


Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics?

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
- Collecting scans;
- Modification, positioning, and analysis of the scans;
- Data analysis and comparison.
2.1. Collecting Scans—Selection Criteria
- Facial expression: only calm, neutral faces with closed mouth and no facial expression were compared;
- Change in BMI: only pairs of scans separated by less than 7 days were included;
- Extreme artifacts: only CBCTs without extensive artifacts were included.
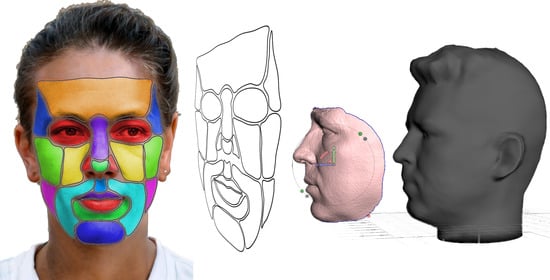
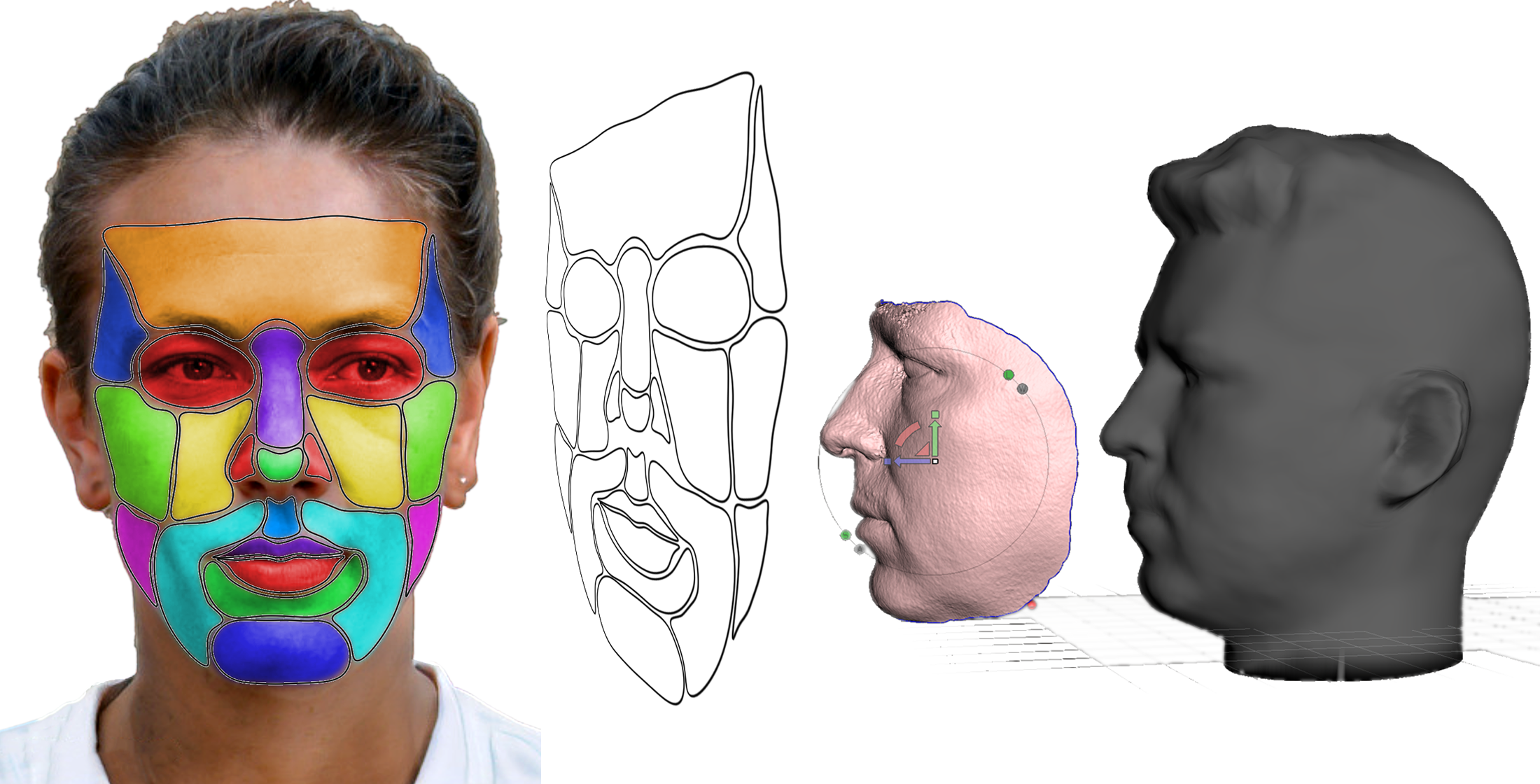
2.2. Modification, Positioning and Analyzing of the Scans
2.3. Data Analysis and Comparison
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vogt, M.; Rips, A.; Emmelmann, C. Comparison of IPad Pro®’s LiDAR and TrueDepth Capabilities with an Industrial 3D Scanning Solution. Technologies 2021, 9, 25. [Google Scholar] [CrossRef]
- Breitbarth, A.; Schardt, T.; Kind, C.; Brinkmann, J.; Dittrich, P.-G.; Notni, G. Measurement Accuracy and Dependence on External Influences of the IPhone X TrueDepth Sensor. Photonics Educ. Meas. Sci. 2019, 11144, 27–33. [Google Scholar] [CrossRef]
- Pellitteri, F.; Brucculeri, L.; Spedicato, G.A.; Siciliani, G.; Lombardo, L. Comparison of the Accuracy of Digital Face Scans Obtained by Two Different Scanners: An in Vivo Study. Angle Orthod. 2021, 91, 641–649. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Al-Mashraqi, A.A.; Alnami, R.H.; Ashqar, N.M.; Alamir, O.H.; Halboub, E.; Reda, R.; Testarelli, L.; Patil, S. Diagnostics Accuracy and Reproducibility of Facial Measurements of Digital Photographs and Wrapped Cone Beam Computed Tomography (CBCT) Photographs. Diagnostics 2021, 11, 757. [Google Scholar] [CrossRef]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically Applicable Artificial Intelligence System for Dental Diagnosis with CBCT. Sci. Rep. 2021, 11, 15006. [Google Scholar] [CrossRef]
- Pauwels, R. What Is CBCT and How Does It Work? In Maxillofacial Cone Beam Computed Tomography: Principles, Techniques and Clinical Applications; Springer: Berlin/Heidelberg, Germany, 2018; pp. 13–42. [Google Scholar] [CrossRef]
- Jain, S.; Choudhary, K.; Nagi, R.; Shukla, S.; Kaur, N.; Grover, D. New Evolution of Cone-Beam Computed Tomography in Dentistry: Combining Digital Technologies. Imaging Sci. Dent. 2019, 49, 179–190. [Google Scholar] [CrossRef]
- Mao, W.-Y.; Lei, J.; Lim, L.Z.; Gao, Y.; A Tyndall, D.; Fu, K. Comparison of Radiographical Characteristics and Diagnostic Accuracy of Intraosseous Jaw Lesions on Panoramic Radiographs and CBCT. Dentomaxillofac. Radiol. 2021, 50, 20200165. [Google Scholar] [CrossRef] [PubMed]
- Shujaat, S.; Bornstein, M.M.; Price, J.B.; Jacobs, R. Integration of Imaging Modalities in Digital Dental Workflows—Possibilities, Limitations, and Potential Future Developments. Dentomaxillofac. Radiol. 2021, 50, 20210268. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Waczulíková, I.; Kurilová, V.; Mriňáková, B.; Kosnáčová, H.; Gális, B.; Varga, I.; Matajs, M.; Novák, B. Dental Care and Education Facing Highly Transmissible SARS-CoV-2 Variants: Prospective Biosafety Setting: Prospective, Single-Arm, Single-Center Study. Int. J. Environ. Res. Public Health 2022, 19, 7693. [Google Scholar] [CrossRef]
- Thurzo, A.; Kurilová, V.; Varga, I. Artificial Intelligence in Orthodontic Smart Application for Treatment Coaching and Its Impact on Clinical Performance of Patients Monitored with AI-Telehealth System. Healthcare 2021, 9, 1695. [Google Scholar] [CrossRef]
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Dzelzkalēja, L.; Knēts, J.K.; Rozenovskis, N.; Sīlītis, A. Mobile Apps for 3D Face Scanning. Lect. Notes Netw. Syst. 2022, 295, 34–50. [Google Scholar] [CrossRef]
- Amornvit, P.; Sanohkan, S. The Accuracy of Digital Face Scans Obtained from 3D Scanners: An In Vitro Study. Int. J. Environ. Res. Public Health 2019, 16, 5061. [Google Scholar] [CrossRef]
- Gupta, M. Digital Diagnosis and Treatment Planning. In Digitization in Dentistry; Springer Nature: Berlin, Germany, 2021; pp. 29–63. [Google Scholar] [CrossRef]
- BCC Research Editorial Brief History of LiDAR, Its Evolution and Market Definition. Available online: https://blog.bccresearch.com/brief-history-of-lidar-evolution-and-market-definition (accessed on 30 July 2022).
- Schmid, K.; Carter, J.; Waters, K.; Betzhold, L.; Hadley, B.; Mataosky, R.; Halleran, J. Lidar 101: An Introduction to Lidar Technology, Data, and Applications; NOAA: Washington, DC, USA, 2012. [Google Scholar]
- Cruz, R.D.; Malong, B. Reality Bytes It’s Real Life, Only Better; Outlook Publishing India Pvt. Ltd.: New Delhi, India, 2020. [Google Scholar]
- How Accurate Are Facial Recognition Systems—and Why Does It Matter?|Center for Strategic and International Studies. Available online: https://www.csis.org/blogs/technology-policy-blog/how-accurate-are-facial-recognition-systems-%E2%80%93-and-why-does-it-matter (accessed on 3 September 2022).
- TrueDepth|Apple Wiki|Fandom. Available online: https://apple.fandom.com/wiki/TrueDepth (accessed on 3 September 2022).
- What Is Apple Face ID and How Does It Work? Available online: https://www.pocket-lint.com/phones/news/apple/142207-what-is-apple-face-id-and-how-does-it-work (accessed on 3 September 2022).
- Kołakowska, A.; Szwoch, W.; Szwoch, M. A Review of Emotion Recognition Methods Based on Data Acquired via Smartphone. Sensors 2020, 20, 6367. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, Y.; Zhang, S.; Ogai, H. Deep 3D Object Detection Networks Using LiDAR Data: A Review. IEEE Sens. J. 2020, 21, 1152–1171. [Google Scholar] [CrossRef]
- Ko, K.; Gwak, H.; Thoummala, N.; Kwon, H.; Kim, S. SqueezeFace: Integrative Face Recognition Methods with LiDAR Sensors. J. Sens. 2021, 2021, 4312245. [Google Scholar] [CrossRef]
- Cameron, A.; Custódio, A.L.N.; Bakr, M.; Reher, P. A Simplified CAD/CAM Extraoral Surgical Guide for Therapeutic Injections. J. Dent. Anesthesia Pain Med. 2021, 21, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Alazzam, A.; Aljarba, S.; Alshomer, F.; Alawirdhi, B. The Utility of Smartphone 3D Scanning, Open-Sourced Computer-Aided Design, and Desktop 3D Printing in the Surgical Planning of Microtia Reconstruction: A Step by Step Guide and Concept Assessment. JPRAS Open 2021, 30, 17–22. [Google Scholar] [CrossRef]
- Alisha, K.H.; Batra, P.; Raghavan, S.; Sharma, K.; Talwar, A. A New Frame for Orienting Infants with Cleft Lip and Palate during 3-Dimensional Facial Scanning. Cleft Palate-Craniofacial J. 2021, 59, 946–950. [Google Scholar] [CrossRef]
- Jayaratne, Y.S.; McGrath, C.P.; Zwahlen, R.A. A Comparison of CBCT Soft Tissue with Bellus3D Facial Scan Superimposition. PLoS ONE 2012, 7, e49585. [Google Scholar] [CrossRef]
- Here Is How Face ID with a Mask Works to Unlock Your IPhone|NextPit. Available online: https://www.nextpit.com/how-to-use-face-id-with-mask-ios-iphone (accessed on 3 September 2022).
- Fountoulaki, G.; Thurzo, A. Change in the Constricted Airway in Patients after Clear Aligner Treatment: A Retrospective Study. Diagnostics 2022, 12, 2201. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Palomo, J.M.; Matthaios, S.; Tsolakis, A.I. Dental and Skeletal Side Effects of Oral Appliances Used for the Treatment of Obstructive Sleep Apnea and Snoring in Adult Patients—A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 483. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Gizani, S.; Tsolakis, A.I.; Panayi, N. Three-Dimensional-Printed Customized Orthodontic and Pedodontic Appliances: A Critical Review of a New Era for Treatment. Children 2022, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Verikokos, C.; Perrea, D.; Bitsanis, E.; Tsolakis, A.I. Effects of Diet Consistency on Mandibular Growth. A Review. J. Hell. Veter. Med. Soc. 2019, 70, 1603–1610. [Google Scholar] [CrossRef]
- Qiang, J.; Wu, D.; Du, H.; Zhu, H.; Chen, S.; Pan, H. Review on Facial-Recognition-Based Applications in Disease Diagnosis. Bioengineering 2022, 9, 273. [Google Scholar] [CrossRef]
- Latorre-Pellicer, A.; Ascaso, Á.; Trujillano, L.; Gil-Salvador, M.; Arnedo, M.; Lucia-Campos, C.; Antoñanzas-Pérez, R.; Marcos-Alcalde, I.; Parenti, I.; Bueno-Lozano, G.; et al. Evaluating Face2Gene as a Tool to Identify Cornelia de Lange Syndrome by Facial Phenotypes. Int. J. Mol. Sci. 2020, 21, 1042. [Google Scholar] [CrossRef]
- Wu, Z.; Zhang, Q. A PorTable 3D Shape Measurement System Developed with a Smartphone PorTable 3D Shape Measurement Based on Mobile Platform View Project Flapping Wing Compliant Mechanism View Project A PorTable 3D Shape Measurement System Developed with a Smartphone. 2019. Available online: https://doi.org/10.13140/RG.2.2.21942.45126 (accessed on 10 October 2022).
- Rudy, H.L.; Wake, N.; Yee, J.; Garfein, E.S.; Tepper, O.M. Three-Dimensional Facial Scanning at the Fingertips of Patients and Surgeons: Accuracy and Precision Testing of IPhone X Three-Dimensional Scanner. Plast. Reconstr. Surg. 2020, 146, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Mandolini, M.; Brunzini, A.; Facco, G.; Mazzoli, A.; Forcellese, A.; Gigante, A. Comparison of Three 3D Segmentation Software Tools for Hip Surgical Planning. Sensors 2022, 22, 5242. [Google Scholar] [CrossRef]
- Rawlani, R.; Qureshi, H.; Rawlani, V.; Turin, S.Y.; Mustoe, T.A. Volumetric Changes of the Mid and Lower Face with Animation and the Standardization of Three-Dimensional Facial Imaging. Plast. Reconstr. Surg. 2019, 143, 76–85. [Google Scholar] [CrossRef]
- le Fur, I.; Reinberg, A.; Lopez, S.; Morizot, F.; Mechkouri, M.; Tschachler, E. Analysis of Circadian and Ultradian Rhythms of Skin Surface Properties of Face and Forearm of Healthy Women. J. Investig. Dermatol. 2001, 117, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Reinberg, A.; Koulbanis, C.; Soudant, E.; Nicolai, A.; Mechkouri, M.; Smolensky, M. Day-Night Differences in Effects of Cosmetic Treatments on Facial Skin. Effects on Facial Skin Appearance. Chronobiol. Int. 2009, 7, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Sforza, C.; Poggio, C.E.; Schmitz, J.H. Facial Volume Changes During Normal Human Growth and Development. Anat. Rec. 1998, 250, 480–487. [Google Scholar] [CrossRef]
- Mailey, B.; Baker, J.L.; Hosseini, A.; Collins, J.; Suliman, A.; Wallace, A.M.; Cohen, S.R. Evaluation of Facial Volume Changes after Rejuvenation Surgery Using a 3-Dimensional Camera. Aesthetic Surg. J. 2015, 36, 379–387. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Revilla-León, M.; Zandinejad, A.; Nair, M.K.; Barmak, B.A.; Feilzer, A.J.; Özcan, M. Accuracy of a Patient 3-Dimensional Virtual Representation Obtained from the Superimposition of Facial and Intraoral Scans Guided by Extraoral and Intraoral Scan Body Systems. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- D’Ettorre, G.; Farronato, M.; Candida, E.; Quinzi, V.; Grippaudo, C. A Comparison between Stereophotogrammetry and Smartphone Structured Light Technology for Three-Dimensional Face Scanning. Angle Orthod. 2022, 92, 358–363. [Google Scholar] [CrossRef]
- Quinzi, V.; Polizzi, A.; Ronsivalle, V.; Santonocito, S.; Conforte, C.; Manenti, R.J.; Isola, G.; Giudice, A. Facial Scanning Accuracy with Stereophotogrammetry and Smartphone Technology in Children: A Systematic Review. Children 2022, 9, 1390. [Google Scholar] [CrossRef]
- Saif, W.; Alshibani, A. Smartphone-Based Photogrammetry Assessment in Comparison with a Compact Camera for Construction Management Applications. Appl. Sci. 2022, 12, 1053. [Google Scholar] [CrossRef]
- Nahajowski, M.; Lis, J.; Sarul, M. The Use of Microsensors to Assess the Daily Wear Time of Removable Orthodontic Appliances: A Prospective Cohort Study. Sensors 2022, 22, 2435. [Google Scholar] [CrossRef]
- Chae, J.M.; Rogowski, L.; Mandair, S.; Bay, R.C.; Park, J.H. A CBCT Evaluation of Midpalatal Bone Density in Various Skeletal Patterns. Sensors 2021, 21, 7812. [Google Scholar] [CrossRef]
- Cho, M.H.; Hegazy, M.A.A.; Cho, M.H.; Lee, S.Y. Cone-Beam Angle Dependency of 3D Models Computed from Cone-Beam CT Images. Sensors 2022, 22, 1253. [Google Scholar] [CrossRef]
- Pojda, D.; Tomaka, A.A.; Luchowski, L.; Tarnawski, M. Integration and Application of Multimodal Measurement Techniques: Relevance of Photogrammetry to Orthodontics. Sensors 2021, 21, 8026. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Jančovičová, V.; Hain, M.; Thurzo, M.; Novák, B.; Kosnáčová, H.; Lehotská, V.; Moravanský, N.; Varga, I. Human Remains Identification Using Micro-CT, Spectroscopic and A.I. Methods in Forensic Experimental Reconstruction of Dental Patterns after Concentrated Acid Significant Impact. Molecules 2022, 27, 4035. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervals of Deviation (mm) | Approximation | Clinical Explanation |
|---|---|---|
| 0 | 0 | clinically irrelevant |
| 0–1 | 0.5 | clinically irrelevant |
| 1–3 | 2 | clinically relevant only in extreme detail evaluations for micro-aesthetics |
| 3+ | 4 | clinically relevant, questioning suitability of this method |
| Facial Location | >3mm Men | >3mm Women | >3mm Total | Fisher’s Exact Test (2-Sided) |
|---|---|---|---|---|
| apex of nose | 15.8% | 2.4% | 6.7% | 0.116 |
| ala nasi L | 26.3% | 29.3% | 28.3% | 1.000 |
| ala nasi R | 42.1% | 46.3% | 45.0% | 0.788 |
| nasal bridge L | 5.3% | 4.9% | 5.0% | 0.797 |
| nasal bridge R | 5.3% | 4.9% | 5.0% | 0.797 |
| sulcus nasolabialis L | 0 | 2.4% | 1.7% | 0.850 |
| sulcus nasolabialis R | 0 | 4.9% | 3.3% | 1.000 |
| philtrum | 0 | 0 | 0 | 0.365 |
| vermilion border | 26.3% | 9.8% | 15.0% | 0.171 |
| vermilion | 36.8% | 17.1% | 23.3% | 0.182 |
| oral/labial commisure L | 10.5% | 19.5% | 16.7% | 0.453 |
| oral/labial commisure R | 10.5% | 9.8% | 10.0% | 0.147 |
| oral fissure | 26.3% | 36.6% | 33.3% | 0.342 |
| sulcus mentolabialis | 5.3% | 7.3% | 6.7% | 0.908 |
| zygomatic region | 0 | 2.4% | 1.7% | 0.243 |
| temporal region | 15.8% | 41.5% | 33.3% | 0.140 |
| frontal region | 47.4% | 17.1% | 26.7% | 0.047 |
| orbital region L | 78.9% | 58.5% | 65.0% | 0.154 |
| orbital region R | 89.5% | 58.5% | 68.3% | 0.019 |
| infraorbital region | 0 | 4.9% | 3.3% | 1.000 |
| mental region | 21.1% | 9.8% | 13.3% | 0.601 |
| parotid-masseteric region | 26.3% | 12.2% | 16.7% | 0.406 |
| buccal region | 0 | 12.2% | 8.3% | 0.184 |
| Location | Rank |
|---|---|
| sulcus mentolabialis | 2.80 |
| philtrum | 3.08 |
| apex of nose | 4.01 |
| mental region | 4.33 |
| Vermillion border | 4.34 |
| frontal region | 4.50 |
| oral fissure | 4.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thurzo, A.; Strunga, M.; Havlínová, R.; Reháková, K.; Urban, R.; Surovková, J.; Kurilová, V. Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors 2022, 22, 7752. https://doi.org/10.3390/s22207752
Thurzo A, Strunga M, Havlínová R, Reháková K, Urban R, Surovková J, Kurilová V. Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors. 2022; 22(20):7752. https://doi.org/10.3390/s22207752
Chicago/Turabian StyleThurzo, Andrej, Martin Strunga, Romana Havlínová, Katarína Reháková, Renata Urban, Jana Surovková, and Veronika Kurilová. 2022. "Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics?" Sensors 22, no. 20: 7752. https://doi.org/10.3390/s22207752
APA StyleThurzo, A., Strunga, M., Havlínová, R., Reháková, K., Urban, R., Surovková, J., & Kurilová, V. (2022). Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors, 22(20), 7752. https://doi.org/10.3390/s22207752