
Explainable Convolutional Neural Networks for Brain Cancer Detection and Localisation

 ,
, 
Abstract
:1. Introduction
- Grade I: Pilocytic astrocytoma. These are the least aggressive astrocytomas. They are often referred to as pilocytic astrocytomas and typically have well-defined borders. These are typically slow-growing and have a good prognosis.
- Grade II: Diffuse astrocytoma. These are low-grade astrocytomas. They show some abnormal characteristics in the tumor cells and may have infiltrative growth into nearby tissues. These are low-grade tumors with a moderate potential to become more aggressive over time.
- Grade III: Anaplastic astrocytoma. These are anaplastic astrocytomas. They are considered intermediate-grade tumors with more abnormal cells and more aggressive behavior compared to grade II tumors. These are high-grade tumors that tend to grow more quickly and are more aggressive than Grade II astrocytomas.
- Grade IV: Glioblastoma (also known as glioblastoma multiforme). These are the most malignant and aggressive astrocytomas known as glioblastomas. Glioblastomas are high-grade tumors characterised by highly abnormal and rapidly dividing cells. They are invasive and have a tendency to infiltrate surrounding brain tissue. This is the most aggressive and malignant type of astrocytoma with a poor prognosis.
- Determine the exact type and grade of the brain tumor: A precise diagnosis helps guide treatment decisions and allows healthcare teams to tailor therapies specifically to the patient’s condition.
- Plan the most effective treatment approach: Based on the diagnosis, doctors can develop a comprehensive treatment plan, which may include surgery, radiation therapy, chemotherapy, targeted therapies, or a combination of these approaches.
- Manage symptoms and improve patient comfort: Early diagnosis facilitates the early management of symptoms associated with brain cancer, such as headaches, seizures, cognitive changes, and motor difficulties. This can help improve the patient’s overall well-being and quality of life.
- Monitor disease progression and response to treatment: With an early diagnosis, healthcare professionals can closely monitor the tumor’s progression and assess the response to treatment. This allows for timely adjustments to the treatment plan if needed.
- A method aimed at detecting medical images related to brain cancer, by means of explainabile deep learning, is proposed;
- Four different deep learning networks are exploited, i.e., VGG16, Resnet50, Alex_Net, and MobileNet;
- We provide prediction explainability by considering the Grad-CAM, aimed at localising the area on the medical images responsible for the brain cancer detection, thus providing a valuable tool for radiologists and domain experts;
- A dataset composed of 600 patients is analysed, obtaining an accuracy equal to 99.67%;
- A comparison (in terms of the number of analysed patients, accuracy, the focus of the paper, and localisation) between the proposed method and the state-of-the-art is proposed with the aim of better highlighting the effectiveness of our method.
2. Literature Survey
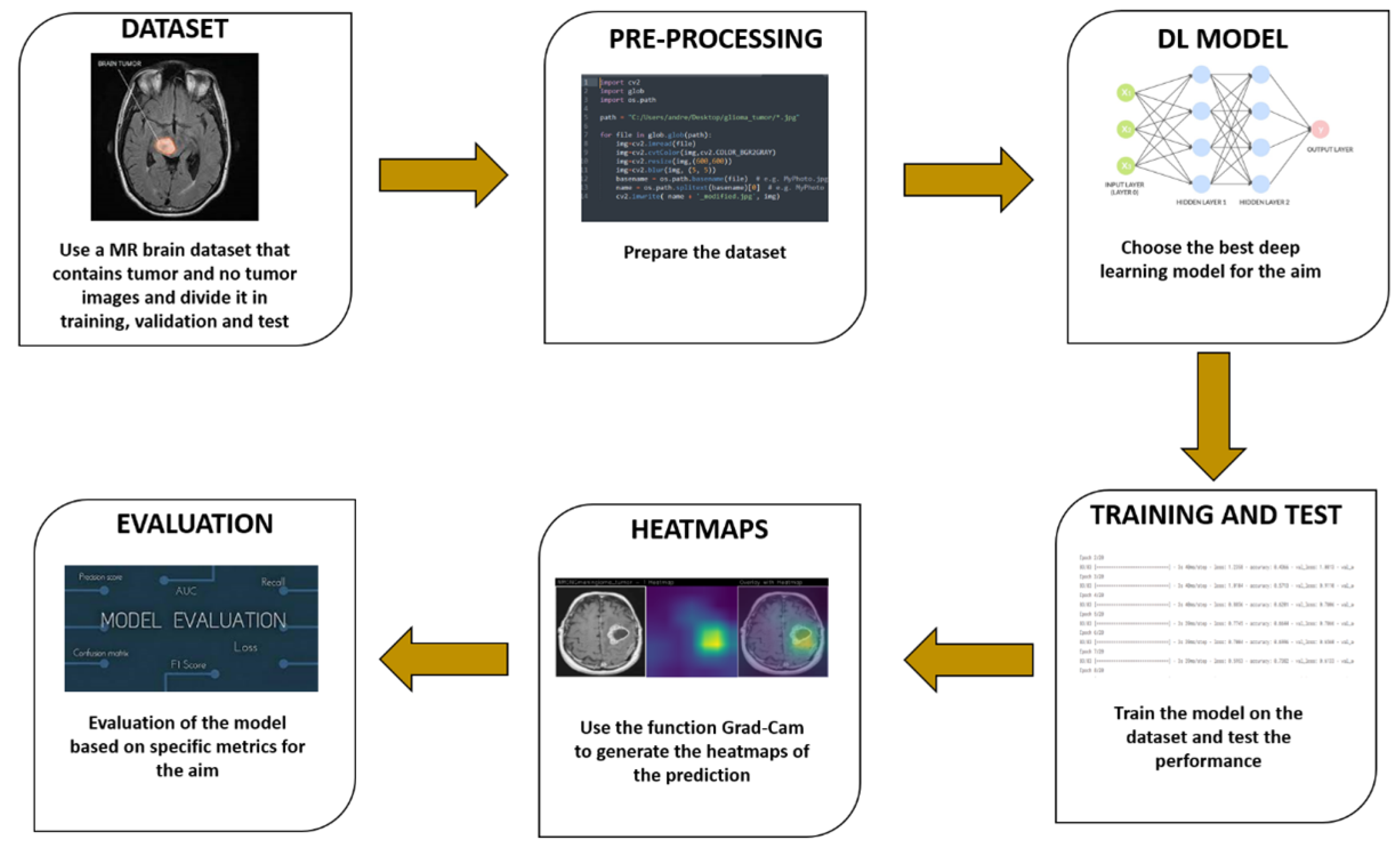
3. The Method
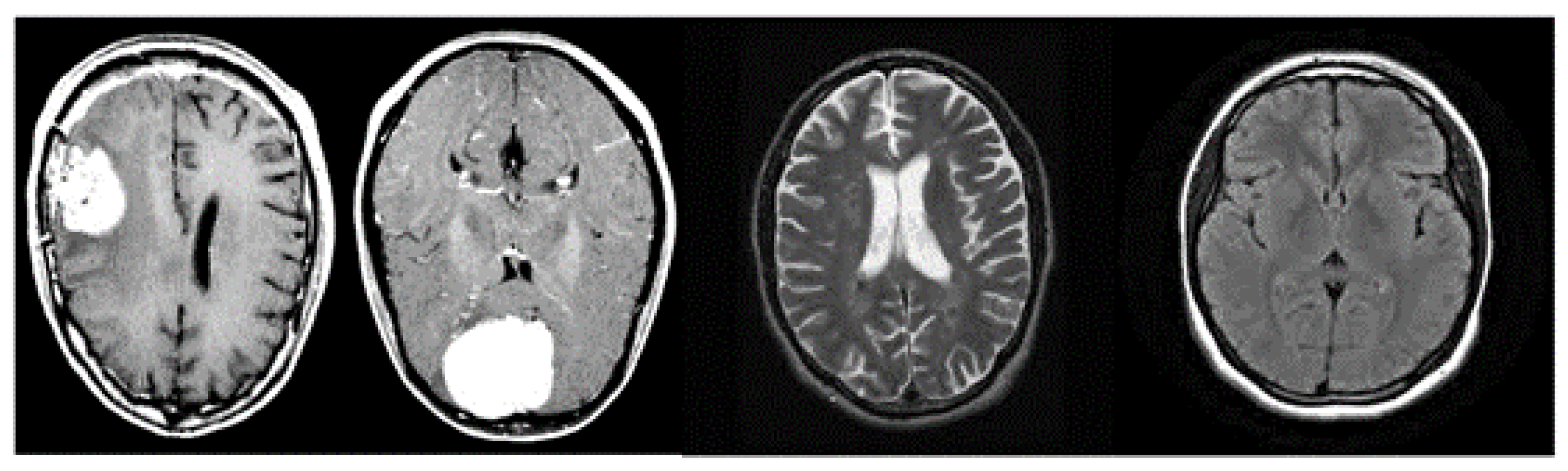
- The dataset used in machine learning methods, including those for brain cancer diagnosis, plays a crucial role in generating an effective model. It is essential to have a carefully labelled dataset that includes both healthy brain images and images of brains affected by cancer. To ensure the robustness and generalisability of the model, it is important to have a diverse and representative dataset. Medical specialists may use different imaging setups or protocols to capture brain images, so it is necessary to include images from various sources and imaging modalities. This variability helps the classifier learn patterns that are applicable across different scenarios, improving its ability to generalise and make accurate predictions on unseen data. By including a wide range of images, encompassing different patients, disease stages, imaging techniques, and variations in data acquisition, the trained model can better capture the complex and diverse nature of brain cancer. This increases the chances of obtaining a classifier that performs well on a variety of real-world scenarios and contributes to its clinical applicability. However, it is important to note that acquiring a diverse and representative dataset can be challenging due to factors such as data availability, privacy concerns, and ethical considerations. In summary, a well-constructed dataset with a good degree of variability is vital for training machine learning models for brain cancer diagnosis. It allows the model to learn from diverse examples and enhances its ability to generalise and make accurate predictions in real-world scenarios.
- Once a dataset is obtained for brain cancer diagnosis, it is necessary to preprocess the images to ensure uniformity and remove any biases introduced by different imaging machines or settings. Preprocessing steps are essential for improving the consistency and quality of the dataset. One common preprocessing technique is to adjust the brightness of the images, particularly during the training phase. Randomly adjusting brightness can help mitigate any variations in image intensity caused by differences in imaging equipment or settings. By applying brightness adjustments, the model can learn to be less sensitive to these variations and focus more on the underlying features and patterns indicative of brain cancer. It is important to note that preprocessing techniques may vary depending on the specific requirements of the dataset and the characteristics of the images. Other preprocessing steps commonly used in medical imaging applications include image resizing, normalisation, noise reduction, and contrast enhancement. These techniques aim to standardise the input data and improve the effectiveness of the machine learning algorithms. The choice of preprocessing techniques should be based on a careful consideration of the dataset characteristics, the specific goals of the study, and domain knowledge from medical experts. It is also crucial to validate the impact of preprocessing steps on the model’s performance and ensure they do not introduce unintended biases or distortions in the data. In summary, the preprocessing of brain cancer images involves various techniques to standardise the dataset and remove the biases introduced by imaging equipment and settings. Randomly adjusting brightness is one such technique that helps improve consistency and reduce sensitivity to variations in image intensity. However, the selection and evaluation of preprocessing techniques should be done with care and consideration of the specific dataset and goals of the study.
- Once the data collection and preprocessing phases are complete, the next step in developing a brain cancer diagnosis model is the selection of deep learning models. The literature offers a wide range of models to choose from, so the objective is to identify the most suitable one. Evaluating the accuracy of predictions is important, but it is also crucial to consider the quality of predictions and provide explainability. Explainability refers to understanding and interpreting the reasoning behind the model’s predictions. This is especially important in medical applications where decisions can have significant implications. Models that offer explainability can help medical professionals and researchers gain insights into the factors influencing the predictions and provide a clearer understanding of the decision-making process. In addition to selecting a suitable model, setting hyperparameters is another important step. Hyperparameters are values that determine the behavior and performance of the model during training. Examples of hyperparameters include the number of epochs (the number of times the model sees the entire dataset during training), batch size (the number of samples processed before updating the model’s parameters), and learning rate (the step size for adjusting the model’s parameters during training).
- Conv2D: This layer performs 2D convolution, such as spatial convolution over images. It generates a convolution kernel applied to the input layer, producing an output tensor.
- MaxPooling2D: This operation conducts maximum pooling on 2D spatial data. It downsamples the input across height and width, retaining the maximum value within each input window defined by the pool_size.
- Flatten: This layer transforms input into a flattened form, commonly transitioning from convolutional to fully connected layers. It does not affect batch size.
- Dropout: By applying Dropout, this layer randomly sets input units to 0 during training with a specified rate. This aids in preventing overfitting. Non-zero inputs are scaled by 1/(1 − rate), keeping their sum consistent.
- Dense: Neurons in this deep layer receive input from all previous layer neurons. It is widely used for classification tasks, involving matrix–vector multiplication with trainable parameters updated through back-propagation.
- (a)
- Interpretability: Grad-CAM provides a transparent and interpretable way to visualise the CNN’s decision-making process. It allows researchers and practitioners to understand which parts of the input image were critical in influencing the network’s classification decision.
- (b)
- No Architecture Modification: One significant advantage of Grad-CAM is that it does not require any changes or modifications to the CNN architecture. It can be applied to pre-trained models without the need for retraining, making it a convenient tool for visualising existing models.
- (c)
- Localisation: Grad-CAM provides localisation information, indicating the exact regions within the input image that the network focused on while making its classification decision. This information is valuable for tasks where understanding what parts of the image contribute to the decision is crucial, such as medical image analysis or object detection.
- (d)
- High-Level Visual Patterns: By using gradients from the final convolutional layers, Grad-CAM can capture high-level visual patterns in the input image. This makes it particularly useful for tasks that require understanding complex visual cues.
- (e)
- Preservation of Spatial Information: Grad-CAM retains spatial information from the original input image, ensuring that the visualised heatmap aligns accurately with the relevant regions in the image.
- (f)
- Applicability to Different Tasks: Grad-CAM is a versatile technique that can be applied to various CNN-based tasks, including image classification, object detection, and image segmentation. Its adaptability makes it a widely applicable tool in computer vision research.
- (g)
- Model Debugging: When a CNN produces unexpected or erroneous results, Grad-CAM can be used as a debugging tool to visualise where the model focused its attention. This can help identify potential weaknesses or biases in the network’s decision-making process.
- (h)
- Explainable AI: In contexts where explainability and transparency are essential, Grad-CAM can provide insights into how a CNN arrives at its predictions, increasing user trust and confidence in the model’s outputs.
- 4.
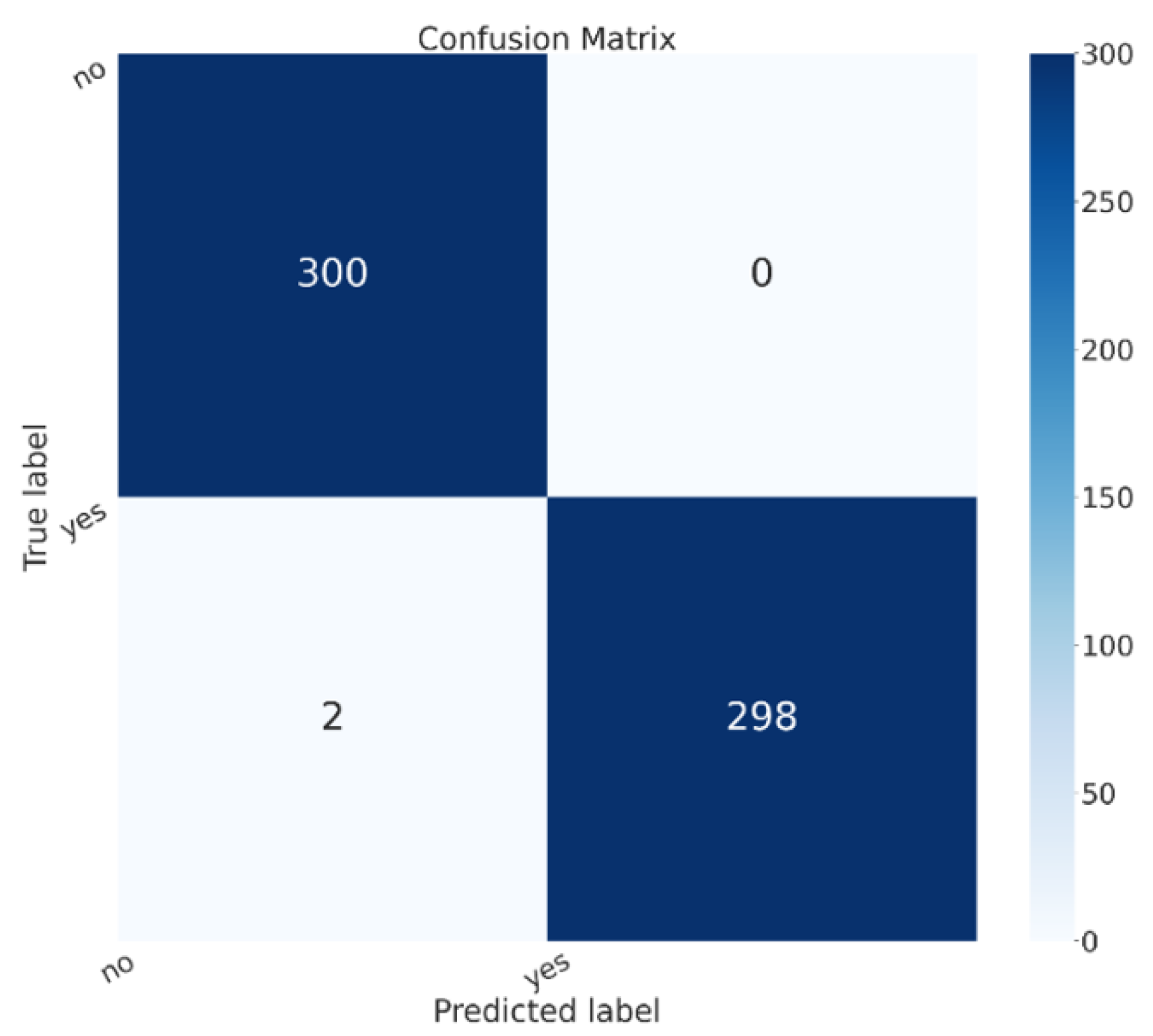
- The last step is the evaluation one, where we collect the metrics (i.e., Accuracy, Precision, and Recall) obtained from the testing of the employed models. Moreover, we consider the confusion matrix with the aim to understand the exact number of misclassifications per class.
4. Experimental Analysis
5. Conclusions and Future Work
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Mercaldo, F.; Santone, A. Transfer learning for mobile real-time face mask detection and localization. J. Am. Med. Inform. Assoc. 2021, 28, 1548–1554. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Martinelli, F.; Mercaldo, F.; Santone, A. Deep learning for heart disease detection through cardiac sounds. Procedia Comput. Sci. 2020, 176, 2202–2211. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Neural networks for lung cancer detection through radiomic features. In Proceedings of the 2019 International Joint Conference on Neural Networks (IJCNN), Budapest, Hungary, 14–19 July 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–10. [Google Scholar]
- Cimitile, A.; Martinelli, F.; Mercaldo, F. Machine Learning Meets iOS Malware: Identifying Malicious Applications on Apple Environment. In Proceedings of the ICISSP, Porto, Portugal, 19–21 February 2017; pp. 487–492. [Google Scholar]
- Mercaldo, F.; Nardone, V.; Santone, A. Diabetes Mellitus Affected Patients Classification and Diagnosis through Machine Learning Techniques. Procedia Comput. Sci. 2017, 112, 2519–2528. [Google Scholar] [CrossRef]
- Mercaldo, F.; Visaggio, C.A.; Canfora, G.; Cimitile, A. Mobile malware detection in the real world. In Proceedings of the IEEE/ACM International Conference on Software Engineering Companion (ICSE-C), Austin, TX, USA, 14–22 May 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 744–746. [Google Scholar]
- Bernardi, M.L.; Cimitile, M.; Martinelli, F.; Mercaldo, F. A time series classification approach to game bot detection. In Proceedings of the 7th International Conference on Web Intelligence, Mining and Semantics, Amantea, Italy, 19–22 June 2017; pp. 1–11. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Ramteke, R.; Monali, Y.K. Automatic medical image classification and abnormality detection using K-Nearest Neighbour. Int. J. Adv. Comput. Res. 2012, 2, 190–196. [Google Scholar]
- Isselmou, A.E.K.; Zhang, S.; Xu, G. A novel approach for brain tumor detection using MRI images. J. Biomed. Sci. Eng. 2016, 9, 44. [Google Scholar] [CrossRef]
- Sharma, K.; Kaur, A.; Gujral, S. Brain tumor detection based on machine learning algorithms. Int. J. Comput. Appl. 2014, 103, 7–11. [Google Scholar] [CrossRef]
- Babu, B.S.; Varadarajan, S. Detection of Brain Tumour in MRI Scanned Images using DWT and SVM. Int. J. Eng. Technol. 2017, 9, 2528–2533. [Google Scholar]
- Gadpayleand, P.; Mahajani, P. Detection and classification of brain tumor in MRI images. Int. J. Emerg. Trends Electr. Electron. 2013, 5, 2320–9569. [Google Scholar]
- Jafari, M.; Shafaghi, R. A hybrid approach for automatic tumor detection of brain MRI using support vector machine and genetic algorithm. Glob. J. Sci. Eng. Technol. 2012, 3, 1–8. [Google Scholar]
- Chaddad, A. Automated feature extraction in brain tumor by magnetic resonance imaging using gaussian mixture models. J. Biomed. Imaging 2015, 2015, 868031. [Google Scholar] [CrossRef]
- Kharrat, A.; Halima, M.B.; Ayed, M.B. MRI brain tumor classification using support vector machines and meta-heuristic method. In Proceedings of the 2015 15th International Conference on Intelligent Systems Design and Applications (ISDA), Marrakech, Morocco, 14–16 December 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 446–451. [Google Scholar]
- Ghosh, D.; Bandyopadhyay, S.K. Brain tumor detection from MRI image: An approach. IJAR 2017, 3, 1152–1159. [Google Scholar]
- Zahran, B.M. Classification of brain tumor using neural network. Comput. Softw. 2014, 673. [Google Scholar] [CrossRef]
- Khawaldeh, S.; Pervaiz, U.; Rafiq, A.; Alkhawaldeh, R. Noninvasive grading of glioma tumor using magnetic resonance imaging with convolutional neural networks. Appl. Sci. 2017, 8, 27. [Google Scholar] [CrossRef]
- Zacharaki, E.I.; Wang, S.; Chawla, S.; Soo Yoo, D.; Wolf, R.; Melhem, E.R.; Davatzikos, C. Classification of brain tumor type and grade using MRI texture and shape in a machine learning scheme. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2009, 62, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- El-Dahshan, E.S.A.; Mohsen, H.M.; Revett, K.; Salem, A.B.M. Computer-aided diagnosis of human brain tumor through MRI: A survey and a new algorithm. Expert Syst. Appl. 2014, 41, 5526–5545. [Google Scholar] [CrossRef]
- Iftekharuddin, K.M.; Zheng, J.; Islam, M.A.; Ogg, R.J. Fractal-based brain tumor detection in multimodal MRI. Appl. Math. Comput. 2009, 207, 23–41. [Google Scholar] [CrossRef]
- El-Dahshan, E.S.A.; Hosny, T.; Salem, A.B.M. Hybrid intelligent techniques for MRI brain images classification. Digit. Signal Process. 2010, 20, 433–441. [Google Scholar] [CrossRef]
- Gurusamy, R.; Subramaniam, V. A machine learning approach for MRI brain tumor classification. Comput. Mater. Contin. 2017, 53, 91–108. [Google Scholar]
- Rathi, V.; Palani, S. Brain tumor MRI image classification with feature selection and extraction using linear discriminant analysis. arXiv 2012, arXiv:1208.2128. [Google Scholar]
- Vani, N.; Sowmya, A.; Jayamma, N. Brain Tumor Classification using Support Vector Machine. Int. Res. J. Eng. Technol. (IRJET) 2017, 4, 792–796. [Google Scholar]
- Georgiadis, P.; Cavouras, D.; Kalatzis, I.; Daskalakis, A.; Kagadis, G.C.; Sifaki, K.; Malamas, M.; Nikiforidis, G.; Solomou, E. Improving brain tumor characterization on MRI by probabilistic neural networks and non-linear transformation of textural features. Comput. Methods Programs Biomed. 2008, 89, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, S.; Sun, P.; Phillips, P. Pathological brain detection based on wavelet entropy and Hu moment invariants. Bio-Med. Mater. Eng. 2015, 26, S1283–S1290. [Google Scholar] [CrossRef] [PubMed]
- Abidin, A.Z.; Dar, I.; D’Souza, A.M.; Lin, E.P.; Wismüller, A. Investigating a quantitative radiomics approach for brain tumor classification. In Proceedings of the Medical Imaging 2019: Biomedical Applications in Molecular, Structural, and Functional Imaging, San Diego, CA, USA, 19–21 February 2019; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 10953, p. 109530B. [Google Scholar]
- Papageorgiou, E.; Spyridonos, P.; Glotsos, D.T.; Stylios, C.D.; Ravazoula, P.; Nikiforidis, G.; Groumpos, P.P. Brain tumor characterization using the soft computing technique of fuzzy cognitive maps. Appl. Soft Comput. 2008, 8, 820–828. [Google Scholar] [CrossRef]
- Sajjad, M.; Khan, S.; Muhammad, K.; Wu, W.; Ullah, A.; Baik, S.W. Multi-grade brain tumor classification using deep CNN with extensive data augmentation. J. Comput. Sci. 2019, 30, 174–182. [Google Scholar] [CrossRef]
- Kharrat, A.; Gasmi, K.; Messaoud, M.B.; Benamrane, N.; Abid, M. A hybrid approach for automatic classification of brain MRI using genetic algorithm and support vector machine. Leonardo J. Sci. 2010, 17, 71–82. [Google Scholar]
- Barker, J.; Hoogi, A.; Depeursinge, A.; Rubin, D.L. Automated classification of brain tumor type in whole-slide digital pathology images using local representative tiles. Med. Image Anal. 2016, 30, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.L.C.; Lo, C.M.; Hsiao, C.J. Computer-aided grading of gliomas based on local and global MRI features. Comput. Methods Programs Biomed. 2017, 139, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.H.; Mousavi, H.S.; Monga, V.; Rao, G.; Rao, U.A. Histopathological image classification using discriminative feature-oriented dictionary learning. IEEE Trans. Med. Imaging 2015, 35, 738–751. [Google Scholar] [CrossRef]
- David, D.S. Parasagittal Meningioma Brain Tumor Classification System Based on Mri Images and Multi Phase Level Set Formulation. Biomed. Pharmacol. J. 2019, 12, 939–946. [Google Scholar] [CrossRef]
- Qurat-Ul-Ain, G.L.; Kazmi, S.B.; Jaffar, M.A.; Mirza, A.M. Classification and segmentation of brain tumor using texture analysis. In Proceedings of the WSEAS International Conference on Artificial Intelligence, Knowledge Engineering and Data Bases (AIKED’10), Cambridge, UK, 20–22 February 2010; pp. 147–155. [Google Scholar]
- Cui, G.; Jeong, J.J.; Lei, Y.; Wang, T.; Liu, T.; Curran, W.J.; Mao, H.; Yang, X. Machine-learning-based classification of Glioblastoma using MRI-based radiomic features. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis, San Diego, CA, USA, 17–20 February 2019; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 10950, p. 1095048. [Google Scholar]
- Amin, S.E.; Mageed, M. Brain tumor diagnosis systems based on artificial neural networks and segmentation using MRI. In Proceedings of the IEEE International Conference on Wireless Information Technology and Systems, Maui, HI, USA, 11–16 November 2012; pp. 15–25. [Google Scholar]
- Badran, E.F.; Mahmoud, E.G.; Hamdy, N. An algorithm for detecting brain tumors in MRI images. In Proceedings of the 2010 International Conference on Computer Engineering & Systems (ICCES), Cairo, Egypt, 30 November–2 December 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 368–373. [Google Scholar]
- Xuan, X.; Liao, Q. Statistical structure analysis in MRI brain tumor segmentation. In Proceedings of the ICIG 2007 Fourth International Conference on Image and Graphics, Chengdu, China, 22–24 August 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 421–426. [Google Scholar]
- Ibrahim, W.H.; Osman, A.A.A.; Mohamed, Y.I. MRI brain image classification using neural networks. In Proceedings of the 2013 International Conference on Computing, Electrical and Electronics Engineering (ICCEEE), Khartoum, Sudan, 26–28 August 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 253–258. [Google Scholar]
- Mohsen, H.; El-Dahshan, E.S.A.; El-Horbaty, E.S.M.; Salem, A.B.M. Classification using deep learning neural networks for brain tumors. Future Comput. Inform. J. 2018, 3, 68–71. [Google Scholar] [CrossRef]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain tumor type classification via capsule networks. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 3129–3133. [Google Scholar]
- Zia, R.; Akhtar, P.; Aziz, A. A new rectangular window based image cropping method for generalization of brain neoplasm classification systems. Int. J. Imaging Syst. Technol. 2018, 28, 153–162. [Google Scholar] [CrossRef]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Wang, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. An ensemble learning approach for brain cancer detection exploiting radiomic features. Comput. Methods Programs Biomed. 2020, 185, 105134. [Google Scholar] [CrossRef] [PubMed]
- Ballester, P.; Araujo, R.M. On the performance of GoogLeNet and AlexNet applied to sketches. In Proceedings of the Thirtieth AAAI Conference on Artificial Intelligence, Phoenix, AZ, USA, 12–17 February 2016. [Google Scholar]
- Mascarenhas, S.; Agarwal, M. A comparison between VGG16, VGG19 and ResNet50 architecture frameworks for Image Classification. In Proceedings of the 2021 International Conference on Disruptive Technologies for Multi-Disciplinary Research and Applications (CENTCON), Bengaluru, India, 19–21 November 2021; IEEE: Piscataway, NJ, USA, 2021; Volume 1, pp. 96–99. [Google Scholar]
- Nan, Y.; Ju, J.; Hua, Q.; Zhang, H.; Wang, B. A-MobileNet: An approach of facial expression recognition. Alex. Eng. J. 2022, 61, 4435–4444. [Google Scholar] [CrossRef]
- Mukti, I.Z.; Biswas, D. Transfer learning based plant diseases detection using ResNet50. In Proceedings of the 2019 4th International Conference on Electrical Information and Communication Technology (EICT), Khulna, Bangladesh, 20–22 December 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–6. [Google Scholar]
- Cimitile, A.; Martinelli, F.; Mercaldo, F.; Nardone, V.; Santone, A.; Vaglini, G. Model checking for mobile android malware evolution. In Proceedings of the 2017 IEEE/ACM 5th International FME Workshop on Formal Methods in Software Engineering (FormaliSE), Buenos Aires, Argentina, 20–28 May 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 24–30. [Google Scholar]
- Martinelli, F.; Mercaldo, F.; Nardone, V.; Santone, A.; Sangaiah, A.K.; Cimitile, A. Evaluating model checking for cyber threats code obfuscation identification. J. Parallel Distrib. Comput. 2018, 119, 203–218. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Patients | Accuracy | Focus | Localisation |
|---|---|---|---|---|
| [10] | n.a. | 0.95 | benign/malign | ✗ |
| [11] | 121 | 0.91 | benign/malign | ✗ |
| [9] | 51 | 0.80 | benign/malign | ✗ |
| [12] | 130 | 0.98 | benign/malign | ✗ |
| [13] | 20 | 0.72 | benign/malign | ✗ |
| [14] | n.a. | 0.83 | benign/malign | ✗ |
| [15] | 17 | 0.97 | benign/malign | ✗ |
| [16] | 83 | 0.95 | benign/malign | ✗ |
| [17] | 45 | 0.89 | benign/malign | ✗ |
| [18] | 57 | 0.83 | benign/malign | ✗ |
| [19] | 130 | 0.91 | L/H | ✗ |
| [20] | 102 | 0.80 | L/H | ✗ |
| [21] | 101 | 0.99 | benign/malign | ✗ |
| [22] | 9 | 0.90 | benign/malign | ✗ |
| [23] | 70 | 0.98 | benign/malign | ✗ |
| [24] | n.a. | 0.97 | benign/malign | ✗ |
| [25] | 20 | 0.98 | benign/malign | ✗ |
| [26] | 130 | 0.82 | L/H | ✗ |
| [27] | 67 | 0.81 | L/H | ✗ |
| [28] | n.a. | 1 | benign/malign | ✗ |
| [29] | 52 | 0.71 | L/H | ✗ |
| [30] | 100 | 0.92 | L/H | ✗ |
| [33] | 302 | 0.93 | L/H | ✗ |
| [34] | 107 | 0.88 | L/H | ✗ |
| [35] | 190 | 0.94 | L/H | ✗ |
| [36] | 50 | 0.87 | L/H | ✗ |
| [37] | n.a. | 0.99 | benign/malign | ✗ |
| [38] | 50 | 0.92 | benign/malign | ✗ |
| [39] | 30 | 0.78 | L/H | ✗ |
| [40] | n.a. | 0.85 | benign/malign | ✗ |
| [41] | 140 | 0.96 | benign/malign | ✗ |
| [42] | n.a. | 0.96 | benign/malign | ✗ |
| [43] | 66 | 0.97 | benign/malign | ✗ |
| Our method | 3000 | 0.99 | benign/malign | ✓ |
| Metric | VGG16 | Resnet50 | Alex_Net | MobileNet |
|---|---|---|---|---|
| Accuracy | 97.83% | 99.67% | 99.33% | 98.5% |
| Precision | 97.83% | 99.67% | 99.33% | 98.5% |
| Recall | 97.83% | 99.67% | 99.33% | 98.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercaldo, F.; Brunese, L.; Martinelli, F.; Santone, A.; Cesarelli, M. Explainable Convolutional Neural Networks for Brain Cancer Detection and Localisation. Sensors 2023, 23, 7614. https://doi.org/10.3390/s23177614
Mercaldo F, Brunese L, Martinelli F, Santone A, Cesarelli M. Explainable Convolutional Neural Networks for Brain Cancer Detection and Localisation. Sensors. 2023; 23(17):7614. https://doi.org/10.3390/s23177614
Chicago/Turabian StyleMercaldo, Francesco, Luca Brunese, Fabio Martinelli, Antonella Santone, and Mario Cesarelli. 2023. "Explainable Convolutional Neural Networks for Brain Cancer Detection and Localisation" Sensors 23, no. 17: 7614. https://doi.org/10.3390/s23177614
APA StyleMercaldo, F., Brunese, L., Martinelli, F., Santone, A., & Cesarelli, M. (2023). Explainable Convolutional Neural Networks for Brain Cancer Detection and Localisation. Sensors, 23(17), 7614. https://doi.org/10.3390/s23177614