

Validity of Two Consumer Multisport Activity Tracker and One Accelerometer against Polysomnography for Measuring Sleep Parameters and Vital Data in a Laboratory Setting in Sleep Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Laboratory Procedures
2.3. Devices and Sleep Parameters
2.3.1. Accelerometer ActiGraph GT9X
2.3.2. Garmin Forerunner 945
2.3.3. Polar Ignite
2.3.4. Data Extraction and Scoring
2.4. Statistical Analysis
3. Results
3.1. Vital Data Measurement
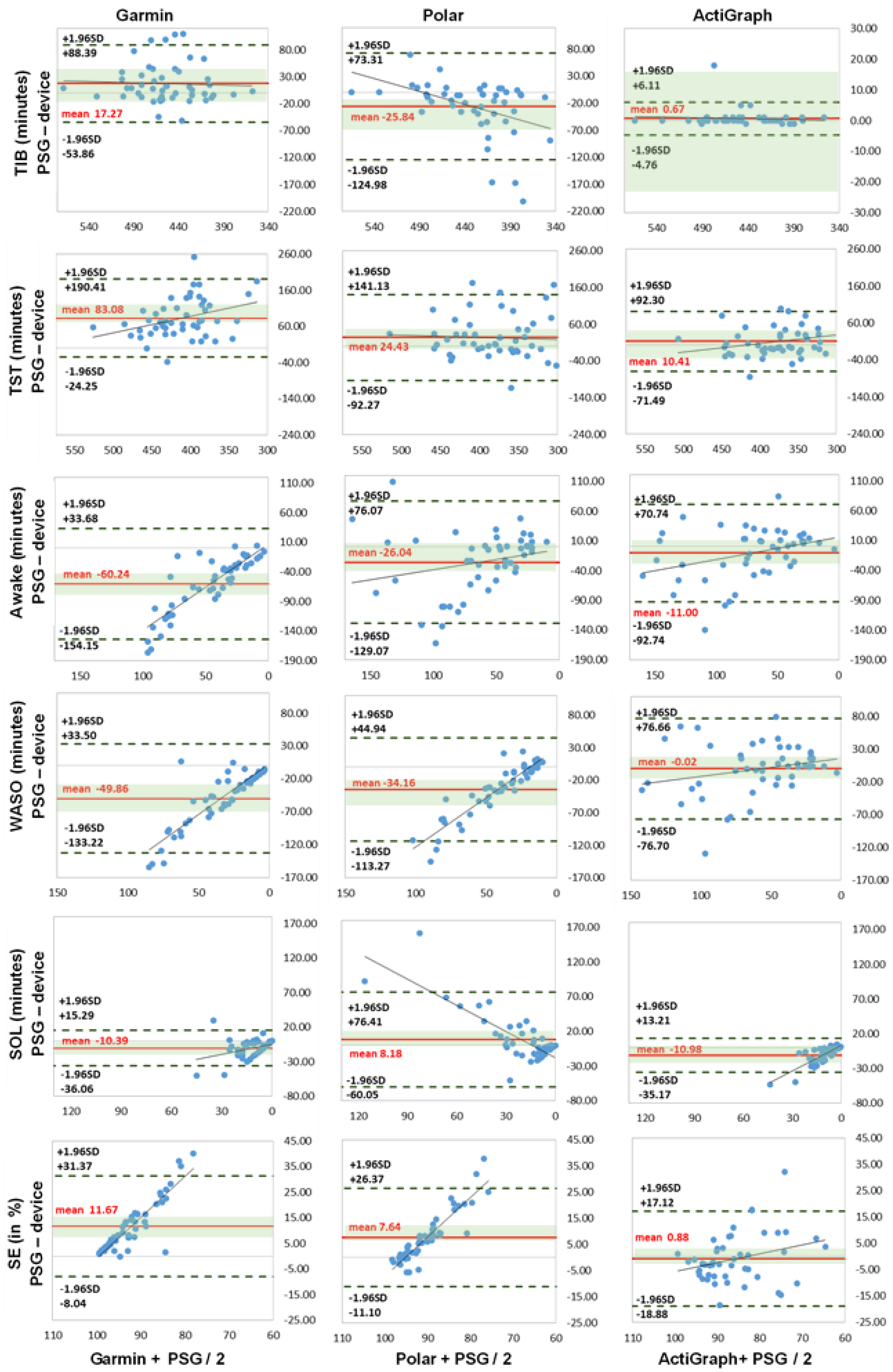
3.2. Sleep Parameters
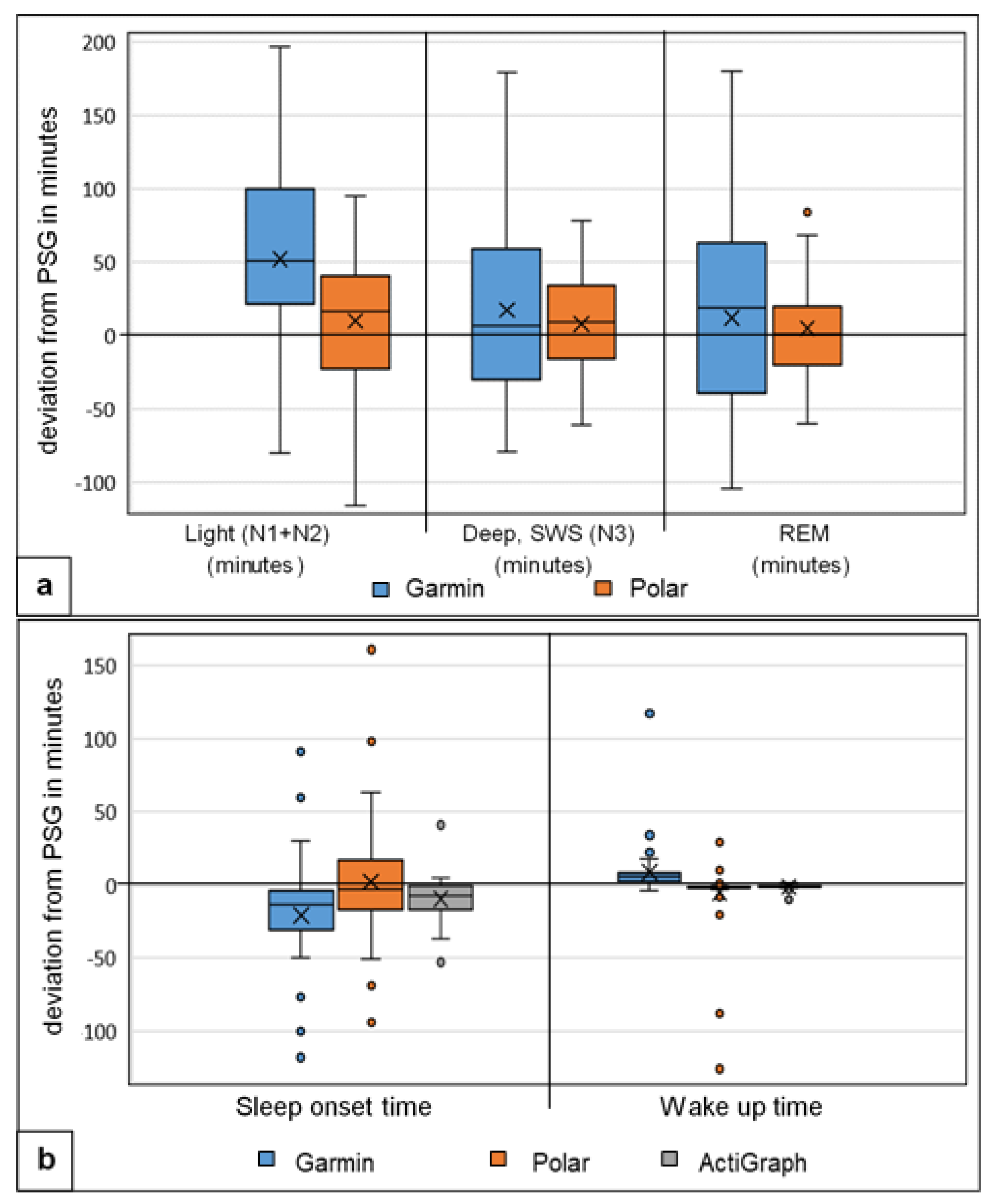
3.3. Sleep Stages
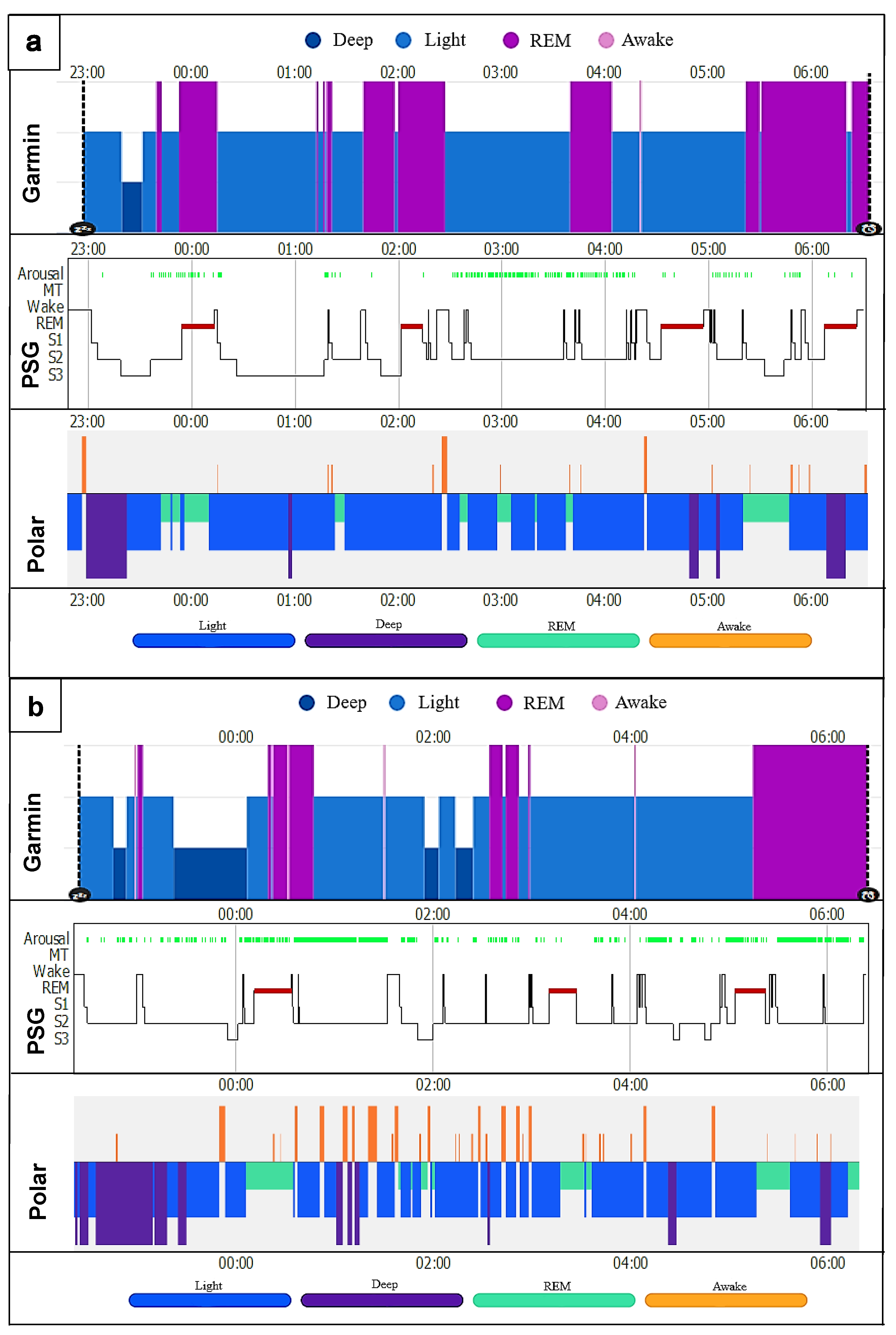
3.4. Hypnogram Analysis
3.5. MSLT Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Düking, P.; Giessing, L.; Frenkel, M.O.; Koehler, K.; Holmberg, H.-C.; Sperlich, B. Wrist-Worn Wearables for Monitoring Heart Rate and Energy Expenditure While Sitting or Performing Light-to-Vigorous Physical Activity: Validation Study. JMIR Mhealth Uhealth 2020, 8, e16716. [Google Scholar] [CrossRef]
- Miller, D.J.; Roach, G.D.; Lastella, M.; Scanlan, A.T.; Bellenger, C.R.; Halson, S.L.; Sargent, C. A Validation Study of a Commercial Wearable Device to Automatically Detect and Estimate Sleep. Biosensors 2021, 11, 185. [Google Scholar] [CrossRef]
- Laricchia, F. Fitness Trackers—Statistics & Facts. Available online: https://www.statista.com/topics/4393/fitness-and-activity-tracker/#topicHeader__wrapper (accessed on 17 November 2022).
- Li, X.; Zhang, Y.; Jiang, F.; Zhao, H. A novel machine learning unsupervised algorithm for sleep/wake identification using actigraphy. Chronobiol. Int. 2020, 37, 1002–1015. [Google Scholar] [CrossRef]
- Topalidis, P.; Florea, C.; Eigl, E.-S.; Kurapov, A.; Leon, C.A.B.; Schabus, M. Evaluation of a Low-Cost Commercial Actigraph and Its Potential Use in Detecting Cultural Variations in Physical Activity and Sleep. Sensors 2021, 21, 3774. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, V.; Silva, J.; Navarro, E.; Cauli, O. Sleep assessment devices: Types, market analysis, and a critical view on accuracy and validation. Expert Rev. Med. Devices 2019, 16, 1041–1052. [Google Scholar] [CrossRef]
- Perez-Pozuelo, I.; Posa, M.; Spathis, D.; Westgate, K.; Wareham, N.; Mascolo, C.; Brage, S.; Palotti, J. Detecting sleep outside the clinic using wearable heart rate devices. Sci. Rep. 2022, 12, 7956. [Google Scholar] [CrossRef]
- Benington, J.H.; Craig Heller, H. Restoration of brain energy metabolism as the function of sleep. Prog. Neurobiol. 1995, 45, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.R.L.; Roth, T. Neurophysiology of sleep and wakefulness: Basic science and clinical implications. Curr. Neuropharmacol. 2008, 6, 367–378. [Google Scholar] [CrossRef]
- Imeri, L.; Opp, M.R. How (and why) the immune system makes us sleep. Nat. Rev. Neurosci. 2009, 10, 199–210. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Grandner, M.A.; Brown, D.; Conroy, M.B.; Jean-Louis, G.; Coons, M.; Bhatt, D.L.; American Heart Association Obesity, Behavior Change, Diabetes, and Nutrition Committees of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Sleep Duration and Quality: Impact on Lifestyle Behaviors and Cardiometabolic Health: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e367–e386. [Google Scholar] [CrossRef]
- Liang, Z.; Chapa Martell, M.A. Validity of Consumer Activity Wristbands and Wearable EEG for Measuring Overall Sleep Parameters and Sleep Structure in Free-Living Conditions. J. Healthc. Inf. Res. 2018, 2, 152–178. [Google Scholar] [CrossRef] [PubMed]
- Natale, V.; Léger, D.; Martoni, M.; Bayon, V.; Erbacci, A. The role of actigraphy in the assessment of primary insomnia: A retrospective study. Sleep Med. 2014, 15, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A.; Dement, W.C. Normal Human Sleep. Princ. Pract. Sleep Med. 2011, 4, 16–26. [Google Scholar] [CrossRef]
- Perez-Pozuelo, I.; Zhai, B.; Palotti, J.; Mall, R.; Aupetit, M.; Garcia-Gomez, J.M.; Taheri, S.; Guan, Y.; Fernandez-Luque, L. The future of sleep health: A data-driven revolution in sleep science and medicine. NPJ Digit. Med. 2020, 3, 42. [Google Scholar] [CrossRef]
- Hao, Y.; Foster, R. Wireless body sensor networks for health-monitoring applications. Physiol. Meas. 2008, 29, R27–R56. [Google Scholar] [CrossRef] [PubMed]
- Latshang, T.D.; Mueller, D.J.; Lo Cascio, C.M.; Stöwhas, A.-C.; Stadelmann, K.; Tesler, N.; Achermann, P.; Huber, R.; Kohler, M.; Bloch, K.E. Actigraphy of Wrist and Ankle for Measuring Sleep Duration in Altitude Travelers. High Alt. Med. Amp. Biol. 2016, 17, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Sargent, C.; Lastella, M.; Halson, S.L.; Roach, G.D. The validity of activity monitors for measuring sleep in elite athletes. J. Sci. Med. Sport 2016, 19, 848–853. [Google Scholar] [CrossRef]
- Haghayegh, S.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R.; Castriotta, R.J. Performance assessment of new-generation Fitbit technology in deriving sleep parameters and stages. Chronobiol. Int. 2019, 37, 47–59. [Google Scholar] [CrossRef]
- Van De Water, A.T.M.; Holmes, A.; Hurley, D.A. Objective measurements of sleep for non-laboratory settings as alternatives to polysomnography—A systematic review. J. Sleep Res. 2011, 20, 183–200. [Google Scholar] [CrossRef]
- Hamill, K.; Jumabhoy, R.; Kahawage, P.; Zambotti, M.; Walters, E.M.; Drummond, S.P.A. Validity, potential clinical utility and comparison of a consumer activity tracker and a research—Grade activity tracker in insomnia disorder II: Outside the laboratory. J. Sleep Res. 2019, 29, e12944. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.; Li, Y.; Rueschman, M.N.; Winkelman, J.W.; Ellenbogen, J.M.; Solet, J.M.; Dulin, H.; Berkman, L.F.; Buxton, O.M. Measuring sleep: Accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep 2013, 36, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Montgomery-Downs, H.E.; Insana, S.P.; Bond, J.A. Movement toward a novel activity monitoring device. Sleep Breath. 2011, 16, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Beattie, Z.; Oyang, Y.; Statan, A.; Ghoreyshi, A.; Pantelopoulos, A.; Russell, A.; Heneghan, C. Estimation of sleep stages in a healthy adult population from optical plethysmography and accelerometer signals. Physiol. Meas. 2017, 38, 1968–1979. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Cole, R.; Alessi, C.; Chambers, M.; Moorcroft, W.; Pollak, C.P. The Role of Actigraphy in the Study of Sleep and Circadian Rhythms. Sleep 2003, 26, 342–392. [Google Scholar] [CrossRef]
- de Zambotti, M.; Cellini, N.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Wearable Sleep Technology in Clinical and Research Settings. Med. Sci. Sport Exerc. 2019, 51, 1538–1557. [Google Scholar] [CrossRef]
- de Zambotti, M.; Baker, F.C.; Colrain, I.M. Validation of Sleep-Tracking Technology Compared with Polysomnography in Adolescents. Sleep 2015, 38, 1461–1468. [Google Scholar] [CrossRef]
- de Zambotti, M.; Claudatos, S.; Inkelis, S.; Colrain, I.M.; Baker, F.C. Evaluation of a consumer fitness-tracking device to assess sleep in adults. Chronobiol. Int. 2015, 32, 1024–1028. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Hiruma, L.S.; Avis, K.; Montgomery-Downs, H.; Valentin, J. Comparison of a Commercial Accelerometer with Polysomnography and Actigraphy in Children and Adolescents. Sleep 2015, 38, 1323–1330. [Google Scholar] [CrossRef]
- Liang, Z.; Martell, M.A.C. Measurement Accuracy of Consumer Sleep Tracking Wristbands is Associated to User-Specific Factors. J. Phys. Fit. Sports Med. Misc. 2019, 8, 388–394. [Google Scholar] [CrossRef]
- Kolla, B.P.; Mansukhani, S.; Mansukhani, M.P. Consumer sleep tracking devices: A review of mechanisms, validity and utility. Expert Rev. Med. Devices 2016, 13, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Chapa-Martell, M.A. Accuracy of Fitbit Wristbands in Measuring Sleep Stage Transitions and the Effect of User-Specific Factors. JMIR Mhealth Uhealth 2019, 7, e13384. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.K.; Pu, Y. Heart rate variability, sleep and sleep disorders. Sleep Med. Rev. 2012, 16, 47–66. [Google Scholar] [CrossRef] [PubMed]
- Xiao, M.; Yan, H.; Song, J.; Yang, Y.; Yang, X. Sleep stages classification based on heart rate variability and random forest. Biomed. Signal Process. Control 2013, 8, 624–633. [Google Scholar] [CrossRef]
- de Zambotti, M.; Willoughby, A.R.; Franzen, P.L.; Clark, D.B.; Baker, F.C.; Colrain, I.M. K-Complexes: Interaction between the Central and Autonomic Nervous Systems during Sleep. Sleep 2016, 39, 1129–1137. [Google Scholar] [CrossRef]
- Kinnunen, H.; Rantanen, A.; Kenttä, T.; Koskimäki, H. Feasible assessment of recovery and cardiovascular health: Accuracy of nocturnal HR and HRV assessed via ring PPG in comparison to medical grade ECG. Physiol. Meas. 2020, 41, 4NT01. [Google Scholar] [CrossRef]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; NissilÄ, J.; Virtanen, P.; Karjalainen, J.; Tulppo, M.P. Daily Exercise Prescription on the Basis of HR Variability among Men and Women. Med. Amp. Sci. Sport Amp. Exerc. 2010, 42, 1355–1363. [Google Scholar] [CrossRef]
- Badra, L.J.; Cooke, W.H.; Hoag, J.B.; Crossman, A.A.; Kuusela, T.A.; Tahvanainen, K.U.O.; Eckberg, D.L. Respiratory modulation of human autonomic rhythms. Am. J. Physiol.-Heart Circ. Physiol. 2001, 280, H2674–H2688. [Google Scholar] [CrossRef]
- Eckberg, D.L. The human respiratory gate. J. Physiol. 2003, 548, 339–352. [Google Scholar] [CrossRef]
- Berryhill, S.; Morton, C.J.; Dean, A.; Berryhill, A.; Provencio-Dean, N.; Patel, S.I.; Estep, L.; Combs, D.; Mashaqi, S.; Gerald, L.B.; et al. Effect of wearables on sleep in healthy individuals: A randomized crossover trial and validation study. J. Clin. Sleep Med. 2020, 16, 775–783. [Google Scholar] [CrossRef]
- Yasuma, F.; Hayano, J.-I. Respiratory Sinus Arrhythmia: Why Does the Heartbeat Synchronize With Respiratory Rhythm? Chest 2004, 125, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Douglas, N.J.; White, D.P.; Pickett, C.K.; Weil, J.V.; Zwillich, C.W. Respiration during sleep in normal man. Thorax 1982, 37, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.; Murawski, B.; Short, C.E.; Rebar, A.L.; Schoeppe, S.; Alley, S.; Vandelanotte, C.; Kirwan, M. Activity Trackers Implement Different Behavior Change Techniques for Activity, Sleep, and Sedentary Behaviors. Interact. J. Med. Res. 2017, 6, e13. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Cuellar, J.A.; Huwa, K.E.; Jameson, J.T.; Watson, C.H.; Bessman, S.C.; Hirsch, D.A.; Cooper, A.D.; Drummond, S.P.A.; Markwald, R.R. Performance of seven consumer sleep-tracking devices compared with polysomnography. Sleep 2021, 44, zsaa291. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, S.; Sica, M.; Ancillao, A.; Timmons, S.; Barton, J.; O’Flynn, B. Validity Evaluation of the Fitbit Charge2 and the Garmin vivosmart HR+ in Free-Living Environments in an Older Adult Cohort. JMIR Mhealth Uhealth 2019, 7, e13084. [Google Scholar] [CrossRef] [PubMed]
- de Zambotti, M.; Goldstone, A.; Claudatos, S.; Colrain, I.M.; Baker, F.C. A validation study of Fitbit Charge 2™ compared with polysomnography in adults. Chronobiol. Int. 2018, 35, 465–476. [Google Scholar] [CrossRef]
- Moreno-Pino, F.; Porras-Segovia, A.; López-Esteban, P.; Artés, A.; Baca-García, E. Validation of Fitbit Charge 2 and Fitbit Alta HR Against Polysomnography for Assessing Sleep in Adults With Obstructive Sleep Apnea. J. Clin. Sleep Med. 2019, 15, 1645–1653. [Google Scholar] [CrossRef]
- Giurgiu, M.; Timm, I.; Becker, M.; Schmidt, S.; Wunsch, K.; Nissen, R.; Davidovski, D.; Bussmann, J.B.J.; Nigg, C.R.; Reichert, M.; et al. Quality Evaluation of Free-living Validation Studies for the Assessment of 24-Hour Physical Behavior in Adults via Wearables: Systematic Review. JMIR Mhealth Uhealth 2022, 10, e36377. [Google Scholar] [CrossRef]
- Miller, D.J.; Sargent, C.; Roach, G.D. A Validation of Six Wearable Devices for Estimating Sleep, Heart Rate and Heart Rate Variability in Healthy Adults. Sensors 2022, 22, 6317. [Google Scholar] [CrossRef]
- Klier, K.; Wagner, M. Agreement of Sleep Measures-A Comparison between a Sleep Diary and Three Consumer Wearable Devices. Sensors 2022, 22, 6189. [Google Scholar] [CrossRef]
- Henriksen, A.; Svartdal, F.; Grimsgaard, S.; Hartvigsen, G.; Hopstock, L.A. Polar Vantage and Oura Physical Activity and Sleep Trackers: Validation and Comparison Study. JMIR Form. Res. 2022, 6, e27248. [Google Scholar] [CrossRef] [PubMed]
- Kubala, A.G.; Barone Gibbs, B.; Buysse, D.J.; Patel, S.R.; Hall, M.H.; Kline, C.E. Field-based Measurement of Sleep: Agreement between Six Commercial Activity Monitors and a Validated Accelerometer. Behav. Sleep Med. 2020, 18, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Pesonen, A.-K.; Kuula, L. The Validity of a New Consumer-Targeted Wrist Device in Sleep Measurement: An Overnight Comparison Against Polysomnography in Children and Adolescents. J. Clin. Sleep Med. 2018, 14, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic Sleep/Wake Identification From Wrist Activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef]
- Burkart, S.; Beets, M.W.; Armstrong, B.; Hunt, E.T.; Dugger, R.; von Klinggraeff, L.; Jones, A.; Brown, D.E.; Weaver, R.G. Comparison of multichannel and single-channel wrist-based devices with polysomnography to measure sleep in children and adolescents. J. Clin. Sleep Med. 2021, 17, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; McCrae, C.S.; Cheung, J.; Martin, J.L.; Harrod, C.G.; Heald, J.L.; Carden, K.A. Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2018, 14, 1231–1237. [Google Scholar] [CrossRef]
- Lee, J.-M.; Byun, W.; Keill, A.; Dinkel, D.; Seo, Y. Comparison of Wearable Trackers’ Ability to Estimate Sleep. Int. J. Environ. Res. Public Health 2018, 15, 1265. [Google Scholar] [CrossRef]
- Full, K.M.; Kerr, J.; Grandner, M.A.; Malhotra, A.; Moran, K.; Godoble, S.; Natarajan, L.; Soler, X. Validation of a physical activity accelerometer device worn on the hip and wrist against polysomnography. Sleep Health 2018, 4, 209–216. [Google Scholar] [CrossRef]
- Wan, T.; Luo, Q. Literature Review of the Application of Wearable Device GT3X in Monitoring Physical Activity. Adv. Intell. Syst. Comput. 2019, 1018, 569–575. [Google Scholar] [CrossRef]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.M.; Jackson, A.S. Exercise Concepts, Calculations, and Computer Applications; Benchmark Press: Carmel, CA, USA, 1990. [Google Scholar]
- Wier, L.T.; Ayers, G.W.; Jackson, A.S.; Rossum, A.C.; Carlos Poston, W.S.; Foreyt, J.P. Determining the amount of physical activity needed for long-term weight control. Int. J. Obes. 2001, 25, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Littner, M.R.; Kushida, C.; Wise, M.; Davila, D.G.; Morgenthaler, T.; Lee-Chiong, T.; Hirshkowitz, M.; Loube, D.L.; Bailey, D.; Berry, R.B.; et al. Practice Parameters for Clinical Use of the Multiple Sleep Latency Test and the Maintenance of Wakefulness Test. Sleep 2005, 28, 113–121. [Google Scholar] [CrossRef]
- Stuck, B.A.; Maurer, J.T.; Schlarb, A.A.; Schredl, M.; Weeß, H.-G. Praxis der Schlafmedizin; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- Peter, H.; Penzel, T.; Peter, J.H. Enzyklopädie der Schlafmedizin; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar] [CrossRef]
- ActiGraph, L. User Guide, ActiGraph GT9X Link + ActiLife. Available online: https://s3.amazonaws.com/actigraphcorp.com/wp-content/uploads/2020/03/05155628/ActiGraph_Link_UserGuide_E.200.6001_Revision6_FINAL.pdf (accessed on 20 September 2022).
- Madrid-Navarro, C.J.; Puertas Cuesta, F.J.; Escamilla-Sevilla, F.; Campos, M.; Ruiz Abellán, F.; Rol, M.A.; Madrid, J.A. Validation of a Device for the Ambulatory Monitoring of Sleep Patterns: A Pilot Study on Parkinson’s Disease. Front. Neurol. 2019, 10, 356. [Google Scholar] [CrossRef] [PubMed]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.L.; Quan, S. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, NY, USA, 2007. [Google Scholar]
- Garmin. Forerunner 945 Owner’s Manual. Available online: https://www8.garmin.com/manuals/webhelp/forerunner945/EN-US/Forerunner_945M_OM (accessed on 20 September 2022).
- Polar, E.O. Polar Ignite User Manual. Available online: https://support.polar.com/e_manuals/ignite/polar-ignite-user-manual-english/manual.pdf (accessed on 20 September 2022).
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate—A Practical and Powerful Approach to Multiple Testing. J. Royal Stat. Soc. Series B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Martin, J.L.; Blackwell, T.; Buenaver, L.; Liu, L.; Meltzer, L.J.; Sadeh, A.; Spira, A.P.; Taylor, D.J. The SBSM Guide to Actigraphy Monitoring: Clinical and Research Applications. Behav. Sleep Med. 2015, 13, S4–S38. [Google Scholar] [CrossRef]
- Menghini, L.; Cellini, N.; Goldstone, A.; Baker, F.C.; de Zambotti, M. A standardized framework for testing the performance of sleep-tracking technology: Step-by-step guidelines and open-source code. Sleep 2021, 44, zsaa170. [Google Scholar] [CrossRef] [PubMed]
- Grandner, M.A.; Rosenberger, M.E. Chapter 12-Actigraphic sleep tracking and wearables: Historical context, scientific applications and guidelines, limitations, and considerations for commercial sleep devices. In Sleep and Health; Grandner, M.A., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 147–157. [Google Scholar] [CrossRef]
- Mühlen, J.M.; Stang, J.; Lykke Skovgaard, E.; Judice, P.B.; Molina-Garcia, P.; Johnston, W.; Sardinha, L.B.; Ortega, F.B.; Caulfield, B.; Bloch, W.; et al. Recommendations for determining the validity of consumer wearable heart rate devices: Expert statement and checklist of the Interlive Network. Br. J. Sport Med. 2021, 55, 767–779. [Google Scholar] [CrossRef]
- Düking, P.; Fuss, F.K.; Holmberg, H.-C.; Sperlich, B. Recommendations for Assessment of the Reliability, Sensitivity, and Validity of Data Provided by Wearable Sensors Designed for Monitoring Physical Activity. JMIR Mhealth Uhealth 2018, 6, e102. [Google Scholar] [CrossRef]
- Nelson, B.W.; Low, C.A.; Jacobson, N.; Areán, P.; Torous, J.; Allen, N.B. Guidelines for wrist-worn consumer wearable assessment of heart rate in biobehavioral research. NPJ Digit. Med. 2020, 3, 90. [Google Scholar] [CrossRef]
- Shcherbina, A.; Mattsson, C.M.; Waggott, D.; Salisbury, H.; Christle, J.W.; Hastie, T.; Wheeler, M.T.; Ashley, E.A. Accuracy in Wrist-Worn, Sensor-Based Measurements of Heart Rate and Energy Expenditure in a Diverse Cohort. J. Pers. Med. 2017, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Gilgen-Ammann, R.; Schweizer, T.; Wyss, T. RR interval signal quality of a heart rate monitor and an ECG Holter at rest and during exercise. Eur. J. Appl. Physiol. 2019, 119, 1525–1532. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum Associates: Hillsdale, Australia, 1988; p. 567. [Google Scholar]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Altini, M.; Kinnunen, H. The Promise of Sleep: A Multi-Sensor Approach for Accurate Sleep Stage Detection Using the Oura Ring. Sensors 2021, 21, 4302. [Google Scholar] [CrossRef]
- Nuuttila, O.-P.; Korhonen, E.; Laukkanen, J.; Kyröläinen, H. Validity of the Wrist-Worn Polar Vantage V2 to Measure Heart Rate and Heart Rate Variability at Rest. Sensors 2021, 22, 137. [Google Scholar] [CrossRef]
- Budig, M.; Keiner, M.; Stoohs, R.; Hoffmeister, M.; Höltke, V. Heart Rate and Distance Measurement of Two Multisport Activity Trackers and a Cellphone App in Different Sports: A Cross-Sectional Validation and Comparison Field Study. Sensors 2021, 22, 180. [Google Scholar] [CrossRef]
- Charlton, P.H.; Birrenkott, D.A.; Bonnici, T.; Pimentel, M.A.F.; Johnson, A.E.W.; Alastruey, J.; Tarassenko, L.; Watkinson, P.J.; Beale, R.; Clifton, D.A. Breathing Rate Estimation From the Electrocardiogram and Photoplethysmogram: A Review. IEEE Rev. Biomed. Eng. 2018, 11, 2–20. [Google Scholar] [CrossRef]
- Cheung, J.; Leary, E.B.; Lu, H.; Zeitzer, J.M.; Mignot, E. PSG Validation of minute-to-minute scoring for sleep and wake periods in a consumer wearable device. PLoS ONE 2020, 15, e0238464. [Google Scholar] [CrossRef]
- Svensson, T.; Chung, U.-I.; Tokuno, S.; Nakamura, M.; Svensson, A.K. A validation study of a consumer wearable sleep tracker compared to a portable EEG system in naturalistic conditions. J. Psychosom. Res. 2019, 126, 109822. [Google Scholar] [CrossRef] [PubMed]
- Roomkham, S.; Hittle, M.; Cheung, J.; Lovell, D.; Mignot, E.; Perrin, D. Sleep monitoring with the Apple Watch: Comparison to a clinically validated actigraph. F1000Research 2019, 8, 754. [Google Scholar] [CrossRef]
- Ameen, M.S.; Cheung, L.M.; Hauser, T.; Hahn, M.A.; Schabus, M. About the Accuracy and Problems of Consumer Devices in the Assessment of Sleep. Sensors 2019, 19, 4160. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Redline, S.; Kirchner, H.L.; Quan, S.F.; Gottlieb, D.J.; Kapur, V.; Newman, A. The Effects of Age, Sex, Ethnicity, and Sleep-Disordered Breathing on Sleep Architecture. Arch. Intern. Med. 2004, 164, 406. [Google Scholar] [CrossRef]
- Cooke, J.R.; Ancoli-Israel, S. Normal and abnormal sleep in the elderly. Handb. Clin. Neurol. 2011, 98, 653–665. [Google Scholar] [CrossRef]
- Moraes, W.; Piovezan, R.; Poyares, D.; Bittencourt, L.R.; Santos-Silva, R.; Tufik, S. Effects of aging on sleep structure throughout adulthood: A population-based study. Sleep Med. 2014, 15, 401–409. [Google Scholar] [CrossRef]
- Liang, Z.; Martell, M.A.C. Considering interpersonal differences in validating wearable sleep-tracking technologies. In Proceedings of the 2017 Tenth International Conference on Mobile Computing and Ubiquitous Network (ICMU), Toyama, Japan, 3–5 October 2017. [Google Scholar]
- Jeon, S.; Park, T.; Paul, A.; Lee, Y.-S.; Son, S.H. A Wearable Sleep Position Tracking System Based on Dynamic State Transition Framework. IEEE Access 2019, 7, 135742–135756. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Characteristic | Male (n = 30) | Female (n = 19) | Total (n = 49) | |
|---|---|---|---|---|
| Age (year) | Mean +/− SD | 52.10 +/− 9.63 | 59.58 +/− 9.56 | 55.01 +/− 10.19 |
| Range | 27–66 | 37–74 | 27–74 | |
| Height (meter) | Mean +/− SD | 182.7 +/− 6.38 | 165.8 +/− 5.50 | 176.2 +/− 10.24 |
| Range | 171–198 | 158–178 | 158–198 | |
| Weight (Kg) | Mean +/− SD | 98.10 +/− 13.77 | 89.37 +/− 25.40 | 94.71 +/− 19.36 |
| Range | 75.20–125.00 | 60.60–150.40 | 60.60–150.40 | |
| BMI (kg × m−2) | Mean +/− SD | 29.43 +/− 4.23 | 32.37 +/− 8.49 | 30.57 +/− 6.32 |
| Range | 21.63–41.04 | 22.61–52.04 | 21.36–52.04 | |
| Underweight (BMI < 18.5) | 0 | 0 | 0 | |
| Normal (BMI 18.5–24.9) | 4 | 4 | 8 | |
| Pre-obesity (BMI 25.0–29,9) | 11 | 5 | 16 | |
| Obesity (BMI > 29.9) | 15 | 10 | 25 | |
| Skin color type | Mean +/− SD | 2.60 +/− 0.62 | 2.37 +/− 0.76 | 2.51 +/− 0.68 |
| Range | 1.0–4.0 | 1.0–4.0 | 1.0–4.0 | |
| Activity level | Mean +/− SD | 4.9 +/− 2.59 | 4.63 +/− 2.71 | 4.80 +/− 2.61 |
| Range | 0.0–9.0 | 1.0–9.0 | 0.0–9.0 |
| Sleep Parameters | Definition |
| TIB | Time in bed in minutes from lights off to lights on. |
| TST | Total sleep time in minutes of NREM (N1, N2 and N3) + REM from lights off to lights on in the morning. |
| Awake | Total time in minutes in absence of any NREM stage and REM from lights off to lights on (WASO + SOL). |
| WASO | Time in minutes of wakefulness after sleep onset. |
| SOL | Time in minutes from lights off to the first epoch of sleep scored. |
| SE | Percentage of sleep time from lights off to lights on (TST/TIB × 100). |
| Sleep cycle | One sleep cycle consists of an individual sequence of NREM and REM sleep, expressed in total numbers. |
| Sleep Stages | Definition |
| Light sleep | Sleep stages NREM1 + NREM2, expressed in minutes. |
| Deep sleep | Sleep stage NREM3 (also termed slow-wave sleep; SWS), expressed in minutes. |
| REM sleep | Characterized by rapid eye movements and EMG decrement, expressed in minutes. |
| Vital Parameters | Definition |
| HR | Heart rate, measured in beats per minute. |
| HRV | Heart rate variability, RMSSD (root mean square of successive differences) measured in 5 min intervals, expressed in milliseconds. |
| Beat to beat | Average delta of R–R intervals in milliseconds. |
| SpO2 | Measurement of arterial oxygen saturation in percent %. |
| Respiratory rate | Defined as respiratory cycles per minute. |
| Sleep Parameters | MAE | MAPE % | Min | Max | SD +/− | |
|---|---|---|---|---|---|---|
| TIB (in minutes) | Garmin vs. PSG | 26.94 | 6.32 | 0.00 | 110.00 | 29.67 |
| Polar vs. PSG | 34.00 | 7.53 | 0.00 | 201.00 | 45.39 | |
| ActiGraph GT9X vs. PSG | 0.92 | 0.21 | 0.00 | 18.00 | 2.70 | |
| Garmin vs. Polar | 49.22 | 13.48 | 0.00 | 197.00 | 51.82 | |
| TST (in minutes) | Garmin vs. PSG | 84.63 | 25.32 | 0.00 | 252.00 | 52.28 |
| Polar vs. PSG | 45.08 | 13.80 | 1.00 | 172.00 | 45.60 | |
| ActiGraph GT9X vs. PSG | 31.39 | 9.33 | 1.00 | 139.00 | 29.17 | |
| Garmin vs. Polar | 60.29 | 17.43 | 2.00 | 200.00 | 53.29 | |
| Awake (in minutes) | Garmin vs. PSG | 60.53 | 76.03 | 3.00 | 176.00 | 47.55 |
| Polar vs. PSG | 50.04 | 41.06 | 14.00 | 188.00 | 39.77 | |
| ActiGraph GT9X vs. PSG | 31.24 | 64.89 | 0.00 | 140.00 | 29.43 | |
| Garmin vs. Polar | 37.84 | 70.81 | 1.00 | 177.00 | 37.76 | |
| WASO (in minutes) | Garmin vs. PSG | 50.35 | 83.02 | 5.00 | 154.00 | 41.94 |
| Polar vs. PSG | 38.24 | 62.38 | 0.00 | 145.00 | 36.43 | |
| ActiGraph GT9X vs. PSG | 28.51 | 84.79 | 0.00 | 130.00 | 26.47 | |
| Garmin vs. Polar | 18.18 | 74.83 | 2.00 | 44.00 | 10.38 | |
| SOL (in minutes) | Garmin vs. PSG | 12.16 | 72.09 | 0.00 | 50.00 | 11.41 |
| Polar vs. PSG | 21.71 | 141.61 | 1.00 | 161.00 | 28.40 | |
| ActiGraph GT9X vs. PSG | 11.67 | 70.41 | 0.00 | 53.00 | 11.67 | |
| Garmin vs. Polar | 24.02 | 105.31 | 0.00 | 163.00 | 34.62 | |
| SE (in %) | Garmin vs. PSG | 11.67 | 15.30 | 0.15 | 40.06 | 10.05 |
| Polar vs. PSG | 8.68 | 11.56 | 0.22 | 37.81 | 8.60 | |
| ActiGraph GT9X vs. PSG | 6.99 | 8.65 | 0.03 | 32.22 | 5.94 | |
| Garmin vs. Polar | 4.44 | 4.78 | 0.12 | 11.26 | 2.61 |
| Sleep Parameters | F-Value (p-Value)/ ή2-Value | Devices | Mean Diff. | SD+/− | p-Value | 95% CI | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| TIB (in minutes) | F = 6.758 (p = 0.000)/ ή2 = 0.096 | Garmin vs. PSG | 17.27 | 36.29 | 0.367 | −10.04 | 44.58 |
| Polar vs. PSG | −25.84 | 50.58 | 0.072 | −53.15 | 1.47 | ||
| ActiGraph GT9X vs. PSG | 0.67 | 2.77 | 1.000 | −26.64 | 27.98 | ||
| Garmin vs. Polar | 43.11 | 57.12 | 0.000 | 15.79 | 70.41 | ||
| TST (in minutes) | F = 25.021 (p = 0.000)/ ή2 = 0.281 | Garmin vs. PSG | 83 | 54.76 | 0.000 | 53.49 | 112.67 |
| Polar vs. PSG | 24.43 | 59.54 | 0.147 | −5.16 | 54.02 | ||
| ActiGraph GT9X vs. PSG | 10.41 | 41.78 | 0.805 | −19.18 | 40.00 | ||
| Garmin vs. Polar | 59 | 55.12 | 0.000 | 29.06 | 88.24 | ||
| Awake (in minutes) | F = 48.024 (p = 0.000)/ ή2 = 0.429 | Garmin vs. PSG | −60.25 | 47.92 | 0.000 | −81.73 | −38.76 |
| Polar vs. PSG | −26.04 | 52.57 | 0.010 | −47.53 | −4.55 | ||
| ActiGraph GT9X vs. PSG | −11.00 | 41.70 | 0.556 | −32.49 | 10.49 | ||
| Garmin vs. Polar | −34.20 | 41.14 | 0.000 | −55.69 | −12.72 | ||
| WASO (in minutes) | F = 36.138 (p = 0.000)/ ή2 = 0.361 | Garmin vs. PSG | −49.86 | 42.53 | 0.000 | −66.50 | −33.22 |
| Polar vs. PSG | −34.16 | 40.36 | 0.000 | −50.80 | −17.52 | ||
| ActiGraph GT9X vs. PSG | −0.02 | 39.12 | 1.000 | −16.66 | 16.62 | ||
| Garmin vs. Polar | −15.69 | 13.92 | 0.073 | −32.34 | 0.95 | ||
| SOL (in minutes) | F = 9.612 (p = 0.000)/ ή2 = 0.131 | Garmin vs. PSG | −10.39 | 13.10 | 0.000 | −14.15 | −6.63 |
| Polar vs. PSG | 8.12 | 34.81 | 0.292 | −3.69 | 19.93 | ||
| ActiGraph GT9X vs. PSG | −10.98 | 12.34 | 0.000 | −14.52 | −7.43 | ||
| Garmin vs. Polar | −18.51 | 37.85 | 0.000 | −30.32 | −6.70 | ||
| SE (in %) | F = 39.407 (p = 0.000)/ ή2 = 0.381 | Garmin vs. PSG | 14.86 | 10.05 | 0.000 | 10.81 | 18.91 |
| Polar vs. PSG | 10.83 | 9.56 | 0.000 | 6.78 | 14.88 | ||
| ActiGraph GT9X vs. PSG | 2.31 | 9.19 | 0.461 | −1.74 | 6.36 | ||
| Garmin vs. Polar | 4.03 | 3.21 | 0.052 | −0.02 | 8.08 | ||
| Sleep Stages | MAE | MAPE % | Min | Max | SD +/− | |
|---|---|---|---|---|---|---|
| Light sleep (in minutes) | Garmin vs. PSG | 64.94 | 30.08 | 0.00 | 197.00 | 42.01 |
| Polar vs. PSG | 40.14 | 18.24 | 1.00 | 116.00 | 27.69 | |
| Garmin vs. Polar | 57.98 | 26.75 | 1.00 | 239.00 | 49.89 | |
| Deep sleep (in minutes) | Garmin vs. PSG | 47.33 | 116.50 | 0.00 | 179.00 | 38.55 |
| Polar vs. PSG | 28.06 | 87.36 | 2.00 | 78.00 | 19.09 | |
| Garmin vs. Polar | 54.04 | 91.66 | 1.00 | 189.00 | 40.89 | |
| REM sleep (in minutes) | Garmin vs. PSG | 53.10 | 97.54 | 4.00 | 180.00 | 35.29 |
| Polar vs. PSG | 24.80 | 49.13 | 0.00 | 88.00 | 21.37 | |
| Garmin vs. Polar | 45.69 | 61.64 | 1.00 | 145.00 | 33.33 | |
| Sleep cycle (total number) | Garmin vs. PSG | 1.14 | 32.66 | 0.00 | 4.00 | 1.00 |
| Polar vs. PSG | 1.12 | 33.25 | 0.00 | 4.00 | 0.99 | |
| Garmin vs. Polar | 1.04 | 22.41 | 0.00 | 3.00 | 0.93 |
| Sleep Stages | Mean Diff. | SD+/− | t-Value z-Value | p-Value | d-Value | 95% CI | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Light sleep (in minutes) | Garmin vs. PSG | 52.20 | 57.34 | 6.374 | 0.000 | 1.840 | 26.91 | 77.50 |
| Polar vs. PSG | 9.73 | 48.12 | 1.416 | 0.637 | 0.409 | −15.56 | 35.03 | |
| Garmin vs. Polar | 42.47 | 63.87 | 4.654 | 0.000 | 1.343 | 17.18 | 67.76 | |
| Deep sleep (in minutes) | Garmin vs. PSG | 17.29 | 58.88 | 2.055 | 0.045 | 0.593 | 0.37 | 34.20 |
| Polar vs. PSG | 7.92 | 33.26 | 1.667 | 0.632 | 0.481 | −12.51 | 28.34 | |
| Garmin vs. Polar | 9.37 | 67.57 | 0.970 | 0.337 | 0.280 | −10.04 | 28.78 | |
| REM sleep (in minutes) | Garmin vs. PSG | 11.84 | 63.10 | 1.313 | 0.351 | 0.379 | −8.31 | 31.98 |
| Polar vs. PSG | 4.71 | 32.58 | 1.013 | 0.846 | 0.292 | −15.43 | 24.86 | |
| Garmin vs. Polar | 7.12 | 56.48 | 0.883 | 0.683 | 0.255 | −13.02 | 27.27 | |
| Sleep cycle (total numbers) | Garmin vs. PSG | 0.76 | 1.63 | −2.981z | 0.003 | 0.658 | 0.20 | 1.31 |
| Polar vs. PSG | 1.10 | 1.37 | −4.572z | 0.000 | 1.036 | 0.55 | 1.65 | |
| Garmin vs. Polar | −0.35 | 1.36 | −1.797z | 0.072 | 0.318 | −0.90 | 0.20 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budig, M.; Stoohs, R.; Keiner, M. Validity of Two Consumer Multisport Activity Tracker and One Accelerometer against Polysomnography for Measuring Sleep Parameters and Vital Data in a Laboratory Setting in Sleep Patients. Sensors 2022, 22, 9540. https://doi.org/10.3390/s22239540
Budig M, Stoohs R, Keiner M. Validity of Two Consumer Multisport Activity Tracker and One Accelerometer against Polysomnography for Measuring Sleep Parameters and Vital Data in a Laboratory Setting in Sleep Patients. Sensors. 2022; 22(23):9540. https://doi.org/10.3390/s22239540
Chicago/Turabian StyleBudig, Mario, Riccardo Stoohs, and Michael Keiner. 2022. "Validity of Two Consumer Multisport Activity Tracker and One Accelerometer against Polysomnography for Measuring Sleep Parameters and Vital Data in a Laboratory Setting in Sleep Patients" Sensors 22, no. 23: 9540. https://doi.org/10.3390/s22239540
APA StyleBudig, M., Stoohs, R., & Keiner, M. (2022). Validity of Two Consumer Multisport Activity Tracker and One Accelerometer against Polysomnography for Measuring Sleep Parameters and Vital Data in a Laboratory Setting in Sleep Patients. Sensors, 22(23), 9540. https://doi.org/10.3390/s22239540