
Open-Ended Transmission Coaxial Probes for Sarcopenia Assessment

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
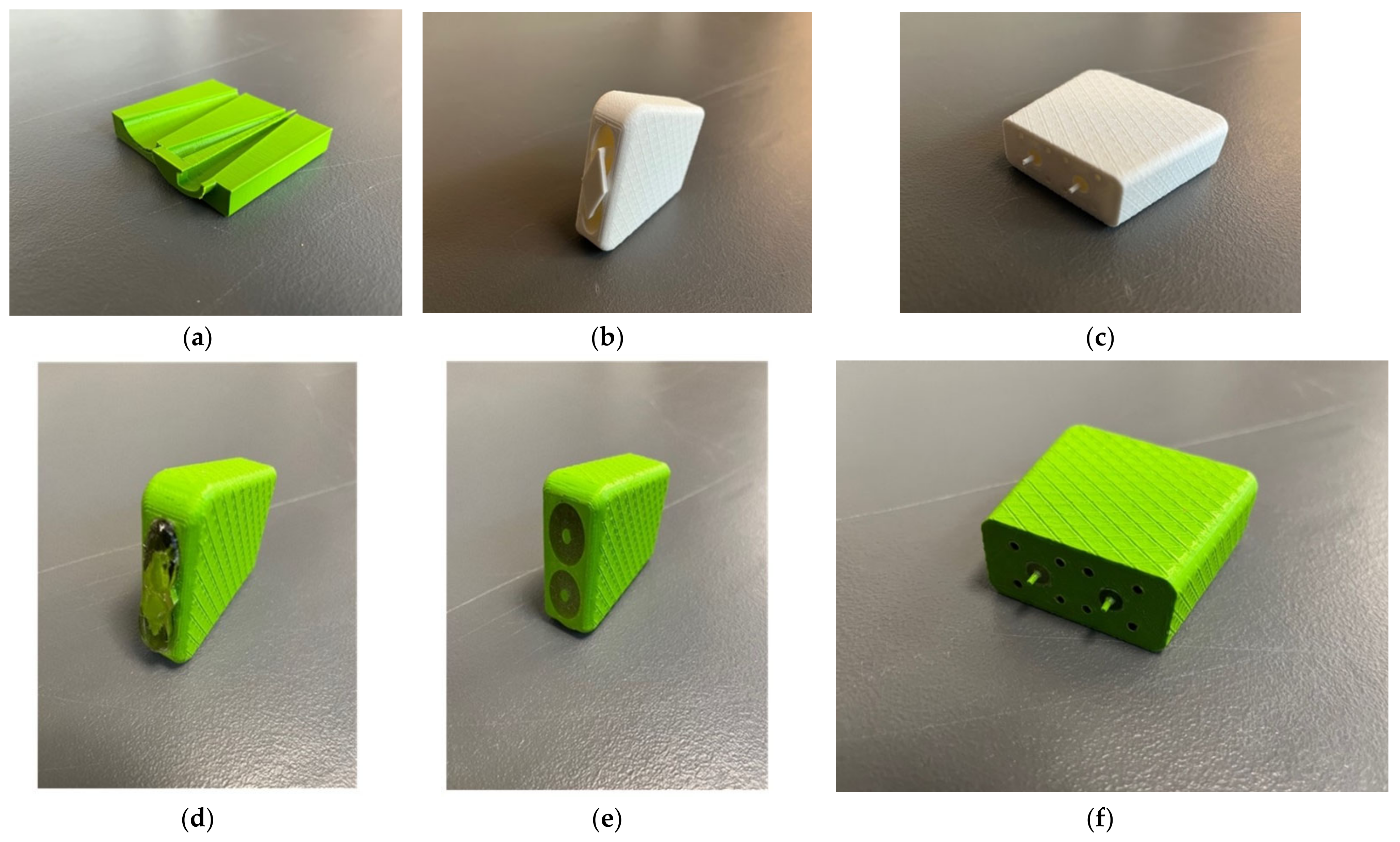
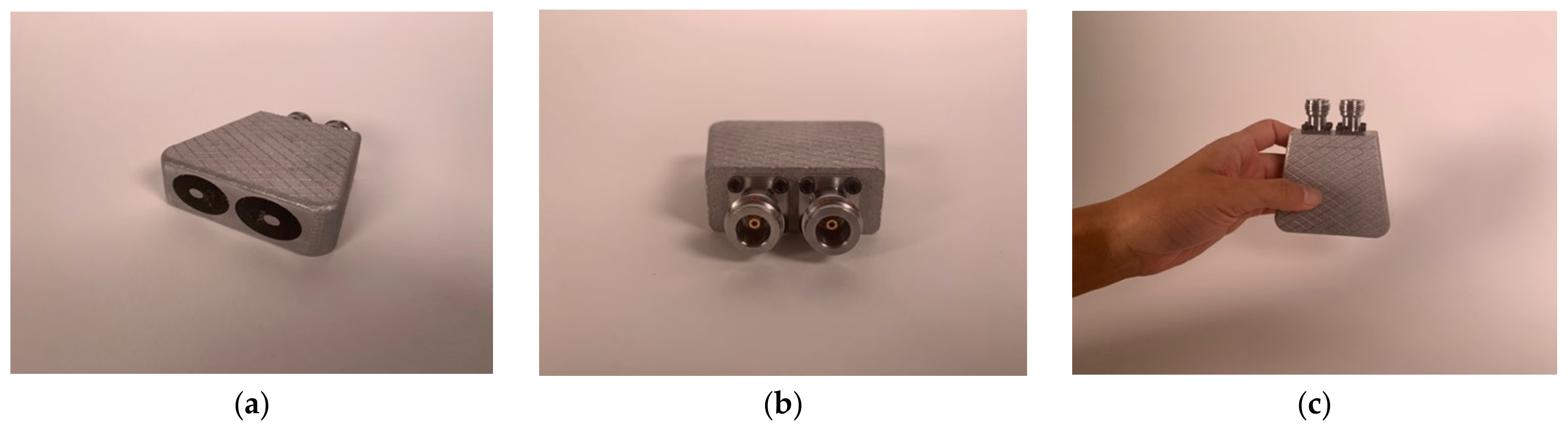
2.1. Transducer Fabrication
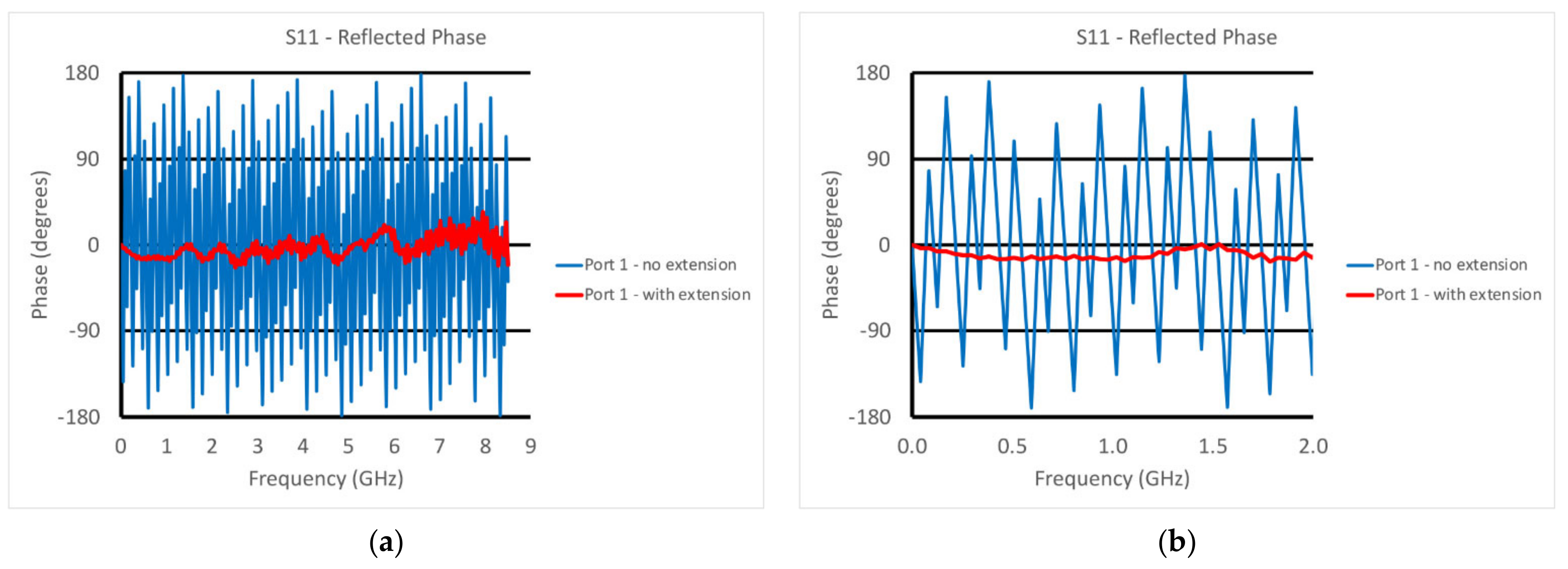
2.2. Reference Plane Calibration
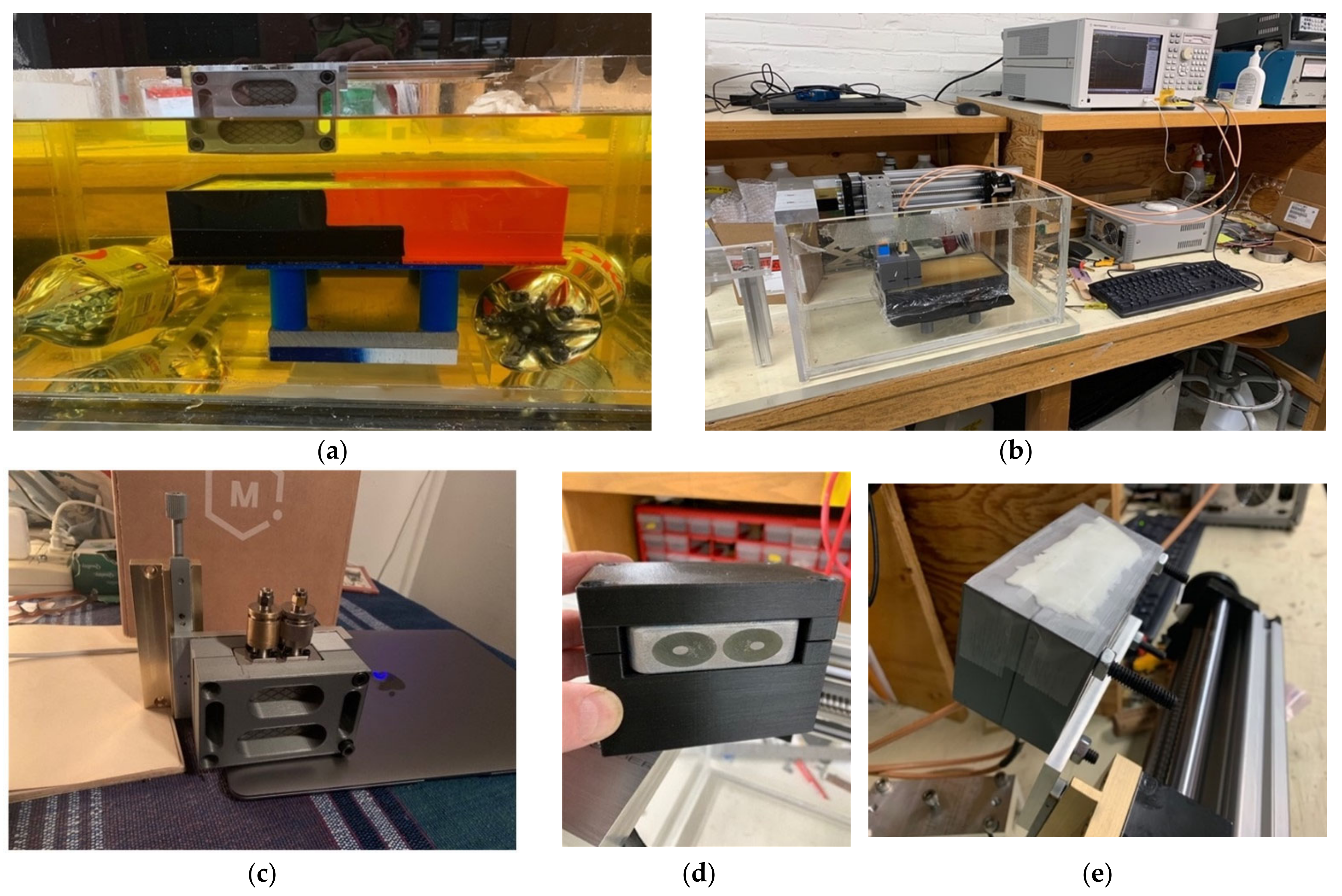
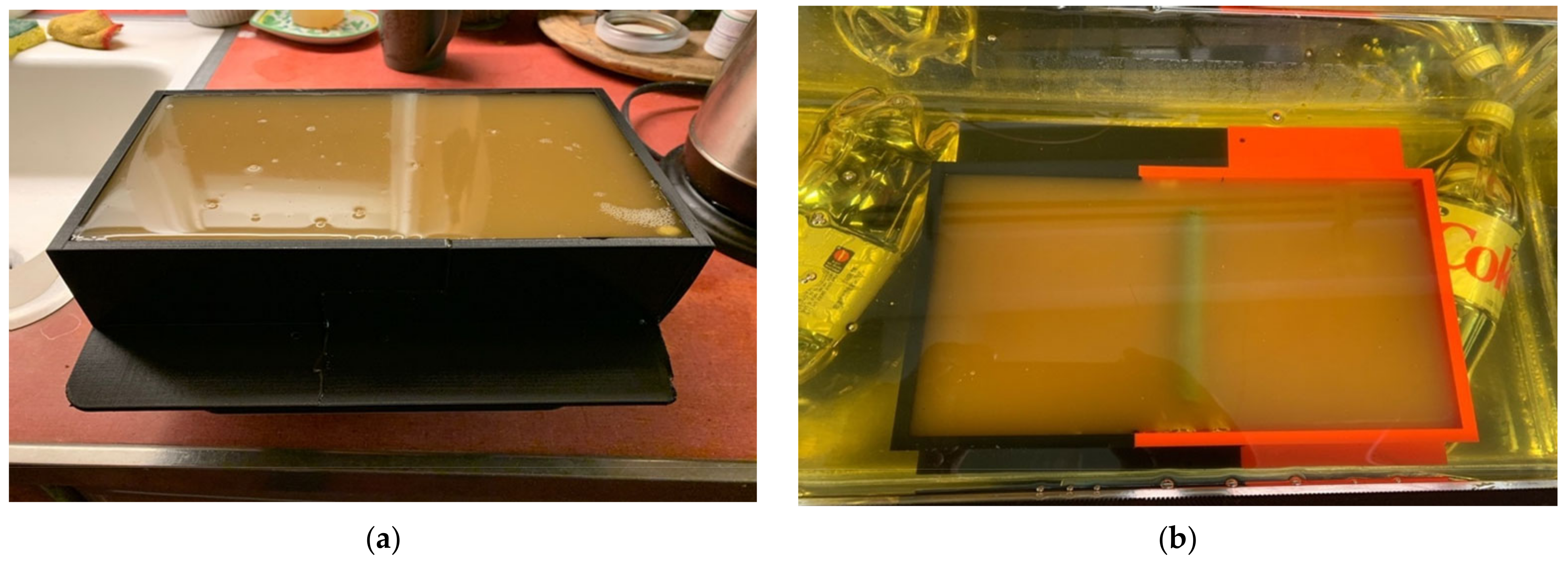
2.3. Phantom Experiments
3. Results
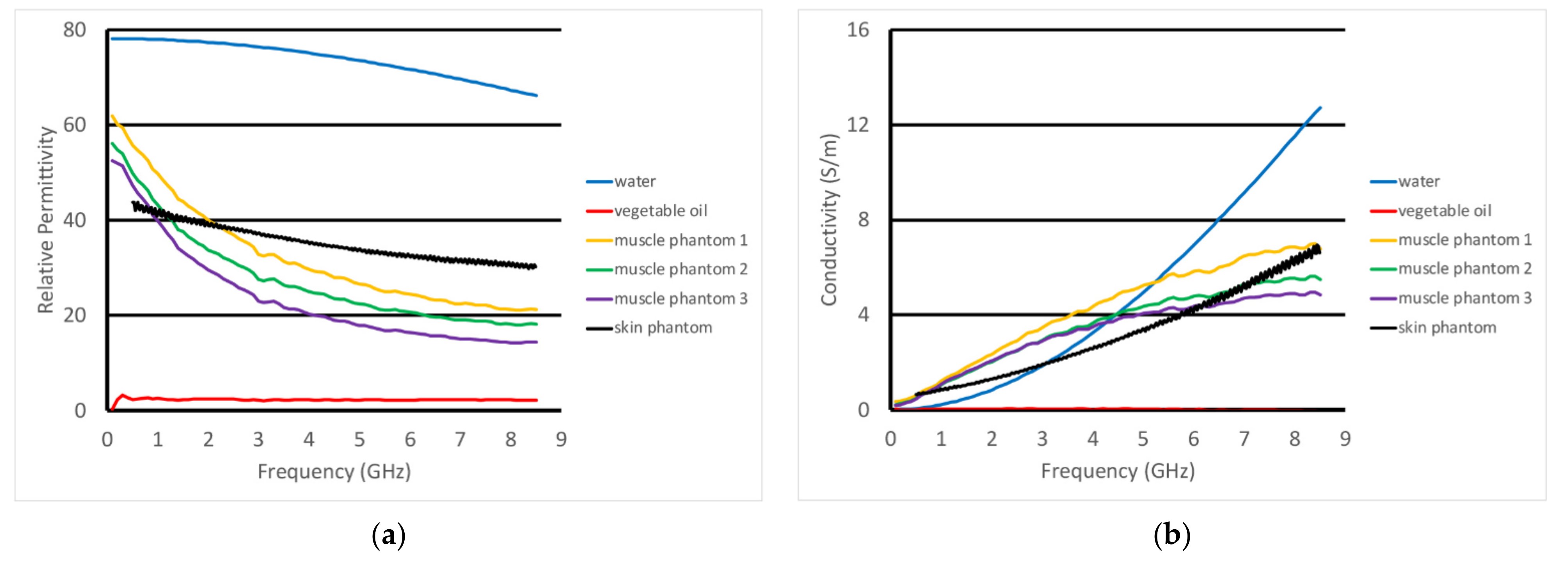
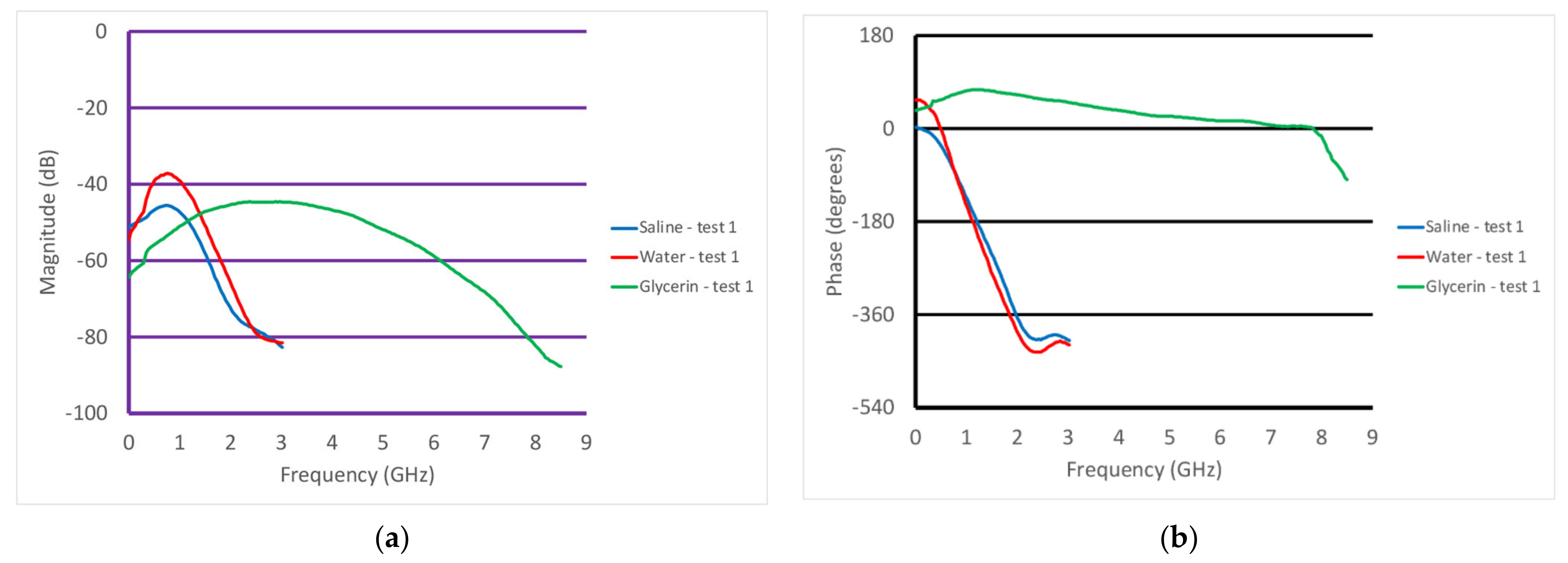
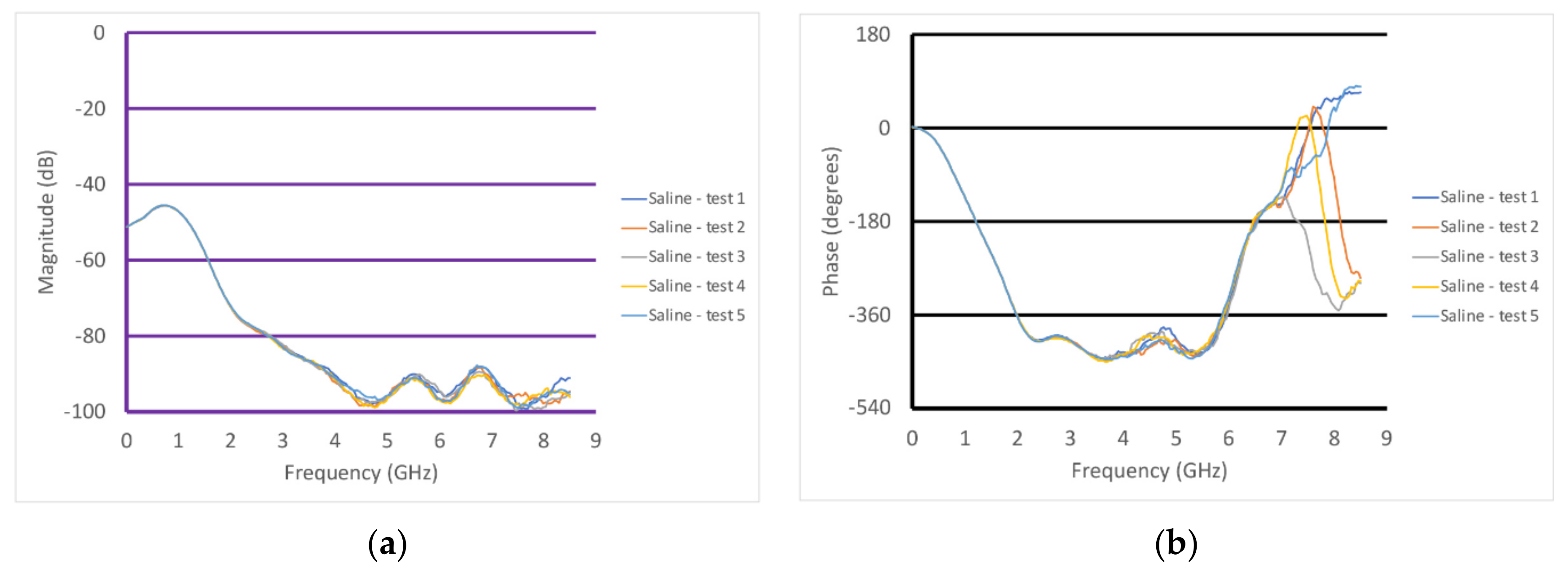
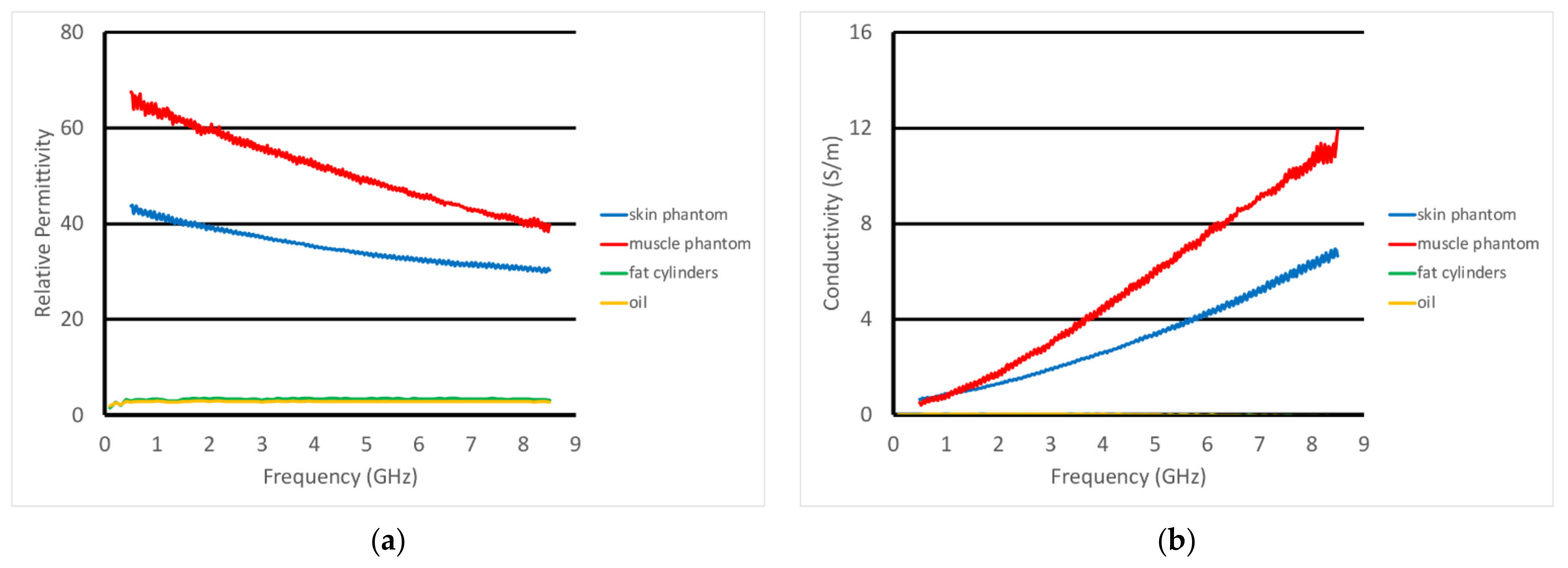
3.1. Homogeneous Liquid Tests
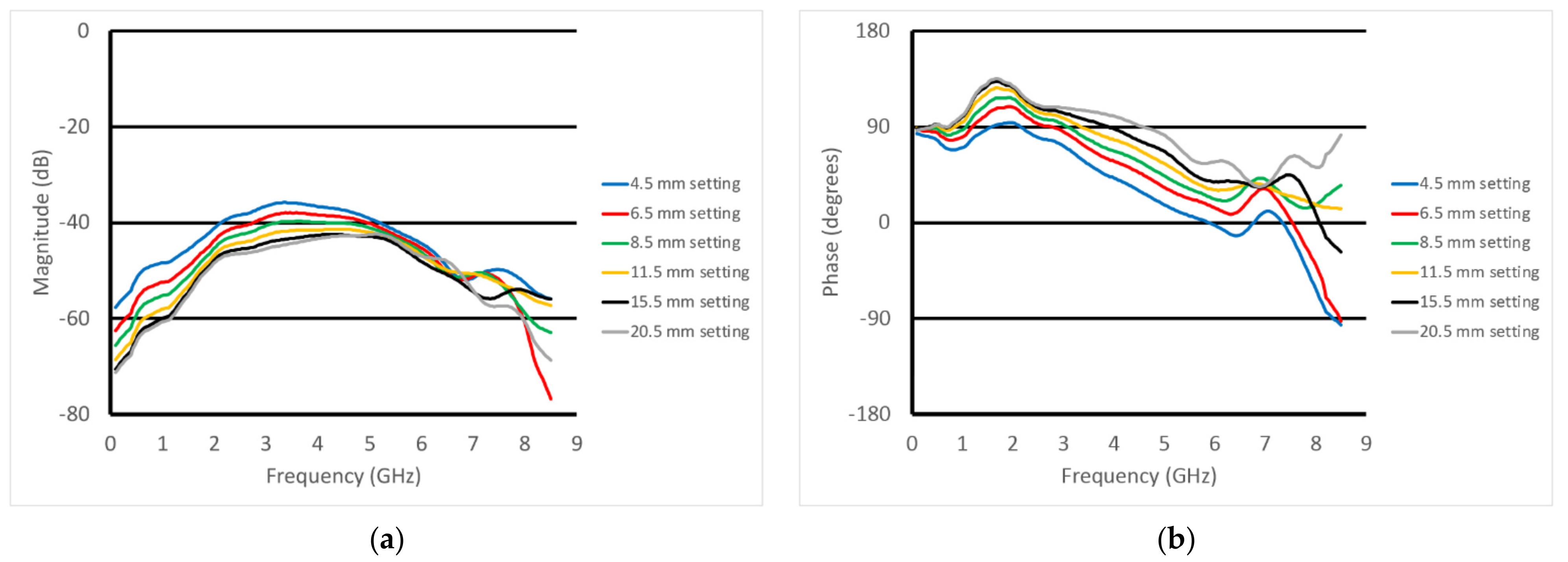
3.2. Homogeneous Muscle Phantom Tests
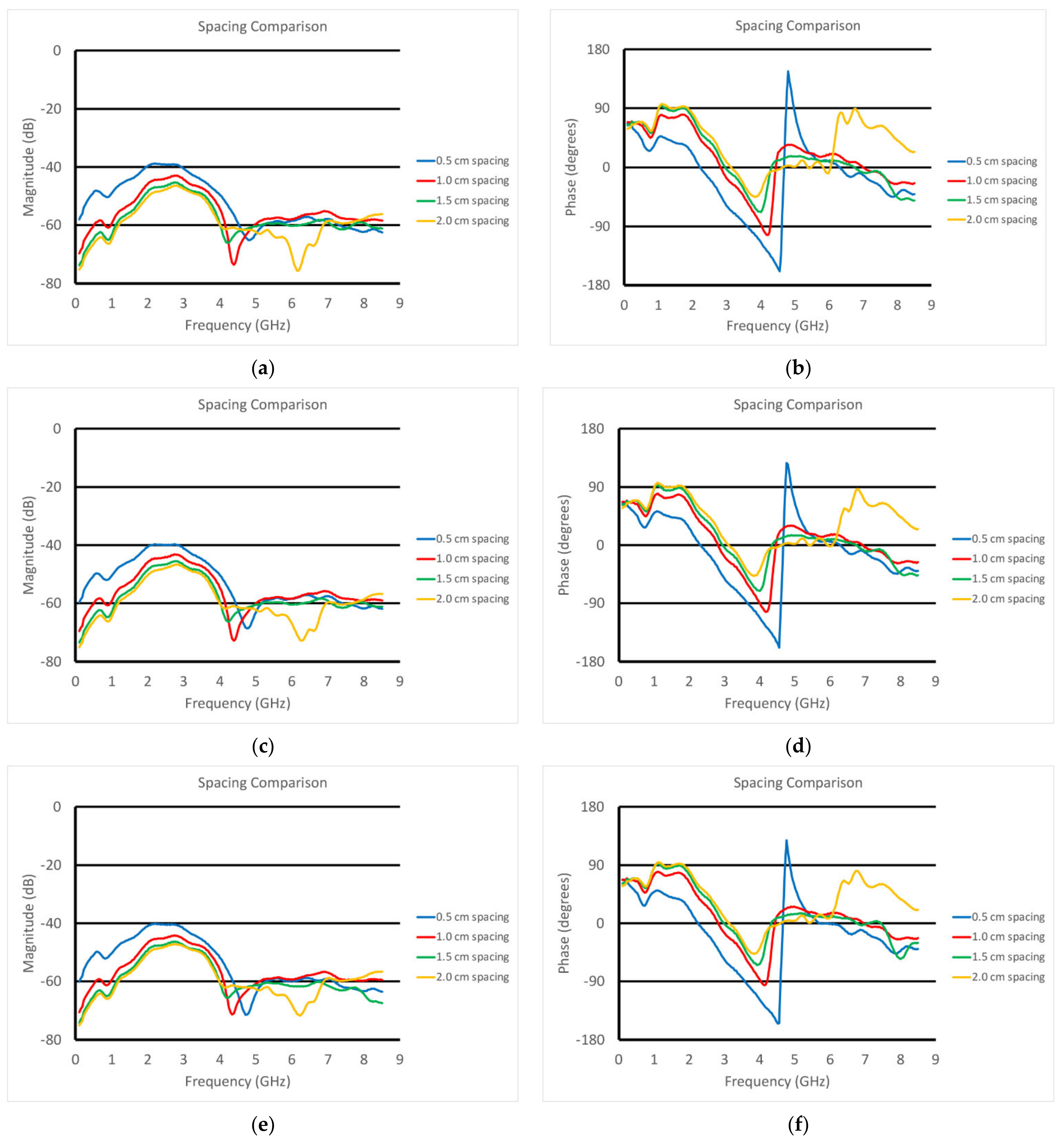
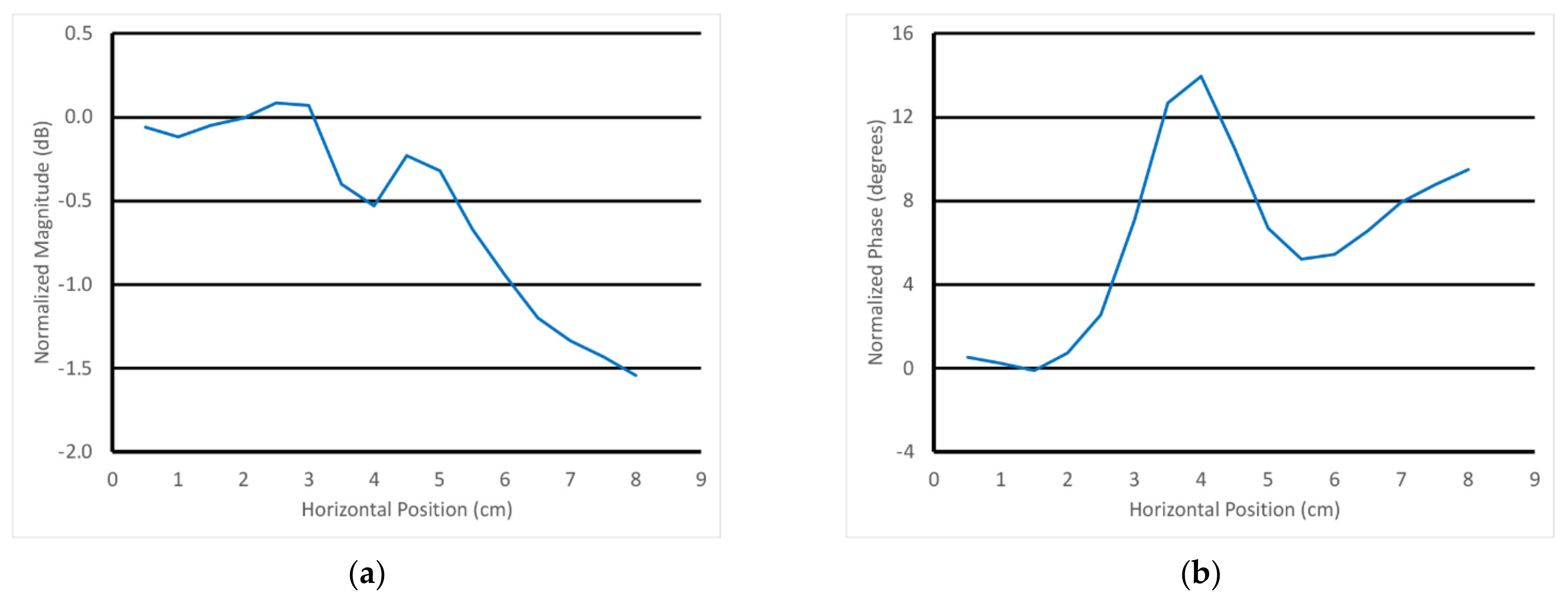
3.3. Inhomogeneous Muscle Phantom Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Orav, J.E.; Kanis, J.A.; Rizzoli, R.; Schlögl, M.; Staehelin, H.B.; Willett, W.C.; Dawson-Hughes, B. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos. Int. 2015, 26, 2793–2802. [Google Scholar] [CrossRef]
- Schaap, L.A.; Van Schoor, N.M.; Lips, P.; Visser, M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The longitudinal aging study Amsterdam. J. Gerentol. Ser. A 2018, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, R.J.S.; Hasni, S. Pathogenesis and Management of Sarcopenia. Clin. Geriatr. Med. 2017, 33, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Shen, Y.; Tan, L.; Li, W. Prognostic value of sarcopenia in lung cancer: A systematic review and meta-analysis. Chest 2019, 156, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Caan, B.J.; Quesenbery, C.P.; Lee, C. Body composition and overall survival in patients with nonmetastatic breast cancer—Reply. JAMA Oncol. 2019, 5, 115–116. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Morley, J.E. Sarcopenia is recognized as an independent condition by an international classification of disease, tenth revision, clinical modification (ICD-10-CM) code. J. Post-Acute Long Term Care Med. 2016, 17, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Ataa, A.M.; Karaa, M.; Kaymaka, B.; Gürcay, E.; Cakir, B.; Unlü, H.; Akinci, A.; Ozcakar, L. Regional and total muscle mass, muscle strength and physical performance: The potential use of ultrasound imaging for sarcopenia. Arch. Gerontol. Geriatr. 2019, 83, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Shin, Y.; Huh, Y.; Sung, Y.S.; Lee, I.-S.; Yoon, K.-H.; Kim, K.W. Recent Issues on Body Composition Imaging for Sarcopenia Evaluation. Musculoskelet. Med. 2019, 20, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Aleixo, G.F.P.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B.; Battaglini, C.L.; Williams, G.R. Bioelectrical impedance analysis for the assessment of sarcopenia in patients with cancer: A systematic review. Oncologist 2020, 25, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Benton, E.; Liteplo, A.S.; Shokoohi, H.; Loesche, M.A.; Yacoub, S.; Thatphet, P.; Wongtangman, T.; Liu, S.W. A pilot study examining the use of ultrasound to measure sarcopenia, frailty and fall in older patients. Am. J. Emerg. Med. 2021, 46, 310–316. [Google Scholar] [CrossRef]
- Davis, M.P.; Panikkar, R. Sarcopenia associated with chemotherapy and targeted agents for cancer therapy. Ann. Palliat. Med. 2019, 8, 86–101. [Google Scholar] [CrossRef]
- Magudia, K.; Bridge, C.P.; Bay, C.P.; Babic, A.; Fintelmann, F.J.; Troschel, F.M.; Miskin, N.; Wrobel, W.C.; Brais, L.K.; Andriole, K.P.; et al. Population-Scale CT-based Body Composition Analysis of a Large Outpatient Population Using Deep Learning to Derive Age-, Sex-, and Race-specific Reference Curves. Radiology 2020, 298, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Stringer, H.J.; Wilson, D. The role of ultrasound as a diagnostic tool for sarcopenia. J. Frailty Aging 2018, 7, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Mombiela, R.M. Ultrasound Biomarkers for Sarcopenia: What Can We Tell So Far? Semin. Musculoskelet. Radiol. 2020, 24, 181–193. [Google Scholar] [CrossRef]
- Wijntjes, J.; van Alfen, N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve 2021, 63, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Rajewsky, B. Ultra-short waves: Their medical and biological applications. In Results of Biophysical Research; Danzer, V.H., Hollmann, H.E., Rajewsky, B., Schaefer, H., Schliephake, E., Eds.; Georg Thieme: Leipzig, Germany, 1938. [Google Scholar]
- Wilson, J.N. The dielectric constants of polar liquids. Chem. Rev. 1939, 25, 377–406. [Google Scholar] [CrossRef]
- Foster, K.R.; Schwan, H.P. Dielectric properties of tissues and biological materials: A critical review. Crit. Rev. Biomed. Eng. 1989, 17, 25–104. [Google Scholar]
- Johansson, K.; Darkeh, M.H.; Lahtinen, T.; Bjork-Eriksson, T.; Axelsson, R. Two-year follow-up of temporal changes of breast edema after breast cancer treatment with surgery and radiation evaluated by tissue dielectric constant (TDC). Eur. J. Lymphol. Relat. Probl. 2015, 27, 15–21. [Google Scholar]
- Sugitani, T.; Kubota, S.-I.; Kuroki, S.-I.; Sogo, K.; Arihiro, K.; Okada, M.; Kadoya, T.; Hide, M.; Oda, M.; Kikkawa, T. Complex permittivities of breast tumor tissues obtained from cancer surgeries. Appl. Phys. Lett. 2014, 104, 253702. [Google Scholar] [CrossRef]
- Martellosio, A.; Pasian, M.; Bozzi, M.; Perregrini, L.; Mazzanti, A.; Svelto, F.; Summers, P.E.; Renne, G.; Preda, L.; Bellomi, M. Dielectric properties characterization from 0.5 to 50 GHz of breast cancer tissues. IEEE Trans. Microw. Theory 2017, 65, 998–1011. [Google Scholar] [CrossRef]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093–6115. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Fhager, A.; Trefna, H.D.; Yu, Y.; McKelvey, T.; Pegenius, G.; Karlsson, J.-E.; Elam, M. Microwave-based stroke diagnosis making global prehospital thrombolytic treatment possible. IEEE Trans. Biomed. Eng. 2014, 61, 2806–2817. [Google Scholar] [CrossRef] [PubMed]
- Amin, B.; Elahi, M.A.; Shahzad, A.; Porter, E.; McDermott, B.; O’Halloran, M. Dielectric properties of bones for the monitoring of osteoporosis. Med. Biol. Eng. Comput. 2019, 57, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Meaney, P.M.; Zhou, T.; Goodwin, D.; Golnabi, A.; Attardo, E.; Paulsen, K.D. Bone dielectric property variation as a function of mineralization at microwave frequencies. Int. J. Biomed. Imaging 2012, 2012, 649612. [Google Scholar] [CrossRef] [PubMed]
- Preece, A.W.; Craddock, I.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection. J. Med. Imaging 2016, 3, 033502. [Google Scholar] [CrossRef]
- Vasquez, J.A.T.; Scapaticci, R.; Turvani, G.; Bellizzi, G.; Rodriguez-Duarte, D.O.; Joachimowicz, N.; Duchene, B.; Tedeschi, E.; Casu, M.R.; Crocco, L.; et al. A Prototype Microwave System for 3D Brain Stroke Imaging. Sensors 2020, 20, 2607. [Google Scholar] [CrossRef]
- Fasoula, A.; Duchesne, L.; Cano, J.D.G.; Lawrence, P.; Robin, G.; Bernard, J.-G. On-site validation of a microwave breast imaging system, before first patient study. Diagnostics 2018, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Bourqui, J.; Sill, J.M.; Fear, E.C. A prototype system for measuring microwave frequency reflections from the breast. Int. J. Biomed. Imaging 2012, 2012, 851234. [Google Scholar] [CrossRef]
- Athey, T.W.; Stuchly, M.A.; Stuchly, S.S. Measurement of radio frequency permittivity of biological tissues with an open-ended coaxial line: Part I. IEEE Trans. Microw. Theory Tech. 1982, 30, 82–86. [Google Scholar] [CrossRef]
- Gabriel, C.; Chan, T.Y.A.; Grant, E.H. Admittance models for open ended coaxial probes and their place in dielectric spectroscopy. Phys. Med. Biol. 1994, 39, 2183–2200. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.P.; Clarke, R.N.; Hodgetts, T.E.; Symm, G.T. RF and Dielectric Measurements upon Layered Materials Using Coaxial Sensors; Report MAT 13; National Physical Laboratory: Teddington, UK, 2008. [Google Scholar]
- Meaney, P.M.; Gregory, A.P.; Seppälä, J.; Lahtinen, T. Open-ended coaxial dielectric probe effective penetration depth determination. IEEE Trans. Microw. Theory Tech. 2016, 64, 915–923. [Google Scholar] [CrossRef]
- Salah-Ud-Din, S.; Meaney, P.M.; Porter, E.; O’Halloran, M. Investigation of abscissa scales for dielectric measurements of biological tissues. Biomed. Phys. Eng. Express 2017, 3, 015020. [Google Scholar]
- Gaikovich, K.P.; Gaikovich, P.K. Inverse problem of near-field scattering in multilayer media. Inverse Probl. 2010, 26, 125013. [Google Scholar] [CrossRef][Green Version]
- Gaikovich, K.P.; Gaikovich, P.K.; Maksimovitch, Y.S.; Badeev, V.A. Pseudopulse near-field subsurface tomography. Phys. Rev. Lett. 2012, 108, 163902. [Google Scholar] [CrossRef]
- Meaney, P.M.; Rydholm, T.; Brisby, H. A transmission-based dielectric property probe for clinical applications. Sensors 2018, 18, 3484. [Google Scholar] [CrossRef]
- Meaney, P.M.; Raynolds, T. Systems and Methods for Non-Invasive Microwave Testing of Bottles of Wine. U.S. Patent Application No. 20,210,311,012, 30 July 2019. [Google Scholar]
- Hammerstad, E.O.; Bekkadal, F. A Microstrip Handbook, ELAB Report; STF 44 A74169; University of Trondheim: Trondheim, Norway, 1975; pp. 98–110. [Google Scholar]
- Pozar, D.M. Microwave Engineering, 4th ed.; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Schepps, J.L.; Foster, K.R. The UHF and microwave dielectric properties of normal and tumour tissues: Variation in dielectric properties with tissue water content. Phys. Med. Biol. 1980, 25, 1149–1159. [Google Scholar] [CrossRef]
- Guy, A.W. Analysis of electromagnetic fields induced in biological tissues by thermographic studies and equivalent phantom models. IEEE Trans. Microw. Theory Tech. 1971, 19, 205–213. [Google Scholar] [CrossRef]
- Mattsson, V.; Ackermans, L.L.G.C.; Mandal, B.; Perez, M.D.; Vesseur, M.A.M.; Meaney, P.M.; Ten Bosch, J.A.; Blokhuis, T.J.; Augustine. R. MAS: Standalone microwave resonator to assess muscle quality. Sensors 2021, 21, 5485. [Google Scholar] [CrossRef] [PubMed]
- Asan, N.B.; Hassan, E.; Velander, J.; Mohd, S.S.R.; Noreland, D.; Blokhuis, T.J.; Wadbro, E.; Berggren, M.; Voight, T.; Augustine, R. Characterization of the fat channel for intra-body communication at R-band frequencies. Sensors 2018, 18, 2752. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (All Dimensions in Centimeters) | Inner Conductor | Outer Conductor |
|---|---|---|
| Connector end diameter | 0.17 | 0.66 |
| Minor (ellipse) | 0.38 | 1.52 |
| Major (ellipse) | 0.64 | 2.54 |
| Length | 6.35 | |
| Spacing of connectors | 2.03 | |
| Spacing of ellipse centers | 2.79 | |
| Off-center spacing of ellipse center conductor | 0.19 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meaney, P.; Geimer, S.D.; diFlorio-Alexander, R.M.; Augustine, R.; Raynolds, T. Open-Ended Transmission Coaxial Probes for Sarcopenia Assessment. Sensors 2022, 22, 748. https://doi.org/10.3390/s22030748
Meaney P, Geimer SD, diFlorio-Alexander RM, Augustine R, Raynolds T. Open-Ended Transmission Coaxial Probes for Sarcopenia Assessment. Sensors. 2022; 22(3):748. https://doi.org/10.3390/s22030748
Chicago/Turabian StyleMeaney, Paul, Shireen D. Geimer, Roberta M. diFlorio-Alexander, Robin Augustine, and Timothy Raynolds. 2022. "Open-Ended Transmission Coaxial Probes for Sarcopenia Assessment" Sensors 22, no. 3: 748. https://doi.org/10.3390/s22030748
APA StyleMeaney, P., Geimer, S. D., diFlorio-Alexander, R. M., Augustine, R., & Raynolds, T. (2022). Open-Ended Transmission Coaxial Probes for Sarcopenia Assessment. Sensors, 22(3), 748. https://doi.org/10.3390/s22030748