


Epileptic Disorder Detection of Seizures Using EEG Signals

Abstract
:1. Introduction
2. Related Works
3. Datasets
4. The Proposed System
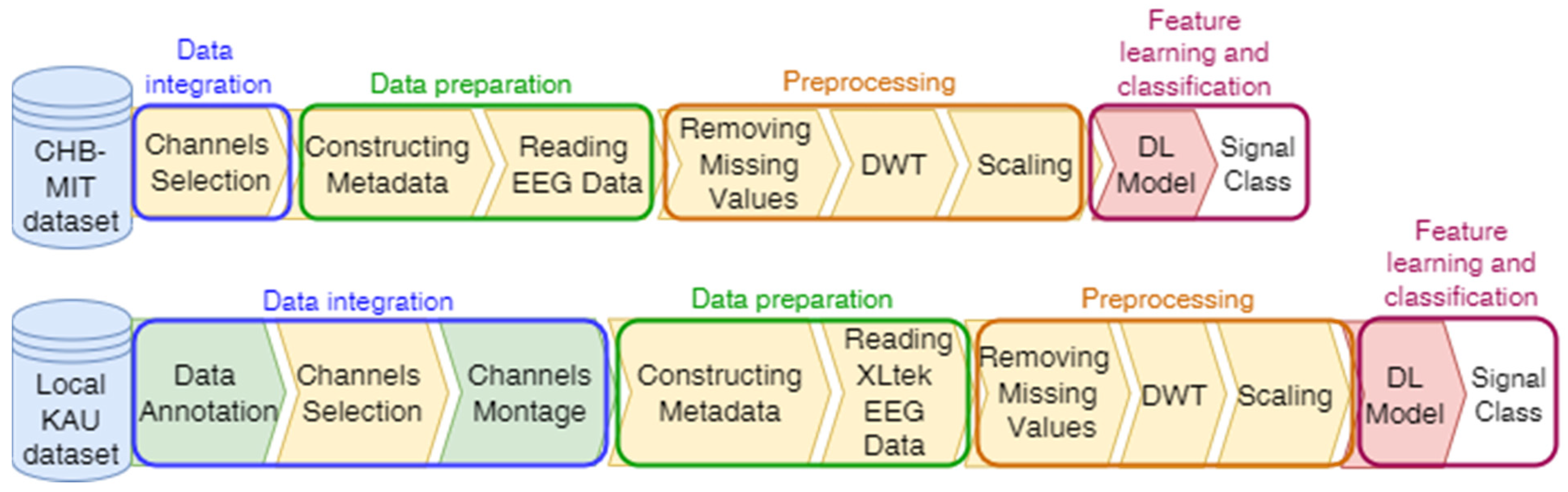
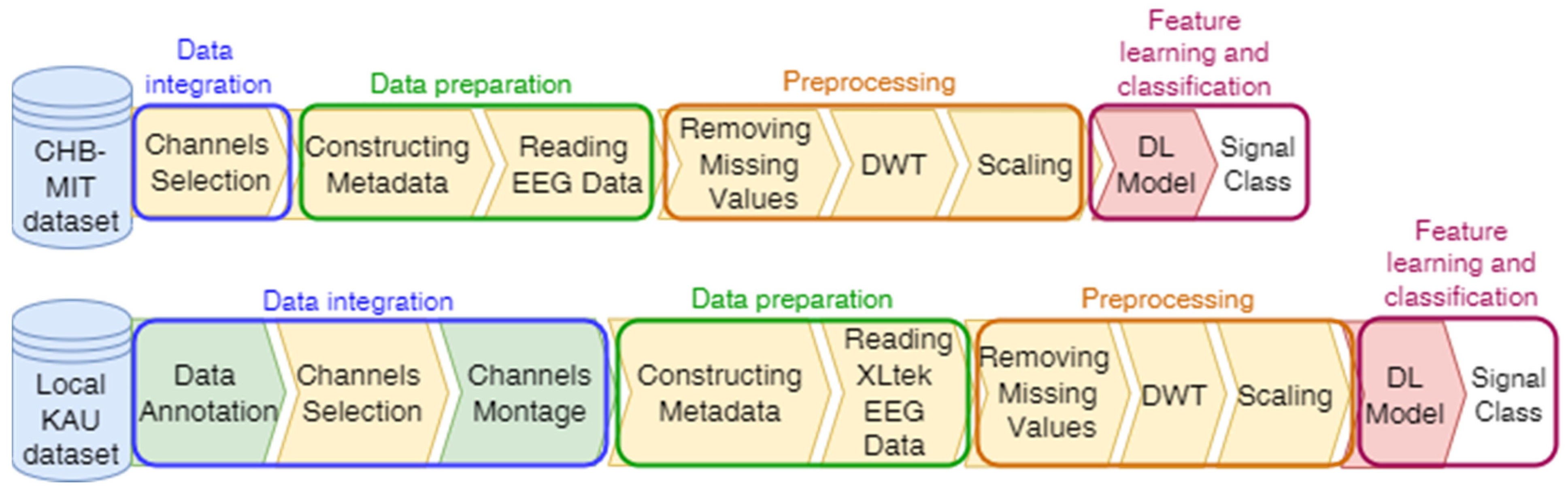
4.1. Compatibility Framework for Data Integration
| Algorithm 1. Reading XLtek EEG Data Algorithm. | |||||
| Input: An EEG signal and the size of window in seconds | |||||
| Output: Array of EEG data samples that constitute the epochs | |||||
| 1 | FUNCTION get_epoch(s, min_secs = 10) | ||||
| 2 | // Extracting signal start time, sample rate, channel names, and number of samples | ||||
| 3 | start_time, s_rate, ch_names, n_samples ← s.return_hdr() | ||||
| 4 | s_rate ← int(round(s_rate)) | ||||
| 5 | // Extracting the creation time for the erd file that holds the raw data | ||||
| 6 | erd_time ← s.return_hdr() [−1][‘creation_time’] | ||||
| 7 | // Excluding samples between the start time of recording and the actual acquisition | ||||
| 8 | stc_erd_diff ← (erd_time–start_time). total_seconds() | ||||
| 9 | // Computing the number of samples required from each channel | ||||
| 10 | stride ← min_secs ∗ s_rate | ||||
| 11 | start_index ← int(stc_erd_diff) ∗ s_rate | ||||
| 12 | end_index ← start_index + stride | ||||
| 13 | findings ← [ ] | ||||
| 14 | WHILE end_index ≤ n_samples DO | ||||
| 15 | t ← s.return_dat ([1], start_index, end_index) | ||||
| 16 | // Excluding the epochs that may contain NaN values | ||||
| 17 | IF ! np.any(np.isnan(t), axis = 1) THEN | ||||
| 18 | data ← s.return_dat(range(len(ch_names)), start_index, end_index) | ||||
| 19 | IF s_rate > 256 THEN | ||||
| 20 | data ← decimate(data, q = 2) | ||||
| 21 | ENDIF | ||||
| 22 | // Converting numpy array to a pandas data frame | ||||
| 23 | df ← pd.DataFrame(data = data.T, columns = ch_names) | ||||
| 24 | findings.append(montage(df, model_modified_channels)) | ||||
| 25 | ENDIF | ||||
| 26 | start_index ← start_index + stride | ||||
| 27 | end_index ← end_index + stride | ||||
| 28 | ENDWHILE | ||||
| 29 | return findings | ||||
| 30 | ENDFUNCTION | ||||
4.2. Seizure Detection Model
5. The Experimental Result
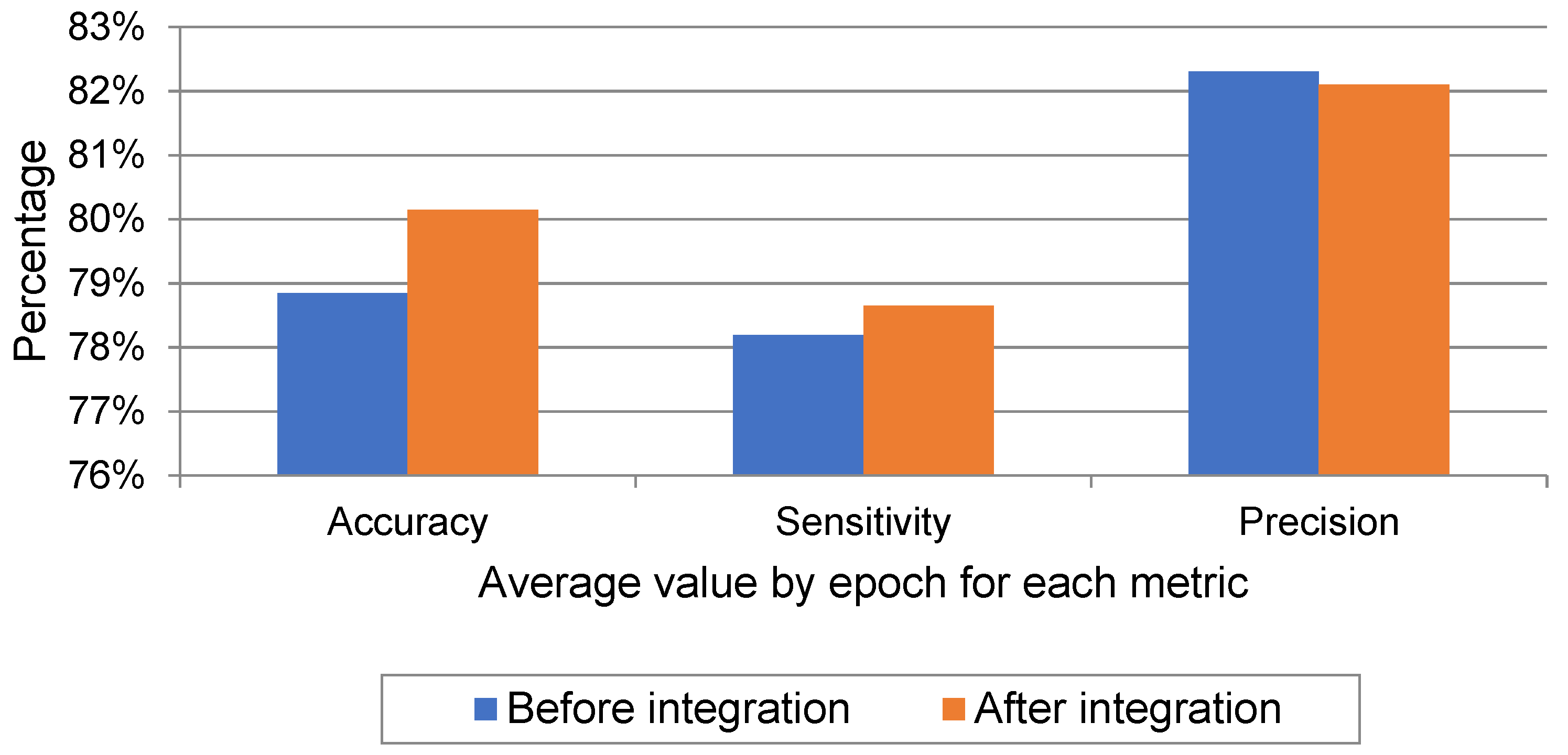
5.1. Evaluating the Compatibility Framework
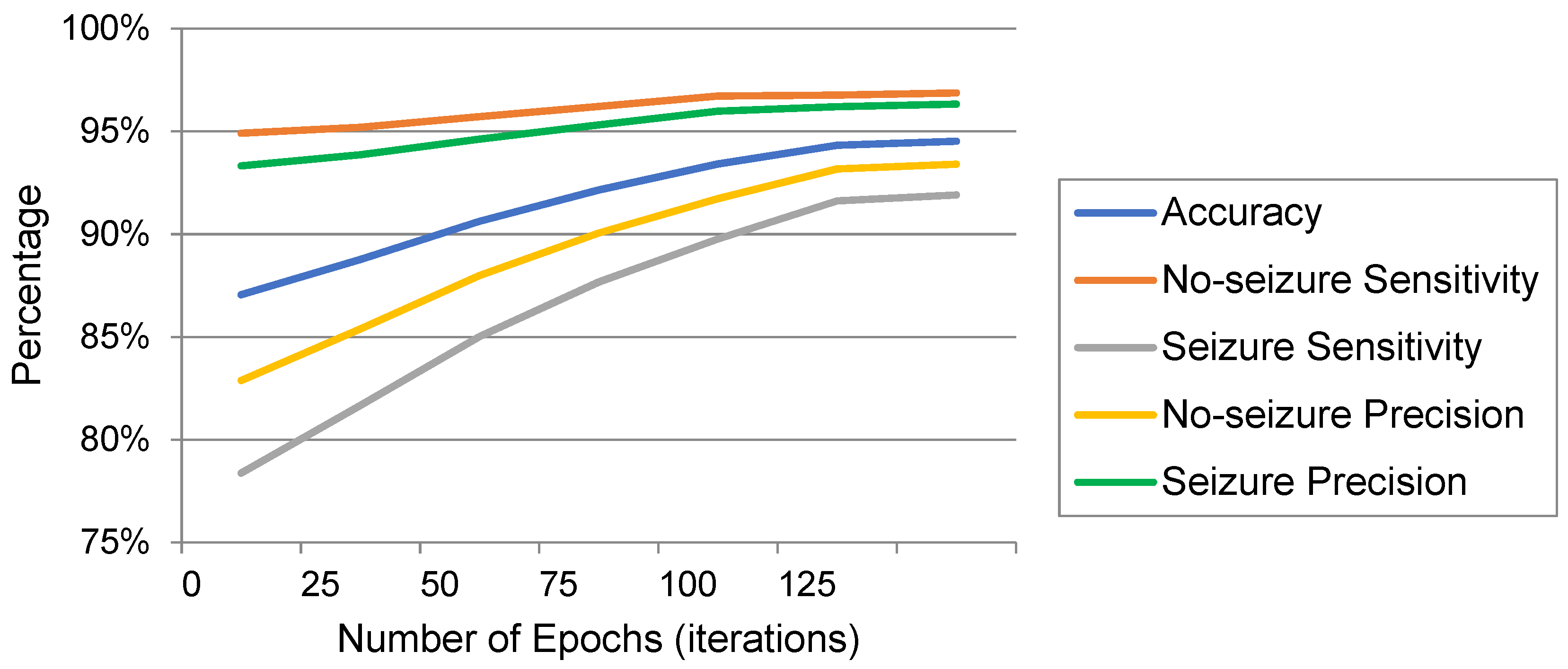
5.2. Evaluating the Seizure Detection Model
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Panayiotopoulos, C. A Clinical Guide to Epileptic Syndromes and Their Treatment; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- World Health Organization. Epilepsy. 2018. Available online: http://www.who.int/en/news-room/fact-sheets/detail/epilepsy (accessed on 20 August 2018).
- Background to Seizures. Epilepsy Research UK. 2018. Available online: https://www.epilepsyresearch.org.uk/about-epilepsy/background-to-seizures/ (accessed on 15 August 2018).
- Bell, G.; Sinha, S.; Tisi, J.; Stephani, C.; Scott, C.; Harkness, W.; McEvoy, A.; Peacock, J.; Walker, M.; Smith, S.; et al. Premature mortality in refractory partial epilepsy: Does surgical treatment make a difference? J. Neurol. Neurosurg. Psychiatry 2010, 81, 716–718. [Google Scholar] [PubMed]
- Ulate-Campos, A.; Coughlin, F.; Gaínza-Lein, M.; Fernández, I.; Pearl, P.; Loddenkemper, T. Automated seizure detection systems and their effectiveness for each type of seizure. Seizure 2016, 40, 88–101. [Google Scholar] [PubMed]
- EEG (Electroencephalogram)—Mayo Clinic. 2022. Available online: https://www.mayoclinic.org/tests-procedures/eeg/about/pac-20393875 (accessed on 3 August 2021).
- Nacy, S.; Kbah, S.; Jafer, H.; Al-Shaalan, I. Controlling a Servo Motor Using EEG Signals from the Primary Motor Cortex. Am. J. Biomed. Eng. 2016, 6, 139–146. [Google Scholar]
- Tatum, W.O. Ellen R. grass lecture: Extraordinary EEG. Neurodiagnostic J. 2014, 54, 3–21. [Google Scholar]
- Birjandtalab, J.; Heydarzadeh, M.; Nourani, M. Automated EEGbased epileptic seizure detection using deep neural networks. In Proceedings of the 2017 IEEE International Conference on Healthcare Informatics (ICHI), Park City, UT, USA, 23–26 August 2017; pp. 552–555. [Google Scholar]
- Buda, M.; Maki, A.; Mazurowski, M.A. A systematic study of the class imbalance problem in convolutional neural networks. Neural Netw. 2018, 106, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Shoeb, A. Application of Machine Learning to Epileptic Seizure Onset Detection and Treatment. Ph.D. Thesis, Massa-Chusetts Institute of Technology, Cambridge, MA, USA, 2009. [Google Scholar]
- Antoniades, A.; Spyrou, L.; Took, C.C.; Sanei, S. Deep learning for epileptic intracranial EEG data. In Proceedings of the 2016 IEEE 26th International Workshop on Machine Learning for Signal Processing (MLSP), Vietri sul Mare, Italy, 13–16 September 2016; pp. 1–6. [Google Scholar]
- Yuan, Y.; Xun, G.; Ma, F.; Suo, Q.; Xue, H.; Jia, K.; Zhang, A. A novel channel-aware attention framework for multi-channel EEG seizure detection via multi-viewdeep learning. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Las Vegas, NV, USA, 4–7 March 2018; pp. 206–209. [Google Scholar]
- Ullah, I.; Hussain, M.; Qazi, E.-U.-H.; Aboalsamh, H. An automated system for epilepsy detection using EEG brain signals based on deep learning approach. Expert Syst. Appl. 2018, 107, 61–71. [Google Scholar] [CrossRef]
- Zabihi, M.; Kiranyaz, S.; Jantti, V.; Lipping, T.; Gabbouj, M. Patient-Specific Seizure Detection Using Nonlinear Dynamics and Nullclines. IEEE J. Biomed. Health Inform. 2019, 24, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Avcu, M.T.; Zhang, Z.; Chan, D.W.S. Seizure detection using least EEG channels by deep convolutional neural network. In Proceedings of the ICASSP 2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 1120–1124. [Google Scholar]
- Hu, X.; Yuan, Q. Epileptic EEG Identification Based on Deep Bi-LSTM Network. In Proceedings of the 2019 IEEE 11th International Conference on Advanced Infocomm Technology (ICAIT), Jinan, China, 18–20 October 2019; pp. 63–66. [Google Scholar] [CrossRef]
- Chandel, G.; Farooq, O.; Khan, Y.; Varshney, Y. Patient Specific Seizure Onset-Offset Latency Detection using Long- term EEG Signals. In Proceedings of the 2019 International Conference on Electrical, Electronics and Computer Engineering (UPCON), Aligarh, India, 8–10 November 2019.
- Kaziha, O.; Bonny, T. A Convolutional Neural Network for Seizure Detection. In Proceedings of the 2020 Advances in Science and Engineering Technology International Conferences (ASET), Dubai, United Arab Emirates, 4 February–9 April 2020. [Google Scholar]
- Huang, C.; Chen, W.; Chen, M.; Yuan, B. A Feature Fusion Framework and Its Application to Automatic Seizure Detection. IEEE Signal Process. Lett. 2021, 28, 753–757. [Google Scholar] [CrossRef]
- Jeong, S.; Jeon, E.; Ko, W.; Suk, H. Fine-grained Temporal Attention Network for EEG-based Seizure Detection. In Proceedings of the 2021 9th International Winter Conference on Brain-Computer Interface (BCI), Gangwon, Korea, 22–24 February 2021.
- Holmes, G. Consequences of Epilepsy through the Ages: When is the Die Cast? Epilepsy Curr. 2012, 12, 4–6. [Google Scholar] [CrossRef]
- Jadeja, N.M. Montages. In How to Read an EEG; Cambridge University Press: Cambridge, MA, USA, 2021; pp. 17–22. [Google Scholar]
- Sharmila, A.; Geethanjali, P. DWT Based Detection of Epileptic Seizure From EEG Signals Using Naive Bayes and k-NN Classifiers. In Proceedings of the 2017 International Conference on Trends in Electronics and Informatics (ICEI), Tirunelveli, India, 11–12 May 2017; Volume 4, pp. 7716–7727. [Google Scholar] [CrossRef]
- Zhang, T.; Chen, W.; Li, M. AR based quadratic feature extraction in the VMD domain for the automated seizure detection of EEG using random forest classifier. Biomed. Signal Process. Control 2017, 31, 550–559. [Google Scholar] [CrossRef]
- Khan, Y.U.; Farooq, O.; Sharma, P. Automatic detection of seizure onset in pediatric EEG. Int. J. Embed. Syst. Appl. 2012, 2, 81–89. [Google Scholar] [CrossRef]
- Akwei-Sekyere, S. Powerline noise elimination in biomedical signals via blind source separation and wavelet analysis. PeerJ 2015, 3, e1086. [Google Scholar] [CrossRef] [PubMed]
- Frost, J. Z-score: Definition, Formula, and Uses. Statistics by Jim. 2022. Available online: https://statisticsbyjim.com/basics/z-score/ (accessed on 5 February 2022).
- Kingma, P.D.; Ba, J.L. Adam: A method for stochastic optimization. arXiv 2017, arXiv:1412.6980v9. [Google Scholar] [CrossRef]
- Albawi, S.; Mohammed, T.A.; Al-Zawi, S. Understanding of a convolutional neural network. In Proceedings of the 2017 International Conference on Engineering and Technology (ICET), Antalya, Turkey, 21–23 August 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Ramachandran, P.; Zoph, B.; Le, Q.V. Searching for activation functions. arXiv 2017, arXiv:1710.05941. [Google Scholar]
- Murray, N.; Perronnin, F. Generalized Max Pooling. In Proceedings of the 2014 IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014. [Google Scholar] [CrossRef] [Green Version]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- Aggarwal, R. Bi-LSTM. Medium. 2019. Available online: https://medium.com/@raghavaggarwal0089/bi-lstm-bc3d68da8bd0 (accessed on 18 February 2022).
- Verma, Y. A Beginner’s Guide to Using Attention Layer in Neural Networks. Analytics India Magazine. 2022. Available online: https://analyticsindiamag.com/a-beginners-guide-to-using-attention-layer-in-neural-networks/ (accessed on 13 July 2022).
- Unzueta, D. Convolutional Layers vs. Fully Connected Layers. Towards Data Science. 2021. Available online: https://towardsdatascience.com/convolutional-layers-vs-fully-connected-layers-364f05ab460b (accessed on 20 February 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency | Bandwidth | Normal Tasks | Abnormal Tasks |
|---|---|---|---|
| 0.1–4 Hz | Delta (δ) | sleep, artifacts, hyperventilation | structural lesion, seizures, encephalopathy |
| 4–8 Hz | Theta (θ) | drowsiness, idling | encephalopathy |
| 8–12 Hz | Alpha (α) | closing the eyes, inhabitation | coma, seizures |
| 12–30 Hz | Beta (β) | effect of medication, drowsiness | drug overdose, seizures |
| 30–70 Hz | Gamma (γ) | voluntary motor movement, learning and memory | seizures |
| Cite | Published Year | Approach | Layers | Dataset | Channels | Accuracy | Window Size |
|---|---|---|---|---|---|---|---|
| [12] | 2016 | CNN | 2 | King’s College London Hospital dataset | 12 channels | 87.51% | 80 ms |
| [9] | 2017 | Deep Neural Networks | 4 | 23 epileptic patients from Boston Children’s Hospital | Ranges from 18 to 23 channels | 95% | 10 s |
| [13] | 2018 | Channel-aware Attention Framework | 23 | CHB-MIT dataset | 23 channels (in few cases 24 or 26) | 96.61% | NA |
| [14] | 2018 | Pyramidal one-dimensional CNN models | 3 | Bonn university dataset | 1 channel | 99% | 10 s |
| [15] | 2019 | Nonlinear dynamics (NLD) with Linear Discriminant Analysis (LDA) and Artificial Neural Network (ANN) | 5 | CHB-MIT dataset | 23 | 95.11% | 1 s |
| [16] | 2019 | Deep CNN | 4 | 29 pediatric patients from KK Women’s and Children’s Hospital, Singapore | 2 channels | 93.3% | 5 s |
| [17] | 2019 | Deep Bi-LSTM Network | 5 | Bonn university dataset | 1 channel | 98.56% | NA |
| [18] | 2019 | Discrete Wavelet Transform (DWT) + linear classifier | NA | CHB-MIT dataset | 23 channels (in few cases 24 or 26) | 98.60% | 1 s |
| [19] | 2020 | CNN | 18 | CHB-MIT dataset | 23 channels (in few cases 24 or 26) | 96.74% | 100 s |
| [20] | 2021 | Gradient-Boosted Decision Trees (GBDT) with Deep Neural Network (DNN) | NA | CHB-MIT dataset | 23 channels (in few cases 24 or 26) | NA | 20 s |
| [21] | 2021 | CNN | 20 | CHB-MIT dataset | 23 channels (in few cases 24 or 26) | 89% | NA |
| Category | Description |
|---|---|
| Open eyes | EEG recording for a relaxed patient in awake state with eyes open |
| Closed eyes | EEG recording of a relaxed or sleeping patient with eyes closed |
| Pre-ictal | EEG recording for a patient in a state prior to epileptic seizure |
| Ictal | EEG recording for a patient during epileptic seizures |
| Post-ictal | EEG recording for a patient in a state posterior to epileptic seizure |
| Inter-ictal | EEG recording for a patient in seizure-free interval between seizures |
| Artifacts | Signals recorded by EEG that might mimic seizures but generated from outside the brain |
| Subject No. | Total Number of Seizures | Total Seizures Duration (Seconds) | Average Seizure Duration (Seconds) |
|---|---|---|---|
| 1 | 7 | 449 | 64.14 |
| 3 | 7 | 409 | 58.43 |
| 5 | 4 | 280 | 70 |
| 7 | 10 | 94 | 9.4 |
| 9 | 6 | 323 | 53.83 |
| EXP No. | DB | Avg. Epoch ACC | Avg. Epoch Sen. for Seizure | Avg. Epoch Sen. for No-Seizure | Avg. Epoch PRC for Seizure | Avg. Epoch PRC for No-Seizure |
|---|---|---|---|---|---|---|
| 1 | CHB-MIT | 79.25 | 64.16 | 93.14 | 89.2 | 75.29 |
| 2 | CHB-MIT | 81.93 | 68.43 | 94.41 | 91.54 | 78.03 |
| 3 | CHB-MIT | 75.38 | 54.95 | 94.02 | 89.26 | 70.53 |
| Avg. | CHB-MIT | 78.85 | 62.51 | 93.86 | 90 | 74.62 |
| 4 | CHB-MIT + KAU | 77.81 | 66.76 | 88.01 | 84.01 | 76.99 |
| 5 | CHB-MIT + KAU | 80.90 | 75.34 | 84.66 | 78.09 | 86.03 |
| 6 | CHB-MIT + KAU | 81.73 | 62.29 | 94.8 | 87.71 | 79.78 |
| Avg. | CHB-MIT + KAU | 80.15 | 68.13 | 89.16 | 83.27 | 80.93 |
| Cite | No. of Channels | No. of Subjects | Sen. | PRC | ACC | Speed of Convergence |
|---|---|---|---|---|---|---|
| [13] | 23 channels (in few cases 24 or 26) | 23 | - | 96.51 | 96.61 | NA |
| [15] | 23 | 25% of the dataset | 91.15 | - | 95.11 | NA |
| [18] | 23 | 14 specific patients | 96.43 | - | 98.60 | NA |
| [19] | 23 channels (in few cases 24 or 26) | 23 | 82.35 | - | 96.74 | Around 60 epochs |
| [21] | 23 channels (in few cases 24 or 26) | 23 | 90.97 | - | - | NA |
| [20] | 23 channels (in few cases 24 or 26) | 23 | 94 | - | 89 | NA |
| The proposed model | 18 channel | 23 | 96.85 | 96.98 | 96.87 | Around 130 epochs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alharthi, M.K.; Moria, K.M.; Alghazzawi, D.M.; Tayeb, H.O. Epileptic Disorder Detection of Seizures Using EEG Signals. Sensors 2022, 22, 6592. https://doi.org/10.3390/s22176592
Alharthi MK, Moria KM, Alghazzawi DM, Tayeb HO. Epileptic Disorder Detection of Seizures Using EEG Signals. Sensors. 2022; 22(17):6592. https://doi.org/10.3390/s22176592
Chicago/Turabian StyleAlharthi, Mariam K., Kawthar M. Moria, Daniyal M. Alghazzawi, and Haythum O. Tayeb. 2022. "Epileptic Disorder Detection of Seizures Using EEG Signals" Sensors 22, no. 17: 6592. https://doi.org/10.3390/s22176592
APA StyleAlharthi, M. K., Moria, K. M., Alghazzawi, D. M., & Tayeb, H. O. (2022). Epileptic Disorder Detection of Seizures Using EEG Signals. Sensors, 22(17), 6592. https://doi.org/10.3390/s22176592