


A Systematic Review of Internet of Things in Clinical Laboratories: Opportunities, Advantages, and Challenges

 , ,
, ,  , and
, and
Abstract
1. Background
1.1. Defining IoT
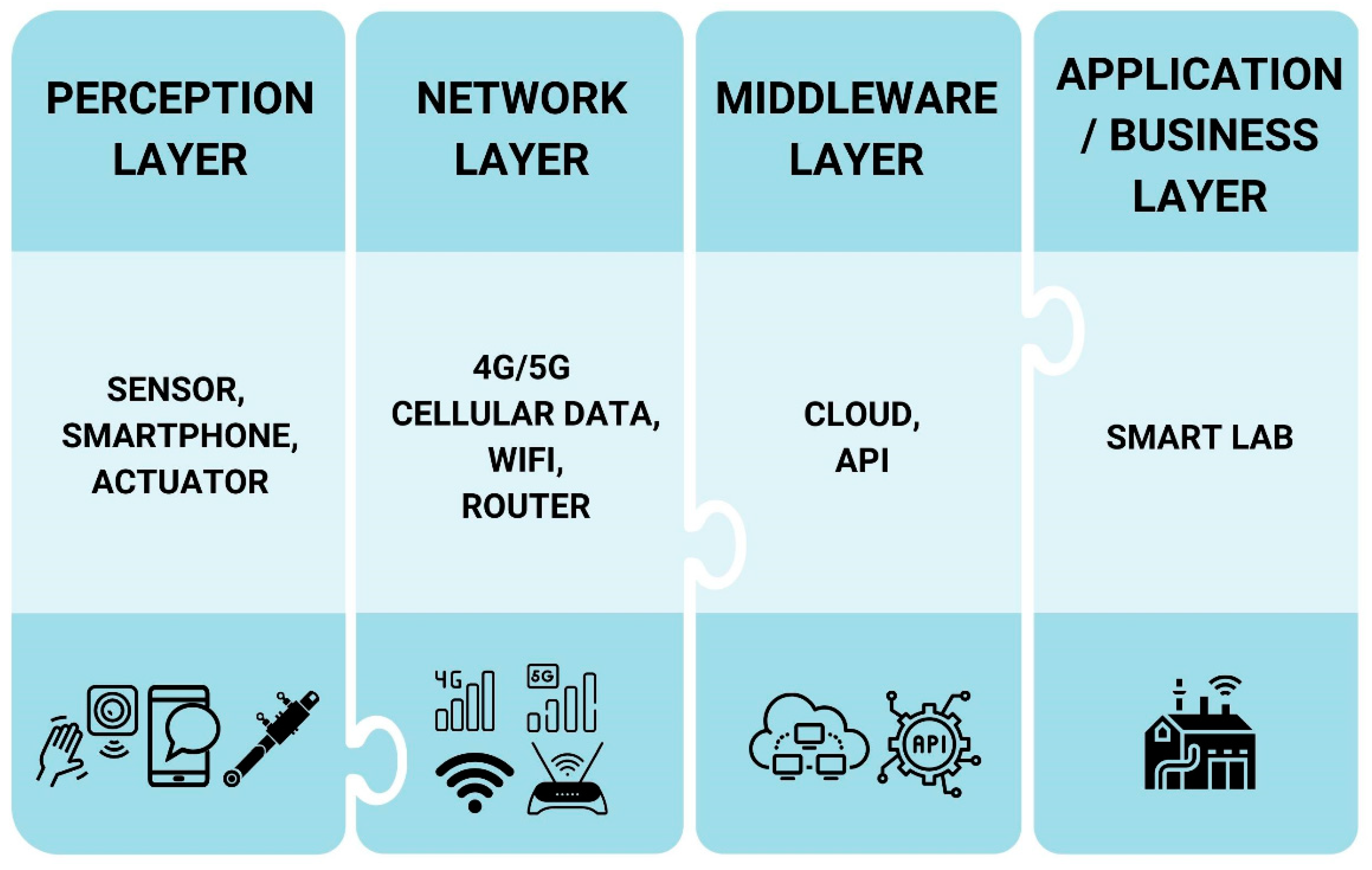
1.2. IoT Architecture
- Perception layer: The lowest layer of a conventional IoT architecture, this layer is also known as the sensor, physical, or hardware layer. It has sensors that collect physical signals or stimuli as data from various sensors, medical devices, or direct data entry from lab scientists. Once collected, the data are sent to the network layer.
- Network layer: This layer connects all smart devices and transmits clinical laboratory data from different users to the base station. Data may be securely transferred from other physical signals such as WiFi, Bluetooth, and Zigbee.
- Middleware layer: This layer, also known as the processing layer, stores, analyzes, and processes a huge set of data received from the network layer. Cloud computing is common for many technologies, whereas other databases may also be set up via this layer. Data analysis tools such as deep learning and lab protocol automation may be performed through this layer.
- Application/business layer: This layer delivers specific services to users, such as smart labs. It also includes applications, business models, and users’ privacy. This layer can be used for decision making by patients, hospitals, or lab scientists.
1.3. Approaches and Scopes of IoT
- Sensor-based approaches: this approach can be divided into two different categories, including wearable or environmental sensors.
- Resource-based approaches: this approach can be divided into five different categories, including scheduling, resource allocation, offloading, load balancing, and provisioning.
- Communication-based approaches: this approach can be divided into two categories, including technological and algorithmic.
- Application-based systems: this approach can be divided into two components: monitoring and recommender systems.
- Security-based systems: this approach can be divided into four components, including privacy, access control, confidentiality, and trust.
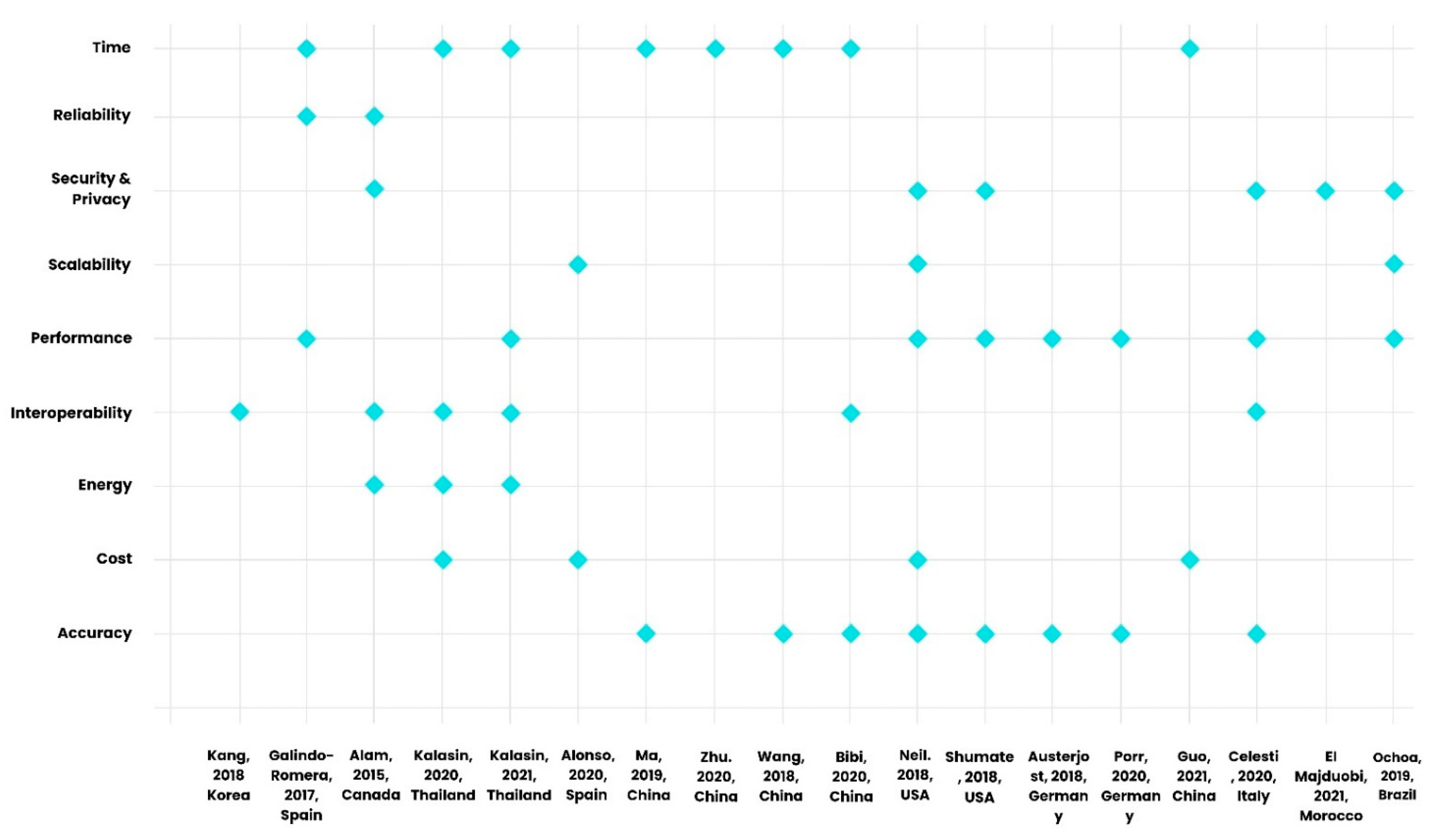
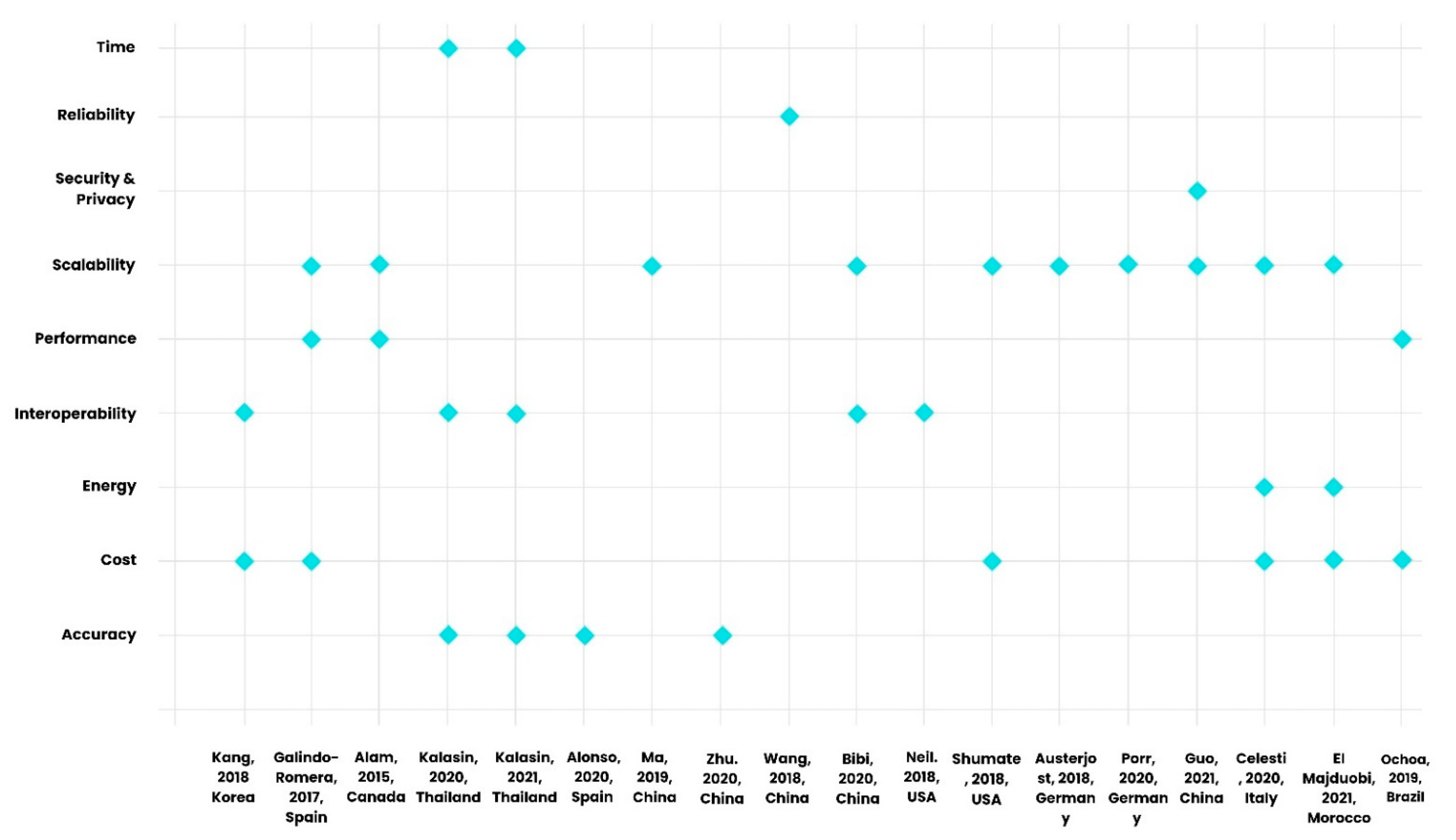
1.4. IoT Metrics
- Accuracy: In clinical laboratory systems, accuracy is essential for all users, including patients and lab scientists. Data accuracy in clinical laboratories refers to low error margins and high precision levels. Such precision must be considered when analyzing a data set, protocol criteria, and lab technique [35].
- Cost: This metric refers to the total expenses the clinical laboratory service user requires. The prices may include communication, sensors, network, hardware, software, and data processing [34].
- Energy: This metric assesses the energy resources required for data signaling and processing. As the “things” are interconnected in IoT, communication is the most energy-consuming task, increasing costs and emitting carbon into the environment [34].
- Interoperability: Interoperability is “the ability of two or more systems or components to exchange data and use information” across clinical laboratories and hospitals [34]. Communication between different systems requires unified and wide-spectrum protocols for interoperability as many heterogeneous systems exist, e.g., sensors, hardware, software, and service.
- Performance: Issues that may arise are related to network quality of service (QoS) parameters associated with the network layer, including latency, delivery rate, and bandwidth usage. Other considerations defined as performance are load balancing, resource utilization, overhead, and computational time. This metric is necessary during all stages, including data collection, processing, and service delivery [36].
- Scalability: This metric refers to the ability of the clinical laboratories to increase the total capacity when there is an increase in service demand without reducing the performance. Clinical laboratory systems can improve scalability by increasing the capability of existing and additional hardware or services [37]. Different types of scalability include vertical, which refers to increasing the capacity of existing hardware or software by adding more resources, and horizontal, which refers to scaling out by adding more nodes to a system by connecting multiple hardware or software [37].
- Security and privacy: Security and privacy are essential as a building block of IoT to protect clinical lab data. The lack of standardization and regulation the IoT has, however, may precipitate many security and privacy issues. Users such as lab technicians may not have the necessary insight to control, service, update, and address concerns such as cyber-attacks which are required to preserve the integrity of the devices or services. Measures including architectural resilience to attacks, data authentication, access control, and user privacy must be established to preserve security and privacy [38,39].
- Reliability: The ability to successfully deliver services required in clinical laboratory systems is defined as reliability. This metric assesses the ability of clinical laboratory systems to perform relevant tasks in the given time and conditions [40].
- Time: As the name suggests, this metric assesses the time required for service delivery. Different measures include run-time, computational time, average response time, and latency in clinical laboratory systems [41].
1.5. Review of Related Literature
1.5.1. Surveys
1.5.2. Case Studies
1.5.3. Systematic Literature Reviews
1.6. Aims and Objectives
1.7. Motivation for This Study
1.8. Structure
2. Materials and Methods
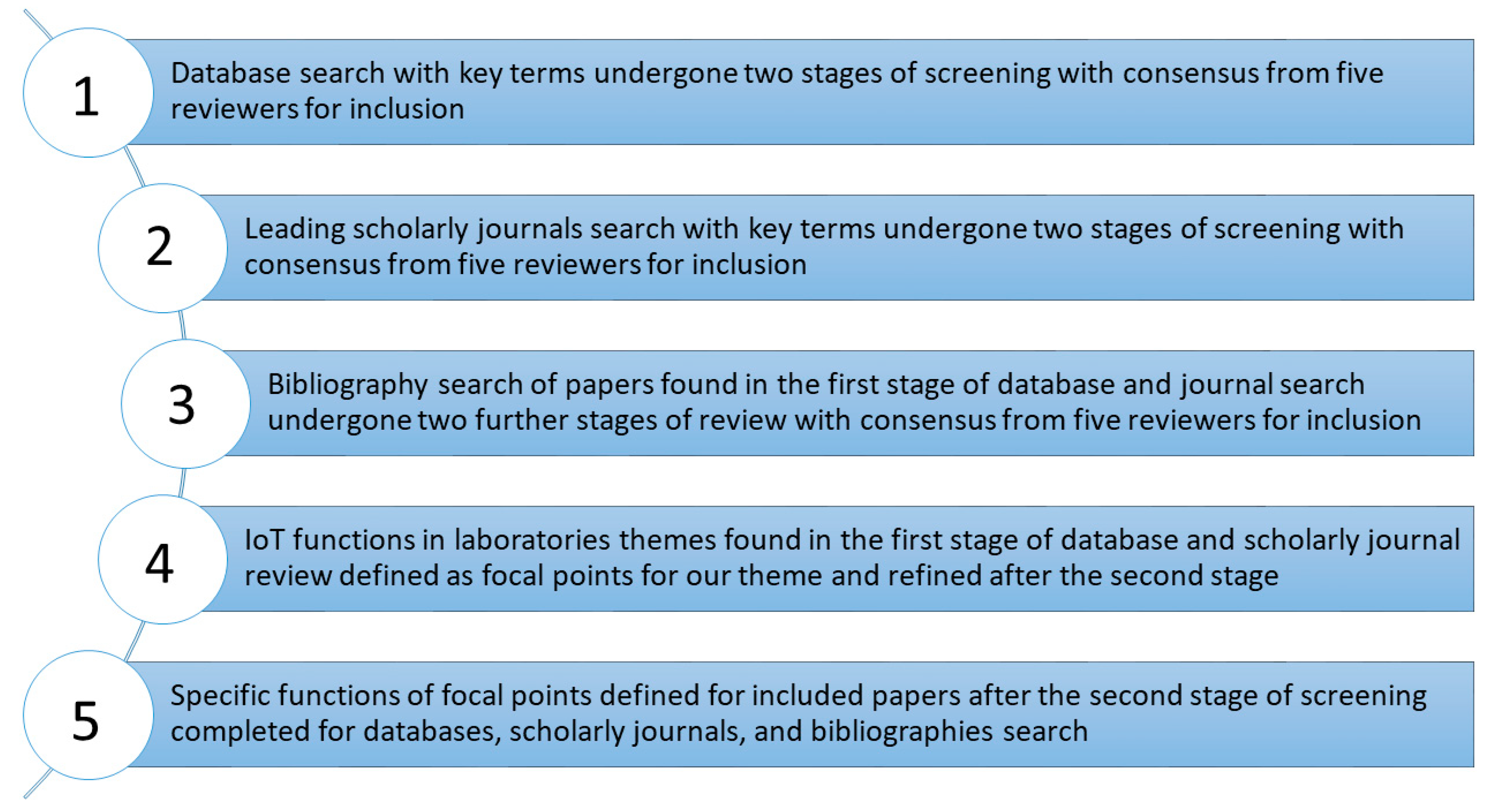
2.1. Theoretical Framework and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Synthesis
2.4. Critical Appraisal and Bias Assessment
3. Results
3.1. Risk of Bias
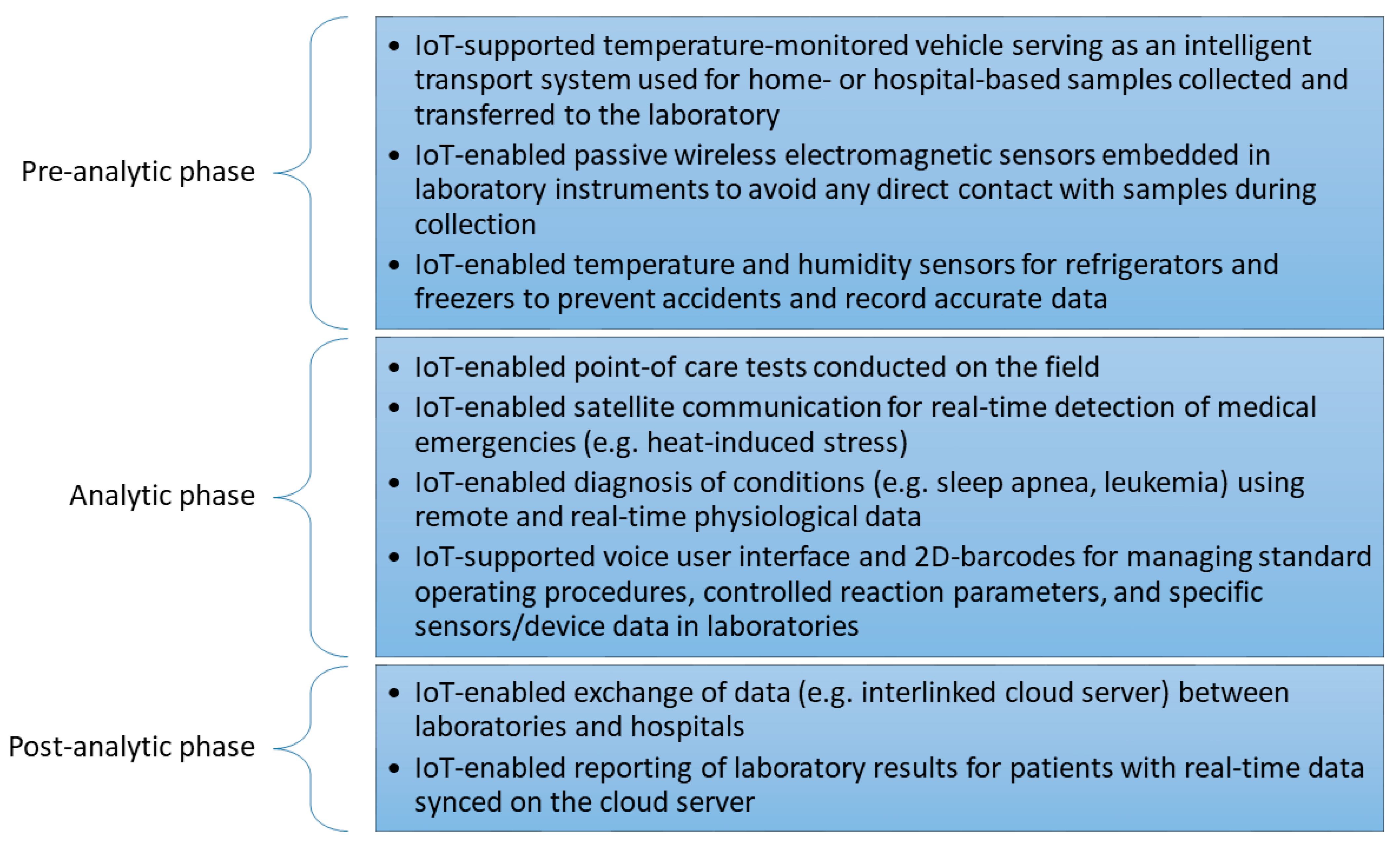
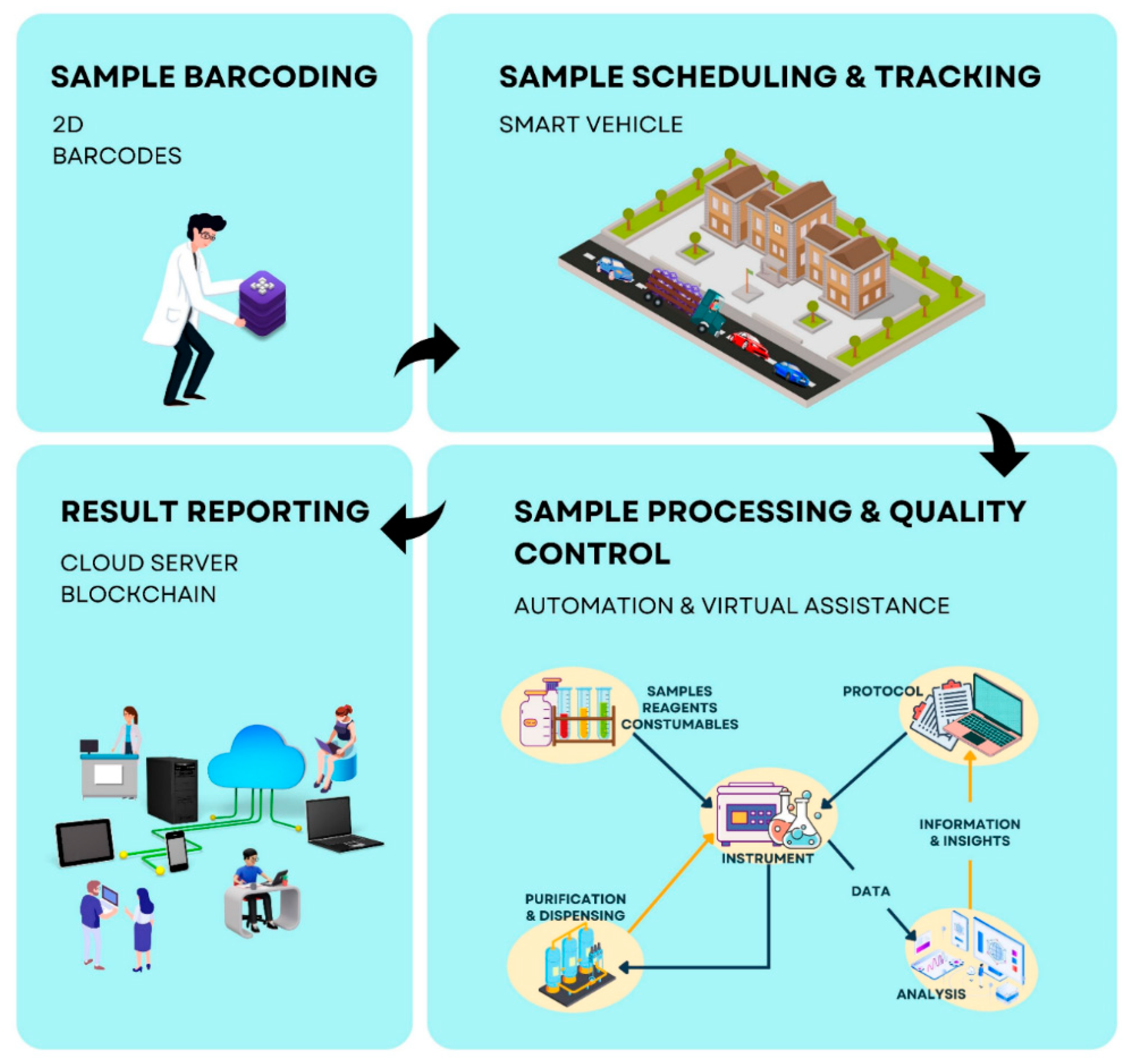
3.2. IoT in the Preanalytic Laboratory Phase
3.2.1. Clinical Laboratory Monitoring and Support
3.2.2. Smart Vehicle and Transport
3.3. IoT in the Analytic Laboratory Phase
3.3.1. IoT-Supported Point-of-Care Testing
3.3.2. Virtual Assistance and Quality Control of Central Laboratory Services
3.4. IoT in the Postanalytical Laboratory Phase
3.4.1. 5G-Enabled Data Sharing
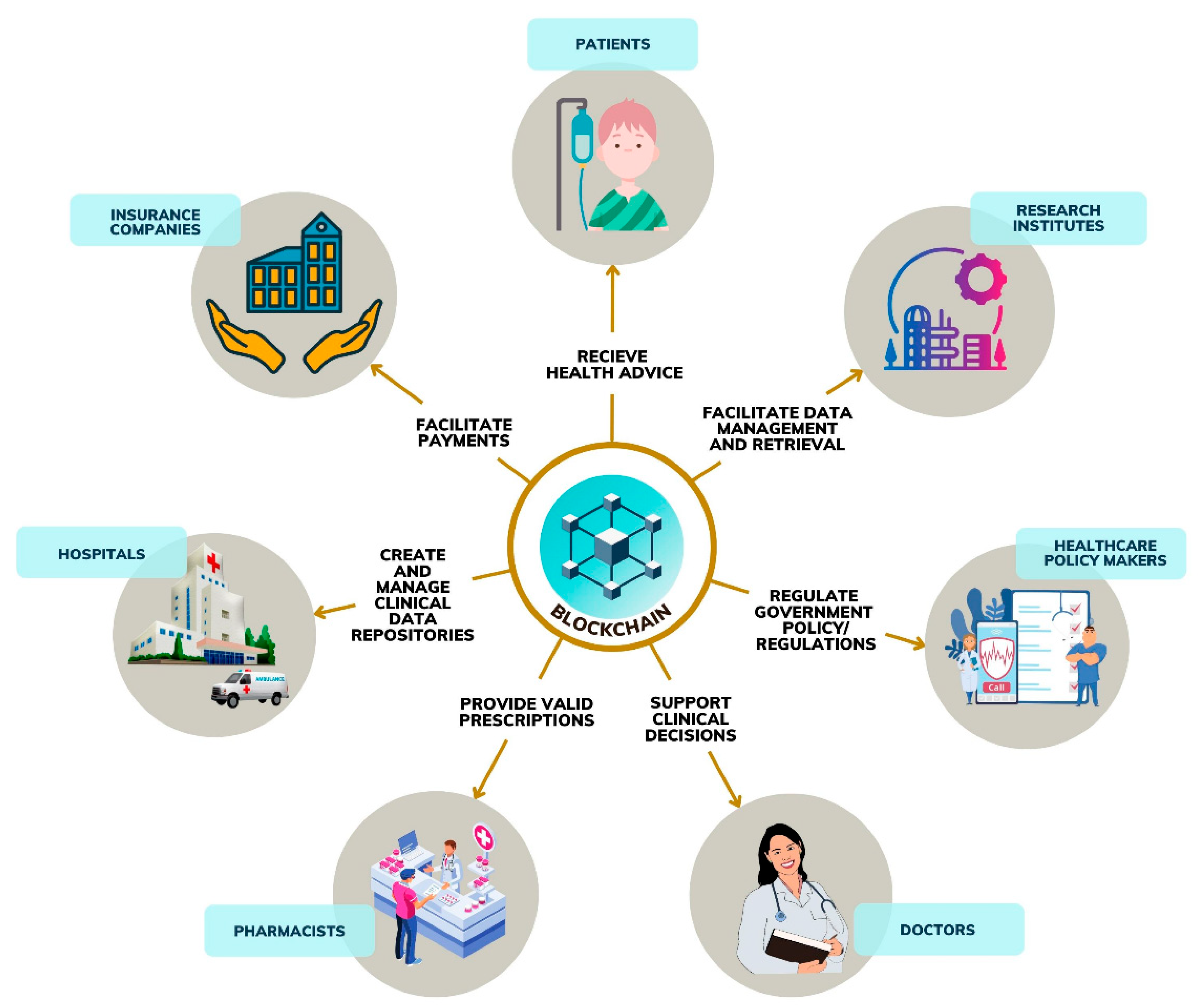
3.4.2. Blockchain-Enabled Data Sharing
4. Discussion
4.1. Open Concerns, Challenges, and Future Trends
4.1.1. Open Challenges and Concerns
4.1.2. Future Trends
- Clinical data sharing;
- Health consultation;
- Electronic health record (EHR) management;
- Pharmaceutical supply chain;
- Billing.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oztemel, E.; Gursev, S. Literature review of Industry 4.0 and related technologies. J. Intell. Manuf. 2018, 31, 127–182. [Google Scholar] [CrossRef]
- Sarfraz, Z.; Sarfraz, A.; Iftikar, H.M.; Akhund, R. Is COVID-19 pushing us to the Fifth Industrial Revolution (Society 5.0)? Pak. J. Med. Sci. 2021, 37, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Chettri, L.; Bera, R. A Comprehensive Survey on Internet of Things (IoT) Toward 5G Wireless Systems. IEEE Internet Things J. 2019, 7, 16–32. [Google Scholar] [CrossRef]
- Erboz, G. How to Define Industry 4.0: Main Pillars of Industry 4.0. Manag. Trends Dev. Enterp. Glob. Era 2017, 761, 767. [Google Scholar]
- Chui, M.; Ganesan, V.; Patel, M. Taking the Pulse of Enterprise IoT; McKinsey Global Institute: San Francisco, CA, USA, 2017. [Google Scholar]
- Parri, L.; Parrino, S.; Peruzzi, G.; Pozzebon, A. Low Power Wide Area Networks (LPWAN) at Sea: Performance Analysis of Offshore Data Transmission by Means of LoRaWAN Connectivity for Marine Monitoring Applications. Sensors 2019, 19, 3239. [Google Scholar] [CrossRef]
- Chen, H.; Abbas, R.; Cheng, P.; Shirvanimoghaddam, M.; Hardjawana, W.; Bao, W.; Li, Y.; Vucetic, B. Ultra-Reliable Low Latency Cellular Networks: Use Cases, Challenges and Approaches. IEEE Commun. Mag. 2018, 56, 119–125. [Google Scholar] [CrossRef]
- Li, Y.; Chi, Z.; Liu, X.; Zhu, T. Passive-zigbee: Enabling zigbee communication in Iot networks with 1000×+ less power consumption. In Proceedings of the 16th ACM Conference on Embedded Networked Sensor Systems, Shenzhen, China, 4–7 November 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 159–171. [Google Scholar]
- Nieminen, J.; Gomez, C.; Isomaki, M.; Savolainen, T.; Patil, B.; Shelby, Z.; Xi, M.; Oller, J. Networking solutions for connecting bluetooth low energy enabled machines to the internet of things. IEEE Netw. 2014, 28, 83–90. [Google Scholar] [CrossRef]
- Sheth, J.; Dezfouli, B. Enhancing the Energy-Efficiency and Timeliness of IoT Communication in WiFi Networks. IEEE Internet Things, J. 2019, 6, 9085–9097. [Google Scholar] [CrossRef]
- Alsharif, M.H.; Kim, S.; Kuruoğlu, N. Energy Harvesting Techniques for Wireless Sensor Networks/Radio-Frequency Identification: A Review. Symmetry 2019, 11, 865. [Google Scholar] [CrossRef]
- Razdan, S.; Sharma, S. Internet of Medical Things (IoMT): Overview, Emerging Technologies, and Case Studies. IETE Tech. Rev. 2021, 1–14. [Google Scholar] [CrossRef]
- Dwivedi, R.; Mehrotra, D.; Chandra, S. Potential of Internet of Medical Things (IoMT) applications in building a smart healthcare system: A systematic review. J. Oral Biol. Craniofacial Res. 2021, 12, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Joyia, G.J.; Liaqat, R.M.; Farooq, A.; Rehman, S. Internet of Medical Things (IOMT): Applications, Benefits and Future Challenges in Healthcare Domain. J. Commun. 2017, 12, 240–247. [Google Scholar] [CrossRef]
- Omboni, S.; Campolo, L.; Panzeri, E. Telehealth in chronic disease management and the role of the Internet-of-Medical-Things: The Tholomeus® experience. Expert Rev. Med. Devices 2020, 17, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Das, P.K.; Zhu, F.; Chen, S.; Luo, C.; Ranjan, P.; Xiong, G. Smart medical healthcare of internet of medical things (IOMT): Application of non-contact sensing. In Proceedings of the 2019 14th IEEE Conference on Industrial Electronics and Applications (ICIEA), Xi’an, China, 19–21 June 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 375–380. [Google Scholar]
- Ahmad, S.; Kim, D. A multi-device multi-tasks management and orchestration architecture for the design of enterprise IoT applications. Futur. Gener. Comput. Syst. 2019, 106, 482–500. [Google Scholar] [CrossRef]
- Darshan, K.R.; Anandakumar, K.R. A comprehensive review on usage of internet of things (IoT) in healthcare system. In Proceedings of the 2015 International Conference on Emerging Research in Electronics, Computer Science and Technology (ICERECT), Mandya, India, 17–19 December 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 132–136. [Google Scholar]
- Babu, B.S.; Srikanth, K.; Ramanjaneyulu, T.; Narayana, I.L. IoT for Healthcare. Int. J. Sci. Res. 2016, 5, 322–326. [Google Scholar]
- Kashani, M.H.; Madanipour, M.; Nikravan, M.; Asghari, P.; Mahdipour, E. A systematic review of IoT in healthcare: Applications, techniques, and trends. J. Netw. Comput. Appl. 2021, 192, 103164. [Google Scholar] [CrossRef]
- Tyagi, S.; Agarwal, A.; Maheshwari, P. A conceptual framework for IoT-based healthcare system using cloud computing. In Proceedings of the 2016 6th International Conference-Cloud System and Big Data Engineering (Confluence), Noida, India, 14–15 January 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 503–507. [Google Scholar]
- Mathew, P.S.; Pillai, A.S.; Palade, V. Applications of IoT in Healthcare. In Cognitive Computing for Big Data Systems Over IoT.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 263–288. [Google Scholar]
- Bigini, G.; Freschi, V.; Lattanzi, E. A Review on Blockchain for the Internet of Medical Things: Definitions, Challenges, Applications, and Vision. Futur. Internet 2020, 12, 208. [Google Scholar] [CrossRef]
- Irfan, M.; Ahmad, N. Internet of medical things: Architectural model, motivational factors and impediments. In Proceedings of the 2018 15th learning and technology conference (L&T), Jeddah, Saudi Arabia, 25–26 February 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 6–13. [Google Scholar]
- Huang, X.; Craig, P.; Lin, H.; Yan, Z. SecIoT: A security framework for the Internet of Things. Secur. Commun. Netw. 2015, 9, 3083–3094. [Google Scholar] [CrossRef]
- Madakam, S.; Lake, V.; Lake, V.; Lake, V. Internet of Things (IoT): A literature review. J. Comput. Commun. 2015, 3, 164. [Google Scholar] [CrossRef]
- Ornes, S. Core Concept: The Internet of Things and the Explosion of Interconnectivity. Proc. Natl. Acad. Sci. USA 2016, 113, 11059–11060. [Google Scholar] [CrossRef]
- Gigli, M.; Koo, S. Internet of Things: Services and Applications Categorization. Adv. Internet Things 2011, 1, 27–31. [Google Scholar] [CrossRef]
- Insight, F. Internet of Things-From Theory to Reality; Forbes Insight: Jersey City, NJ, USA, 2017. [Google Scholar]
- Al-Qaseemi, S.A.; Almulhim, H.A.; Almulhim, M.F.; Chaudhry, S.R. IoT architecture challenges and issues: Lack of standardization. In Proceedings of the 2016 Future Technologies Conference (FTC), San Francisco, CA, USA, 6–7 December 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 731–738. [Google Scholar]
- Ashton, K. That ‘Internet of Things’ Thing. RFID J. 2009, 22, 97–114. [Google Scholar]
- Sethi, P.; Sarangi, S.R. Internet of things: Architectures, protocols, and applications. J. Electr. Comput. Eng. 2017, 2017. [Google Scholar] [CrossRef]
- Zhu, Z.; Huang, R.-G. Study on the IoT architecture and access technology. In Proceedings of the 2017 16th International Symposium on Distributed Computing and Applications to Business, Engineering and Science (DCABES), AnYang, China, 13–16 October 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 113–116. [Google Scholar]
- Patel, K.K.; Patel, S.M. Internet of Things-IOT: Definition, Characteristics, Architecture, Enabling Technologies, Application & Future Challenges. Int. J. Eng. Sci. Comput. 2016, 6. [Google Scholar] [CrossRef]
- Vamvakas, E.C. Meta-analyses of studies of the diagnostic accuracy of laboratory tests: A review of the concepts and methods. Arch. Pathol. Lab. Med. 1998, 122, 675. [Google Scholar] [PubMed]
- Manishankar, S.; Srinithi, C.R.; Joseph, D. Comprehensive study of wireless networks qos parameters and comparing their performance based on real time scenario. In Proceedings of the 2017 International Conference on Innovations in Information, Embedded and Communication Systems (ICIIECS), Coimbatore, India, 17–18 March 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Gupta, A.; Christie, R.; Manjula, P.R. Scalability in Internet of Things: Features, Techniques and Research Challenges. Int. J. Comput. Intell. Res. 2017, 13, 1617–1627. [Google Scholar]
- Maple, C. Security and Privacy in the Internet of Things. J. Cyber Policy 2017, 2, 155–184. [Google Scholar] [CrossRef]
- Weber, R.H. Internet of Things–New Security and Privacy Challenges. Comput. law Secur. Rev. 2010, 26, 23–30. [Google Scholar] [CrossRef]
- Moore, S.J.; Nugent, C.D.; Zhang, S.; Cleland, I. IoT reliability: A review leading to 5 key research directions. CCF Trans. Pervasive Comput. Interact. 2020, 2, 147–163. [Google Scholar] [CrossRef]
- Kashani, M.H.; Rahmani, A.M.; Navimipour, N.J. Quality of service-aware approaches in fog computing. Int. J. Commun. Syst. 2020, 33, e4340. [Google Scholar] [CrossRef]
- Thilakarathne, N.; Kagita, M.K.; Gadekallu, T.R. The Role of the Internet of Things in Health Care: A Systematic and Comprehensive Study. Int. J. Eng. Manag. Res. 2020, 10, 145–159. [Google Scholar] [CrossRef]
- Dang, L.M.; Piran, J.; Han, D.; Min, K.; Moon, H. A Survey on Internet of Things and Cloud Computing for Healthcare. Electronics 2019, 8, 768. [Google Scholar] [CrossRef]
- Islam, S.M.R.; Kwak, D.; Kabir, M.H.; Hossain, M.; Kwak, K.-S. The Internet of Things for Health Care: A Comprehensive Survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Dhanvijay, M.M.; Patil, S.C. Internet of Things: A survey of enabling technologies in healthcare and its applications. Comput. Netw. 2019, 153, 113–131. [Google Scholar] [CrossRef]
- Yin, Y.; Zeng, Y.; Chen, X.; Fan, Y. The internet of things in healthcare: An overview. J. Ind. Inf. Integr. 2016, 1, 3–13. [Google Scholar] [CrossRef]
- Habibzadeh, H.; Dinesh, K.; Shishvan, O.R.; Boggio-Dandry, A.; Sharma, G.; Soyata, T. A Survey of Healthcare Internet of Things (HIoT): A Clinical Perspective. IEEE Internet Things J. 2019, 7, 53–71. [Google Scholar] [CrossRef]
- Bolhasani, H.; Mohseni, M.; Rahmani, A.M. Deep learning applications for IoT in health care: A systematic review. Inform. Med. Unlocked 2021, 23, 100550. [Google Scholar] [CrossRef]
- Fatoum, H.; Hanna, S.; Halamka, J.D.; Sicker, D.C.; Spangenberg, P.; Hashmi, S.K. Blockchain Integration With Digital Technology and the Future of Health Care Ecosystems: Systematic Review. J. Med. Internet Res. 2021, 23, e19846. [Google Scholar] [CrossRef]
- Sadoughi, F.; Behmanesh, A.; Sayfouri, N. Internet of things in medicine: A systematic mapping study. J. Biomed. Inform. 2020, 103, 103383. [Google Scholar] [CrossRef]
- Nasiri, S.; Sadoughi, F.; Tadayon, M.; Dehnad, A. Security Requirements of Internet of Things-Based Healthcare System: A Survey Study. Acta Inform. Med. 2019, 27, 253–258. [Google Scholar] [CrossRef]
- Webster, J.; Watson, R.T. Analyzing the Past to Prepare for the Future: Writing a Literature Review. MIS Q. 2002, xiii–xxiii. [Google Scholar]
- Leidner, D.; Kayworth, T. Review: A Review of Culture in Information Systems Research: Toward a Theory of Information Technology Culture Conflict. MIS Q. 2006, 30, 357. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McArthur, A.; Klugarová, J.; Yan, H.; Florescu, S. Innovations in the systematic review of text and opinion. Int. J. Evid. -Based Health 2015, 13, 188–195. [Google Scholar] [CrossRef]
- Kang, S.; Baek, H.; Jun, S.; Choi, S.; Hwang, H.; Yoo, S. Laboratory Environment Monitoring: Implementation Experience and Field Study in a Tertiary General Hospital. Health Inform. Res. 2018, 24, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Romera, G.; Carnerero-Cano, J.; Martínez-Martínez, J.J.; Herraiz-Martínez, F.J. An IoT Reader for Wireless Passive Electromagnetic Sensors. Sensors 2017, 17, 693. [Google Scholar] [CrossRef]
- Alam, K.M.; Saini, M.; Saddik, A. El Workload Model Based Dynamic Adaptation of Social Internet of Vehicles. Sensors 2015, 15, 23262–23285. [Google Scholar] [CrossRef]
- Kalasin, S.; Sangnuang, P.; Khownarumit, P.; Tang, I.M.; Surareungchai, W. Salivary Creatinine Detection Using a Cu (I)/Cu (II) Catalyst Layer of a Supercapacitive Hybrid Sensor: A Wireless IoT Device To Monitor Kidney Diseases for Remote Medical Mobility. ACS Biomater. Sci. Eng. 2020, 6, 5895–5910. [Google Scholar] [CrossRef]
- Kalasin, S.; Sangnuang, P.; Surareungchai, W. Satellite-Based Sensor for Environmental Heat-Stress Sweat Creatinine Monitoring: The Remote Artificial Intelligence-Assisted Epidermal Wearable Sensing for Health Evaluation. ACS Biomater. Sci. Eng. 2020, 7, 322–334. [Google Scholar] [CrossRef]
- Alonso, O.; Franch, N.; Canals, J.; Arias-Alpízar, K.; de la Serna, E.; Baldrich, E.; Diéguez, A. An internet of things-based intensity and time-resolved fluorescence reader for point-of-care testing. Biosens. Bioelectron. 2020, 154, 112074. [Google Scholar] [CrossRef]
- Ma, B.; Wu, Z.; Li, S.; Benton, R.; Li, D.; Huang, Y.; Kasukurthi, M.V.; Lin, J.; Borchert, G.M.; Tan, S.; et al. Development of a support vector machine learning and smart phone Internet of Things-based architecture for real-time sleep apnea diagnosis. BMC Med. Inform. Decis. Mak. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Podesva, P.; Liu, X.; Zhang, H.; Teply, T.; Xu, Y.; Chang, H.; Qian, A.; Lei, Y.; Li, Y.; et al. IoT PCR for pandemic disease detection and its spread monitoring. Sens. Actuators B Chem. 2020, 303, 127098. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tao, Y.; Liu, Y.; Zhao, Y.; Song, C.; Zhou, B.; Wang, T.; Gao, L.; Zhang, L.; Hu, H. Rapid detection of urinary soluble intercellular adhesion molecule-1 for determination of lupus nephritis activity. Medicine 2018, 97, e11287. [Google Scholar] [CrossRef] [PubMed]
- Bibi, N.; Sikandar, M.; Ud Din, I.; Almogren, A.; Ali, S. IoMT-Based Automated Detection and Classification of Leukemia Using Deep Learning. J. Healthc. Eng. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Neil, W.; Zipp, G.; Nemeth, G.; Russo, M.F.; Nirschl, D.S. End-to-End Sample Tracking in the Laboratory Using a Custom Internet of Things Device. SLAS Technol. Transl. Life Sci. Innov. 2018, 23, 412–422. [Google Scholar] [CrossRef]
- Shumate, J.; Baillargeon, P.; Spicer, T.P.; Scampavia, L. IoT for Real-Time Measurement of High-Throughput Liquid Dispensing in Laboratory Environments. SLAS Technol. Transl. Life Sci. Innov. 2018, 23, 440–447. [Google Scholar] [CrossRef]
- Austerjost, J.; Porr, M.; Riedel, N.; Geier, D.; Becker, T.; Scheper, T.; Marquard, D.; Lindner, P.; Beutel, S. Introducing a Virtual Assistant to the Lab: A Voice User Interface for the Intuitive Control of Laboratory Instruments. SLAS Technol. Transl. Life Sci. Innov. 2018, 23, 476–482. [Google Scholar] [CrossRef]
- Porr, M.; Lange, F.; Marquard, D.; Niemeyer, L.; Lindner, P.; Scheper, T.; Beutel, S. Implementing a digital infrastructure for the lab using a central laboratory server and the SiLA2 communication standard. Eng. Life Sci. 2020, 21, 208–219. [Google Scholar] [CrossRef]
- Guo, J.; Chen, S.; Tian, S.; Liu, K.; Ni, J.; Zhao, M.; Kang, Y.; Ma, X.; Guo, J. 5G-enabled ultra-sensitive fluorescence sensor for proactive prognosis of COVID-19. Biosens. Bioelectron. 2021, 181, 113160. [Google Scholar] [CrossRef]
- Celesti, A.; Ruggeri, A.; Fazio, M.; Galletta, A.; Villari, M.; Romano, A. Blockchain-Based Healthcare Workflow for Tele-Medical Laboratory in Federated Hospital IoT Clouds. Sensors 2020, 20, 2590. [Google Scholar] [CrossRef]
- El Majdoubi, D.; El Bakkali, H.; Sadki, S. SmartMedChain: A Blockchain-Based Privacy-Preserving Smart Healthcare Framework. J. Health Eng. 2021, 2021, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Ochôa, I.S.; Silva, L.A.; de Mello, G.; da Silva, B.A.; de Paz, J.F.; González, G.V.; Garcia, N.M.; Leithardt, V.R.Q. PRICHAIN: A Partially Decentralized Implementation of UbiPri Middleware Using Blockchain. Sensors 2019, 19, 4483. [Google Scholar] [CrossRef] [PubMed]
- Elkhodr, M.; Shahrestani, S.; Cheung, H. Emerging Wireless Technologies in the Internet of Things: A Comparative Study. Int. J. Wirel. Mob. Netw. 2016, 8, 67–82. [Google Scholar] [CrossRef]
- Chavez-Santiago, R.; Nolan, K.E.; Holland, O.; De Nardis, L.; Ferro, J.M.; Barroca, N.; Borges, L.M.; Velez, F.J.; Goncalves, V.; Balasingham, I. Cognitive radio for medical body area networks using ultra wideband. IEEE Wirel. Commun. 2012, 19, 74–81. [Google Scholar] [CrossRef]
- Kreutz, D.; Ramos, F.M.V.; Verissimo, P.E.; Rothenberg, C.E.; Azodolmolky, S.; Uhlig, S. Software-Defined Networking: A Comprehensive Survey. Proc. IEEE 2015, 103, 14–76. [Google Scholar] [CrossRef]
- Li, Y.; Chen, M. Software-Defined Network Function Virtualization: A Survey. IEEE Access 2015, 3, 2542–2553. [Google Scholar] [CrossRef]
- Ray, P.P. A survey of IoT cloud platforms. Futur. Comput. Inform. J. 2016, 1, 35–46. [Google Scholar] [CrossRef]
- Markovic, D.S.; Zivkovic, D.; Branovic, I.; Popovic, R.; Cvetkovic, D. Smart power grid and cloud computing. Renew. Sustain. Energy Rev. 2013, 24, 566–577. [Google Scholar] [CrossRef]
- Weisbecker, A.; Falkner, J.; Rienhoff, O. MediGRID–grid computing for medicine and life sciences. In Proceedings of the Grid Computing, Taipei, Taiwan, 28 March 2007; Springer: Berlin/Heidelberg, Germany, 2009; pp. 57–65. [Google Scholar]
- Yi, S.; Li, C.; Li, Q. A survey of fog computing: Concepts, applications and issues. In Proceedings of the 2015 Workshop on Mobile Big Data, Hangzhou China, 21 June 2015; Association for Computing Machinery: New York, NY, USA, 2015; pp. 37–42. [Google Scholar]
- Iorga, M.; Feldman, L.; Barton, R.; Martin, M.J.; Goren, N.; Mahmoudi, C. Fog Computing Conceptual Model; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2018. [Google Scholar] [CrossRef]
- Vaquero, L.M.; Rodero-Merino, L. Finding Your Way in the Fog: Towards a Comprehensive Definition of Fog Computing. ACM SIGCOMM Comput. Commun. Rev. 2014, 44, 27–32. [Google Scholar] [CrossRef]
- Mahmud, R.; Kotagiri, R.; Buyya, R. Fog Computing: A Taxonomy, Survey and Future Directions. In Internet of Everything; Springer: Berlin/Heidelberg, Germany, 2018; pp. 103–130. [Google Scholar]
- Miloslavskaya, N.; Tolstoy, A. Big Data, Fast Data and Data Lake Concepts. Procedia Comput. Sci. 2016, 88, 300–305. [Google Scholar] [CrossRef]
- Wolfert, S.; Ge, L.; Verdouw, C.; Bogaardt, M.-J. Big Data in Smart Farming–a Review. Agric. Syst. 2017, 153, 69–80. [Google Scholar] [CrossRef]
- Sousa, M.J.; Pesqueira, A.M.; Lemos, C.; Sousa, M.; Rocha, Á. Decision-Making Based on Big Data Analytics for People Management in Healthcare Organizations. J. Med. Syst. 2019, 43, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Madanian, S.; Parry, D.T.; Airehrour, D.; Cherrington, M. mHealth and big-data integration: Promises for healthcare system in India. BMJ Health Care Inform. 2019, 26, e100071. [Google Scholar] [CrossRef]
- Muniswamaiah, M.; Agerwala, T.; Tappert, C. Big Data in Cloud Computing Review and Opportunities. Int. J. Comput. Sci. Inf. Technol. 2019, 11, 43–57. [Google Scholar] [CrossRef]
- Lv, Z.; Qiao, L. Analysis of healthcare big data. Futur. Gener. Comput. Syst. 2020, 109, 103–110. [Google Scholar] [CrossRef]
- Marjani, M.; Nasaruddin, F.; Gani, A.; Karim, A.; Hashem, I.A.T.; Siddiqa, A.; Yaqoob, I. Big IoT Data Analytics: Architecture, Opportunities, and Open Research Challenges. IEEE Access 2017, 5, 5247–5261. [Google Scholar] [CrossRef]
- Yaacoub, J.-P.A.; Noura, M.; Noura, H.N.; Salman, O.; Yaacoub, E.; Couturier, R.; Chehab, A. Securing internet of medical things systems: Limitations, issues and recommendations. Futur. Gener. Comput. Syst. 2019, 105, 581–606. [Google Scholar] [CrossRef]
- Berger, C.; Eichhammer, P.; Reiser, H.P.; Domaschka, J.; Hauck, F.J.; Habiger, G. A Survey on Resilience in the IoT: Taxonomy, Classification, and Discussion of Resilience Mechanisms. ACM Comput. Surv. 2021, 54, 1–39. [Google Scholar] [CrossRef]
- Pal, S.; Hitchens, M.; Rabehaja, T.; Mukhopadhyay, S. Security Requirements for the Internet of Things: A Systematic Approach. Sensors 2020, 20, 5897. [Google Scholar] [CrossRef]
- Chacko, A.; Hayajneh, T. Security and Privacy Issues with IoT in Healthcare. EAI Endorsed Trans. Pervasive Health Technol. 2018, 4, e2. [Google Scholar] [CrossRef]
- Argaw, S.T.; Troncoso-Pastoriza, J.R.; Lacey, D.; Florin, M.-V.; Calcavecchia, F.; Anderson, D.; Burleson, W.; Vogel, J.-M.; O’Leary, C.; Eshaya-Chauvin, B.; et al. Cybersecurity of Hospitals: Discussing the challenges and working towards mitigating the risks. BMC Med. Inform. Decis. Mak. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kimani, K.; Oduol, V.; Langat, K. Cyber Security Challenges for IoT-Based Smart Grid Networks. Int. J. Crit. Infrastruct. Prot. 2019, 25, 36–49. [Google Scholar] [CrossRef]
- Uddin, A.; Stranieri, A.; Gondal, I.; Balasubramanian, V. A survey on the adoption of blockchain in IoT: Challenges and solutions. Blockchain Res. Appl. 2021, 2, 100006. [Google Scholar] [CrossRef]
- Ratta, P.; Kaur, A.; Sharma, S.; Shabaz, M.; Dhiman, G. Application of Blockchain and Internet of Things in Healthcare and Medical Sector: Applications, Challenges, and Future Perspectives. J. Food Qual. 2021, 2021, 1–20. [Google Scholar] [CrossRef]
- Yu, H.; Sun, H.; Wu, D.; Kuo, T.-T. Comparison of smart contract blockchains for healthcare applications. In Proceedings of the AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2019; Volume 2019, p. 1266. [Google Scholar]
- Ray, P.P.; Dash, D.; Salah, K.; Kumar, N. Blockchain for IoT-Based Healthcare: Background, Consensus, Platforms, and Use Cases. IEEE Syst. J. 2020, 15, 85–94. [Google Scholar] [CrossRef]
- Tang, X.; Yang, C.C. Identifing influential users in an online healthcare social network. In Proceedings of the 2010 IEEE International Conference on Intelligence and Security Informatics, Vancouver, BC, Canada, 23–26 May 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 43–48. [Google Scholar]
- Weitzman, E.R.; Kelemen, S.; Mandl, K.D. Surveillance of an Online Social Network to Assess Population-Level Diabetes Health Status and Healthcare Quality. Online J. Public Health Inform. 2011, 3. [Google Scholar] [CrossRef]
- Azizi, T. The Issues Surrounding Social Network Sites and Healthcare Professionals. J. Perioper. Pr. 2013, 23, 233–236. [Google Scholar] [CrossRef]
- Chao, Y.; Jiang, W.; Wang, X.; Wang, X.; Song, J.; Chen, C.; Zhou, J.; Huang, Q.; Hu, J.; Song, Y. Discovery of efficacy biomarkers for non-small cell lung cancer with first-line anti-PD-1 immunotherapy by data-independent acquisition mass spectrometry. Clin. Exp. Immunol. 2022, 208, 60–71. [Google Scholar] [CrossRef]
- Li, H.; Wang, Y.; Jiang, J.; Zhao, H.; Feng, X.; Zhao, B.; Wang, L. A Novel Human Microbe-Disease Association Prediction Method Based on the Bidirectional Weighted Network. Front. Microbiol. 2019, 10, 676. [Google Scholar] [CrossRef]
- Lin, D.; Wang, Y.; Wang, T.; Zhu, Y.; Lin, X.; Lin, Y.; Feng, S. Metabolite profiling of human blood by surface-enhanced Raman spectroscopy for surgery assessment and tumor screening in breast cancer. Anal. Bioanal. Chem. 2020, 412, 1611–1618. [Google Scholar] [CrossRef]
- Lin, D.; Wu, Q.; Qiu, S.; Chen, G.; Feng, S.; Chen, R.; Zeng, H. Label-free liquid biopsy based on blood circulating DNA detection using SERS-based nanotechnology for nasopharyngeal cancer screening. Nanomed. Nanotechnol. Biol. Med. 2019, 22, 102100. [Google Scholar] [CrossRef]
- Lin, X.; Wang, Y.; Wang, L.; Lu, Y.; Li, J.; Lu, D.; Zhou, T.; Huang, Z.; Huang, J.; Huang, H.; et al. Interference-free and high precision biosensor based on surface enhanced Raman spectroscopy integrated with surface molecularly imprinted polymer technology for tumor biomarker detection in human blood. Biosens. Bioelectron. 2019, 143, 111599. [Google Scholar] [CrossRef]
- Tong, T.; Gao, Q.; Guerrero, R.; Ledig, C.; Chen, L.; Rueckert, D.; Initiative, A.D.N. A Novel Grading Biomarker for the Prediction of Conversion From Mild Cognitive Impairment to Alzheimer’s Disease. IEEE Trans. Biomed. Eng. 2016, 64, 155–165. [Google Scholar] [CrossRef]
- Uehara, F.; Hori, K.; Hasegawa, Y.; Yoshimura, S.; Hori, S.; Kitamura, M.; Akazawa, K.; Ono, T. Impact of Masticatory Behaviors Measured With Wearable Device on Metabolic Syndrome: Cross-sectional Study. JMIR mHealth uHealth 2022, 10, e30789. [Google Scholar] [CrossRef]
- Vashistha, R.; Dangi, A.K.; Kumar, A.; Chhabra, D.; Shukla, P. Futuristic biosensors for cardiac health care: An artificial intelligence approach. 3 Biotech 2018, 8, 1–11. [Google Scholar] [CrossRef]
- Wu, C.; Zhong, J.; Lin, L.; Chen, Y.; Xue, Y.; Shi, P. Segmentation of HE-stained meningioma pathological images based on pseudo-labels. PLoS ONE 2022, 17, e0263006. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Y.; Lin, H.; Liu, X.; Zheng, Z.; Wang, T.; Feng, S. Serum analysis method combining cellulose acetate membrane purification with surface-enhanced Raman spectroscopy for non-invasive HBV screening. IET Nanobiotechnology 2020, 14, 98–104. [Google Scholar] [CrossRef]
- De León-Castañeda, C.D. Salud electrónica (e-Salud): Un marco conceptual de implementación en servicios de salud. Gac. Médica De México 2019, 155, 176–183. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yang, B.; Xiong, S.; Li, Q. Design of Portable Spirometer Based on Internet of Things of Medicine. Zhongguo Yi Liao Qi Xie Za Zhi = Chin. J. Med Instrum. 2018, 42, 103–106. [Google Scholar]
- Azrour, M.; Irshad, A.; Chaganti, R. IoT and Smart Devices for Sustainable Environment; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Calvillo-Arbizu, J. Román-Martínez, I., Reina-Tosina, J. Internet of things in health: Requirements, issues, and gaps. Comput. Methods Programs Biomed. 2021, 208, 106231. [Google Scholar] [CrossRef] [PubMed]
- Dong, T.; Santos, S.; Yang, Z.; Yang, S.; Kirkhus, N.E. Sputum and salivary protein biomarkers and point-of-care biosensors for the management of COPD. Anal. 2019, 145, 1583–1604. [Google Scholar] [CrossRef]
- Gupta, N.; Paiva, S. (Eds.) IoT and ICT for Healthcare Applications; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Inácio, P.R.; Duarte, A.; Fazendeiro, P.; Pombo, N. (Eds.) 5th EAI International Conference on IoT Technologies for HealthCare; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Li, Y.; Lu, H. (Eds.) 3rd EAI International Conference on Robotic Sensor Networks; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Packianather, M.S.; Munizaga, N.L.; Zouwail, S.; Saunders, M. Development of soft computing tools and IoT for improving the performance assessment of analysers in a clinical laboratory. In Proceedings of the 2019 14th Annual Conference System of Systems Engineering (SoSE), Anchorage, AK, USA, 19–22 May 2019; pp. 158–163. [Google Scholar] [CrossRef]
- Velliangiri, S.; Gunasekaran, M.; Karthikeyan, P. Secure Communication for 5G and IoT Networks; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Yang, X.; Wang, X.; Li, X.; Gu, D.; Liang, C.; Li, K.; Zhang, G.; Zhong, J. Exploring emerging IoT technologies in smart health research: A knowledge graph analysis. BMC Med Informatics Decis. Mak. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Ünal, B.; Khademhosseini, A.; Butt, H. Wearables in Medicine. Adv. Mater. 2018, 30, e1706910. [Google Scholar] [CrossRef]
- Yoo, J.S.; Soh, J.Y.; Lee, W.H.; Chang, D.K.; Lee, S.U.; Cha, W.C.; Park, Y.R.; Constantinescu, G. Experience of Emergency Department Patients With Using the Talking Pole Device: Prospective Interventional Descriptive Study. JMIR mHealth uHealth 2018, 6, e191. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study | Author, Year | Main Idea | Selection Strategy | Open Issue(s) | Taxonomy Provided |
|---|---|---|---|---|---|
| Survey | Thilakarathne, 2020, [42] | IoT in healthcare | Not specified | Discussed | No |
| Dang, 2019, [43] | IoT and cloud computing for healthcare | Not specified | Discussed | No | |
| Islam, 2015, [44] | IoT in healthcare | Not specified | Discussed | Yes | |
| Dhanvijay, 2019, [45] | IoT and its applications in healthcare | Not specified | Discussed | No | |
| Case study | Yuehong, 2016, [46] | IoT in healthcare | Not specified | Not discussed | No |
| Habibzadeh, 2019, [47] | IoT in healthcare | Not specified | Discussed | No | |
| Systematic literature review | Bolhasani, 2021, [48] | Deep learning with IoT in healthcare | Specified | Not discussed | Yes |
| Forum, 2021, [49] | Blockchain integration in healthcare | Specified | Not discussed | No | |
| Sadoughi, 2020, [50] | IoT in medicine | Specified | Not discussed | No | |
| Dwivedi, 2022, [13] | IoT applications in smart healthcare | Specified | Discussed | No | |
| Nasiri, [51] | Security requirements of IoT-based healthcare system | Specified | Discussed | No |
| Research Questions | Rationales |
|---|---|
| RQ1: What are the different categories and metrics for IoT integration in clinical laboratory systems? | The purpose is to gain insight into the scope and research scopes that support IoT-enabled clinical laboratory systems. |
| RQ2: What are the existing tools, evaluation techniques, and approaches that enable IoT in clinical laboratory systems? | The purpose is to identify and reveal existing tools and frameworks to advance the current status of IoT in clinical laboratory systems. |
| RQ2: What opportunities are available with the existing IoT techniques in clinical laboratory systems? | The purpose is to reveal the research opportunities in this field and present a coherent understanding of IoT applications in clinical laboratory systems. |
| RQ3: What are the key advantages, open challenges, concerns, and future trends in IoT in clinical laboratory systems? | The purpose is to identify the research considerations required for IoT applications in clinical laboratory systems. |
| No | Primary Author, Year, Country | Journal | Framework/Model | User(s) | Evaluation Tool(s) and Environment(s) | Main Idea | Evaluation Technique(s) | Performance Analysis | Opportunity | Advantage(s) | Challenge(s) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Preanalytic | |||||||||||
| 1 | Kang, 2018, Korea [56] | Healthcare Informatics Research | ZigBee communication | Scientists in the departments of laboratory, pathology, radiology, nuclear medicine, and radiation oncology | SMARTMIEW Cloud (Mbuzzer Co., Seoul, Korea) and Beagleboard (Texas Instruments, Dallas, TX, U.S.A.) using a temperature sensor | Able to maintain required temperature and humidity through a hospital IoT system implementation in the laboratory | Simulation, real-tested | Five issues were identified: sensing and measuring, transmission method, power supply, sensor module shape, and accessibility. | Equipment and environment monitoring in laboratories, device interconnection, and remote patient monitoring | High optimization | High maintenance costs, low reliability, high complexity |
| 2 | Galindo-Romera, 2017, Spain [57] | Sensors (Basel) | Portable Internet-of-Things (IoT) reader for passive wireless electromagnetic sensors based on a four-layer model | Lab scientists | Four functional layers: radiating layer, radiofrequency (R.F.) sensor interface, IoT mini-computer, power unit, MATLAB | Able to identify liquids without direct contact | Simulation, real-tested | A time difference between 3.59 ms and 8.04 ms for values of relative permittivity between 1 and 5.77, corresponding to free space and CHCl3 | Measurement of different liquids without direct contact with readers, which may be used for lab spills with toxic substances | Low detection delay, high efficiency, high performance, low overhead time, low computation time | Low physical range, high costs, low scalability |
| 3 | Alam, 2015, Canada [58] | Sensors (Basel) | Cyber-physical cloud computing (CPCC) for social internet of vehicles (S.U.V.) model | Driver, passengers, social network portal user, transport authority, intelligent vehicle system | Android-based communication (android tablets, laptops, desktop computers), Java | Able to facilitate communication from vehicle-to-vehicle, vehicle-to-infrastructure, and vehicle-to-internet; store the information (e.g., safety, efficiency, and infotainment messages); and provide near-real-time data for vehicle users and offline use cases for smart behaviors of vehicles and transport authorities to promote intelligent transport systems | Simulation, real-tested | N.R. | Effective use of resources and multimedia sensory datasets allow for smart and scalable adaptation vehicles for home- or hospital-based laboratory samples by avoiding traffic jams or accidents | High optimization, high reliability, high efficiency, high security, high privacy | Low scalability, high computation overhead |
| Analytic | |||||||||||
| 4 | Kalasin, 2020, Thailand [59] | A.C.S. Biomaterials Science & Engineering | Stress-free electrochemical-based sensor with IoT | Community health workers, community members | Smartphone, PSRAM-Wifi, Bluetooth, analytical-grade chemicals | Chemical transduction and Bluetooth-enabled P.O.C. technology | Simulation, real-tested | Sensitivity of 97.2% and data transmission was optimal | High outreach to underequipped communities of creatinine P.O.C. testing for those with kidney disorders with a minimal one-time investment | Low detection delay, high efficiency, low cost, high portability | Misuse, high maintenance, variable sensitivity |
| 5 | Kalasin, 2021, Thailand [60] | A.C.S. Biomaterials Science & Engineering | Satellite-based multimodal (artificial intelligence and IoT) sensing platform | Community health workers, community members | Smartphone, PSRAM-WIFI and Bluetooth, analytical-grade chemicals | Chemical transduction and Bluetooth-enabled P.O.C. technology | Simulation, real-tested | Selective efficacy of 96.3% | The concurrent monitoring of heat-stress sweat creatinine and the user’s heart rates allows for early diagnosis of heat stress through a decentralized epidermal sensor. | Low detection delay, moderate efficiency, low cost, high portability | Misuse, high maintenance, variable sensitivity |
| 6 | Alonso, 2020, Spain [61] | Biosensors and Bioelectronics | Field-programmable gate array (FPGA) with IoT capabilities | Community health workers, community members | Sensing system camera, IoT-enabled remote control, ELISA system | IoT-based malaria P.O.C. testing | Simulation, real-tested | Sensitivity, measured as photon detection probability, of the SPADs camera in a wavelength range of 300–1100 nm for overvoltages of 1.3 V and 1.8 V, at room temperature, was always below 15% | PoCT for plasmodium had similar signal trends and levels of detection to commercial fluorescence plate readers | Low cost, high scalability | Variable sensitivity |
| 7 | Ma, 2019, China [62] | B.M.C. Medical Informatics and Decision Making | Support vector machine-based strategy with IoT-enabled data monitoring | Healthcare personnel, community members | Smartphone, monitoring system, portable device, medical cloud monitoring center | Smartphone IoT-based real-time diagnosis of sleep apnea | Simulation | Sensitivity of 87.6%, accuracy of 90.2%, and specificity of 94.1% | Monitoring of sleep apnea in real-time with an early suggestion of abnormal physiological parameters | Low time, high sensitivity | Low scalability |
| 8 | Zhu, 2020, China [63] | Sensors and Actuators B: Chemical | IoT-enabled PCR chip | Community health workers, community members | Smartphone, PCR chip, D.N.A. templates/primers, Bluetooth, IoT cloud | Dengue virus P.O.C. testing | Simulation, real-tested | 40 cycles to detect the cDNA of a DENV required 34 min | IoT-enabled PoCT for DENV can effectively detect complementary deoxyribonucleic acid (cDNA) with the potential to tackle infectious disease outbreaks | Low time | Variable sensitivity |
| 9 | Wang, 2018, China [64] | Medicine | Cloud-assisted IoT construction for strip test results processing | Healthcare personnel, community members | Cloud server, Strip test, IoT device | Lupus nephritis PoC testing with a cloud-assisted IoT | Simulation, real-tested | Sensitivity and specificity were both higher than 80% | A urinary biomarker with excellent potential for monitoring lupus nephritis was identified with IoT-enabled reporting | Low time, moderate sensitivity | Variable reliability |
| 10 | Bibi, 2020, China [65] | Journal of Healthcare Engineering | IoT-enabled microscope for blood smear image and leukemia subtype detection | Healthcare personnel | IoT-enabled microscope, datasets, data augmentation, leukemia cloud, dense convolutional neural network (DenseNet-121), and residual convolutional neural network (ResNet-34) models | IoT-based detection and classification of leukemia | Simulation | Accuracy [ResNet-34 Accuracy: ALL (100%), AML (99.65%), CLL (99.73%), CML (99.73%), Healthy (100%); DenseNet-121: ALL (100%), AML (99.91), CLL (99.91%), CML (100%), Healthy (100%)] | The suggested model is better than existent machine-learning algorithms for healthy-versus-leukemia-subtype identification | High accuracy, high interoperability, low time | Misuse, high complexity, low scalability |
| 11 | Neil, 2018, U.S.A. [66] | SLAS Technology | Lean process | Lab scientists | Biotage V10 centrifugal evaporator, BioMicroLab SampleScan 2D Plus, BlinkStick L.E.D. Strip, Raspberry Pi 3, iHome iM59 Rechargeable Mini Speaker, T.W.D. TradeWinds 30 mL EPA-Style Vial with Data Matrix 2D Barcodes, Biotage V10 Centrifugal Evaporator, Python, Java | Able to track purification analysis from beginning to end | Simulation, real-tested | N.R. | Tracking of laboratory samples in a high-throughput screening | Low costs, high efficiency, high scalability, high performance, high reliability | High communication complexity |
| 12 | Shumate, 2018, USA [67] | SLAS Technology | Computer-aided design model for 3D-printed components | Lab scientists | Arduino Uno, Ethernet Shield, RS232 Shield, Raspberry Pi, Java | Able to provide real-time gravimetric summaries of dispensing and generate timely alerts if problems arise | Simulation, real-tested | Average difference of 1.0% between the weights measured by the JAMS platform and the manual operator weighing | Monitoring the dispense rate of liquids in a high-throughput screening | High efficiency, high performance, high reliability | High costs, low scalability |
| 13 | Austerjost, 2018, Germany [68] | SLAS Technology | Voice user interface | Lab scientist | Node-RED 0.15.2, Java, Amazon’s Alexa Voice Service | Virtual assistant able to control and monitor smart devices in the laboratory | Simulation, real-tested | Mean accuracy of 95% ± 3.62 of speech command recognition | Instrument control, retrieval of experimental data, and protocols to improve workflows | High sensitivity, high performance | Low scalability |
| 14 | Porr, 2020, Germany [69] | Engineering in Life Sciences | Open source Standardization in Lab Automation 2 standard | Lab scientist | Wireless Local Area Network, ESTful Hypertext Transfer Protocol, ControlFlow Runtime, REST-API | The central lab server facilitates device communication and database records of measurements, tasks, and results generated. | Simulation | N.R. | Digitalization of workflow in laboratories enabling device communication and automation | High efficiency, high performance | Low scalability |
| Postanalytical | |||||||||||
| 15 | Guo, 2021, China [70] | Biosensors and Bioelectronics | 5G-enabled fluorescence sensor with cloud infrastructure as a service (IaaS) | Patients, healthcare personnel, medical facilities, government | Hardware devices (personal computers, 5G smartphones, IPTV), 5G cloud server | Quantitative detection of spike protein and nucleocapsid protein of SARS-CoV-2 by using mesoporous silica encapsulated up-conversion nanoparticles (UCNPs@mSiO2) labeled lateral flow immunoassay (LFIA), of which medical data can be transmitted to the fog layer of the network and 5G cloud server for edge computing and big data analysis | Simulation | The sensor can detect spike protein (S.P.) with a detection of limit (L.O.D.) of 1.6 ng/mL and nucleocapsid protein (N.P.) with an L.O.D. of 2.2 ng/mL | A practical and efficient way to treat and prevent COVID-19 and other mass infectious diseases in the future | High optimization, low latency, high reliability, low communication cost | Low scalability, low privacy |
| 16 | Celesti, 2020, Italy [71] | Sensors (Basel) | Blockchain technology with cloud infrastructure as a service (IaaS) | Patients, healthcare personnel, medical facilities, government | Python, Ethereum, and blockchain | Tele-medical laboratory service where technicians perform clinical exams on patients directly in a hospital through IoT medical devices and results are automatically sent via the hospital cloud to doctors of federated hospitals for validation or consultation. | Simulation, real-tested | The average cost of a single transaction to be written in the public Ethereum blockchain is approximately 0.0002 ETH | Virtual telemedical laboratory service may be created through a healthcare workflow operating in a federal hospital IoT cloud environment leveraging blockchain | High transparency, high security, high privacy, high traceability, high efficiency | High cost, low scalability, high energy utility |
| 17 | El Majdoubi, 2021, Morocco [72] | Hindawi | Data sharing through an end-to-end blockchain-based and privacy-preserving framework called SmartMedChain | Patients, healthcare personnel, medical facilities, government | Blockchain | Blockchain-based framework with encrypted health data stored in interplanetary file system (IPFS) that supports data access and usage for smart healthcare | Simulation, real-tested | Average throughput of 39.6 tps and an average delay of 1.34 s at 50 tps workload | Laboratory data integration for improved healthcare provision | High transparency, high security, high privacy, high traceability, high efficiency | High cost, low scalability, high energy utility |
| 18 | Ochôa, 2019, Brazil [73] | Sensors (Basel) | UbiPri middleware | Patients, healthcare personnel, medical facilities, government | Ethereum blockchain, IPFS storage service, middleware, 16-bit Arduino Uno R3 architecture | A smart contract between different architectural layers of IoT, including Ethereum Blockchain Smart, for user privacy | Simulation, real-tested | The user transaction fee was 0.06779326 ETH and 3,389,663 gas was used; the device transaction fee was 0.0277857 ETH and 1,389,285 gas was used; environment transaction fee was 0.02598354 and 1,299,177 gas was used. | Privacy for blockchain architectures in IoT health environments | High scalability, high performance, high privacy | High cost, high energy utility |
| No. | Primary Author, Year, Country | Approach | Scope |
|---|---|---|---|
| 1 | Kang, 2018, Korea [56] | Sensor-based | Environmental sensors |
| Communication-based | Algorithmic approach | ||
| 2 | Galindo-Romera, 2017, Spain [57] | Sensor-based | Environmental sensors |
| Communication-based | Technological approach | ||
| 3 | Alam, 2015, Canada [58] | Resource-based | Scheduling |
| Sensor-based | Environmental sensors | ||
| Communication-based | Algorithmic approach | ||
| 4 | Kalasin, 2020, Thailand [59] | Application-based | Prediction/diagnosis |
| Sensor-based | Wearable sensors | ||
| 5 | Kalasin, 2021, Thailand [60] | Application-based | Prediction/diagnosis |
| Sensor-based | Wearable sensors | ||
| Communication-based | Technological approach | ||
| 6 | Alonso, 2020, Spain [61] | Application-based | Prediction/diagnosis |
| Communication-based | Technological approaches | ||
| 7 | Ma, 2019, China [62] | Application-based | Prediction/diagnosis |
| Communication-based | Technological approach | ||
| 8 | Zhu, 2020, China [63] | Application-based | Prediction/diagnosis |
| Communication-based | Technological approach | ||
| 9 | Wang, 2018, China [64] | Application-based | Prediction/diagnosis |
| Communication-based | Technological approach | ||
| 10 | Bibi, 2020, China [65] | Application-based | Algorithmic approach |
| Communication-based | Technological approach | ||
| 11 | Neil, 2018, USA [66] | Sensor-based | Environmental approach |
| Communication-based | Technological approach | ||
| Resource-based | Resource allocation, offloading, load balancing, and provision | ||
| 12 | Shumate, 2018, USA [67] | Sensor-based | Environmental approach |
| Communication-based | Algorithmic approach | ||
| Resource-based | Resource allocation, offloading, load balancing, and provision | ||
| 13 | Austerjost, 2018, Germany [68] | Communication-based | Algorithmic approach |
| 14 | Porr, 2020, Germany [69] | Communication-based | Algorithmic approach |
| 15 | Guo, 2021, China [70] | Application-based | Prediction/detection |
| 16 | Celesti, 2020, Italy [71] | Security-based | Access control |
| Resource-based | Scheduling | ||
| Communication-based | Algorithmic approach | ||
| 17 | El Majdoubi, 2021, Morocco [72] | Security-based | Privacy |
| Resource-based | Scheduling | ||
| Communication-based | Algorithmic approach | ||
| 18 | Ochôa, 2019, Brazil [73] | Security-based | Privacy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munir, T.; Akbar, M.S.; Ahmed, S.; Sarfraz, A.; Sarfraz, Z.; Sarfraz, M.; Felix, M.; Cherrez-Ojeda, I. A Systematic Review of Internet of Things in Clinical Laboratories: Opportunities, Advantages, and Challenges. Sensors 2022, 22, 8051. https://doi.org/10.3390/s22208051
Munir T, Akbar MS, Ahmed S, Sarfraz A, Sarfraz Z, Sarfraz M, Felix M, Cherrez-Ojeda I. A Systematic Review of Internet of Things in Clinical Laboratories: Opportunities, Advantages, and Challenges. Sensors. 2022; 22(20):8051. https://doi.org/10.3390/s22208051
Chicago/Turabian StyleMunir, Tahir, Muhammad Soomair Akbar, Sadia Ahmed, Azza Sarfraz, Zouina Sarfraz, Muzna Sarfraz, Miguel Felix, and Ivan Cherrez-Ojeda. 2022. "A Systematic Review of Internet of Things in Clinical Laboratories: Opportunities, Advantages, and Challenges" Sensors 22, no. 20: 8051. https://doi.org/10.3390/s22208051
APA StyleMunir, T., Akbar, M. S., Ahmed, S., Sarfraz, A., Sarfraz, Z., Sarfraz, M., Felix, M., & Cherrez-Ojeda, I. (2022). A Systematic Review of Internet of Things in Clinical Laboratories: Opportunities, Advantages, and Challenges. Sensors, 22(20), 8051. https://doi.org/10.3390/s22208051