
Blockchain Based Delay and Energy Harvest Aware Healthcare Monitoring System in WBAN Environment


Abstract
:1. Introduction
- Public blockchain: All participants can have rights to read and write, no centralized entity, high credibility and also high throughput and energy consumption.
- Private blockchain: Only the particular organization that owns the blockchain could have rights to access or write. It is a centralized blockchain with less credibility. It consumes less energy with a high throughput.
- Consortium blockchain: It can be owned by a group of organizations to which all the group organization participants could have access to read and write. It is also referred to as a partially centralized blockchain and has less energy consumption with a high throughput.
- Hybrid blockchain: Similar to the public blockchain, a hybrid blockchain could give access to read and write to all the participants. It provides partial centrality with medium credibility.
1.1. Motivation and Objectives
- Higher energy consumption: Frequent sensor replacement is necessary when sensors drain their energy.
- Security and privacy: Due to wireless channels and limited energy resources of sensors, data confidentiality and privacy are a failure.
- Mobility prediction: Communications must be energy-efficient and secure in patient dynamic movements.
- To propose an energy-efficient, secure and delay-aware health monitoring system that allows patients to sense and transmit data in an energy-efficient manner.
- To ensure QoS constraints while collecting and transmitting the data from all layers (intra-WBAN, inter-WBAN and beyond WBAN).
- To safely store the sensed data in a storage server with satisfying the security requirements (data confidentiality, and integrity).
1.2. Research Contributions
- We deployed dual sinks such as emergency sink and periodic sink to collect the data without congestion. All critical packets are forwarded to the health center without any delay.
- All patients who need to monitor healthcare are registered to the key management server (KMS) using the extended PRESENT algorithm. Clustering is generated using the best objective function (BOF), which is computed by node residual energy, transmission power, bandwidth, and signal to noise ratio (SNR) via spotted hyena optimizer (SHO).
- Faulty data packets are removed in the sink with the use of analyzing the records and it results in low bandwidth and energy consumption. If the CH is drained of its potential to transmit the data, then the next node is selected among the patient body sensors.
- The idle channel is used for emergency packet transmission and selects the optimum channel for the remaining two medical packet types by considering RSS, SNR, channel capacity and radio power. Hence, interference is eliminated in this step.
- We transfer each normal data packet via multihop transmission, which considers packet size, data traffic type, TTL, required delay and data rate. A multi-hop data routing using best forwarders selection by considering node residual energy, RSS, path duration and distance to the CH.
- We sense and classify the environment and healthcare data for each patient using the deep reinforcement learning algorithm. We proposed two stream-DNN in DRL, which outperforms the conventional Markov model.
- We propose a PRESENT algorithm for encryption of medical data and critical data directly transmitted to the CH and then forwarded to the PBA. Finally, data packets are stored in the blockchain and cloud servers based on packet sensing type.
1.3. Paper Layout
2. Review of Related Literature
2.1. QoS Achievement in WBAN/Iot
- It is complex to design a large scale WBAN environment since medical packets are gathered at each gateway in a random way, which leads to large end-to-end delay.
- Some of the medical packets are necessary to meet the QoS requirements, especially delay, which must be met by the predefined period of time.
2.2. Security in WBAN/Iot
2.3. Blockchain in WBAN/Iot
3. Problem Statement
- The clustering process is not effective since it does not ensure that the CF computation always produces the optimum solution and the computation of CF tends to be time consuming when a large number of sensors are used. This paper minimizes the redundant data, but it does not eliminate anomaly (faulty) data. Thus, it results in large bandwidth and energy consumption for CHs.
- When two sensors communicate with the same channel concurrently, they interfere with each other. Multihop transmission via nonoptimal nodes increases energy consumption and reduces the delivery rate.
- Each medical packet is transferred to the BS based on delay constraints. For example, the glucose monitoring delay requirement is <20 ms. When it is transmitted frequently, then the other delay-constrained emergency packets are dropped. If a medical packet has waited more than the delay time, then the packet is dropped from the scheduler.
- The Markov chain does not perform well when the actions are independent and it does not learn the environment to find the current state. Especially, it is needed for WBAN.
- The participation of multiple sensor nodes (256 heterogeneous sensors) causes congestion in data transmission and thus fails to transmit critical data or is dropped.
4. System Model
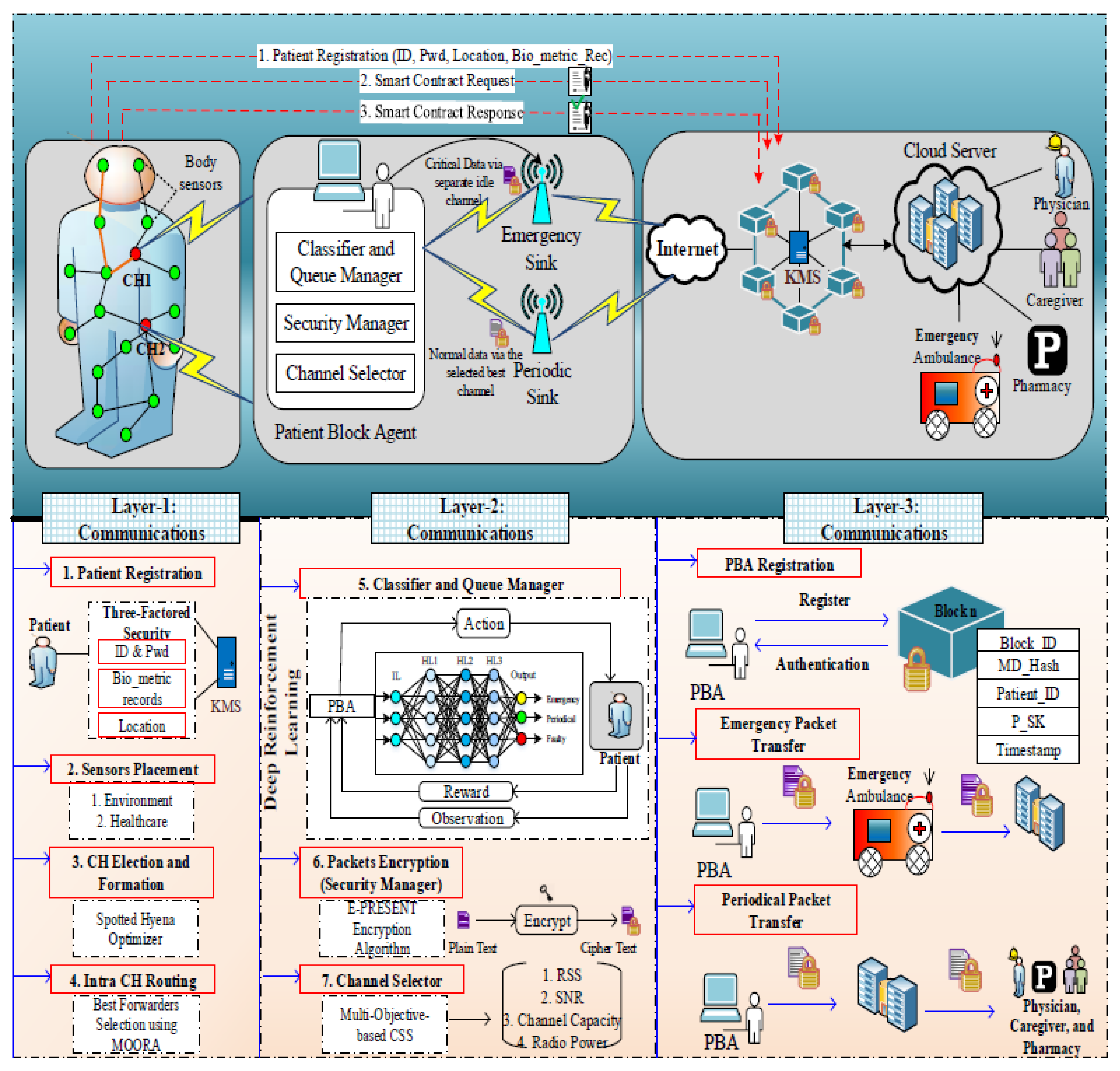
4.1. System Model
- Body sensors: The body sensors are deployed in patients’ bodies to monitor the patient health conditions which monitor such as heartbeat rate, BP rate, etc.
- Environmental sensors: The environmental sensors are located in the environment to monitor the environmental changes based on the patient’s health condition. These sensors monitor the air quality, humidity, etc., in the surroundings of patients’ environment.
- Patient block agent (PBA): The patient block agent is responsible for the transmission of data and also provides authenticity to the users in which three modules are involved namely classifier and queue manager, security manager, and channel selector for classifying and securing the data.
- Emergency sink and periodic sink: These sinks are responsible for storing the data on the internet and cloud server. The emergency sink is used to share the critical data from the PBA while the periodic sink is used to share the normal data from the PBA which helps to transmit the health information with low delay and congestion.
- Blockchain(key management server—KMS): Blockchain is used for the security and privacy of the WBAN IoT networks. The KMS in the blockchain is responsible for managing the key from the users during registration and authentication to verify the legitimacy of the users.
4.2. Key Distribution
4.3. Cluster Based Routing
- Residual Energy Level: This parameter denotes the remaining amount of energy of the node. It is computed using the difference between the initial energy level and the total energy consumed after one round. A node with a higher residual energy level becomes CH and hence the CH is responsible for data collection and aggregation.
- Distance: This parameter is well-known in that it means the distance between one body sensor and the nearby sensor. A node with less distance is applicable for CH election. It is calculated as follows:
- Path Duration: This parameter is the amount of time taken for packet transmission. It is measured using a number of relay nodes to one node.
4.4. Contention Window Size Adjustment
4.5. Patient Block Agent
4.5.1. Classifier and Queue Manager
- Input Layer: This is the first layer that is processed with the input neurons, and BAN packets and environment events are forwarded to the input layer of DNN (1) and DNN (2), respectively. Thus, the sensed packets from the body and environment sensors are represented as follows:
- Hidden Layers: Different numbers of computing weight values for each input parameter of the sensed packets. Based on the input requirements and the expected result, the number of hidden layers is defined. In the previously mentioned parameters, the fitness value is computed in hidden layers. Finally, the fitness function is expressed as follows,where S refers to the sensor nodes of n numbers (i.e., , is the packet size weight value, is the different traffic type weight value, is the TTL weight value, is the weight value for QoS constraints and represents the delay, data rate and bandwidth.
- Output Layer: This layer predicts the classes according to the aforementioned parameters. It chooses the optimal class from the fitness values computed for each packet. Mathematically, it is formulated as follows,where is the activation function.
| Algorithm 1 TS-DNN. |
|
4.5.2. Security Manager
| Algorithm 2 OT-PRESENT algorithm. |
|
4.5.3. Channel Selector
5. Experimental Results and Discussion
5.1. Simulation Environment
- Communication Type: Off-body, on-body, body to body, off to off;
- Scenario Condition: Same room.
5.2. Comparative Analysis
5.2.1. Network Throughput
5.2.2. End-To-End Delay
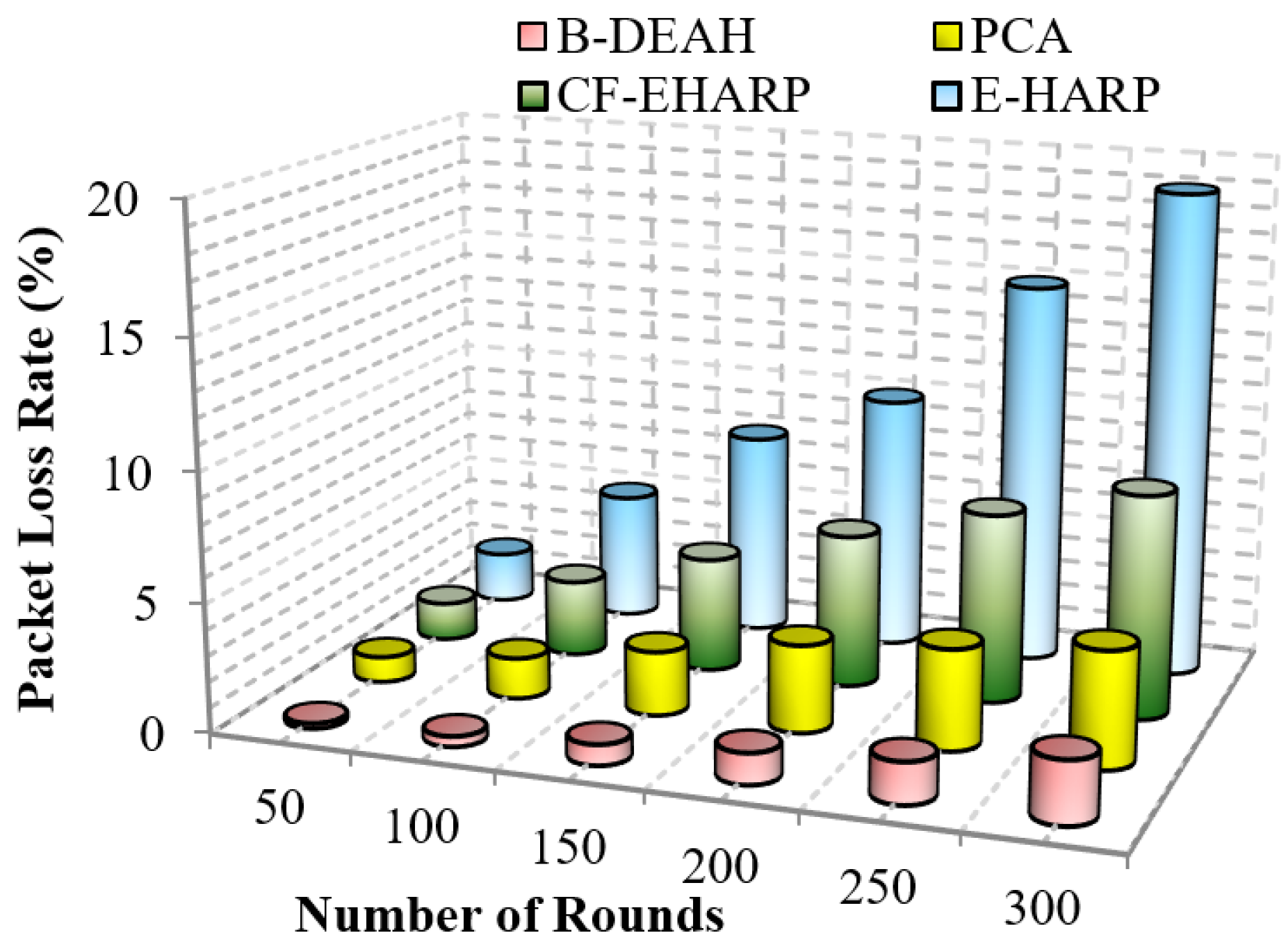
5.2.3. Packet Loss Rate
5.2.4. Authentication Time
5.2.5. Residual Energy
5.2.6. Success Rate
5.3. Security & Efficiency Analysis
- BAN Impersonation Attack: In this attack, unauthorized patients attempt to submit and access data from the cloud. However, the sensors from the body and environment are compromised by the attackers. The authentication to the blockchain cannot be compromised by an attacker and cannot be passed until the correct credentials are submitted.
- Flooding Attack: In this attack, more illegitimate requests are forwarded by attackers. Hence, sink nodes and any other communication devices cannot tolerate a high number of requests. For each BAN, the PBA’s role is to monitor and audit the abnormal packets and notify this information to the blockchain and remote server.
- Path-based DoS Attack: DoS is a denial of service attack in which attackers’ behavior is to exhaust the resources for sink nodes and other devices and creates a busy route. This makes the huge delay in processing legitimate packets, and hence, the emergency packet delay is higher and leads to more packet losses.
5.3.1. Fault Data Elimination Check
5.3.2. Reliability
6. Conclusions and Future Work
- Investigation of mobility since mobility is a crucial parameter of BAN. The human body parts are in motion constantly. Here, we planned to use handover mechanisms for mobility management.
- Duty cycling MAC scheduling is studied for managing the energy level of each body sensor.
- Furthermore, other emerging medical diagnosis applications are concentrated for user physiological parameter analysis, such as diabetes, asthma, Parkinson’s disease, or COVID-19.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abiodun, A.S.; Anisi, M.H.; Khan, M.K. Cloud-based wireless body area networks: Managing data for better health care. IEEE Consum. Electron. Mag. 2019, 8, 55–59. [Google Scholar] [CrossRef]
- Chen, H.; Wang, J.; Dong, X.; Zhao, C. Security design of ECG telemonitoring systems. In Proceedings of the 2020 International Conference on Computer Engineering and Application (ICCEA), Guangzhou, China, 18–20 March 2020; pp. 707–711. [Google Scholar]
- Ivanciu, I.A.; Ivanciu, L.; Zinca, D.; Dobrota, V. Securing Health-Related Data Transmission Using ECG and Named Data Networks. In Proceedings of the 2019 IEEE International Symposium on Local and Metropolitan Area Networks (LANMAN), Paris, France, 1–3 July 2019; pp. 1–6. [Google Scholar]
- Vishwakarma, R.; Mohapatra, R.K. A secure three-party authentication protocol for wireless body area networks. In Proceedings of the 2017 Third International Conference on Sensing, Signal Processing and Security (ICSSS), Chennai, India, 4–5 May 2017; pp. 99–103. [Google Scholar]
- Roy, A.; Roy, C.; Misra, S.; Rahulamathavan, Y.; Rajarajan, M. Care: Criticality-aware data transmission in cps-based healthcare systems. In Proceedings of the 2018 IEEE International Conference on Communications Workshops (ICC Workshops), Kansas City, MO, USA, 20–24 May 2018; pp. 1–6. [Google Scholar]
- Jabeen, T.; Ashraf, H.; Khatoon, A.; Band, S.S.; Mosavi, A. A Lightweight Genetic Based Algorithm for Data Security in Wireless Body Area Networks. IEEE Access 2020, 8, 183460–183469. [Google Scholar] [CrossRef]
- Pillai, R.R.; Lohani, R.B. Abnormality Detection and Energy Conservation in Wireless Body Area Networks using Hidden Markov Models: A Review. In Proceedings of the 2020 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 28–30 July 2020. [Google Scholar]
- Fotouhi, M.; Bayat, M.; Das, A.K.; Far, H.A.N.; Pournaghi, S.M.; Doostari, M.A. A lightweight and secure two-factor authentication scheme for wireless body area networks in health-care IoT. Comput. Netw. 2020, 177, 107333. [Google Scholar] [CrossRef]
- Almuhaideb, A.M.; Alqudaihi, K.S. A lightweight and secure anonymity preserving protocol for WBAN. IEEE Access 2020, 8, 178183–178194. [Google Scholar] [CrossRef]
- Soni, M.; Singh, D.K. LAKA: Lightweight authentication and key agreement protocol for internet of things based wireless body area network. Wirel. Personal Commun. 2021, 1–18. [Google Scholar] [CrossRef]
- Wang, G.; Lu, R.; Guan, Y.L. Achieve privacy-preserving priority classification on patient health data in remote eHealthcare system. IEEE Access 2019, 7, 33565–33576. [Google Scholar] [CrossRef]
- Rani, S.S.; Alzubi, J.A.; Lakshmanaprabu, S.; Gupta, D.; Manikandan, R. Optimal users based secure data transmission on the internet of healthcare things (IoHT) with lightweight block ciphers. Multimed. Tools Appl. 2019, 79, 1–20. [Google Scholar] [CrossRef]
- Chen, W.; Chen, Z.; Cui, F. Collaborative and secure transmission of medical data applied to mobile healthcare. Biomed. Eng. Online 2019, 18, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, H.; Bakar, N.A.A.; Hassan, N.H.; Yaacob, S. IoT security risk management model for secured practice in healthcare environment. Procedia Comput. Sci. 2019, 161, 1241–1248. [Google Scholar] [CrossRef]
- Hai, T.; Bhuiyan, M.Z.A.; Wang, J.; Wang, T.; Hsu, D.F.; Li, Y.; Salih, S.Q.; Wu, J.; Liu, P. DependData: Data collection dependability through three-layer decision-making in BSNs for healthcare monitoring. Inf. Fusion 2020, 62, 32–46. [Google Scholar] [CrossRef]
- Hathaliya, J.J.; Tanwar, S.; Evans, R. Securing electronic healthcare records: A mobile-based biometric authentication approach. J. Inf. Secur. Appl. 2020, 53, 102528. [Google Scholar] [CrossRef]
- Saba, T.; Haseeb, K.; Ahmed, I.; Rehman, A. Secure and energy-efficient framework using Internet of Medical Things for e-healthcare. J. Infect. Public Health 2020, 13, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Luo, N.; Zhou, P. GuardHealth: Blockchain empowered secure data management and Graph Convolutional Network enabled anomaly detection in smart healthcare. J. Parallel Distrib. Comput. 2020, 142, 1–12. [Google Scholar] [CrossRef]
- Esmaeili, S.; Tabbakh, S.R.K.; Shakeri, H. A priority-aware lightweight secure sensing model for body area networks with clinical healthcare applications in Internet of Things. Pervasive Mob. Comput. 2020, 69, 101265. [Google Scholar] [CrossRef] [PubMed]
- Amoon, M.; Altameem, T.; Altameem, A. Internet of things sensor assisted security and quality analysis for health care data sets using artificial intelligent based heuristic health management system. Measurement 2020, 161, 107861. [Google Scholar] [CrossRef]
- Pathak, N.; Mukherjee, A.; Misra, S. Reconfigure and Reuse: Interoperable Wearables for Healthcare IoT. In Proceedings of the IEEE INFOCOM 2020-IEEE Conference on Computer Communications, Toronto, ON, Canada, 6–9 July 2020; pp. 20–29. [Google Scholar]
- Farhan, B.I.; Farhan, R.I.; Hussein, G.A. Security and Privacy Aware Communication in Body Area Networks Using Blockchain Technology. Management 2021. [Google Scholar] [CrossRef]
- Salem, O.; Alsubhi, K.; Mehaoua, A.; Boutaba, R. Markov models for anomaly detection in wireless body area networks for secure health monitoring. IEEE J. Sel. Areas Commun. 2020, 39, 526–540. [Google Scholar] [CrossRef]
- Al Omar, A.; Bhuiyan, M.Z.A.; Basu, A.; Kiyomoto, S.; Rahman, M.S. Privacy-friendly platform for healthcare data in cloud based on blockchain environment. Future Gener. Comput. Syst. 2019, 95, 511–521. [Google Scholar] [CrossRef]
- Rathee, G.; Sharma, A.; Saini, H.; Kumar, R.; Iqbal, R. A hybrid framework for multimedia data processing in IoT-healthcare using blockchain technology. Multimed. Tools Appl. 2019, 79, 1–23. [Google Scholar] [CrossRef]
- Bharathi, R.; Abirami, T.; Dhanasekaran, S.; Gupta, D.; Khanna, A.; Elhoseny, M.; Shankar, K. Energy efficient clustering with disease diagnosis model for IoT based sustainable healthcare systems. Sustain. Comput. Inform. Syst. 2020, 28, 100453. [Google Scholar] [CrossRef]
- Padmaja, K.; Seshadri, R. A real-time secure medical device authentication for personal E-Healthcare services on cloud computing. Int. J. Syst. Assur. Eng. Manag. 2021, 1–11. [Google Scholar] [CrossRef]
- Ullah, Z.; Ahmed, I.; Razzaq, K.; Naseer, M.K.; Ahmed, N. DSCB: Dual sink approach using clustering in body area network. Peer-to-Peer Netw. Appl. 2019, 12, 357–370. [Google Scholar] [CrossRef]
- Selem, E.; Fatehy, M.; Abd El-Kader, S.M.; Nassar, H. THE (temperature heterogeneity energy) aware routing protocol for IoT health application. IEEE Access 2019, 7, 108957–108968. [Google Scholar] [CrossRef]
- Qu, Y.; Zheng, G.; Wu, H.; Ji, B.; Ma, H. An energy-efficient routing protocol for reliable data transmission in wireless body area networks. Sensors 2019, 19, 4238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdu, A.I.; Bayat, O.; Ucan, O.N. Designing insistence-aware medium access control protocol and energy conscious routing in quality-of-service-guaranteed wireless body area network. Int. J. Distrib. Sens. Netw. 2019, 15, 1550147718815843. [Google Scholar] [CrossRef] [Green Version]
- Yi, C.; Cai, J. Transmission management of delay-sensitive medical packets in beyond wireless body area networks: A queueing game approach. IEEE Trans. Mob. Comput. 2018, 17, 2209–2222. [Google Scholar] [CrossRef]
- Yi, C.; Cai, J. Delay-Dependent Priority-Aware Transmission Scheduling for E-Health Networks: A Mechanism Design Approach. IEEE Trans. Veh. Technol. 2019, 68, 6997–7010. [Google Scholar] [CrossRef]
- Qureshi, K.N.; Din, S.; Jeon, G.; Piccialli, F. Link quality and energy utilization based preferable next hop selection routing for wireless body area networks. Comput. Commun. 2020, 149, 382–392. [Google Scholar] [CrossRef]
- Aadil, F.; Mehmood, B.; Ul Hasan, N.; Lim, S.; Ejaz, S.; Zaman, N. Remote Health Monitoring Using IoT-Based Smart Wireless Body Area Network. CMC-Comput. Mater. Contin. 2021, 68, 2499–2513. [Google Scholar] [CrossRef]
- El Zouka, H.A.; Hosni, M.M. Secure IoT communications for smart healthcare monitoring system. Internet Things 2019, 13, 100036. [Google Scholar] [CrossRef]
- Vijayakumar, P.; Obaidat, M.S.; Azees, M.; Islam, S.H.; Kumar, N. Efficient and secure anonymous authentication with location privacy for IoT-based WBANs. IEEE Trans. Ind. Inform. 2019, 16, 2603–2611. [Google Scholar] [CrossRef]
- Tan, H.; Chung, I. Secure authentication and group key distribution scheme for WBANs based on smartphone ECG sensor. IEEE Access 2019, 7, 151459–151474. [Google Scholar] [CrossRef]
- Arfaoui, A.; Kribeche, A.; Senouci, S.M.; Hamdi, M. Game-based adaptive anomaly detection in wireless body area networks. Comput. Netw. 2019, 163, 106870. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Kadiyala, R.; Dhiman, G.; Ashok, G.; Kautish, S.; Yadav, K.; Maruthi Nagendra Prasad, J. A Personalized Eccentric Cyber-Physical System Architecture for Smart Healthcare. Secur. Commun. Netw. 2021, 2021, 1747077. [Google Scholar] [CrossRef]
- Iqbal, J.; Umar, A.I.; Amin, N.; Waheed, A. Efficient and secure attribute-based heterogeneous online/offline signcryption for body sensor networks based on blockchain. Int. J. Distrib. Sens. Netw. 2019, 15, 1550147719875654. [Google Scholar] [CrossRef]
- Ren, Y.; Leng, Y.; Zhu, F.; Wang, J.; Kim, H.J. Data storage mechanism based on blockchain with privacy protection in wireless body area network. Sensors 2019, 19, 2395. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Han, K.; Alexandridis, A.; Chen, Z.; Zilic, Z.; Pang, Y.; Jeon, G.; Piccialli, F. A blockchain-based eHealthcare system interoperating with WBANs. Future Gener. Comput. Syst. 2020, 110, 675–685. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, J.; Xu, C.; Li, H.; Wang, H.; Zhang, Y. CIPPPA: Conditional identity privacy-preserving public auditing for cloud-based WBANs against malicious auditors. IEEE Trans. Cloud Comput. 2019, 9, 1362–1375. [Google Scholar] [CrossRef]
- Ullah, Z.; Ahmed, I.; Khan, F.A.; Asif, M.; Nawaz, M.; Ali, T.; Khalid, M.; Niaz, F. Energy-efficient Harvested-Aware clustering and cooperative Routing Protocol for WBAN (E-HARP). IEEE Access 2019, 7, 100036–100050. [Google Scholar] [CrossRef]
- Ullah, Z.; Ahmed, I.; Ali, T.; Ahmad, N.; Niaz, F.; Cao, Y. Robust and efficient energy harvested-aware routing protocol with clustering approach in body area networks. IEEE Access 2019, 7, 33906–33921. [Google Scholar] [CrossRef]
- Uddin, M.A.; Stranieri, A.; Gondal, I.; Balasubramanian, V. Continuous patient monitoring with a patient centric agent: A block architecture. IEEE Access 2018, 6, 32700–32726. [Google Scholar] [CrossRef]
- Yi, C.; Cai, J. A truthful mechanism for scheduling delay-constrained wireless transmissions in IoT-based healthcare networks. IEEE Trans. Wirel. Commun. 2018, 18, 912–925. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, R.; Zhao, M. A robust authentication scheme with dynamic password for wireless body area networks. Comput. Netw. 2019, 161, 220–234. [Google Scholar] [CrossRef]
- Dhiman, G.; Kumar, V. Spotted hyena optimizer: A novel bio-inspired based metaheuristic technique for engineering applications. Adv. Eng. Softw. 2017, 114, 48–70. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area Focused | Research Gap |
|---|---|
| QoS Achievement [28,29,30,31,32,33,34] |
|
| Security Provisioning [36,37,38,39] |
|
| Blockchain [41,42,43,44] |
|
| Data Collection Factors | IoT Devices | Parameters | Sensing Event Type |
|---|---|---|---|
| Body sensors related data | Heart sensors, Q-sensor, EEG devices, ECG monitor, smart wearable’s, Gastro sensors. | Heart Rate, Blood Pressure, Oxygen Saturation, Temperature, Blood Sugar, Respiration Rate, GI tract, ECG, EEG | High Heart Rate, High Blood Glucose Level, High Blood Glucose Level, Stress, Anxiety, and Restlessness |
| Environment related data | Temperature sensors, Humidity sensors, Chemical detectors, Noise sensors | Temperature, Air Quality, Noise Level, Toxic Waste | High room temperature, High noise level, High light intensity |
| PHP (Octal Symbol) | Data Traffic Type | ||
|---|---|---|---|
| 4 | Emergency (VHP) | ||
| 3 | Periodic (HP) | ||
| 2 | Video (NP) | ||
| 1 | Voice (NP) | ||
| 0 | Others (NP) |
| Parameters | Specifications |
|---|---|
| Simulation Parameters | |
| Simulation Environment | 1000 × 1000 m |
| Number of WBANs | 1–5 |
| Number of Body Sensors (Each BAN) | 12 |
| MAC type | IEEE 802.15.6 MAC |
| Sensing Interval | 0.1 s |
| Multiple access technique | CSMA/CA |
| Packet size | 512 bits |
| Bandwidth | 20 MHz |
| Transmission rate | 20 kpbs |
| Modulation (Data Rate) | DQPSK (1000 Kbps) |
| Energy consumption | 0.5 mW |
| Simulation time | 50 s |
| Number of Sink Nodes | 2(1-Emergency, 2-Periodical) |
| Transmission Rate | 5 Packets/s |
| Number of PBA (each WBAN) | 5 |
| MAC Header Length | 32 |
| Number of Frame Slots | 20 |
| Slot Duration | 1 s |
| Buffer Capacity | 32 |
| Block Size | 2 KB |
| Block Chain Type | Linear/Non-Linear |
| Key Size | 80 bits |
| Passwords | Alphabets/integer |
| System Setup | |
| Operating System | Windows 7 (32-bit) |
| Processor | Dual core |
| RAM | 4 GB and above |
| Body Sensors | Emergency (Data Range Units) | Periodical (Data Range Units) |
|---|---|---|
| ECG | ∼60–100 bpm | > bpm |
| Heart Rate | 60–100 bpm | >100 bpm |
| Blood Pressure | 120/80 mm/Hg | ≥140 mm/Hg |
| Temperature | >100 °F | 97.8–99 °F |
| Oxygen Level | <60 mm/Hg | 80–100 mm/Hg |
| Respiratory | <6 bps | 30–40 bps |
| EEG | <7 Hz | >8 Hz |
| Number of BAN | Fault Data Elimination Check (%) | |
|---|---|---|
| B-DEAH | E-HARP | |
| 1 | 97.6 | 80 |
| 2 | 98.6 | 81.5 |
| 3 | 99.3 | 82.5 |
| 4 | 99.6 | 83.6 |
| 5 | 99.8 | 85 |
| Performance Metrics | CF-EHARP | PCA | E-Harp | B-DEAH | ||
|---|---|---|---|---|---|---|
| Throughput (Kbps) | Emergency Packets | 20.8 ± 0.4 | 22.5 ± 0.3 | 23.8 ± 0.5 | 42.5 ± 0.1 | |
| Periodic Packets | 20.08 ± 0.4 | 22 ± 0.2 | 23.11 ± 0.5 | 41.75 ± 0.1 | ||
| End-to-end delay (s) | Emergency Packets | 0.042 ± 0.3 | 0.039 ± 0.2 | 0.031 ± 0.4 | 0.028 ± 0.1 | |
| Periodic Packets | 0.06 ± 0.3 | 0.052 ± 0.2 | 0.041 ± 0.5 | 0.036 ± 0.1 | ||
| Packet loss rate (%) | Number of rounds | 5.18 ± 0.4 | 2.81 ± 0.2 | 9.83 ± 0.5 | 1.1 ± 0.1 | |
| Residual energy (J) | Simulation Rounds | Emergency Packets | 0.03 ± 0.3 | 0.026 ± 0.2 | 0.03 ± 0.4 | 0.044 ± 0.1 |
| Periodic Packets | 7.55 ± 0.4 | 5.6 ± 0.3 | 5.68 ± 0.5 | 0.039 ± 0.1 | ||
| Simulation time | Emergency Packets | 7.51 ± 0.3 | 5.53 ± 0.2 | 5.6 ± 0.4 | 8.53 ± 0.1 | |
| Periodic Packets | 57.3 ± 0.4 | 70.83 ± 0.3 | 53.33 ± 0.5 | 8.35 ± 0.1 | ||
| Success rate (%) | Emergency Packets | 57.33 ± 0.3 | 70.83 ± 0.2 | 53.33 ± 0.4 | 87.5 ± 0.1 | |
| Periodic Packets | 57.33 ± 0.4 | 70.83 ± 0.2 | 53.33 ± 0.5 | 87.83 ± 0.1 | ||
| Reliability (%) | Packets per second | 57.83 ± 0.4 | 70.83 ± 0.3 | 53.5 ± 0.2 | 87.83 ± 0.1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anbarasan, H.S.; Natarajan, J. Blockchain Based Delay and Energy Harvest Aware Healthcare Monitoring System in WBAN Environment. Sensors 2022, 22, 5763. https://doi.org/10.3390/s22155763
Anbarasan HS, Natarajan J. Blockchain Based Delay and Energy Harvest Aware Healthcare Monitoring System in WBAN Environment. Sensors. 2022; 22(15):5763. https://doi.org/10.3390/s22155763
Chicago/Turabian StyleAnbarasan, Helen Sharmila, and Jaisankar Natarajan. 2022. "Blockchain Based Delay and Energy Harvest Aware Healthcare Monitoring System in WBAN Environment" Sensors 22, no. 15: 5763. https://doi.org/10.3390/s22155763
APA StyleAnbarasan, H. S., & Natarajan, J. (2022). Blockchain Based Delay and Energy Harvest Aware Healthcare Monitoring System in WBAN Environment. Sensors, 22(15), 5763. https://doi.org/10.3390/s22155763