
Accelerometric Classification of Resting and Postural Tremor Amplitude

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
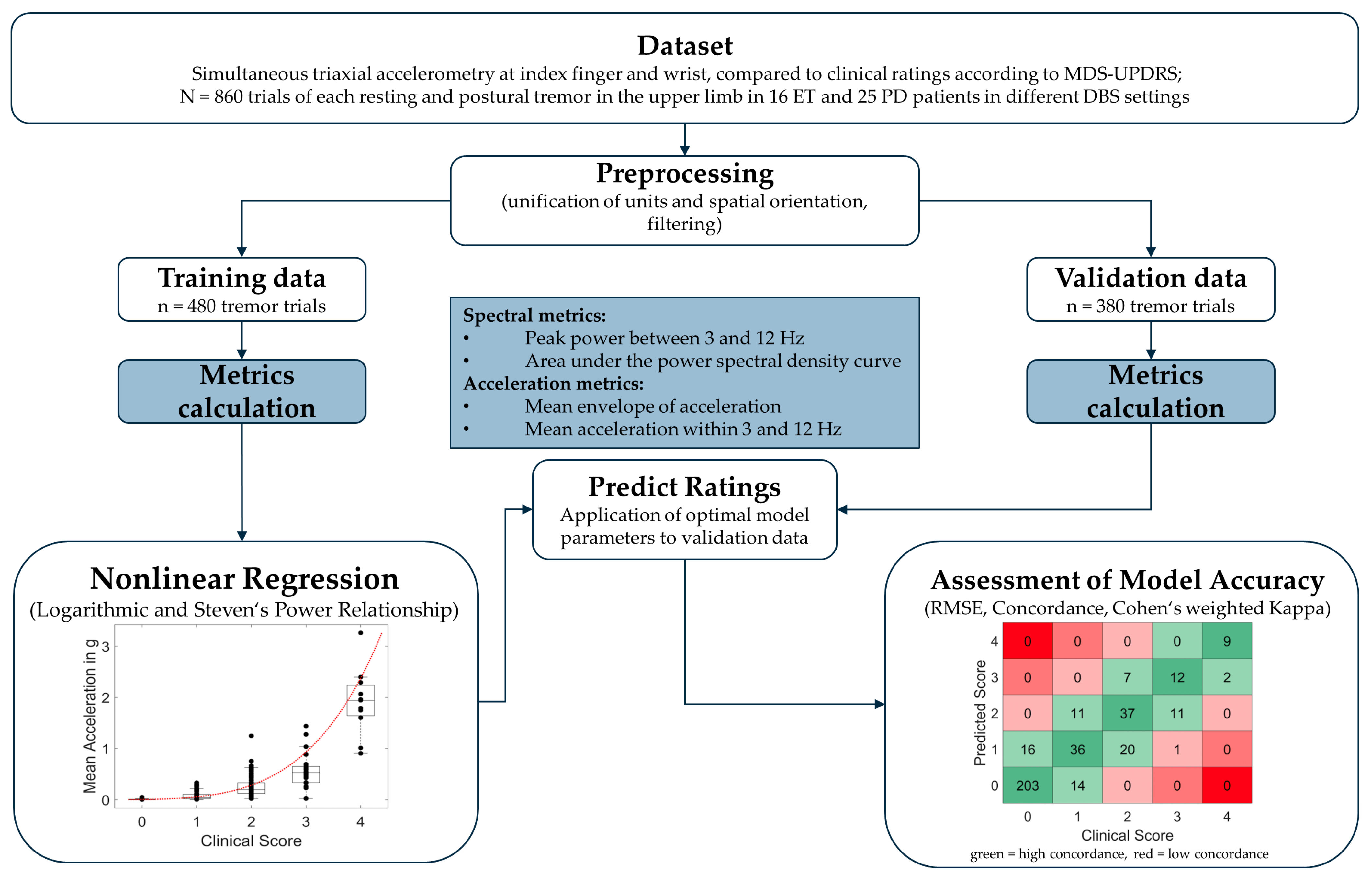
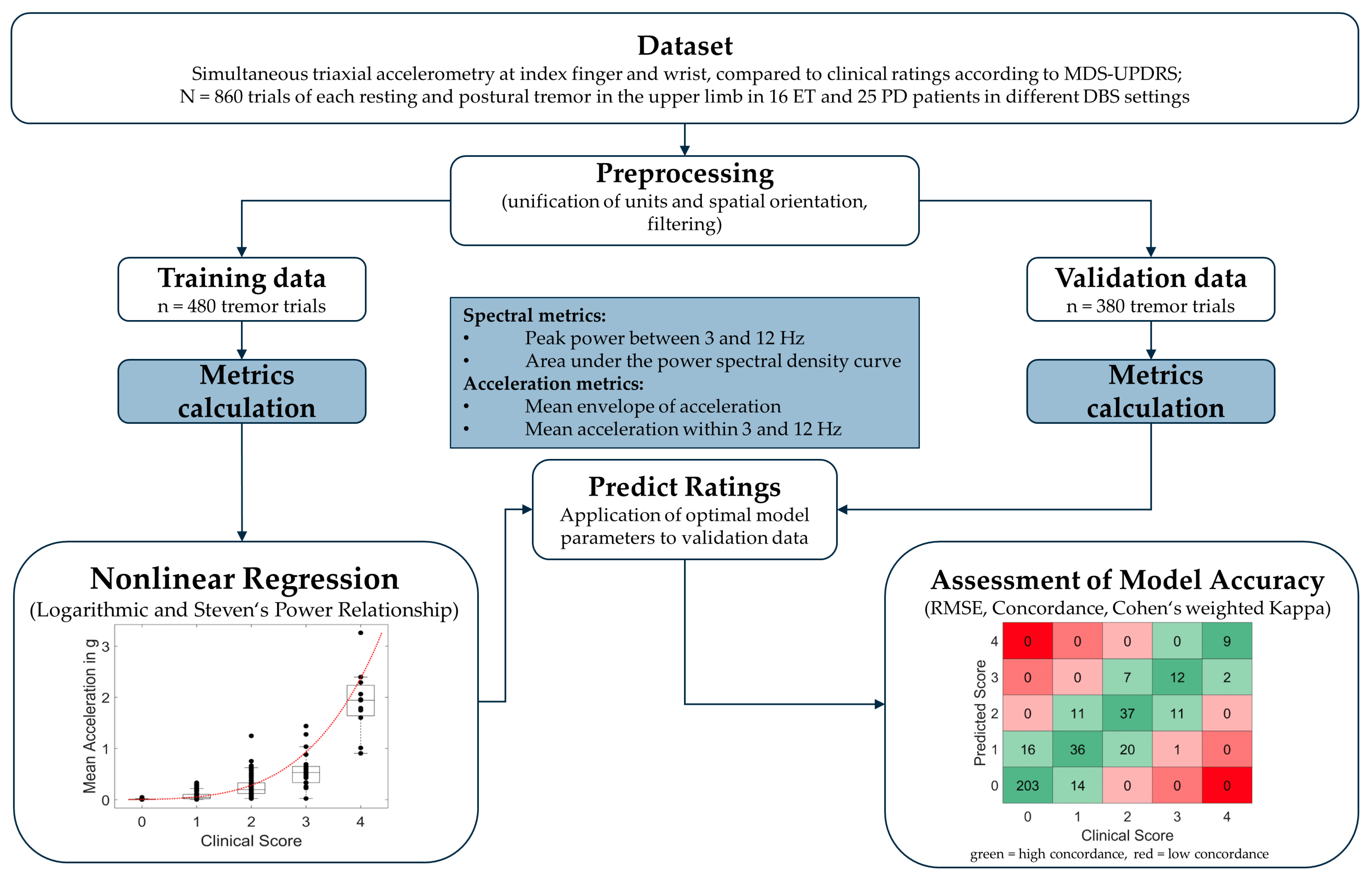
2.1. Dataset
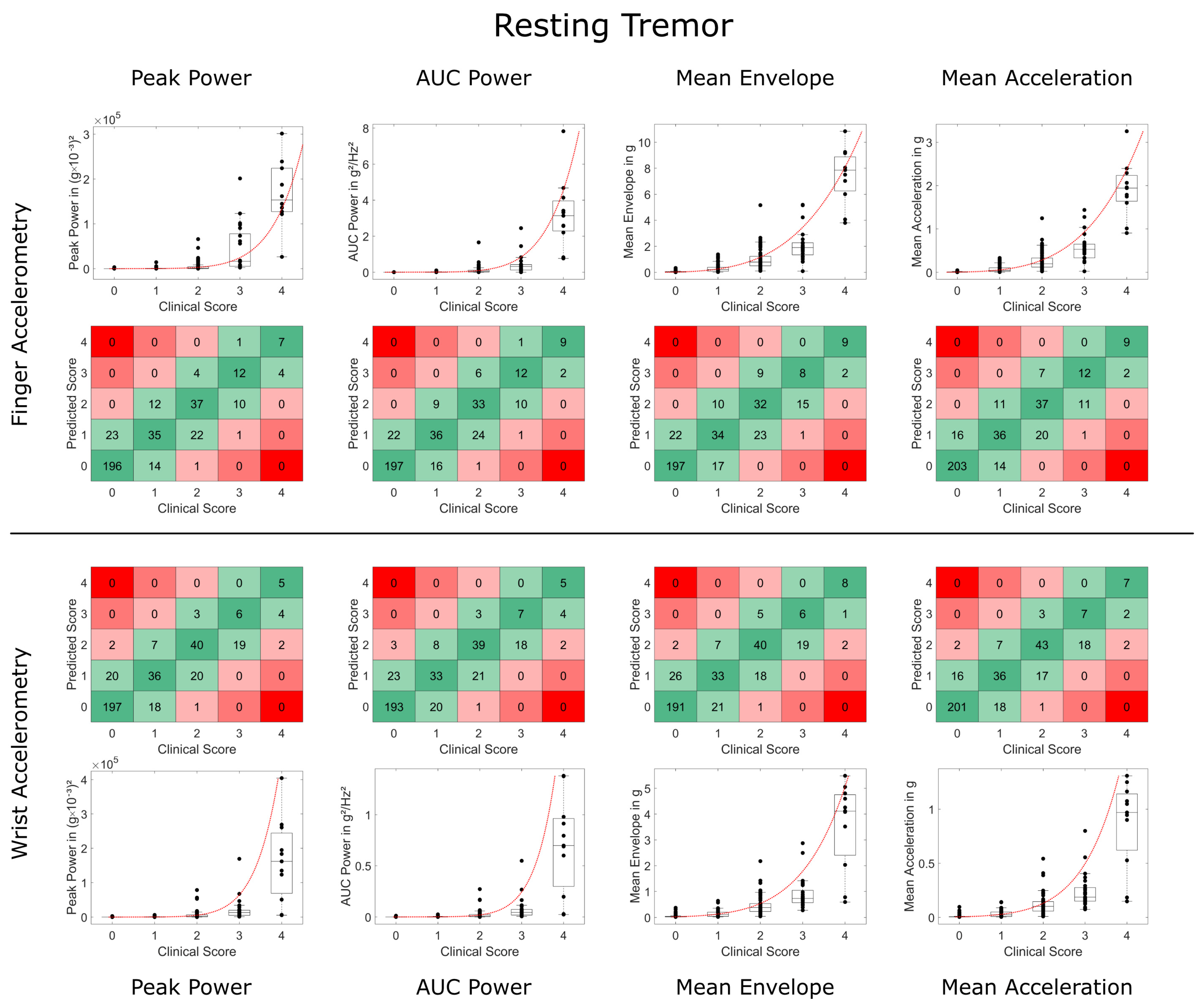
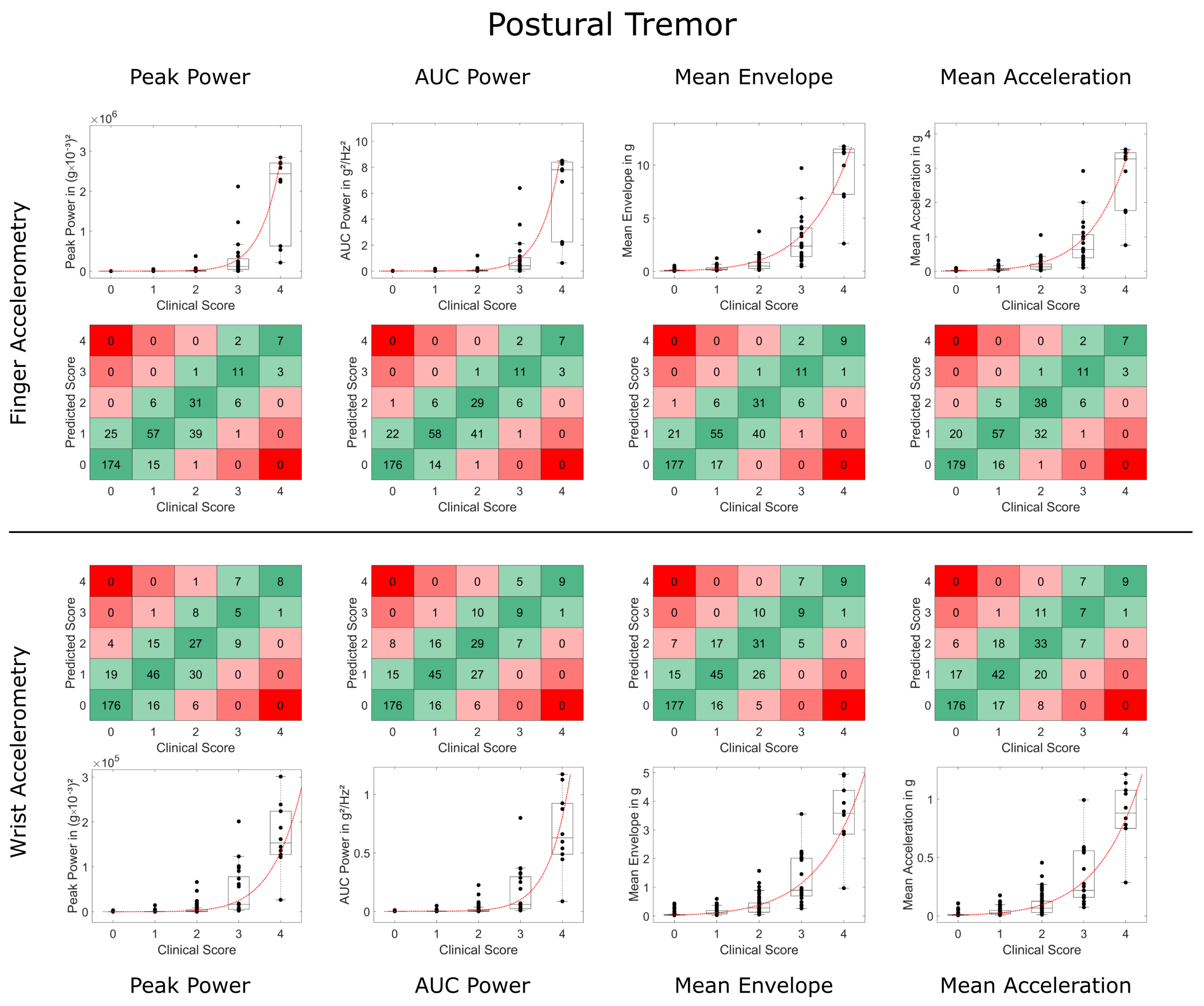
2.2. Tremor Tasks
2.3. Clinical Rating
2.4. Accelerometry
2.5. Preprocessing
2.6. Spectral Metrics of Tremor
2.7. Acceleration Metrics of Tremor
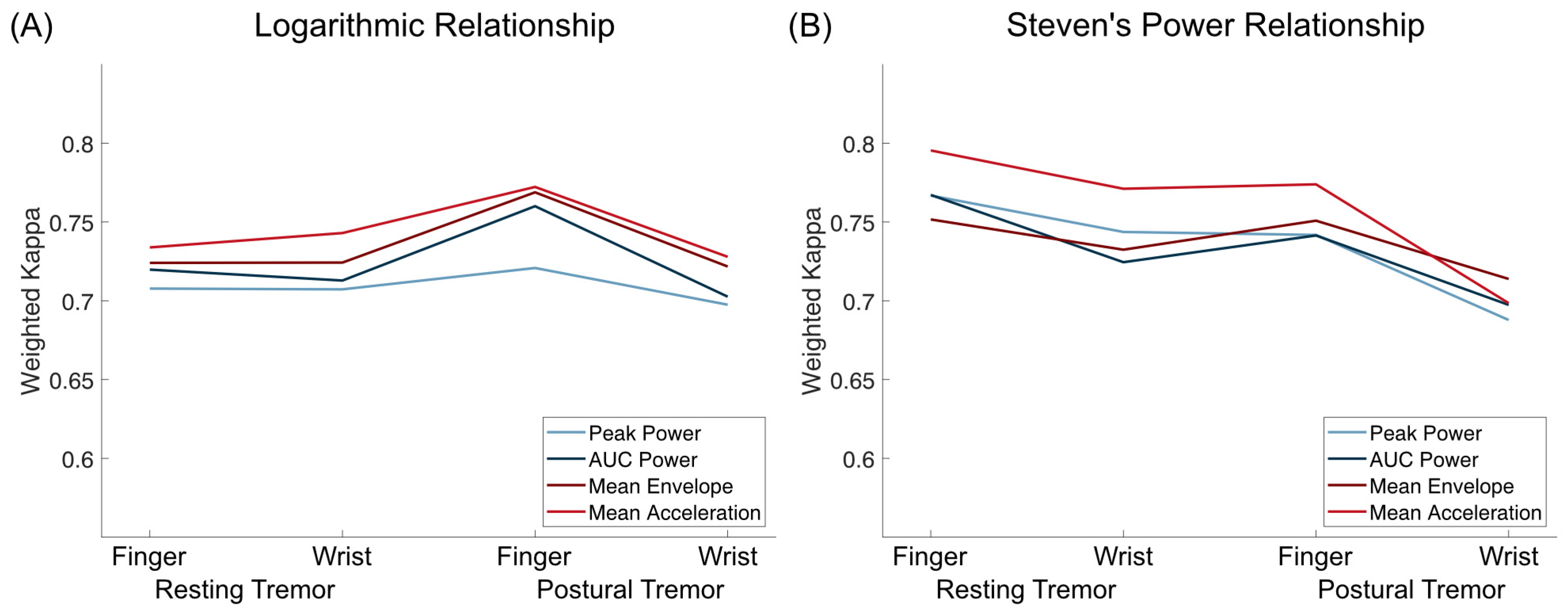
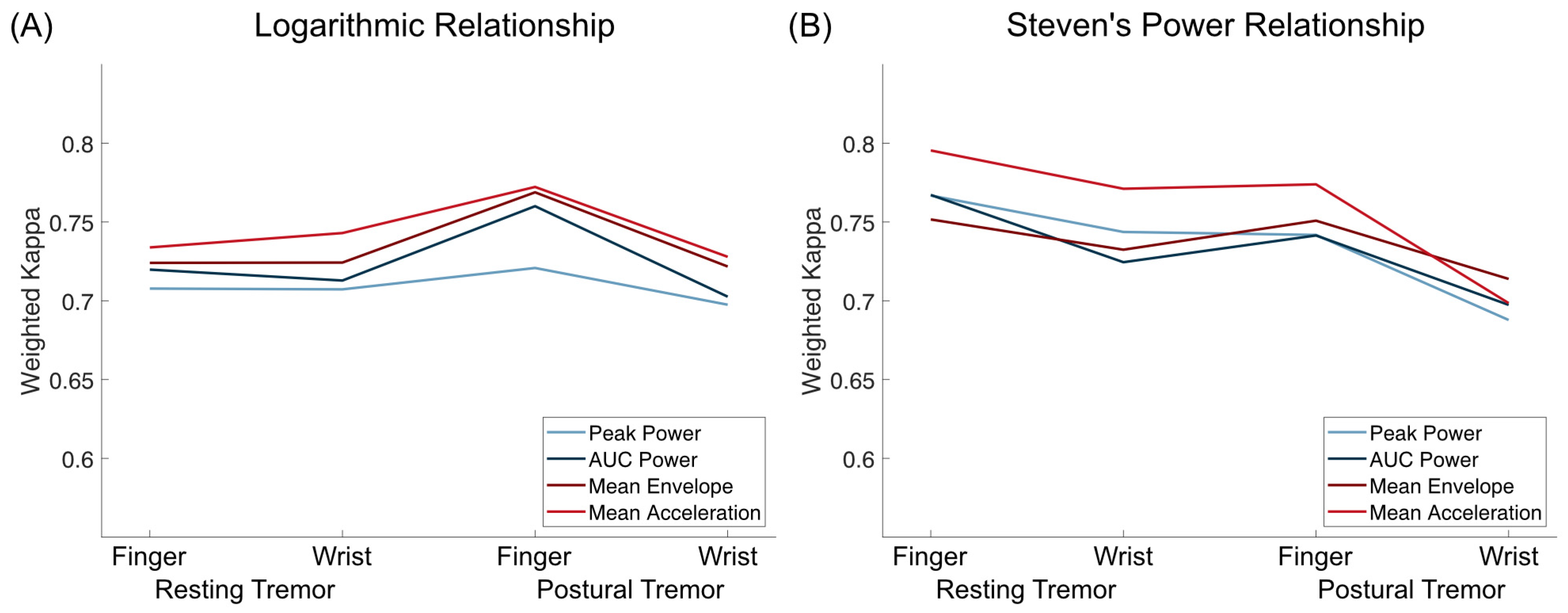
2.8. Relationship to Clinical Ratings
2.9. Statistical Analysis
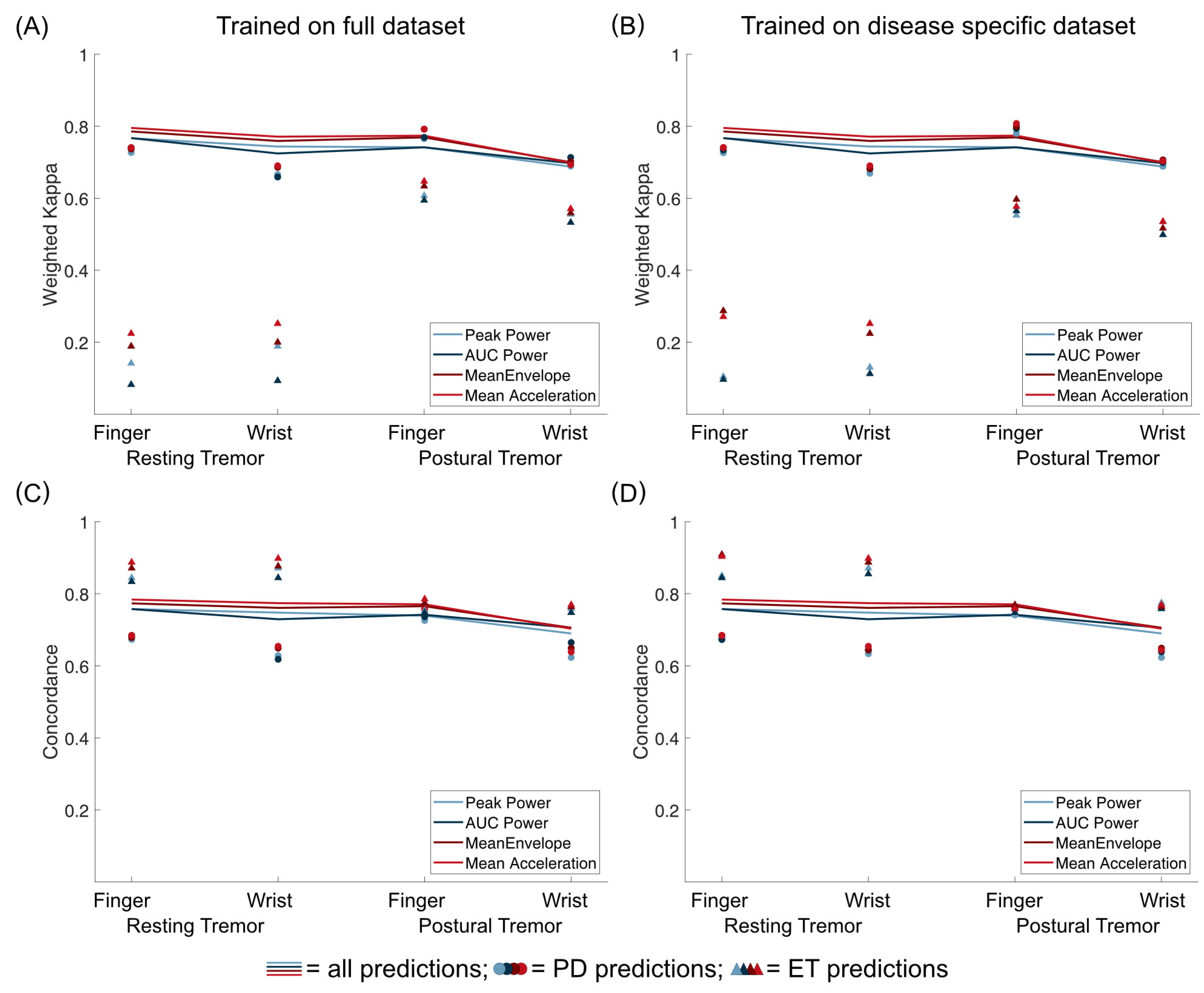
2.10. Post hoc Comparison of ET and PD
2.11. Technical Realization and Data Availability
3. Results
3.1. Training Data
3.2. Validation Data
3.3. Second Rater Data
3.4. Comparison between ET and PD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fahn, S.; Tolosa, E.; Marin, C. Clinical Rating Scale for Tremor. In Parkinson’s Disease and Movement Disorders; Williams and Wilkins: Baltimore, MD, USA, 1993; pp. 271–280. [Google Scholar]
- Elble, R.J. The Essential Tremor Rating Assessment Scale. J. Neurol. 2016, 1, 34–38. [Google Scholar]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J.; Ondo, W. Tremor Rating Scales and Laboratory Tools for Assessing Tremor. J. Neurol. Sci. 2022, 435, 120202. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J.; Pullman, S.L.; Matsumoto, J.Y.; Raethjen, J.; Deuschl, G.; Tintner, R. Tremor Amplitude Is Logarithmically Related to 4- and 5-Point Tremor Rating Scales. Brain 2006, 129, 2660–2666. [Google Scholar] [CrossRef]
- Stacy, M.A.; Elble, R.J.; Ondo, W.G.; Wu, S.-C.; Hulihan, J.; Group, T.S. Assessment of interrater and intrarater reliability of the Fahn–Tolosa–Marin Tremor Rating Scale in essential tremor. Mov. Disord. 2007, 22, 833–838. [Google Scholar] [CrossRef]
- Richards, M.; Marder, K.; Cote, L.; Mayeux, R. Interrater Reliability of the Unified Parkinson’s Disease Rating Scale Motor Examination. Mov. Disord. 1994, 9, 89–91. [Google Scholar] [CrossRef]
- Post, B.; Merkus, M.P.; de Bie, R.M.A.; de Haan, R.J.; Speelman, J.D. Unified Parkinson’s Disease Rating Scale Motor Examination: Are Ratings of Nurses, Residents in Neurology, and Movement Disorders Specialists Interchangeable? Mov. Disord. 2005, 20, 1577–1584. [Google Scholar] [CrossRef]
- Bain, P.G.; Findley, L.J.; Atchison, P.; Behari, M.; Vidailhet, M.; Gresty, M.; Rothwell, J.C.; Thompson, P.D.; Marsden, C.D. Assessing Tremor Severity. J. Neurol. Neurosurg. Psychiatry 1993, 56, 868–873. [Google Scholar] [CrossRef]
- Evers, L.J.W.; Krijthe, J.H.; Meinders, M.J.; Bloem, B.R.; Heskes, T.M. Measuring Parkinson’s Disease over Time: The Real-World within-Subject Reliability of the MDS-UPDRS. Mov. Disord. 2019, 34, 1480–1487. [Google Scholar] [CrossRef]
- Grimaldi, G.; Manto, M. Neurological Tremor: Sensors, Signal Processing and Emerging Applications. Sensors 2010, 10, 1399–1422. [Google Scholar] [CrossRef]
- Gauthier-Lafreniere, E.; Aljassar, M.; Rymar, V.V.; Milton, J.; Sadikot, A.F. A Standardized Accelerometry Method for Characterizing Tremor: Application and Validation in an Ageing Population with Postural and Action Tremor. Front. Neuroinform. 2022, 16, 878279. [Google Scholar] [CrossRef]
- Elble, R.J.; McNames, J. Using Portable Transducers to Measure Tremor Severity. Tremor Hyperkinetic Mov. 2016, 6, 375. [Google Scholar] [CrossRef]
- Lukšys, D.; Jonaitis, G.; Griškevičius, J. Quantitative Analysis of Parkinsonian Tremor in a Clinical Setting Using Inertial Measurement Units. Park. Dis. 2018, 2018, 1683831. [Google Scholar] [CrossRef]
- Smid, A.; Elting, J.W.J.; van Dijk, J.M.C.; Otten, B.; Oterdoom, D.L.M.; Tamasi, K.; Heida, T.; van Laar, T.; Drost, G. Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study. J. Clin. Med. 2022, 11, 2275. [Google Scholar] [CrossRef] [PubMed]
- Zach, H.; Dirkx, M.F.; Roth, D.; Pasman, J.W.; Bloem, B.R.; Helmich, R.C. Dopamine-Responsive and Dopamine-Resistant Resting Tremor in Parkinson Disease. Neurology 2020, 95, e1461–e1470. [Google Scholar] [CrossRef] [PubMed]
- Paschen, S.; Forstenpointner, J.; Becktepe, J.; Heinzel, S.; Hellriegel, H.; Witt, K.; Helmers, A.-K.; Deuschl, G. Long-Term Efficacy of Deep Brain Stimulation for Essential Tremor: An Observer-Blinded Study. Neurology 2019, 92, e1378–e1386. [Google Scholar] [CrossRef]
- Smid, A.; Oterdoom, D.L.M.; Pauwels, R.W.J.; Tamasi, K.; Elting, J.W.J.; Absalom, A.R.; Van Laar, T.; Van Dijk, J.M.C.; Drost, G. The Relevance of Intraoperative Clinical and Accelerometric Measurements for Thalamotomy Outcome. J. Clin. Med. 2023, 12, 5887. [Google Scholar] [CrossRef]
- San-Segundo, R.; Zhang, A.; Cebulla, A.; Panev, S.; Tabor, G.; Stebbins, K.; Massa, R.E.; Whitford, A.; de la Torre, F.; Hodgins, J. Parkinson’s Disease Tremor Detection in the Wild Using Wearable Accelerometers. Sensors 2020, 20, 5817. [Google Scholar] [CrossRef]
- Powers, R.; Etezadi-Amoli, M.; Arnold, E.M.; Kianian, S.; Mance, I.; Gibiansky, M.; Trietsch, D.; Alvarado, A.S.; Kretlow, J.D.; Herrington, T.M.; et al. Smartwatch Inertial Sensors Continuously Monitor Real-World Motor Fluctuations in Parkinson’s Disease. Sci. Transl. Med. 2021, 13, eabd7865. [Google Scholar] [CrossRef]
- Sahin, G.; Halje, P.; Uzun, S.; Jakobsson, A.; Petersson, P. Tremor Evaluation Using Smartphone Accelerometry in Standardized Settings. Front. Neurosci. 2022, 16, 861668. [Google Scholar] [CrossRef]
- Kostikis, N.; Hristu-Varsakelis, D.; Arnaoutoglou, M.; Kotsavasiloglou, C. A Smartphone-Based Tool for Assessing Parkinsonian Hand Tremor. IEEE J. Biomed. Health Inform. 2015, 19, 1835–1842. [Google Scholar] [CrossRef]
- Fujikawa, J.; Morigaki, R.; Yamamoto, N.; Nakanishi, H.; Oda, T.; Izumi, Y.; Takagi, Y. Diagnosis and Treatment of Tremor in Parkinson’s Disease Using Mechanical Devices. Life 2022, 13, 78. [Google Scholar] [CrossRef]
- Shah, A.; Coste, J.; Lemaire, J.-J.; Taub, E.; Schüpbach, W.M.M.; Pollo, C.; Schkommodau, E.; Guzman, R.; Hemm-Ode, S. Intraoperative Acceleration Measurements to Quantify Improvement in Tremor during Deep Brain Stimulation Surgery. Med. Biol. Eng. Comput. 2017, 55, 845–858. [Google Scholar] [CrossRef]
- Mcgurrin, P.; Mcnames, J.; Wu, T.; Hallett, M.; Haubenberger, D. Quantifying Tremor in Essential Tremor Using Inertial Sensors—Validation of an Algorithm. IEEE J. Transl. Eng. Health Med. 2021, 9, 1–10. [Google Scholar] [CrossRef]
- Brainard, D.H. The Psychophysics Toolbox. Spat. Vis. 1997, 10, 433–436. [Google Scholar] [CrossRef]
- Pelli, D.G. The VideoToolbox Software for Visual Psychophysics: Transforming Numbers into Movies. Spat. Vis. 1997, 10, 437–442. [Google Scholar] [CrossRef]
- Vergara-Diaz, G.; Daneault, J.-F.; Parisi, F.; Admati, C.; Alfonso, C.; Bertoli, M.; Bonizzoni, E.; Carvalho, G.F.; Costante, G.; Fabara, E.E.; et al. Limb and Trunk Accelerometer Data Collected with Wearable Sensors from Subjects with Parkinson’s Disease. Sci. Data 2021, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Haubenberger, D.; Hallett, M. Essential Tremor. N. Engl. J. Med. 2018, 378, 1802–1810. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G.; et al. Consensus Statement on the Classification of Tremors. from the Task Force on Tremor of the International Parkinson and Movement Disorder Society. Mov. Disord. 2018, 33, 75–87. [Google Scholar] [CrossRef]
- Portugal, R.D.; Svaiter, B.F. Weber-Fechner Law and the Optimality of the Logarithmic Scale. Minds Mach. 2011, 21, 73–81. [Google Scholar] [CrossRef]
- Delrobaei, M.; Memar, S.; Pieterman, M.; Stratton, T.W.; McIsaac, K.; Jog, M. Towards Remote Monitoring of Parkinson’s Disease Tremor Using Wearable Motion Capture Systems. J. Neurol. Sci. 2018, 384, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Mostile, G.; Giuffrida, J.P.; Adam, O.R.; Davidson, A.; Jankovic, J. Correlation between Kinesia System Assessments and Clinical Tremor Scores in Patients with Essential Tremor. Mov. Disord. 2010, 25, 1938–1943. [Google Scholar] [CrossRef]
- Afaq, S.; Loh, M.; Kooner, J.; Chambers, J. Evaluation of Three Accelerometer Devices for Physical Activity Measurement Amongst South Asians and Europeans. Phys. Act. Health 2020, 4, 1–10. [Google Scholar] [CrossRef]
- Bloem, B.R.; Post, E.; Hall, D.A. An Apple a Day to Keep the Parkinson’s Disease Doctor Away? Ann. Neurol. 2023, 93, 681–685. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tremortype | Location | Metric | TR = a × ln(T) + b | RMSE | Weighted Kappa | Concordance | 1 Pt Deviation | >1 Pt Deviation | |
|---|---|---|---|---|---|---|---|---|---|
| a | b | ||||||||
| Resting Tremor | Finger | Peak Power | 0.223 | −0.257 | 0.528 | 0.708 | 68.1% | 31.4% | 0.5% |
| AUC Power | 0.244 | 2.601 | 0.527 | 0.72 | 69.9% | 29.8% | 0.3% | ||
| Mean Envelope | 0.532 | 1.958 | 0.51 | 0.724 | 70.2% | 29.6% | 0.3% | ||
| Mean Acceleration | 0.502 | 2.68 | 0.492 | 0.734 | 70.7% | 29% | 0.3% | ||
| Wrist | Peak Power | 0.258 | 3.368 | 0.537 | 0.707 | 71.3% | 27.1% | 1.6% | |
| AUC Power | 0.3 | 3.22 | 0.536 | 0.713 | 71.8% | 26.6% | 1.6% | ||
| Mean Envelope | 0.671 | 2.456 | 0.518 | 0.724 | 72.6% | 26.1% | 1.3% | ||
| Mean Acceleration | 0.631 | 3.321 | 0.489 | 0.743 | 74.7% | 23.9% | 1.3% | ||
| Postural Tremor | Finger | Peak Power | 0.281 | 3.084 | 0.515 | 0.721 | 72% | 27.4% | 0.5% |
| AUC Power | 0.318 | 2.852 | 0.511 | 0.76 | 76% | 23.2% | 0.8% | ||
| Mean Envelope | 0.701 | 1.997 | 0.502 | 0.769 | 76.5% | 23% | 0.5% | ||
| Mean Acceleration | 0.655 | 2.932 | 0.485 | 0.772 | 76.8% | 22.7% | 0.5% | ||
| Wrist | Peak Power | 0.296 | 3.707 | 0.581 | 0.697 | 70.3% | 27.4% | 2.4% | |
| AUC Power | 0.363 | 3.7 | 0.581 | 0.703 | 70.8% | 26.1% | 3.2% | ||
| Mean Envelope | 0.819 | 2.802 | 0.569 | 0.722 | 72.6% | 24.2% | 3.2% | ||
| Mean Acceleration | 0.761 | 3.812 | 0.565 | 0.728 | 73.2% | 23.7% | 3.2% | ||
| Tremortype | Location | Metric | TR = a × Tc + b | RMSE | Weighted Kappa | Concordance | 1 Pt Deviation | >1 Pt Deviation | ||
|---|---|---|---|---|---|---|---|---|---|---|
| a | b | c | ||||||||
| Resting Tremor | Finger | Peak Power | 0.757 | −0.83 | 0.13 | 0.448 | 0.767 | 75.7% | 23.7% | 0.5% |
| AUC Power | 3.963 | −0.872 | 0.136 | 0.461 | 0.767 | 75.7% | 23.7% | 0.5% | ||
| Mean Envelope | 2.985 | −1.106 | 0.257 | 0.461 | 0.752 | 73.9% | 25.9% | 0.3% | ||
| Mean Acceleration | 4.315 | −1.244 | 0.226 | 0.438 | 0.795 | 78.4% | 21.4% | 0.3% | ||
| Wrist | Peak Power | 1.586 | −1.669 | 0.098 | 0.505 | 0.744 | 74.7% | 23.9% | 1.3% | |
| AUC Power | 6.919 | −3.28 | 0.069 | 0.52 | 0.724 | 72.9% | 25.5% | 1.6% | ||
| Mean Envelope | 6.793 | −4.296 | 0.123 | 0.51 | 0.732 | 73.2% | 25.5% | 1.3% | ||
| Mean Acceleration | 9.522 | −5.949 | 0.089 | 0.483 | 0.771 | 77.4% | 21.3% | 1.3% | ||
| Postural Tremor | Finger | Peak Power | 2.398 | −2.872 | 0.071 | 0.505 | 0.742 | 73.9% | 25.6% | 0.5% |
| AUC Power | 8.164 | −5.153 | 0.05 | 0.509 | 0.741 | 74.1% | 25.1% | 0.8% | ||
| Mean Envelope | 7.471 | −5.496 | 0.105 | 0.503 | 0.751 | 74.7% | 24.8% | 0.5% | ||
| Mean Acceleration | 11.214 | −8.17 | 0.07 | 0.486 | 0.774 | 77% | 22.4% | 0.5% | ||
| Wrist | Peak Power | 1.346 | −1.492 | 0.119 | 0.592 | 0.688 | 68.9% | 27.9% | 3.2% | |
| AUC Power | 10.157 | −6.048 | 0.05 | 0.585 | 0.697 | 70.5% | 25.5% | 3.9% | ||
| Mean Envelope | 12.235 | −9.358 | 0.077 | 0.575 | 0.714 | 71.3% | 25.5% | 3.2% | ||
| Mean Acceleration | 11.378 | −7.186 | 0.091 | 0.573 | 0.699 | 70.3% | 25.8% | 3.9% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Linden, C.; Berger, T.; Brandt, G.A.; Strelow, J.N.; Jergas, H.; Baldermann, J.C.; Visser-Vandewalle, V.; Fink, G.R.; Barbe, M.T.; Petry-Schmelzer, J.N.; et al. Accelerometric Classification of Resting and Postural Tremor Amplitude. Sensors 2023, 23, 8621. https://doi.org/10.3390/s23208621
van der Linden C, Berger T, Brandt GA, Strelow JN, Jergas H, Baldermann JC, Visser-Vandewalle V, Fink GR, Barbe MT, Petry-Schmelzer JN, et al. Accelerometric Classification of Resting and Postural Tremor Amplitude. Sensors. 2023; 23(20):8621. https://doi.org/10.3390/s23208621
Chicago/Turabian Stylevan der Linden, Christina, Thea Berger, Gregor A. Brandt, Joshua N. Strelow, Hannah Jergas, Juan Carlos Baldermann, Veerle Visser-Vandewalle, Gereon R. Fink, Michael T. Barbe, Jan Niklas Petry-Schmelzer, and et al. 2023. "Accelerometric Classification of Resting and Postural Tremor Amplitude" Sensors 23, no. 20: 8621. https://doi.org/10.3390/s23208621
APA Stylevan der Linden, C., Berger, T., Brandt, G. A., Strelow, J. N., Jergas, H., Baldermann, J. C., Visser-Vandewalle, V., Fink, G. R., Barbe, M. T., Petry-Schmelzer, J. N., & Dembek, T. A. (2023). Accelerometric Classification of Resting and Postural Tremor Amplitude. Sensors, 23(20), 8621. https://doi.org/10.3390/s23208621