
Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2

 , ,
, , 


Abstract
:1. Introduction
2. Materials and Methods
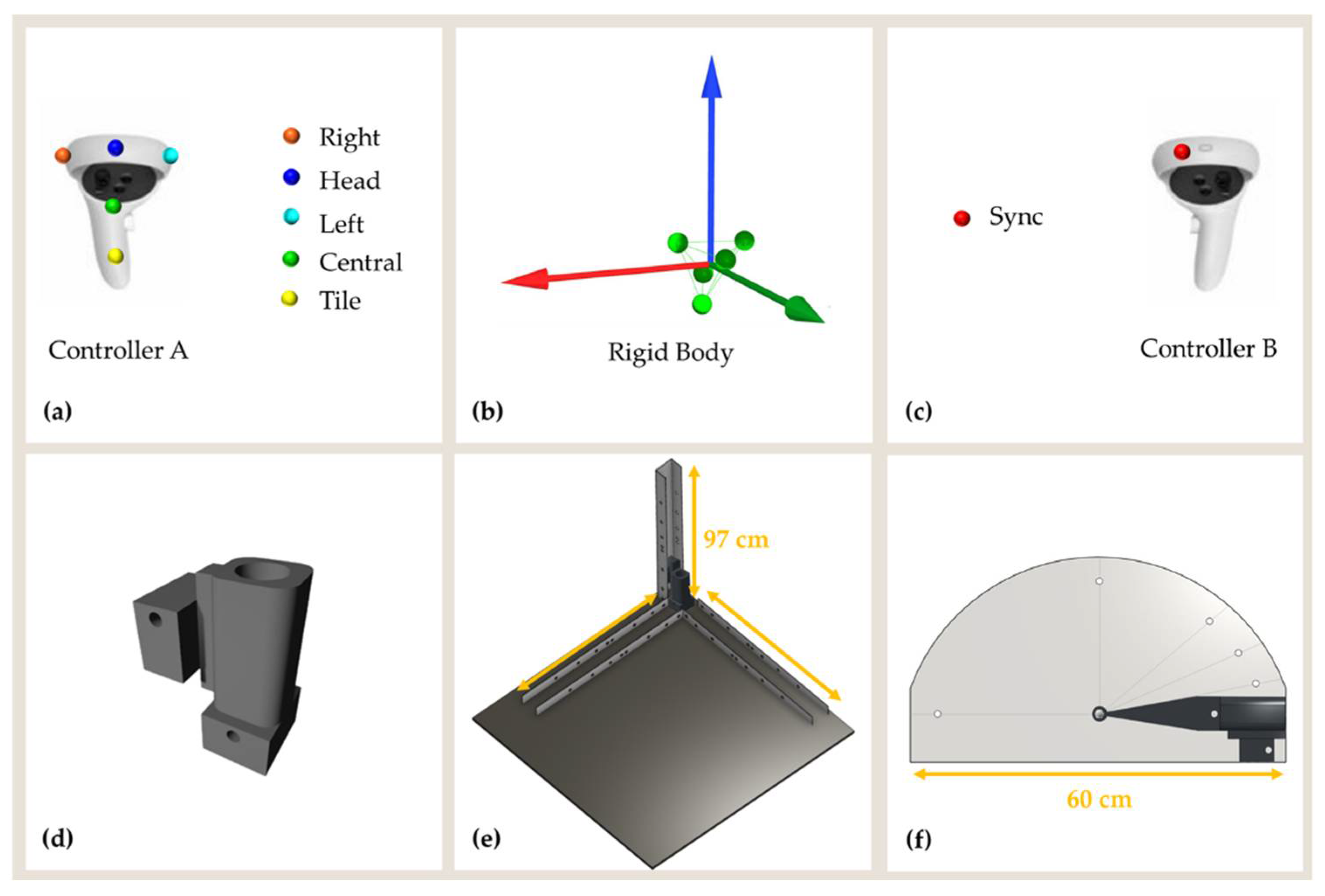
2.1. Experimental Setup
2.2. Experimental Procedure
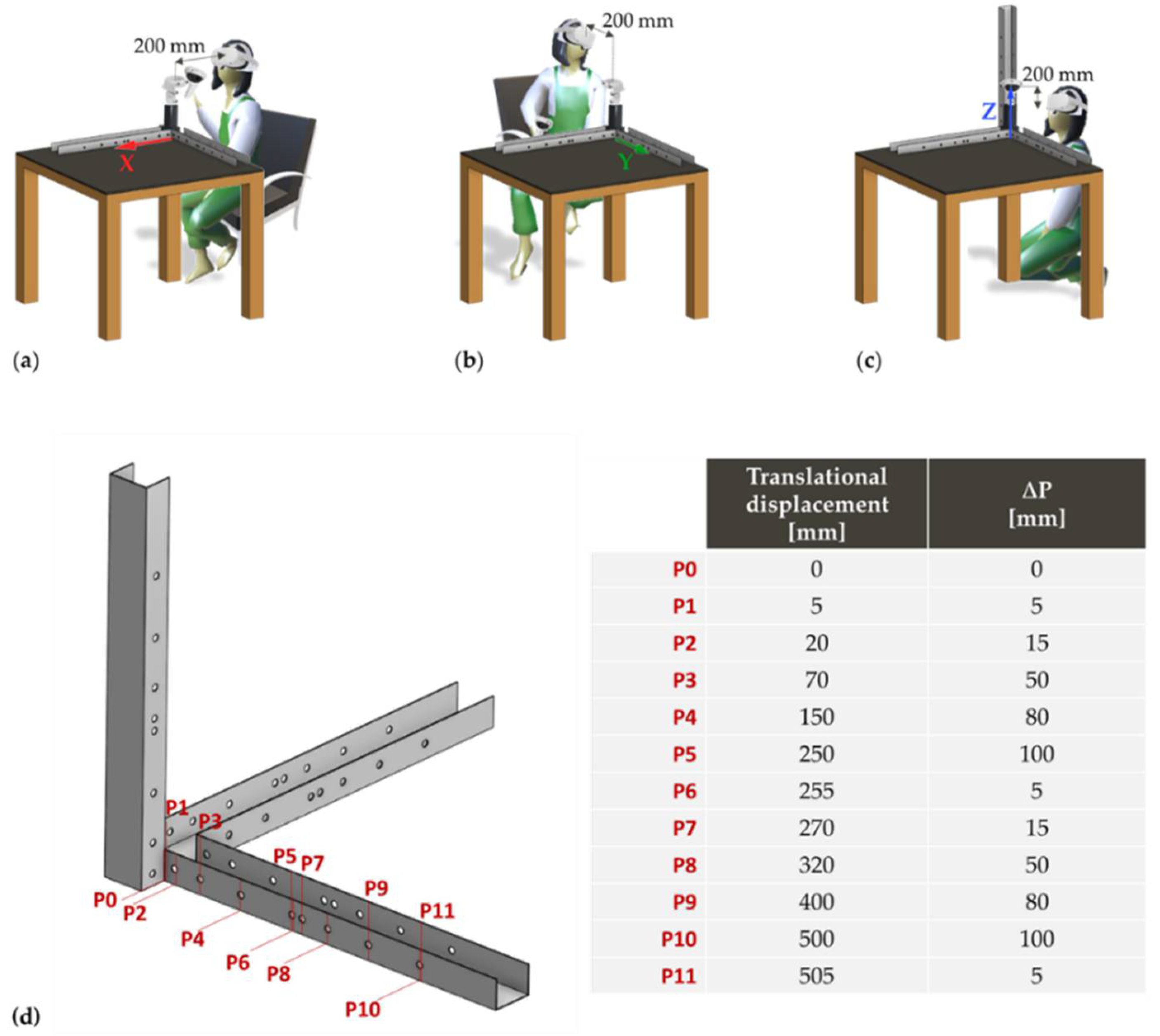
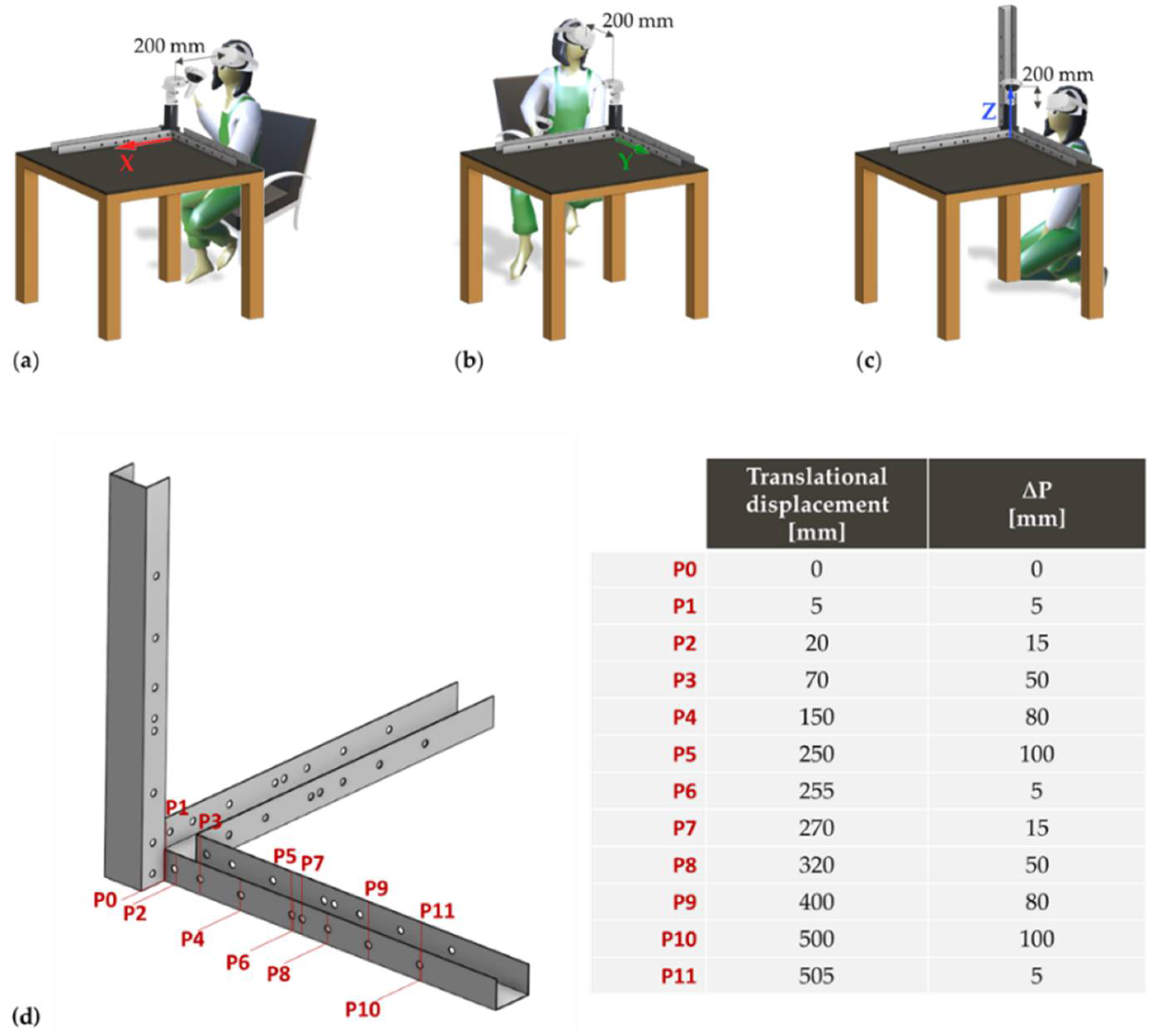
2.2.1. Translational Movements
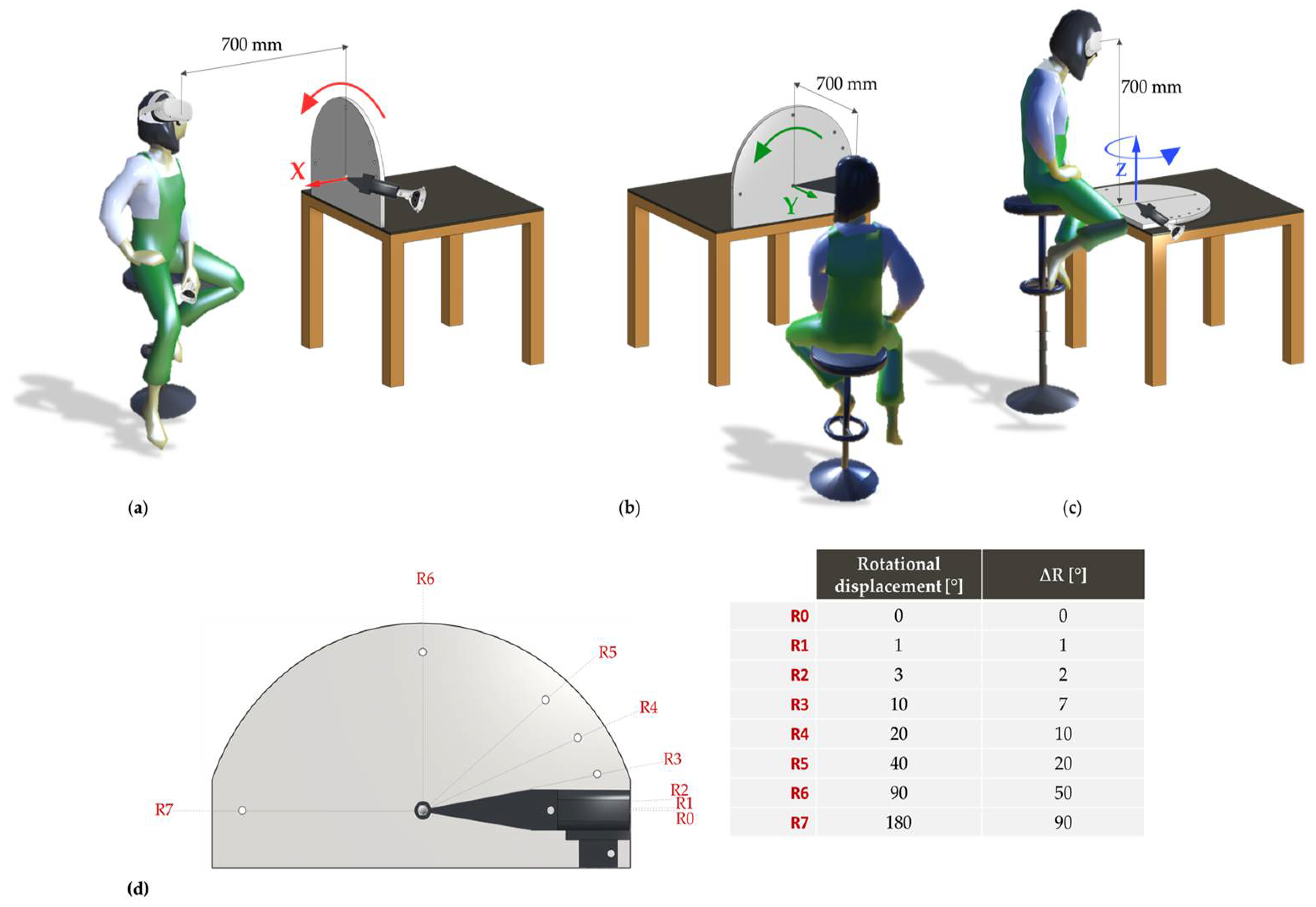
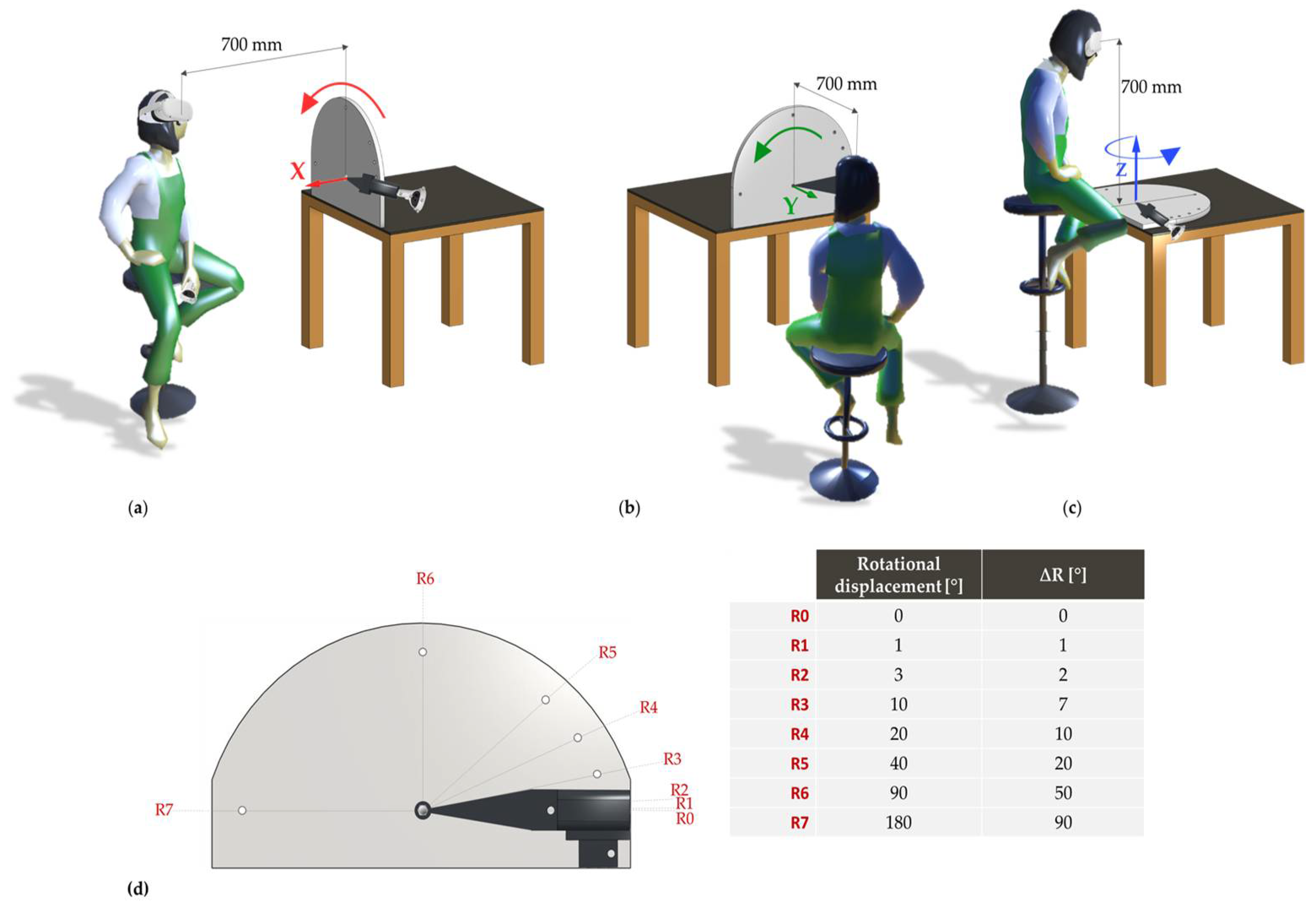
2.2.2. Rotational Movements
2.3. Data Analysis
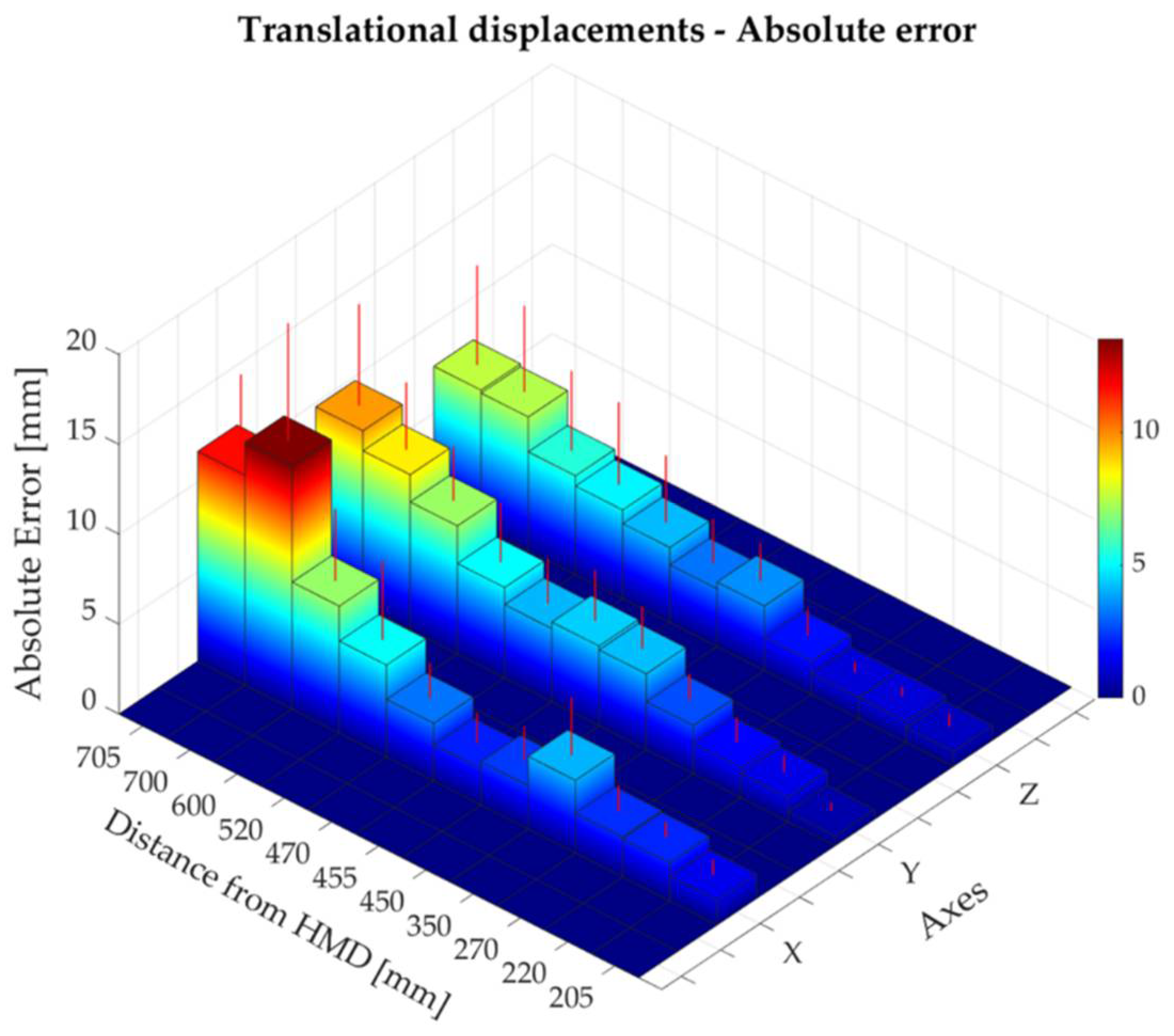
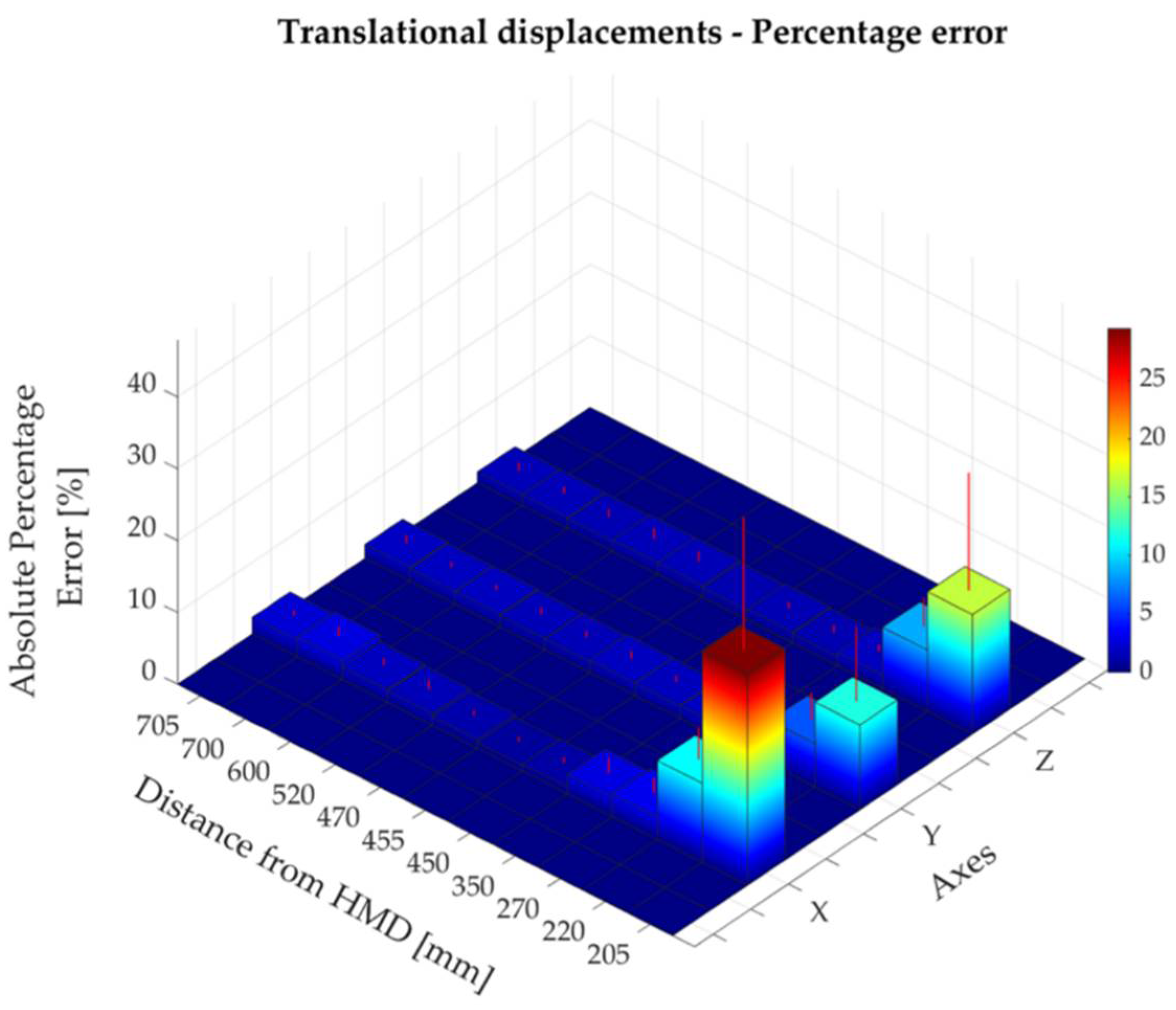
2.3.1. Translational Accuracy
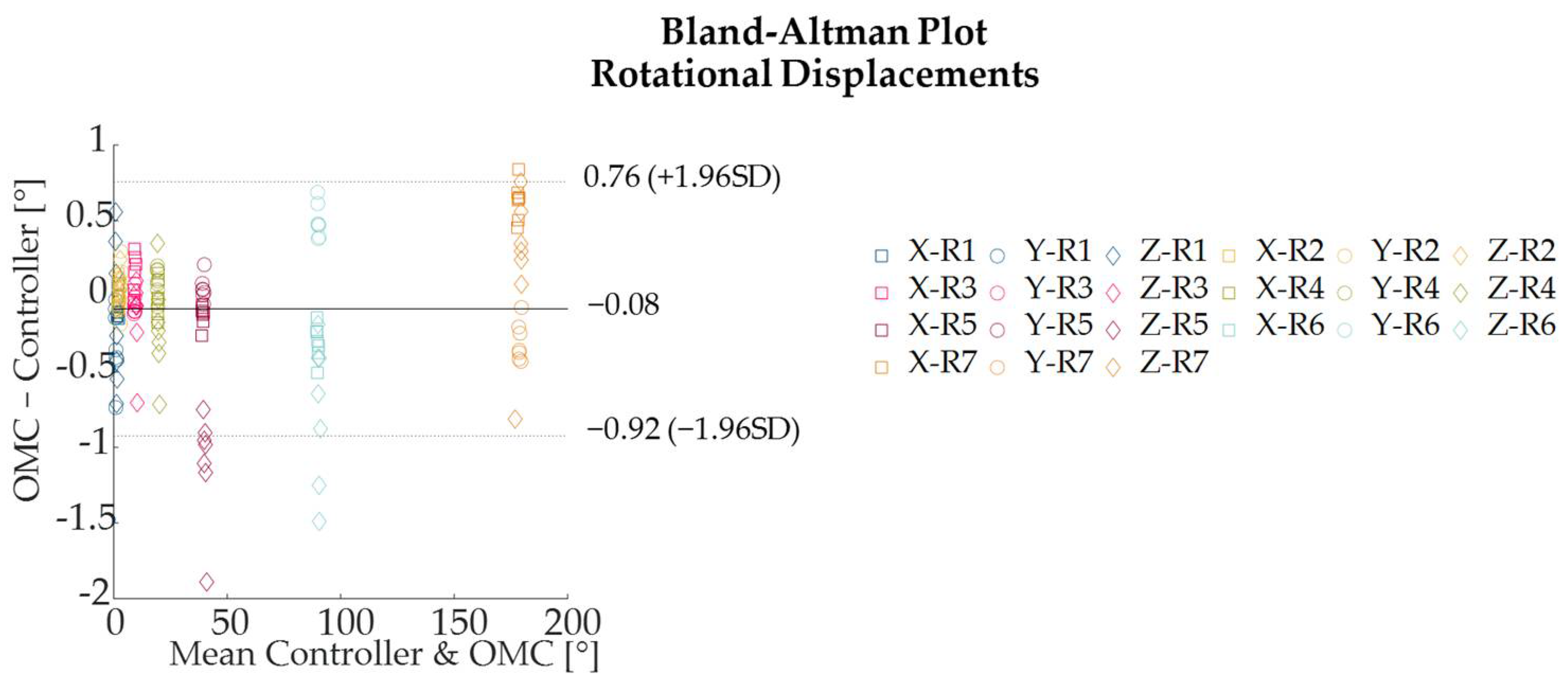
2.3.2. Rotational Accuracy
3. Results
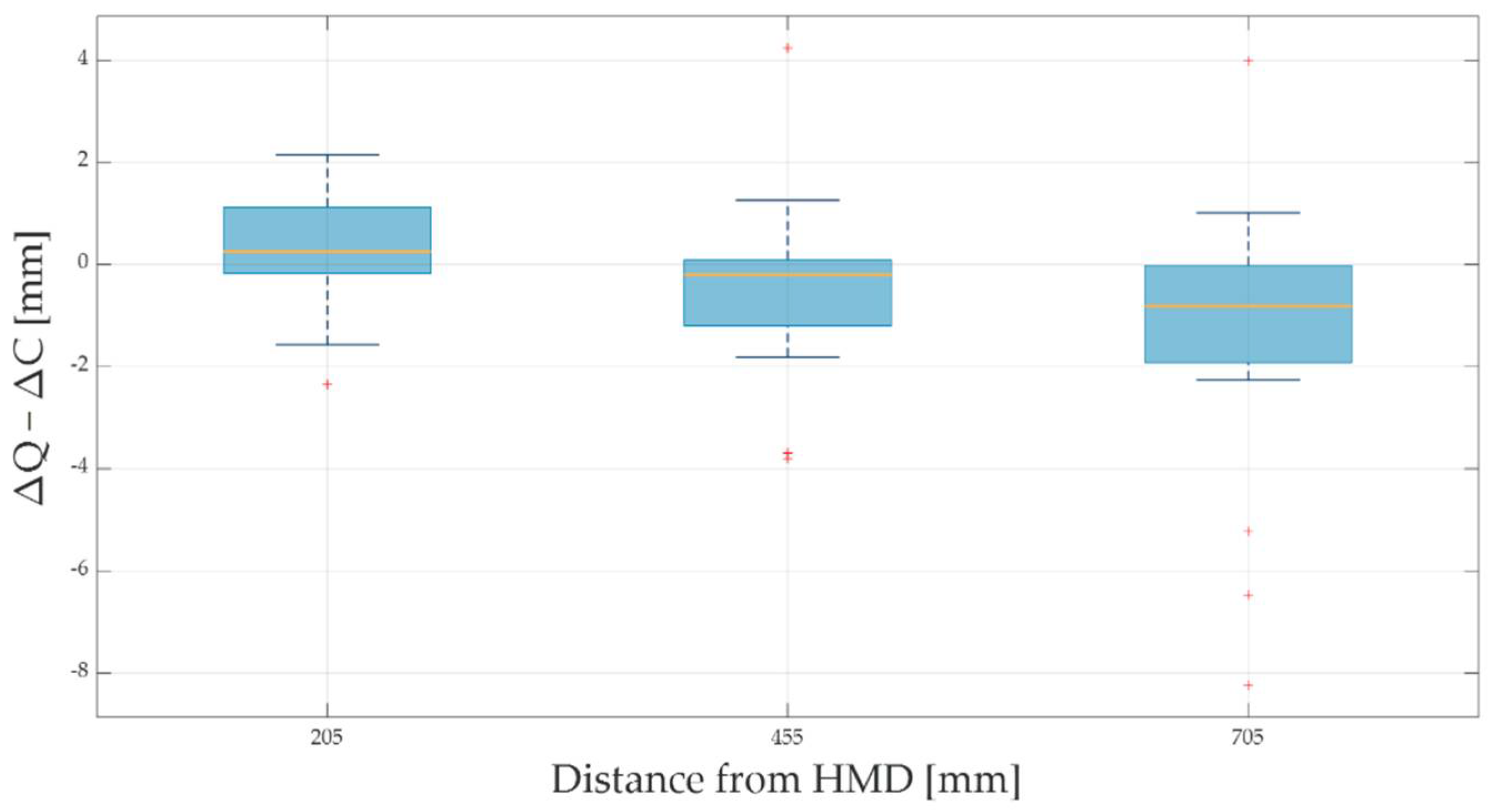
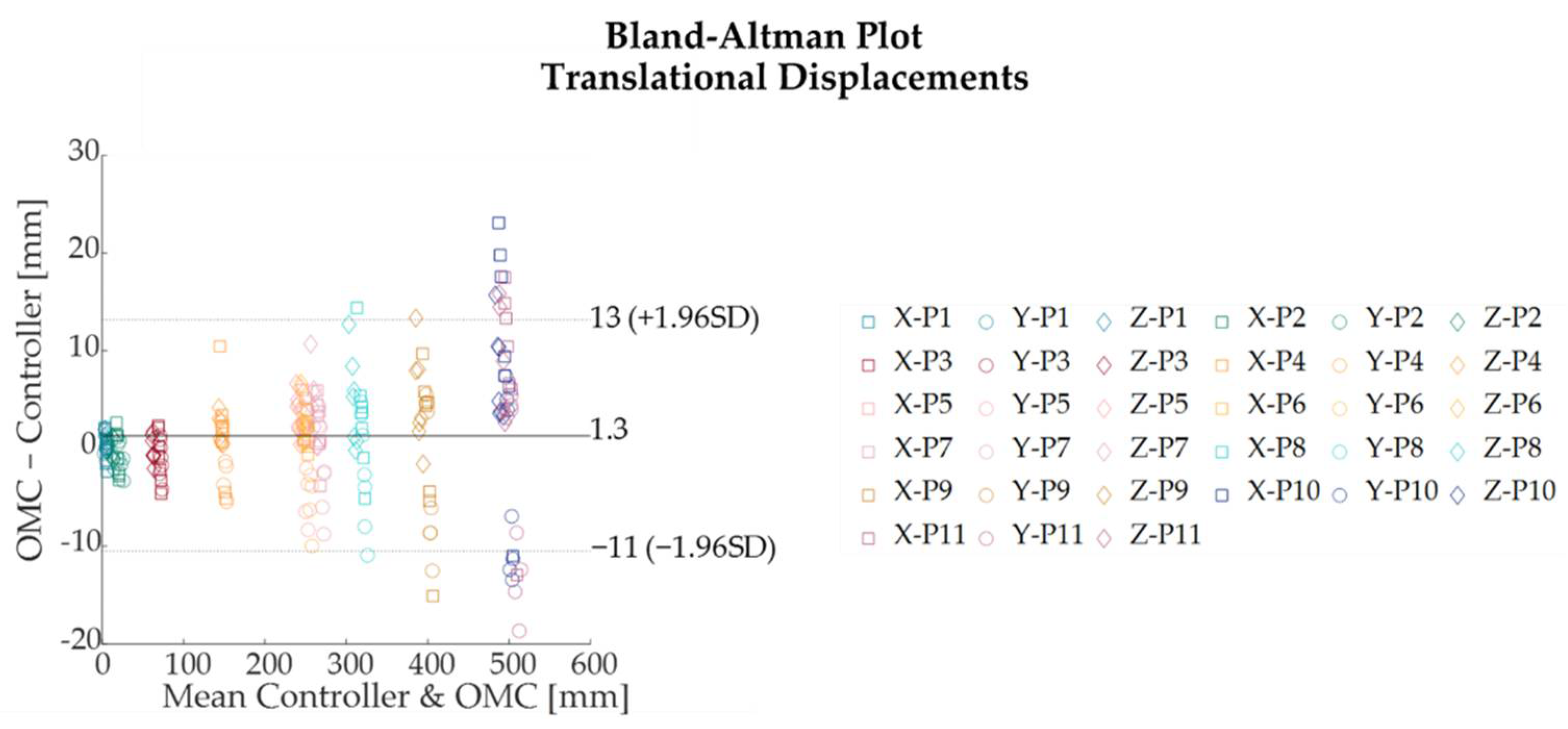
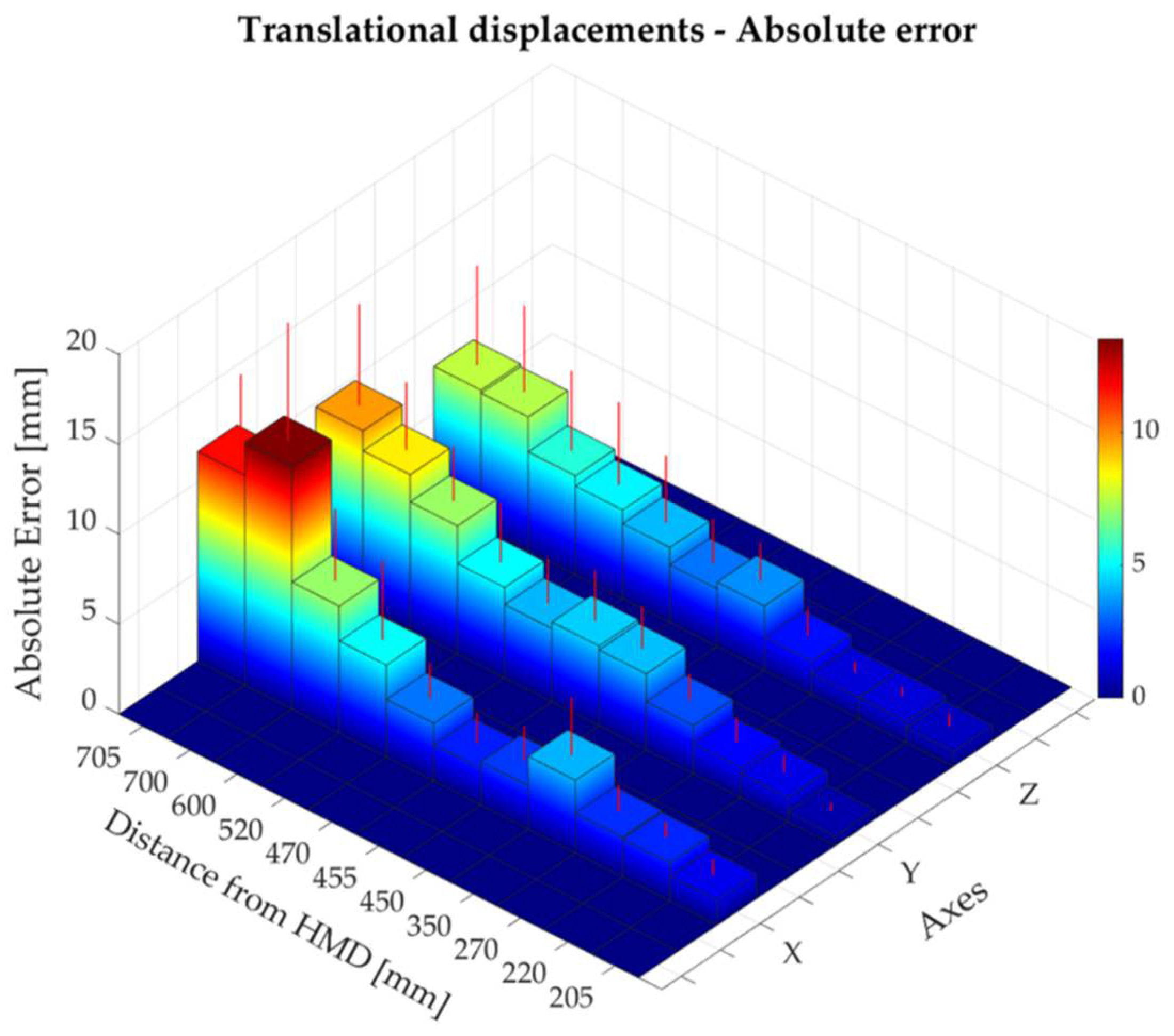
3.1. Translational Accuracy
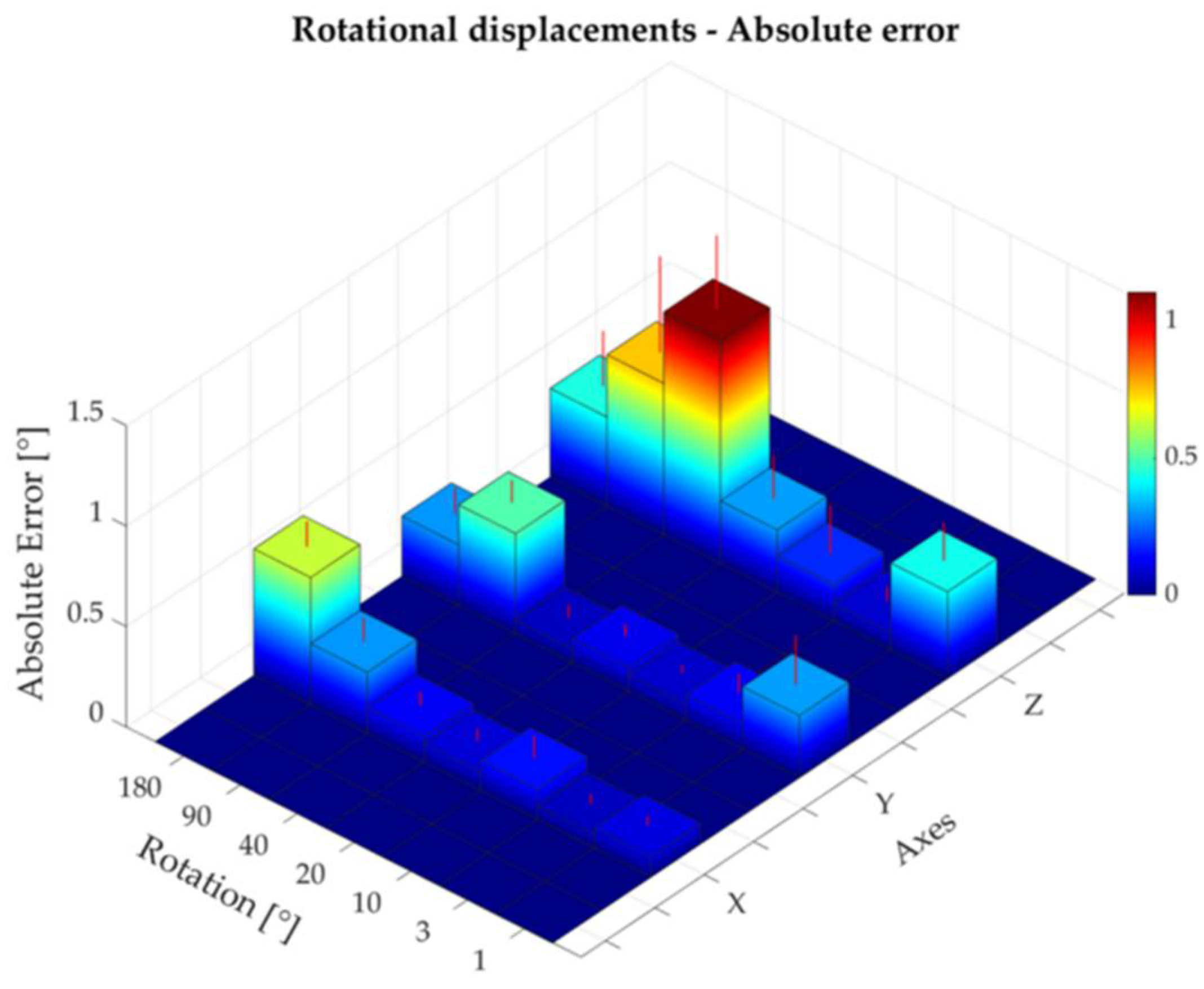
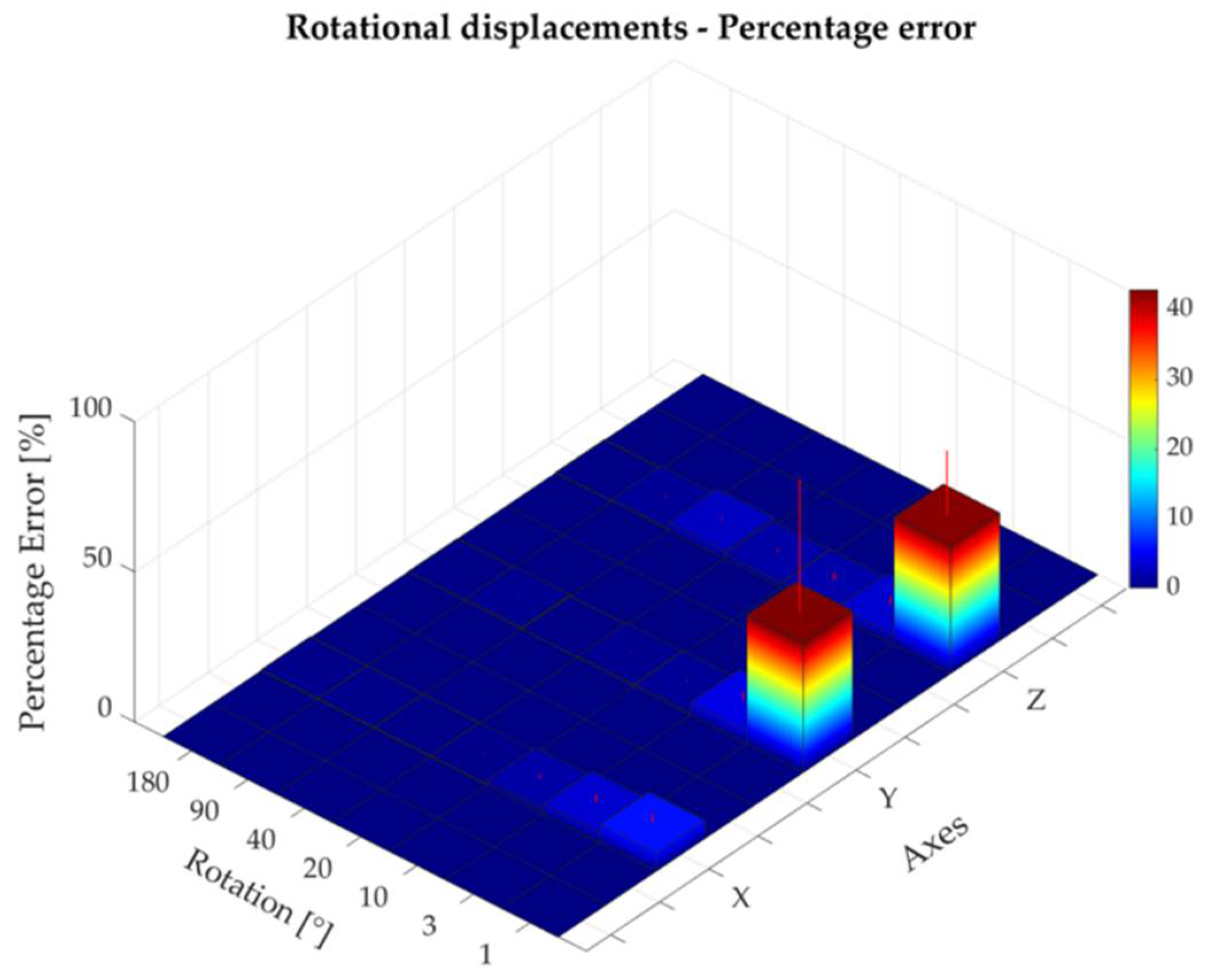
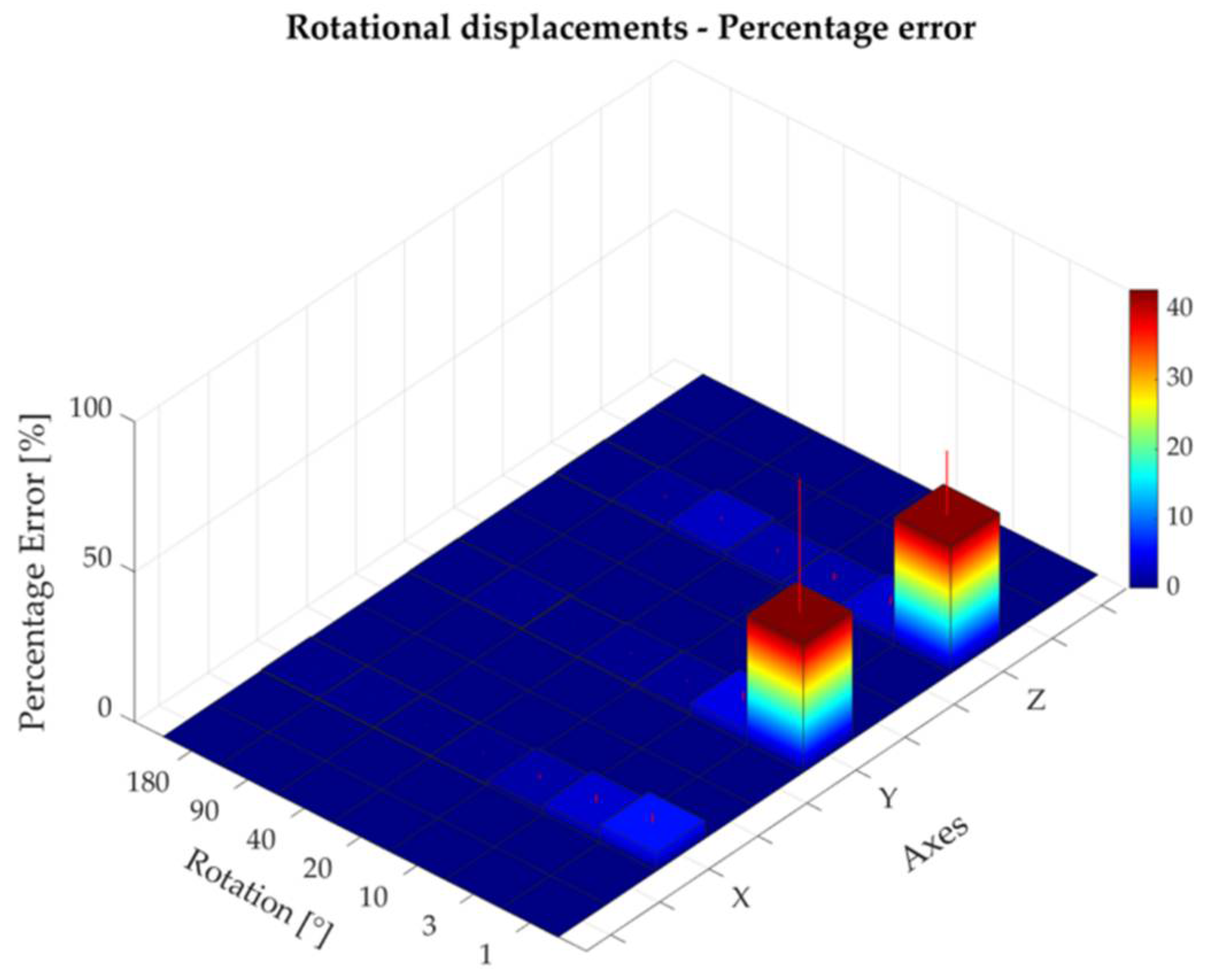
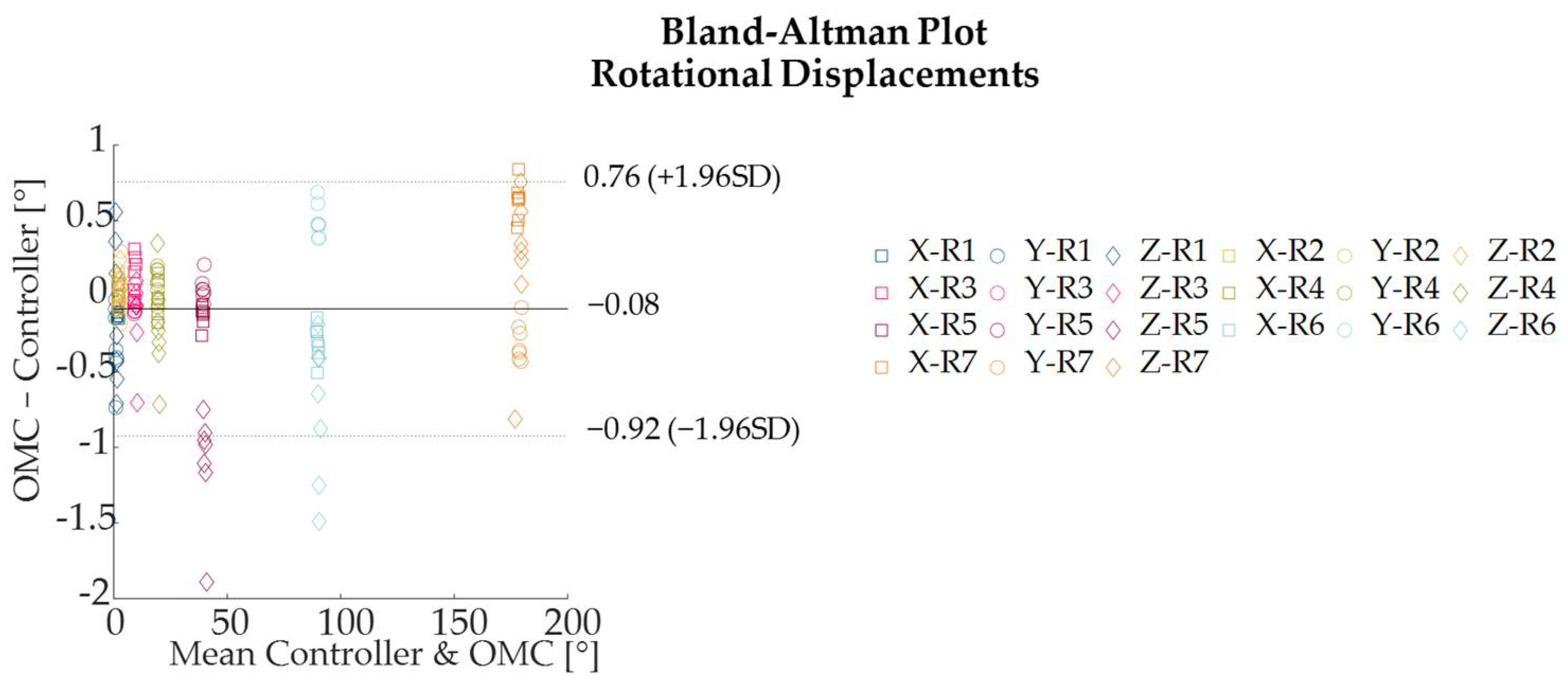
3.2. Rotational Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- do Nascimento, L.M.S.; Bonfati, L.V.; Freitas, M.L.B.; Mendes Junior, J.J.A.; Siqueira, H.V.; Stevan, S.L. Sensors and systems for physical rehabilitation and health monitoring—A review. Sensors 2020, 20, 4063. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Hu, H. Human motion tracking for rehabilitation—A survey. Biomed. Signal Process. Control 2008, 3, 1–18. [Google Scholar] [CrossRef]
- Almasi, S.; Ahmadi, H.; Asadi, F.; Shahmoradi, L.; Arji, G.; Alizadeh, M.; Kolivand, H. Kinect-based rehabilitation systems for stroke patients: A scoping review. BioMed Res. Int. 2022, 2022, 4339054. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, B.; Leardini, A.; Farella, E. Kinect and wearable inertial sensors for motor rehabilitation programs at home: State of the art and an experimental comparison. Biomed. Eng. Online 2020, 19, 25. [Google Scholar] [CrossRef] [Green Version]
- Saposnik, G.; Teasell, R.; Mamdani, M.; Hall, J.; McIlroy, W.; Cheung, D.; Thorpe, K.E.; Cohen, L.G.; Bayley, M. Effectiveness of virtual reality using Wii gaming technology in stroke rehabilitation: A pilot randomized clinical trial and proof of principle. Stroke 2010, 41, 1477–1484. [Google Scholar] [CrossRef] [Green Version]
- Gil-Gómez, J.-A.; Lloréns, R.; Alcañiz, M.; Colomer, C. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: A pilot randomized clinical trial in patients with acquired brain injury. J. Neuroeng. Rehabil. 2011, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Tao, G.; Garrett, B.; Taverner, T.; Cordingley, E.; Sun, C. Immersive virtual reality health games: A narrative review of game design. J. Neuroeng. Rehabil. 2021, 18, 31. [Google Scholar] [CrossRef]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A. Virtual reality, augmented reality, gamification, and telerehabilitation: Psychological impact on orthopedic patients’ rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef]
- Iosa, M.; Aydin, M.; Candelise, C.; Coda, N.; Morone, G.; Antonucci, G.; Marinozzi, F.; Bini, F.; Paolucci, S.; Tieri, G. The Michelangelo Effect: Art Improves the Performance in a Virtual Reality Task Developed for Upper Limb Neurorehabilitation. Front. Psychol. 2021, 11, 3832. [Google Scholar] [CrossRef]
- Sánchez-Herrera-Baeza, P.; Cano-de-la-Cuerda, R.; Oña-Simbaña, E.D.; Palacios-Ceña, D.; Pérez-Corrales, J.; Cuenca-Zaldivar, J.N.; Gueita-Rodriguez, J.; de Quirós, C.B.-B.; Jardón-Huete, A.; Cuesta-Gomez, A. The impact of a novel immersive virtual reality technology associated with serious games in Parkinson’s disease patients on upper limb rehabilitation: A mixed methods intervention study. Sensors 2020, 20, 2168. [Google Scholar] [CrossRef] [Green Version]
- Kipping, B.; Rodger, S.; Miller, K.; Kimble, R.M. Virtual reality for acute pain reduction in adolescents undergoing burn wound care: A prospective randomized controlled trial. Burns 2012, 38, 650–657. [Google Scholar] [CrossRef]
- Winter, C.; Kern, F.; Gall, D.; Latoschik, M.E.; Pauli, P.; Käthner, I. Immersive virtual reality during gait rehabilitation increases walking speed and motivation: A usability evaluation with healthy participants and patients with multiple sclerosis and stroke. J. Neuroeng. Rehabil. 2021, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Risi Ambrogioni, L.; Berton, A.; Candela, V.; Carnevale, A.; Schena, E.; Gugliemelli, E.; Denaro, V. Physical therapy and precision rehabilitation in shoulder rotator cuff disease. Int. Orthop. 2020, 44, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Carnevale, A.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Schena, E.; Denaro, V. Personalized, Predictive, Participatory, Precision, and Preventive (P5) Medicine in Rotator Cuff Tears. J. Pers. Med. 2021, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Baldominos, A.; Saez, Y.; Del Pozo, C.G. An approach to physical rehabilitation using state-of-the-art virtual reality and motion tracking technologies. Procedia Comput. Sci. 2015, 64, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Berton, A.; De Salvatore, S.; Candela, V.; Cortina, G.; Lo Presti, D.; Massaroni, C.; Petrillo, S.; Denaro, V. Delayed Rehabilitation Protocol after Rotator Cuff Repair. Osteology 2020, 1, 29–38. [Google Scholar] [CrossRef]
- Longo, U.G.; Vasta, S.; Maffulli, N.; Denaro, V. Scoring systems for the functional assessment of patients with rotator cuff pathology. Sports Med. Arthrosc. 2011, 19, 310–320. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Ahrens, P.M.; Maffulli, N.; Denaro, V. Clinical tests for the diagnosis of rotator cuff disease. Sports Med. Arthrosc. 2011, 19, 266–278. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Jan, S.V.S. Cost-effective (gaming) motion and balance devices for functional assessment: Need or hype? J. Biomech. 2016, 49, 2561–2565. [Google Scholar] [CrossRef]
- Çubukçu, B.; Yüzgeç, U.; Zileli, R.; Zileli, A. Reliability and validity analyzes of Kinect V2 based measurement system for shoulder motions. Med. Eng. Phys. 2020, 76, 20–31. [Google Scholar] [CrossRef]
- Chen, B.; Wang, W.; Hu, G.; Zhong, R.; Su, X.; Zhi, H.; Niu, W. Concurrent validity of a markerless motion capture system for the assessment of shoulder functional movement. Med. Nov. Technol. Devices 2022, 15, 100131. [Google Scholar] [CrossRef]
- Beshara, P.; Anderson, D.B.; Pelletier, M.; Walsh, W.R. The Reliability of the Microsoft Kinect and Ambulatory Sensor-Based Motion Tracking Devices to Measure Shoulder Range-of-Motion: A Systematic Review and Meta-Analysis. Sensors 2021, 21, 8186. [Google Scholar] [CrossRef] [PubMed]
- Jost, T.A.; Nelson, B.; Rylander, J. Quantitative analysis of the Oculus Rift S in controlled movement. Disabil. Rehabil. Assist. Technol. 2021, 16, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Shum, L.C.; Valdés, B.A.; Van der Loos, H.F.M. Determining the accuracy of oculus touch controllers for motor rehabilitation applications using quantifiable upper limb kinematics: Validation study. JMIR Biomed. Eng. 2019, 4, e12291. [Google Scholar] [CrossRef]
- Qualisys. Available online: https://www.qualisys.com/cameras/miqus/#!%23tech-specs (accessed on 5 May 2022).
- Huston, R.L. Principles of Biomechanics; CRC Press: Boca Raton, FL, USA, 2008; ISBN 0429116896. [Google Scholar]
- Garrett, J.W. The adult human hand: Some anthropometric and biomechanical considerations. Hum. Factors 1971, 13, 117–131. [Google Scholar] [CrossRef]
- Gates, D.H.; Walters, L.S.; Cowley, J.; Wilken, J.M.; Resnik, L. Range of motion requirements for upper-limb activities of daily living. Am. J. Occup. Ther. 2016, 70, 7001350010p1–7001350010p10. [Google Scholar] [CrossRef] [Green Version]
- Myles, P.S.; Cui, J.I. Using the Bland–Altman method to measure agreement with repeated measures. Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Glegg, S.; Colquhoun, H.; Miller, P.; Noubary, F. Virtual reality and active videogame-based practice, learning needs, and preferences: A cross-Canada survey of physical therapists and occupational therapists. Games Health J. 2017, 6, 217–228. [Google Scholar] [CrossRef]
- Pekyavas, N.O.; Ergun, N. Comparison of virtual reality exergaming and home exercise programs in patients with subacromial impingement syndrome and scapular dyskinesis: Short term effect. Acta Orthop. Traumatol. Turc. 2017, 51, 238–242. [Google Scholar] [CrossRef]
- Spitzley, K.A.; Karduna, A.R. Feasibility of using a fully immersive virtual reality system for kinematic data collection. J. Biomech. 2019, 87, 172–176. [Google Scholar] [CrossRef]
- Huber, M.E.; Seitz, A.L.; Leeser, M.; Sternad, D. Validity and reliability of Kinect skeleton for measuring shoulder joint angles: A feasibility study. Physiotherapy 2015, 101, 389–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niehorster, D.C.; Li, L.; Lappe, M. The accuracy and precision of position and orientation tracking in the HTC vive virtual reality system for scientific research. I-Perception 2017, 8, 2041669517708205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 546. [Google Scholar] [CrossRef]
- Carnevale, A.; Schena, E.; Formica, D.; Massaroni, C.; Longo, U.G.; Denaro, V. Skin Strain Analysis of the Scapular Region and Wearables Design. Sensors 2021, 21, 5761. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, A.; Massaroni, C.; Presti, D.L.; Formica, D.; Longo, U.G.; Schena, E.; Denaro, V. Wearable stretchable sensor based on conductive textile fabric for shoulder motion monitoring. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 and IoT, Rome, Italy, 3–5 June 2020. [Google Scholar]
- Faisal, A.I.; Majumder, S.; Mondal, T.; Cowan, D.; Naseh, S.; Deen, M.J. Monitoring methods of human body joints: State-of-the-art and research challenges. Sensors 2019, 19, 2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.-S.; Cho, S.; Ku, J.; Kim, Y.; Lee, K.; Hwang, H.-J.; Paik, N.-J. Clinical application of virtual reality for upper limb motor rehabilitation in stroke: Review of technologies and clinical evidence. J. Clin. Med. 2020, 9, 3369. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Memory | 6 GB |
| Storage | 256 GB |
| Display | LCD 1832 × 1920 per eye @ 72–120 Hz |
| Graphics | Adreno 650 (~1.2 TFLOPS) |
| Sound | 2 built in speaker/3.5 mm headphone jack |
| Input | 6DOF Inside-out tracking through 4 built-in cameras and 2 controllers with accelerometers and gyroscopes Optional: QWERTY keyboard (via Bluetooth) |
| Controller Input | Oculus Touch |
| Camera | 4 infrared cameras |
| Mass | 503 g |
| Directional Axis | Translational Displacement P [mm] | Absolute Error Mean (SD) [mm] | Percentage Error Mean (SD) [%] | |
|---|---|---|---|---|
| X | P1 | 5 | 1.38 (0.85) | 29.5 (18.5) |
| P2 | 20 | 2.13 (0.88) | 11.0 (4.4) | |
| P3 | 70 | 2.22 (1.47) | 3.2 (2.1) | |
| P4 | 150 | 4.04 (3.22) | 2.7 (2.1) | |
| P5 | 250 | 2.41 (1.92) | 1.0 (0.8) | |
| P6 | 255 | 2.03 (1.72) | 0.8 (0.7) | |
| P7 | 270 | 3.21 (1.96) | 1.2 (0.7) | |
| P8 | 320 | 5.11 (4.39) | 1.6 (1.4) | |
| P9 | 400 | 7.06 (3.99) | 1.8 (1.0) | |
| P10 | 500 | 13.52 (6.57) | 2.7 (1.3) | |
| P11 | 505 | 11.67 (4.21) | 2.3 (0.8) | |
| Y | P1 | 5 | 0.55 (0.47) | 11.8 (10.4) |
| P2 | 20 | 1.35 (0.94) | 6.0 (3.7) | |
| P3 | 70 | 1.68 (1.36) | 2.4 (1.9) | |
| P4 | 150 | 2.68 (1.47) | 1.8 (1.0) | |
| P5 | 250 | 4.22 (2.35) | 1.7 (0.9) | |
| P6 | 255 | 4.43 (2.84) | 1.7 (1.1) | |
| P7 | 270 | 4.07 (2.51) | 1.5 (0.9) | |
| P8 | 320 | 5.02 (3.32) | 1.6 (1.0) | |
| P9 | 400 | 7.11 (3.02) | 1.8 (0.8) | |
| P10 | 500 | 8.63 (3.74) | 1.7 (0.8) | |
| P11 | 505 | 9.74 (5.65) | 1.9 (1.1) | |
| Z | P1 | 5 | 0.81 (0.73) | 16.7 (16.4) |
| P2 | 20 | 1.16 (0.52) | 8.5 (3.9) | |
| P3 | 70 | 1.16 (0.57) | 1.8 (0.9) | |
| P4 | 150 | 1.85 (1.48) | 1.3 (1.0) | |
| P5 | 250 | 3.59 (2.12) | 1.5 (0.9) | |
| P6 | 255 | 3.21 (2.51) | 1.3 (1.0) | |
| P7 | 270 | 4.17 (3.72) | 1.6 (1.4) | |
| P8 | 320 | 4.93 (4.60) | 1.6 (1.5) | |
| P9 | 400 | 5.50 (4.43) | 1.4 (1.1) | |
| P10 | 500 | 7.44 (4.78) | 1.5 (1.0) | |
| P11 | 505 | 7.60 (5.56) | 1.5 (1.1) | |
| Directional Axis | Rotational Displacement R [°] | Absolute Error Mean (SD) [°] | Percentage Error Mean (SD) [%] | |
|---|---|---|---|---|
| X | R1 | 1 | 0.10 (0.05) | 5.9 (3.1) |
| R2 | 3 | 0.07 (0.05) | 3.3 (2.4) | |
| R3 | 10 | 0.15 (0.12) | 1.6 (1.2) | |
| R4 | 20 | 0.09 (0.06) | 0.5 (0.3) | |
| R5 | 40 | 0.13 (0.07) | 0.3 (0.2) | |
| R6 | 90 | 0.30 (0.12) | 0.3 (0.1) | |
| R7 | 180 | 0.63 (0.13) | 0.4 (0.1) | |
| Y | R1 | 1 | 0.31 (0.25) | 42.9 (44.6) |
| R2 | 3 | 0.13 (0.10) | 4.2 (3.0) | |
| R3 | 10 | 0.08 (0.04) | 0.9 (0.4) | |
| R4 | 20 | 0.12 (0.06) | 0.6 (0.3) | |
| R5 | 40 | 0.07 (0.07) | 0.2 (0.2) | |
| R6 | 90 | 0.50 (0.11) | 0.6 (0.1) | |
| R7 | 180 | 0.30 (0.13) | 0.2 (0.1) | |
| Z | R1 | 1 | 0.43 (0.19) | 42.6 (21.5) |
| R2 | 3 | 0.09 (0.08) | 3.2 (2.6) | |
| R3 | 10 | 0.18 (0.24) | 1.8 (2.4) | |
| R4 | 20 | 0.31 (0.22) | 1.6 (1.1) | |
| R5 | 40 | 1.11 (0.37) | 2.8 (0.9) | |
| R6 | 90 | 0.75 (0.48) | 0.8 (0.5) | |
| R7 | 180 | 0.44 (0.27) | 0.2 (0.2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carnevale, A.; Mannocchi, I.; Sassi, M.S.H.; Carli, M.; De Luca, G.; Longo, U.G.; Denaro, V.; Schena, E. Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2. Sensors 2022, 22, 5511. https://doi.org/10.3390/s22155511
Carnevale A, Mannocchi I, Sassi MSH, Carli M, De Luca G, Longo UG, Denaro V, Schena E. Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2. Sensors. 2022; 22(15):5511. https://doi.org/10.3390/s22155511
Chicago/Turabian StyleCarnevale, Arianna, Ilaria Mannocchi, Mohamed Saifeddine Hadj Sassi, Marco Carli, Giovanna De Luca, Umile Giuseppe Longo, Vincenzo Denaro, and Emiliano Schena. 2022. "Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2" Sensors 22, no. 15: 5511. https://doi.org/10.3390/s22155511
APA StyleCarnevale, A., Mannocchi, I., Sassi, M. S. H., Carli, M., De Luca, G., Longo, U. G., Denaro, V., & Schena, E. (2022). Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2. Sensors, 22(15), 5511. https://doi.org/10.3390/s22155511