
LBSS: A Lightweight Blockchain-Based Security Scheme for IoT-Enabled Healthcare Environment

Abstract
1. Introduction
- Apply blockchain technology for data transaction integrity in the IoT-enabled healthcare environment;
- Propose a security mechanism for data storing in the IoT-enabled healthcare environment;
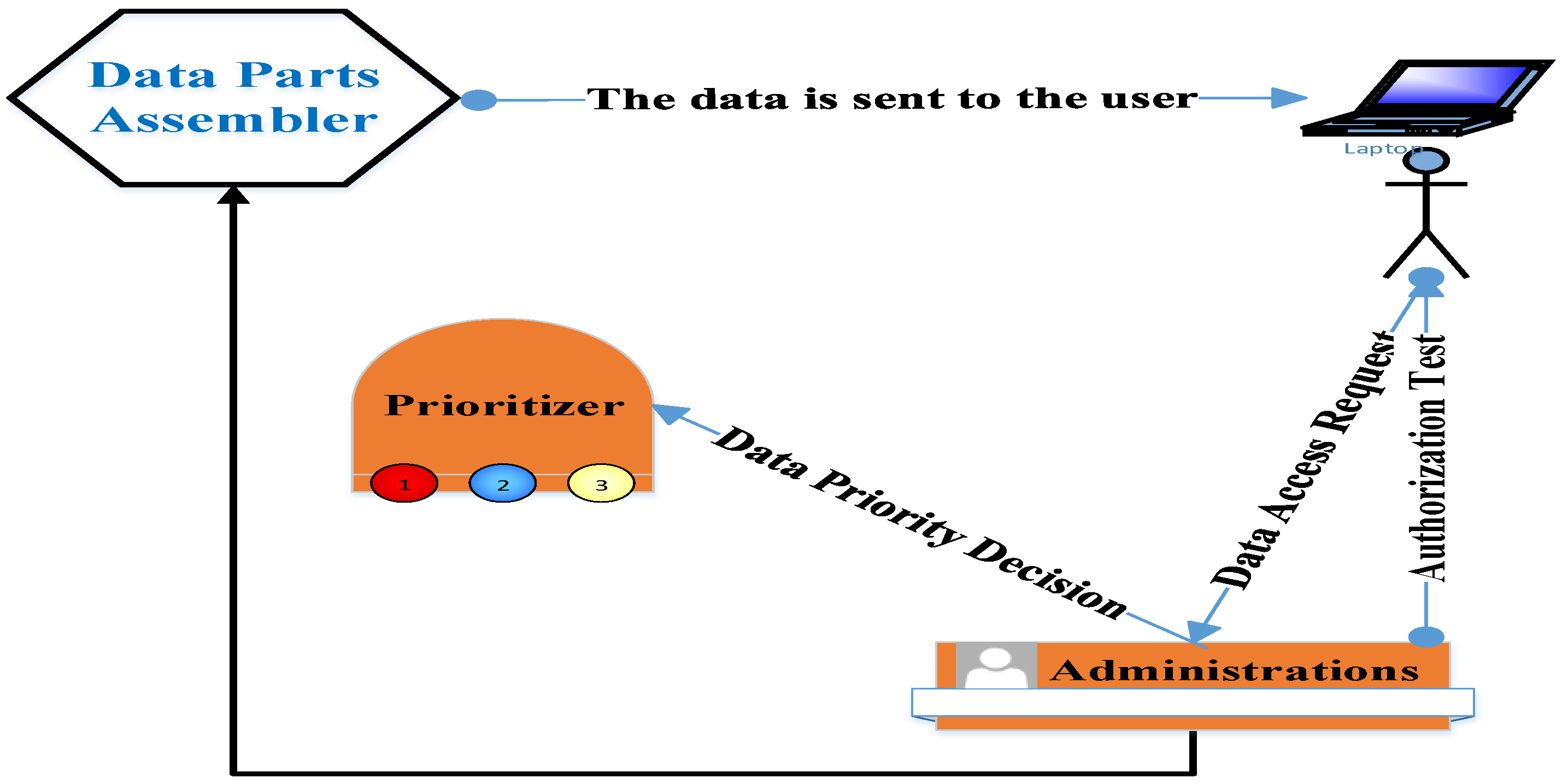
- Propose a security mechanism for data access in the IoT-enabled healthcare environment;
- Construct a simulation for the IoT-enabled healthcare environment and examine the efficiency of the proposed security scheme;
- Finally, show and discuss the simulation results.
2. Related Works
3. Proposed Security Scheme
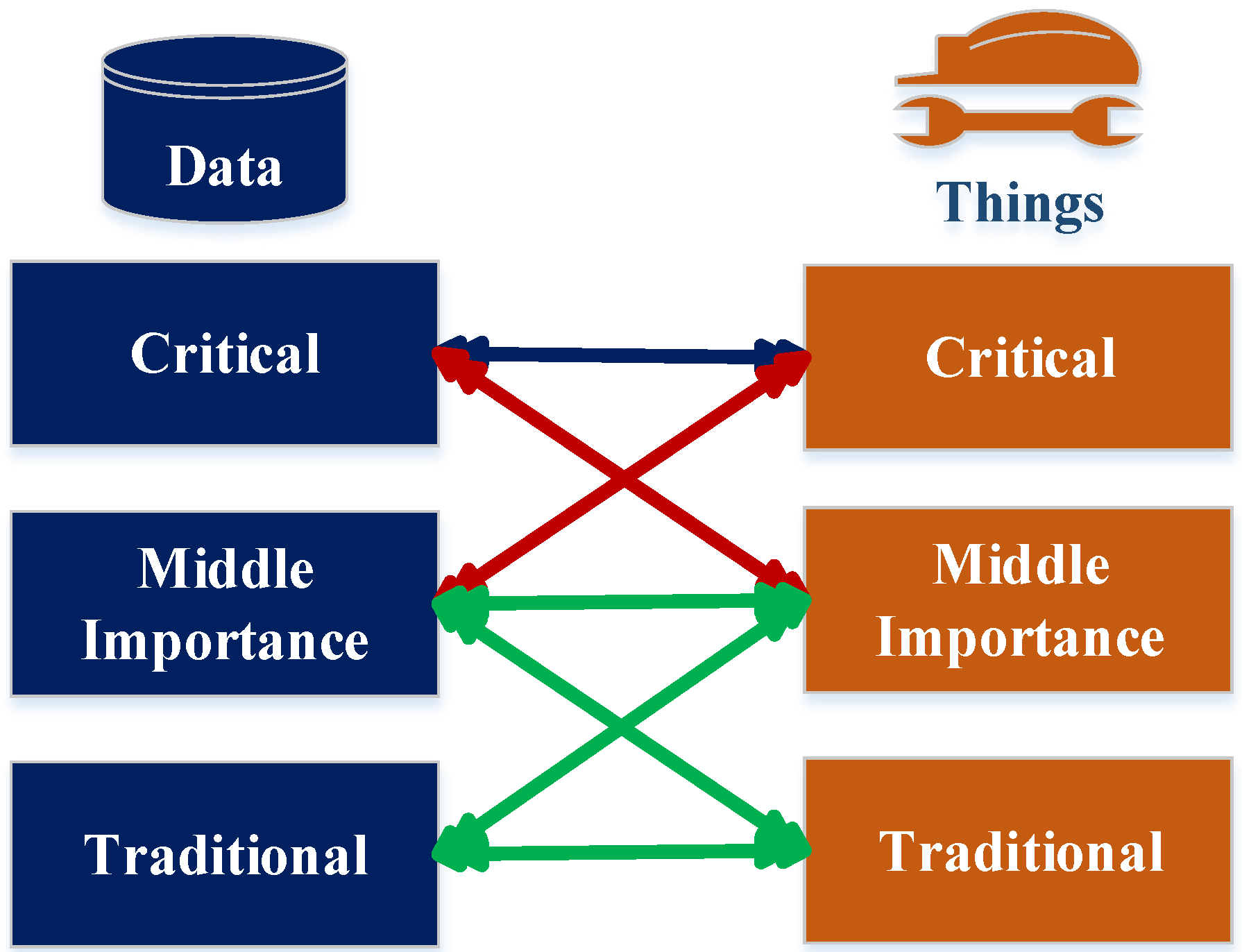
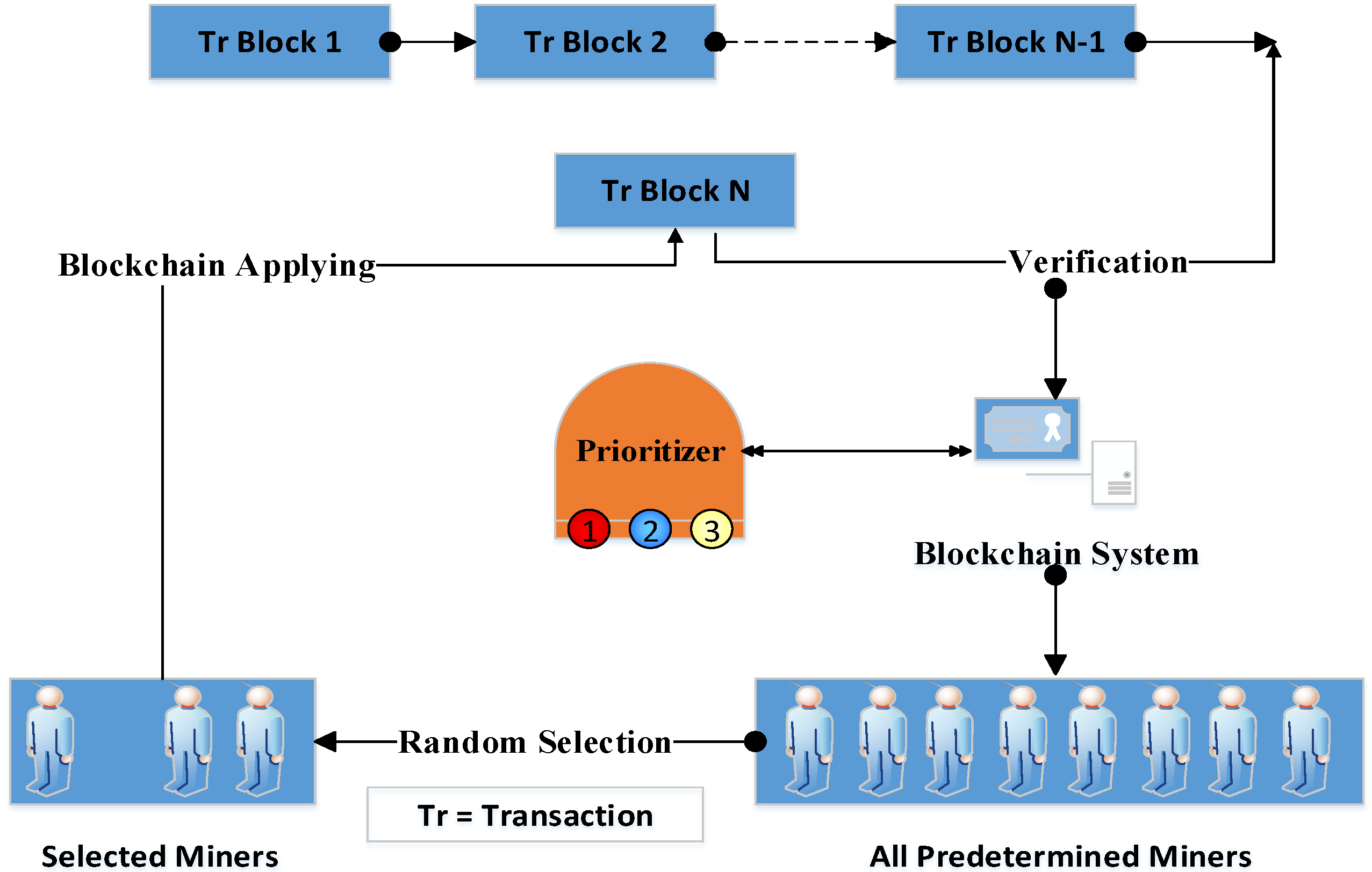
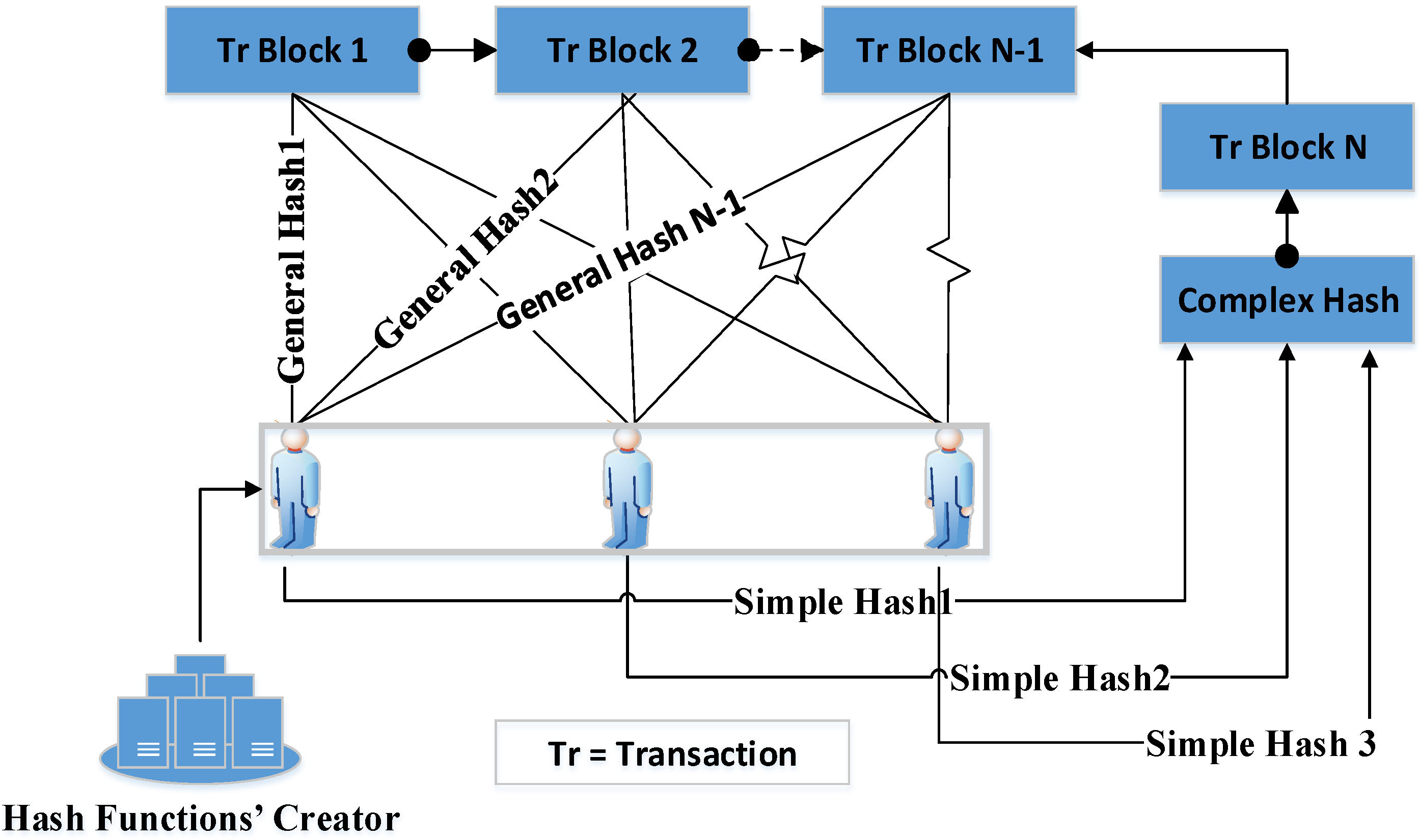
3.1. Integrity
| Algorithm 1: Transaction Integrity | |
| DI | Data Importance |
| L | Importance Level |
| n | Number of Importance Levels |
| HTr | Hashed Transaction |
| HC | Complex Hash |
| m | Number of Minors |
| HS | Simple Hash |
| SS | Security Server |
| Algorithm Begin | |
| 1: | DI = L[i], 1 < i < n |
| 2: | For i = 1 to L |
| 3: | Begin |
| 4: | HTr = HC[i](Tr) |
| 5: | |
| 6: | For j = 1 to m |
| 7: | |
| 8: | While (Tr) |
| 9: | Begin |
| 10: | |
| 11: | … |
| 12: | |
| 13: | |
| 14: | Else |
| 15: | |
| 16: | End |
| 17: | End |
| 18: | End Algorithm |
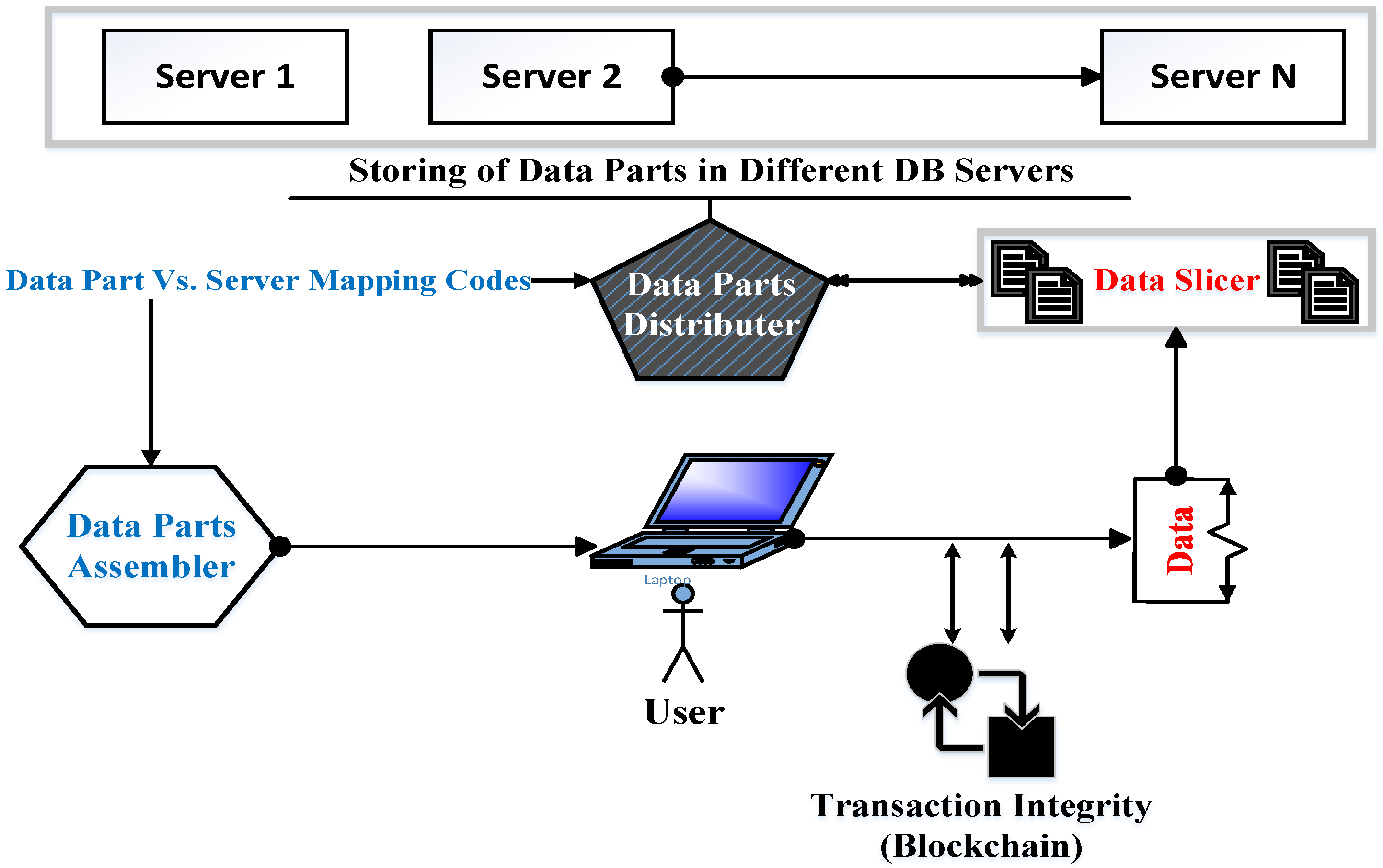
3.2. Confidentiality and Availability
3.3. Mathematical Notations
4. Simulation and Evaluation
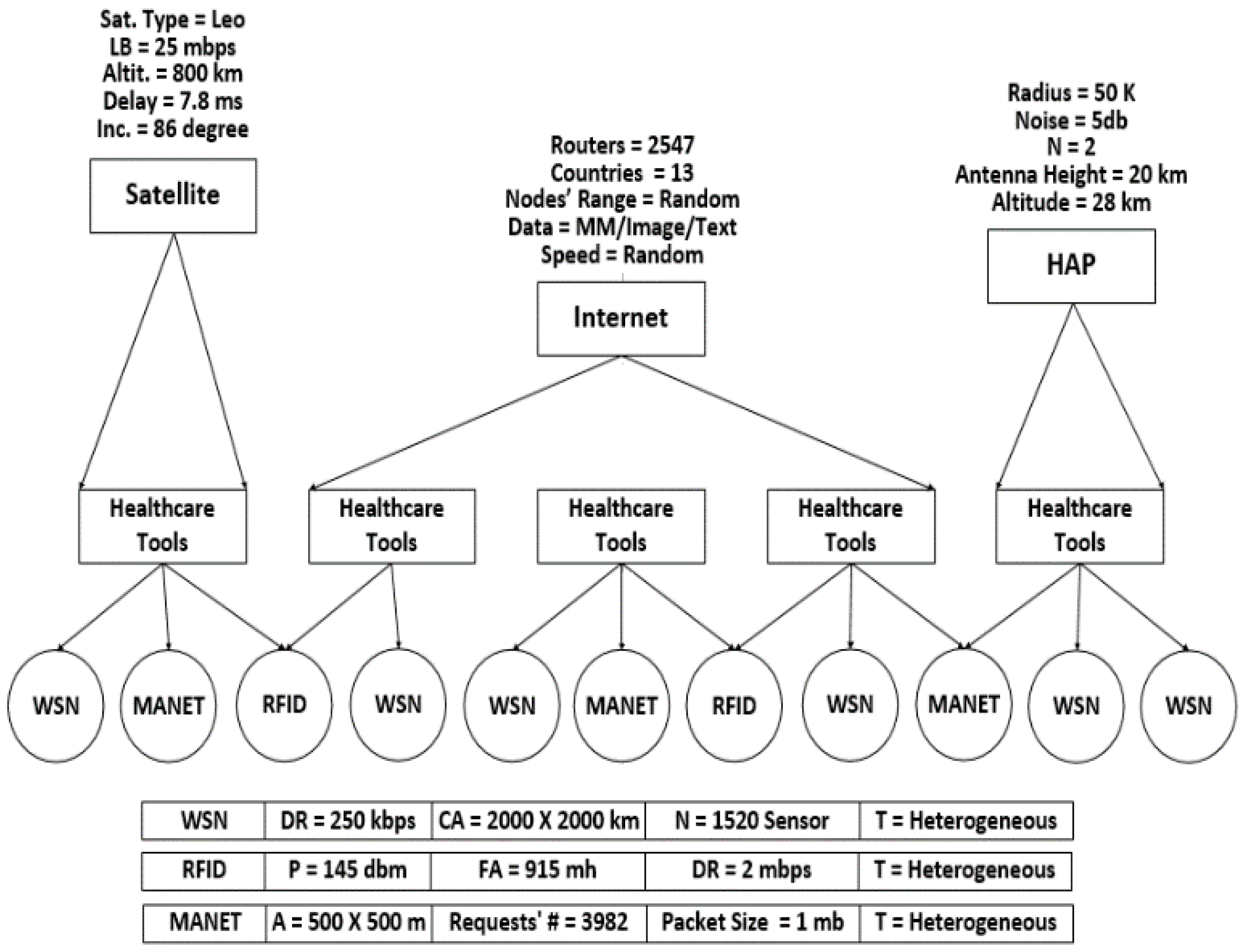
4.1. Simulation Infrastructure
4.2. Results and Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, C.; Qu, Y.; Luan, T.H.; Eklund, P.W.; Xiang, Y.; Gao, L. A Lightweight and Attack-Proof Bidirectional Blockchain Paradigm for Internet of Things. IEEE Internet Things J. 2022, 9, 4371–4384. [Google Scholar] [CrossRef]
- Liqiong, H.; Yuanyuan, W. Congestion Control of Multipath Parallel Transmission of Data for Blockchain Applications. IETE J. Res. 2022, 1–10. [Google Scholar] [CrossRef]
- Mirani, A.A.; Velasco-Hernandez, G.; Awasthi, A.; Walsh, J. Key Challenges and Emerging Technologies in Industrial IoT Architectures: A Review. Sensors 2022, 22, 5836. [Google Scholar] [CrossRef] [PubMed]
- Azamuddin, W.M.H.; Aman, A.H.M.; Hassan, R.; Mansor, N. Comparison of Named Data Networking Mobility Methodology in a Merged Cloud Internet of Things and Artificial Intelligence Environment. Sensors 2022, 22, 6668. [Google Scholar] [CrossRef] [PubMed]
- Lavaur, T.; Lacan, J.; Chanel, C.P.C. Enabling Blockchain Services for IoE with Zk-Rollups. Sensors 2022, 22, 6493. [Google Scholar] [CrossRef]
- Wang, X.; Cai, S. Secure healthcare monitoring framework integrating NDN-based IoT with edge cloud. Futur. Gener. Comput. Syst. 2020, 112, 320–329. [Google Scholar] [CrossRef]
- Fotouhi, M.; Bayat, M.; Das, A.K.; Far, H.A.N.; Pournaghi, S.M.; Doostari, M. A lightweight and secure two-factor authentication scheme for wireless body area networks in health-care IoT. Comput. Netw. 2020, 177, 107333. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.; Wang, X.; Qiu, T.; Yuan, Y.; Ouyang, L.; Guo, Y.; Wang, F.-Y. Blockchain-Powered Parallel Healthcare Systems Based on the ACP Approach. IEEE Trans. Comput. Soc. Syst. 2018, 5, 942–950. [Google Scholar] [CrossRef]
- Ismail, L.; Materwala, H.; Zeadally, S. Lightweight Blockchain for Healthcare. IEEE Access 2019, 7, 149935–149951. [Google Scholar] [CrossRef]
- Haghparast, M.B.; Berehlia, S.; Akbari, M.; Sayadi, A. Developing and evaluating a proposed health security framework in IoT using fuzzy analytic network process method. J. Ambient Intell. Humaniz. Comput. 2020, 12, 3121–3138. [Google Scholar] [CrossRef]
- Gupta, P.K.; Maharaj, B.T.; Malekian, R. A novel and secure IoT based cloud centric architecture to perform predictive analysis of users activities in sustainable health centres. Multimedia Tools Appl. 2016, 76, 18489–18512. [Google Scholar] [CrossRef]
- Ning, Z.; Sun, S.; Wang, X.; Guo, L.; Guo, S.; Hu, X.; Hu, B.; Kwok, R. Blockchain-enabled Intelligent Transportation Systems: A Distributed Crowdsensing Framework. IEEE Trans. Mob. Comput. 2021. [Google Scholar] [CrossRef]
- Lakhan, A.; Mohammed, M.A.; Nedoma, J.; Martinek, R.; Tiwari, P.; Vidyarthi, A.; Alkhayyat, A.; Wang, W. Federated-Learning Based Privacy Preservation and Fraud-Enabled Blockchain IoMT System for Healthcare. IEEE J. Biomed. Health Inform. 2022. [Google Scholar] [CrossRef] [PubMed]
- Manoharan, H.; Selvarajan, S.; Yafoz, A.; Alterazi, H.A.; Uddin, M.; Chen, C.L.; Wu, C.M. Deep Conviction Systems for Biomedical Applications Using Intuiting Procedures with Cross Point Approach. Front. Public Health 2022, 10, 909628. [Google Scholar] [CrossRef]
- Selvarajan, S.; Manoharan, H.; Hasanin, T.; Alsini, R.; Uddin, M.; Shorfuzzaman, M.; Alsufyani, A. Biomedical Signals for Healthcare Using Hadoop Infrastructure with Artificial Intelligence and Fuzzy Logic Interpretation. Appl. Sci. 2022, 12, 5097. [Google Scholar] [CrossRef]
- Anitha, S.; Jayanthi, P.; Chandrasekaran, V. An intelligent based healthcare security monitoring schemes for detection of node replication attack in wireless sensor networks. Measurement 2020, 167, 108272. [Google Scholar] [CrossRef]
- Benil, T.; Jasper, J. Cloud based security on outsourcing using blockchain in E-health systems. Comput. Netw. 2020, 178, 107344. [Google Scholar] [CrossRef]
- Kong, F.; Zhou, Y.; Xia, B.; Pan, L.; Zhu, L. A Security Reputation Model for IoT Health Data Using S-AlexNet and Dynamic Game Theory in Cloud Computing Environment. IEEE Access 2019, 7, 161822–161830. [Google Scholar] [CrossRef]
- Wang, L.; Ali, Y.; Nazir, S.; Niazi, M. ISA Evaluation Framework for Security of Internet of Health Things System Using AHP-TOPSIS Methods. IEEE Access 2020, 8, 152316–152332. [Google Scholar] [CrossRef]
- Abou-Nassar, E.M.; Iliyasu, A.M.; El-Kafrawy, P.M.; Song, O.-Y.; Bashir, A.K.; Abd El-Latif, A.A. DITrust Chain: Towards Blockchain-Based Trust Models for Sustainable Healthcare IoT Systems. IEEE Access 2020, 8, 111223–111238. [Google Scholar] [CrossRef]
- Kavitha, S.; Alphonse, P.; Reddy, Y. An Improved Authentication and Security on Efficient Generalized Group Key Agreement Using Hyper Elliptic Curve Based Public Key Cryptography for IoT Health Care System. J. Med. Syst. 2019, 43, 260. [Google Scholar] [CrossRef] [PubMed]
- Tai, W.; Chang, Y.; Lo, Y. An Anonymity, Availability and Security-Ensured Authentication Model of the IoT Control System for Reliable and Anonymous eHealth Services. J. Med. Biol. Eng. 2019, 39, 443–455. [Google Scholar] [CrossRef]
- Pawar, P.; Parolia, N.; Shinde, S.; Edoh, T.O.; Singh, M. eHealthChain—A blockchain-based personal health information management system. Ann. Telecommun. 2021, 77, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Hasanova, H.; Tufail, M.; Baek, U.-J.; Park, J.-T.; Kim, M.-S. A novel blockchain-enabled heart disease prediction mechanism using machine learning. Comput. Electr. Eng. 2022, 101, 108086. [Google Scholar] [CrossRef]
- Marwan, M.; Kartit, A.; Ouahmane, H. Security Enhancement in Healthcare Cloud using Machine Learning. Procedia Comput. Sci. 2018, 127, 388–397. [Google Scholar] [CrossRef]
- Ding, R.; Zhong, H.; Ma, J.; Liu, X.; Ning, J. Lightweight Privacy-Preserving Identity-Based Verifiable IoT-Based Health Storage System. IEEE Internet Things J. 2019, 6, 8393–8405. [Google Scholar] [CrossRef]
- Li, P.; Xu, C.; Jin, H.; Hu, C.; Luo, Y.; Cao, Y.; Mathew, J.; Ma, Y. ChainSDI: A Software-Defined Infrastructure for Regulation-Compliant Home-Based Healthcare Services Secured by Blockchains. IEEE Syst. J. 2020, 14, 2042–2053. [Google Scholar] [CrossRef]
- Vedaraj, M.; Ezhumalai, P. HERDE-MSNB: A predictive security architecture for IoT health cloud system. J. Ambient. Intell. Humaniz. Comput. 2021, 12, 7333–7342. [Google Scholar] [CrossRef]
- Wang, X.; Ning, Z.; Guo, S.; Wen, M.; Poor, H.V. Minimizing the Age-of-Critical-Information: An Imitation Learning-Based Scheduling Approach under Partial Observations. IEEE Trans. Mob. Comput. 2021, 21, 3225–3238. [Google Scholar] [CrossRef]
- Ning, Z.; Yang, Y.; Wang, X.; Guo, L.; Gao, X.; Guo, S.; Wang, G. Dynamic Computation Offloading and Server Deployment for UAV-Enabled Multi-Access Edge Computing. IEEE Trans. Mob. Comput. 2021. [Google Scholar] [CrossRef]
- Zarour, M.; Ansari, T.J.; Alenezi, M.; Sarkar, A.K.; Faizan, M.; Agrawal, A.; Kumar, R.; Khan, R.A. Evaluating the Impact of Blockchain Models for Secure and Trustworthy Electronic Healthcare Records. IEEE Access 2020, 8, 157959–157973. [Google Scholar] [CrossRef]
- Sharma, H.; Kumar, A.; Pant, S.; Ram, M. 3 Role of Artificial Intelligence, IoT and Blockchain in Smart Healthcare. In Artificial Intelligence, Blockchain and IoT for Smart Healthcare; River Publishers: Aalborg, Denmark, 2022; pp. 25–36. [Google Scholar]
- Xiao, J.; Tian, Y.; Xie, L.; Jiang, X.; Huang, J. A Hybrid Classification Framework Based on Clustering. IEEE Trans. Ind. Inform. 2019, 16, 2177–2188. [Google Scholar] [CrossRef]
- Katarahweire, M.; Bainomugisha, E.; Mughal, K.A. Data Classification for Secure Mobile Health Data Collection Systems. Dev. Eng. 2020, 5, 100054. [Google Scholar] [CrossRef]
- Bera, B.; Chattaraj, D.; Das, A.K. Designing secure blockchain-based access control scheme in IoT-enabled Internet of Drones deployment. Comput. Commun. 2020, 153, 229–249. [Google Scholar] [CrossRef]
- Grunspan, C.; Marco, R. The mathematics of Bitcoin. Eur. Math. Soc. Mag. 2020, 115, 31–37. [Google Scholar] [CrossRef]
- Said, O.; Tolba, A. DORS: A data overhead reduction scheme for hybrid networks in smart cities. Int. J. Commun. Syst. 2020, 33, e4435. [Google Scholar] [CrossRef]
- Roquero, P.; Aracil, J. On Performance and Scalability of Cost-Effective SNMP Managers for Large-Scale Polling. IEEE Access 2021, 9, 7374–7383. [Google Scholar] [CrossRef]
- Badea, A.; Croitoru, V.; Gheorghică, D. Computer networks security based on the detection of user’s behavior. In Proceedings of the 9th International Symposium on Advanced Topics in Electrical Engineering (ATEE), Bucharest, Romania, 7–9 May 2015; pp. 55–60. [Google Scholar] [CrossRef]
- How to Represent a Blockchain through a Mathematical Model? Study Carried Out by the Data Science Practice. Available online: https://canopee-group.com/wp-content/uploads/2020/05/Blockchain-Coperneec.pdf (accessed on 15 October 2022).
- Said, O.; Tolba, A. Design and performance evaluation of mixed multicast architecture for internet of things environment. Supercomput. J. 2018, 74, 3295–3328. [Google Scholar] [CrossRef]
- Forjan, M.; David, V.; Wagner, M.; Dolesch, L.; Lechner, M.; Sauermann, S. Conceptualization of an ICU Infrastructure for Simulation Based Education in Medical Engineering & eHealth. In Proceedings of the 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4186–4189. [Google Scholar] [CrossRef]
- Kim, H.H.; Bruce, N.; Park, S.; Jo, J.; Lee, H.J. Modeling and Simulation of Identification Protocol for Wireless Medical Devices in Healthcare System Communication. In Information Science and Applications; Lecture Notes in Electrical Engineering; Kim, K., Ed.; Springer: Berlin/Heidelberg, Germany, 2015; p. 339. [Google Scholar] [CrossRef]
- Avventuroso, G.; Silvestri, M.; Frazzon, E. Additive Manufacturing Plant for Large Scale Production of Medical Devices: A Simulation Study. IFAC-PapersOnLine 2018, 51, 1442–1447. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Ref. | Contributions | Limitation Factors | |||
|---|---|---|---|---|---|---|---|
| IoT Rep. | IoT Sut. | SW | Rev. | ||||
| Wang et al. | 2020 | [6] | Proposed a security mechanism for healthcare systems. This mechanism combined the edge cloud and IoT technologies to secure the retrieval of data. | ✓ | ✗ | ✓ | ✗ |
| Fotouhi et al. | 2020 | [7] | Introduced an authentication scheme to prevent attacks targeted at wireless body area networks. | ✓ | ✗ | ✗ | ✗ |
| Wang et al. | 2020 | [8] | Demonstrated a parallel healthcare system in which the blockchain technology and care auditability were applied. | ✓ | ✗ | ✗ | ✗ |
| Ismail et al. | 2019 | [9] | Introduced a blockchain system for healthcare environments. It divided the network into clusters to apply its security model. | ✓ | ✗ | ✓ | ✗ |
| Haghparast et al. | 2020 | [10] | Proposed a security framework for IoT-based e-health systems. This framework consisted of four layers of sensors. Each layer achieved function(s) from the framework target. | ✓ | ✗ | ✗ | ✗ |
| Gupta | 2017 | [11] | Demonstrated a generalized architecture for the security and management of cloud servers in IoT healthcare systems. It divided the cloud centers into three categories to guarantee the secure communication of information. | ✓ | ✗ | ✗ | ✗ |
| Ning, et al. | 2021 | [12] | Demonstrated a blockchain framework for distributed traffic management in transportation systems. It analyzed this framework into two sub-problems to decrease its complexity. | ✓ | ✗ | ✓ | ✗ |
| Lakhan et al. | 2022 | [13] | Identified and ensured the fraud of medical data in addition to privacy preservation at local fog nodes and clouds, with minimum delay and energy consumption. | ✓ | ✗ | ✓ | ✗ |
| Manoharan et al. | 2022 | [14] | Presented a model to analyze the biomedical signals behavior and complete the output tracking mechanism of the transceiver results with low power consumption. | ✓ | ✗ | ✓ | ✗ |
| Selvarajan, et al., | 2022 | [15] | Introduced a system to minimize the loss of functionalities in the biomedical signals. Additionally, an activation function was presented in the middle stage. | ✓ | ✗ | ✓ | ✗ |
| Anitha et al. | 2021 | [16] | Proposed a security method that detected the replication attack. This security method was for the healthcare system, which was based on a Wireless Sensor Network (WSN). | ✗ | ✓ | ✓ | ✗ |
| Benil et al. | 2020 | [17] | Demonstrated a security scheme to verify and audit medical cloud servers using blockchain technology. | ✗ | ✓ | ✗ | ✗ |
| Kong et al. [11] | 2019 | [18] | Introduced a security model using a neural network and the pre-classification of health data and dynamic gaming theory. | ✗ | ✓ | ✗ | ✗ |
| Wang et al. [12] | 2020 | [19] | Introduced a security framework used to evaluate the security specs of Internet of Health Things (IoHT). | ✗ | ✓ | ✗ | ✗ |
| AbouNassar et al. | 2020 | [20] | Proposed a security model based on blockchain technology. It used a smart contract to enhance the Trustworthy Factor (TF) and establish trustworthy communications in the IoHT infrastructure. | ✗ | ✓ | ✗ | ✗ |
| Kavitha et al. | 2019 | [21] | Introduced a security framework to deal with the security flaws of the personal data records, which were found in healthcare systems. It used the hyperelliptic curve-based public key cryptosystem instead of the traditional cryptographic framework to ensure the group communications were secure. | ✗ | ✓ | ✗ | ✗ |
| Tai | 2019 | [22] | Introduced a security model for IoT healthcare data in which the control operations for the IoT system were adjusted and the user anonymity is considered to introduce an authentication model. Additionally, the control system for IoT has the ability to ensure reliable e-Health services. | ✗ | ✓ | ✓ | ✗ |
| Pawar et al. | 2018 | [23] | Demonstrated a system model that was based on the blockchain technology to manage the health data that were obtained from the medical devices. | ✗ | ✓ | ✗ | ✗ |
| Hasanova, et al. | 2022 | [24] | Presented an algorithm that was based on machine learning technology to predict heart diseases using the blockchain data. | ✗ | ✓ | ✗ | ✗ |
| Marwan et al. | 2018 | [25] | Proposed a security method to prevent unauthorized users from accessing healthcare records. This method used machine-learning technology. | ✗ | ✗ | ✓ | ✗ |
| Ding et al. | 2019 | [26] | Introduced a security system that handles the limited capabilities of sensors. It also verified data integrity and reduced the computation overhead cost. | ✗ | ✗ | ✓ | ✗ |
| Li et al. | 2020 | [27] | Introduced a framework to apply the blockchain technology to guarantee secure data sharing in addition to computing the sensitive data of patients. | ✗ | ✗ | ✓ | ✗ |
| Vedaraj et al. | 2020 | [28] | Provided an effective security framework for the health data in addition to predicting the patients’ diseases. Additionally, it can encrypt and decrypt using a special security algorithm. | ✗ | ✗ | ✓ | ✗ |
| Wang et al. | 2021 | [29] | Introduced a system to quantify the freshness of information using critical-level changes. It was an optimized problem of minimization of the Age-of-Critical-Information (AoCI). Furthermore, an information-aware heuristic algorithm was introduced. | ✗ | ✗ | ✓ | ✗ |
| Ning, et al. | 2021 | [30] | Used Unmanned Aerial Vehicles (UAV) to investigate Multi-access Edge Computing (MEC) that considered edge server deployment and offloading computation. Moreover, two learning algorithms were demonstrated to reach the Nash Equilibrium (NE). | ✗ | ✗ | ✓ | ✗ |
| Zarour et al. | 2015 | [31] | Introduced a study to determine the impact of using blockchain technology on the healthcare system from groups of experts and specialists. | ✗ | ✗ | ✗ | ✓ |
| Sharma et al. | 2022 | [32] | Introduced a literate review of the relationship between the blockchain technology, IoT technology, and the healthcare system. | ✗ | ✗ | ✗ | ✓ |
| Part | Description | Used Network |
|---|---|---|
| Patients | Wearable devices (glucometer, fitness bands, heart rate monitoring cuffs, ingestible, and blood pressure), RFID tags, mobiles, and smart watches | WSN and RFID and MANET |
| Physicians | RFID tags, mobiles, sensors (monitoring and medical), clothes, cars, keys, sonar, surgical tools, laparoscopes, respiratory devices, emergency devices, etc. | WSN and RFID and MANET |
| Inventories | RFID tags, sensors (weight, temperature, motion, monitoring, and humidity), cargo, lamps, workers, books, offices, etc. | WSN and RFID |
| Pharmacy | RFID tags, sensors (temperature, touch, motion, monitoring and humidity), mobile applications, refractometer, thermometer, microscope, vacuum oven, etc. | WSN and RFID and MANET |
| Insurance Company | RFID tags, sensors (temperature, monitoring, and touch), and selected insurance company devices | WSN and RFID |
| Part | Description |
|---|---|
| Hash | Secure Hash Algorithm (SHA)-256 |
| Block size | 1 MB |
| Number of clusters | Random (10 to 100) |
| Cluster size | Random (50 to 100) |
| Total number of miners | Random (10,000 to 200,000) |
| Number of selected miners | Random (10 to 50) |
| Number of blocks | Random (144 to 288) |
| Importance of block | Random (1/2 H: 1/4 M: 1/4 L) |
| Number of digital signatures | Random (1 to 10) |
| Total number of nodes | Random (20,000 to 40,000) |
| Performance Metric | Enhancement |
|---|---|
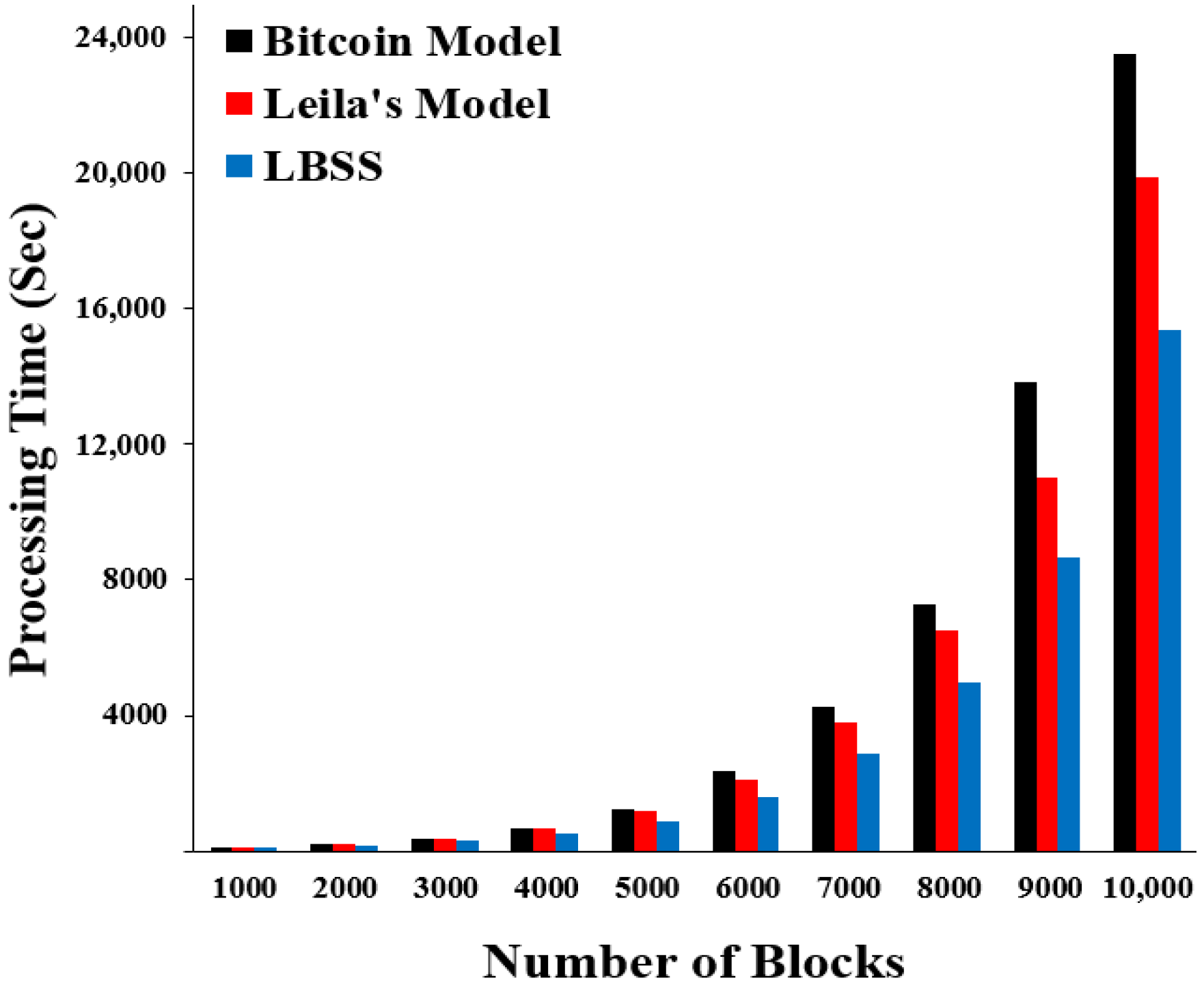
| The average processing time for transaction integrity | Decreased by ≈ 22.727% ↓—Leila’s model. Decreased by ≈ 34.349% ↓—Bitcoin model |
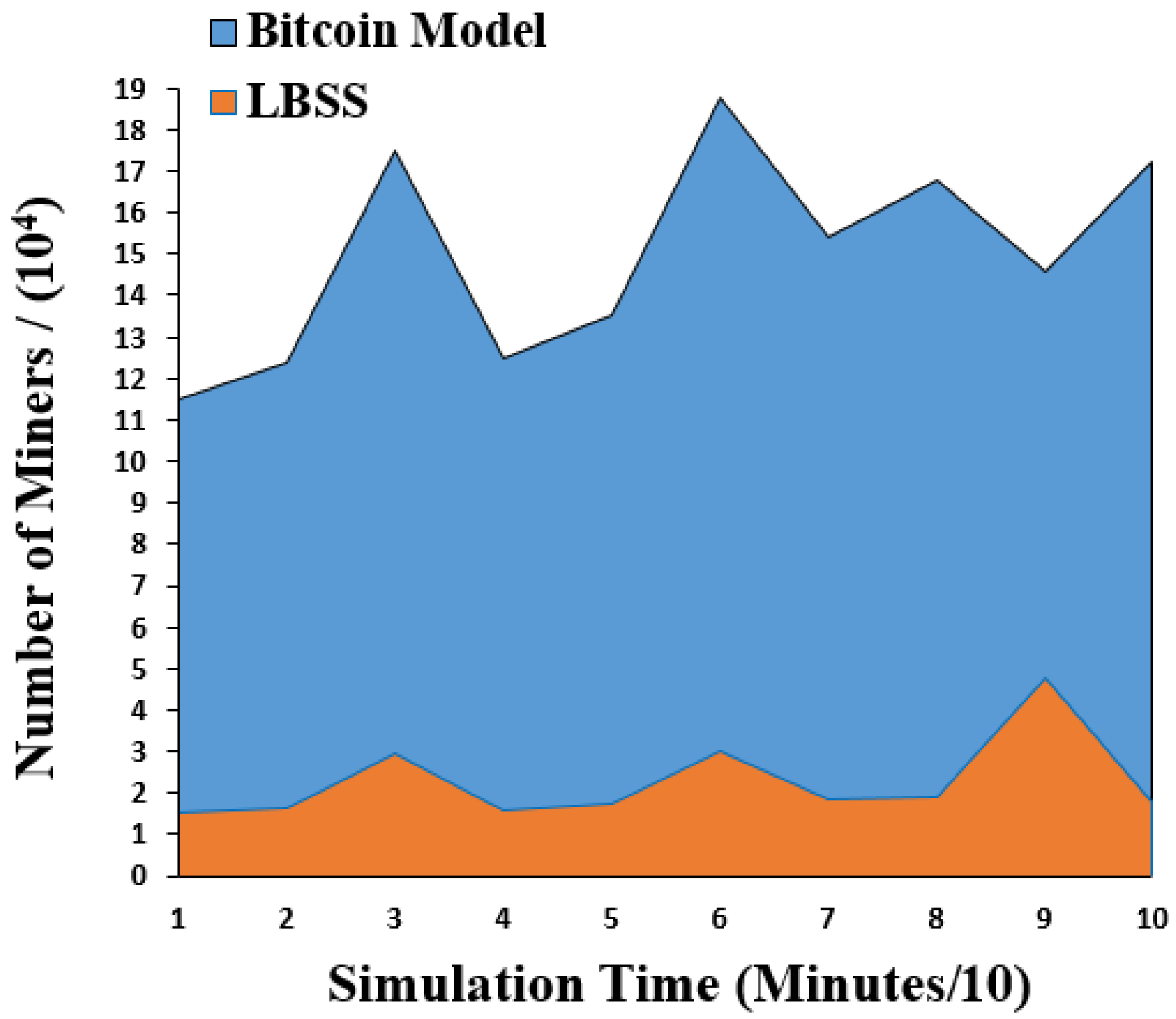
| The changing rate of miners | Decreased by ≈ 84.821% ↓—Bitcoin model. |
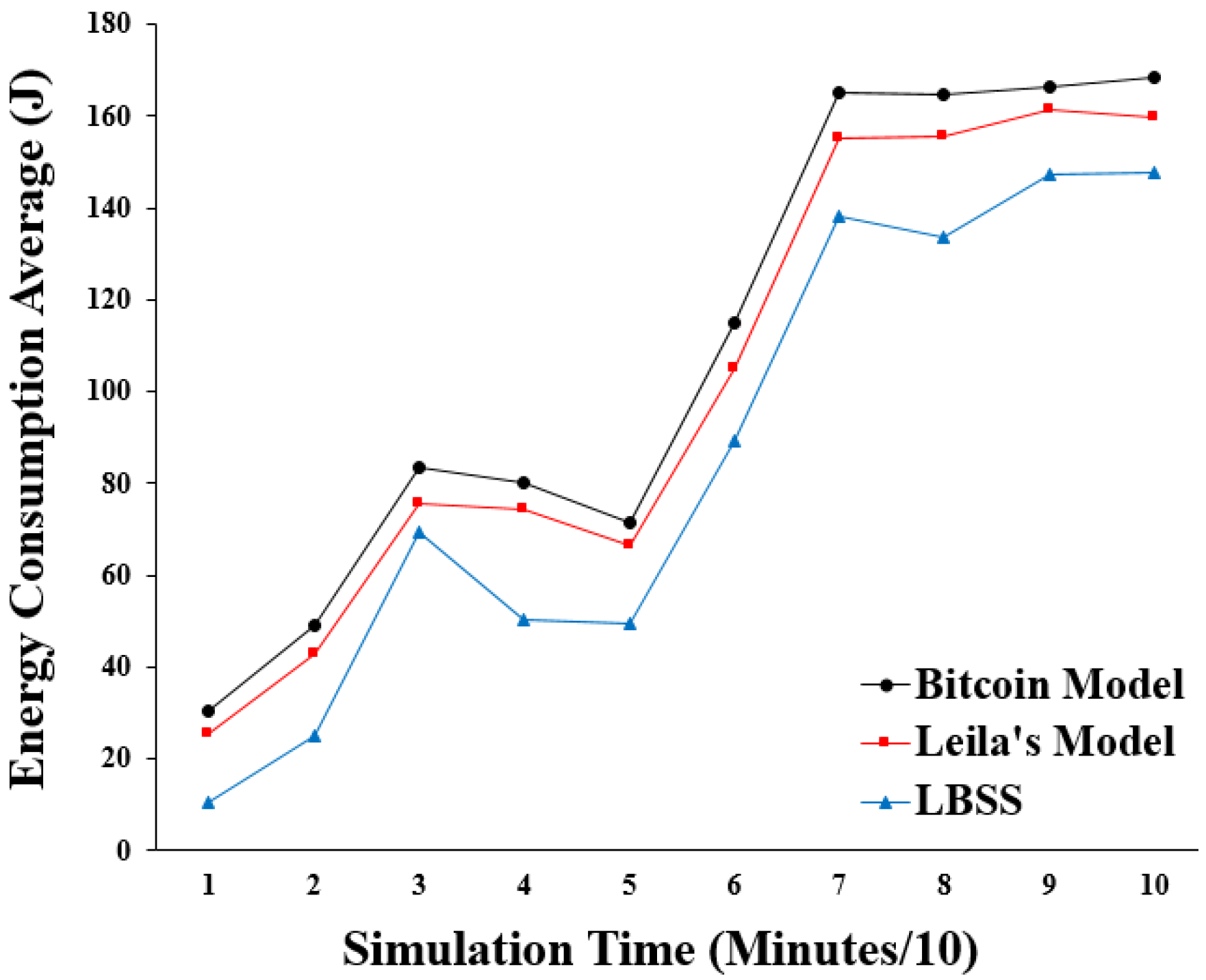
| The energy consumption average | Decreased by ≈ 15.752% ↓—Leila’s model. Decreased by ≈ 21.367% ↓—Bitcoin model. |
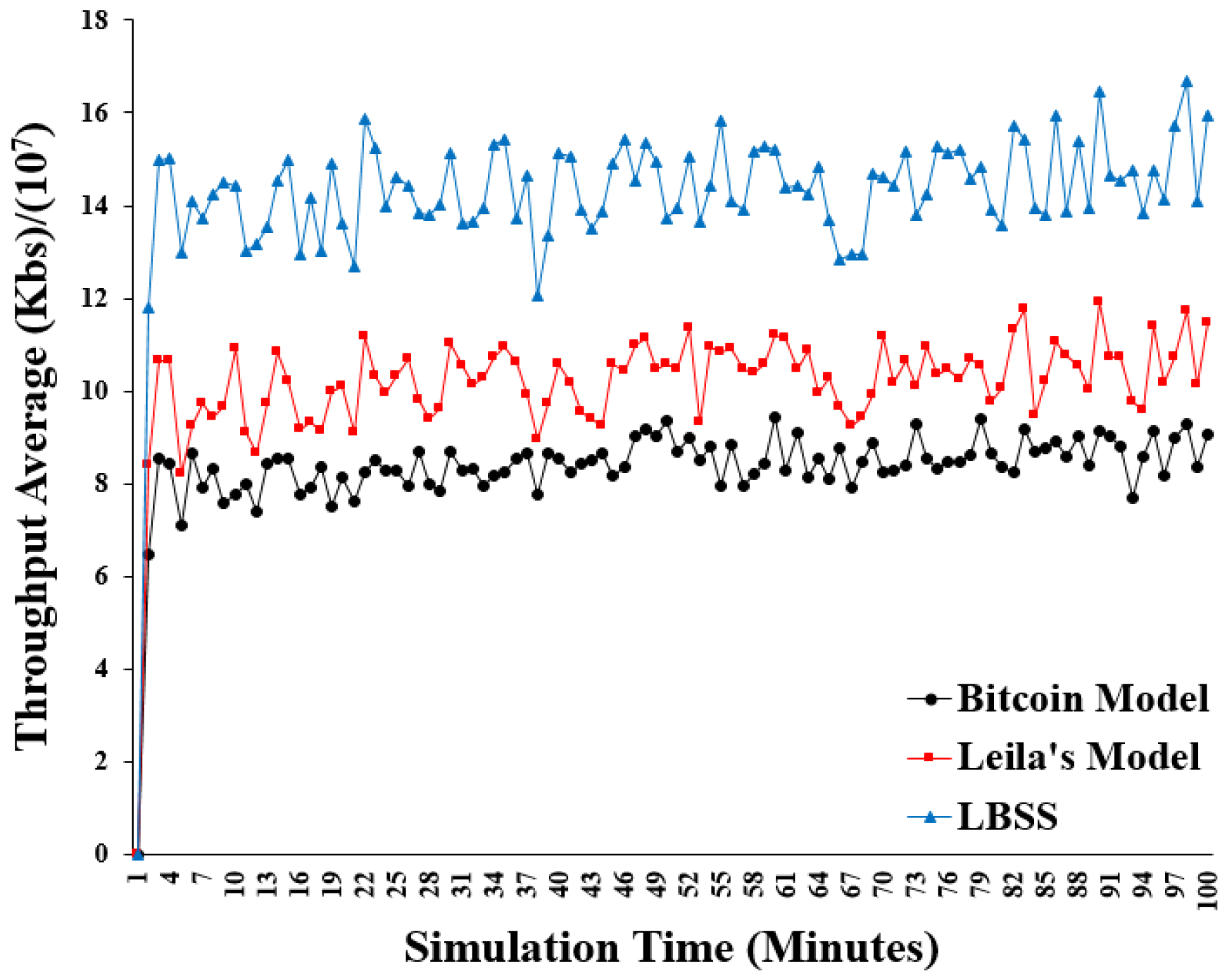
| The average throughput | Increased by ≈ 28.643% ↑—Leila’s model. Increased by ≈ 41.347% ↑—Bitcoin model. |
| The end-to-end delay | Decreased by ≈ 25.865% ↓—Leila’s model. Decreased by ≈ 42.171% ↓—Bitcoin model. |
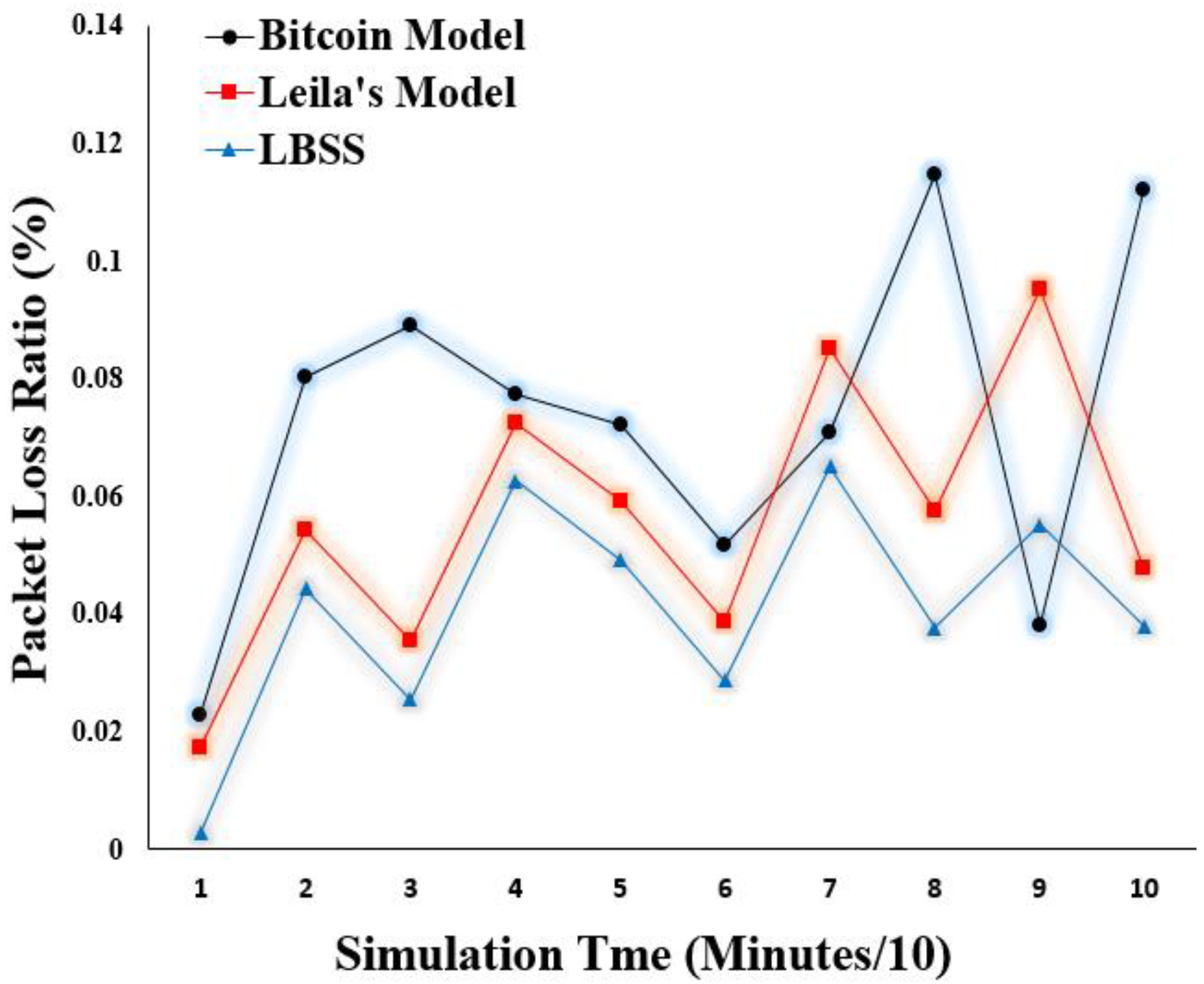
| The packet loss ratio | Decreased by ≈ 27.404% ↓—Leila’s model. Decreased by ≈ 43.880% ↓—Bitcoin model. |
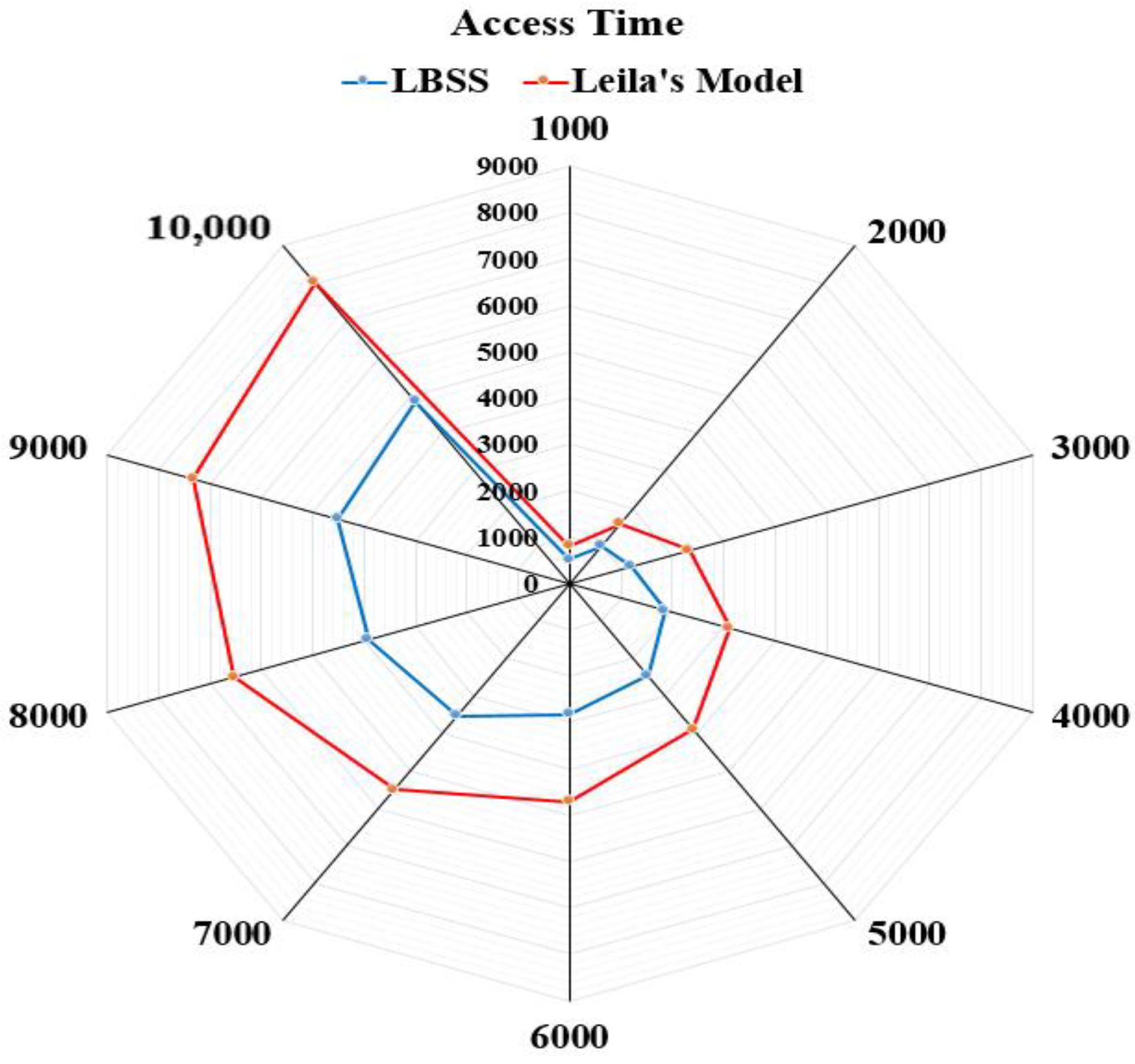
| The access time for the healthcare data blocks | Decreased by ≈ 39.189% ↓—Leila’s model. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, O. LBSS: A Lightweight Blockchain-Based Security Scheme for IoT-Enabled Healthcare Environment. Sensors 2022, 22, 7948. https://doi.org/10.3390/s22207948
Said O. LBSS: A Lightweight Blockchain-Based Security Scheme for IoT-Enabled Healthcare Environment. Sensors. 2022; 22(20):7948. https://doi.org/10.3390/s22207948
Chicago/Turabian StyleSaid, Omar. 2022. "LBSS: A Lightweight Blockchain-Based Security Scheme for IoT-Enabled Healthcare Environment" Sensors 22, no. 20: 7948. https://doi.org/10.3390/s22207948
APA StyleSaid, O. (2022). LBSS: A Lightweight Blockchain-Based Security Scheme for IoT-Enabled Healthcare Environment. Sensors, 22(20), 7948. https://doi.org/10.3390/s22207948