3.1. Evaluation Results Based on Personal Features
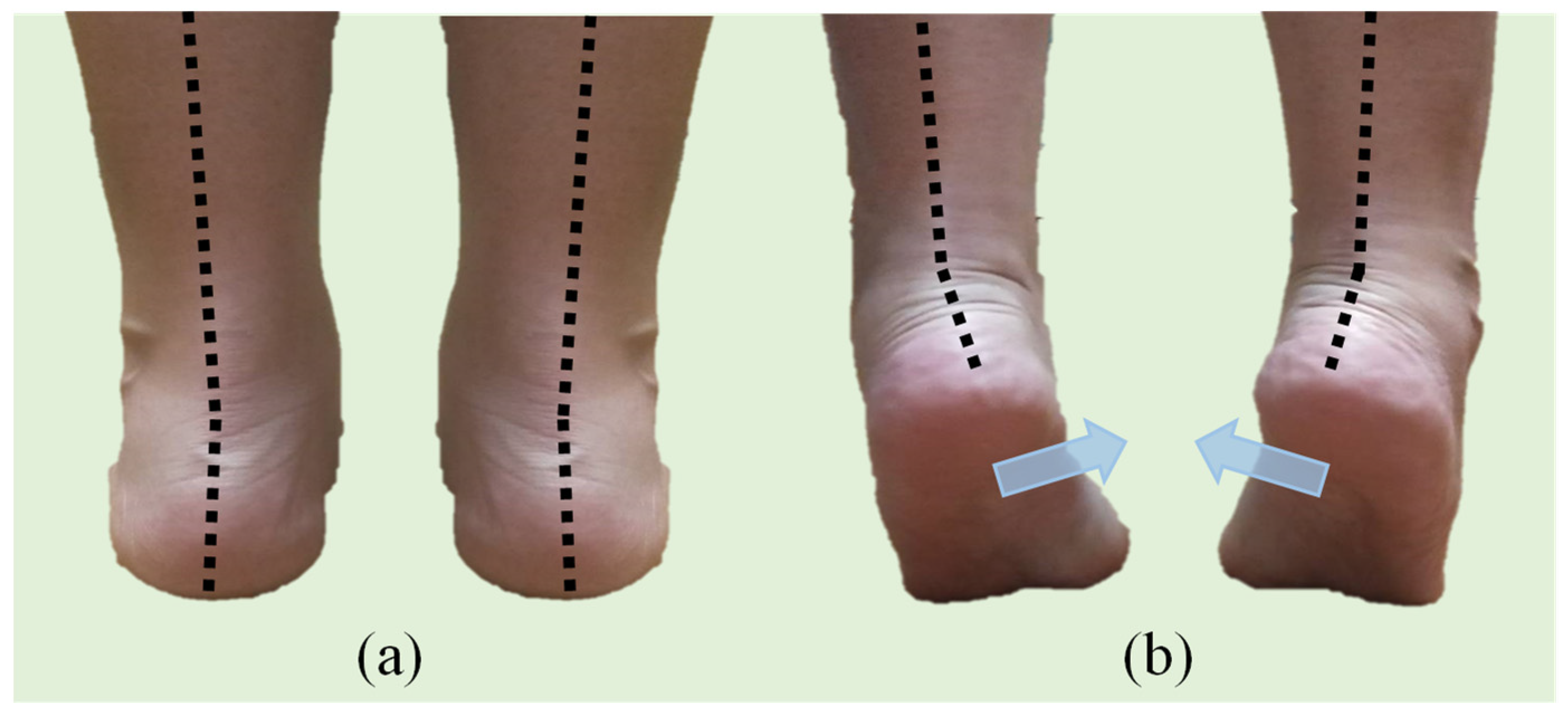
Table 1 lists the summary statistics for the personal features. The participants’ average age, height, and weight were 21 years, 160 cm, and 52 kg, respectively. The basic characteristics for the left and the right feet were similar. The average foot length, forefoot width, foot height, and foot step were 24, 9.4, 5, and 22 cm, respectively. The average most convex point of the navicular bone (MCP-NB) and arch rate were 3 cm and 12.56%. The average HVA and QVA were roughly 12° and 10°, respectively, and those for the left foot were slightly larger than those for the right foot. The average rearfoot width was 6.3 cm. The average angles of the rearfoot for the left and the right foot differed slightly, being 0.89° and 0.80°, respectively. Because this study only included healthy female participants, the variation in the CVA of the rearfoot was small. This variable was categorized into three groups according to the CVA of the rearfoot: 0°, 1°, and >1°. By using 0° as the reference group, two dummy variables CVA1 and CVA2 were created for establishing the model.
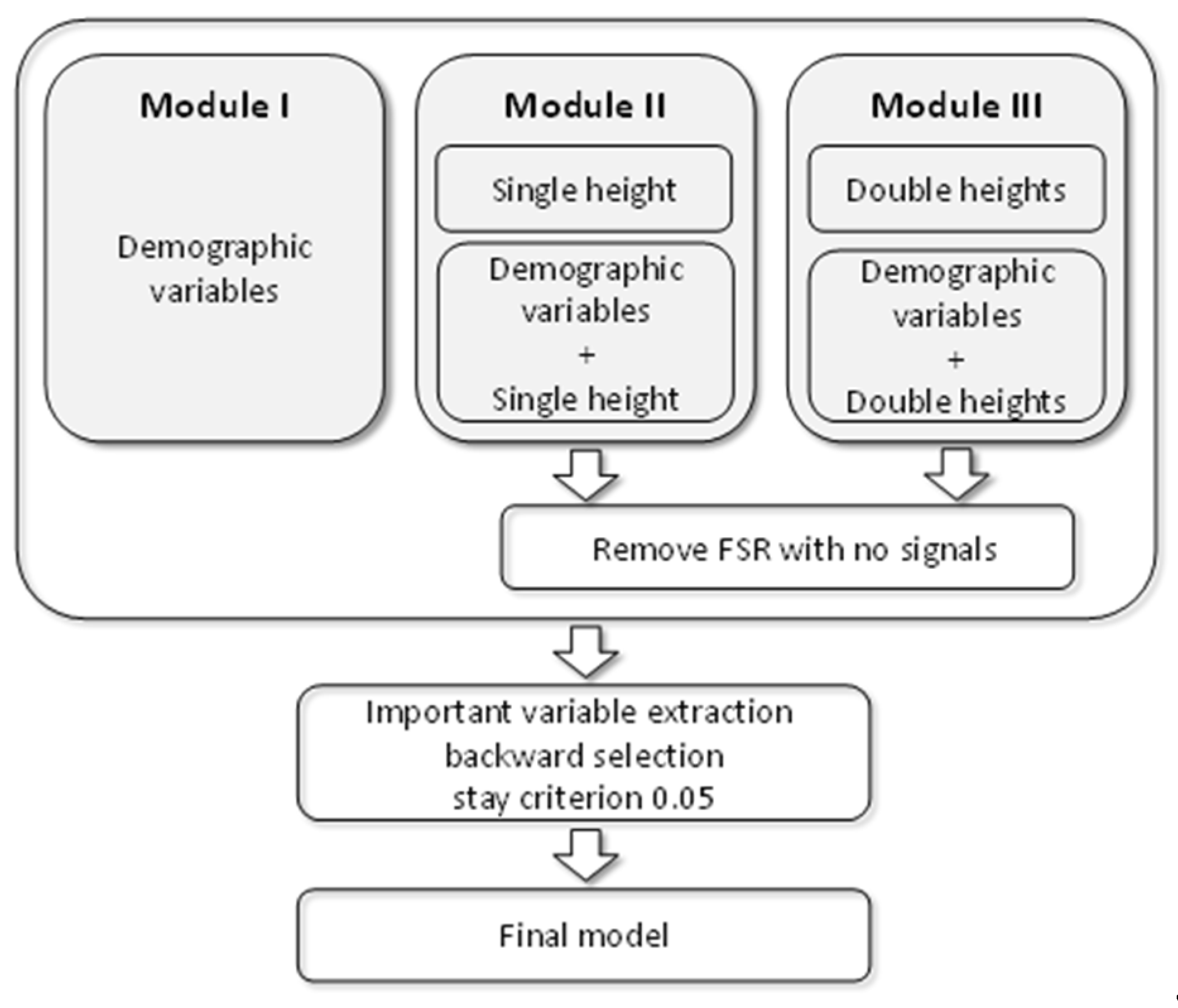
Module I used all personal features to build the model shown in
Table 2. By using 0.05 as the selection for a staying criterion, three features—height, weight, and MCP-NB—for both feet were found to be significant. Both height and MCP-NB were positively associated with DHH, and weight was negatively associated. For the right foot, MCP-NB was the most significant predictor for the DHH, followed by the height. By contrast, for the left foot, height was the most significant predictor, followed by MCP-NB. These variables explained approximately 17% and 14% of the variation for the right and left foot, respectively.
3.2. Evaluation Results Based on FSR Sensors from One Height
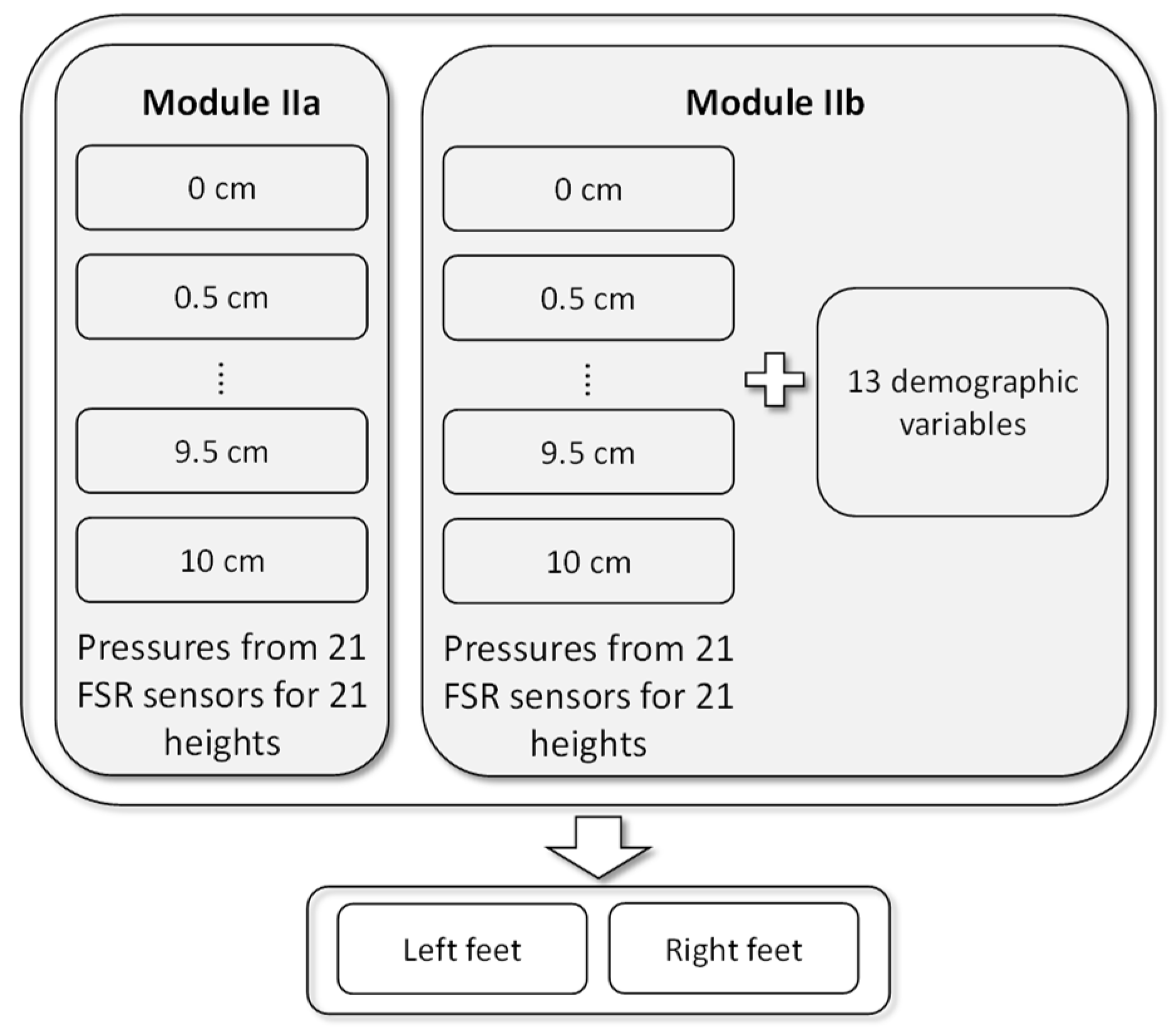
Module II used the plantar pressure data collected from FSR sensors for 21 heights to predict the DHH. A total of 21 models were generated for each foot. When 0.05 was the selection for a staying criterion,
Figure 8a shows the percentage of the variation explained by Module IIa based on the plantar pressure data, where
● and ○, respectively, denote the right and left foot and the number indicates the height for the two highest predictive powers. For the right foot, the plantar pressure data measured at all heights had some ability to predict DHH. In particular, the plantar pressure data measured at 0.5 cm provided the highest
R2. For the left foot, only the plantar pressure data measured at heights of 0, 5.5, 7, 8, 9, 9.5, and 10 cm had some ability to predict DHH. The plantar pressure data measured at heights 8 and 10 offered more information to predict DHH.
For the right foot, all models had some predictive power. The highest predictive power for the model using data measured at a height of 0.5 cm was 17%. As shown in
Table 3, FSR31, FSR39, and FSR49 were chosen when data measured at this height were used. FSR31 was negatively associated with DHH, whereas the other two sensors were positively associated. For the left foot, the highest predictive power for the model using data measured at heights of 8 and 10 cm was 11%.
Table 3 shows the model when using data measured at 10 cm; the model when using data measured at 8 cm is not shown. FSR08 and FSR17 were significantly and negatively associated with DHH.
Figure 8b shows the percentage of variation explained by Module IIb based on the plantar pressure data and the personal features, where
● and ○, respectively, denote the right and left foot and the number indicates the height for the two highest predictive powers. The predictive power increased gradually. For the right foot, the highest predictive powers for the model using data measured at 3.5 and 9.5 cm were 34% and 32%, respectively. By contrast, for the left foot, the highest predictive powers for the model using data measured at 7.5 and 10 cm were 26% and 28%, respectively.
Table 4 shows the significant predictors for the model using data measured at 3.5 cm for the right foot. Four FSR sensors—FSR34, FSR39, FSR48, and FSR50—were significantly and positively associated with DHH and FSR33 was negatively associated. The personal features including height, weight, MCP-NB, CVA1, CVA2, and forefoot width were found to be significantly associated with DHH, and of these, only weight was negatively associated. For the model using data measured at 3.5 cm, the most significant predictors were weight, FSR34, and height.
Table 4 shows the model estimates obtained using measurements at 10 cm for the left foot. FSR08 and FSR17 were significantly and negatively associated with DHH. Personal features including height, weight, MCP-NB, CVA1, and CVA2 were also significantly associated with DHH, whereas only weight was negatively associated.
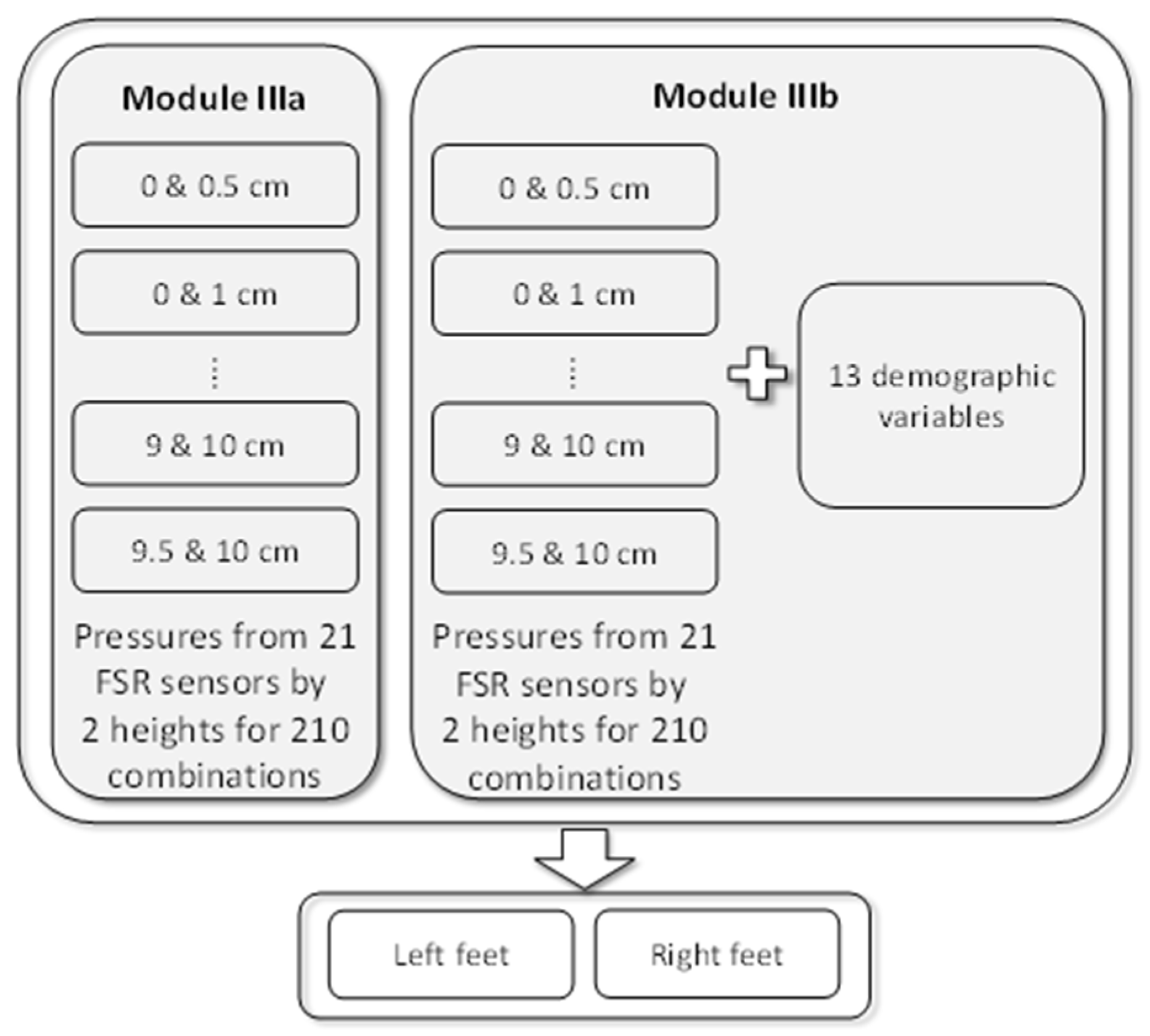
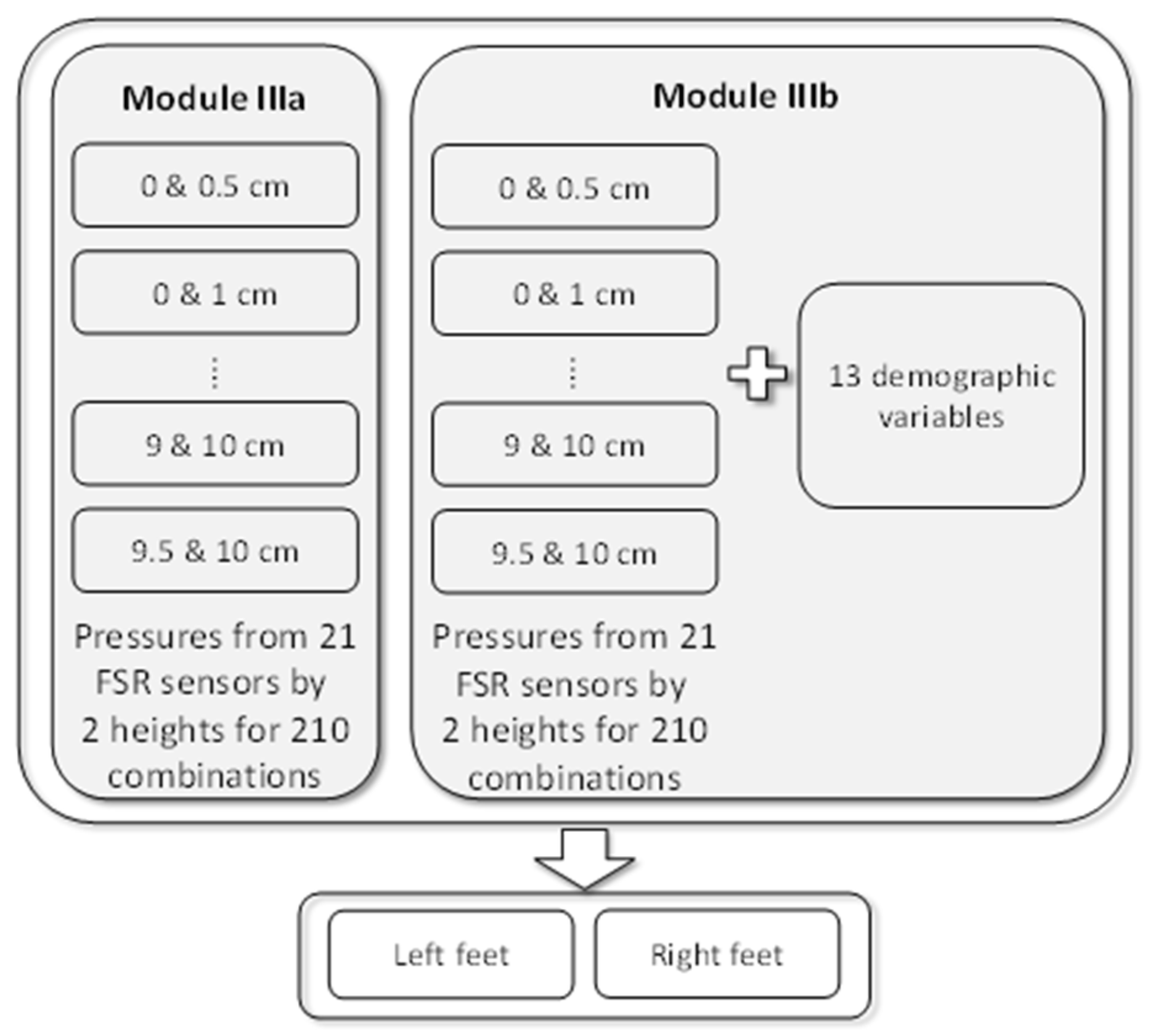
3.3. Evaluation Results Based on FSR Sensors from Two Heights
Module III was established using sensor data collected from two heights. Selecting two heights from among 21 heights resulted in 210 possible combinations, and thus, 210 models were established for each foot.
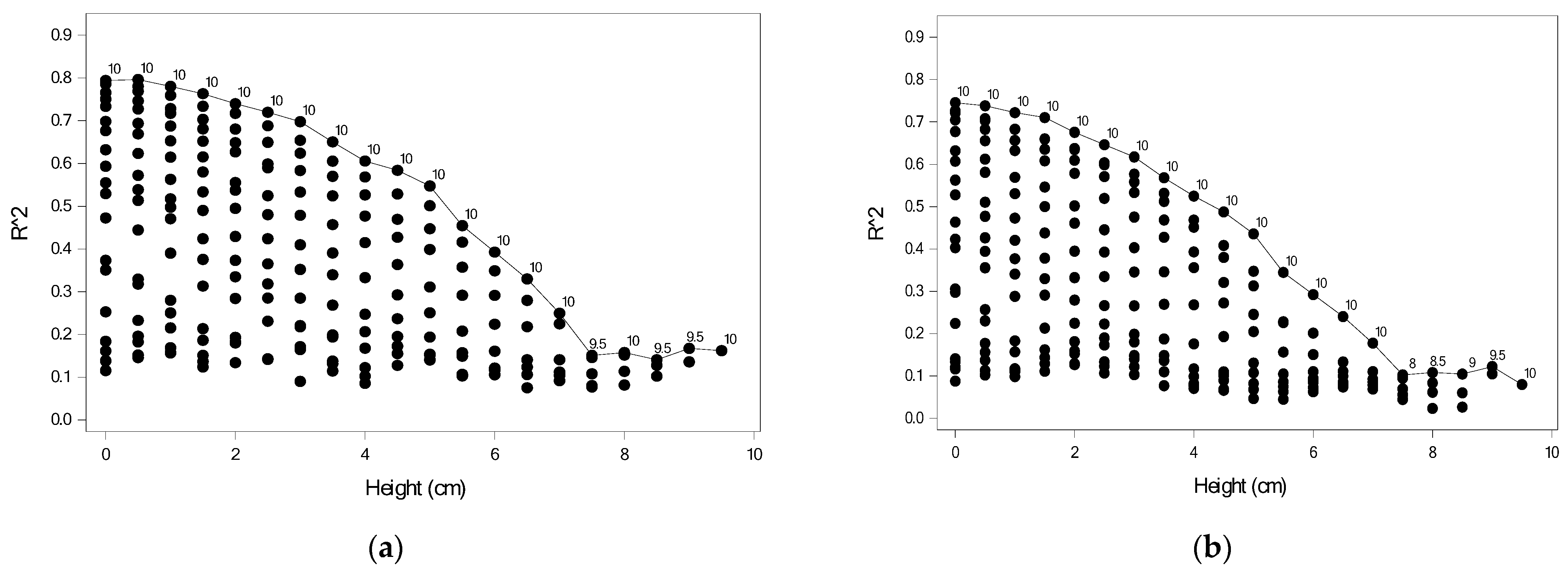
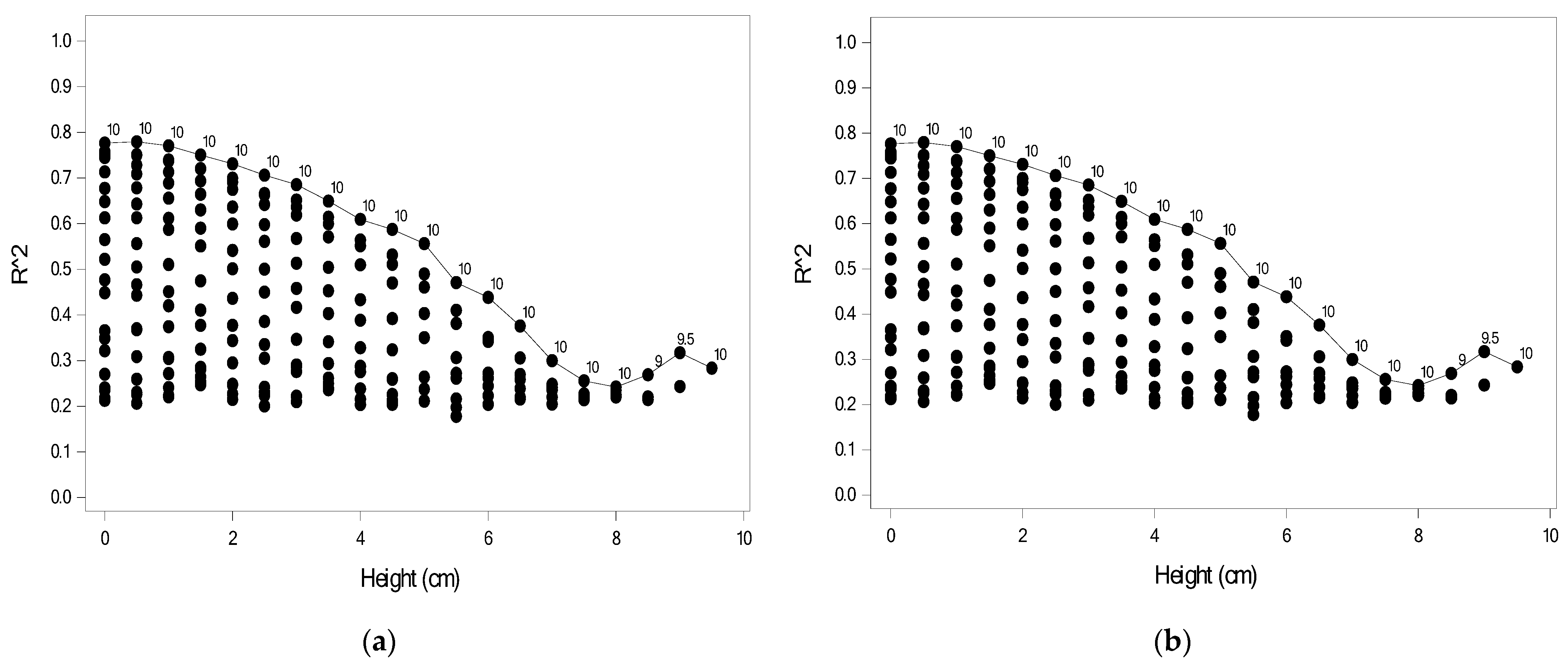
Figure 9 shows the predictive power of Module IIIa for the 210 models for the right and left feet, where each point indicates
R2 for one combination. For a given height, the number indicates the second height for the highest
R2. When using data collected from two extreme heights, the model would yield the highest predictive power. For example, for the right foot as shown in
Figure 9a, the models using data measured at 0.5 and 10 cm had the highest predictive power (
R2 = 0.806), followed by the model using data measured at 0 and 10 cm (
R2 = 0.796).
Figure 9b displayed the result for the left foot and the models using data measured at 0 and 10 cm had the highest predictive power (
R2 = 0.746), followed by the model using data measured at 0.5 and 10 cm (
R2 = 0.738).
Table 5 shows the model estimates for the model with the highest predictive power for the right foot. Nine FSR sensors were significantly associated with DHH; specifically, FSR32, FSR34, FSR35, FSR36, and FSR50 were negatively associated, whereas FSR39, FSR 44, FSR47, and FSR51 were positively associated.
Table 5 also shows the model estimates for the model with the highest predictive power for the left foot. Eight FSR sensors were significantly associated with DHH; specifically, FSR04, FSR05, FSR06, and FSR20 were negatively associated, whereas FSR08, FSR11, FSR13, and FSR17 were positively associated.
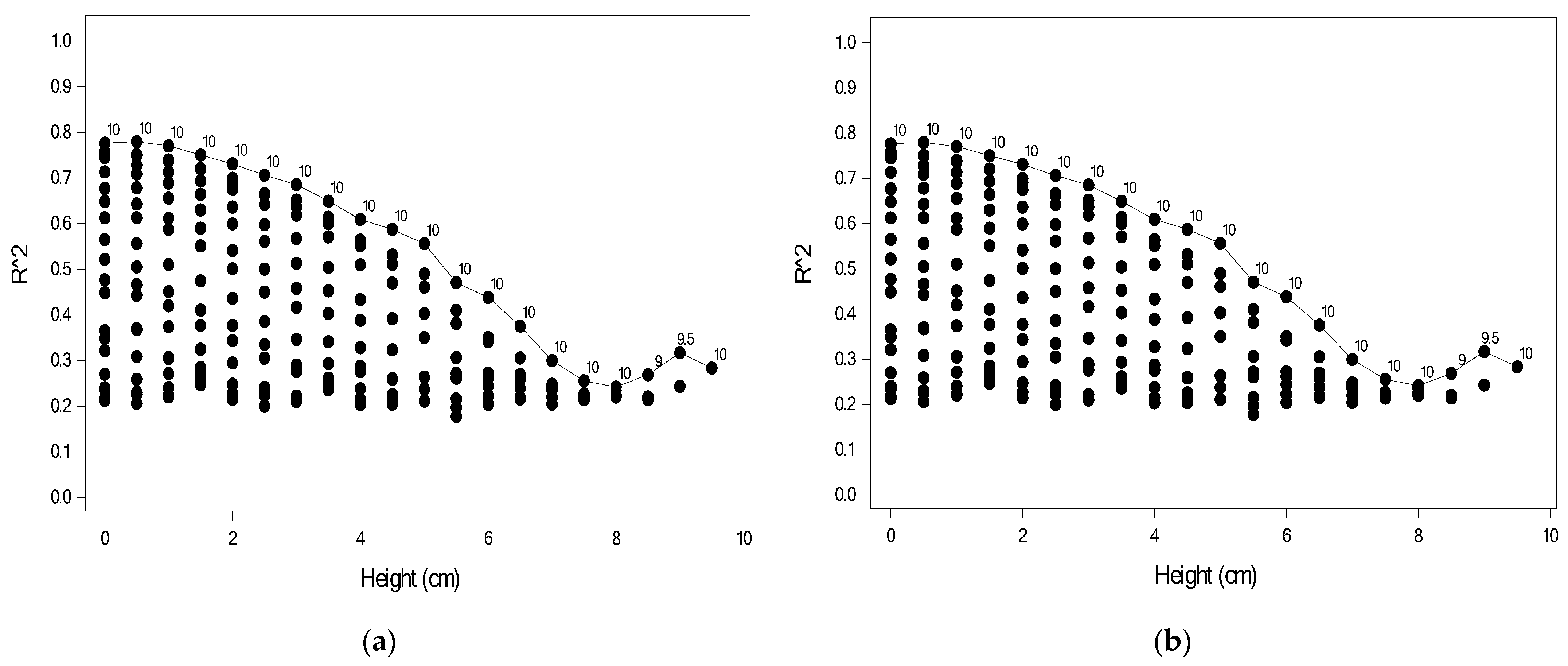
In addition to the FSR sensor data, 210 models including the personal features for each foot were built.
Figure 10 shows the predictive power of Module IIIb for 210 models for the right and left foot, where each point indicates
R2 for one combination. When the personal features were added, the predictive power increased. The model with the highest predictive power was derived from the sensor data measured at two extreme heights, as shown in
Figure 10. For the right foot, the models using data measured at 0.5 and 10 cm had the highest predictive power (
R2 = 0.820), followed by the model using data measured at 0 and 10 cm (
R2 = 0.817). For the left foot, the models using data measured at 0.5 and 10 cm had the highest predictive power (
R2 = 0.779), followed by the model using data measured at 0 and 10 cm (
R2 = 0.777). The predictive power with the combination of 0 and 10 cm was similar to that with the combination of 0.5 and 10 cm. However, the combination of 0 and 10 cm avoids the need for raising the measurement platform one time, making it more convenient in practice.
Table 6 shows the estimates for the model using data measured at heights of 0.5 and 10 cm for the right foot. FSR32, FSR33, FSR34, FSR35, FSR36, and FSR50 were negatively associated with DHH, whereas FSR39, FSR40, FSR44, FSR47, and FSR51were positively associated. Furthermore, MCP-NB and HVA were positively associated with DHH. The fitted model for the right foot was given as (2).
Table 6 also shows the model estimates for the model using data measured at heights of 0 and 10 cm for the left foot. FSR02, FSR04, FSR05, FSR06, and FSR20 were negatively associated with DHH, whereas FSR11, FSR13, and FSR17 were positively associated. Additionally, height, CVA1, and CVA2 were positively associated with DHH. Overall, both models selected the same significant variables and had similar estimates. The fitted model for the left foot was given as (3).
Table 5 and
Table 6 show the most important variables for the left and right feet individually, including the most important FSR numbers. We compared the more important FSRs in
Table 5 and
Table 6 according to the front, middle, and back positions of the soles of the feet, and organize them into
Table 7.
If we want to know which personal features besides FSRs have better predictive ability for the height of high heels, we can organize and compare the data in
Table 2 and
Table 6, which can be organized into
Table 8.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}