
Artifacts in EEG-Based BCI Therapies: Friend or Foe?

 ,
,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Motivation
1.2. EEG Artifacts and Processing Pipelines
1.3. Study Design
2. Materials and Methods
2.1. Participants
2.2. Experimental Setup
2.3. Virtual Reality Presentation
2.4. Task Protocol
2.5. Data Preprocessing
2.5.1. EMG Data
2.5.2. EEG Data
2.5.3. The Time-Frequency Approach
2.5.4. The Bandpower Approach
2.5.5. Common Spatial Patterns (CSP)
2.6. Classifier Properties
2.6.1. The Time-Frequency Approach
2.6.2. The Bandpower Approach
3. Results
3.1. Summary
3.2. EMG Analysis
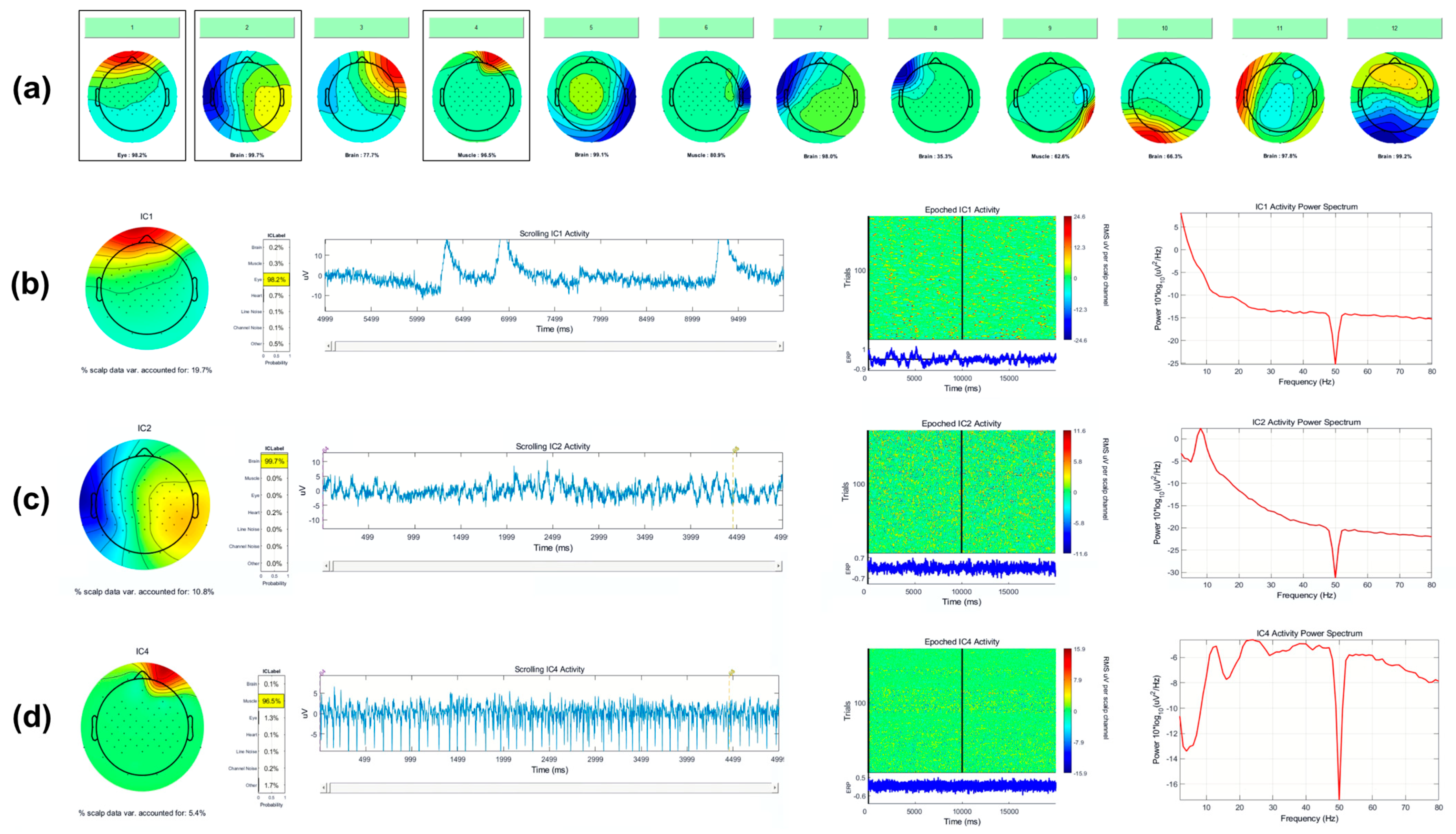
3.3. Artifact Characterization
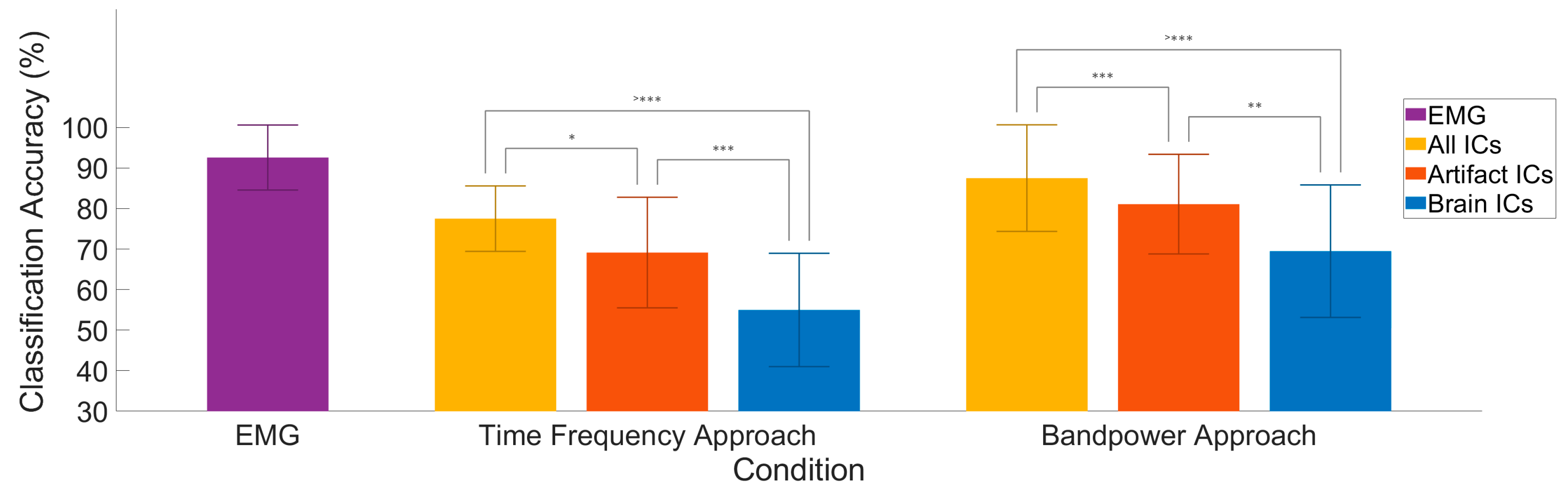
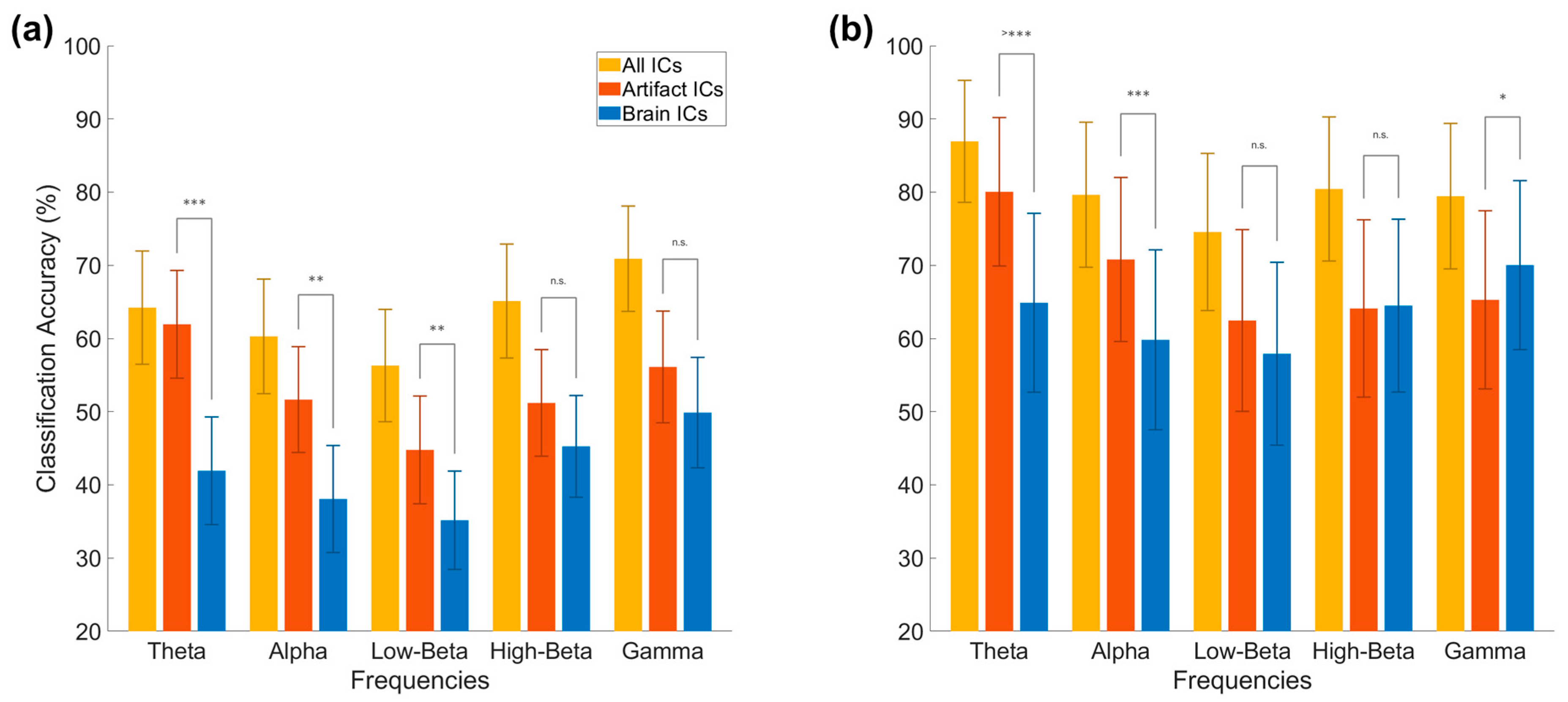
3.4. Classification Accuracy
3.5. Interpretation of Classifier Results
3.5.1. Motivation
3.5.2. Visualization of TFA Approach
3.5.3. Visualization of Bandpower Approach
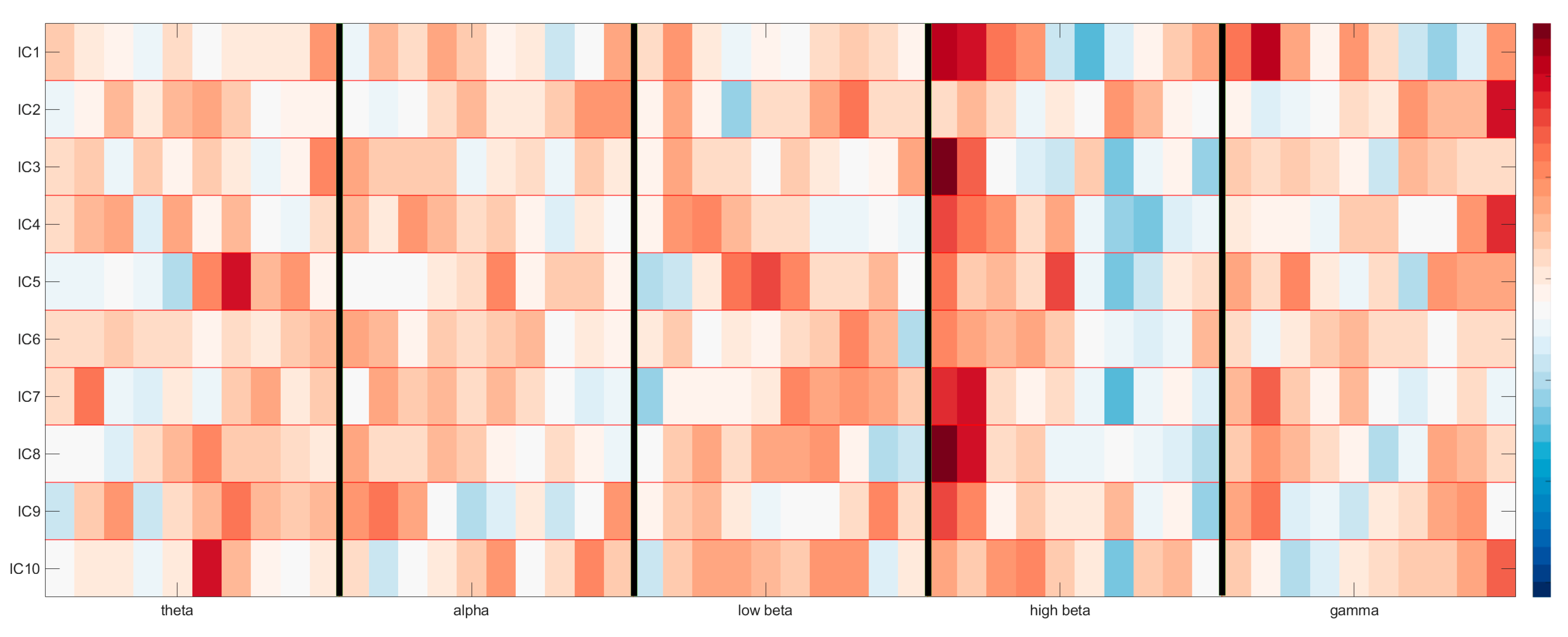
3.6. Common Spatial Patterns (CSP) for Feature Selection
4. Discussion
4.1. Implications
4.2. Comparison with Previous Work
4.3. Significance
4.4. Limitations
4.5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Fatourechi, M.; Bashashati, A.; Ward, R.; Birch, G. EMG and EOG artifacts in brain computer interface systems: A survey. Clin. Neurophysiol. 2007, 118, 480–494. [Google Scholar] [CrossRef]
- Vaughan, T.; Heetderks, W.; Trejo, L.; Rymer, W.; Weinrich, M.; Moore, M.; Kübler, A.; Dobkin, B.; Birbaumer, N.; Donchin, E.; et al. Brain-computer interface technology: A review of the Second International Meeting. IEEE Trans. Neural Syst. Rehabil. Eng. 2003, 11, 94–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, E.J.; Metsomaa, J.; Belardinelli, P.; Grosse-Wentrup, M.; Ziemann, U.; Zrenner, C. Predicting motor behavior: An efficient EEG signal processing pipeline to detect brain states with potential therapeutic relevance for VR-based neurorehabilitation. Virtual Real. 2021, 25, 1–23. [Google Scholar] [CrossRef]
- Barlow, J. Artifact processing (rejection and minimization) in EEG data processing. In Handbook of Electroencephalography and Clinical Neurophysiology; Revised series vol. 2; Elsevier: Amsterdam, The Netherlands, 1986; pp. 15–62. [Google Scholar]
- Fisch, B.; Spehlmann, R. Fisch and Spehlmann’s EEG Primer: Basic Principles of Digital and Analog EEG; Elsevier: Amsterdam, The Netherlands, 1999. [Google Scholar]
- Kim, J.; Caire, G.; Molisch, A. Quality-aware streaming and scheduling for device-to-device video delivery. IEEE/ACM Trans. Netw. 2015, 24, 2319–2331. [Google Scholar] [CrossRef]
- Snider, J.; Plank, M.; Lee, D.; Poizner, H. Simultaneous neural and movement recording in large-scale immersive virtual environments. IEEE Trans. Biomed. Circuits Syst. 2013, 7, 713–721. [Google Scholar] [CrossRef]
- Steinisch, M.; Tana, M.; Comani, S. A post-stroke rehabilitation system integrating robotics, VR and high-resolution EEG imaging. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 849–859. [Google Scholar] [CrossRef]
- Teo, W.; Muthalib, M.; Yamin, S.; Hendy, A.; Bramstedt, K.; Kotsopoulos, E.; Perrey, S.; Ayaz, H. Does a combination of virtual reality, neuromodulation and neuroimaging provide a comprehensive platform for neurorehabilitation? A narrative review of the literature. Front. Hum. Neurosci. 2016, 10, 284. [Google Scholar] [CrossRef]
- Lotte, F.; Guan, C. Regularizing common spatial patterns to improve BCI designs: Unified theory and new algorithms. IEEE Trans. Biomed. Eng. 2010, 58, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Ramoser, H.; Muller-Gerking, J.; Pfurtscheller, G. Optimal spatial filtering of single trial EEG during imagined hand movement. IEEE Trans. Rehabil. Eng. 2000, 8, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Gao, S.; Gao, X. Common spatial pattern method for channel selection in motor imagery based brain-computer interface. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006. [Google Scholar]
- Barua, S.; Begum, S. A review on machine learning algorithms in handling EEG artifacts. In Proceedings of the Swedish AI Society (SAIS) Workshop SAIS, Stockholm, Sweden, 22–23 May 2014. [Google Scholar]
- Urigüen, J.A.; Garcia-Zapirain, B. EEG artifact removal—State-of-the-art and guidelines. J. Neural Eng. 2015, 12, 031001. [Google Scholar] [CrossRef]
- Chambayil, B.; Singla, R.; Jha, R. Virtual keyboard BCI using Eye blinks in EEG. In Proceedings of the 2010 IEEE 6th International Conference on Wireless and Mobile Computing, Networking and Communications, Niagara Falls, ON, Canada, 11–13 October 2010. [Google Scholar]
- Ma, W.; Tran, D.; Le, T.; Lin, H.; Zhou, S.-M. Using EEG artifacts for BCI applications. In Proceedings of the 2014 International Joint Conference on Neural Networks (IJCNN), Beijing, China, 6–11 July 2014. [Google Scholar]
- Mane, R.; Chouhan, T.; Guan, C. BCI for stroke rehabilitation: Motor and beyond. J. Neural Eng. 2020, 17, 041001. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; Lange, B.; George, S.; Deutsch, J.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Stroke 2018, 49, 160–161. [Google Scholar] [CrossRef]
- McDermott, E.J.; Himmelbach, M. Effects of arm weight and target height on hand selection: A low-cost virtual reality paradigm. PLoS ONE 2019, 14, e0207326. [Google Scholar] [CrossRef] [Green Version]
- McDermott, E.J.; Zwiener, T.; Ziemann, U.; Zrenner, C. Real-time decoding of 5 finger movements from 2 EMG channels for mixed reality human-computer interaction. bioRxiv 2021. [Google Scholar] [CrossRef]
- Oostenveld, R.; Praamstra, P. The five percent electrode system for high-resolution EEG and ERP measurements. Clin. Neurophysiol. 2001, 112, 713–719. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Hyvarinen, A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans. Neural Netw. 1999, 10, 626–634. [Google Scholar] [CrossRef] [Green Version]
- Grosse-Wentrup, M.; Buss, M. Multiclass common spatial patterns and information theoretic feature extraction. IEEE Trans. Biomed. Eng. 2008, 55, 1991–2000. [Google Scholar] [CrossRef] [PubMed]
- Fürnkranz, J. Round robin classification. J. Mach. Learn. Res. 2002, 2, 721–747. [Google Scholar]
- Haufe, S.; Meinecke, F.; Görgen, K.; Dähne, S.; Haynes, J.-D.; Blankertz, B.; Bießmann, F. On the interpretation of weight vectors of linear models in multivariate neuroimaging. NeuroImage 2014, 87, 96–110. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.-H.; Jeong, J.-H.; Shim, K.-H.; Lee, S.-W. Classification of high-dimensional motor imagery tasks based on an end-to-end role assigned convolutional neural network. In Proceedings of the 2020 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Barcelona, Spain, 4–8 May 2020. [Google Scholar]
- Shenoy, H.; Vinod, A.; Guan, C. Multi-direction hand movement classification using EEG-based source space analysis. In Proceedings of the 38th Annual International Conference IEEE Engineering Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 4551–4554. [Google Scholar]
- Shenoy, H.; Vinod, A.; Guan, C. EEG source space analysis of the supervised factor analytic approach for the classification of multi-directional arm movement. J. Neural Eng. 2017, 14, 46008. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Chen, X.; Yan, Y.; Wei, W.; Wang, Z.J. Classification of EEG signals using a multiple kernel learning support vector machine. Sensors 2014, 14, 12784–12802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.-H.; Jeong, J.-H.; Lee, S.-W. SessionNet: Feature similarity-based weighted ensemble learning for motor imagery classification. IEEE Access 2020, 8, 134524–134535. [Google Scholar] [CrossRef]
- Shenoy, P.; Miller, K.J.; Ojemann, J.G.; Rao, R.P. Finger movement classification for an electrocorticographic BCI. In Proceedings of the 2007 3rd International IEEE/EMBS Conference on Neural Engineering, Kohala Coast, HI, USA, 2–5 May 2007. [Google Scholar]
- Pion-Tonachini, L.; Kreutz-Delgado, K.; Makeig, S. ICLabel: An automated electroencephalographic independent component classifier, dataset, and website. NeuroImage 2019, 198, 181–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zrenner, D.; Desideri, D.; Belardinelli, P.; Ziemann, U. Real-time EEG-defined excitability states determine efficacy of TMS-induced plasticity in human motor cortex. Brain Stimul. 2018, 11, 74–389. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDermott, E.J.; Raggam, P.; Kirsch, S.; Belardinelli, P.; Ziemann, U.; Zrenner, C. Artifacts in EEG-Based BCI Therapies: Friend or Foe? Sensors 2022, 22, 96. https://doi.org/10.3390/s22010096
McDermott EJ, Raggam P, Kirsch S, Belardinelli P, Ziemann U, Zrenner C. Artifacts in EEG-Based BCI Therapies: Friend or Foe? Sensors. 2022; 22(1):96. https://doi.org/10.3390/s22010096
Chicago/Turabian StyleMcDermott, Eric James, Philipp Raggam, Sven Kirsch, Paolo Belardinelli, Ulf Ziemann, and Christoph Zrenner. 2022. "Artifacts in EEG-Based BCI Therapies: Friend or Foe?" Sensors 22, no. 1: 96. https://doi.org/10.3390/s22010096
APA StyleMcDermott, E. J., Raggam, P., Kirsch, S., Belardinelli, P., Ziemann, U., & Zrenner, C. (2022). Artifacts in EEG-Based BCI Therapies: Friend or Foe? Sensors, 22(1), 96. https://doi.org/10.3390/s22010096