
Effect of Brain and Pulse Waves on Safety Consciousness and Safety Commitment of Workers at Construction Sites


Abstract
1. Introduction
2. Theoretical Background
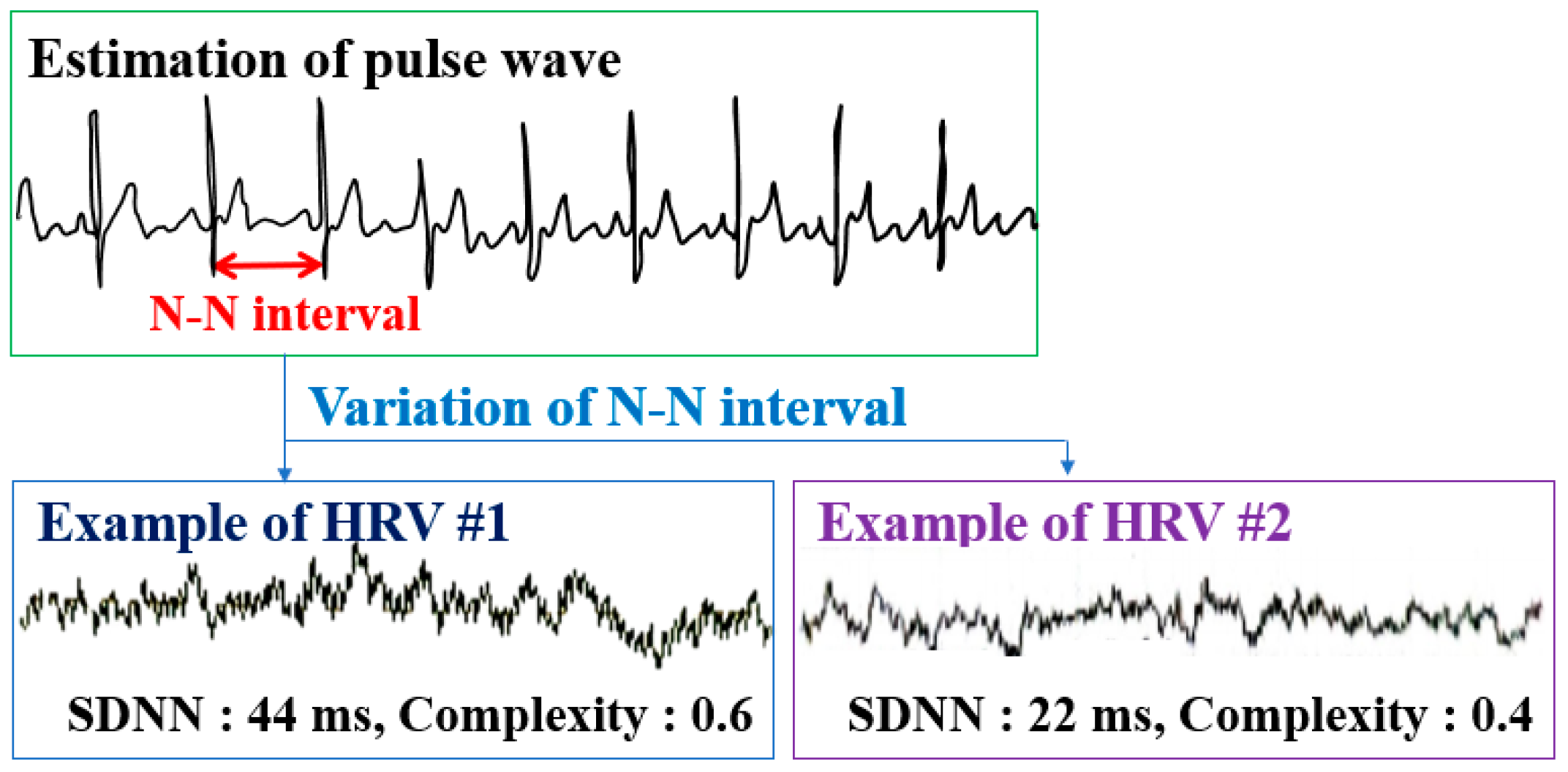
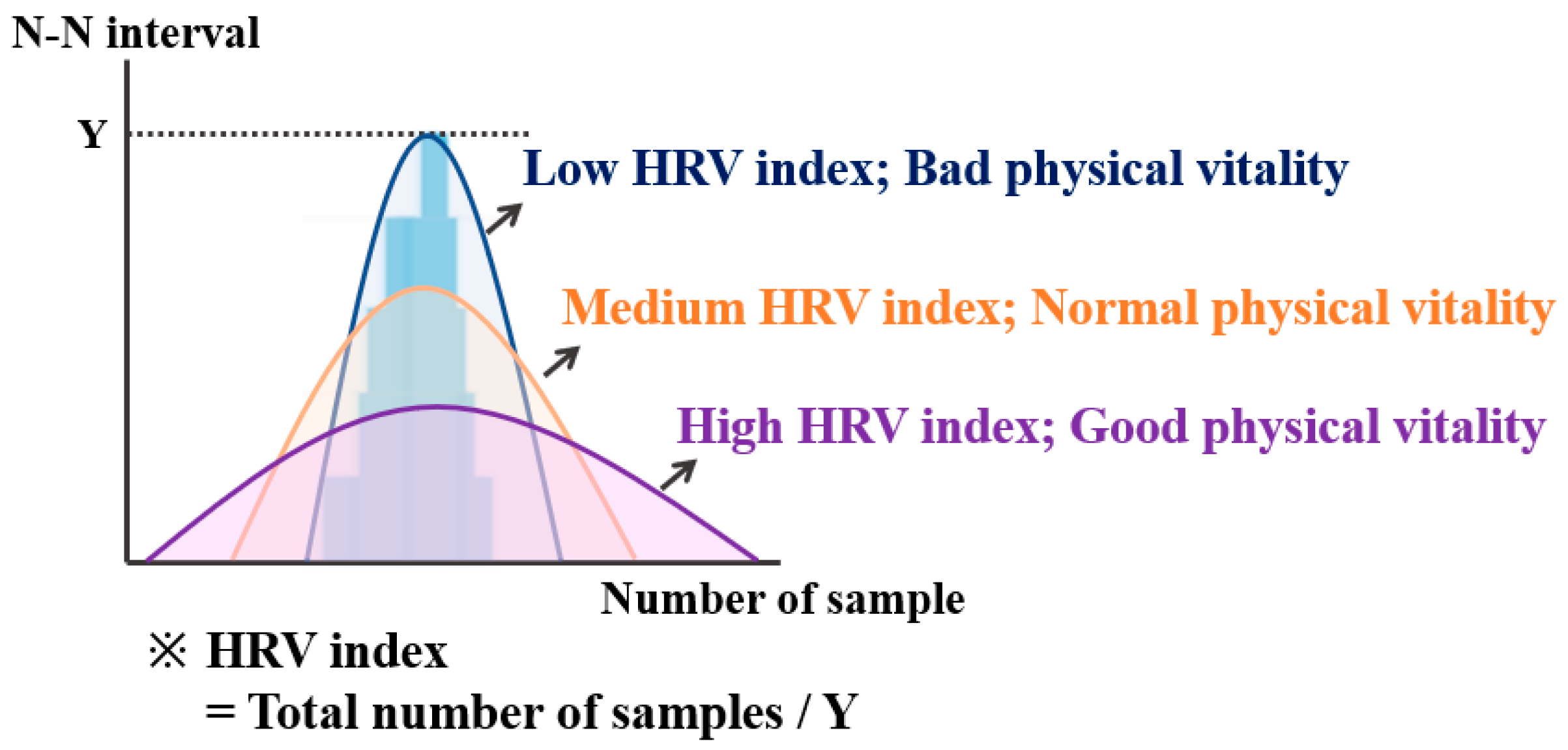
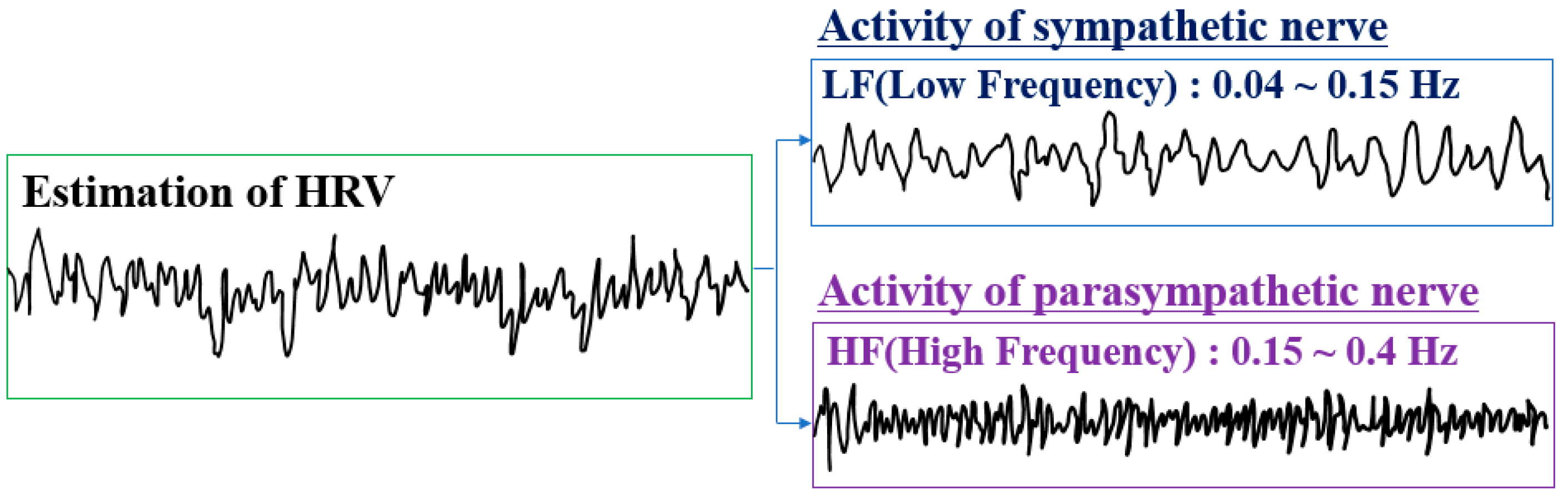
2.1. Analysis of Pulse Waves
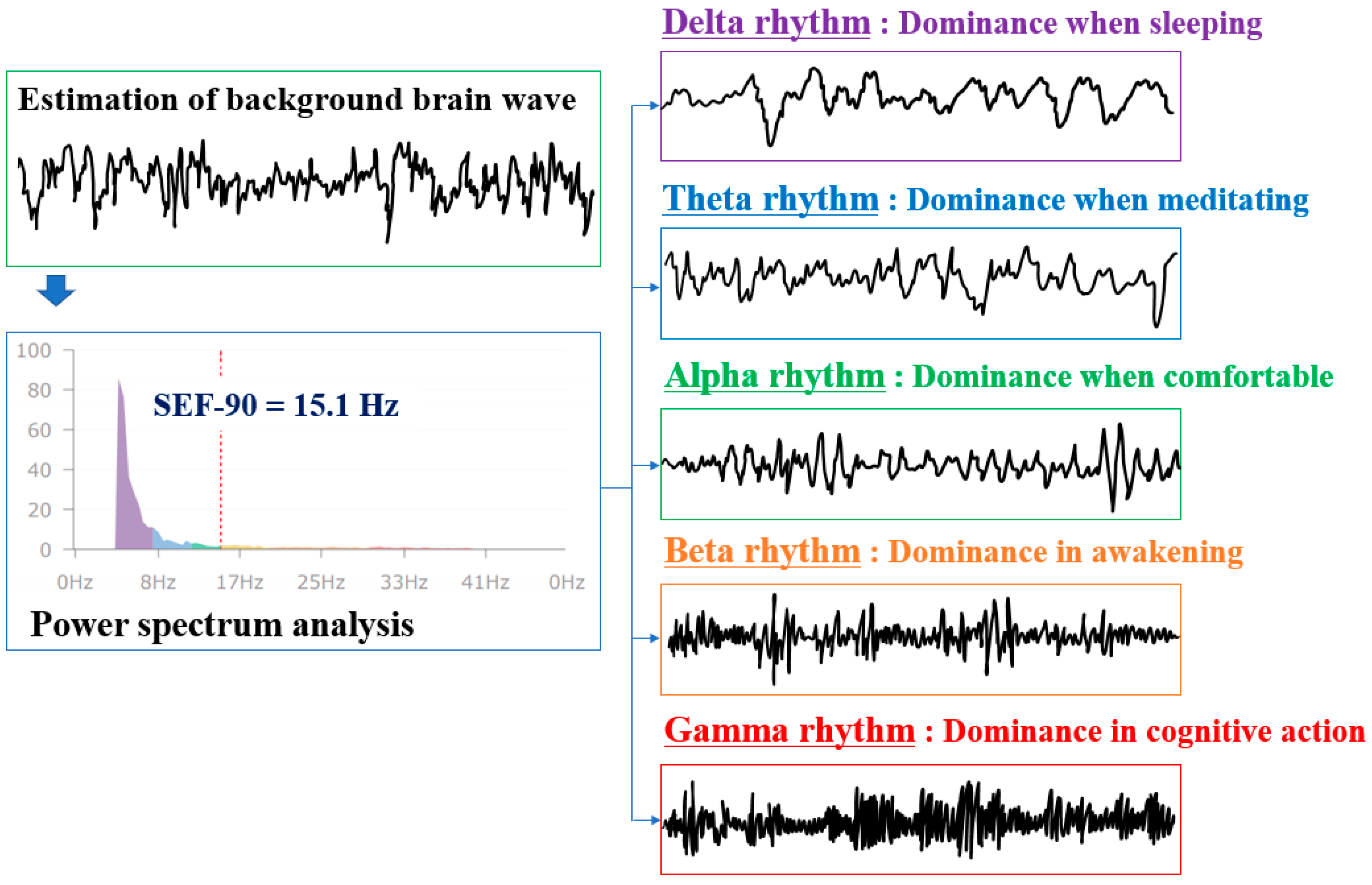
2.2. Analysis of Brain Waves
3. Research Method
3.1. Research Subjects and Bio-Signal Measurement Method
3.2. Safety Consciousness and Safety Commitment Determination through a Survey
4. Brain Waves and Brain Wave Analysis Results
4.1. Analysis of Difference in Safety Consciousness and Safety Commitment According to Brain Waves of Workers at Construction Sites
4.2. Analysis of Difference in Safety Consciousness and Safety Commitment According to Pulse Waves of Workers at Construction Sites
5. Discussion
6. Conclusions
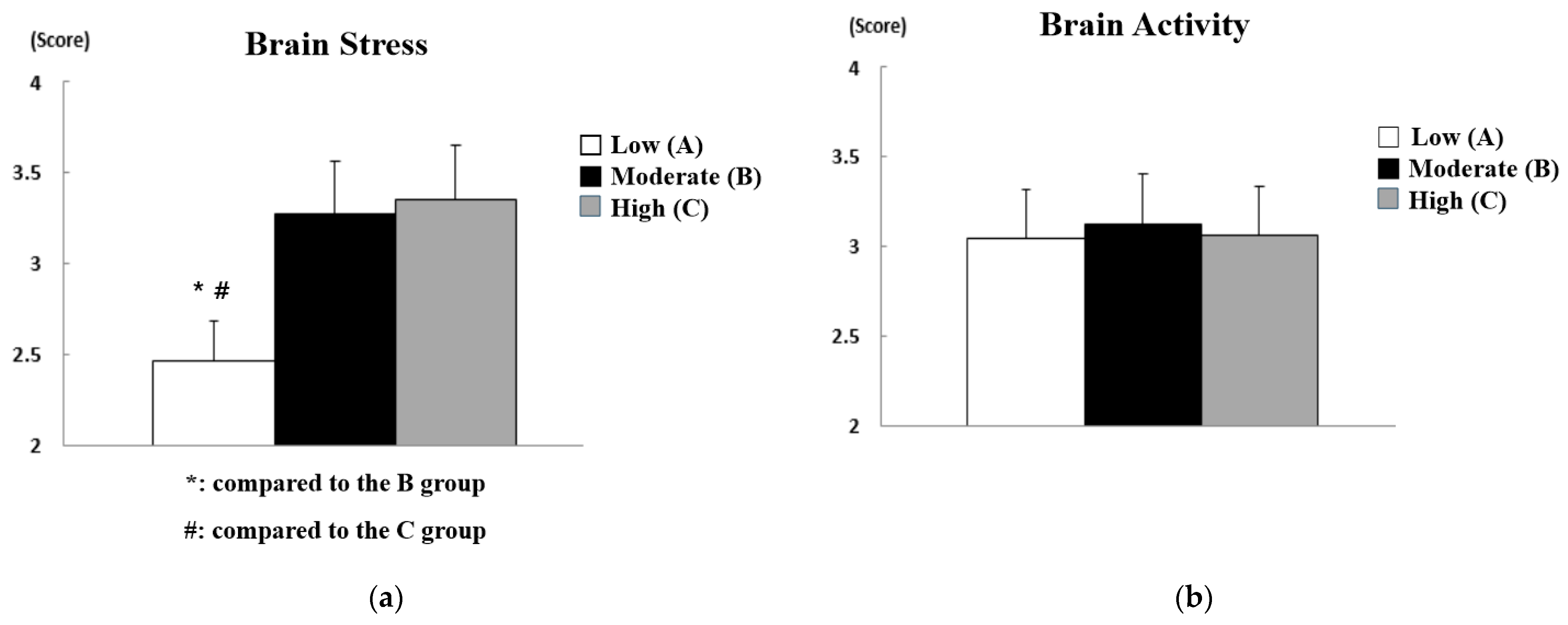
- First, as a result of analyzing the difference in the safety consciousness of workers at construction sites according to brain waves, the safety consciousness was higher when brain stress and concentration were higher. An appropriate level of stress is an essential factor in human growth that can play not only a dysfunctional role but also a functional role. In other words, it was found that a certain level of brain stress is required to have the safety consciousness to cope with construction site workers’ safety accidents. However, it was observed that the level of brain activity did not significantly affect the safety consciousness of workers at construction sites. On the other hand, more whole-brained workers had higher safety consciousness. The safety consciousness can be improved when the left and right brains interact without being biased to either side and form experiences through integrated processing because the two hemispheres of the brain share stimuli with each other through the corpus callosum and work as an integrated whole.
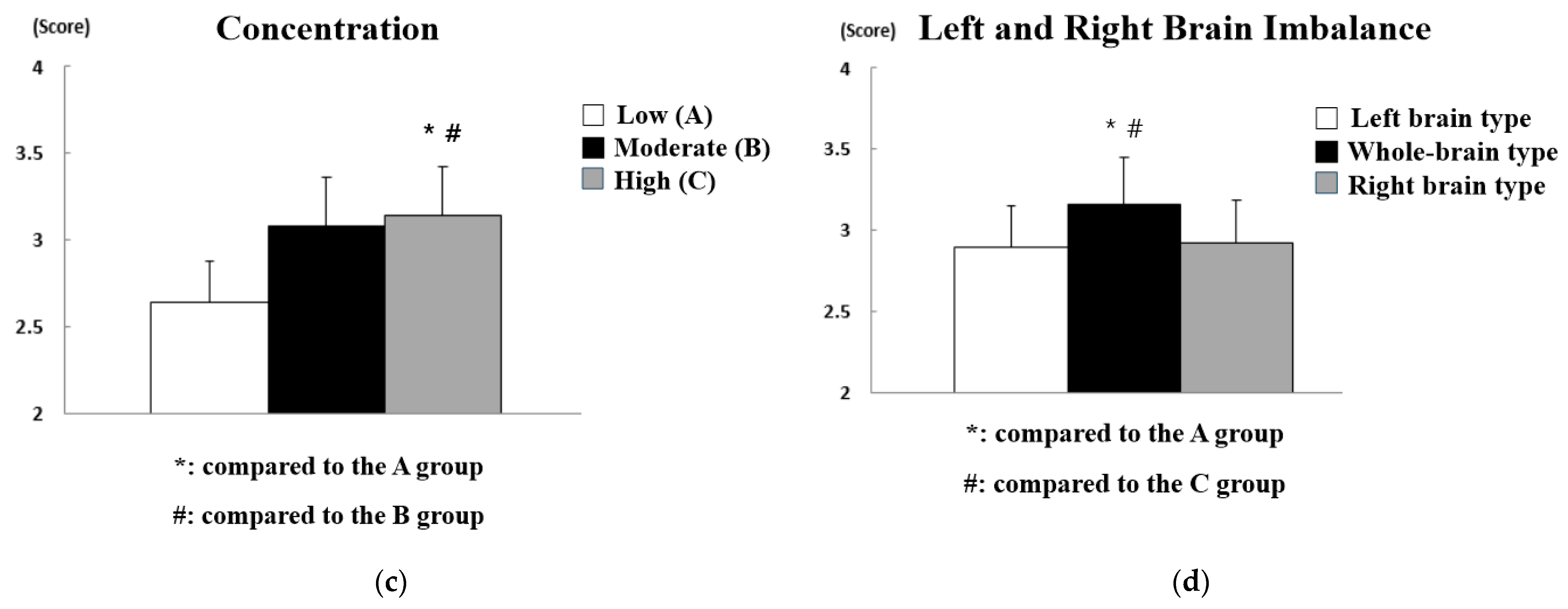
- As in safety consciousness, in terms of the safety commitment of workers at construction sites, according to brain waves, the safety commitment of whole-brain-type workers with high brain stress and concentration was observed to be higher. In particular, it was found that workers showed better safety commitment when the level of brain activity was higher, unlike in the case of safety consciousness. In other words, not only a certain level of brain stress but also the level of brain activity needs to be high to continuously maintain the behavior of preventing safety accidents within the organization through commitment. In addition, workers with low levels of brain activity work without correctly recognizing their fatigued physical state or negative emotional states such as stress, tension, and fear. If this condition persists, it may negatively affect the brain, leading to a decrease in brain stress and concentration.
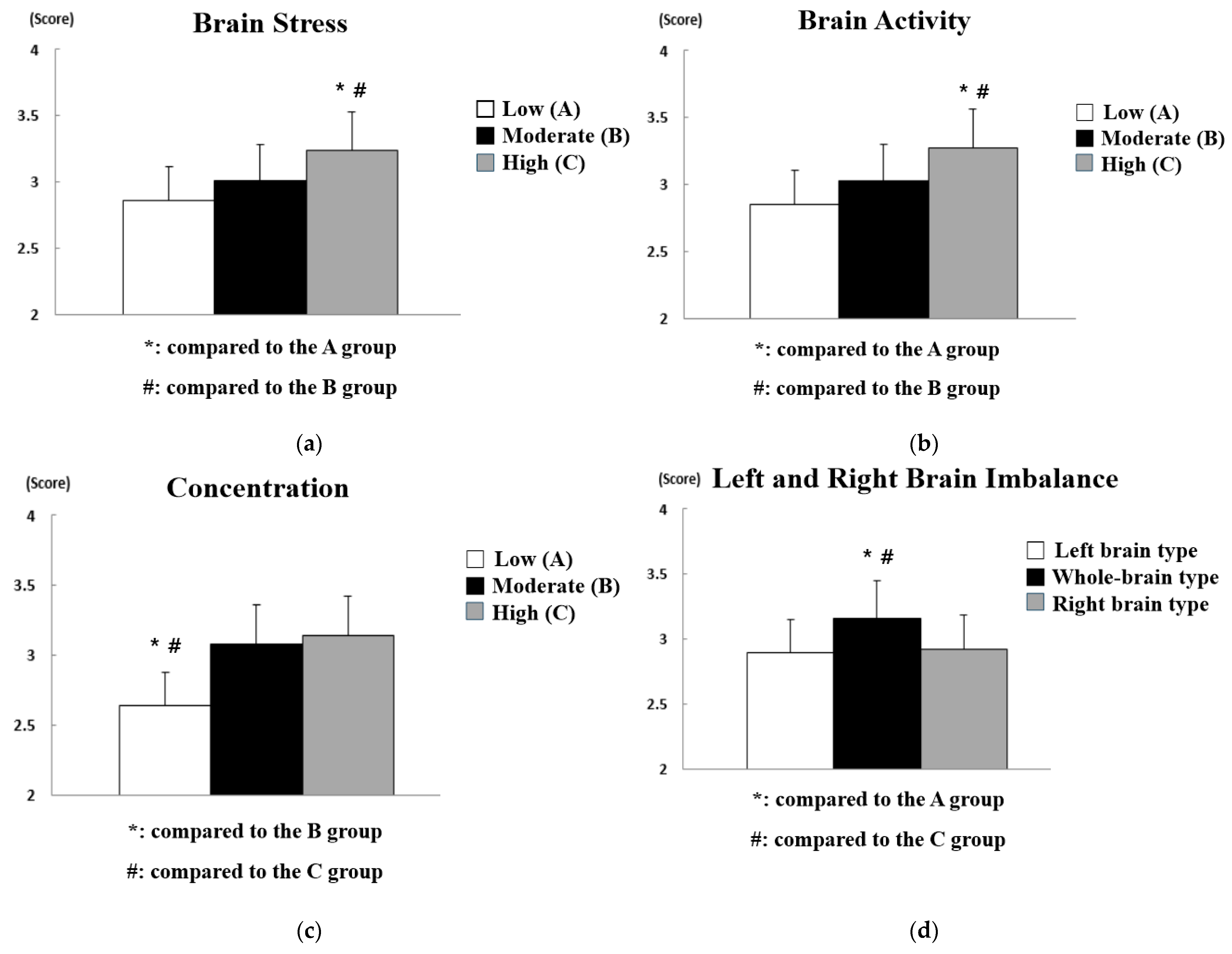
- According to the pulse wave, both safety consciousness and safety commitment were high when cumulative fatigue was normal and physical vitality was normal or high. In addition, both safety consciousness and safety commitment were high when the autonomic nerve was balanced. However, the health of the autonomic nerve was found to have a greater impact on safety consciousness than on safety commitment. If the stress due to internal and environmental changes persists in the body, humans cannot adequately respond to external stimuli due to cumulative fatigue and cannot maintain safety consciousness because the heart rate decreases due to the decreased ability to control stress. This phenomenon may be clearly observed as the autonomic nerve activation decreases.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministry of Employment and Labor. 2017 Industrial Accident Analysis; Korea Occupational Safety and Health Agency: Seoul, Korea, 2017. [Google Scholar]
- Lee, J.; Oh, S.; Moon, K. An effect of safety leadership coaching program on safety behaviors of construction workers: Based on behavior based safety. J. Korean Soc. Saf. 2018, 33, 115–122. [Google Scholar]
- Zhenhua, Z.; Park, M.-W.; Christian, K.; Mohamad, S.; Amin, H.; Khashayar, D. Predicting movements of onsite workers and mobile equipment for enhancing construction site safety. Autom. Constr. 2016, 68, 95–101. [Google Scholar]
- Lee, K. Enhancement of Safety and Health Education towards Improved Awareness of Construction Workers. Master’s Thesis, Graduate School of Engineering, Hanyang University, Seoul, Korea, 2020. [Google Scholar]
- Choudhry, R.M.; Fang, D.; Mohamed, S. Developing a model of construction safety culture. J. Manag. Eng. 2007, 23, 207–212. [Google Scholar] [CrossRef]
- Park, J. A study on the Impact of Emergency Work on Construction Site Safety Management—Focusing on Overseas Construction Sites. Master’s Thesis, Graduate School of Energy and Environment, Seoul National University of Science and Technology, Seoul, Korea, 2016. [Google Scholar]
- Jiang, Z.; Fang, D.; Zhang, M. Understanding the causation of construction workers’ unsafe behaviors based on system dynamics modeling. J. Manag. Eng. 2014, 31, 04014099. [Google Scholar] [CrossRef]
- Fang, D.; Zhao, C.; Zhang, M. A cognitive model of construction workers’ unsafe behaviors. J. Constr. Eng. Manag. 2016, 142, 04016039. [Google Scholar] [CrossRef]
- Woo, J. Proposal for Regulation of the Use of BBS Programs for Industrial Safety. Master’s Thesis, Graduate School, Hoseo University, Asan, Korea, 2019. [Google Scholar]
- Marland, S.K.; James, A.E.; Ralph, B.C.; John, E.R. Fundamentals of Safety Education, 2nd ed.; MacMillina Co: New York, NY, USA, 1973. [Google Scholar]
- Kim, K. The Effect of Airlines Safety Management System on Safety Perception and Safety Behavior. Ph.D. Thesis, Graduate School, Kyonggi University, Suwon, Korea, 2016. [Google Scholar]
- Kim, O.; Yoon, Y. The relationship between construction workers’ safety consciousness, organizational trust and turn-over intention. Korean J. Constr. Eng. Manag. 2020, 21, 65–75. [Google Scholar]
- Moon, K.; Lee, J.; Oh, S. The effect of organizational commitment on safety behaviors: Moderating effects of safety climate. Korean J. Ind. Organ. Psychol. 2011, 24, 51–73. [Google Scholar] [CrossRef]
- Kim, H. A Study on the Relationship between Corporate Safety Culture and Accidents: By Using the Parameter of Safety Behavior Immersion. Doctoral Thesis, Graduate School, Soongsil University, Seoul, Korea, 2019. [Google Scholar]
- Yoon, J. Improvement Measures of Safety & Health Education for Construction Disaster Reduction. Master’s Thesis, Graduate School, Hanbat University, Daejeon, Korea, 2017. [Google Scholar]
- Lim, U.; Park, Y. A grounded theoretical study on the experience of preventing safety accidents of workers at construction sites. J. Humanit. Soc. Sci. 2020, 21, 2099–2114. [Google Scholar]
- Pete, K.; Lars, P.S.; Soren, S.; Kim, L.M.; Johnny, D.; Dov, Z. Improving construction site safety through leader-based verbal safety communication. J. Saf. Res. 2010, 41, 399–406. [Google Scholar]
- Kim, S. A Study on Improving Safety Management through an Analysis of Construction Site Managers’ Perceptions. Ph.D. Thesis, Graduate School, Mokpo National University, Mokpo, Korea, 2017. [Google Scholar]
- Moon, Y. Influencing Factors of Sensibility Factor and Self-Esteem on Safe and Unsafe Behaviors. Master’s Thesis, Graduate School of Construction and Industry, Kyonggi University, Suwon, Korea, 2017. [Google Scholar]
- Lee, Y. Risk Analysis for Cardiovascular Disease in Small Construction Site Workers. Master’s Thesis, Graduate School, Seoul National University of Science and Technology, Seoul, Korea, 2017. [Google Scholar]
- Park, S. A Study on the Key Factors to Prevent Unsafe Behavior of Construction Workers. Master’s Thesis, Graduate School of Industry, Seoul National University of Science and Technology, Seoul, Korea, 2015. [Google Scholar]
- Lee, G.; Shin, J. Effects of the barefoot walking experience program on EEG and brain utilization ability of elementary school students. J. Learn. Cent. Curric. Instr. 2019, 19, 219–238. [Google Scholar] [CrossRef]
- Lee, M. Effects of Exercise Rehabilitation on Behavioral Change and Autonomic Nervous Function in Children with Autism Spectrum Disorder. Ph.D. Thesis, Graduate School, Sangmyung University, Seoul, Korea, 2015. [Google Scholar]
- Electrophysiology, Task Force of the European Society of Cardiology the North American Society of Pacing. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Corr, P.B. Mechanisms controlling cardiac autonomic function and their relation to arrhythmogenesis. In The Heart and Cardiovascular System; Raven Press: New York, NY, USA, 1986. [Google Scholar]
- Schwartz, P.J. Sympathetic nervous system and cardiac arrhythmia. Card. Electrophysiol. Cell Bedside 1990, 22, 330–343. [Google Scholar]
- Choi, B.; Roh, G. Heart rate variability (HRV). Korean J. Anesthesiol. 2004, 8, 45–86. [Google Scholar]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Berger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Pomeranz, B.; Macaulay, R.J.; Caudill, M.A.; Kutz, I.; Adam, D.; Gordon, D.; Kilborn, K.M.; Barger, A.C.; Shannon, D.C.; Cohen, R.J.; et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am. J. Physiol. Heart Circ. Physiol. 1985, 248, H151–H153. [Google Scholar] [CrossRef]
- Dreifus, L.S.; Agarwal, J.B.; Botvinick, E.H.; Ferdinand, K.C.; Fisch, C.; Fisher, J.D.; Kennedy, J.W.; Kerber, R.E.; Lambert, C.R.; Okike, O.N.; et al. Heart rate variability for risk stratification of life-threatening arrhythmias. J. Am. Coll. Cardiol. 1993, 22, 948–950. [Google Scholar] [CrossRef]
- Saul, J.P.; Rea, R.F.; Eckberg, D.L.; Berger, R.D.; Cohen, R.J. Heart rate and muscle sympathetic nerve variability during reflex changes of autonomic activity. Am. J. Physiol. Heart Circ. Physiol. 1990, 258, H713–H721. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Bigger, J.T.; Bosner, M.S.; Chung, M.K.; Cook, J.R.; Rolnitzky, L.M.; Steinman, R.; Fleiss, J.L. Stability over time of variables measuring heart rate variability in normal subjects. Am. J. Cardiol. 1991, 68, 626–630. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr.; Fleiss, J.L.; Rolnitzky, L.M.; Steinman, R.C. Stability over time of heart period variability in patients with previous myocardial infarction and ventricular arrhythmias. Am. J. Cardiol. 1992, 69, 718–723. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Schneider, W.J.; Stein, P.K. RR variability in healthy, middle-aged persons compared with patients with chronic coronary heart disease or recent acute myocardial infarction. Circulation 1995, 91, 1936–1943. [Google Scholar] [CrossRef]
- Langewitz, W.; Rüddel, H.; Schächinger, H. Reduced parasympathetic cardiac control in patients with hypertension at rest and under mental stress. Am. Heart J. 1994, 127, 122–128. [Google Scholar] [CrossRef]
- Bigger, J.T.; Fleiss, J.L.; Rolnitzky, L.M.; Steinman, R.C. Frequency domain measures of heart period variability to assess risk late after myocardial infarction. J. Am. Coll. Cardiol. 1993, 21, 729–736. [Google Scholar] [CrossRef]
- Rodriguez, E.; George, N.; Lachaux, J.P.; Martinerie, J.; Renault, B.; Varela, F.J. Perception’s shadow: Long-distance synchronization of human brain activity. Nature 1999, 397, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Hillyard, S.A.; Anllo-Vento, L. Event-related brain potentials in the study of visual selective attention. Proc. Natl. Acad. Sci. USA 1998, 95, 781–787. [Google Scholar] [CrossRef]
- Cowan, J.; Allen, T. Using brainwave biofeedback to train the sequence of concentration and relaxation in athletic activities. In Proceedings of the 15th Association for the Advancement of Applied Sport Psychology, Nashville, TN, USA, 18–21 October 2000; p. 95. [Google Scholar]
- König, T.; Prichep, L.; Dierks, T.; Hubl, D.; Wahlund, L.O.; John, E.R.; Jelic, V. Decreased EEG synchronization in Alzheimer’s disease and mild cognitive impairment. Neurobiol. Aging 2005, 26, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Prichep, L.S.; John, E.R.; Ferris, S.H.; Rausch, L.; Fang, Z.; Cancro, R.; Torossian, C.; Reisberg, B. Prediction of longitudinal cognitive decline in normal elderly with subjective complaints using electrophysiological imaging. Neurobiol. Aging 2006, 27, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Kopell, N.; Ermentrout, G.B.; Whittington, M.A.; Traub, R.D. Gamma rhythms and beta rhythms have different synchronization properties. Proc. Natl. Acad. Sci. USA 2000, 97, 1867–1872. [Google Scholar] [CrossRef]
- Karakaş, S.; Bekçi, B.; Erzengin, Ö.U. Early gamma response in human neuroelectric activity is correlated with neuropsychological test scores. Neurosci. Lett. 2003, 340, 37–40. [Google Scholar] [CrossRef]
- Ryu, K.; Myung, R. Evaluation of mental workload with a combined measure based on physiological indices during a dual task of tracking and mental arithmetic. Int. J. Ind. Ergon. 2005, 35, 991–1009. [Google Scholar] [CrossRef]
- Boksem, M.A.; Meijman, T.F.; Lorist, M.M. Effects of mental fatigue on attention: An ERP study. Cogn. Brain Res. 2005, 25, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Murata, A.; Uetake, A.; Takasawa, Y. Evaluation of mental fatigue using feature parameter extracted from event-related potential. Int. J. Ind. Ergon. 2005, 35, 761–770. [Google Scholar] [CrossRef]
- Ergen, M.; Marbach, S.; Brand, A.; Başar-Eroğlu, C.; Demiralp, T. P3 and delta band responses in visual oddball paradigm in schizophrenia. Neurosci. Lett. 2008, 440, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhapillai, A.; Tang, Y.; Ranganathan, M.; Rangaswamy, M.; Jones, K.A.; Chorlian, D.B.; Kamarajan, C.; Stimus, A.; Kuperman, S.; Rohrbaugh, J.; et al. Evoked gamma band response in male adolescent subjects at high risk for alcoholism during a visual oddball task. Int. J. Psychophysiol. 2006, 62, 262–271. [Google Scholar] [CrossRef]
- Maurage, P.; Philippot, P.; Verbanck, P.; Noel, X.; Kornreich, C.; Hanak, C.; Campanella, S. Is the P300 deficit in alcoholism associated with early visual impairments (P100, N170)? An oddball paradigm. Clin. Neurophysiol. 2007, 118, 633–644. [Google Scholar] [CrossRef]
- Başar-Eroglu, C.; Strüber, D.; Kruse, P.; Başar, E.; Stadler, M. Frontal gamma-band enhancement during multistable visual perception. Int. J. Psychophysiol. 1996, 24, 113–125. [Google Scholar] [CrossRef]
- Lindgren, K.A.; Larson, C.L.; Schaefer, S.M.; Abercrombie, H.C.; Ward, R.T.; Oakes, T.R.; Holden, J.E.; Perlman, S.B.; Benca, R.M.; Davidson, R.J. Thalamic metabolic rate predicts EEG alpha power in healthy control subjects but not in depressed patients. Biol. Psychiatry 1999, 45, 943–952. [Google Scholar] [CrossRef]
- Kim, J.; Choi, K. The effect of forest experience program on brain waves & pulse waves. J. Korea Entertain. Ind. Assoc. 2019, 13, 185–194. [Google Scholar]
- Kim, G.; Min, J. Effects of elastic taping on the variation of brain and pulse waves in walking exercise. Korea J. Sport 2020, 18, 681–687. [Google Scholar] [CrossRef]
- Kim, B.; Lee, J.; Lee, S.; Kwon, H.; Kwon, Y.; Park, Y.; Chae, B. The relationship study between cumulative fatigue and stress of seafarers by evaluating autonomic nervous functions and survey studies. J. Korean Soc. Integr. Med. 2018, 6, 1–13. [Google Scholar]
- Porges, S.W. Vagal tone: A physiologic markers of stress vulnerability. Pediatrics 1992, 90, 498–504. [Google Scholar]
- Laxtha Co. Brain Wave Data Equivalence Evaluation of Neuronicle FX2; Laxtha Co.: Daejeon, Korea, 2018. [Google Scholar]
- Ryu, H. A Study on the Effects of Safety Climate and Safety Consciousness Level in Construction Site on Workers’ Safety Behaviors. Master’s Thesis, Seoul National University of Science and Technology, Seoul, Korea, 2017. [Google Scholar]
- Kim, J. Development and Validation of Safety Commitment Scale. Ph.D. Thesis, Graduate School, The Catholic University of Korea, Bucheon, Korea, 2019. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Kim, G.S. Clinical study for statistical standardization of quantitative EEG and PTG parameters based on healthy volunteers. In Proceedings of the Korean Society for Emotion and Sensibility Conference, Jeju, Korea, 22 May 2009; Volume 2009, p. 15. [Google Scholar]
- Lomax, R.G. Statistical Concepts: A Second Course, 3rd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2007. [Google Scholar]
- Scheffe, H. The Analysis of Variance; John Wiley & Sons: Chichester, UK, 1999. [Google Scholar]
- Qu, M. The Effect of Self-Regulation and Stress by Brain Wave Training on Height Growth. Master’s Thesis, Graduate School, Seokyeong University, Seoul, Korea, 2019. [Google Scholar]
- Kang, B. Neuroscience: Exploring the Brain; Biomedbook: Seoul, Korea, 2018. [Google Scholar]
- Shin, D. The Structural Analysis between Safety Factors Having an Effect on the Construction Workers’ Behavior. Master’s Thesis, Graduate School, Kyungpook National University, Daegu, Korea, 2013. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Information | n1 | Ratio |
|---|---|---|---|
| Age | Aged in their 20s | 8 | 4.44% |
| Aged in their 30s | 29 | 16.11% | |
| Aged in their 40s | 45 | 25.00% | |
| Aged over 50 | 98 | 54.44% | |
| Gender | Male | 172 | 95.56% |
| Female | 8 | 4.44% | |
| Career | Less than 5 years | 28 | 15.56% |
| 5–10 years | 39 | 21.67% | |
| 10–15 years | 53 | 29.44% | |
| More than 15 years | 60 | 33.33% |
| Variable | Grade | n1 |
|---|---|---|
| Brain stress | Low (A) | 52 |
| Moderate (B) | 83 | |
| High (C) | 45 | |
| Brain activity | Low (A) | 34 |
| Moderate (B) | 108 | |
| High (C) | 38 | |
| Concentration | Low (A) | 46 |
| Moderate (B) | 94 | |
| High (C) | 40 | |
| Left and right brain imbalance | Left-brain type (A) | 42 |
| Whole-brain type (B) | 98 | |
| Right-brain type (C) | 40 |
| Variable | Grade | n1 |
|---|---|---|
| Cumulative fatigue | Normal (A) | 45 |
| Caution (B) | 82 | |
| Dangerous (C) | 53 | |
| Physical vitality | Low (A) | 40 |
| Moderate (B) | 99 | |
| High (C) | 41 | |
| Autonomic balance | Dominant sympathetic nervous system (A) | 38 |
| Balanced (B) | 101 | |
| Dominant parasympathetic nervous system (C) | 41 | |
| Autonomic nerve health | At risk (A) | 43 |
| Moderate (B) | 97 | |
| Healthy (C) | 40 |
| Item | No. | Questionnaire | Cronbach’s α |
|---|---|---|---|
| Safety consciousness | 1 | I think the safety rules of the workplace must be complied with. | 0.863 |
| 2 | I think accidents can happen at any time during work. | ||
| 3 | I think safety needs to be taught before working. | ||
| 4 | I have a fear of accidents. | ||
| 5 | I think safety comes first over progress of process. | ||
| 6 | Safety accidents can be prevented only when all workers are careful. | ||
| 7 | I’m more conscious of safety than other workers. | ||
| Safety commitment | 1 | I know the methods to cope with safety accidents. | 0.894 |
| 2 | I know the safety regulations and procedures of the workplace. | ||
| 3 | I’m familiar with the risk factors of accidents on work machines and facilities. | ||
| 4 | I know the protective equipment required for the job. | ||
| 5 | I have a steady interest in preventing safety accidents. | ||
| 6 | I know the safety hazards in the workplace. | ||
| 7 | A moment of inattention can lead to an accident. | ||
| 8 | Minor carelessness can lead to safety accidents. | ||
| 9 | Safety accidents can happen at any time. | ||
| 10 | It is everyone’s duty to comply with safety regulations and procedures. | ||
| 11 | Safety is connected to my life. | ||
| 12 | There is a high possibility of a safety accident if safety regulations and procedures are not complied with. | ||
| 13 | I comply to the procedure for any job. | ||
| 14 | I do not enter hazardous areas. | ||
| 15 | I do not ignore even the slightest risk factors. | ||
| 16 | I’m not overconfident in my skills. | ||
| 17 | It’s more important to work safely than to get jobs done quickly. |
| Variable | Grade | n | M 1 | SD 2 | p-Value | Post Hoc Analysis |
|---|---|---|---|---|---|---|
| Brain stress | Low (A) | 52 | 2.46 | 0.874 | 0.004 | A < B A < C |
| Moderate (B) | 83 | 3.27 | 0.563 | |||
| High (C) | 45 | 3.35 | 0.662 | |||
| Brain activity | Low (A) | 34 | 3.04 | 0.598 | 0.104 | - |
| Moderate (B) | 108 | 3.12 | 0.646 | |||
| High (C) | 38 | 3.06 | 0.642 | |||
| Concentration | Low (A) | 46 | 2.78 | 0.732 | 0.002 | A < C B < C |
| Moderate (B) | 94 | 2.80 | 0.578 | |||
| High (C) | 40 | 3.45 | 0.689 | |||
| Left and right brain imbalance | Left-brain type (A) | 42 | 2.90 | 0.650 | 0.024 | A < B C < B |
| Whole-brain type (B) | 98 | 3.24 | 0.568 | |||
| Right-brain type (C) | 40 | 2.97 | 0.683 |
| Variable | Grade | n | M 1 | SD 2 | p-Value | Post Hoc Analysis |
|---|---|---|---|---|---|---|
| Brain stress | Low (A) | 52 | 2.86 | 0.835 | 0.005 | A < C B < C |
| Moderate (B) | 83 | 3.01 | 0.535 | |||
| High (C) | 45 | 3.24 | 0.658 | |||
| Brain activity | Low (A) | 34 | 2.85 | 0.578 | 0.006 | A < C B < C |
| Moderate (B) | 108 | 3.03 | 0.636 | |||
| High (C) | 38 | 3.27 | 0.637 | |||
| Concentration | Low (A) | 46 | 2.64 | 0.732 | 0.003 | A < B A < C |
| Moderate (B) | 94 | 3.08 | 0.578 | |||
| High (C) | 40 | 3.14 | 0.689 | |||
| Left and right brain imbalance | Left-brain type (A) | 42 | 2.89 | 0.783 | 0.032 | A < B C < B |
| Whole-brain type (B) | 98 | 3.16 | 0.683 | |||
| Right-brain type (C) | 40 | 2.92 | 0.649 |
| Variable | Grade | n | M 1 | SD 2 | p-Value | Post Hoc Analysis |
|---|---|---|---|---|---|---|
| Cumulative Fatigue | Normal (A) | 45 | 3.43 | 0.674 | 0.001 | B < A C < A |
| Caution (B) | 82 | 3.02 | 0.536 | |||
| Dangerous (C) | 53 | 2.67 | 0.635 | |||
| Physical vitality | Low (A) | 40 | 2.78 | 0.542 | 0.027 | A < B A < C |
| Moderate (B) | 99 | 3.22 | 0.629 | |||
| High (C) | 41 | 3.34 | 0.625 | |||
| Autonomic balance | Dominant sympathetic (A) | 38 | 3.02 | 0.742 | 0.007 | C < A C < B |
| Balanced (B) | 101 | 3.14 | 0.526 | |||
| Dominant parasympathetic (C) | 41 | 2.87 | 0.627 | |||
| Autonomic nerve health | At risk (A) | 43 | 2.86 | 0.638 | 0.029 | A < B A < C |
| Moderate (B) | 97 | 3.01 | 0.537 | |||
| Healthy (C) | 40 | 3.23 | 0.627 |
| Variable | Grade | n | M 1 | SD 2 | p-Value | Post Hoc Analysis |
|---|---|---|---|---|---|---|
| Cumulative Fatigue | Normal (A) | 45 | 3.24 | 0.455 | 0.003 | C < A C < B |
| Caution (B) | 82 | 3.12 | 0.532 | |||
| Dangerous (C) | 53 | 2.79 | 0.636 | |||
| Physical vitality | Low (A) | 40 | 2.78 | 0.578 | 0.006 | A < C B < C |
| Moderate (B) | 99 | 3.02 | 0.628 | |||
| High (C) | 41 | 3.23 | 0.638 | |||
| Autonomic balance | Dominant sympathetic (A) | 38 | 2.84 | 0.683 | 0.001 | C < A C < B |
| Balanced (B) | 101 | 3.34 | 0.527 | |||
| Dominant parasympathetic (C) | 41 | 2.89 | 0.680 | |||
| Autonomic nerve health | At risk (A) | 43 | 3.02 | 0.630 | 0.085 | - |
| Moderate (B) | 97 | 3.04 | 0.563 | |||
| Healthy (C) | 40 | 3.10 | 0.620 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.-J.; Lim, U.-N.; Park, S.; Shin, J.-H. Effect of Brain and Pulse Waves on Safety Consciousness and Safety Commitment of Workers at Construction Sites. Sensors 2021, 21, 2753. https://doi.org/10.3390/s21082753
Park Y-J, Lim U-N, Park S, Shin J-H. Effect of Brain and Pulse Waves on Safety Consciousness and Safety Commitment of Workers at Construction Sites. Sensors. 2021; 21(8):2753. https://doi.org/10.3390/s21082753
Chicago/Turabian StylePark, Young-Jun, Un-Na Lim, Sangwoo Park, and Jae-Han Shin. 2021. "Effect of Brain and Pulse Waves on Safety Consciousness and Safety Commitment of Workers at Construction Sites" Sensors 21, no. 8: 2753. https://doi.org/10.3390/s21082753
APA StylePark, Y.-J., Lim, U.-N., Park, S., & Shin, J.-H. (2021). Effect of Brain and Pulse Waves on Safety Consciousness and Safety Commitment of Workers at Construction Sites. Sensors, 21(8), 2753. https://doi.org/10.3390/s21082753