
Biofeedback Respiratory Rehabilitation Training System Based on Virtual Reality Technology

Abstract
:1. Introduction
2. Related Work
2.1. Application of Virtual Reality Technology in Medical Field
2.2. Biofeedback Technology
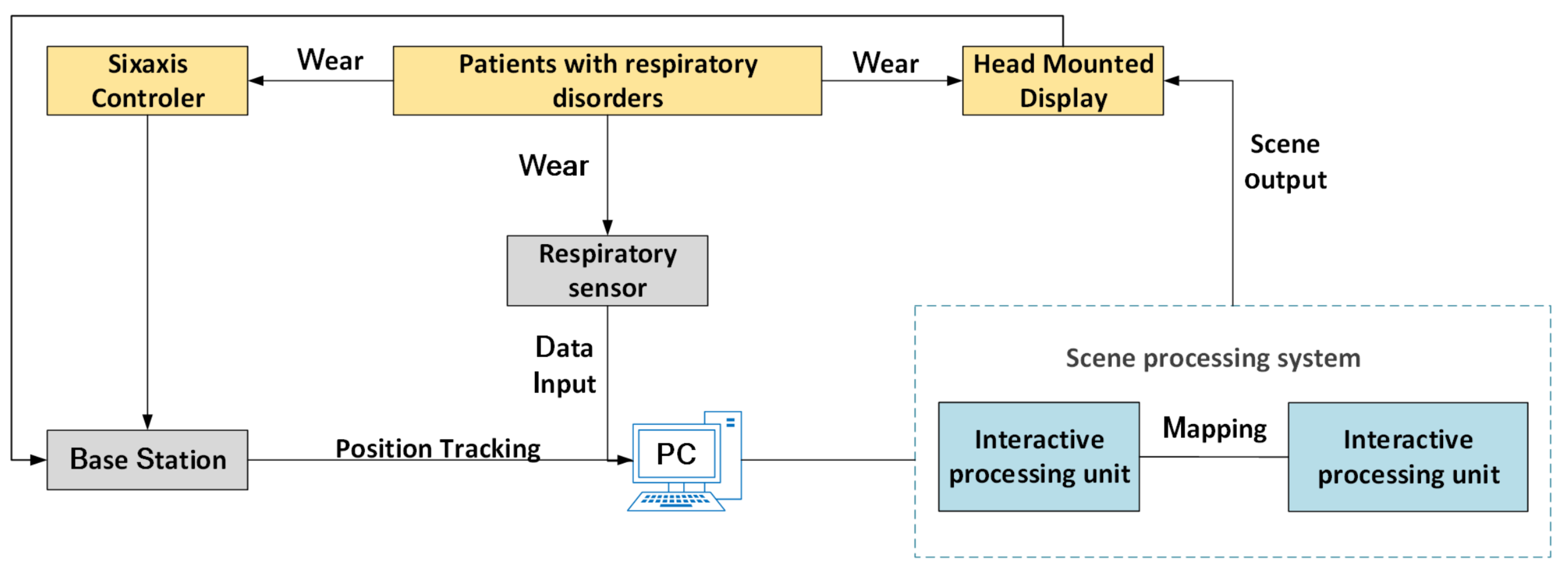
3. System Architecture
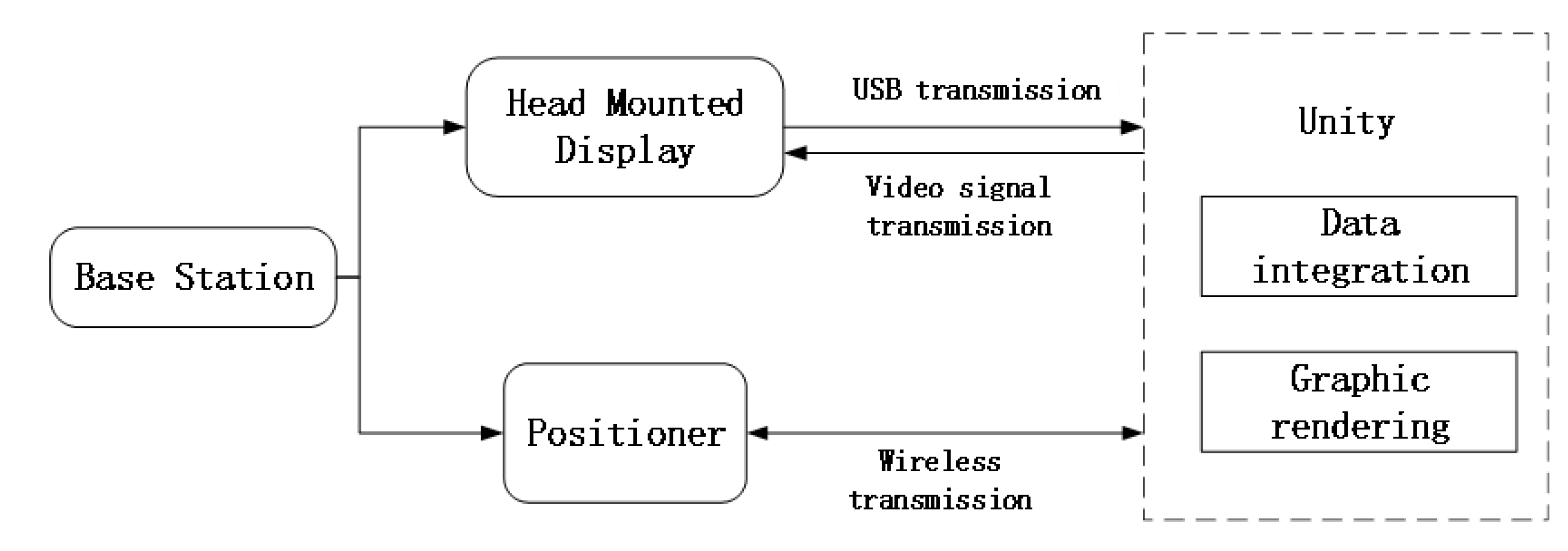
3.1. System Framework Structure
3.2. Hardware Equipment
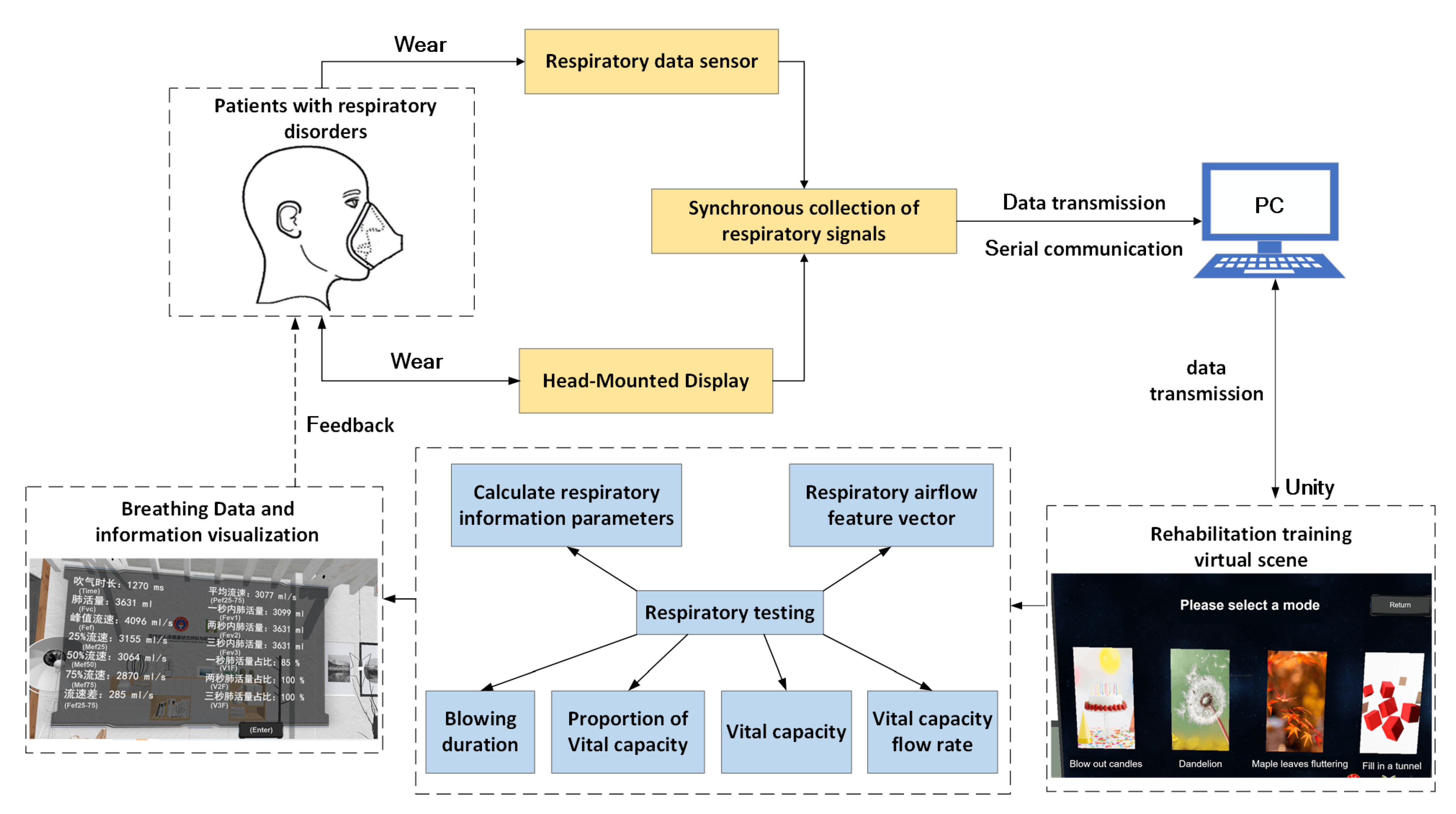
3.3. Interaction between Breathing Data and Virtual Scenes
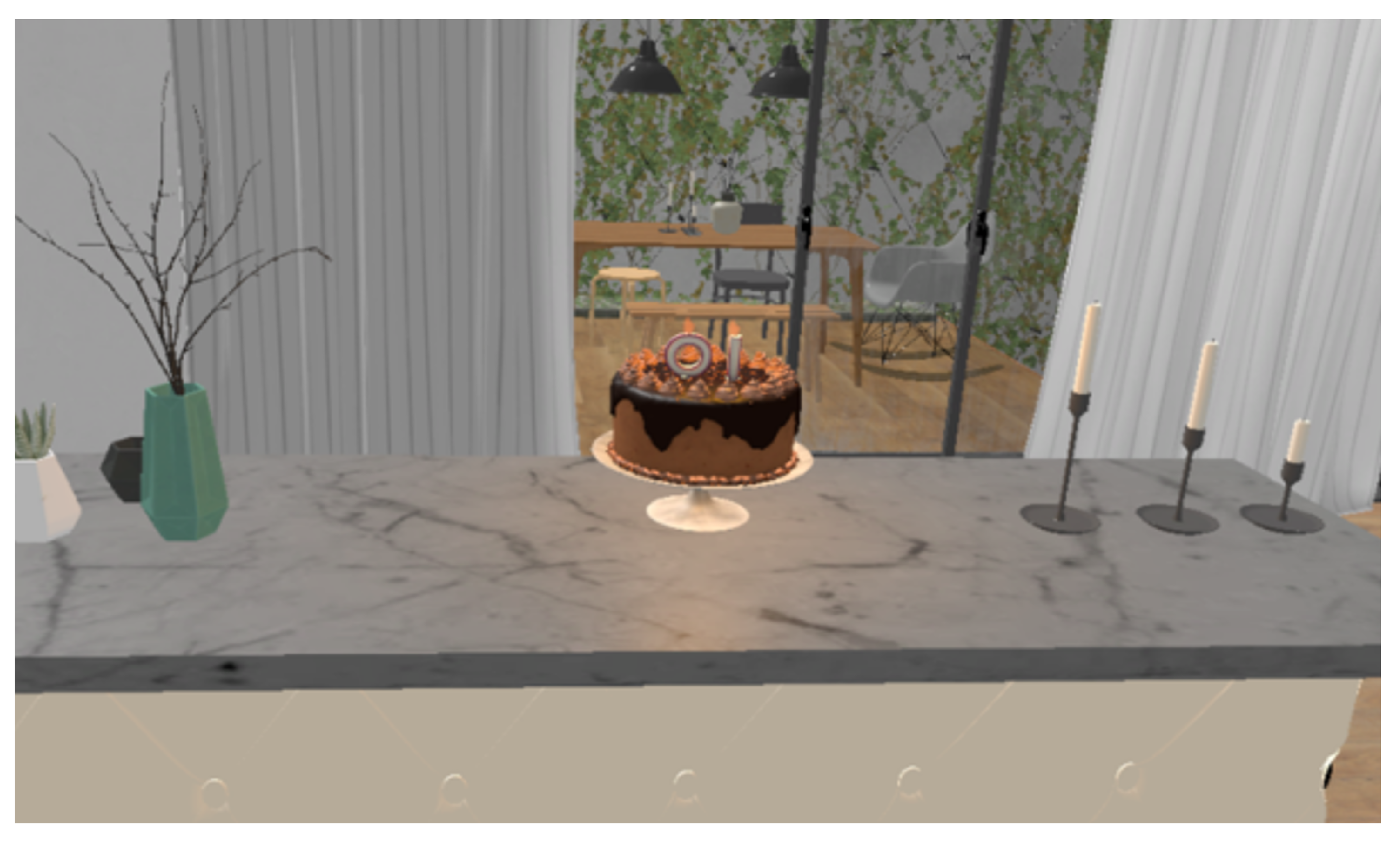
3.4. Virtual Scene Design
3.5. Breathing Data Collection Interaction and Visualization
3.5.1. Respiratory Data Collection
3.5.2. Analysis of Respiratory Data
| Algorithm 1: Respiratory data analysis algorithm. |
Input: collected respiratory data collection “cache” Output: Hexadecimal respiratory data set “lungData” 1. if cache.Count!=0 then 2. for int i = cache.Count-1; i >= 0; i– do 3. if i! = 0 then 4. if cache[i] == 0xc1&&cache[i-1] == 0xf0 then 5. Array.Copy(cache.ToArray(),i + 1,endData,0,endData.Length) 6. isReceived = true 7. cache.Clear() 8. if isReceived then 9. for int i = 0; i < endData.Length; i++ do 10. if i < 22 &&i % 2 == 0 then 11. hex += endData[i].ToString(“X2”) 12. hex += endData[i + 1].ToString(“X2”) 13. lungData.data.Add(Explain(hex)) 14. else if i < 25 then 15. hex += endData[i].ToString(“X2”) 16. data.Add(Explain(hex)) 17. lungData.GetDetail() |
3.5.3. Analysis of Respiratory Data
| Algorithm 2: Respiratory data interaction and visualization algorithm. |
1. if data.Count == 14 then 2. time = data[0],fvc = data[1],fef = data[2],mef25 = data[3],mef50 = data[4], mef75 = data[5],fef25–75 = data[6],pef25-75 = data[7],fev1 = data[8], fev2 = data[9],fev3 = data[10],v1f = data[11],v2f = data[12],v3f = data[13] 3. data.Clear() 4. if data.fvc > 1000 then 5. foreach var item in particle then 6. item.Stop() 7. item.transform.GetChild(0).gameObject.SetActive(false) 8. if Target ! = null then 9. if flag == false then 10. StartPort port = new StartPort() 11. byte[] data = GetData(port) 12. localClient.Send(data) 13. StartPort() 14. DebugMessage.Log() 15. Break |
4. Experiments and Results
4.1. Participants
- Meet the diagnostic criteria for COPD;
- During the rehabilitation training period, there is no resistance to cooperate with training and other behaviors;
- Good compliance during rehabilitation training and tolerance during training.
4.2. Experimental Process
- During training, do you feel bored?
- During the training process, are you distracted and have trouble concentrating?
- During the training process, are you able to keep up with the training pace?
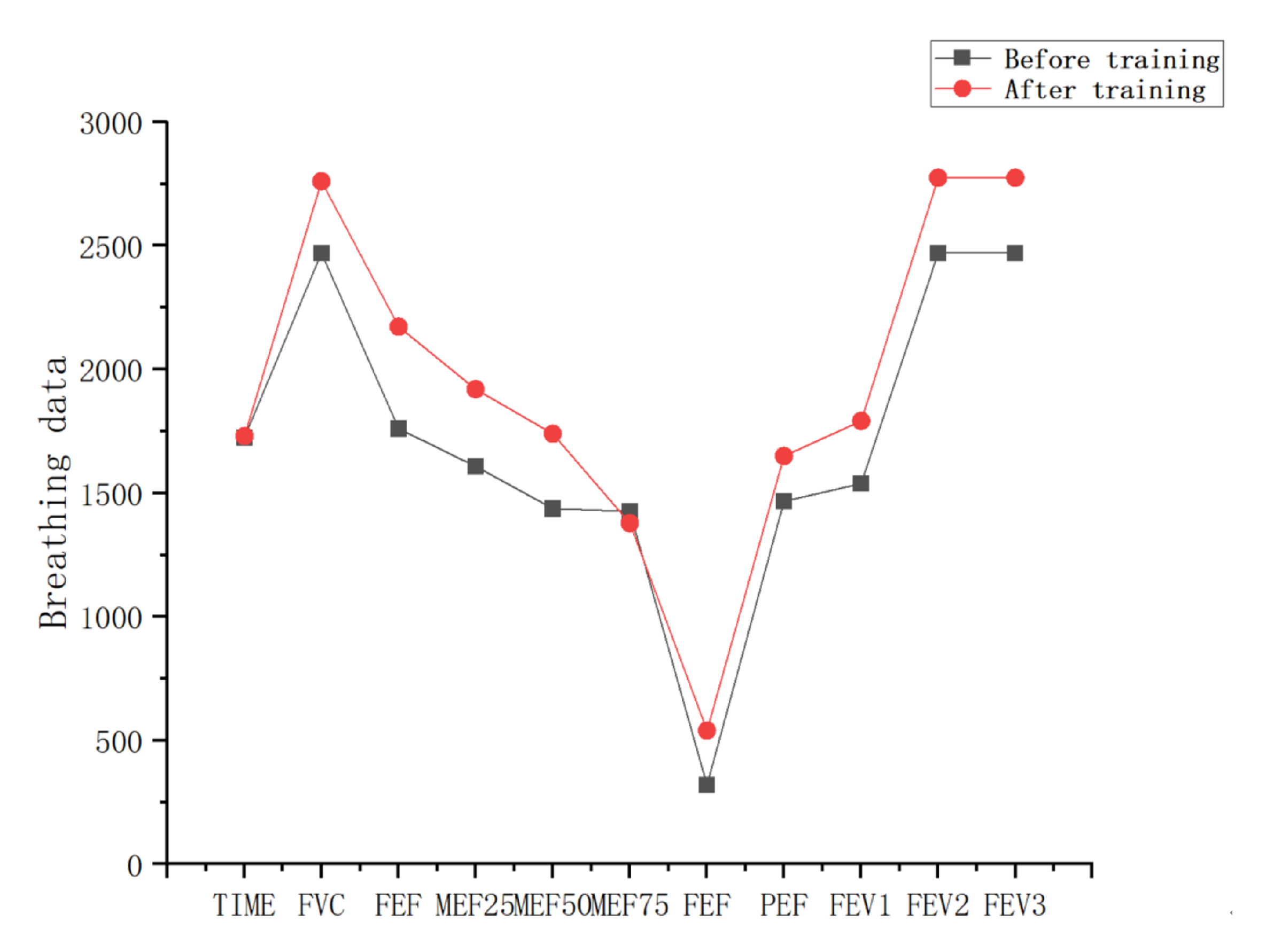
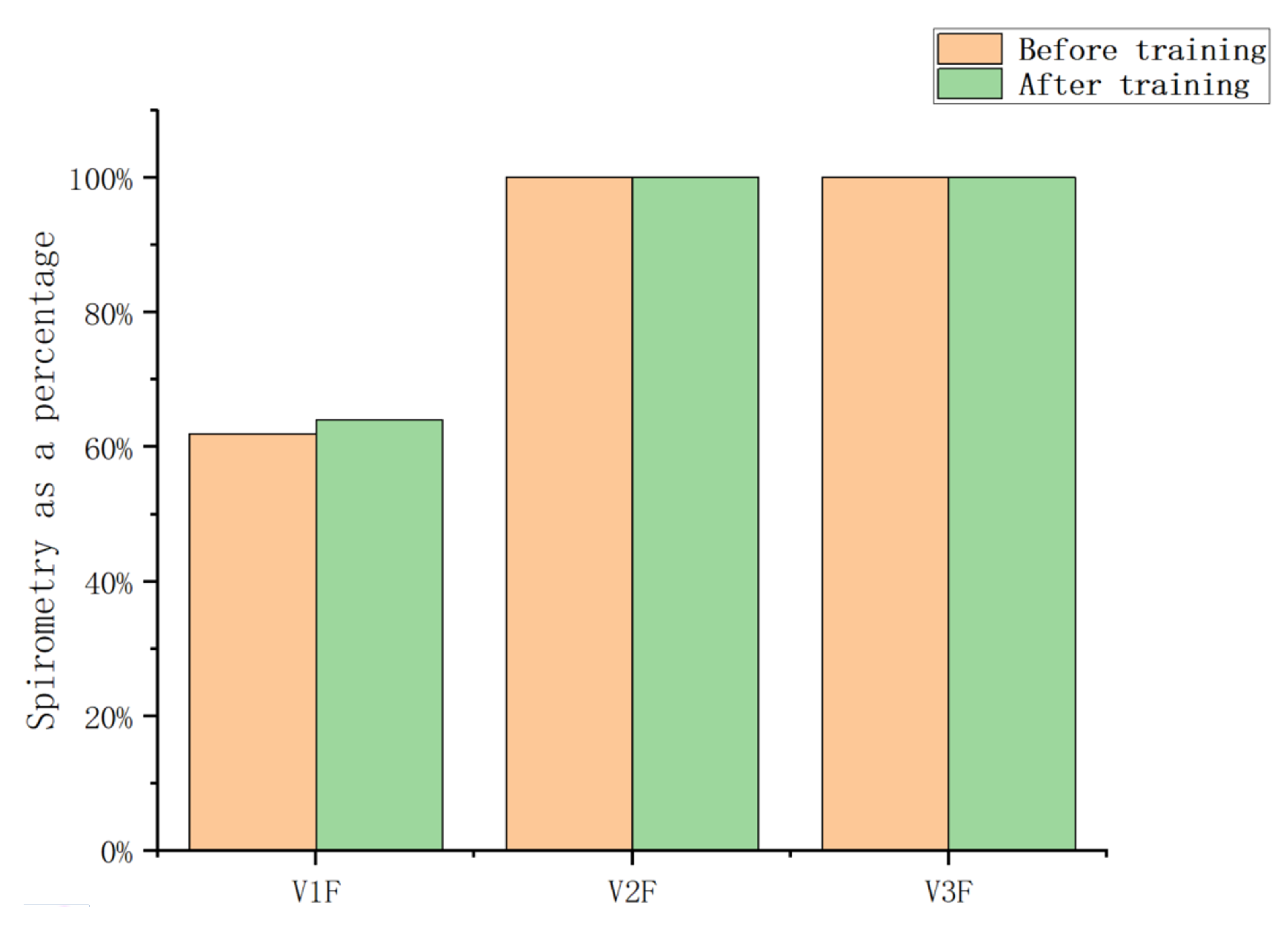
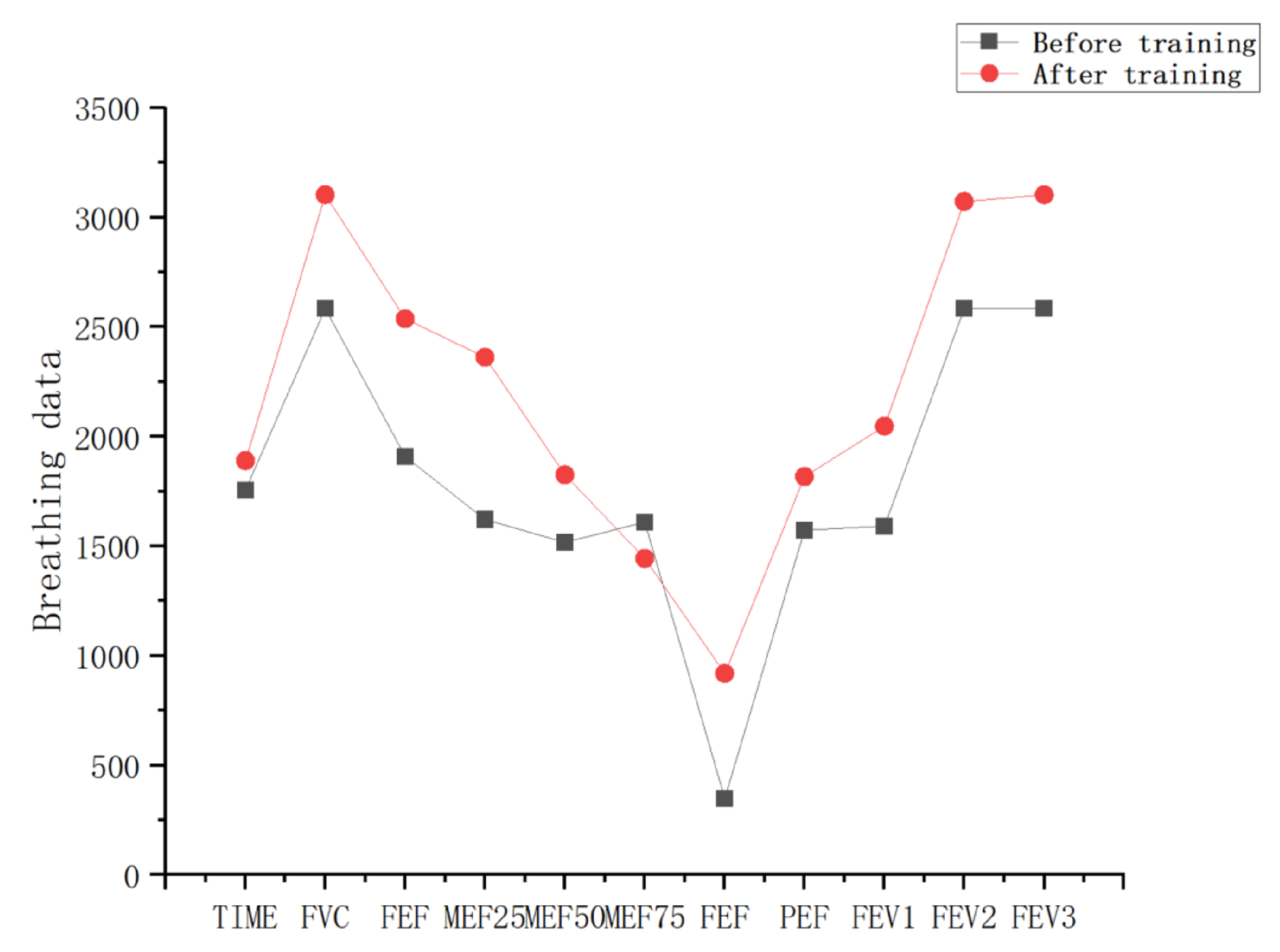
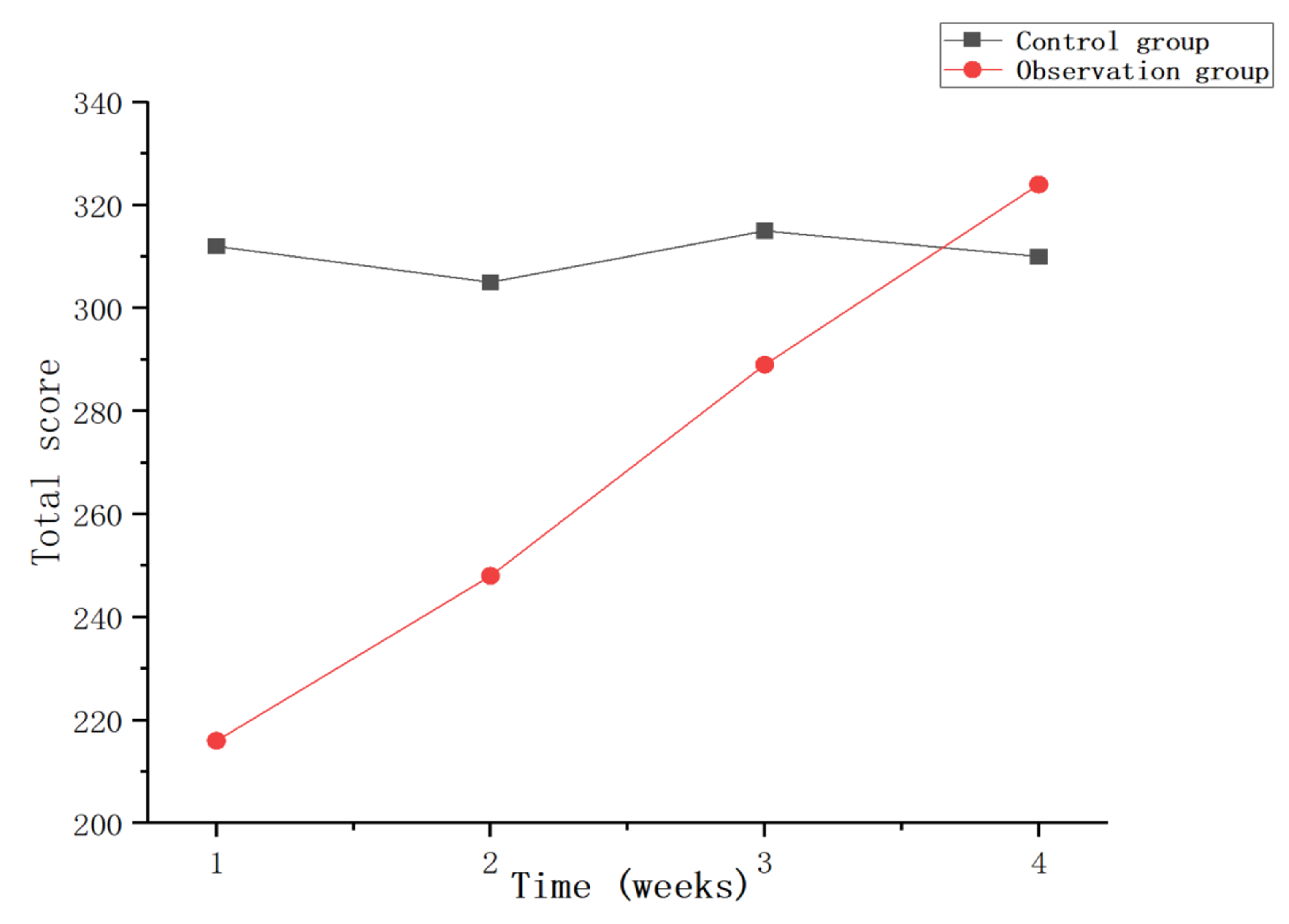
4.3. Experimental Results and Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Annesi-Maesano, I.; Forastiere, F.; Balmes, J.; Garcia, E.; Harkema, J.; Holgate, S.; Kelly, F.; Khreis, H.; Hoffmann, B.; Maesano, C.N.; et al. The clear and persistent impact of air pollution on chronic respiratory diseases: A call for interventions. Eur. Respir. J. 2021, 57, 2002981. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez Villegas, C.; Paz-Zulueta, M.; Herrero-Montes, M.; Parás-Bravo, P.; Madrazo Pérez, M. Cost analysis of chronic obstructive pulmonary disease (COPD): A systematic review. Health Econ. Rev. 2021, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, P.; Li, N.; Wang, Z.; Li, J.; Liu, X.; Wu, W. Effects of home-based breathing exercises in subjects with COPD. Respir. Care 2020, 65, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-Y.; Meijer, K.; Delbressine, J.M.; Willems, P.J.; Wouters, E.F.M. Spruit MA.Effects of Pulmonary Rehabilitation on Gait Characteristics in Patients with COPD. J. Clin. Med. 2019, 8, 459. [Google Scholar] [CrossRef]
- Respiratory Disease Branch of Chinese Geriatrics Society, Respiratory Rehabilitation Professional Committee of China Rehabilitation Medical Institutions Alliance. Chinese expert consensus on the application of inhalation therapy in respiratory rehabilitation. Chin. J. Tuberc. Respir. Med. 2022, 45, 753–761. [Google Scholar]
- Fen, D.; Ling, Y.; Lu, Z.; Lan, H. Respiratory function exercise for patients with frailty and pulmonary heart disease. Chin. J. Lung Dis. Electron. Vers. 2020, 13, 429–431. [Google Scholar]
- Liu, X.; Wang, J.; Sun, J.; Pan, K.; Wu, K.; Sun, C.; Ma, H. Effects of respiratory function exercise combined with psychological nursing on cardiopulmonary function index, exercise tolerance, and quality of life in patients with stable chronic obstructive pulmonary. Int. J. Early Child. Spec. Educ. INT-JECSE 2021, 30, 138–148. [Google Scholar]
- Liu, G. Application of abdominal breathing training + balloon blowing in rehabilitation care of patients with chronic persistent asthma. Heilongjiang Med. 2022, 46, 2518–2520. [Google Scholar]
- Zheng, L. Effect of intensive cough and respiratory function training on pulmonary rehabilitation in adult patients with spontaneous pneumothorax undergoing closed drainage. Tibet. Med. 2022, 43, 108–110. [Google Scholar]
- Sadiq, N.; Sadiq, T.; Baloch, W.A.; Khan, H.F.; Rajpoot, N.N.; Ali, S. Modulation of Heart Rate Variability in Stressed Medical Students Via Breathing Exercise. Pak. J. Med. Health Sci. 2023, 17, 117. [Google Scholar] [CrossRef]
- Bortone, I.; Leonardis, D.; Mastronicola, N.; Crecchi, A.; Bonfiglio, L.; Procopio, C.; Solazzi, M.; Frisoli, A. Wearable haptics and immersive virtual reality rehabilitation training in children with neuromotor impairments. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1469–1478. [Google Scholar] [CrossRef] [PubMed]
- Chandrasiri, A.; Collett, J.; Fassbender, E.; De Foe, A. A virtual reality approach to mindfulness skills training. Virtual Real. 2020, 24, 143–149. [Google Scholar] [CrossRef]
- Lan, K.C.; Li, C.W.; Cheung, Y. Slow breathing exercise with multimodal virtual reality: A feasibility study. Sensors 2021, 21, 5462. [Google Scholar] [CrossRef]
- Colombo, V.; Aliverti, A.; Sacco, M. Virtual reality for COPD rehabilitation: A technological perspective. Pulmonology 2022, 28, 119–133. [Google Scholar]
- Mitsea, E.; Drigas, A.; Skianis, C. Breathing, Attention & Consciousness in Sync: The role of Breathing Training, Metacognition & Virtual Reality. Technium Soc. Sci. J. 2022, 29, 79. [Google Scholar]
- Patsaki, I.; Avgeri, V.; Rigoulia, T.; Zekis, T.; Koumantakis, G.A.; Grammatopoulou, E. Benefits from Incorporating Virtual Reality in Pulmonary Rehabilitation of COPD Patients: A Systematic Review and Meta-Analysis. Adv. Respir. Med. 2023, 91, 324–336. [Google Scholar] [CrossRef]
- Gouveia, É.R.; Campos, P.; França, C.S.; Rodrigues, L.M.; Martins, F.; França, C.; Gonçalves, F.; Teixeira, F.; Ihle, A.; Gouveia, B.R. Virtual Reality Gaming in Rehabilitation after Musculoskeletal Injury—User Experience Pilot Study. Appl. Sci. 2023, 13, 2523. [Google Scholar] [CrossRef]
- Pur, D.R.; Lee-Wing, N.; Bona, M.D. The use of augmented reality and virtual reality for visual field expansion and visual acuity improvement in low vision rehabilitation: A systematic review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 1743–1755. [Google Scholar] [CrossRef]
- Si, T.; Zhu, Y.; Zongni, L. Application and Prospect of Immersive Virtual Reality Technology in Rehabilitation Practice of Autistic Children. Appl. Educ. Psychol. 2022, 3, 59–67. [Google Scholar]
- Ciorap, R.; Andriţoi, D.; Casuţă, A.; Ciorap, M.; Munteanu, D. Game-based virtual reality solution for post-stroke balance rehabilitation. IOP Conf. Ser. Mater. Sci. Eng. 2022, 1254, 012037. [Google Scholar]
- Rockstroh, C.; Blum, J.; Göritz, A.S. A mobile VR-based respiratory biofeedback game to foster diaphragmatic breathing. Virtual Real. 2021, 25, 539–552. [Google Scholar]
- Rutkowski, S.; Buekers, J.; Rutkowska, A.; Cieślik, B.; Szczegielniak, J. Monitoring physical activity with a wearable sensor in patients with copd during in-hospital pulmonary rehabilitation program: A pilot study. Sensors 2021, 21, 2742. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Zhou, Z.; Wu, Y.; Zhang, M. Application of mindfulness-based stress reduction therapy combined with music biofeedback therapy in infertile patients. Qilu Nurs. Mag. 2022, 28, 16–19. [Google Scholar]
- Patibanda, R.; Mueller, F.F.; Leskovsek, M.; Duckworth, J. Life Tree: Understanding the Design of Breathing Exercise Games. In Proceedings of the CHI PLAY ’17: The Annual Symposium on Computer-Human Interaction in Play, Amsterdam, The Netherlands, 15–18 October 2017; pp. 19–31. [Google Scholar]
- Greinacher, R.; Kojić, T.; Meier, L.; Parameshappa, R.G.; Möller, S.; Voigt-Antons, J.N. Impact of Tactile and Visual Feedback on Breathing Rhythm and User Experience in VR Exergaming. In Proceedings of the 2020 Twelfth International Conference on Quality of Multimedia Experience (QoMEX), Athlone, Ireland, 26–28 May 2020. [Google Scholar]
- Blum, J.; Rockstroh, C.; Göritz, A.S. Development and pilot test of a virtual reality respiratory biofeedback approach. Appl. Psychophysiol. Biofeedback 2020, 45, 153–163. [Google Scholar]
- Ji, W. Research on Interactive Design of Virtual Reality (VR) Animation; Central Academy of Fine Arts: Beijing, China, 2017. [Google Scholar]
- LoMauro, A.; Colli, A.; Colombo, L.; Aliverti, A. Breathing patterns recognition: A functional data analysis approach. Comput. Methods Programs Biomed. 2022, 217, 106670. [Google Scholar] [CrossRef]
- Keener, A. Redefining the diagnostic criteria for COPD. Nature 2020, 581, S4. [Google Scholar] [CrossRef]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I.; NIHR RESPIRE Global Respiratory Health Unit. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Byte Number | High and Low Byte Types | Respiration Data Type | |
|---|---|---|---|
| 0 | TIMEH Exhalation time high byte | Exhalation time | TIME |
| 1 | TIMEL Expiration time low byte | ||
| 2 | FVCH Vital Capacity FVC High Byte | Forced vital capacity | FVC |
| 3 | FVCL Vital Capacity FVC Low Byte | ||
| 4 | FEEH Peak flow rate high byte | Peak flow rate | FEF |
| 5 | FEEL Peak flow rate low byte | ||
| 6 | MEF25H Flow rate high byte | Flow rate at 25% vital capacity | MEF25 |
| 7 | MEF25L Flow rate low byte | ||
| 8 | MEF50H Flow rate high byte | Flow rate at 50% vital capacity | MEF25 |
| 9 | MEF50L Flow rate low byte | ||
| 10 | MEF75H Flow rate high byte | Flow rate at 75% vital capacity | MEF25 |
| 11 | MEF75L Flow rate low byte | ||
| 12 | FEF25-75H 25–75% flow rate difference high byte | Exhalation time | FEF25-75 |
| 13 | FEF25-75L 25–75% flow rate difference low byte | ||
| 14 | PEF25-75H 25–75% average velocity high byte | Average flow rate | PEF25-75 |
| 15 | PEF25-75L 25–75% average flow rate low byte | ||
| 16 | FEV1H Vital capacity high byte in the previous second | Vital capacity in one second | FEV1 |
| 17 | FEV1L Vital capacity low byte in the previous second | ||
| 18 | FEV2H Vital capacity high byte in the first two seconds | Two-second vital capacity | FEV2 |
| 19 | FEV2L Vital capacity low byte in the first two seconds | ||
| 20 | FEV3H Vital capacity high byte in the first three seconds | Three-second vital capacity | FEV3 |
| 21 | FEV3L Vital capacity low byte in the first three seconds | ||
| 22 | V1F Vital capacity in one second as a percentage of FEV1/FVC | Unit:% | |
| 23 | V2F Vital capacity in two seconds as a percentage of FEV2/FVC | ||
| 24 | V3F Three-second vital capacity as a percentage of FEV3/FVC | ||
| Participant ID | Gender | Age | Other Medical History | Tolerance | V1F |
|---|---|---|---|---|---|
| 1 | Man | 60 | NO | Well | <70% |
| 2 | Woman | 63 | NO | Well | <70% |
| 3 | Woman | 64 | NO | Well | <70% |
| 4 | Man | 59 | NO | Well | <70% |
| 5 | Man | 57 | NO | Well | <70% |
| 6 | Man | 64 | NO | Well | <70% |
| 7 | Man | 65 | NO | Well | <70% |
| 8 | Woman | 56 | NO | Well | <70% |
| 9 | Woman | 62 | NO | Well | <70% |
| 10 | Man | 58 | NO | Well | <70% |
| Serial Number | Question | Very Much Agree | Agree | General | Disagree | Strongly Disagree |
|---|---|---|---|---|---|---|
| 1 | During training, do you feel bored? | 1 | 2 | 3 | 4 | 5 |
| 2 | During training, are you distracted and unable to concentrate? | 1 | 2 | 3 | 4 | 5 |
| 3 | During training, are you unable to keep up with the training pace? | 1 | 2 | 3 | 4 | 5 |
| ID | TIME | FVC | FEF | MEF25 | MEF50 | MEF75 | FEF | PEF | FEV1 | FEV2 | FEV3 | V1F | V2F | V3F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ms) | (mL) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL) | (mL) | (mL) | (%) | (%) | (%) | |
| 1 | 1810 | 2311 | 1529 | 1297 | 1161 | 1487 | 190 | 1298 | 1244 | 2311 | 2311 | 53 | 100 | 100 |
| 2 | 1910 | 2497 | 1615 | 1601 | 1399 | 1001 | 600 | 1314 | 1494 | 2497 | 2497 | 59 | 100 | 100 |
| 3 | 1690 | 2689 | 1860 | 1729 | 1614 | 1605 | 124 | 1680 | 1700 | 2689 | 2689 | 63 | 100 | 100 |
| 4 | 1590 | 2420 | 1909 | 1667 | 1432 | 1274 | 393 | 1440 | 1585 | 2420 | 2420 | 65 | 100 | 100 |
| 5 | 1620 | 2431 | 1883 | 1747 | 1578 | 1757 | 290 | 1599 | 1668 | 2431 | 2431 | 68 | 100 | 100 |
| AVG | 1724 | 2470 | 1760 | 1609 | 1437 | 1425 | 319 | 1466 | 1538 | 2470 | 2470 | 62 | 100 | 100 |
| ID | TIME | FVC | FEF | MEF25 | MEF50 | MEF75 | FEF | PEF | FEV1 | FEV2 | FEV3 | V1F | V2F | V3F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ms) | (mL) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL) | (mL) | (mL) | (%) | (%) | (%) | |
| 1 | 1870 | 2719 | 1980 | 1652 | 1372 | 1312 | 340 | 1373 | 1555 | 2791 | 2791 | 57 | 100 | 100 |
| 2 | 1790 | 2686 | 2247 | 1825 | 1599 | 1244 | 581 | 1444 | 1688 | 2686 | 2686 | 62 | 100 | 100 |
| 3 | 1730 | 2582 | 1862 | 1712 | 1544 | 1355 | 357 | 1555 | 1649 | 2582 | 2582 | 63 | 100 | 100 |
| 4 | 1620 | 3379 | 2653 | 2396 | 2537 | 1646 | 750 | 2252 | 2341 | 3379 | 3379 | 69 | 100 | 100 |
| 5 | 1640 | 2432 | 2118 | 2010 | 1642 | 1335 | 675 | 1621 | 1724 | 2432 | 2432 | 70 | 100 | 100 |
| AVG | 1730 | 2760 | 2172 | 1919 | 1739 | 1378 | 540 | 1649 | 1791 | 2774 | 2774 | 64 | 100 | 100 |
| ID | TIME | FVC | FEF | MEF25 | MEF50 | MEF75 | FEF | PEF | FEV1 | FEV2 | FEV3 | V1F | V2F | V3F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ms) | (mL) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL) | (mL) | (mL) | (%) | (%) | (%) | |
| 6 | 1640 | 2543 | 1771 | 1708 | 1614 | 1489 | 219 | 1609 | 1665 | 2543 | 2543 | 65 | 100 | 100 |
| 7 | 1970 | 2393 | 1544 | 1410 | 1223 | 1078 | 332 | 1208 | 1360 | 2393 | 2393 | 56 | 100 | 100 |
| 8 | 1590 | 2908 | 2634 | 1941 | 1710 | 2634 | 639 | 1964 | 1870 | 2908 | 2908 | 64 | 100 | 100 |
| 9 | 1740 | 2833 | 1975 | 1539 | 1901 | 1716 | 177 | 1839 | 1685 | 2833 | 2833 | 59 | 100 | 100 |
| 10 | 1840 | 2244 | 1614 | 1509 | 1138 | 1129 | 380 | 1246 | 1381 | 2244 | 2244 | 61 | 100 | 100 |
| AVG | 1756 | 2584 | 1908 | 1621 | 1517 | 1609 | 349 | 1573 | 1592 | 2584 | 2584 | 61 | 100 | 100 |
| ID | TIME | FVC | FEF | MEF25 | MEF50 | MEF75 | FEF | PEF | FEV1 | FEV2 | FEV3 | V1F | V2F | V3F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ms) | (mL) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL/s) | (mL) | (mL) | (mL) | (%) | (%) | (%) | |
| 6 | 1590 | 2777 | 2327 | 2291 | 1785 | 1735 | 556 | 1851 | 1957 | 2777 | 2777 | 70 | 100 | 100 |
| 7 | 2180 | 3471 | 2620 | 2461 | 1751 | 1287 | 1174 | 1770 | 2117 | 3418 | 3471 | 60 | 100 | 100 |
| 8 | 1820 | 2903 | 2226 | 2062 | 1786 | 1418 | 644 | 1748 | 1918 | 2903 | 2903 | 66 | 100 | 100 |
| 9 | 1990 | 3160 | 2497 | 2134 | 1779 | 1396 | 738 | 1736 | 1990 | 3160 | 3160 | 62 | 100 | 100 |
| 10 | 1870 | 3205 | 3013 | 2864 | 2025 | 1382 | 1482 | 1978 | 2251 | 3205 | 3205 | 70 | 100 | 100 |
| AVG | 1890 | 3103 | 2537 | 2362 | 1825 | 1444 | 919 | 1817 | 2047 | 3072 | 3103 | 66 | 100 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, L.; Liu, F.; Liu, Y.; Wang, R.; Zhang, J.; Zhao, Z.; Zhao, J. Biofeedback Respiratory Rehabilitation Training System Based on Virtual Reality Technology. Sensors 2023, 23, 9025. https://doi.org/10.3390/s23229025
Shi L, Liu F, Liu Y, Wang R, Zhang J, Zhao Z, Zhao J. Biofeedback Respiratory Rehabilitation Training System Based on Virtual Reality Technology. Sensors. 2023; 23(22):9025. https://doi.org/10.3390/s23229025
Chicago/Turabian StyleShi, Lijuan, Feng Liu, Yuan Liu, Runmin Wang, Jing Zhang, Zisong Zhao, and Jian Zhao. 2023. "Biofeedback Respiratory Rehabilitation Training System Based on Virtual Reality Technology" Sensors 23, no. 22: 9025. https://doi.org/10.3390/s23229025
APA StyleShi, L., Liu, F., Liu, Y., Wang, R., Zhang, J., Zhao, Z., & Zhao, J. (2023). Biofeedback Respiratory Rehabilitation Training System Based on Virtual Reality Technology. Sensors, 23(22), 9025. https://doi.org/10.3390/s23229025