
Reported Outcome Measures in Studies of Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Source of Evidence Screening and Selection
2.3. Data Extraction
2.4. Analysis and Presentation of Results
3. Results
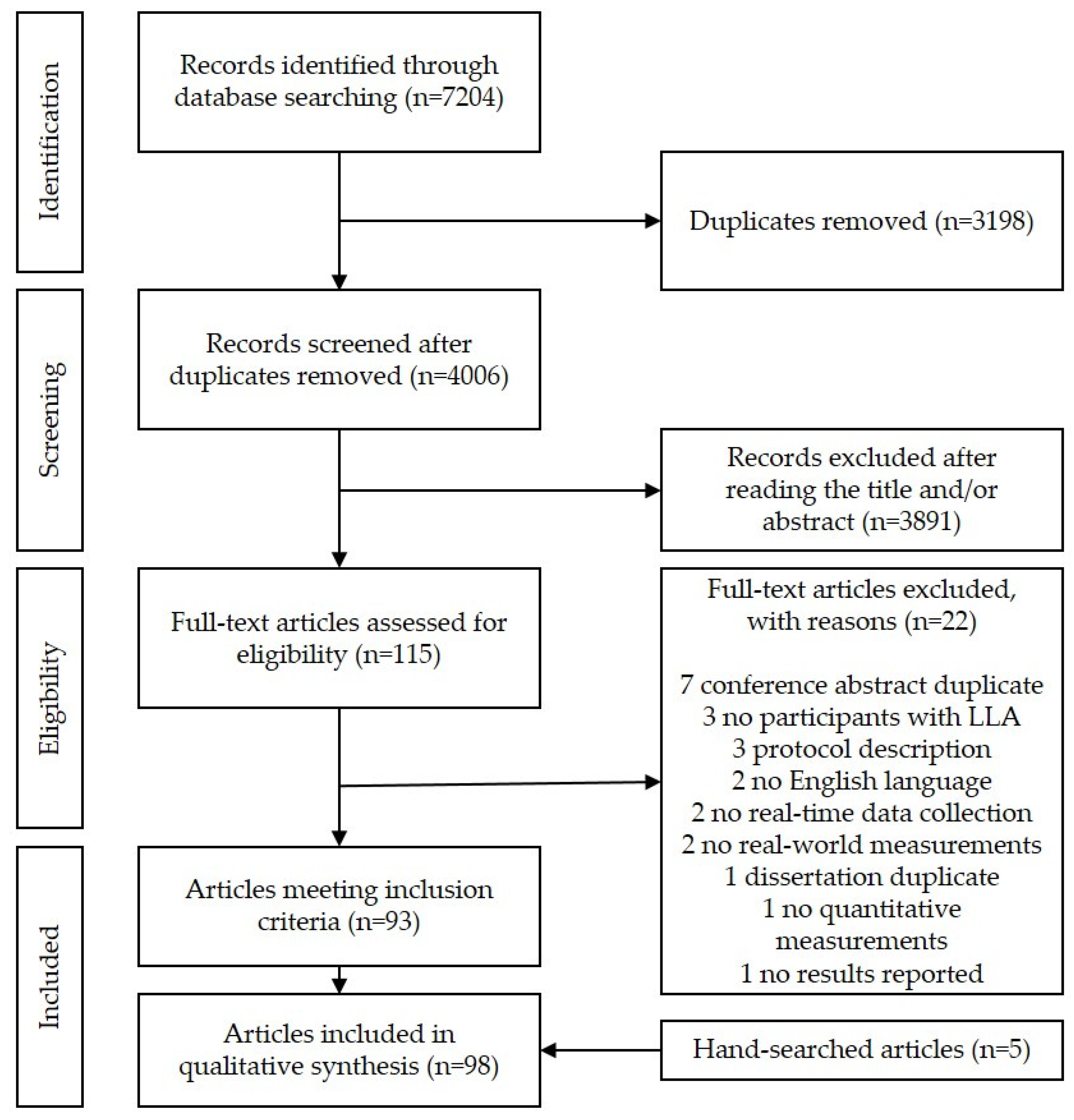
3.1. Search Results
3.2. Inclusion of Sources of Evidence
3.3. Review Findings
3.3.1. Categories of Reported Outcome Measures
Step Count
Fitness and Intensity of Activity
Type of Activity and Body Posture
Commercial Scores
Prosthetic Use and Fit
Gait Quality
GPS
Accuracy
3.3.2. Reported Outcome Measure in Categories Per Study Design
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
| MEDLINE Search | |
| 1 | Artificial Limbs/or exp Amputation/ |
| 2 | (amput * or prosthe * or prothes * or “artificial limb *”).ti,ab. |
| 3 | (limb adj3 (remov* or loss)).ti,ab. |
| 4 | 1 or 2 or 3 |
| 5 | gait/or gait analysis/ |
| 6 | Walking/ |
| 7 | (gait or step or steps or stepping or cadence or walk or walking or ambulat * or activit * or mobility or performance).ti,ab. |
| 8 | 5 or 6 or 7 |
| 9 | Monitoring, Ambulatory/ |
| 10 | (monitor * or track * or quantif * or assess * or measur * or count or counting or stepwatch or fitbit or acceleromet* or pedomet * or sensor or actigraph or IMU * or “inertial sensor” or “inertial measurement unit*”).ti,ab. |
| 11 | 9 or 10 |
| 12 | lower extremity/or ankle/or knee/or leg/or thigh/ |
| 13 | (“lower limb *” or “lower extremit *” or transfem * or trans-fem * or transtibial or trans-tibial or “above knee” or “below knee”).ti,ab. |
| 14 | 12 or 13 |
| 15 | 4 and 8 and 11 and 14 |
| 16 | limit 15 to yr = “1999-Current” |
References
- WHO. International Classification of Functioning, Disability and Health: ICF. Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 28 October 2021).
- Kamrad, I.; Söderberg, B.; Örneholm, H.; Hagberg, K. SwedeAmp-the Swedish Amputation and Prosthetics Registry: 8-year data on 5762 patients with lower limb amputation show sex differences in amputation level and in patient-reported outcome. Acta Orthop. 2020, 91, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Batten, H.; Lamont, R.; Kuys, S.; McPhail, S.; Mandrusiak, A. What are the barriers and enablers that people with a lower limb amputation experience when walking in the community? Disabil. Rehabil. 2020, 42, 3481–3487. [Google Scholar] [CrossRef] [PubMed]
- Stepien, J.M.; Cavenett, S.; Taylor, L.; Crotty, M. Activity levels among lower-limb amputees: Self-report versus step activity monitor. Arch. Phys. Med. Rehabil. 2007, 88, 896–900. [Google Scholar] [CrossRef] [PubMed]
- George, K.; Batterham, A.; Sullivan, I. Validity in clinical research: A review of basic concepts and definitions. Phys. Sport 2000, 1, 19–27. [Google Scholar] [CrossRef]
- Shawen, N.; Lonini, L.; Mummidisetty, C.K.; Shparii, I.; Albert, M.V.; Kording, K.; Jayaraman, A. Fall detection in individuals with lower limb amputations using mobile phones: Machine learning enhances robustness for real-rorld applications. JMIR Mhealth Uhealth 2017, 5, e151. [Google Scholar] [CrossRef]
- Kluge, F.; Del Din, S.; Cereatti, A.; Gaßner, H.; Hansen, C.; Helbostad, J.L.; Klucken, J.; Küderle, A.; Müller, A.; Rochester, L.; et al. Consensus based framework for digital mobility monitoring. PLoS ONE 2021, 16, e0256541. [Google Scholar] [CrossRef]
- Hafner, B.J.; Morgan, S.J.; Abrahamson, D.C.; Amtmann, D. Characterizing mobility from the prosthetic limb user’s perspective: Use of focus groups to guide development of the Prosthetic Limb Users Survey of Mobility. Prosthet. Orthot. Int. 2016, 40, 582–590. [Google Scholar] [CrossRef]
- Evenson, K.R.; Goto, M.M.; Furberg, R.D. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int. J. Behav. Nutr. 2015, 12, 159. [Google Scholar] [CrossRef]
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Van Heerden, D.; Luan, H.; Cullen, K.; et al. Reliability and validity of commercially available wearable devices for measuring steps, energy expenditure, and heart rate: Systematic review. JMIR Mhealth Uhealth 2020, 8, e18694. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R.; Fantigrassi, M.; Motel, I. The efficacy of wearable activity tracking technology as part of a weight loss program: A systematic review. J. Sports Med. Phys. Fit. 2018, 58, 534–548. [Google Scholar] [CrossRef]
- Brickwood, K.J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-based wearable activity trackers increase physical activity participation: Systematic review and meta-analysis. JMIR Mhealth Uhealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]
- Pericleous, P.; van Staa, T.P. The use of wearable technology to monitor physical activity in patients with COPD: A literature review. Int. J. Chron. Obs. Pulmon. Dis. 2019, 14, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.A.; Jones, T.M.; Simpson, D.B.; Fini, N.A.; Kuys, S.S.; Borschmann, K.; Kramer, S.; Johnson, L.; Callisaya, M.L.; Mahendran, N.; et al. Activity monitors for increasing physical activity in adult stroke survivors. Cochrane Database Syst. Rev. 2018, 7, Cd012543. [Google Scholar] [CrossRef] [PubMed]
- Straiton, N.; Alharbi, M.; Bauman, A.; Neubeck, L.; Gullick, J.; Bhindi, R.; Gallagher, R. The validity and reliability of consumer-grade activity trackers in older, community-dwelling adults: A systematic review. Maturitas 2018, 112, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; Rissland, M.S.; Madagan, D.M.; Jones, K.N. A scoping review of physical activity in people with lower-limb loss: 10,000 steps per day? Phys. Ther. 2021, 101, pzab115. [Google Scholar] [CrossRef]
- Chadwell, A.; Diment, L.; Micó-Amigo, M.; Morgado Ramírez, D.Z.; Dickinson, A.; Granat, M.; Kenney, L.; Kheng, S.; Sobuh, M.; Ssekitoleko, R.; et al. Technology for monitoring everyday prosthesis use: A systematic review. J. Neuroeng. Rehabil. 2020, 17, 93. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. Scoping Reviews. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Mellema, M.; Gjøvaag, T. Outcome Measures Used in Studies to Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review Protocol. Available online: https://osf.io/7pf2u/ (accessed on 23 September 2021).
- Coleman, K.L.; Smith, D.G.; Boone, D.A.; Joseph, A.W.; del Aguila, M.A. Step activity monitor: Long-term, continuous recording of ambulatory function. J. Rehabil. Res. Dev. 1999, 36, 8–18. [Google Scholar] [PubMed]
- Bramer, W.; Bain, P. Updating search strategies for systematic reviews using EndNote. J. Med. Libr. Assoc. 2017, 105, 285–289. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Tolani, A.S.; Wurdeman, S.R.; Billing, B.; O’Brien, E.; England, D.L.; Stevens, P.M.; Flores, A. Understanding changes in physical activity among lower limb prosthesis users: A COVID-19 case series [clinical letter]. PMR 2021, 13, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, N.J.; Stachowiak, A.; Reddin, C. Prosthetic disuse leads to lower balance confidence in a long-term user of a transtibial prosthesis. Adv. Wound Caref. 2021, 10, 529–533. [Google Scholar] [CrossRef]
- Miller, M.J.; Blankenship, J.M.; Kline, P.W.; Melanson, E.L.; Christiansen, C.L. Patterns of sitting, standing, and stepping after lower limb amputation. Phys. Ther. 2021, 101, pzaa212. [Google Scholar] [CrossRef] [PubMed]
- Mellema, M.; Risnes, M.; Mirtaheri, P.; Gjøvaag, T. Impact of the COVID-19 restrictions on physical activity and quality of life in adults with lower limb amputation. Prosthet. Orthot. Int. 2021. [Google Scholar] [CrossRef]
- Mellema, M.; Mirtaheri, P.; Gjøvaag, T. Relationship between level of daily activity and upper-body aerobic capacity in adults with a lower limb amputation. Prosthet. Orthot. Int. 2021, 45, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Davis-Wilson, H.; Christiansen, C.; Gaffney, B.; Murray, A. Cumulative loading in individuals with non-traumatic lower limb amputation, individuals with diabetes mellitus, and healthy individuals [abstract]. In Proceedings of the Virtual 2021 OARSI World Congress on Osteoarthritis, Berlin, Germany, 29 April–1 May 2021; pp. 169–170. [Google Scholar]
- Chihuri, S.T.; Youdan, G.A., Jr.; Wong, C.K. Quantifying the risk of falls and injuries for amputees beyond annual fall rates—A longitudinal cohort analysis based on person-step exposure over time. Prev. Med. Rep. 2021, 24, 101626. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.B.; Miller, M.J.; Murray, A.M.; Fields, T.T.; So, N.F.; Christiansen, C.L. Falls after dysvascular transtibial amputation: A secondary analysis of falling characteristics and reduced physical performance. PMR 2021, 13, 19–29. [Google Scholar] [CrossRef]
- Miller, M.J.; Morris, M.A.; Magnusson, D.M.; Putnam, K.; Cook, P.F.; Schenkman, M.L.; Christiansen, C.L. Psychosocial factors influence physical activity after dysvascular amputation: A convergent mixed-methods study. PMR 2020, 13, 737–745. [Google Scholar] [CrossRef]
- Hofstad, C.J.; Bongers, K.T.J.; Didden, M.; van Ee, R.F.; Keijsers, N.L.W. Maximal walking distance in persons with a lower limb amputation [letter]. Sensors 2020, 20, 6770. [Google Scholar] [CrossRef]
- Beisheim, E.H.; Arch, E.S.; Horne, J.R.; Sions, J.M. Performance-based outcome measures are associated with cadence variability during community ambulation among individuals with a transtibial amputation. Prosthet. Orthot. Int. 2020, 44, 215–224. [Google Scholar] [CrossRef]
- Zhang, X.; Fiedler, G.; Liu, Z. Evaluation of gait variable change over time as transtibial amputees adapt to a new prosthesis foot. BioMed Res. Int. 2019, 2019, 9252368. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.; Roberts, A.; Murray, K.; Deans, S.; Jarvis, H. Daily step count of British military males with bilateral lower limb amputations: A comparison of in-patient rehabilitation with the consecutive leave period between admissions. Prosthet. Orthot. Int. 2019, 43, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Pepin, M.-E.; Devour, A.; Coolsaet, R.; Galen, S. Correlation between functional ability and physical activity in individuals with transtibial amputations: A cross-sectional study. Cardiopulm. Phys. Ther. J. 2019, 30, 70–78. [Google Scholar] [CrossRef]
- Musig, J.A.; Brauner, T.; Kroger, I.; Varady, P.A.; Brand, A.; Klopfer-Kramer, I.; Simmel, S.; Horstmann, T.; Augat, P. Relation between the amount of daily activity and gait quality in transfemoral amputees. Int. J. Rehabil. Res. 2019, 42, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.J.; Cook, P.F.; Kline, P.W.; Anderson, C.B.; Stevens-Lapsley, J.E.; Christiansen, C.L. Physical function and pre-amputation characteristics explain daily step count after dysvascular amputation. PMR 2019, 11, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Klute, G.K.; Berge, J.S. Daily step counts and use of activity monitors by individuals with lower-limb loss [abstract]. In Proceedings of the 45th Academy Annual Meeting and Scientific Symposium, Orlando, FL, USA, 6–9 March 2019; p. 15. [Google Scholar]
- Balkman, G.S.; Vamos, A.C.; Sanders, J.E.; Larsen, B.G.; Hafner, B.J. Prosthetists’ perceptions of information obtained from a lower-limb prosthesis monitoring system: A pilot study. J. Prosthet. Orthot. 2019, 31, 112–120. [Google Scholar] [CrossRef]
- Sions, J.M.; Arch, E.S.; Horne, J.R. Self-reported functional mobility, balance confidence, and prosthetic use are associated with daily step counts among individuals with a unilateral transtibial amputation. J. Phys. Act. Health 2018, 15, 423–429. [Google Scholar] [CrossRef]
- Sanders, J.E.; Youngblood, R.T.; Hafner, B.J.; Ciol, M.A.; Allyn, K.J.; Gardner, D.; Cagle, J.C.; Redd, C.B.; Dietrich, C.R. Residual limb fluid volume change and volume accommodation: Relationships to activity and self-report outcomes in people with trans-tibial amputation. Prosthet. Orthot. Int. 2018, 42, 415–427. [Google Scholar] [CrossRef]
- Esposito, E.R.; Schnall, B.L.; Hendershot, B.D.; Wilken, J.M. Daily step counts in service members with lower limb amputation [abstract]. In Proceedings of the American College of Sports Medicine Annual Meeting, Minneapolis, MN, USA, 29 May–2 June 2018; pp. 391–392. [Google Scholar]
- Samuelsen, B.T.; Andrews, K.L.; Houdek, M.T.; Terry, M.; Shives, T.C.; Sim, F.H. The Impact of the immediate postoperative prosthesis on patient mobility and quality of life after transtibial amputation. Am. J. Phys. Med. Rehabil. 2017, 96, 116–119. [Google Scholar] [CrossRef]
- Juszczak, M.; King, A.; Shin, R.; Van De Walle, N.; Bushnik, T.; Cohen, J. Developing an evidence based approach to address functional level changes in persons following amputation [abstract]. In Proceedings of the American Congress of Rehabilitation Medicine 94th Annual Conference, Atlanta, GA, USA, 23–28 October 2017; p. e166. [Google Scholar]
- Paxton, R.J.; Murray, A.M.; Stevens-Lapsley, J.E.; Sherk, K.A.; Christiansen, C.L. Physical activity, ambulation, and comorbidities in people with diabetes and lower-limb amputation. J. Rehabil. Res. Dev. 2016, 53, 1069–1078. [Google Scholar] [CrossRef]
- Orendurff, M.S.; Raschke, S.U.; Winder, L.; Moe, D.; Boone, D.A.; Kobayashi, T. Functional level assessment of individuals with transtibial limb loss: Evaluation in the clinical setting versus objective community ambulatory activity. J. Rehabil. Assist. Technol. Eng. 2016, 3, 2055668316636316. [Google Scholar] [CrossRef] [PubMed]
- Mandel, A.; Paul, K.; Paner, R.; Devlin, M.; Dilkas, S.; Pauley, T. Balance confidence and activity of community-dwelling patients with transtibial amputation. J. Rehabil. Res. Dev. 2016, 53, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Desveaux, L.; Goldstein, R.S.; Mathur, S.; Hassan, A.; Devlin, M.; Pauley, T.; Brooks, D. Physical activity in adults with diabetes following prosthetic rehabilitation. Can. J. Diabetes 2016, 40, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.K.G.; Wong, M.S. Comparison of prosthetic outcomes between adolescent transtibial and transfemoral amputees after Sichuan earthquake using Step Activity Monitor and Prosthesis Evaluation Questionnaire. Prosthet. Orthot. Int. 2016, 40, 58–64. [Google Scholar] [CrossRef]
- Arch, E.S.; Higginson, J.S.; Buckley, J.M.; Madden, C.; Galbraith, M.; Lewis, J.; Erol, O.; Bortz, C.; Rossi, A.; Horne, J. Real-world walking performance of individuals with lower-limb amputation classified as medicare functional classification level 2 and 3. J. Prosthet. Orthot. 2016, 28, 51–57. [Google Scholar] [CrossRef]
- Kent, J.A.; Stergiou, N.; Wurdeman, S.R. Step activity and stride-to-stride fluctuations are negatively correlated in individuals with transtibial amputation. Clin. Biomech. 2015, 30, 1225–1229. [Google Scholar] [CrossRef]
- Hordacre, B.; Barr, C.; Crotty, M. Community activity and participation are reduced in transtibial amputee fallers: A wearable technology study. BMJ Innov. 2015, 1, 10–16. [Google Scholar] [CrossRef]
- Parry, I.S.; Bagley, A.; Sen, S.; Greenhalgh, D.G.; Palmieri, T.L. Gait outcome of pediatric lower extremity amputation patients with and without skin grafts [abstract]. In Proceedings of the 46th Annual Meeting of the American Burn Association, Boston, MA, USA, 25–28 March 2014; p. 78. [Google Scholar]
- Lin, S.-J.; Winston, K.D.; Mitchell, J.; Girlinghouse, J.; Crochet, K. Physical activity, functional capacity, and step variability during walking in people with lower-limb amputation. Gait Posture 2014, 40, 140–144. [Google Scholar] [CrossRef]
- Hordacre, B.; Barr, C.; Crotty, M. Use of an activity monitor and GPS device to assess community activity and participation in transtibial amputees. Sensors 2014, 14, 5845–5859. [Google Scholar] [CrossRef]
- Halsne, E.G.; Waddingham, M.G.; Hafner, B.J. Long-term activity in and among persons with transfemoral amputation. J. Rehabil. Res. Dev. 2013, 50, 515–530. [Google Scholar] [CrossRef]
- Highsmith, M.J.; Kahle, J.T.; Quillen, W.S.; Mengelkoch, L.J. Spatiotemporal parameters and Step Activity of a specialized stepping pattern used by a transtibial amputee during a denali mountaineering expedition. J. Prosthet. Orthot. 2012, 24, 153–157. [Google Scholar] [CrossRef]
- van den Berg-Emons, R.J.; Bussmann, J.B.; Stam, H.J. Accelerometry-based activity spectrum in persons with chronic physical conditions. Arch. Phys. Med. Rehabil. 2010, 91, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Parker, K.; Kirby, R.L.; Adderson, J.; Thompson, K. Ambulation of people with lower-limb amputations: Relationship between capacity and performance measures. Arch. Phys. Med. Rehabil. 2010, 91, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, D.; Brandes, M.; Hardes, J.; Gosheger, G.; Rodl, R. Physical activity levels after limb salvage surgery are not related to clinical scores-objective activity assessment in 22 patients after malignant bone tumor treatment with modular prostheses. J. Surg. Oncol. 2008, 98, 97–100. [Google Scholar] [CrossRef]
- Bussmann, J.B.; Schrauwen, H.J.; Stam, H.J. Daily physical activity and heart rate response in people with a unilateral traumatic transtibial amputation. Arch. Phys. Med. Rehabil. 2008, 89, 430–434. [Google Scholar] [CrossRef]
- Kanade, R.V.; van Deursen, R.W.M.; Price, P.; Harding, K. Risk of plantar ulceration in diabetic patients with single-leg amputation. Clin. Biomech. 2006, 21, 306–313. [Google Scholar] [CrossRef]
- Kanade, R.V.; van Deursen, R.W.M.; Harding, K.; Price, P. Walking performance in people with diabetic neuropathy: Benefits and threats. Diabetologia 2006, 49, 1747–1754. [Google Scholar] [CrossRef]
- Hopyan, S.; Tan, J.W.; Graham, H.K.; Torode, I.P. Function and upright time following limb salvage, amputation, and rotationplasty for pediatric sarcoma of bone. J. Pediatr. Orthop. 2006, 26, 405–408. [Google Scholar] [CrossRef]
- Bussmann, J.B.; Grootscholten, E.A.; Stam, H.J. Daily physical activity and heart rate response in people with a unilateral transtibial amputation for vascular disease. Arch. Phys. Med. Rehabil. 2004, 85, 240–244. [Google Scholar] [CrossRef]
- Vanicek, N.; Coleman, E.; Watson, J.; Bell, K.; McDaid, C.; Barnett, C.; Twiste, M.; Jepson, F.; Salawu, A.; Harrison, D.; et al. STEPFORWARD study: A randomised controlled feasibility trial of a self-aligning prosthetic ankle-foot for older patients with vascular-related amputations. BMJ Open 2021, 11, e045195. [Google Scholar] [CrossRef]
- Kaluf, B.; Cox, C.; Shoemaker, E. Hydraulic- and microprocessor-controlled ankle-foot prostheses for limited community ambulators with unilateral transtibial amputation: Pilot study. J. Prosthet. Orthot. 2021, 33, 294–303. [Google Scholar] [CrossRef]
- Kim, J.; Wensman, J.; Colabianchi, N.; Gates, D.H. The influence of powered prostheses on user perspectives, metabolics, and activity: A randomized crossover trial. J. Neuroeng. Rehabil. 2021, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Guerra, G.; Rattanakoch, J.; Miyata, Y.; Suntharalingam, S. Sustainable Development: A Below-Knee Prostheses Liner for Resource Limited Environments [technical brief]. J. Med. Device 2020, 14, 014501. [Google Scholar] [CrossRef]
- Miyata, Y.; Sasaki, K.; Guerra, G.; Rattanakoch, J. Sustainable, affordable and functional: Reimagining prosthetic liners in resource limited environments. Disabil. Rehabil. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Halsne, E.G.; Czerniecki, J.M.; Shofer, J.B.; Morgenroth, D.C. The effect of prosthetic foot stiffness on foot-ankle biomechanics and relative foot stiffness perception in people with transtibial amputation. Clin. Biomech. 2020, 80, 105141. [Google Scholar] [CrossRef] [PubMed]
- Gaunaurd, I.; Gailey, R.; Springer, B.; Symsack, A.; Clemens, S.; Lucarevic, J.; Kristal, A.; Bennett, C.; Isaacson, B.; Agrawal, V.; et al. The effectiveness of the DoD/VA mobile cevice outcomes-based rehabilitation program for high functioning service members and veterans with lower limb amputation. Mil. Med. 2020, 185, 480–489. [Google Scholar] [CrossRef]
- Christiansen, C.L.; Miller, M.J.; Kline, P.W.; Fields, T.T.; Sullivan, W.J.; Blatchford, P.J.; Stevens-Lapsley, J.E. Biobehavioral intervention targeting physical activity behavior change for older veterans after nontraumatic amputation: A randomized controlled trial. PMR 2020, 12, 957–966. [Google Scholar] [CrossRef]
- Annis, S.; Bryant, J.; Chen, M.; Cunningham, C.; Morshed, S. Can improved prosthetic alignment increase activity level in patients with lower-extremity amputations? [abstract]. In Proceedings of the 45th Academy Annual Meeting and Scientific Symposium, Orlando, FL, USA, 6–9 March 2019; p. 12. [Google Scholar]
- Littman, A.J.; Haselkorn, J.K.; Arterburn, D.E.; Boyko, E.J. Pilot randomized trial of a telephone-delivered physical activity and weight management intervention for individuals with lower extremity amputation. Disabil. Health J. 2019, 12, 43–50. [Google Scholar] [CrossRef]
- Morgan, S.J.; McDonald, C.L.; Halsne, E.G.; Cheever, S.M.; Salem, R.; Kramer, P.A.; Hafner, B.J. Laboratory- and community-based health outcomes in people with transtibial amputation using crossover and energy-storing prosthetic feet: A randomized crossover trial. PLoS ONE 2018, 13, e0189652. [Google Scholar] [CrossRef]
- McDonald, C.L.; Kramer, P.A.; Morgan, S.J.; Halsne, E.G.; Cheever, S.M.; Hafner, B.J. Energy expenditure in people with transtibial amputation walking with crossover and energy storing prosthetic feet: A randomized within-subject study. Gait Posture 2018, 62, 349–354. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Bernhardt, K.A.; Symms, K. Functional assessment and satisfaction of transfemoral amputees with low mobility (FASTK2): A clinical trial of microprocessor-controlled vs. non-microprocessor-controlled knees. Clin. Biomech. 2018, 58, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, C.L.; Miller, M.J.; Murray, A.M.; Stephenson, R.O.; Stevens-Lapsley, J.E.; Hiatt, W.R.; Schenkman, M.L. Behavior-change intervention targeting physical function, walking, and disability after dysvascular amputation: A randomized controlled pilot trial. Arch. Phys. Med. Rehabil. 2018, 99, 2160–2167. [Google Scholar] [CrossRef] [PubMed]
- Wurdeman, S.R.; Schmid, K.K.; Myers, S.A.; Jacobsen, A.L.; Stergiou, N. Step activity and 6-Minute Walk Test outcomes when wearing low-activity or high-activity prosthetic feet. Am. J. Phys. Med. Rehabil. 2017, 96, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.E.; Youngblood, R.T.; Hafner, B.J.; Cagle, J.C.; McLean, J.B.; Redd, C.B.; Dietrich, C.R.; Ciol, M.A.; Allyn, K.J. Effects of socket size on metrics of socket fit in trans-tibial prosthesis users. Med. Eng. Phys. 2017, 44, 32–43. [Google Scholar] [CrossRef]
- Imam, B.; Miller, W.C.; Finlayson, H.; Eng, J.J.; Jarus, T. A randomized controlled trial to evaluate the feasibility of the Wii Fit for improving walking in older adults with lower limb amputation. Clin. Rehabil. 2017, 31, 82–92. [Google Scholar] [CrossRef]
- Andrysek, J.; Wright, F.V.; Rotter, K.; Garcia, D.; Valdebenito, R.; Mitchell, C.A.; Rozbaczylo, C.; Cubillos, R. Long-term clinical evaluation of the automatic stance-phase lock-controlled prosthetic knee joint in young adults with unilateral above-knee amputation. Disabil. Rehabil. Assist. Technol. 2017, 12, 378–384. [Google Scholar] [CrossRef]
- Klute, G.K.; Bates, K.J.; Berge, J.S.; Biggs, W.; King, C. Prosthesis management of residual-limb perspiration with subatmospheric vacuum pressure. J. Rehabil. Res. Dev. 2016, 53, 721–728. [Google Scholar] [CrossRef]
- Highsmith, M.J.; Kahle, J.T.; Wernke, M.M.; Carey, S.L.; Miro, R.M.; Lura, D.J.; Sutton, B.S. Effects of the Genium knee system on functional level, stair ambulation, perceptive and economic outcomes in transfemoral amputees. Technol. Innov. 2016, 18, 139–150. [Google Scholar] [CrossRef]
- Raschke, S.U.; Orendurff, M.S.; Mattie, J.L.; Kenyon, D.E.A.; Jones, O.Y.; Moe, D.; Winder, L.; Wong, A.S.; Moreno-Hernandez, A.; Highsmith, M.J.; et al. Biomechanical characteristics, patient preference and activity level with different prosthetic feet: A randomized double blind trial with laboratory and community testing. J. Biomech. 2015, 48, 146–152. [Google Scholar] [CrossRef]
- Hafner, B.J.; Askew, R.L. Physical performance and self-report outcomes associated with use of passive, adaptive, and active prosthetic knees in persons with unilateral, transfemoral amputation: Randomized crossover trial. J. Rehabil. Res. Dev. 2015, 52, 677–700. [Google Scholar] [CrossRef]
- Segal, A.D.; Kracht, R.; Klute, G.K. Does a torsion adapter improve functional mobility, pain, and fatigue in patients with transtibial amputation? Clin. Orthop. Relat. Res. 2014, 472, 3085–3092. [Google Scholar] [CrossRef] [PubMed]
- Buis, A.W.P.; Dumbleton, T.; Murray, K.D.; McHugh, B.F.; McKay, G.; Sexton, S. Measuring the daily stepping activity of people with transtibial amputation using the ActivPAL™ Activity Monitor. J. Prosthet. Orthot. 2014, 26, 43–47. [Google Scholar] [CrossRef]
- Theeven, P.J.; Hemmen, B.; Geers, R.P.J.; Smeets, R.J.E.M.; Brink, P.R.G.; Seelen, H.A.M. Influence of advanced prosthetic knee joints on perceived performance and everyday life activity level of low-functional persons with a transfemoral amputation or knee disarticulation. J. Rehabil. Med. 2012, 44, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Gailey, R.S.; Gaunaurd, I.; Agrawal, V.; Finnieston, A.; O’Toole, C.; Tolchin, R. Application of self-report and performance-based outcome measures to determine functional differences between four categories of prosthetic feet. J. Rehabil. Res. Dev. 2012, 49, 597–612. [Google Scholar] [CrossRef]
- Klute, G.K.; Berge, J.S.; Biggs, W.; Pongnumkul, S.; Popovic, Z.; Curless, B. Vacuum-assisted socket suspension compared with pin suspension for lower extremity amputees: Effect on fit, activity, and limb volume. Arch. Phys. Med. Rehabil. 2011, 92, 1570–1575. [Google Scholar] [CrossRef]
- Agrawal, V. A Comparison of Gait Kinetics between Prosthetic Feet during Functional Activities—Symmetry in External Work (SEW) Approach. Ph.D. Thesis, University of Miami, Coral Gables, FL, USA, 2010. [Google Scholar]
- Hafner, B.J.; Willingham, L.L.; Buell, N.C.; Allyn, K.J.; Smith, D.G. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch. Phys. Med. Rehabil. 2007, 88, 207–217. [Google Scholar] [CrossRef]
- Darter, B.J. The Effects of an Integrated Motor Learning Based Treadmill Mobility and Aerobic Exercise Training Program in Persons with a Transfemoral Amputation. Ph.D. Thesis, University of Iowa, Iowa City, IA, USA, 2007. [Google Scholar]
- Klute, G.K.; Berge, J.S.; Orendurff, M.S.; Williams, R.M.; Czerniecki, J.M. Prosthetic intervention effects on activity of lower-extremity amputees. Arch. Phys. Med. Rehabil. 2006, 87, 717–722. [Google Scholar] [CrossRef]
- Hsu, M.-J.; Nielsen, D.H.; Lin-Chan, S.-J.; Shurr, D. The effects of prosthetic foot design on physiologic measurements, self-selected walking velocity, and physical activity in people with transtibial amputation. Arch. Phys. Med. Rehabil. 2006, 87, 123–129. [Google Scholar] [CrossRef]
- Berge, J.S.; Czerniecki, J.M.; Klute, G.K. Efficacy of shock-absorbing versus rigid pylons for impact reduction in transtibial amputees based on laboratory, field, and outcome metrics. J. Rehabil. Res. Dev. 2005, 42, 795–808. [Google Scholar] [CrossRef]
- Coleman, K.L.; Boone, D.A.; Laing, L.S.; Mathews, D.E.; Smith, D.G. Quantification of prosthetic outcomes: Elastomeric gel liner with locking pin suspension versus polyethylene foam liner with neoprene sleeve suspension. J. Rehabil. Res. Dev. 2004, 41, 591–602. [Google Scholar] [CrossRef]
- Srisuwan, B.; Klute, G.K. Locomotor activities of individuals with lower-limb amputation. Prosthet. Orthot. Int. 2021, 45, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Murray, L.; Stankovic, L.; Stankovic, V.; Buis, A. Human activity recognition of individuals with lower limb amputation in free-living conditions: A pilot study. Sensors 2021, 21, 8377. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, B.; Diment, L.; Granat, M.H. A machine learning classification model for monitoring the daily physical behaviour of lower-limb amputees. Sensors 2021, 21, 7458. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Colabianchi, N.; Wensman, J.; Gates, D.H. Wearable sensors quantify mobility in people with lower limb amputation during daily life. IEEE Trans. Neural Syst. 2020, 28, 1282–1291. [Google Scholar] [CrossRef]
- Weathersby, E.J.; Cagle, J.C.; Larsen, B.G.; Henrikson, K.M.; Sanders, J.E. Development of a magnetic composite material for measurement of residual limb displacements in prosthetic sockets. J. Rehabil. Assist. Technol. Eng. 2018, 5, 2055668318763481. [Google Scholar] [CrossRef]
- Swanson, E.C.; McLean, J.B.; Allyn, K.J.; Redd, C.B.; Sanders, J.E. Instrumented socket inserts for sensing interaction at the limb-socket interface. Med. Eng. Phys. 2018, 51, 111–118. [Google Scholar] [CrossRef]
- Arch, E.S.; Erol, O.; Bortz, C.; Madden, C.; Galbraith, M.; Rossi, A.; Lewis, J.; Higginson, J.S.; Buckley, J.M.; Horne, J. Method to quantify cadence variability of individuals with lower-limb amputation. J. Prosthet. Orthot. 2017, 29, 73–79. [Google Scholar] [CrossRef]
- Gardner, D.W.; Redd, C.B.; Cagle, J.C.; Sanders, J.E.; Hafner, B.J. Monitoring prosthesis user activity and doffing using an activity monitor and proximity sensors. J. Prosthet. Orthot. 2016, 28, 68–77. [Google Scholar] [CrossRef]
- Jayaraman, A.; Deeny, S.; Eisenberg, Y.; Mathur, G.; Kuiken, T. Global position sensing and step activity as outcome measures of community mobility and social interaction for an individual with a transfemoral amputation due to dysvascular disease. Phys. Ther. 2014, 94, 401–410. [Google Scholar] [CrossRef]
- Redfield, M.T.; Cagle, J.C.; Hafner, B.J.; Sanders, J.E. Classifying prosthetic use via accelerometry in persons with transtibial amputations. J. Rehabil. Res. Dev. 2013, 50, 1201–1212. [Google Scholar] [CrossRef]
- Frossard, L.; Stevenson, N.; Sullivan, J.; Uden, M.; Pearcy, M. Categorization of activities of daily living of lower limb amputees during short-term use of a portable kinetic recording system: A preliminary study. J. Prosthet. Orthot. 2011, 23, 2–13. [Google Scholar] [CrossRef]
- Frossard, L.; Stevenson, N.; Smeathers, J.; Haggstrom, E.; Hagberg, K.; Sullivan, J.; Ewins, D.; Gow, D.L.; Gray, S.; Branemark, R. Monitoring of the load regime applied on the osseointegrated fixation of a trans-femoral amputee: A tool for evidence-based practice. Prosthet. Orthot. Int. 2008, 32, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, B.; Berdan, J.; Nuntapreda Kirk, M.; Rosenbaum Chou, T. The accuracy and validity of Modus Trex Activity Monitor in determining functional level in veterans with transtibial amputations. J. Prosthet. Orthot. 2018, 30, 20–30. [Google Scholar] [CrossRef]
- Arch, E.S.; Sions, J.M.; Horne, J.; Bodt, B.A. Step count accuracy of StepWatch and FitBit One TM among individuals with a unilateral transtibial amputation. Prosthet. Orthot. Int. 2018, 42, 518–526. [Google Scholar] [CrossRef]
- Orendurff, M.S.; Kobayashi, T.; Villarosa, C.Q.; Coleman, K.L.; Boone, D.A. Comparison of a computerized algorithm and prosthetists’ judgment in rating functional levels based on daily step activity in transtibial amputees. J. Rehabil. Assist. Technol. Eng. 2016, 3, 2055668316670535. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.V.; Deeny, S.; McCarthy, C.; Valentin, J.; Jayaraman, A. Monitoring daily function in persons with transfemoral amputations using a commercial activity monitor: A feasibility study. PMR 2014, 6, 1120–1127. [Google Scholar] [CrossRef]
- Albert, M.V.; McCarthy, C.; Valentin, J.; Herrmann, M.; Kording, K.; Jayaraman, A. Monitoring functional capability of individuals with lower limb amputations using mobile phones. PLoS ONE 2013, 8, e65340. [Google Scholar] [CrossRef]
- van Dam, M.S.; Kok, G.J.; Munneke, M.; Vogelaar, F.J.; Vliet Vlieland, T.P.; Taminiau, A.H. Measuring physical activity in patients after surgery for a malignant tumour in the leg. The reliability and validity of a continuous ambulatory activity monitor. J. Bone Jt. Surg. Am. 2001, 83, 1015–1019. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Han, H.; Aguiar, E.J.; Barreira, T.V.; Schuna, J.M., Jr.; Kang, M.; Rowe, D.A. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: A narrative review. Br. J. Sports Med. 2018, 52, 776–788. [Google Scholar] [CrossRef]
- Yildiz, N.T.; Kocaman, H.; Yazıcıoğlu, F.G. Outcome measures used in lower extremity amputation: Review of clinical use and psychometric properties. J. Surg. Med. 2021, 5, 544–549. [Google Scholar] [CrossRef]
- Naschitz, J.E.; Lenger, R. Why traumatic leg amputees are at increased risk for cardiovascular diseases. QJM 2008, 101, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Deans, S.A.; McFadyen, A.K.; Rowe, P.J. Physical activity and quality of life: A study of a lower-limb amputee population. Prosthet. Orthot. Int. 2008, 32, 186–200. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Rowe, D.A. Using cadence to study free-living ambulatory behaviour. Sports Med. 2012, 42, 381–398. [Google Scholar] [CrossRef] [PubMed]
- Brunswik, E. Representative design and probabilistic theory in a functional psychology. Psychol. Rev. 1955, 62, 193–217. [Google Scholar] [CrossRef]
- Kihlstrom, J.F. Ecological validity and “Ecological validity”. Perspect. Psychol. Sci. 2021, 16, 466–471. [Google Scholar] [CrossRef]
- Czerniecki, J.M.; Morgenroth, D.C. Metabolic energy expenditure of ambulation in lower extremity amputees: What have we learned and what are the next steps? Disabil. Rehabil. 2017, 39, 143–151. [Google Scholar] [CrossRef]
- Holleman, G.A.; Hooge, I.T.C.; Kemner, C.; Hessels, R.S. The ‘Real-World Approach’ and its problems: A critique of the term ecological validity. Front. Psychol. 2020, 11, 721. [Google Scholar] [CrossRef]
- Seth, M.; Coyle, P.C.; Pohlig, R.T.; Beisheim, E.H.; Horne, J.R.; Hicks, G.E.; Sions, J.M. Gait asymmetry is associated with performance-based physical function among adults with lower-limb amputation. Physiother. Theory Pract. 2021, 1–11. [Google Scholar] [CrossRef]
- Jayakaran, P.; Johnson, G.M.; Sullivan, S.J.; Nitz, J.C. Instrumented measurement of balance and postural control in individuals with lower limb amputation: A critical review. Int. J. Rehabil. Res. 2012, 35, 187–196. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | First Author (Year, Country) | Title | Objective(s) | Study Population (n (Female)); Mean ± SD Age; Level (n); Etiology (n) | Technology; Placement; Duration | Reported Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|---|
| Observational studies | |||||||
| 1 | Tolani (2021, USA) [24] | Understanding changes in physical activity among lower limb prosthesis users: A COVID-19 case series (clinical letter) | Understand potential changes to Physical Activity (PA) during shutdown and “shelter-in-place” orders. | n = 4(0); between 20–79; 2 Trans-Tibial Amputation (TTA), 1 Trans-Femoral Amputation (TFA), 1 Knee Disarticulation (KD); 3 non-dysvascular, 1 dysvascular/diabetic | EmpowerGO; prosthesis; between 74 and 200 days | Steps per day (overall, pre-index, post-index); supplemental data: number of bouts; steps per bout; time per bout; steps per day normalized to pre-index step count | Two participants demonstrated clear signs of overall reduced activity through beginning stages of the COVID-19 pandemic. |
| 2 | Rosenblatt (2021, USA) [25] | Prosthetic disuse leads to lower balance confidence in a long-term user of a transtibial prosthesis | Assess the impact of prosthesis disuse on balance, gait, PA and balance confidence. | n = 1(0); 76; TTA; cancer | StepWatch 3; prosthetis; 2 × 7 days | Steps per day | Balance confidence, walking speed and steps per day decreased with 19%, 12%, and 19%, respectively, following 4 months of prosthesis disuse; functional measures were not impacted. |
| 3 | Miller (2021, USA) [26] | Patterns of sitting, standing, and stepping after lower limb amputation | Describe sitting, standing, and stepping patterns and compare the patterns between people with dysvascular Lower Limb Amputation (LLA) and traumatic LLA. | n = 32(5); 62.6 ± 7.8; 22 TTA, 7 TFA/KD; 15 trauma, 17 dysvascular | ActivPAL; thigh; 10 days | Steps per day; wake time (min/day); number of sit-to-stand transitions; sitting, standing and stepping in categorized bout durations (min/day), proportion/day, bouts/day) | Participants spent most time sitting. PA bouts were mostly <1 min. Significant between-etiology differences for sitting and standing time. |
| 4 | Mellema (2021, Norway) [27] | Impact of the COVID-19 restrictions on physical activity and quality of life in adults with lower limb amputation | Investigate the impact of COVID-19 restrictions on ambulatory activity and Health-Related Quality of Life (HR-QoL). | n = 20(4); 56.2 ± 11.9; 12 TTA, 2 KD, 5 TFA, 1 bilateral TTA; 9 trauma, 4 cancer, 2 diabetes, 5 others | StepWatch 4; prosthetic ankle; 2 × 7 days | Steps per day; prosthetic wear time (hours/day); time in low, moderate, and high intensity level | Prosthetic wear time decreased significantly. Daily step count, moderate-intensity and high-intensity ambulation, and HR-QoL increased, but low-intensity ambulation decreased. |
| 5 | Mellema (2021, Norway) [28] | Relationship between level of daily activity and upper-body aerobic capacity in adults with a lower limb amputation | Investigate the relationship between upper-body peak aerobic capacity (VO2peak), PA levels, and walking capacity. | n = 14(2); 55.7 ± 10.1; 7 TTA, 2 KD, 5 TFA; 8 trauma, 2 cancer, 1 congenital, 3 others | StepWatch 4; prosthetic ankle; 7 days | Steps per day, time in sedentary, low, moderate, high intensity (%); peak intensity level | VO2peak correlated significantly with daily step count, sedentary time, high-intensity activity level, and peak-intensity activity level, preferred walking speed, and 2-min walking test. |
| 6 | Davis-Wilson (2021, USA) [29] | Cumulative loading in individuals with non-traumatic lower limb amputation, individuals with diabetes mellitus, and healthy individuals (conference abstract) | Determine if differences existed in cumulative loading between individuals with diabetes + LLA, individuals with diabetes, and healthy individuals of similar health. | n = 6(0); 58 ± 6; level and etiology of amputation N/A | ActiGraph GT3X; hip; 10 days | Steps per day; cumulative loading (body weight/day) | No differences in cumulative loading between diabetes + LLA and diabetes groups, but diabetes + LLA had lower cumulative loading compared to healthy individuals. |
| 7 | Chihuri (2021, USA) [30] | Quantify the risk of falls and injuries for amputees beyond annual fall rates—A longitudinal cohort analysis based on person-step exposure over time | Determine all-cause fall and injury rates over time, accounting for daily per person-step exposure. | n = 10(3); 48.7 ± 12.5; 7 TTA, 3 TFA; 6 Peripheral Artery Disease (PVD), 2 trauma, 2 non-chronic medical cause | StepWatch 4; prosthetic ankle; 5 × 1 week | Steps per day | Limited community walking ability was associated with higher incidence of falls and injuries when accounting for person-steps. |
| 8 | Anderson (2020, USA) [31] | Falls after dysvascular transtibial amputation: A secondary analysis of falling characteristics and reduced physical performance | Characterize falls using existing Fall-Type Classification Framework and describe functional characteristics across the framework categories. | n = 69(N/A); 64.5 ± 8.6; 64 TTA, 1 TFA, 1 KD, 1 bilateral TTA & TFA, 2 bilateral TTA; all dysvascular | ActiGraph GT3X-BT; waist belt; 10 days | Steps per day | 43.5% of participants reported falls, of which the incidence was highest for intrinsic destabilization sources, from incorrect weight shift patterns during transfer activities. |
| 9 | Miller (2020, USA) [32] | Psychosocial factors influence physical activity after dysvascular amputation: A convergent mixed-methods study | Identify psychosocial factors with potential to influence clinically relevant measures of PA, physical function, and disability. | n = 20(2); 63.4 (57.5 70.0 interquartile range); 15 TTA, 2 TFA, 3 bilateral; all dysvascular | ActivPAL 3; thigh; 10 days | Steps per day | PA results from an interaction among perceptions of prosthesis, fear during mobility, influence of LLA on life activities, and positive outlook within social interactions. |
| 10 | Hofstad (2020, The Netherlands) [33] | Maximal walking distance in persons with a lower limb amputation (letter) | Assess the number of consecutive steps and walking bouts, using an accelerometer sensor. | n = 20(7); 68 (range 60–74); 9 TTA, 4 KD, 7 TFA; 6 trauma, 10 dysvascular, 2 cancer, 2 other | 3 tri-axial piezo-capacitive MiniMods Dynaport; 2 on each side of trouser pocket, 1 on sternum; 2 days | Maximal consecutive steps; frequency per hour of number of steps per bin; maximal walking distance (meters) | The SIGAM mobility grade did not reflect what participants do in daily life. Objective assessment of maximal number of consecutive steps or maximal covered distance is recommended. |
| 11 | Beisheim (2020, USA) [34] | Performance-based outcome measures are associated with cadence variability during community ambulation among individuals with a transtibial amputation | Evaluate whether physical performance (10—meter Walk Test-based walking speeds, L-Test, and Figure-of-8 Walk Test scores) is associated with community-based cadence variability. | n = 41(15); 58.3 (range 54.6–62.0); all TTA; 24 dysvascular, 13 trauma, 1 cancer, 1 congenital, 2 other | FitBit One; ankle; 7 days | Cadence variability (Weibul probability density) (steps/min); cadence variability scale parameter | Beyond covariates, faster self-selected gait speed best predicted increased cadence variability during community ambulation. |
| 12 | Zhang (2019, US) [35] | Evaluation of gait variable change over time as transtibial amputees adapt to a new prosthesis foot | Investigate whether gait variables were affected by the duration of accommodation period, and assess relationship between measures outcomes and subjective perception. | n = 7(0); 53.0 ± 15.2; all TTA; etiology N/A | Up move; prosthesis; 5 days | Total steps (for each participant) | Significant changes in gait speed and double support time during early phase, but gait variables did not significantly change during day 2–5. Visual Analog Scale (VAS) scores correlated with step count and cadence. |
| 13 | Sherman (2019, UK) [36] | Daily step count of British military males with bilateral lower limb amputations: A comparison of in-patient rehabilitation with the consecutive leave period between admissions | Determine whether mean daily step count changed between in-patient rehabilitation and consecutive leave periods. | n = 9(0); 26.0 ± 6.0; all bilateral TTA/TFA/Trans-Humeral (THA)/Trans-Radial (TRA)/KD; all trauma | Long-Term Activity Monitor (LAM2); prosthesis; 2 × 2 weeks | Steps per day | Step count decreased when away from rehabilitation. |
| 14 | Pepin (2019, USA) [37] | Correlation between functional ability and physical activity in individuals with transtibial amputations: A cross-sectional study | Investigate association between functional ability and PA. | n = 19(4); 59.6 ± 10.8; all TTA; 2 trauma, 17 non-traumatic | ActivPAL; thigh; 7 days | Steps per day; duration lying/sitting, standing (hours); duration stepping, walking (minutes) | Number of steps per day had a moderate to good correlation with the Amputee Mobility Predictor (AMP) and a fair correlation with the Timed Up and Go (TUG) and 2 Minute Walk Test (2MWT). |
| 15 | Musig (2019, Germany) [38] | Relation between the amount of daily activity and gait quality in transfemoral amputees | Examine kinematic variability during walking and the association with daily activity. | n = 15(1); 44.0 ± 9.0; 11 TFA, 4 KD; etiology N/A | VitaMove (Activ 8), prosthesis stem, 7 days | PA per day (min/day) | Significant correlation between daily activity and variability in the trunk and pelvis, and gait velocity. |
| 16 | Miller (2019, USA) [39] | Physical function and pre-amputation characteristics explain daily step count after dysvascular amputation | Identify factors that contribute to daily step count. | n = 58(3); 64.4 ± 9.0; 55 TTA, 3 other; all dysvascular | ActiGraph GT3X-BT; waist; 10 days | Steps per day; prosthetic wear time (minutes) | Physical function, cardiovascular disease, and pre-amputation walking time explained 62% of daily step count. |
| 17 | Klute (2019, USA) [40] | Daily step counts and use of activity monitors by individuals with lower-limb loss (conference abstract) | Observe and determine willingness to use smart activity monitors in daily life, and discover if self-monitoring increases PA levels. | n = 74(N/A); 52.0 ± 15.0; 56 TTA, 11 TFA, 1 KD; 42 trauma, 14 dysvascular, 18 other | Fitbit Zip; placement N/A; multi-year period (no specific duration reported) | Steps per day; habitual device use (%) | Self-monitoring of activity levels did not result in higher activity. Participants demonstrated habitual use approximately one quarter of the time. |
| 18 | Balkman (2019, USA) [41] | Prosthetists’ perceptions of information obtained from a lower limb prosthesis monitoring system: a pilot study | Assess prosthetists’ perceptions of prosthesis use and activity information obtained by a monitoring system. | n = 3(1); 50.1 ± 22.7; all TTA; 1 trauma, 2 dysvascular | Proximity sensor (WAFER) and 2 ActiGraph GT3X+; socket, thigh and ankle; 2 weeks | Prosthesis use (hours/day); time sitting, standing, walking (hours/day); times doffing prosthesis (for each participant) | Prosthetists over- and under-estimated patient activity, relative to monitored activity, and found features of multiple report formats clinically useful. |
| 19 | Sions (2018, USA) [42] | Self-reported functional mobility, balance confidence, and prosthetic use are associated with daily step counts among individuals with a unilateral transtibial amputation | Determine if functional mobility, balance confidence, and prosthetic use are associated with PA. | n = 47(16); 58.5 ± 12.0; all TTA; 20 infection, 16 trauma, 5 dysvascular, 2 cancer | StepWatch; prosthesis; 7 days | Steps per day | Self-reported functional mobility and balance confidence each explained 13% of the variance in step count, whereas prosthetic use explained 10%. |
| 20 | Sanders (2018, USA) [43] | Residual limb fluid volume change and volume accommodation: Relationships to activity and self-report outcomes in people with trans-tibial amputation | Examine how activities and self-report outcomes relate to daily changes in residual limb fluid volume and volume accommodation. | n = 29(5); 56.7 ± 14.8; all TTA; 20 trauma, 7 dysvascular, 2 congenital | ActiGraph GT3X-BT; prosthesis; 3 h | Time sitting, walking, standing, weight-bearing (sum of standing and walking), and prosthesis doffed (%) | Morning-to-afternoon percent limb fluid volume change per hour was not strongly correlated to percent time weight-bearing or to self-report outcomes. |
| 21 | Esposito (2018, USA) [44] | Daily step counts in Service Members with lower limb amputation (conference abstract) | Quantify PA in the months following amputation. | n = 27(N/A); 16 TTA, 7 TFA, 1 bilateral TTA, 3 bilateral TFA; etiology N/A | StepWatch 3; placement N/A; 7 days | Steps per day | Participants walked 3.142 ± 1.308 steps per day. No indications that step count increased farther along in the rehabilitative process. |
| 22 | Samuelsen (2017, USA) [45] | The impact of the immediate postoperative prosthesis on patient mobility and quality of life after transtibial amputation | Examine activity level and quality of life for patients receiving an immediate postoperative prosthesis. | n = 10(1); 58 (range 22–69); all TTA; all PVD | ActiGraph GT3X-BT; waist; 6 weeks | Cadence; time in sedentary, light activity, and moderate to vigorous activity (cutoff values 0–99, 100–2019, 2020–5998, and >5999, respectively) (%) | Participants spent 88% of their time sedentary, 11.5% in light, and 0.3% in moderate to vigorous activity level, and had low physical and emotional scores. |
| 23 | Juszczak (2017, USA) [46] | Developing an evidence based approach to address functional level changes in persons following amputation (conference abstract) | Incorporate ambulatory activity monitors (SAM) to collect objective functional mobility data to assess functional improvements during the rehabilitation and to improve prosthetic prescription. | n = 10(N/A); 53.2 ± 13.4; all TFA; etiology N/A | StepWatch; placement N/A; duration N/A | Steps per day; time moderate/intense level of ambulation (%) | Patients with higher K-level classification ambulated to a greater capacity, higher intensity, and for a sustained period of time compared to lower K-level. SAM may be effective for evaluating functional level change and assessing prosthetic needs. |
| 24 | Paxton (2017, USA) [47] | Physical activity, ambulation, and comorbidities in people with diabetes and lower-limb amputation | Characterize PA and its relation to physical function and comorbidities for diabetes and transtibial amputation (DM + AMP), diabetes without AMP (DM), and nondisabled adults. | n = 46(7) (22 with AMP); 62.3 ± 10.3; level N/A; all (22) dysvascular | ActiGraph GT3X-BT; waist; 10 days | Steps per day; time in sedentary, light, moderate, vigorous and very vigorous intensity (%) | Nondisabled group had more PA than DM, who performed more than DM + AMP. PA was related to physical function in DM and DM + AMP, but not to number of comorbidities. |
| 25 | Orendurff (2016,USA) [48] | Functional level assessment of individuals with transtibial limb loss: Evaluation in the clinical setting versus objective community ambulatory activity | Determine relationship between K-level determined in the clinic and K-level based on real world ambulatory activity. | n = 12(1); 57 ± 12; all TTA; etiology N/A | StepWatch; prosthesis; 7 days | Calculated K-level | Good agreement between the two methods of determining K-level. Clinic-based ambulatory capacity correlated with real-world ambulatory behavior. |
| 26 | Mandel (2016, Canada) [49] | Balance confidence and activity of community-dwelling patients with transtibial amputation | Examine relationship between balance confidence and community-based PA | n = 22(8); 61.4 ± 7.6; all TTA; 14 dysvascular/diabetes, 6 trauma, 2 cancer | StepWatch; prosthesis; 7 days | Steps per day; steps in frequency categories low (<16 steps/min), medium (16–40 steps/min), high (>40 steps/min) | Balance confidence was significantly lower among subjects with <3.000 steps/day. Balance confidence was significantly correlated with total steps. |
| 27 | Desveaux (2016, Canada) [50] | Physical activity in adults with diabetes following prosthetic rehabilitation | Determine if adults with diabetes and TTA meet PA guidelines, if PA is maintained post-rehabilitation and if physical functions are associated with PA. | n = 15(5); 61 ± 12; all TTA, all dysvascular | StepWatch; ankle intact limb; 9 days | Steps per day; weekly minutes of Moderate to Vigorous PA (>90 steps/min) (MVPA) | Participants took 3809 ± 2189 steps per day and 24 ± 41 weekly minutes of MVPA, below the guidelines. Outcomes remained stable post-rehabilitation. PA was correlated to 2MWT and gait speed. |
| 28 | Chu (2016, Hong Kong) [51] | Comparison of prosthetic outcomes between adolescent transtibial and transfemoral amputees after Sichuan earthquake using Step Activity Monitor and Prosthesis Evaluation Questionnaire | Investigate daily step activities and prosthesis-related quality of life amputees after the earthquake. | n = 21(5); 14.6 ± 2.3; 11 TTA, 10 TFA; all trauma | StepWatch; prosthesis; 3 months | Steps per day; duration low (<15 steps/min), medium (15–40 steps/min), high (>40 steps/min) (hours); peak activity index; endurance score; cardiovascular score; peak 5-min burst, peak 1–min burst | TTA had significantly higher step activity than TFA (4577 ± 849, 2551 ± 693, respectively). All participants showed daily wearing time > 12 h/day. Prosthesis Evaluation Questionnaire (PEQ) was not different between-groups. |
| 29 | Arch (2016, USA) [52] | Real-world walking performance of individuals with lower-limb amputation classified as Medicare functional Classification level 2 and 3 | Investigate outcomes of in-clinic performance-based evaluations and real-world walking performance measures. | n = 27(6); 56.8 ± 12.2; 20 TTA, 7 TFA, etiology N/A | Fitbit One; prosthetic ankle; 7 days | Total steps; total activity (minutes); activity in low (1–30 steps/min), moderate (>30–60 steps/min), high (>60 steps/min) activity (%) | K2 had significantly slower walking speed, shorter distance walked in 6 min, total step count and fewer active minutes than K3. |
| 30 | Kent (2015, USA) [53] | Step activity and stride-to-stride fluctuations are negatively correlated in individuals with transtibial amputation | Determine if increased stride-to-stride fluctuations correspond to a reduced level of activity. | n = 22(N/A); 52.0 ± 10.9; all TTA; 13 trauma, 5 diabetes, 2 dysvascular, 1 cancer, 1 infection | ActiGraph; pylon; 3 weeks | Steps per day | Increased stride-to-stride fluctuations were related to decreased activity levels. |
| 31 | Hordacre (2015, Australia) [54] | Community activity and participation are reduced in transtibial amputee fallers: A wearable technology study | Use wearable technology to assess activity and participation characteristics in the home and various community settings for fallers and non-fallers. | n = 47(11); 59.7 (range 19–98); all TTA; 18 PVD, 17 trauma, 11 other | StepWatch 3, QStarz BT-Q1000XT Global Positioning System (GPS); prosthesis; 7 days | Step count, number of visits, total steps and visits per community categories (employment, residential, commercial, health service, recreational, social, other); total steps at home | Fallers had significantly lower community activity levels and participation than non-fallers, specifically for recreational and commercial roles. |
| 32 | Parry (2014, USA) [55] | Gait outcome of pediatric lower extremity amputation patients with and without skin grafts (conference abstract) | Test hypothesis that lower extremity amputees with skin grafts on the amputation site had poorer function than those without skin grafts. | n = 13(N/A); 13.5 ± 4.6; level N/A, all trauma | Step Activity Monitor; placement N/A; 3 days | Steps per day | The two groups demonstrate comparable gait quality, gait efficiency, prosthetic use and self-reported functional ability. |
| 33 | Lin (2014, USA) [56] | Physical activity, functional capacity, and step variability during walking in people with lower-limb amputation | Explore relationship between PA and 6 Minute Walk Test (6MWT), step length variability, step width variability and Preferred Walking Speed (PWS) | n = 20(5); 50.6 ± 10.6; 12 TTA, 7 TFA, 1 KD; 12 trauma, 7 dysvascular, 1 other | Impulse model B-1 Pedometer; waist; 7 days | Steps per day | PA correlated strongly to PWS, 6MWT, and fairly to step width variability, but was inversely related to step length variability of both legs. |
| 34 | Hordacre (2014, Australia) [57] | Use of an activity monitor and GPS device to assess community activity and participation in transtibial amputees. | Assess ability to use wearable technology to measure community activity and participation, and determine if community activity and participation was different for predicted K-levels. | n = 46(N/A); 64.7 ± 13.8; all TTA; 19 trauma, 18 PVD, 9 other | StepWatch 3 and QStarz BT-Q1000XT GPS; prosthesis; 7 days | Step count, number of visits, total steps and visits per community categories (employment, residential, commercial, health service, recreational, social, other, home, lost in linkage, unidentified); total steps at home; community step count and visits per K-level (K1/2, K3, K4) | Participants completed on average 16.645 community steps and 16 visits over seven days. K1 and K2 had significant lower levels of community activity and participation than K3 and K4. |
| 35 | Halsne (2013, USA) [58] | Long-term activity in and among persons with transfemoral amputation | Study habitual activity in free-living environments, and explore relationships between Medicare Functional Classification Levels (MFCL) and performance. | n = 17(4); 49.1 ± 16.4; all TFA; 10 trauma, 3 malignancy, 1 dysfunction, 1 vascular, 1 infection | StepWatch; prosthesis; 12 months | Steps per day (for each participant); steps per day (sample mean); change in step count per season and per month (%) | Subjects took 1.540 steps per day, and activity increased with MFCL. Warmer seasons and months promoted higher activity, but peak temperatures and humidity depressed activity. |
| 36 | Highsmith (2012, USA) [59] | Spatiotemporal parameters and step activity of a specialized stepping pattern used by a transtibial amputee during a Denali mountaineering expedition | Describe spatiotemporal differences between the specialized French technique and traditional stepping and report step activity during a climbing expedition in Denali, AK, USA. | n = 1(0); 51; TTA; trauma | Sportline ThinQ XA Model 305 Pedometer; on a lanyard around the neck; 8 days | Steps per day; total step count; steps per technique (n, %) | The French technique had higher stride, step, and double support times than traditional stepping, but lower velocity and stride and step lengths. 27% of the steps were taken using the French technique. |
| 37 | Van den Berg-Emons (2010, The Netherlands) [60] | Accelerometry-based activity spectrum in persons with chronic physical conditions | Give an overview on the impact of chronic physical conditions on everyday PA and identify high-risk conditions, and compare objective activity levels with the levels estimated by rehabilitation physicians. | n = 18(1); 56 ± 13; all bilateral TTA; 9 trauma, 9 vascular | 5 ADXL202 uniaxial piezoresistive accelerometers; 2 thigh, 2 sternum, 1 wrist; 48 h | Duration physical activities (% of 24h-day); proportion of physical activities of able-bodied subjects (%) | Lowest activity levels were among vascular TTA, spinal cord injury, and myelomeningocele, less than 40% of the able-bodied level. Rehabilitation physicians considerably underestimated the magnitude of inactivity. |
| 38 | Parker (2010, Canada) [61] | Ambulation of people with lower-limb amputations: relationships between capacity and performance measures | Examine relationship between ambulation capacity and community performance, and explore what demographic and clinical variables influence ambulation performance. | n = 52(11); 55.2 ± 4.5; 30 TTA, 16 TFA, 6 bilateral TTA; 26 trauma, 20 vascular, 6 other | StepWatch 3; prosthetic ankle; 7 days | Steps per day; activity per day (minutes), time in low (1–30 steps/min), medium (>30–60 steps/min), high (>60 steps/min) activity (%); peak activity index (mean of highest 30 min steps/min) | 2MWT was significantly related to step activity measures and Trinity Amputation and Prosthesis Experiences Scales (TAPES). Depressive symptoms were a significant predictor of decreased performance. |
| 39 | Rosenbaum (2008, Germany) [62] | Physical activity levels after limb salvage surgery are not related to clinical scores—Objective activity assessment in 22 patients after malignant bone tumor treatment with modular prostheses | Assess PA levels with two objective measurement devices. | n = 22(8); 34.5 ± 18.4; 18 TFA, 4 TTA; all tumor | 3 DynaPort ADL (2 waist, 1 thigh), Step Activity Monitor (developer N/A); 7 days with SAM and 1st day with DynaPort | Steps per day; steps per weekday and weekend day (for each participant); duration intensity intervals 1–10, 11–20, 21–30, 31–40, 41–50, >50 steps/min (minutes and %); duration lying, sitting, standing, locomotion, undefined (%); movement intensity during walking (m/s2); physical activity index | Participants took 4.786 ± 1.770 steps per day. Sitting activity accounted for 54 ± 18% of the recorded time, followed by standing (27 ± 16%), locomotion (10 ± 6%) and lying (8 ± 6%). No correlation between clinical scores and step count measures. |
| 40 | Bussmann (2008, The Netherlands) [63] | Daily physical activity and heart rate response in people with a unilateral traumatic transtibial amputation | Investigate if people with unilateral traumatic TTA are less active than people without an amputation, and explore if both groups have a similar heart rate response while walking. | n = 9(0); 55.4 (range 21–73); all TTA; all trauma | 2 uniaxial, 1 biaxial ADX202 (TEMEC Instruments); 2 upper leg, 2 sternum; 2 days | Duration dynamic activities, walking, dynamic activities besides walking (%); sit-to-stand transitions (n); overall and walking body motility (g); resting heart rate; absolute heart rate during walking, normalized heart rate during walking (bpm); heart rate reserve (%) | Participants with amputation had lower percentage dynamic activities and body motility during walking than controls. No significant differences in heart rate and percentage heart rate reserve during walking. |
| 41 | Stepien (2007, Australia) [4] | Activity levels among lower-limb amputees: Self-report versus Step Activity Monitor | Determine the accuracy of self-reported activity. | n = 77(17); 60 ± 15; 54 TTA, 23 TFA; 39 trauma, 23 vascular, 15 other | StepWatch 3; prosthesis; 8 days | Steps per day; duration rest, low (1–15 steps/min), medium (16–40 steps/min), high (40+ steps/min) intensity activity (%) | Strong agreement between self-reported and measured activity between 9.00am–9:00pm for 34% of participants. Poor agreement between self-reported and measured time spent in various activity intensities. |
| 42 | Kanade (2006, UK) [64] | Risk of plantar ulceration in diabetic patients with single-leg amputation | Explore plantar loading of the surviving foot within a wider context of daily walking activity to investigate the precise risk to the surviving limb. | n = 21(2); 62.9 ± 6.2; all TTA; all diabetes | StepWatch (Prosthetic Research Study); prosthetic leg; 8 days | Steps per day; daily plantar cumulative stress (DPCS) (MPa/day) | The amputee group walked 30% slower, had reduced cadence, shorter strides and less steps per day than controls without amputation. |
| 43 | Kanade (2006, UK) [65] | Walking performance in people with diabetic neuropathy: benefits and threats | Evaluate walking activity on the basis of capacity, performance and potential risk of plantar injury. | n = 22(2); 62.9 ± 6.1; all TTA; all diabetes | StepWatch (Prosthetic Research Study); prosthetic leg; 8 days | Steps per day | Total heart beat index increased. Gait velocity and daily stride count fell with progression of foot complications. |
| 44 | Hopyan (2006, Australia) [66] | Function and upright time following limb salvage, amputation, and rotationplasty for pediatric sarcoma of bone | Determine the relative physical and psychosocial merits of limb-sparing reconstruction, above-knee amputation, and rotationplasty in survivors of childhood and adolescent lower extremity bone sarcoma. | n = 45(23) (20 with amputation); 26 ± 7; 19 TFA, 1 TTA; 20 limb salvage, 19 TFA, 5 rotationplasty, 1 TTA | Uptimer device; thigh; 24-h of weekend day | Uptime (%) | Uptime was highest in persons with rotationplasty, and similar between persons with limb-sparing reconstruction and above-knee amputation. |
| 45 | Bussmann (2004, The Netherlands) [67] | Daily physical activity and heart rate response in people with a unilateral transtibial amputation for vascular disease | Study the activity level and heart rate response, objectively measured during normal daily life. | n = 9(1); 55 (range 44–76); all TTA; all vascular | 2 uniaxial, 1 biaxial ADX202 (TEMEC Instruments); 2 upper leg, 1 sternum; 2 days | Duration dynamic activities, walking, (%); sit-to-stand transitions (n); overall and walking body motility (g); resting heart rate; absolute heart rate during walking; normalized heart rate during walking (bpm); percentage heart rate reserve (%) | Participants with amputation had lower activity levels and body motility during walking than controls. No differences in normalized heart rate during walking. |
| 46 | Coleman (1999, USA) [21] | Step activity monitor: long-term, continuous recording of ambulatory function | Provide guidelines for use of the Step Activity Monitor (SAM), and results of accuracy and reliability testing, and case study descriptions. | n = 2(1); age N/A; 2 TTA; etiology N/A | Step Activity Monitor (later StepWatch); ankle; 2 × 1 week | Total steps; duration inactivity (hours/day), low, moderate and high activity | SAM is accurate, reliable, and can be used to perform long-term step counting on a range of subjects. It is viable means for monitoring gait activity outside of the laboratory during normal daily activities. |
| Interventional studies | |||||||
| 1 | Vanicek (2021, UK) [68] | STEPFORWARD study: a randomized controlled feasibility trial of a self-aligning prosthetic ankle-foot for older patients with vascular-related amputations | Determine the feasibility of a Randomized Controlled Trial (RCT) of the effectiveness and cost-effectiveness of a self-aligning prosthetic ankle-foot compared with a standard prosthetic ankle-foot. | n = 55(8); 68.8 ± 9.6; all TTA; all non-traumatic (diabetes, PVD, blood clot, or other) | ActivPAL4; prosthesis; 2 × 1 week) | Steps per day; stepping (min/day) (baseline, final) | The consent, retention and completion rates demonstrate that it is feasible to recruit and retain participants to a future trial. |
| 2 | Kaluf (2021, USA) [69] | Hydraulic- and microprocessor-controlled ankle-foot prostheses for limited community ambulators with unilateral amputation: pilot study | Examine the benefit of hydraulic- and microprocessor-controlled prosthetic ankles. | n = 1(0); 58; TTA; trauma | StepWatch; prosthesis; 3 × 2 weeks | Steps per day; cadence; cadence variability; daily distance, stance/swing time; modus index; ambulation energy index; peak performance index | The four treatments had a varying level of benefits. The hydraulic ankle scored highest in patient-reported outcome measures and step activity data. |
| 3 | Kim (2021, USA) [70] | The influence of powered prostheses on user perspectives, metabolics and activity: a randomized crossover trial | Quantify differences between powered and unpowered prostheses and explore relationships between perceptions and functional outcomes in-lab and daily life. | n = 10(0); 52.6 ± 11.3; all TTA; 7 trauma, 3 vascular | 2 ActiGraph GT9X Link; prosthetic foot and pylon; 2 weeks | Steps per day; steps per day away from home; walking speed (m/s) | No universal benefits of the powered prosthesis. However, effect were subject-specific, and self-reported preferences did not often correlate with objective measures. |
| 4 | Sasaki (2020, Thailand) [71] | Sustainable development: a below-knee prostheses liner for resource limited environments (technical briefs) | Develop an affordable ethyl-vinyl-acetate roll-on (AERO) liner for resource-limited environments. | n = 1(0); 28; TTA; congenital | Omron HJ-329 Pedometer; prosthetic liner; 2 × 30 days | Steps per day | AERO liner results in increased comfort and speed, and slightly higher residuum temperature. Step count was similar to thermoplastic elastomer (TPE) liner. |
| 5 | Miyata (2020, Thailand) [72] | Sustainable, affordable and functional: reimagining prosthetic liners in resource limited environments | Evaluate function and performance of an affordable liner in three types of socket designs. | n = 5(2); 60.2 ± 7.4; all TTA; all trauma | Omron HJ-329 Pedometer; in pocket on prosthetic side; 2 × 30 days | Steps per day | AERO liner was suitable for use in both resource limited environments and developed settings standard of care prosthetic treatments. |
| 6 | Halsne (2020, USA) [73] | The effect of prosthetic foot stiffness on foot-ankle biomechanics and foot stiffness perception in people with transtibial amputation | Determine the effect of commercial prosthetic foot stiffness category on foot-ankle biomechanics, gait symmetry, community ambulation and relative foot stiffness perception. | n = 17(0); 51.0 ± 14.6; all TTA; 11 trauma, 3 dysvascular, 2 infection, 1 other | StepWatch 2; prosthesis; 3 × 2 weeks | Steps per day | Prosthetic foot stiffness category was significantly associated with changes in prosthetic foot-ankle biomechanics, but not with changes in gait symmetry, community ambulation and relative foot stiffness perception. |
| 7 | Gaunaurd (2020, USA) [74] | The effectiveness of the DoD/VA mobile device outcomes-based rehabilitation program (MDORP) for high functioning service members and veterans with lower limb amputation | Determine if the MDORP improved strength, mobility and gait quality. | n = 17(5); 39.5 ± 11.6; 12 TTA, 4 TFA/KD, 1 bilateral TTA; 14 trauma, 2 infection, 1 cancer | Rehabilitative Lower Limb Orthopedic Analysis Device (ReLOAD) with 5 IMUs; 2 on shank, 2 on thigh and 1 at the sacrum; 8 weeks | Decreased balance, decreased toe load, decreased knee flexion or no deviation (machine learning-derived classifier) (only reported for 1 exemplar participant). | Significant improvements in hip extensor strength, basic and high-level mobility, musculoskeletal endurance, and gait quality after 8–weeks MDORP. |
| 8 | Christiansen (2020, USA) [75] | Biobehavioral intervention targeting physical activity behavior change for older veterans after nontraumatic amputation: A randomized controlled trial | Test feasibility of a biobehavioral intervention designed to promote PA. | n = 31(0); 65.7 ± 7.6; 26 TTA, 5 TFA; all dysvascular | ActiGraph GT3X-BT; waist; 10 days | Steps per day | The intervention resulted in acceptable participant retention, low dose goal attainment, high participant acceptability, and low safety risk |
| 9 | Annis (2019, USA) [76] | Can improved prosthetic alignment increase activity level in patients with lower-extremity amputations? (conference abstract) | Determine if alterations in prosthetic alignment correlate with objective and subjective changes in activity level, function and pain and prosthetic satisfaction. | n = 9(1); age N/A; all TTA; 4 trauma, 4 dysvascular, 1 infection | FitBix Flex; prosthesis; 3 weeks | Steps per week | Smart pyramid-guided alignment showed less favorable functional outcomes; recommendations must be used in conjunction with current transtibial dynamic alignment protocols. |
| 10 | Littman (2019, USA) [77] | Pilot randomized trial of a telephone-delivered physical activity and weight management intervention for individuals with lower extremity amputation | Test feasibility, acceptability and safety of a weight management and PA intervention and obtain preliminary efficacy estimates for changes in weight, body composition, and physical functioning. | n = 15(4); 56.5 ± 11.0; 14 below knee (TTA or toe level), 1 above knee; 6 infection, 5 trauma, 1 cancer, 2 other | StepWatch; prosthesis; 2 × 7 days | Steps per day; sedentary time (hours/day) | Coached participants had greater decreases in waist circumference than the self-directed control group. The home-based intervention was promising in terms of efficacy, safety and acceptability. |
| 11 | Morgan (2018, USA) [78] | Laboratory- and community-based health outcomes in people with transtibial amputation using crossover and energy-storing prosthetic feet: A randomized crossover trial | Assess the effects of XF (crossover feet) and ESF (energy storing feet) on health outcomes. | n = 27(5); 42.3 ± 11.0; all TTA; 20 trauma, 2 infection, 1 cancer, 4 other | StepWatch; prosthesis; 2 × 4 weeks | Steps per day | XF users experienced improvements in mobility, fatigue, balance confidence, activity restrictions, and functional satisfaction, and exhibited longer sound steps compared to ESF. |
| 12 | McDonald (2018, USA) [79] | Energy expenditure in people with transtibial amputation walking with crossover and energy storing prosthetic feet: A randomized within-subject study | Compare energy expenditure at slow, comfortable, and fast walking speeds with XF (crossover feet) and ESF (energy storing feet). | n = 27(5); 42.3 ± 11.0; all TTA; 20 trauma, 2 infection, 1 cancer, 4 other | StepWatch; prosthetis; 2 × 4 weeks | Steps per day | Lower oxygen consumption with the XF compared to ESF at each self-selected walking speed, but this was not significant. |
| 13 | Kaufman (2018, USA) [80] | Functional assessment and satisfaction of transfemoral amputees with low mobility (FASTK2): A clinical trial of microprocessor-controlled vs. non-microprocessor-controlled knees | Determine if limited community ambulators would benefit from a microprocessor-controlled knee | n = 50(22); 69.0 ± 9.0; all TFA; 25 PVD, 13 infection, 5 trauma, 4 thrombosis, 2 cancer, 1 blood disorder | 4 ActiGraph GT3X+; waist, thigh and ankles; 4 days | Duration sitting, time up-right activity (%); gait entropy | Improved outcomes with a microprocessor-controlled knee, i.e. fall reduction, less time sitting, and increased activity level. Participants reported significantly improved ambulation, appearance, and utility. |
| 14 | Christiansen (2018, USA) [81] | Behavior-change intervention targeting physical function, walking, and disability after dysvascular amputation: A randomized controlled pilot trial | Determine preliminary efficacy of a home-based behavior-change intervention designed to promote exercise, walking activity, and disease self-management. | n = 38(3); 63.5; all TTA; all dysvascular | ActiGraph GT3X-BT; waist; 10 days | Steps per day; duration sedentary, light, and moderate/vigorous intensity (%) | The behavior-change intervention group showed within-group increase in daily step count, and had a higher increase in daily step count than the control group, demonstrating that the intervention might increase walking activity. |
| 15 | Wurdeman (2017, USA) [82] | Step activity and 6-Minute Walk Test outcomes when wearing low-activity or high-activity prosthetic feet | Determine changes in daily step count and 6MWT with Low-Activity feet (LA) and high-activity Energy-Storage-And-Return (ESAR) feet, and examine sensitivity of these measures to classify different feet. | n = 28(N/A); 53.6 ± 11.3; all TTA (4 bilateral); 16 trauma, 8 dysvascular/diabetes, 2 cancer, 2 infection | ActiGraph GT3X-BT; pylon; 2 × 3 weeks | Steps per day | Performance on the 6MWT and daily step counts were similar with the LA and ESAR foot. Correct classification for the 6MWT and step count were 51.9% and 61.5% for the ESAR, and 50% and 50% for the LA foot. |
| 16 | Sanders (2017, USA) [83] | Effects of socket size on metrics of socket fit in trans-tibial prosthesis users | Conduct a preliminary effort to identify quantitative metrics to distinguish a good socket from an oversized socket. | n = 9(2); 54.1 ± 15.9; all TTA; 6 trauma, 2 congenital, 1 infection | ActiGraph GT3X+; prosthesis; 2 × 4 weeks | Duration activity (hours/day) | Visual analysis showed largest effects for step time asymmetry, step width asymmetry, anterior and anterior-distal morning-to-afternoon fluid volume change, socket comfort scores, and self-reported utility, satisfaction, and residual limb health. |
| 17 | Imam (2017, Canada) [84] | A randomized controlled trial to evaluate the feasibility of the Wii Fit for improving walking in older adults with lower limb amputation | Assess the feasibility of Wii.n.Walk for improving walking capacity. | n = 28(10); median 62 (range 50–78); 15 TTA, 13 TFA/KD; 15 trauma, 12 dysvascular, 1 cancer | StepWatch, prosthesis; 3 × 1 week | Steps per day | Feasibility of the Wii.n.Walk showed a medium effect size for improving walking capacity. |
| 18 | Andrysek (2017, Chile) [85] | Long-term clinical evaluation of the automatic stance-phase lock-controlled prosthetic knee joint in young adults with unilateral above-knee amputation | Evaluate the Automatic Stance-Phase Lock (ASPL) knee mechanism against participants’ existing Weight-Activated Braking (WAB) prosthetic knee. | n = 10(4); 20.9 ± 3.1; all TFA; 5 disease, 4 trauma, 1 congenital | Power Walker EX-510; socket; duration N/A | Steps per week | Energy expenditure was lower for ASPL than WAB, but walking speed and step counts were similar. ASPL preference attributed to knee stability and improved walking, while limitations included noise. |
| 19 | Klute (2016, USA) [86] | Prosthesis management of residual-limb perspiration with subatmospheric vacuum pressure | Compare a Dynamic Air Exchange (DAE) prosthesis designed to expel accumulated perspiration with a total surface bearing Suction socket that cannot. | n = 5(N/A); 44 ± 15; all TTA; 3 trauma, 2 infection | StepWatch; placement N/A; 2 × 1 week | Steps per day | No difference in step activity levels, skin temperatures, and participants’ receptiveness between prostheses. |
| 20 | Highsmith (2016, USA) [87] | Effects of the Genium knee system on functional level, stair ambulation, perceptive and economic outcomes in transfemoral amputees | Determine if laboratory determined benefits of Genium are detectable using common clinical assessments and if there are economic benefits with its use. | n = 29(4); 46.5 ± 14.2; all TFA; 14 trauma, 4 malignancy, 2 dysvascular | StepWatch; prosthesis; 2 weeks | Galileo-derived K-level | Genium use improved stair walking, multi-directional stepping, functional level, and perceived function. Genium was preferred, and while more costly, the improvements may be worth funding. |
| 21 | Raschke (2015, USA) [88] | Biomechanical characteristics, patient preference and activity level with different prosthetic feet: A randomized double blind trial with laboratory and community testing | Measure sagittal moments during walking with three prosthetic feet categories: stiff, intermediate, and compliant forefoot stiffness. | n = 11(1); 57 ± 18; all TTA; etiology N/A | StepWatch; placement N/A; 3 × 7 days | Galileo-derived K-level | Participants preferred compliant stiffness. Compliant and intermediate feet had 15% lower maximum sagittal moments, but activity level was not significantly different between feet. |
| 22 | Hafner (2015, USA) [89] | Physical performance and self-report outcomes associated with use of passive, adaptive, and active prosthetic knees in persons with unilateral, transfemoral amputation: Randomized crossover trial | Assess and compare physical performance and self-reported outcomes of prosthetic knees with passive, adaptive, and active control. | n = 12(0); 58.8 ± 6.1; all TFA; 10 trauma, 2 tumor | StepWatch 3; prosthetic ankle; duration N/A | Steps per day | Adaptive control significantly improved comfortable TUG time and reported physical function compared to passive control. Active control significantly increased comfortable TUG, fast TUG, ramp times and balance confidence compared with passive control. |
| 23 | Segal (2014, USA) [90] | Does a torsion adapter improve functional mobility, pain, and fatigue in patients with transtibial amputation? | Explore effects of a torsion adapter on functional mobility and self-perceived pain and fatigue. | n = 10(1); 56 ± 12; all TTA; 5 trauma, 4 dysvascular/diabetes, 1 tumor | StepWatch 3; prosthetic pylon; 7 days | Steps per day; steps in low (<15 steps/min), medium (15–40 steps/min), high (>40 steps/min) intensity | Participants wearing a torsion adapter tended to take more low- and medium-intensity steps per day, and experienced less pain than with a rigid adapter. |
| 24 | Buis (2014, UK) [91] | Measuring the daily stepping activity of people with transtibial amputation using the ActivPAL™ activity monitor | Compare general activity during 1 week and detailed activity during 24 h period for Patellar Tendon-Bearing (PTB) and Total Surface Bearing (TSB) sockets. | n = 48(8); 55.3 ± 13.4; all TTA; 12 PVD, 36 other | ActivPAL; ankle; 6 days | Steps per day; duration walking (%); duration walking per prosthetic socket (%); mean cadence per prosthetic socket (%) | Despite differences in prosthetic socket design, activity levels were similar for both groups. |
| 25 | Theeven (2012, The Netherlands) [92] | Influence of advanced prosthetic knee joints on perceived performance and everyday life activity level of low-functional persons with a transfemoral amputation or knee disarticulation | Assess the effects of two types of Microprocessor-controlled Prosthetic Knee (MPK) joints on perceived performance and everyday life activity level. | n = 30(8); 59.1 ± 13.0; 24 TTA, 6 KD; 23 trauma, 6 vascular, 1 tumor | ActiGraph GT1M; waist; 3 × 1 week | Up-time (minutes); activity bouts during up-time (n); active-time (% of up-time); activity during up-time (n, for total group, and subgroups low, intermediate and high) | Participants report benefitting in their performance from using an MPK, but this was not reflected in the daily activity levels. |
| 26 | Gailey (2012, USA) [93] | Application of self-report and performance-based outcome measures to determine functional differences between four categories of prosthetic feet | Determine if self-report and performance-based measurements detect functional differences between four categories of prosthetic feet, and if differences exist between with and without PVD. | n = 10(1); 55.8 ± 4.1; all TTA; 5 PVD, 5 other | Step Activity Monitor (developer N/A); prosthetic ankle; 5 × 10–14 days | Steps per day; duration activity (hours/day) (for PVD and non-PVD) | Significant differences between PVD and non-PVD groups in Amputee Mobility Predictor (AMPRO) and 6MWT with the Proprio foot. AMPRO was significantly different between baseline and selected feet in PVD group. No differences in self-report measures, PEQ–13, Locomotor Capabilities Index (LCI), 6MWT and SAM. |
| 27 | Klute (2011, USA) [94] | Vacuum-assisted socket suspension compared with pin suspension for lower extremity amputees: effect on fit, activity, and limb volume | Investigate effect of a Vacuum-Assisted Socket Suspension system (VASS) as compared with pin suspension. | n = 5(N/A); 56 ± 9; all TTA; 4 trauma, 1 dysvascular | StepWatch 3; placement N/A; 2 × 2 weeks | Total steps | Activity levels and residual limb pistoning were significantly lower with VASS. Participants ranked residual limb health higher, were less frustrated and experienced easier ambulation with pin suspension compared to VASS. |
| 28 | Agrawal (2010, Germany) [95] | A comparison of gait kinetics between prosthetic feet during functional activities—symmetry in external work (SEW) approach (Ph.D. Thesis) | Determine gait differences among four prosthetic feet, using the Symmetry in External Work (SEW) approach. | n = 11(2); 54.8 ± 7.0; all TTA, 6 PVD; 4 trauma, 1 tumor | StepWatch; placement N/A; 4 × 10–14 days | Steps per day; duration low (1–15 steps/min), medium (16–40 steps/min), high (>40 steps/min) activity (hours); duration inactivity and activity (hours) | SEW were significantly different between the K3 foot and other feet during level walking and decline walking. No difference in steps or activity level. |
| 29 | Hafner (2007, USA) [96] | Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee | Evaluate differences in function, performance, and preference between mechanical and microprocessor prosthetic knee (C-leg) control technologies. | n = 17(4); 49.1 ± 16.4; all TFA; 10 trauma, 3 malignancy, 2 infection 1 vascular, 1 dysfunction, | StepWatch 2; placement N/A; 4 × 2 weeks | Steps per day; distance walked per day (meters/day) | Result showed improvements in stairs and hills, reduced frequency of stumbling and falling and a preference for the C-leg compared to the mechanical control prosthetic knee. |
| 30 | Darter (2007, USA) [97] | The effects of an integrated motor learning based treadmill mobility and aerobic exercise training program in persons with a transfemoral amputation (Ph.D. Thesis) | Investigate the effects of a home-based multiple speed treadmill exercise program. | n = 8(3); 41.4 ± 12.1; all TFA; all trauma/tumor | AMP 331 tri-axial activity monitor; prosthesis; 6 weeks | Steps per day; distance walked (meters/day); speed (meters/min/day) | Pre-training distance increased from 1.200 m/day to 1.537 m/day post-training. Steps per day increased from 2.639 pre-training to about 3.488 post-training. Speed changed little over the course of the training. |
| 31 | Klute (2006, USA) [98] | Prosthetic intervention effects on activity of lower-extremity amputees | Investigate the effect of prosthetic interventions on the functional mobility. | n = 12(N/A); 54 ± 6; all TTA; 7 trauma, 4 dysvascular, 1 infection | StepWatch 3; prosthetic ankle; 2 × 7 days | Steps per day; duration activity (minutes/weekdays, weekend days and all days); figure including number of bouts (dots), bout duration (x-axis) and cadence (y-axis) | Pylon type and knee type had no effect on daily activity level or activity duration. |
| 32 | Hsu (2006, Taiwan) [99] | The effects of prosthetic foot design on physiologic measurements, self-selected walking velocity, and physical activity in people with transtibial amputation | Investigate the physiologic differences during multispeed treadmill walking and PA profiles for the Otto Bock C-Walk foot (C-walk), Flex-Foot, and Solid Ankle Cushion Heel (SACH) foot. | n = 8(0); 36 ± 15; all TTA; all trauma | Yamax Digiwalker Pedometer; iliac crest of amputation side; 1 month | Steps per day | C-walk had a trend of improved physiologic responses compared with the SACH. Flex-Foot showed significantly lower percentage of age-predicted maximum heart rate and RPE values compared to C-Walk and SACH. |
| 33 | Berge (2005, USA) [100] | Efficacy of shock-absorbing versus rigid pylons for impact reduction in transtibial amputees based on laboratory, field, and outcome metrics | Compare Shock-Absorbing Pylons (SAPs) with a conventional rigid pylon, assess effect on gait mechanics, measure transmitted accelerations in situ, and determine functional outcomes using step counts and questionnaires. | n = 15(0); 51 ± 9; all TTA; 10 trauma, 4 dysvascular, 1 infection | StepsWatch 2; prosthetic ankle; 2 × 1 week | Steps per week | The only significant difference was for the prosthetic-side knee angle at initial contact, which was higher with the rigid pylon than the SAP while walking a controlled speed, suggesting SAP is as effective as rigid pylon. |
| 34 | Coleman (2004, USA) [101] | Quantification of prosthetic outcomes: Elastomeric gel liner with locking pin suspension versus polyethylene foam liner with neoprene sleeve suspension | Compare transtibial socket suspension systems: the Alpha liner with distal locking pin and the Pe-Lite liner with neoprene suspension sleeve. | n = 13(3); 49.4 ± 9.6; all TTA; all trauma | StepWatch; prosthetic ankle; 2 × 2 weeks | Steps per day; duration inactivity, low, moderate, high (>30 steps/min) intensity activity (hours/day); distribution low, moderate, high intensity of active time (%); socket wear time (hours/day) | Participants spent 82% more time wearing the Pe-Lite and took 83% more steps per day. Ambulatory intensity distribution and questionnaire results were not different between sockets. |
| Algorithm/method development studies | |||||||
| 1 | Srisuwan (2021, USA) [102] | Locomotor activities of individuals with lower-limb amputation | Describe a novel method for activity monitoring and use it to identify step count distribution of locomotor activities in the home, work, and community environments. | n = 10(0); 48.7 ± 17.0; all TTA; 8 trauma, 2 diabetes | Custom instrument including ADXL345 triaxial accelerometer and L3G4200D triaxial rate gyroscope; prosthetic pylon; 34.7 ± 13 h | Total number of steps; steps per activity classifications straight, turn right/left, stair up/down, ramp up/down, turn prosthetic leg/nonamputated leg inside | The method can be used to accurately classify locomotor activities in home, work, and community environments. |
| 2 | Jamieson (2021, UK) [103] | Human activity recognition of individuals with lower limb amputation in free-living conditions: A pilot study | Investigate the implementation of supervised classifiers and a neural network for the recognition of activities. | n = 4(1); 50 ± 7.7; 3 TTA, 1 bilateral TTA; 3 trauma, 1 vascular | ActivPAL4+; chest-mounted camera, GPS on iPhone 6; thigh; 7 days | 5-Fold accuracy per model (%); 5-Fold accuracy per level label (%); F1 scores per level label resolution; Leave One Subject Out (LOSO) accuracy (%, for each participant); confusion matrices (per level label resolution and model) | The models Support Vector Machine (SVM) and Long Short-Term Memory Network (LSTM) showed 77–78% classification accuracy, but fell with increased label detail. Classifiers trained on individuals without gait impairment could not recognize activities carried out by LLAs. |
| 3 | Griffiths (2021, UK) [104] | A machine learning classification model for monitoring the daily physical behavior of lower-limb amputees | Develop a model capable of accurately classifying lower-limb amputee postures by using data from a single shank-worn accelerometer. | n = 1(N/A); age N/A; bilateral TFA; etiology N/A | 2 ActivPAL PAL3; thigh and shank; 7 days | F-scores and confusion matrices for 8 models and 4 posture classes (sitting, standing, stepping, lying) | A random forest classifier with 15–s window length provided a 93% weighted average F-score accuracy, and between 88 and 98% classification accuracy across four posture classes. |
| 4 | Kim (2020, USA) [105] | Wearable sensors quantify mobility in people with lower limb amputation during daily life | Explore the clinical viability of using wearable sensors to characterize functional mobility. | n = 17(2); 47.9 ± 14.5; 16 TTA, 1 bilateral TTA & TFA; 10 trauma, 6 dysvascular, 1 congenital | 2 ActiGraph GR9X Link and GPS enabled smartphone; ankle and foot on prosthesis; 2 weeks | Steps per day; steps per bout; stride length (meters), home and away from home; total IMU straight-line walking strides (with successful GPS match); cadence (strides/min); walking speed (m/s) | Functional capacity measured in the lab was not reflected in routine walking during daily life. This approach can be used to aid in prosthetic prescription or in the assessment of interventions. |
| 5 | Weathersby (2018, USA) [106] | Development of a magnetic composite material for measurement of residual limb displacements in prosthetic sockets | Design and evaluate a novel wearable inductive sensor system for long-term measurements of limb-socket displacements. | n = 2(0); age N/A; all TTA; all trauma | Custom sensor design including chip, antenna, capacitor and sheath with embedded magnetic particles; liner; 2 and 4 weeks | Signal loss per test location (%) | Field testing demonstrated less than 3% signal degradation after four weeks; the developed sensor meets durability and performance needs and is ready for large-scale clinical testing. |
| 6 | Swanson (2018, USA) [107] | Instrumented socket inserts for sensing interaction at the limb-socket interface | Investigate a strategy for designing and fabricating computer-manufactured socket inserts with sensors that measure limb-socket interactions. | n = 1(0); 74; TTA; trauma | Custom sensor design including proximity, force sensing resistor and inductive sensor; socket; 2 days | Sensor change (proximity (a.u. × 104, distance (mm); pressure (kPa)); change in sensor behavior (yes, no, minimal) | Multiple sensor types were necessary in analysis of field collected data to interpret how sock changes affected limb-socket interactions. |
| 7 | Arch (2017, USA) [108] | Method to quantify cadence variability of individuals with lower-limb amputation | Develop and demonstrate feasibility of a method to quantify real-world cadence variability. | n = 27(6); 56.8 ± 12.2; 20 TTA, 7 TFA; etiology N/A | Fitbit One; prosthesis; 7 days | Average cadence; maximum cadence (steps/min); cadence variability scale parameter; cadence variability (Weibul probability density) | K2 walked with significantly less cadence variability than K3. The method was able to differentiate cadence characteristics between K2 and K3 ambulators. |
| 8 | Gardner (2016, USA) [109] | Monitoring prosthesis user activity and doffing using an activity monitor and proximity sensors | Develop a method to incorporate doffing and donning information into activity characterization. | n = 23(N/A); 55.6 ± 14.9; all TTA; etiology N/A | 2 Actigraph GT3X+ (prosthesis, thigh); 2 proximity sensors (socket brim); 3 h | Doffing, sitting, standing and walking (n) | Detected activities matched participants’ descriptions of activities well, of which 95% of doffs were detected, making the developed technology relevant to use. |
| 9 | Jayaraman (2014, USA) [110] | Global position sensing and step activity as outcome measures of community mobility and social interaction for an individual with a transfemoral amputation due to dysvascular disease | Examine the combined use of GPS and a step activity monitor to quantify community mobility and social interaction. | n = 1(1); 76; TFA; dysvascular | StepWatch 3.1 and GPS (Travel Recorder XT); placement N/A; 1 month | Steps per day; steps per day at home; steps per day outside of home; duration at community locations (commercial, religious, other residential, open space, mixed use), and at home (hours and minutes); trips (n, car, wheelchair, walking, and undetermined trips) | GPS and step activity monitor provided quantitative details on the patient’s steps taken in and out of the home, wheelchair use, prosthesis use, driving trips, and time spent on social and community trips. |
| 10 | Redfield (2013, USA) [111] | Classifying prosthetic use via accelerometry in persons with trans-tibial amputations | Classify the movements and body postures by using commercially-available accelerometers and a custom software algorithm. | n = 8(2); 53.0 ± 11.6; all TTA; 8 trauma, 1 infection, 1 tumor | 2 ActiGraph GT3X+; prosthesis and thigh; 2 days | Agreement between activity classifications (doffed, sitting, standing, active) (%) | The classifier achieved a mean accuracy of 96.6%. |
| 11 | Frossard (2011, Australia) [112] | Categorization of activities of daily living of lower limb amputees during short-term use of a portable kinetic recording system: A preliminary study | Determine the relevance of the categorization of the load regime data to assess the functional output and prosthetic use. | n = 1(0); 33; TFA; etiology N/A | Custom instrument, including multiaxial transducer; prosthesis; 5 h | Number of steps; cadence; activity categories directional locomotion, localized locomotion, stationary loading, inactivity (n, hours, %); duration gait cycle, swing and support phases (seconds); forces (N), moments (Nm), impulse (kN·s) along anteroposterior, mediolateral and long axis (per activity category) | The proposed categorization and apparatus have the potential to complement conventional instrument, particularly for difficult cases. |
| 12 | Frossard (2008, Australia) [113] | Monitoring of the load regime applied on the osseointegrated fixation of a trans-femoral amputee: A tool for evidence-based practice | Describe the continuous recording of the true load regime experienced during daily living by the abutment of a transfemoral amputee fitted with an osseointegrated fixation. | n = 1(0); 33; TFA; etiology N/A | Set Activity Monitor Pedometer, and custom instrument, including multiaxial transducer; prosthesis; 5 h | Number of steps; cadence; duration gait cycle, swing and support phases (seconds); activity and inactivity (%); forces (N) and moments (Nm) on the anteroposterior, mediolateral and long axes of the abutment | The overall load profile presented variable length of inactivity (64%) and activity (36%). The maximum load applied on the mediolateral, anteroposterior, and the long axes represented 21%, 21% and 120% of the body weight, respectively. |
| Validity/Feasibility studies | |||||||
| 1 | Godfrey (2018, USA) [114] | The accuracy and validity of Modus Trex Activity Monitor in determining functional level in veterans with transtibial amputations | Investigate the accuracy and reliability of Modus Trex-derived K-level to differentiate between Medicare Functional Classification levels (K-levels). | n = 27(0); 60.5 ± 18.6; all TTA; 13 trauma, 11 dysvascular, 3 other | StepWatch and GPS device; prosthesis; 2 weeks | Steps per day; peak cadence; Modus Trex-derived K-level and Modified Clinical K-level | The Modus Trex-derived K-level correlated most strongly with the MCK-levels. |
| 2 | Arch (2018, USA) [115] | Step count accuracy of StepWatch and FitBit One among individuals with a unilateral transtibial amputation | Evaluate the step count accuracy of both monitors during forward-linear and complex walking and compare monitor step counts in the free-living environment. | n = 50(N/A); age N/A; all TTA; etiology N/A | StepWatch and Fitbit One; prosthesis; 7 days | Total steps (for each participant) | Both monitors accurately counted steps during forward linear walking, StepWatch was more accurate than FitBit during complex walking, and FitBit counted fewer steps than StepWatch during free-living walking. |
| 3 | Orendurff (2016, USA) [116] | Comparison of a computerized algorithm and prosthetists’ judgment in rating functional levels based on daily step activity in transtibial amputees | Compare prosthetists’ ratings of functional levels based on a visual inspection of step activity patterns with the ratings calculated by the computerized algorithm based on the same step activity. | n = 14(N/A); age N/A; all TTA; etiology N/A | StepWatch; placement N/A; 5–7 days | Calculated K-level; prosthetists’ rating of K-level | The computerized algorithm produced functional level closely matched the average of the rating by the 14 experienced prosthetists. |
| 4 | Albert (2014, USA) [117] | Monitoring daily function in persons with transfemoral amputations using a commercial activity monitor: A feasibility study | Assess mobility using data collected from a popular, consumer-oriented activity monitor Fitbit. | n = 9(4); 53 ± 12; all TFA; 6 trauma, 2 vascular, 1 cancer | Fitbit One; waist; 7 days | Steps per day; duration lightly active, fairly active, very active (%); duration total daily activity (%); calories; Fitbit activity score; miles walked; floors climbed (n) | Fitbit results correlate with K-level, and Fitbit activity score is independent of variations in age, weight, and height compared with estimated calories. |
| 5 | Albert (2013, USA) [118] | Monitoring functional capability of individuals with lower limb amputations using mobile phones | Provide evidence that accelerometry using mobile phones can be used to objectively quantify activity levels. | n = 10(5); 53.1 ± 11.9; all TFA; 7 trauma, 2 dysvascular, 1 cancer | Mobile phone; in belt in center of the back; 7 days | Duration low (0.1–0.5 m/s2), medium (0.5–1.0 m/s2), high (1.0+ m/s2) activity | K-level was correlated to the proportion of moderate to high activity, which suggests that mobile phones can be used to evaluate real world activity for mobility assessment. |
| 6 | Van Dam (2001, The Netherlands) [119] | Measuring physical activity in patients after surgery for a malignant tumour in the leg. The reliability and validity of a continuous ambulatory activity monitor | Investigate reliability and validity of an ambulatory activity monitor in measuring the intensity of PA in patients who underwent radical surgery for a malignant tumour in the femur or tibia. | n = 20(10) (8 with amputation); 49 (median, range 18–69); 3 TFA, 3 KD, 2 rotationplasty; all tumor | 3 Dynaport ADL; 2 waist and 1 thigh; 2 × at least 24 h. | Duration walking, standing, sitting (%); movement intensity of walking, standing, sitting (m/s2); test-rest reliability (ICC values) | Reliability was satisfactory, with intraclass correlation coefficients ranging from 0.65 to 0.91. |
| Study Design | No. of Studies | Step Count | Fitness/ Intensity Activity | Type Activity/ Posture | Commercial Scores | Prosthetic Use/Fit | Gait Quality | GPS | Accuracy |
|---|---|---|---|---|---|---|---|---|---|
| Observational | 46 | 36 (78) | 15 (33) | 12 (26) | 4 (9) | 6 (13) | 1 (2) | 2 (4) | 0 |
| Interventional | 34 | 28 (82) | 8 (24) | 9 (26) | 7 (21) | 2 (6) | 3 (9) | 1 (3) | 0 |
| Algorithm/method development | 12 | 5 (42) | 3 (25) | 4 (33) | 1 (8) | 3 (25) | 3 (25) | 1 (8) | 3 (25) |
| Validity/Feasibility | 6 | 3 (50) | 4 (67) | 1 (17) | 3 (50) | 0 | 0 | 1 (17) | 1 (17) |
| Total | 98 | 72 (73) | 30 (31) | 26 (27) | 15 (15) | 11 (11) | 7 (7) | 5 (5) | 4 (4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mellema, M.; Gjøvaag, T. Reported Outcome Measures in Studies of Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review. Sensors 2022, 22, 2243. https://doi.org/10.3390/s22062243
Mellema M, Gjøvaag T. Reported Outcome Measures in Studies of Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review. Sensors. 2022; 22(6):2243. https://doi.org/10.3390/s22062243
Chicago/Turabian StyleMellema, Mirjam, and Terje Gjøvaag. 2022. "Reported Outcome Measures in Studies of Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review" Sensors 22, no. 6: 2243. https://doi.org/10.3390/s22062243
APA StyleMellema, M., & Gjøvaag, T. (2022). Reported Outcome Measures in Studies of Real-World Ambulation in People with a Lower Limb Amputation: A Scoping Review. Sensors, 22(6), 2243. https://doi.org/10.3390/s22062243