865. https://doi.org/10.3390/s23249865
Fozilov K, Colan J, Davila A, Misawa K, Qiu J, Hayashi Y, Mori K, Hasegawa Y. Endoscope Automation Framework with Hierarchical Control and Interactive Perception for Multi-Tool Tracking in Minimally Invasive Surgery. Sensors. 2023; 23(24):9865. https://doi.org/10.3390/s23249865
Chicago/Turabian StyleFozilov, Khusniddin, Jacinto Colan, Ana Davila, Kazunari Misawa, Jie Qiu, Yuichiro Hayashi, Kensaku Mori, and Yasuhisa Hasegawa. 2023. "Endoscope Automation Framework with Hierarchical Control and Interactive Perception for Multi-Tool Tracking in Minimally Invasive Surgery" Sensors 23, no. 24: 9865. https://doi.org/10.3390/s23249865
APA StyleFozilov, K., Colan, J., Davila, A., Misawa, K., Qiu, J., Hayashi, Y., Mori, K., & Hasegawa, Y. (2023). Endoscope Automation Framework with Hierarchical Control and Interactive Perception for Multi-Tool Tracking in Minimally Invasive Surgery. Sensors, 23(24), 9865. https://doi.org/10.3390/s23249865