
A Raspberry Pi-Based Traumatic Brain Injury Detection System for Single-Channel Electroencephalogram


 and
and 
Abstract
1. Introduction
1.1. Background
1.2. Related Works
2. Materials and Methods
2.1. Dataset Details
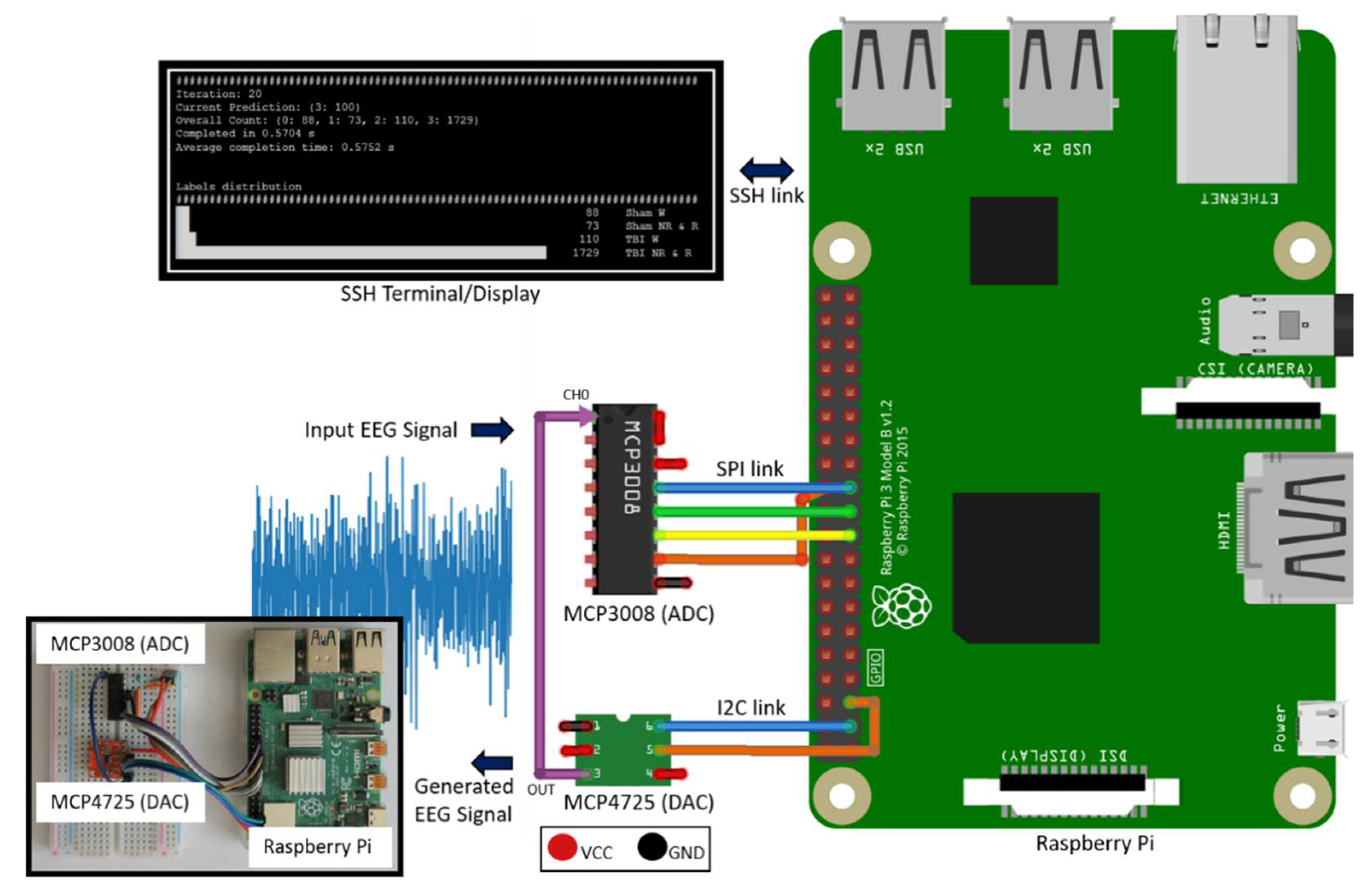
2.2. System Design
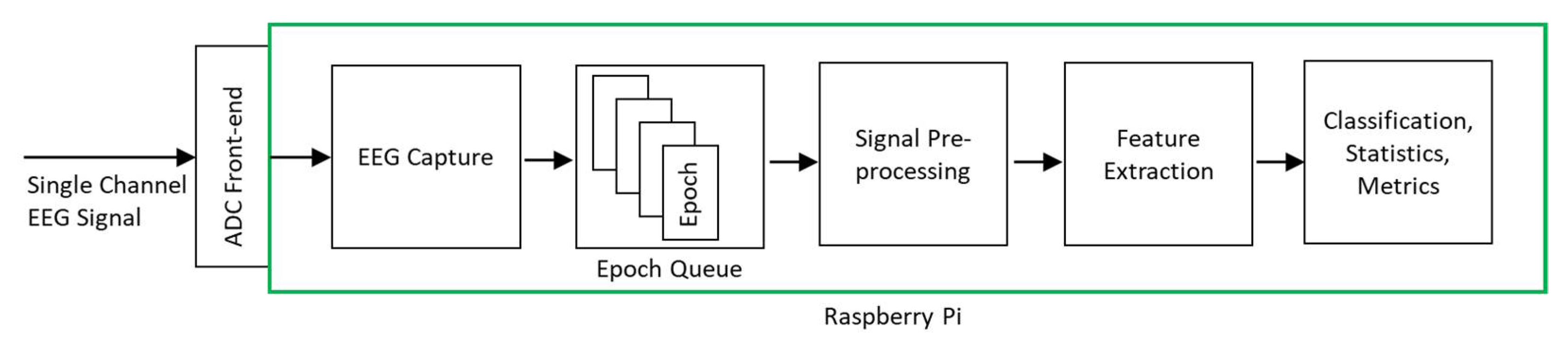
2.3. Classification System
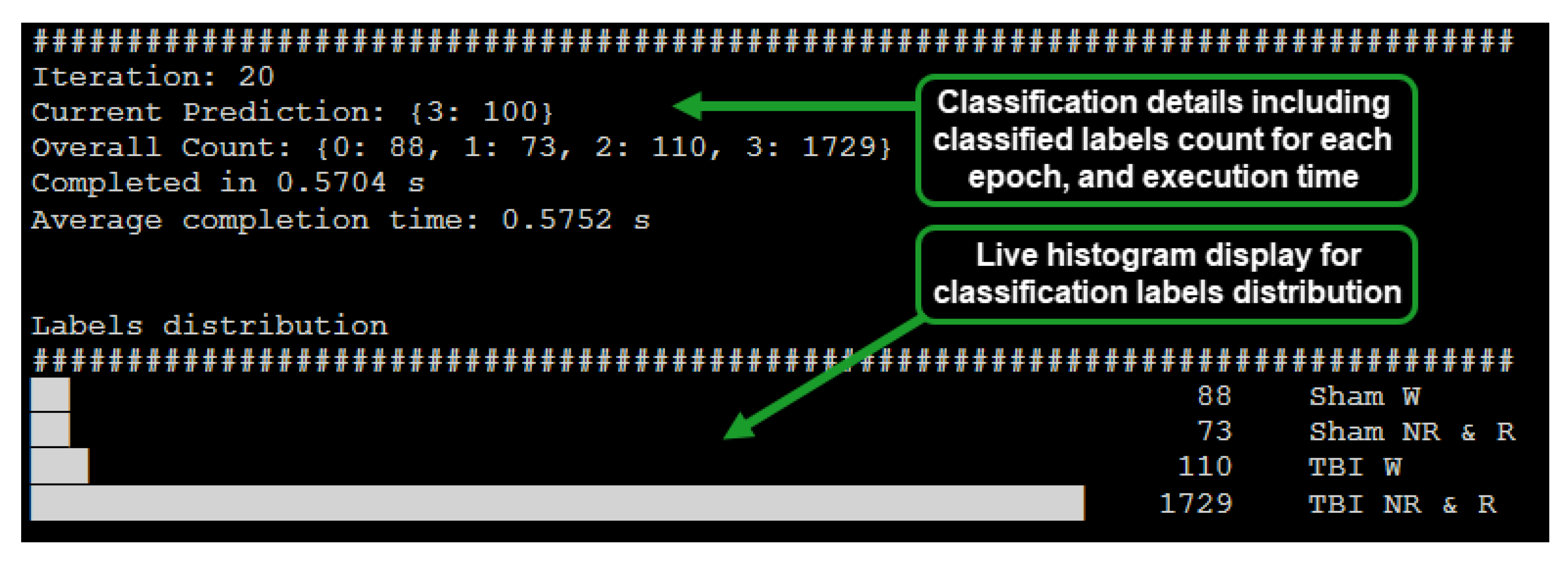
2.4. System Operation
2.5. System Verification
3. Results
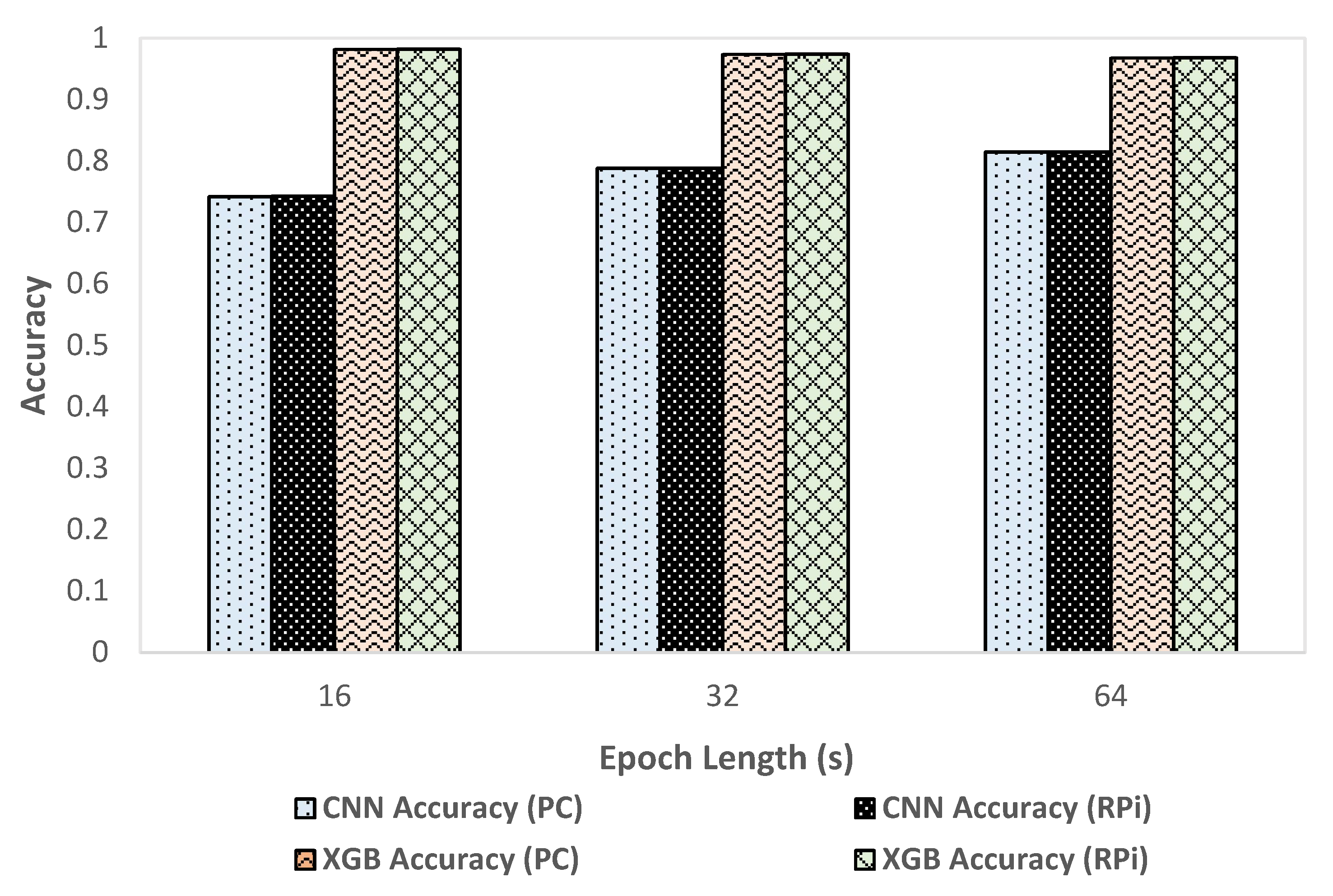
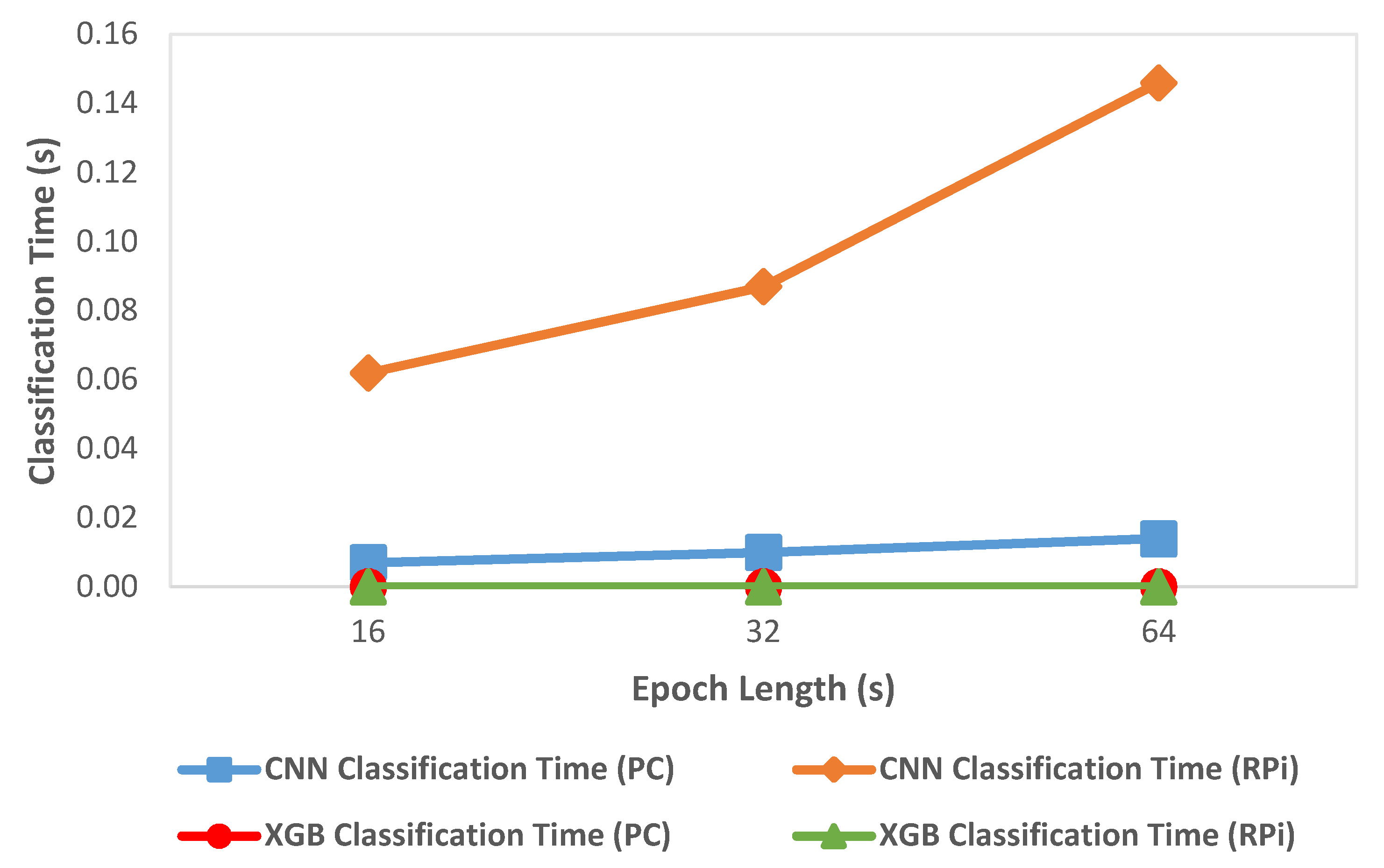
3.1. Performance Comparison of RPi with HPC
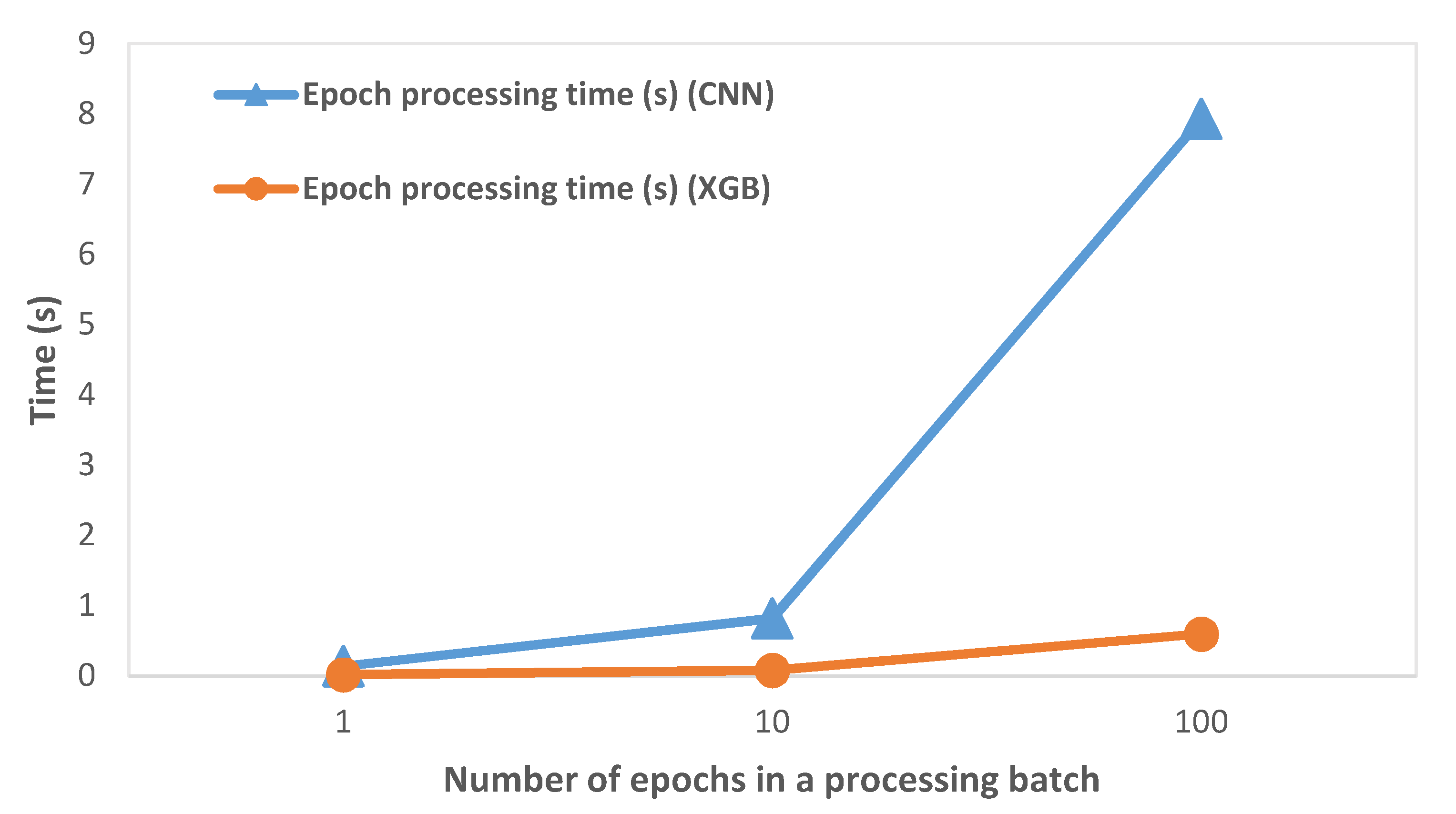
3.2. Epoch Processing Time
3.3. Generated EEG Signal Quality
3.4. Performance Comparison of CNN and XGBoost
3.5. Queue-Based Processing System Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Traumatic Brain Injury Information Page. National Institute of Neurological Disorders and Stroke. Available online: https://www.ninds.nih.gov/Disorders/All-Disorders/Traumatic-Brain-Injury-Information-Page (accessed on 7 January 2021).
- TBI: Get the Facts|Concussion|Traumatic Brain Injury|CDC Injury Center. Available online: https://www.cdc.gov/traumaticbraininjury/get_the_facts.html (accessed on 5 January 2021).
- Lim, M.M.; Elkind, J.; Xiong, G.; Galante, R.; Zhu, J.; Zhang, L.; Lian, J.; Rodin, J.; Kuzma, N.N.; Pack, A.I.; et al. Dietary Therapy Mitigates Persistent Wake Deficits Caused by Mild Traumatic Brain Injury. Sci. Transl. Med. 2013, 5, 215ra173. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Newberg, A. Neuroimaging in Traumatic Brain Imaging. NeuroRx 2005, 2, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R. Two Decades of Advances in Understanding of Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2005, 20, 5–18. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, M.E.; Carlson, K.; Storzbach, D.; Brenner, L.; Freeman, M.; Quiñones, A.; Motu’apuaka, M.; Ensley, M.; Kansagara, D. Complications of Mild Traumatic Brain Injury in Veterans and Military Personnel: A Systematic Review. In VA Evidence-Based Synthesis Program Reports; Department of Veterans Affairs: Washington, DC, USA, 2013. [Google Scholar]
- Carroll, L.J.; Cassidy, J.D.; Holm, L.; Kraus, J.; Coronado, V.G. Methodological issues and research recommendations for mild traumatic brain injury: The who collaborating centre task force on mild traumatic brain injury. J. Rehabil. Med. 2004, 36, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Dixon, C.E.; Lyeth, B.G.; Povlishock, J.T.; Findling, R.L.; Hamm, R.J.; Marmarou, A.; Young, H.F.; Hayes, R.L. A fluid percussion model of experimental brain injury in the rat. J. Neurosurg. 1987, 67, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Byrom, B.; Mc Carthy, M.; Schuleler, P.; Muehlhausen, W. Brain Monitoring Devices in Neuroscience Clinical Research: The Potential of Remote Monitoring Using Sensors, Wearables, and Mobile Devices. Clin. Pharmacol. Ther. 2018, 104, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016. [Google Scholar] [CrossRef]
- Vishwanath, M.; Jafarlou, S.; Shin, I.; Lim, M.M.; Dutt, N.; Rahmani, A.M.; Cao, H. Investigation of Machine Learning Approaches for Traumatic Brain Injury Classification via EEG Assessment in Mice. Sensors 2020, 20, 2027. [Google Scholar] [CrossRef] [PubMed]
- Sandsmark, D.K.; Elliott, J.E.; Lim, M.M. Sleep-Wake Disturbances After Traumatic Brain Injury: Synthesis of Human and Animal Studies. Sleep 2017, 40. [Google Scholar] [CrossRef] [PubMed]
- Modarres, M.H.; Kuzma, N.N.; Kretzmer, T.; Pack, A.I.; Lim, M.M. EEG slow waves in traumatic brain injury: Convergent findings in mouse and man. Neurobiol. Sleep Circadian Rhythm. 2017, 2, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Rapp, P.E.; Keyser, P.D.O.; Ealbano, A.; Ehernandez, R.; Gibson, D.B.; Zambon, R.A.; Hairston, W.D.; Hughes, J.D.; Ekrystal, A.; Nichols, A.S. Traumatic Brain Injury Detection Using Electrophysiological Methods. Front. Hum. Neurosci. 2015, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Modarres, M.H.; Opel, R.A.; Weymann, K.B.; Lim, M.M. Strong correlation of novel sleep electroencephalography coherence markers with diagnosis and severity of posttraumatic stress disorder. Sci. Rep. 2019, 9, 4247. [Google Scholar] [CrossRef] [PubMed]
- Sutandi, A.; Dhillon, N.; Lim, M.; Cao, H.; Si, D. Detection of Traumatic Brain Injury Using Single Channel Electroencephalogram in Mice. In Proceedings of the 2020 IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 5 December 2020; Volume 16, pp. 1–8. [Google Scholar]
- Konstantinidis, E.; Conci, N.; Bamparopoulos, G.; Sidiropoulos, E.; De Natale, F.; Bamidis, P. Introducing Neuroberry, a Platform for Pervasive EEG Signaling in the IoT Domain. In Proceedings of the 5th EAI International Conference on Wireless Mobile Communication and Healthcare (MOBIHEALTH’15); ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering): Brussels, Belgium, 2015; pp. 166–169. [Google Scholar] [CrossRef]
- Arif, R.; Wijaya, S.; Prawito; Gani, H. Design of EEG Data Acquisition System Based on Raspberry Pi 3 for Acute Ischemic Stroke Identification. In Proceedings of the 2018 International Conference on Signals and Systems (ICSigSys), Bali, Indonesia, 1–3 May 2018; pp. 271–275. [Google Scholar] [CrossRef]
- Zgallai, W.; Brown, J.T.; Ibrahim, A.; Mahmood, F.; Mohammad, K.; Khalfan, M.; Mohammed, M.; Salem, M.; Hamood, N. Deep Learning AI Application to an EEG Driven BCI Smart Wheelchair. In Proceedings of the 2019 Advances in Science and Engineering Technology International Conferences (ASET), Dubai, United Arab Emirates, 26 March–10 April 2019; pp. 1–5. [Google Scholar] [CrossRef]
- Albert, B.; Zhang, J.; Noyvirt, A.; Setchi, R.; Sjaaheim, H.; Velikova, S.; Strisland, F. Automatic EEG Processing for the Early Diagnosis of Traumatic Brain Injury. In Proceedings of the 2016 World Automation Congress (WAC), Rio Grande, Puerto Rico, 31 July–4 August 2016. [Google Scholar]
- MCP3008—Analog to Digital Converters. Available online: https://www.microchip.com/wwwproducts/en/MCP3008 (accessed on 5 January 2021).
- MCP4725—Digital to Analog Converters. Available online: https://www.microchip.com/wwwproducts/en/MCP4725 (accessed on 6 January 2021).
- XGBoost Parameters Xgboost 1.4.0-SNAPSHOT Documentation. Available online: https://xgboost.readthedocs.io/en/latest/parameter.html (accessed on 21 March 2021).
- dmlc/xgboost. Available online: https://github.com/dmlc/xgboost (accessed on 22 March 2021).
- scipy.signal.welch. SciPy v1.6.1 Reference Guide. Available online: https://docs.scipy.org/doc/scipy/reference/generated/scipy.signal.welch.html#scipy.signal.welch (accessed on 22 March 2021).
- Cyton Biosensing Board (8-Channels). Available online: https://shop.openbci.com/products/cyton-biosensing-board-8-channel (accessed on 25 January 2021).
- brainHat: Raspberry Pi + OpenBCI = Plug and Play LSL. Available online: https://openbci.com/community/brainhat-raspberry-pi-openbci-plug-and-play-lsl/ (accessed on 25 January 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | PC | RPi | PC | RPi | PC | RPi |
|---|---|---|---|---|---|---|
| Epoch | 16 | 16 | 32 | 32 | 64 | 64 |
| Accuracy | 0.982 | 0.982 | 0.974 | 0.974 | 0.968 | 0.968 |
| Sham Wake | ||||||
| Precision | 0.972 | 0.972 | 0.981 | 0.981 | 0.981 | 0.981 |
| Recall | 0.986 | 0.986 | 0.986 | 0.986 | 0.982 | 0.982 |
| Sham Sleep | ||||||
| Precision | 0.973 | 0.973 | 0.951 | 0.951 | 0.937 | 0.937 |
| Recall | 0.951 | 0.951 | 0.945 | 0.945 | 0.948 | 0.948 |
| mTBI Wake | ||||||
| Precision | 0.989 | 0.989 | 0.961 | 0.961 | 0.951 | 0.951 |
| Recall | 0.990 | 0.990 | 0.961 | 0.961 | 0.934 | 0.934 |
| mTBI Sleep | ||||||
| Precision | 0.998 | 0.998 | 0.997 | 0.997 | 0.989 | 0.989 |
| Recall | 0.997 | 0.997 | 0.995 | 0.995 | 0.990 | 0.990 |
| Number of Epochs | Epoch Collection Time (s) | Epoch Processing Time (s) | Processing Time as % of Collection Time |
|---|---|---|---|
| 1 | 64 | 0.02 | 0.03% |
| 10 | 640 | 0.08 | 0.01% |
| 100 | 6400 | 0.6 | 0.01% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhillon, N.S.; Sutandi, A.; Vishwanath, M.; Lim, M.M.; Cao, H.; Si, D. A Raspberry Pi-Based Traumatic Brain Injury Detection System for Single-Channel Electroencephalogram. Sensors 2021, 21, 2779. https://doi.org/10.3390/s21082779
Dhillon NS, Sutandi A, Vishwanath M, Lim MM, Cao H, Si D. A Raspberry Pi-Based Traumatic Brain Injury Detection System for Single-Channel Electroencephalogram. Sensors. 2021; 21(8):2779. https://doi.org/10.3390/s21082779
Chicago/Turabian StyleDhillon, Navjodh Singh, Agustinus Sutandi, Manoj Vishwanath, Miranda M. Lim, Hung Cao, and Dong Si. 2021. "A Raspberry Pi-Based Traumatic Brain Injury Detection System for Single-Channel Electroencephalogram" Sensors 21, no. 8: 2779. https://doi.org/10.3390/s21082779
APA StyleDhillon, N. S., Sutandi, A., Vishwanath, M., Lim, M. M., Cao, H., & Si, D. (2021). A Raspberry Pi-Based Traumatic Brain Injury Detection System for Single-Channel Electroencephalogram. Sensors, 21(8), 2779. https://doi.org/10.3390/s21082779