
Smart-Home Concept for Remote Monitoring of Instrumental Activities of Daily Living (IADL) in Older Adults with Cognitive Impairment: A Proof of Concept and Feasibility Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
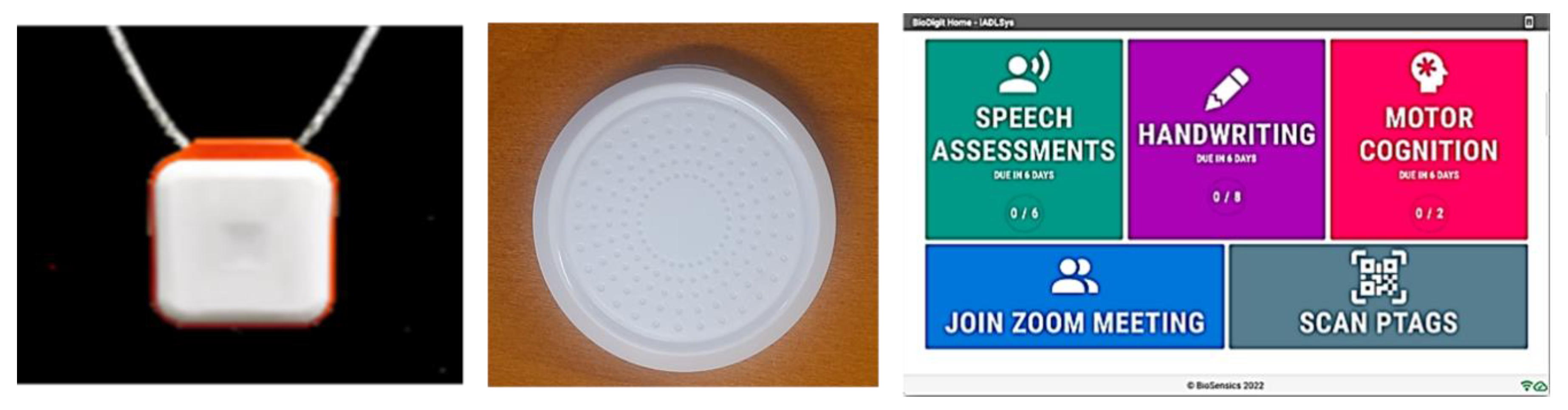
2.1. Concept and Components: IADLSys
- (1)
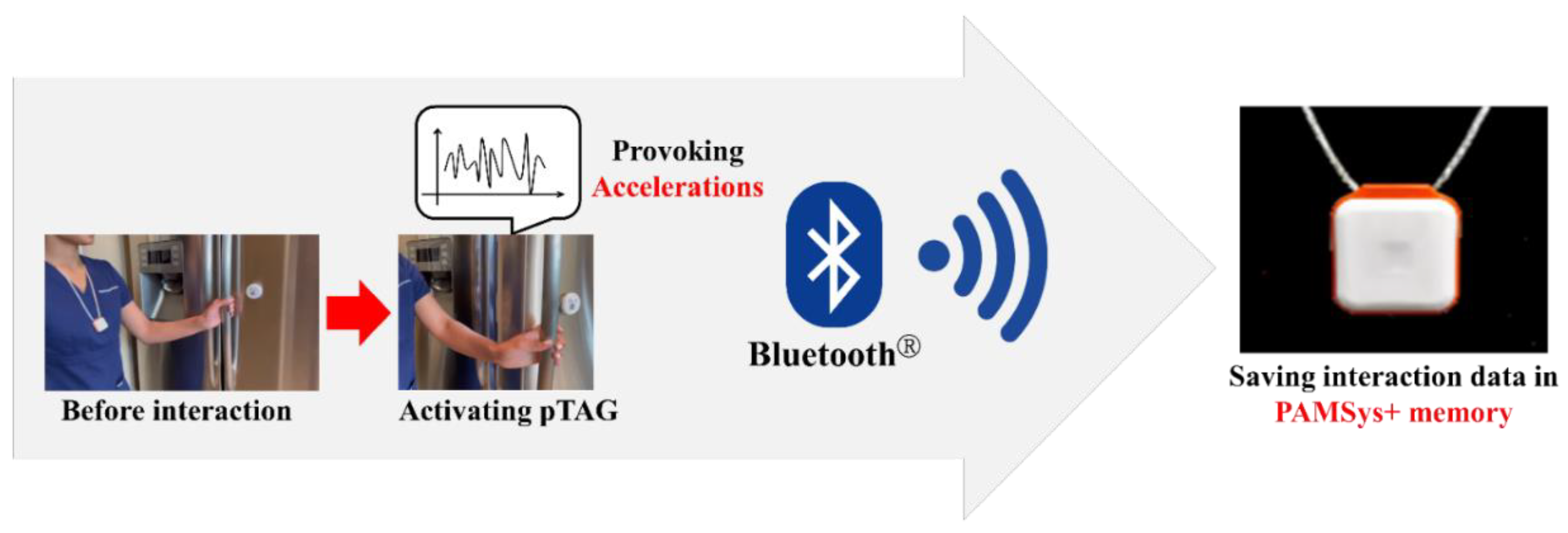
- Physical tag (pTAG): A wireless-based sensor that can be attached to various objects to monitor interactions with these objects in the user’s environment
- (2)
- Monitoring pendant (PAMSys+): A pendant-type wearable sensor monitors the user’s physical activities, as well as interacts when the user is in proximity to the pTAG.
- (3)
- Interactive-tablet PC: The voice-enabled tablet PC can remotely measure and collect questionnaires and other clinical tests such as speech assessment, Trail Making Tests, etc. The collected data can transfer to a secured cloud.
2.2. pTAGs Locations for Objective IADL Assessment
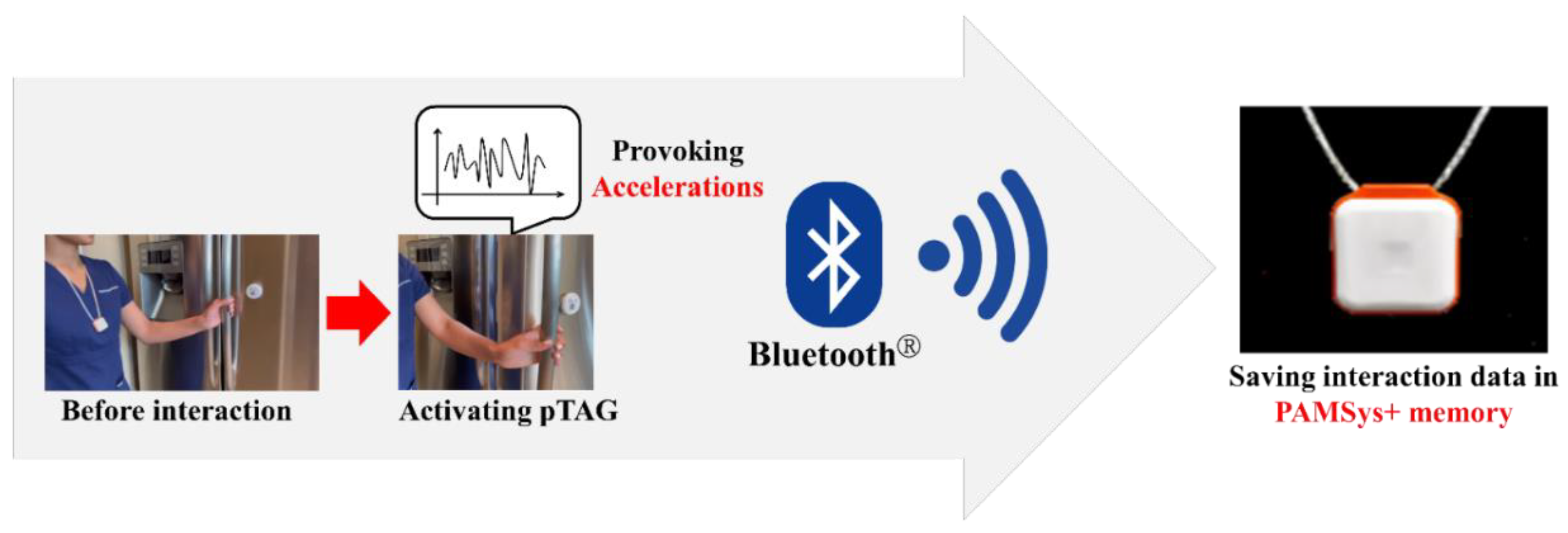
2.3. Principle of the Objective IADL Data Acquisition Using IADLSys
2.4. Data Analysis for the Objective IADL Derived from the IADLSys
2.5. Validity Tests for Assessing Different Components of IADLSys
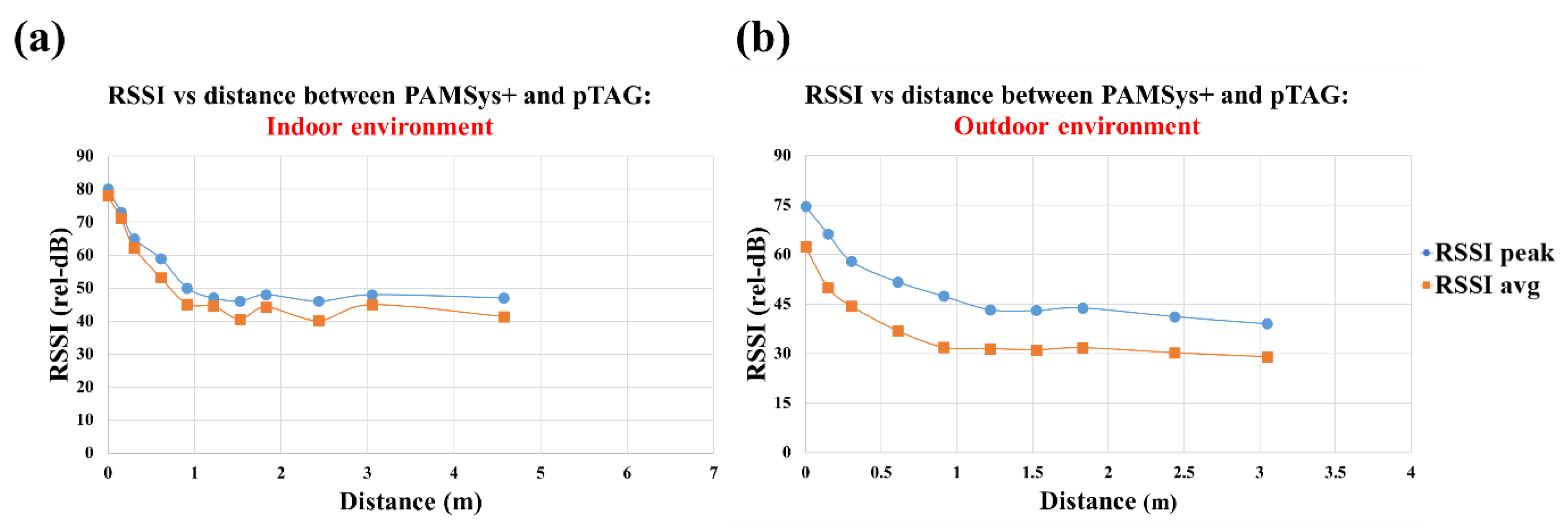
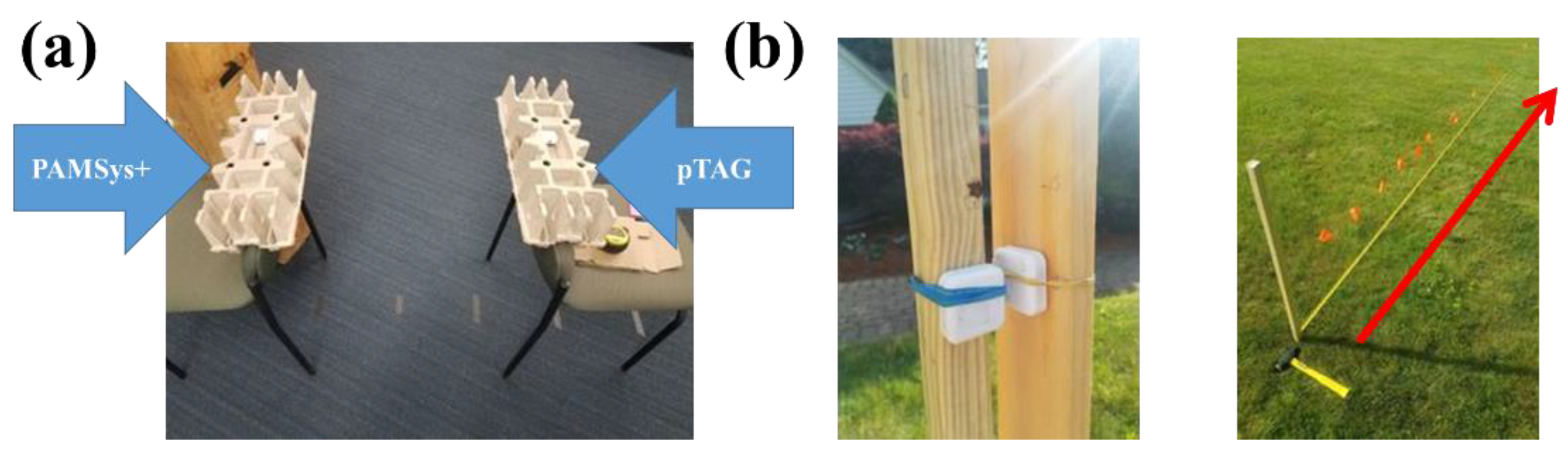
2.5.1. Simulated Tests to Determine Accuracy of Proximity Detection Algorithm
2.5.2. Testing Accuracy of IADLSys to Detect Simulated IADLs
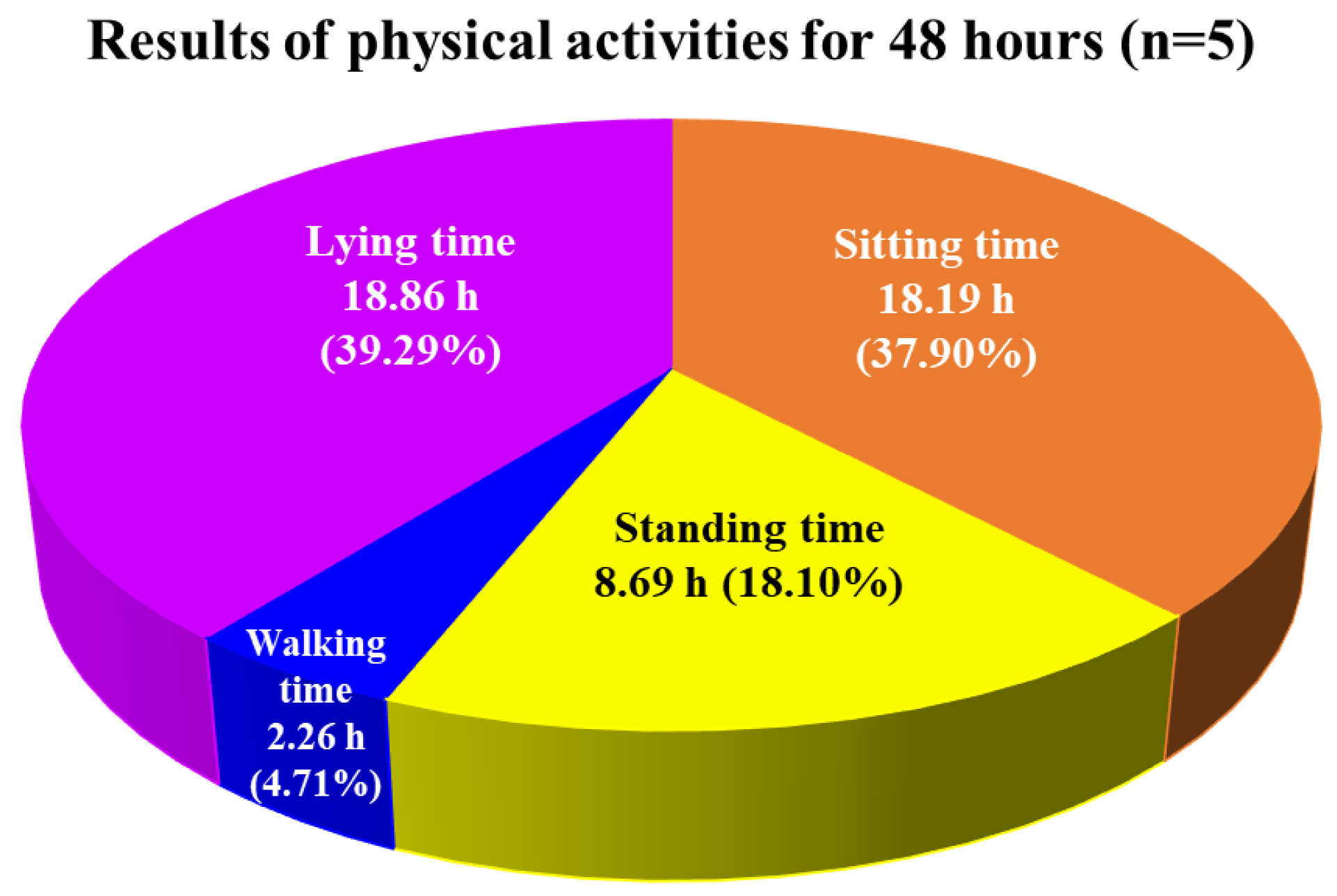
2.5.3. Acceptability of IADLSys to Monitor Daily Physical Activities: Preliminary Test
2.5.4. Proof of Concept of IADLSys to Detect IADLs of Interest during Activities of Daily Living: Case Report
3. Results
3.1. Results of Test 1: Accuracy of Proximity Detection
3.2. Results of Test 2: Accuracy of IADLSys Detection
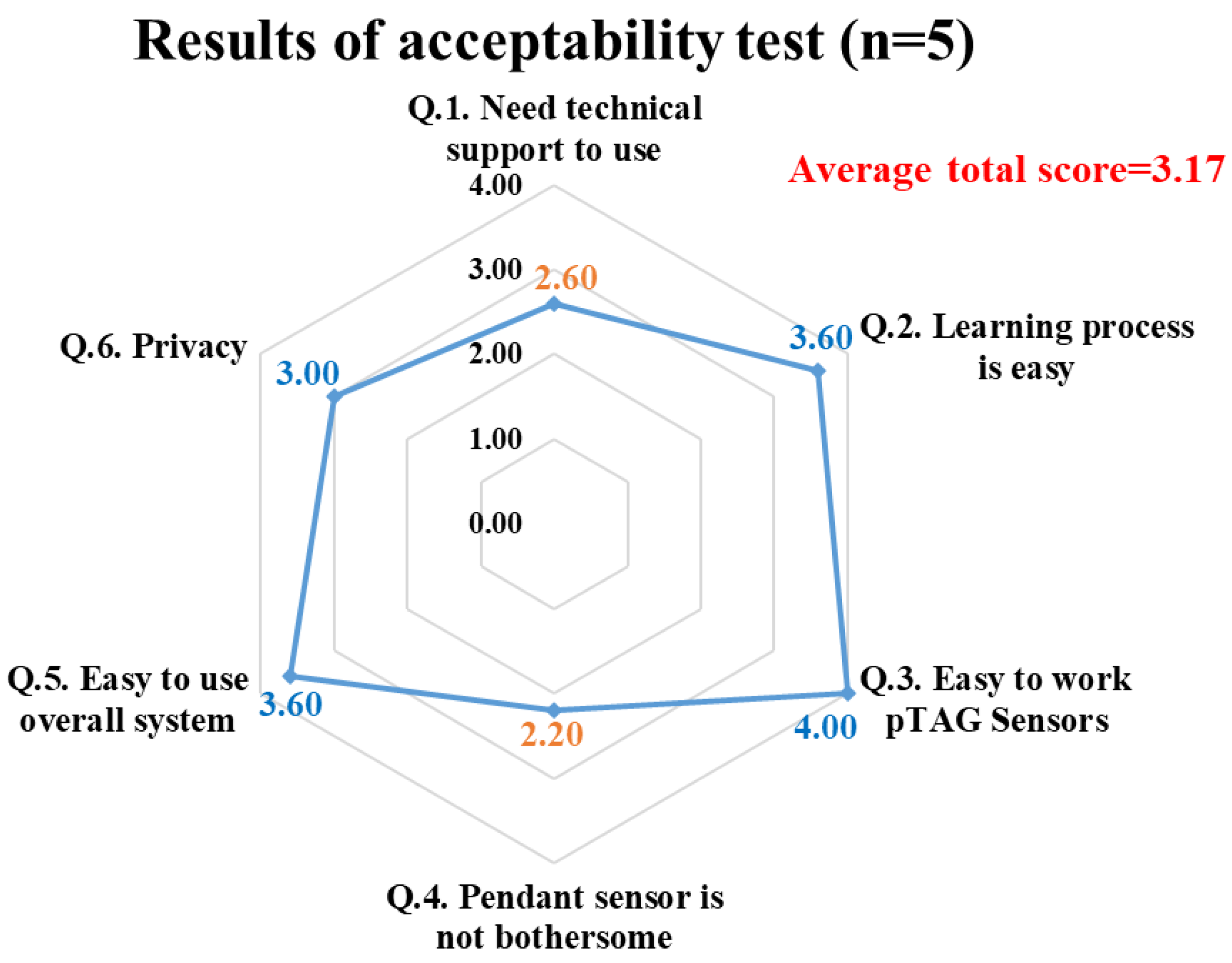
3.3. Results of Test 3: Preliminary Tests of Acceptability on IADLSys
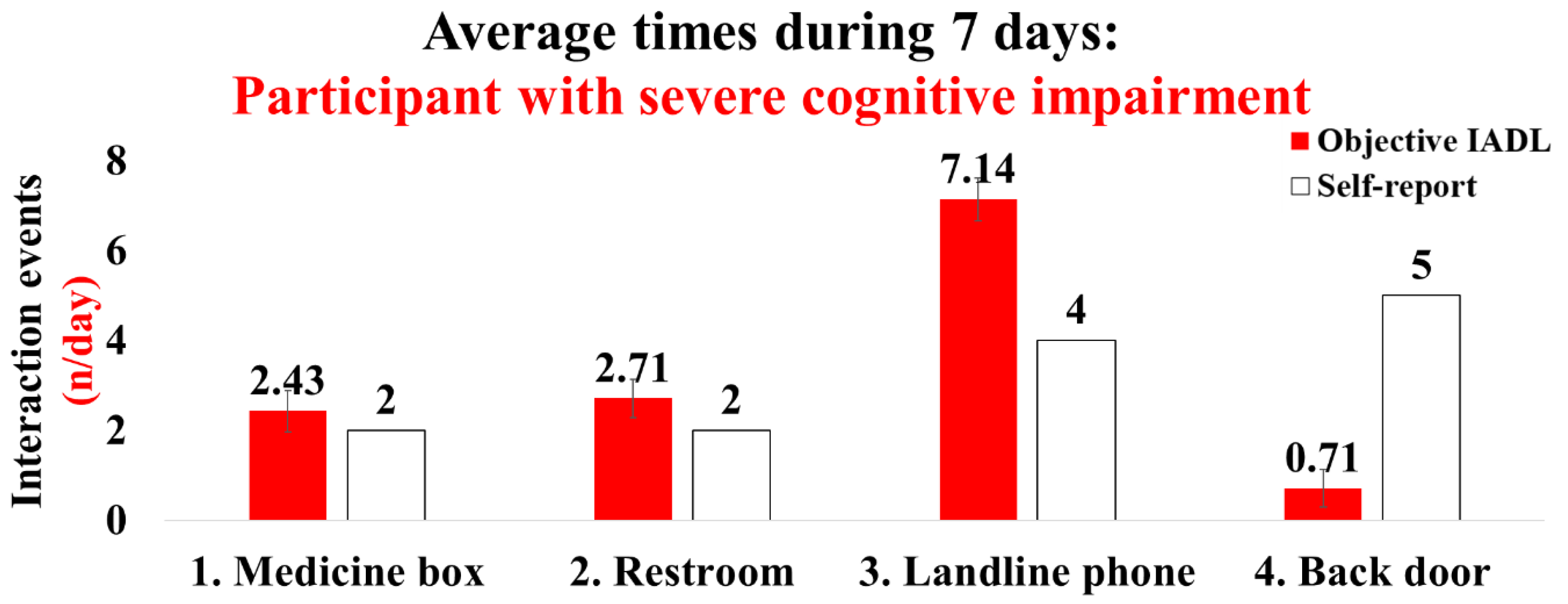
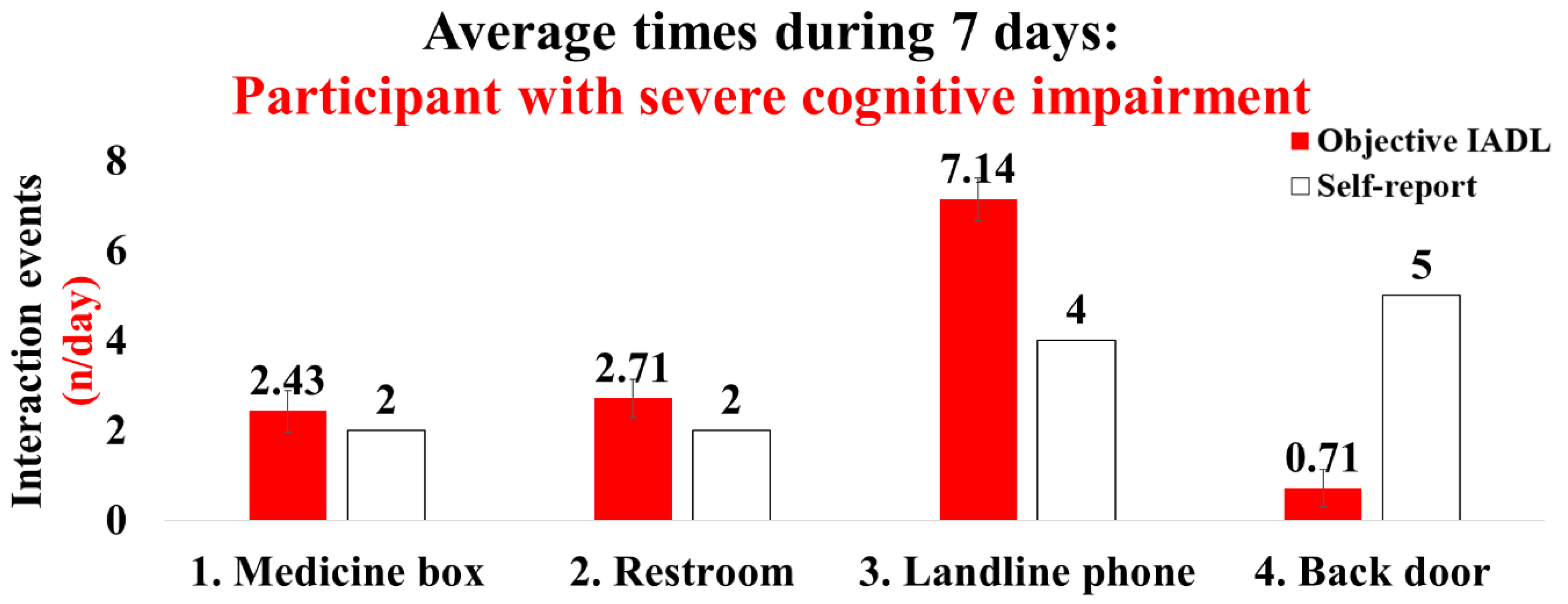
3.4. Results of Test 4: Case Report for IADLSys According to the Cognitive Impairment
4. Discussion
4.1. Demonstrating Feasibility in IADLSys: Objective Home-Based Remote Monitoring System for Assessing IADL
4.2. Strengths and Limitations in This Study
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gale, S.A.; Acar, D.; Daffner, K.R. Dementia. Am. J. Med. 2018, 131, 1161–1169. [Google Scholar] [CrossRef]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef]
- Soria Lopez, J.A.; Gonzalez, H.M.; Leger, G.C. Alzheimer’s disease. Handb. Clin. Neurol. 2019, 167, 231–255. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health and Older Adults. Available online: http://www.who.int/mediacentre/factsheets/fs381/en/ (accessed on 10 June 2022).
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016: Improving Healthcare for People Living with Dementia: Coverage, Quality and Costs Now and in the Future. Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2016.pdf (accessed on 10 June 2022).
- Dutzi, I.; Schwenk, M.; Kirchner, M.; Bauer, J.M.; Hauer, K. Cognitive Change in Rehabilitation Patients with Dementia: Prevalence and Association with Rehabilitation Success. J. Alzheimer’s Dis. 2017, 60, 1171–1182. [Google Scholar] [CrossRef]
- Hauer, K.; Schwenk, M.; Zieschang, T.; Essig, M.; Becker, C.; Oster, P. Physical training improves motor performance in people with dementia: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 8–15. [Google Scholar] [CrossRef]
- Schwenk, M.; Zieschang, T.; Oster, P.; Hauer, K. Dual-task performances can be improved in patients with dementia: A randomized controlled trial. Neurology 2010, 74, 1961–1968. [Google Scholar] [CrossRef]
- Cornelis, E.; Gorus, E.; Beyer, I.; Bautmans, I.; De Vriendt, P. Early diagnosis of mild cognitive impairment and mild dementia through basic and instrumental activities of daily living: Development of a new evaluation tool. PLoS Med. 2017, 14, e1002250. [Google Scholar] [CrossRef]
- Jekel, K.; Damian, M.; Wattmo, C.; Hausner, L.; Bullock, R.; Connelly, P.J.; Dubois, B.; Eriksdotter, M.; Ewers, M.; Graessel, E.; et al. Mild cognitive impairment and deficits in instrumental activities of daily living: A systematic review. Alzheimer’s Res. Ther. 2015, 7, 17. [Google Scholar] [CrossRef]
- Tung, J.Y.; Rose, R.V.; Gammada, E.; Lam, I.; Roy, E.A.; Black, S.E.; Poupart, P. Measuring life space in older adults with mild-to-moderate Alzheimer’s disease using mobile phone GPS. Gerontology 2014, 60, 154–162. [Google Scholar] [CrossRef]
- James, B.D.; Boyle, P.A.; Buchman, A.S.; Barnes, L.L.; Bennett, D.A. Life space and risk of Alzheimer disease, mild cognitive impairment, and cognitive decline in old age. Am. J. Geriatr. Psychiatry 2011, 19, 961–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uemura, K.; Shimada, H.; Makizako, H.; Yoshida, D.; Doi, T.; Yamada, M.; Suzuki, T. Factors associated with life-space in older adults with amnestic mild cognitive impairment. Geriatr. Gerontol. Int. 2013, 13, 161–166. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Gold, D.A. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2012, 34, 11–34. [Google Scholar] [CrossRef]
- Stalvey, B.T.; Owsley, C.; Sloane, M.E.; Ball, K. The Life Space Questionnaire: A measure of the extent of mobility of older adults. J. Appl. Gerontol. 1999, 18, 460–478. [Google Scholar] [CrossRef]
- Hancock, P.; Larner, A. The diagnosis of dementia: Diagnostic accuracy of an instrument measuring activities of daily living in a clinic-based population. Dement. Geriatr. Cogn. Disord. 2007, 23, 133–139. [Google Scholar] [CrossRef]
- Okonkwo, O.C.; Wadley, V.G.; Griffith, H.R.; Belue, K.; Lanza, S.; Zamrini, E.Y.; Harrell, L.E.; Brockington, J.C.; Clark, D.; Raman, R.; et al. Awareness of Deficits in Financial Abilities in Patients With Mild Cognitive Impairment: Going Beyond Self-Informant Discrepancy. Am. J. Geriatr. Psychiatry 2008, 16, 650–659. [Google Scholar] [CrossRef]
- Steward, K.A.; Bull, T.P.; Wadley, V.G. Differences in self-awareness of functional deficits between amnestic single-and multidomain mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2019, 41, 544–553. [Google Scholar] [CrossRef]
- Steward, K.A.; Kennedy, R.; Erus, G.; Nasrallah, I.M.; Wadley, V.G. Poor awareness of IADL deficits is associated with reduced regional brain volume in older adults with cognitive impairment. Neuropsychologia 2019, 129, 372–378. [Google Scholar] [CrossRef]
- Pol, M.C.; Poerbodipoero, S.; Robben, S.; Daams, J.; van Hartingsveldt, M.; de Vos, R.; de Rooij, S.E.; Kröse, B.; Buurman, B.M. Sensor monitoring to measure and support daily functioning for independently living older people: A systematic review and road map for further development. J. Am. Geriatr. Soc. 2013, 61, 2219–2227. [Google Scholar] [CrossRef]
- Jekel, K.; Damian, M.; Storf, H.; Hausner, L.; Frölich, L. Development of a proxy-free objective assessment tool of instrumental activities of daily living in mild cognitive impairment using smart home technologies. J. Alzheimer’s Dis. 2016, 52, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Zylstra, B.; Netscher, G.; Jacquemot, J.; Schaffer, M.; Shen, G.; Bowhay, A.D.; Braley, T.L.; Possin, K.L.; Miller, B.L.; Bayen, A.M. Extended, continuous measures of functional status in community dwelling persons with Alzheimer’s and related dementia: Infrastructure, performance, tradeoffs, preliminary data, and promise. J. Neurosci. Methods 2018, 300, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Cullen, A.; Mazhar, M.K.A.; Smith, M.D.; Lithander, F.E.; Ó Breasail, M.; Henderson, E.J. Wearable and Portable GPS Solutions for Monitoring Mobility in Dementia: A Systematic Review. Sensors 2022, 22, 3336. [Google Scholar] [CrossRef] [PubMed]
- BioDigit Cloud: BioSensics LLC. Available online: https://biosensics.com/products/biodigit-cloud (accessed on 18 August 2022).
- Mishra, R.; Park, C.; York, M.K.; Kunik, M.E.; Wung, S.-F.; Naik, A.D.; Najafi, B. Decrease in mobility during the COVID-19 pandemic and its association with increase in depression among older adults: A longitudinal remote mobility monitoring using a wearable sensor. Sensors 2021, 21, 3090. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Armstrong, D.G.; Mohler, J. Novel Wearable Technology for Assessing Spontaneous Daily Physical Activity and Risk of Falling in Older Adults with Diabetes; SAGE Publications Sage CA: Los Angeles, CA, USA, 2013; pp. 1147–1160. [Google Scholar]
- Schwenk, M.; Mohler, J.; Wendel, C.; Fain, M.; Taylor-Piliae, R.; Najafi, B. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: Baseline results of the Arizona frailty cohort study. Gerontology 2015, 61, 258–267. [Google Scholar] [CrossRef]
- Razjouyan, J.; Najafi, B.; Horstman, M.; Sharafkhaneh, A.; Amirmazaheri, M.; Zhou, H.; Kunik, M.E.; Naik, A. Toward using wearables to remotely monitor cognitive frailty in community-living older adults: An observational study. Sensors 2020, 20, 2218. [Google Scholar] [CrossRef]
- Najafi, B.; Aminian, K.; Paraschiv-Ionescu, A.; Loew, F.; Bula, C.J.; Robert, P. Ambulatory system for human motion analysis using a kinematic sensor: Monitoring of daily physical activity in the elderly. IEEE Trans. Biomed. Eng. 2003, 50, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef]
- Lindberg, C.M.; Srinivasan, K.; Gilligan, B.; Razjouyan, J.; Lee, H.; Najafi, B.; Canada, K.J.; Mehl, M.R.; Currim, F.; Ram, S.; et al. Effects of office workstation type on physical activity and stress. Occup. Environ. Med. 2018, 75, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Aminian, K.; Loew, F.; Blanc, Y.; Robert, P.A. Measurement of stand-sit and sit-stand transitions using a miniature gyroscope and its application in fall risk evaluation in the elderly. IEEE Trans. Biomed. Eng. 2002, 49, 843–851. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, E.D.; Najafi, B.; Murer, K.; Uebelhart, D.; Aminian, K. Quantification of everyday motor function in a geriatric population. J. Rehabil. Res. Dev. 2007, 44, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Crews, R.T.; Wrobel, J.S. Importance of time spent standing for those at risk of diabetic foot ulceration. Diabetes Care 2010, 33, 2448–2450. [Google Scholar] [CrossRef] [PubMed]
- Falck, R.S.; Landry, G.J.; Best, J.R.; Davis, J.C.; Chiu, B.K.; Liu-Ambrose, T. Cross-sectional relationships of physical activity and sedentary behavior with cognitive function in older adults with probable mild cognitive impairment. Phys. Ther. 2017, 97, 975–984. [Google Scholar] [CrossRef]
- Lu, Z.; Harris, T.B.; Shiroma, E.J.; Leung, J.; Kwok, T. Patterns of physical activity and sedentary behavior for older adults with Alzheimer’s disease, mild cognitive impairment, and cognitively normal in Hong Kong. J. Alzheimer’s Dis. 2018, 66, 1453–1462. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Box (Medicine Box) | Cabinet (Refrigerator) | |||
| Positive | Negative | Positive | Negative | |
| Positive (Real activations) | True positive n = 9 | False positive n = 0 | True positive n = 10 | False positive n = 0 |
| Negative (No activations) | False negative n = 0 | True negative n = 10 | False negative n = 0 | True negative n = 9 |
| Sensitivity/Specificity | 100% | 100% | 100% | 100% |
| Accuracy | 100% | 100% | ||
| Cabinet door (Moderate to high) | Room door (Slow) | |||
| Positive | Negative | Positive | Negative | |
| Positive (Real activations) | True positive n = 6 | False positive n = 0 | True positive n = 9 | False positive n = 0 |
| Negative (No activations) | False negative n = 0 | True negative n = 12 | False negative n = 3 | True negative n = 6 |
| Sensitivity/Specificity | 100% | 100% | 75% | 100% |
| Accuracy | 100% | 83.3% | ||
| Variables | Older Adults with Cognitive Impairment (n = 5) |
|---|---|
| Age, yrs | 69.6 (5.4) |
| BMI, kg/m2 | 26.7 (2.8) |
| Gender, female % | 80% |
| Cognitive function (MoCA), score | 23.0 (1.2) |
| IADL (Lawton–Brody IADL), score | 7.8 (0.4) |
| Life-space, score | 5.2 (0.4) |
| Depression (CES-D), score | 5.0 (5.1) |
| Concerns for falling (FES-I), score | 25.4 (15.1) |
| Subjects | Age, yrs | BMI, kg/m2 | MoCA, Score | FES-I, Score | LAWTON, Score | Life-Space, Score |
|---|---|---|---|---|---|---|
| Participant 1 (Female) | 82 | 23.4 | 6 | 21 | 5 | 5 |
| Participant 2 (Female) | 66 | 20.5 | 23 | 33 | 8 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Mishra, R.K.; Momin, A.; El-Refaei, N.; Bagheri, A.B.; York, M.K.; Kunik, M.E.; Derhammer, M.; Fatehi, B.; Lim, J.; et al. Smart-Home Concept for Remote Monitoring of Instrumental Activities of Daily Living (IADL) in Older Adults with Cognitive Impairment: A Proof of Concept and Feasibility Study. Sensors 2022, 22, 6745. https://doi.org/10.3390/s22186745
Lee M, Mishra RK, Momin A, El-Refaei N, Bagheri AB, York MK, Kunik ME, Derhammer M, Fatehi B, Lim J, et al. Smart-Home Concept for Remote Monitoring of Instrumental Activities of Daily Living (IADL) in Older Adults with Cognitive Impairment: A Proof of Concept and Feasibility Study. Sensors. 2022; 22(18):6745. https://doi.org/10.3390/s22186745
Chicago/Turabian StyleLee, Myeounggon, Ram Kinker Mishra, Anmol Momin, Nesreen El-Refaei, Amir Behzad Bagheri, Michele K. York, Mark E. Kunik, Marc Derhammer, Borna Fatehi, James Lim, and et al. 2022. "Smart-Home Concept for Remote Monitoring of Instrumental Activities of Daily Living (IADL) in Older Adults with Cognitive Impairment: A Proof of Concept and Feasibility Study" Sensors 22, no. 18: 6745. https://doi.org/10.3390/s22186745
APA StyleLee, M., Mishra, R. K., Momin, A., El-Refaei, N., Bagheri, A. B., York, M. K., Kunik, M. E., Derhammer, M., Fatehi, B., Lim, J., Cole, R., Barchard, G., Vaziri, A., & Najafi, B. (2022). Smart-Home Concept for Remote Monitoring of Instrumental Activities of Daily Living (IADL) in Older Adults with Cognitive Impairment: A Proof of Concept and Feasibility Study. Sensors, 22(18), 6745. https://doi.org/10.3390/s22186745