
Human Body Performance with COVID-19 Affectation According to Virus Specification Based on Biosensor Techniques


 , , and
, , and 
Abstract
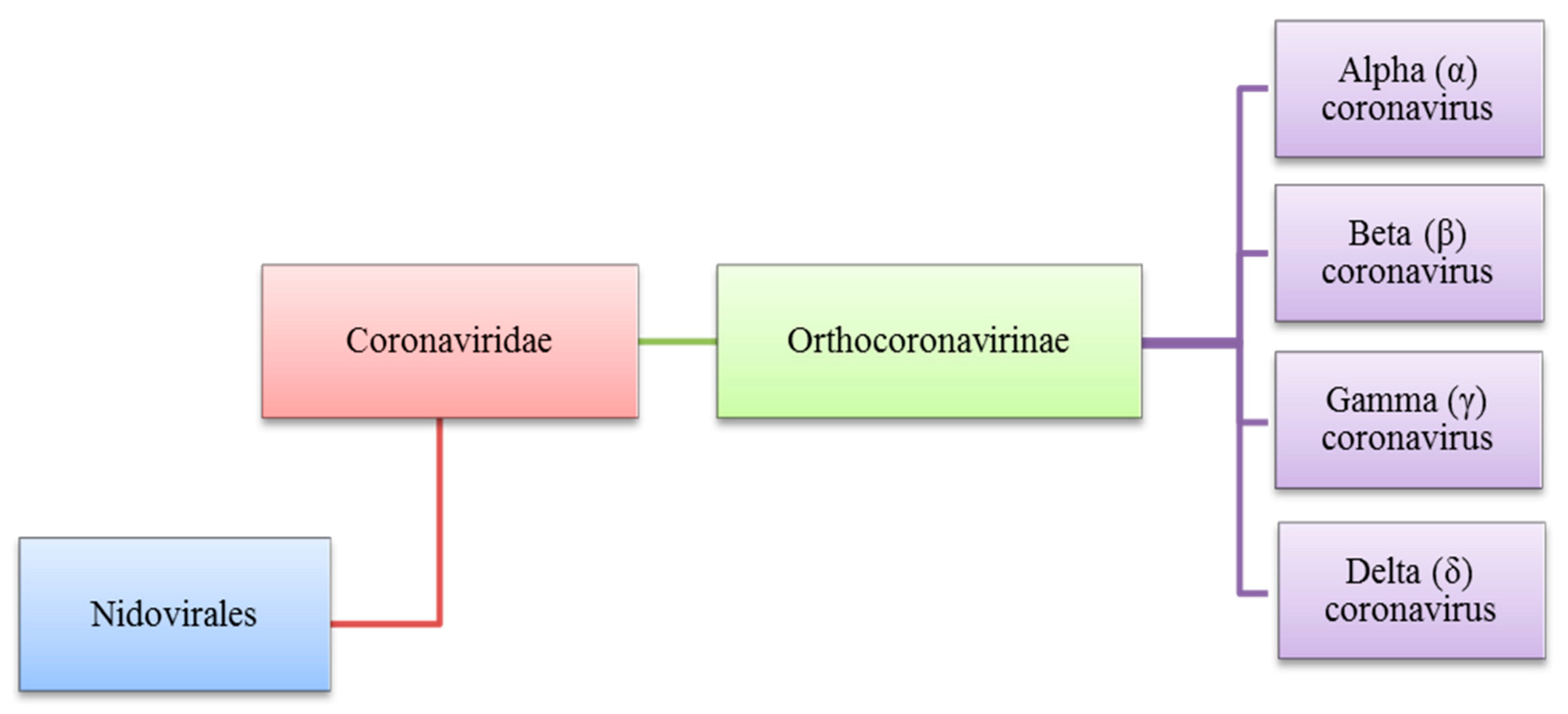
:1. Introduction and Overview of Coronaviruses:
1.1. Coronaviruses That Infect the Human Body Respiratory System
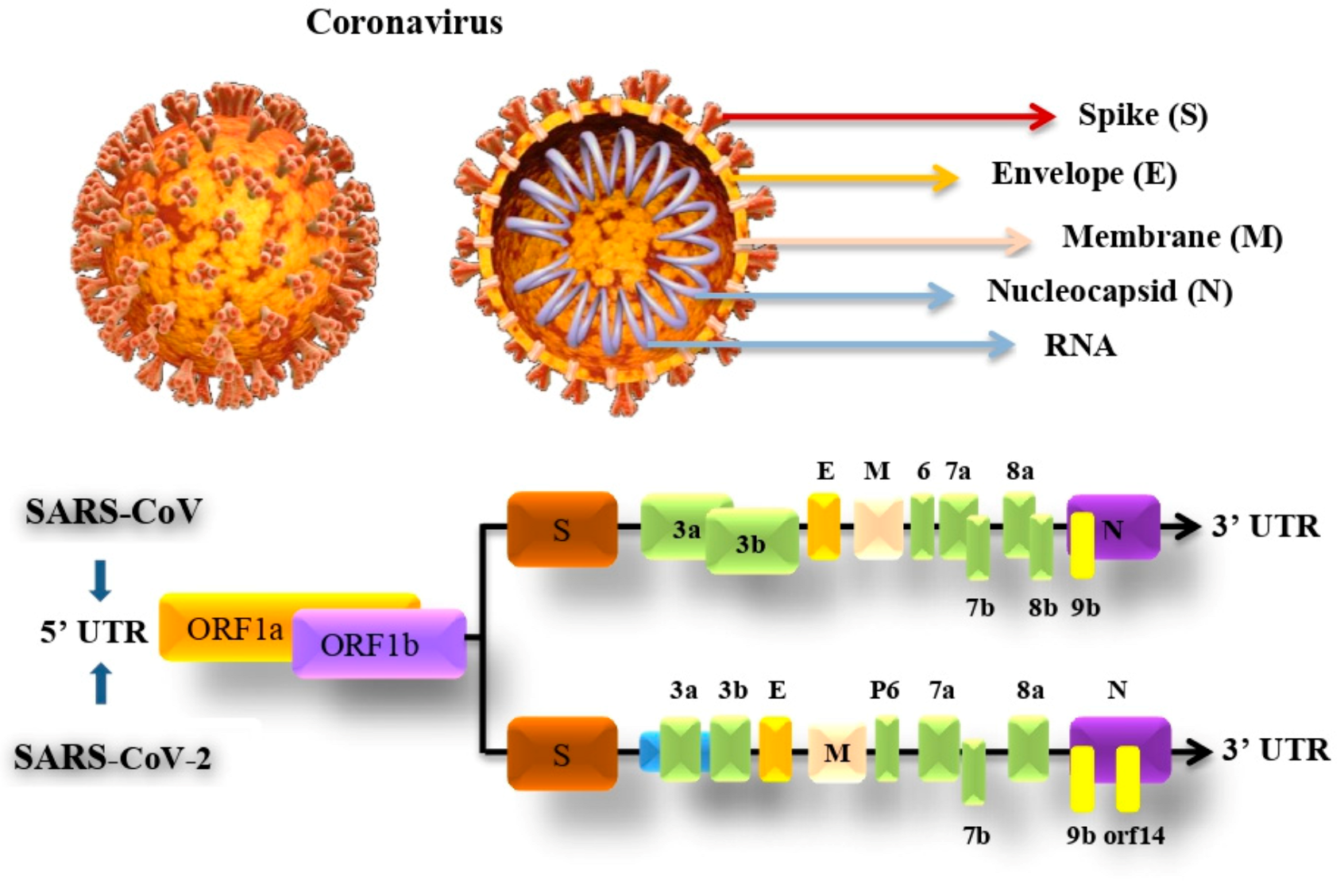
1.2. SARS-CoV and SARS-CoV-2 Genomic Structure and Proteins
2. Background of COVID-19 Virus Detection
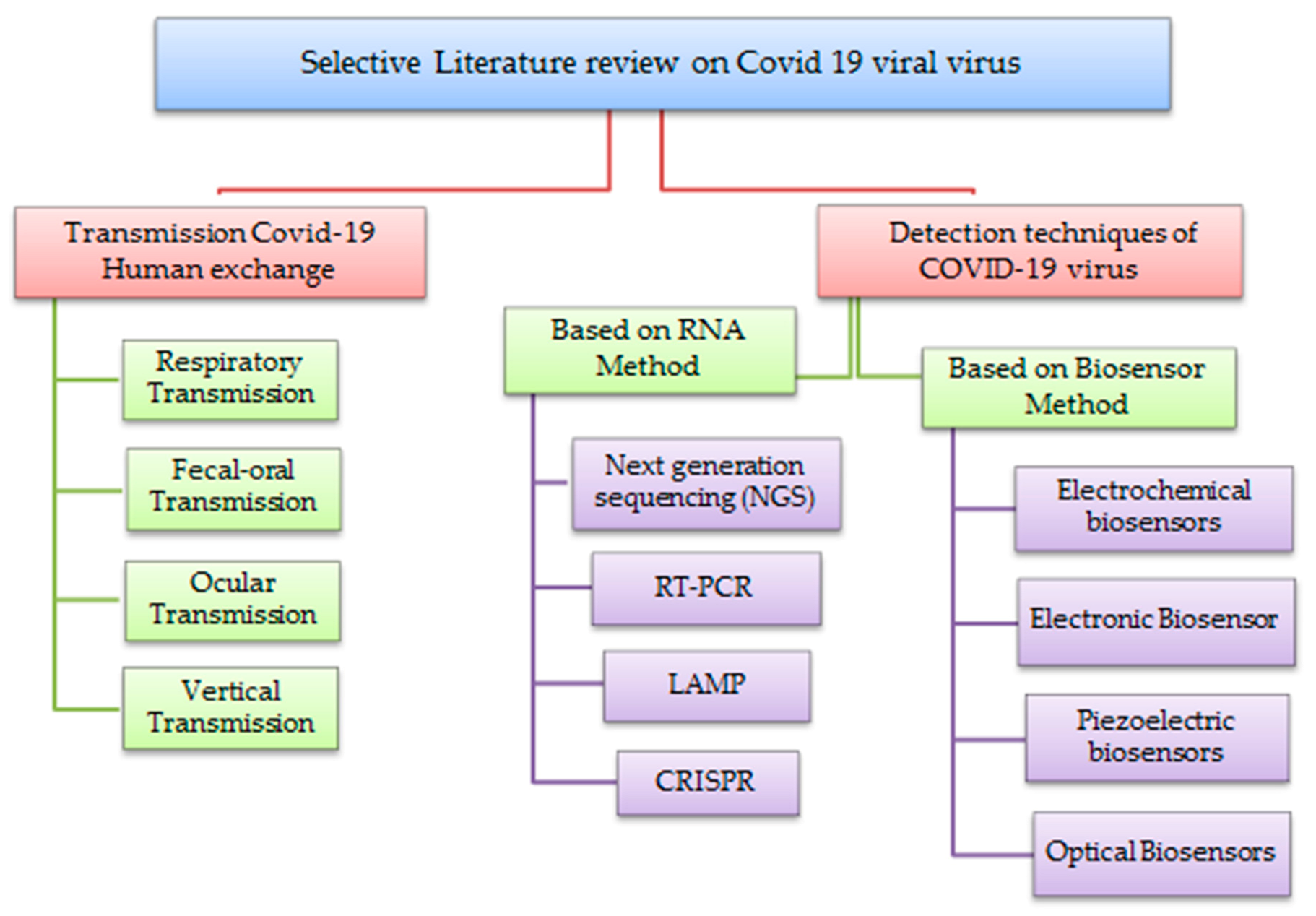
3. Taxonomy of Literature Reviews on COVID-19 Viral Virus
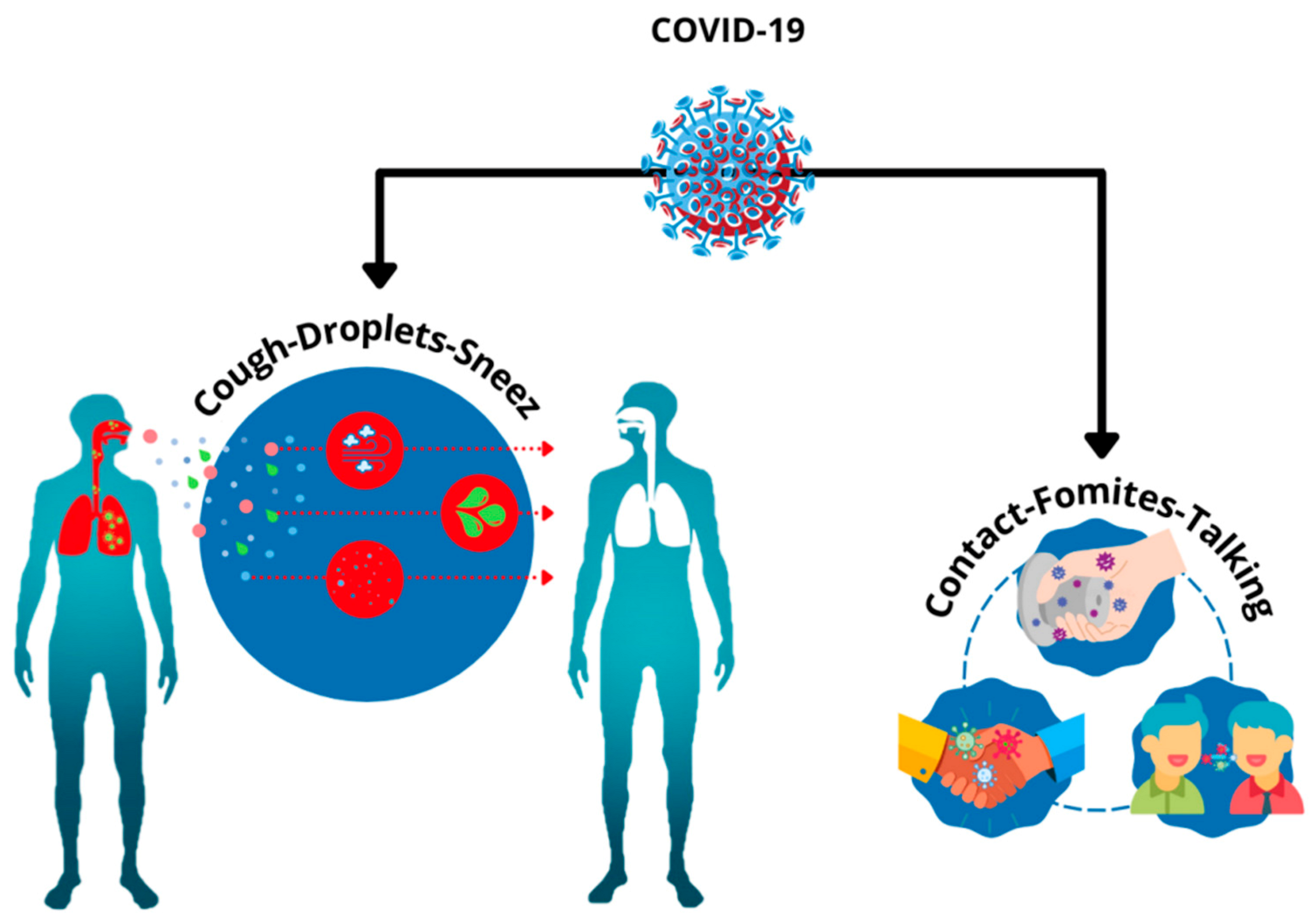
4. Transmission COVID-19 Human Exchange
4.1. Respiratory Transmission
4.2. Fecal–Oral Transmission
4.3. Ocular Transmission
4.4. Vertical Transmission
5. Comparison for Transmission COVID-19 Human Exchange
6. Detection Techniques of COVID-19 Virus
6.1. Based on Ribonucleic Acid (RNA) Method
6.1.1. Next-Generation Sequencing (NGS)
6.1.2. Reverse Transcription-Polymerase Chain Reaction (RT-PCR)
6.1.3. Loop-Mediated Isothermal Amplification (LAMP)
6.1.4. Clusters of Regularly Interspaced Short Palindromic Repeats (CRISPR)
6.1.5. RNA Corona Virus Detection Methods Analysis Based on RT-PCR, LAMP, and CRISPR
6.2. Based on Biosensor Techniques
6.2.1. Electrochemical Biosensors
6.2.2. Electronic Biosensors
6.2.3. Piezoelectric Biosensors
6.2.4. Optical Biosensors
7. Coronavirus Detection Methods Analysis Based on Biosensor Usage
8. COVID-19 Detection Techniques Advantages and Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Description |
| AuNPs | Gold nanoparticles |
| COVID-19 | Coronavirus disease |
| DNA | Deoxyribonucleic acid |
| EWA | Evanescent Wave Absorbance |
| FET | Field-effect transistor |
| GOF | Glass optical fiber |
| LAMP | Loop-mediated isothermal amplification |
| LSPCF | Localized surface plasmon coupled fluorescence |
| MERS-CoV | Middle East Respiratory Syndrome |
| NGS | Next-generation sequencing |
| PFAB | Plasmonic fiber-optic absorbance biosensor |
| RNA | Ribonucleic Acid |
| CRISPR | Clusters of regularly interspaced short palindromic repeats |
| RT-PCR | Reverse Transcription-Polymerase Chain Reaction |
| SARS-CoV | Coronavirus Severe Acute Respiratory Syndrome |
| SARS-CoV-2 | Coronavirus Severe Acute Respiratory Syndrome 2 |
| SPR | Surface plasmon resonance |
References
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Qianyun, L.; Deyin, G. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91. [Google Scholar] [PubMed]
- Estola, T. Coronaviruses, a new group of animal RNA viruses. Avian Dis. 1970, 14, 330–336. [Google Scholar] [CrossRef]
- Wu, D.; Tiantian, W.; Qun, L.; Zhicong, Y. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar]
- Bchetnia, M.; Girard, C.; Duchaine, C.; Laprise, C. The outbreak of the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): A review of the current global status. J. Infect. Public Health 2020, 13, 1601–1610. [Google Scholar] [CrossRef]
- Weiss, S.R.; Navas-Martin, S. Coronavirus pathogenesis and the emerging pathogen severe acute respiratory syndrome coronavirus. Microbiol. Mol. Biol. Rev. 2005, 69, 635–664. [Google Scholar] [CrossRef] [Green Version]
- Wevers, B.A.; van der Hoek, L. Recently discovered human coronaviruses. Clin. Lab. Med. 2009, 29, 715–724. [Google Scholar] [CrossRef]
- Lau, S.K.; Woo, P.C.; Li, K.S.; Huang, Y.; Tsoi, H.W.; Wong, B.H.; Wong, S.Y.W.; Leung, S.-Y.; Chan, K.-H.; Yuen, K.-Y. Severe acute respiratory syndrome coronavirus-like virus in Chinese horseshoe bats. Proc. Natl. Acad. Sci. USA 2005, 102, 14040–14045. [Google Scholar] [CrossRef] [Green Version]
- Antiochia, R. Nanobiosensors as new diagnostic tools for SARS, MERS and COVID-19: From past to perspectives. Microchim. Acta 2020, 187, 1–13. [Google Scholar] [CrossRef]
- Tsang, T.; Lai-Yin, T.; Pak-Yin, L.; Lee, M. Update: Outbreak of severe acute respiratory syndrome-worldwide, 2003. MMWR Morb. Mortal. Wkly. Rep. 2003, 52, 241. [Google Scholar]
- Poutanen, S.M.; Low, D.E.; Henry, B.; Finkelstein, S.; Rose, D.; Green, K.; Tellier, R.; Draker, R.; Adachi, D.; Ayers, M.; et al. Identification of severe acute respiratory syndrome in Canada. N. Engl. J. Med. 2003, 348, 1995–2005. [Google Scholar] [CrossRef]
- Lee, N.; Hui, D.; Wu, A.; Chan, P.; Cameron, P.; Joynt, G.M.; Ahuja, A.; Yung, M.Y.; Leung, C.; To, K.; et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N. Engl. J. Med. 2003, 348, 1986–1994. [Google Scholar] [CrossRef]
- Peiris, J.S.M.; Lai, S.T.; Poon, L.L.M.; Guan, Y.; Yam, L.Y.C.; Lim, W.; Nicholls, J.; Yee, W.K.S.; Yan, W.W.; Cheung, M.T.; et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 2003, 361, 1319–1325. [Google Scholar] [CrossRef] [Green Version]
- Holmes, K.V. SARS coronavirus: A new challenge for prevention and therapy. J. Clin. Investig. 2003, 111, 1605–1609. [Google Scholar] [CrossRef]
- Drosten, C.; Günther, S.; Preiser, W.; Van Der Werf, S.; Brodt, H.R.; Becker, S.; Holger, R.; Panning, M.; Kolesnikova, L.; Fouchier, R.A.M.; et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N. Engl. J. Med. 2003, 348, 1967–1976. [Google Scholar] [CrossRef]
- Mohd, H.A.; Memish, Z.A.; Alfaraj, S.H.; McClish, D.; Altuwaijri, T.; Alanazi, M.S.; Aloqiel, S.A.; Alenzi, A.M.; Bafaqeeh, F.; Mohammed, A.M.; et al. Predictors of MERS-CoV infection: A large case control study of patients presenting with ILI at a MERS-CoV referral hospital in Saudi Arabia. Travel Med. Infect. Dis. 2016, 14, 464–470. [Google Scholar] [CrossRef]
- Eifan, S.A.; Nour, I.; Hanif, A.; Zamzam, A.M.; Al Johani, S.M. A pandemic risk assessment of Middle East respiratory syndrome coronavirus (MERS-CoV) in Saudi Arabia. Saudi J. Biol. Sci. 2017, 24, 1631–1638. [Google Scholar] [CrossRef]
- Azhar, E.I.; Hui, D.S.; Memish, Z.A.; Drosten, C.; Zumla, A. The middle east respiratory syndrome (MERS). Infect. Dis. Clin. 2019, 33, 891–905. [Google Scholar] [CrossRef]
- Alqahtani, A.S.; Rashid, H.; Basyouni, M.H.; Alhawassi, T.M.; BinDhim, N.F. Public response to MERS-CoV in the Middle East: iPhone survey in six countries. J. Infect. Public Health 2017, 10, 534–540. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, L.; Geng, H.; Deng, Y.; Huang, B.; Guo, Y.; Zhao, Z.; Tan, W. The structural and accessory proteins M, ORF 4a, ORF 4b, and ORF 5 of Middle East respiratory syndrome coronavirus (MERS-CoV) are potent interferon antagonists. Protein Cell 2013, 4, 951–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siu, K.L.; Yeung, M.L.; Kok, K.H.; Yuen, K.S.; Kew, C.; Lui, P.Y.; Chan, C.P.; Tse, H.; Woo, P.C.; Yuen, K.Y. Middle east respiratory syndrome coronavirus 4a protein is a double-stranded RNA-binding protein that suppresses PACT-induced activation of RIG-I and MDA5 in the innate antiviral response. J. Virol. 2014, 88, 4866–4876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.; Yan, Y.; Wang, L. Coronavirus disease 2019: Coronaviruses and blood safety. Transfus. Med. Rev. 2020, 34, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Worldometer. 2021. Available online: https://www.worldometers.info/coronavirus/ (accessed on 29 August 2021).
- Haleem, A.; Javaid, M.; Vaishya, R. Effects of COVID-19 pandemic in daily life. Curr. Med. Res. Pract. 2020, 10, 78. [Google Scholar] [CrossRef]
- Cheval, S.; Adamescu, C.M.; Georgiadis, T.; Herrnegger, M.; Piticar, A.; Legates, D.R. Observed and Potential Impacts of the COVID-19 Pandemic on the Environment. Int. J. Environ. Res. Public Health 2020, 17, 4140. [Google Scholar] [CrossRef]
- Li, H.O.-Y.; Huynh, D. Long-term social distancing during COVID-19: A social isolation crisis among seniors? CMAJ 2020, 192, E588. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Perez, G.I.P.; Abadi, A.T.B. Ongoing challenges faced in the global control of COVID-19 pandemic. Arch. Med. Res. 2020, 51, 574–576. [Google Scholar] [CrossRef]
- Ehrlich, H.; McKenney, M.; Elkbuli, A. Protecting our healthcare workers during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 1527–1528. [Google Scholar] [CrossRef]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents. 2020, 55, 105955. [Google Scholar] [CrossRef]
- Taha, B.A.; Al Mashhadany, Y.; Bachok, N.N.; Bakar, A.A.; Hafiz Mokhtar, M.H.; Dzulkefly Bin Zan, M.S.; Arsad, N. Detection of COVID-19 Virus on Surfaces Using Photonics: Challenges and Perspectives. Diagnostics. 2021, 11, 1119. [Google Scholar] [CrossRef]
- Mohapatra, R.K.; Pintilie, L.; Kandi, V.; Sarangi, A.K.; Das, D.; Sahu, R.; Perekhoda, L. The recent challenges of highly contagious COVID-19, causing respiratory infections: Symptoms, diagnosis, transmission, possible vaccines, animal models, and immunotherapy. Chem. Biol. Drug Design. 2020, 96, 1187–1208. [Google Scholar] [CrossRef]
- Abdul-Rasool, S.; Fielding, B.C. Understanding human coronavirus HCoV-NL63. Open Virol. J. 2010, 4, 76. [Google Scholar] [CrossRef]
- Liu, D.X.; Liang, J.Q.; Fung, T.S. Human Coronavirus-229E,-OC43,-NL63, and-HKU1 (Coronaviridae). Encycl. Virol. 2021, 428. [Google Scholar]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Alexandar, S.; Ravisankar, M.; Kumar, R.S.; Jakkan, K. A comprehensive review on Covid-19 Delta variant. Int. J. Pharmacol. Clin. Res. (IJPCR) 2021, 5, 83–85. [Google Scholar]
- Bárcena, M.; Oostergetel, G.T.; Bartelink, W.; Faas, F.G.; Verkleij, A.; Rottier, P.J. Koster, A.J.; Bosch, B.J. Cryo-electron tomography of mouse hepatitis virus: Insights into the structure of the coronavirion. Proc. Natl. Acad. Sci. USA 2009, 106, 582–587. [Google Scholar] [CrossRef] [Green Version]
- Neuman, B.W.; Adair, B.D.; Yoshioka, C.; Quispe, J.D.; Orca, G.; Kuhn, P.; Milligan, R.A.; Yeager, M.; Buchmeier, M.J. Supramolecular architecture of severe acute respiratory syndrome coronavirus revealed by electron cryomicroscopy. J. Virol. 2006, 80, 7918–7928. [Google Scholar] [CrossRef] [Green Version]
- Rossi, J.J.; Rossi, D. Oligonucleotides and the COVID-19 pandemic: A perspective. Nucleic Acid Ther. 2020, 30, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Y.; Tan, Y.W.; Liu, D.X. Recent progress in studies of arterivirus-and coronavirus-host interactions. Viruses 2012, 4, 980–1010. [Google Scholar]
- Sun, C.; Chen, L.; Yang, J.; Luo, C.; Zhang, Y.; Li, J.; Yang, J.; Zhang, J.; Xie, L. SARS-CoV-2 and SARS-CoV spike-RBD structure and receptor binding comparison and potential implications on neutralizing antibody and vaccine development. Biorxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Hillyer, C.; Du, L. Neutralizing antibodies against SARS-CoV-2 and other human coronaviruses. Trends Immunol. 2020, 41, 355–359. [Google Scholar] [CrossRef]
- Zhang, F.; Walters, M.D. Pathogen Genomics and Host Cellular Susceptibility Factors of COVID-19. Glob. Clin. Transl. Res. 2020, 2, 107–126. [Google Scholar] [CrossRef]
- Hamed, A.M. Image processing of corona virus using interferometry. Opt. Photonics J. 2016, 6, 75. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Xing, Y.; Peng, J.; Zheng, Z.; Tang, W.; Sun, Y.; Xu, C.; Peng, F. Chest CT for detecting COVID-19: A systematic review and meta-analysis of diagnostic accuracy. Eur. Radiol. 2020, 30, 5720–5727. [Google Scholar] [CrossRef]
- Panahi, A.H.; Rafiei, A.; Rezaee, A. FCOD: Fast COVID-19 Detector based on deep learning techniques. Inform. Med. Unlocked 2021, 22, 100506. [Google Scholar] [CrossRef]
- Degerli, A.; Ahishali, M.; Yamac, M.; Kiranyaz, S.; Chowdhury, M.E.H.; Hameed, K.; Hamid, T.; Mazhar, R.; Gabbouj, M. COVID-19 infection map generation and detection from chest X-ray images. Health Inf. Sci. Syst. 2021, 9, 1–6. [Google Scholar] [CrossRef]
- Chandra, T.B.; Verma, K.; Singh, B.K.; Jain, D.; Netam, S.S. Coronavirus disease (COVID-19) detection in chest X-ray images using majority voting based classifier ensemble. Expert Syst. Appl. 2021, 165, 113909. [Google Scholar] [CrossRef]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation, and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020, 14, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Naudé, W. Artificial Intelligence against COVID-19: An Early Review; Institute of Labor Economics (IZA): Bonn, Germany, 2020. [Google Scholar]
- Sethy, P.K.; Behera, S.K. Detection of coronavirus disease (COVID-19) based on deep features. Int. J. Math. Eng. Manag. Sci. 2020. [Google Scholar] [CrossRef]
- Majeed, T.; Rashid, R.; Ali, D.; Asaad, A. Problems of deploying cnn transfer learning to detect covid-19 from chest x-rays. MedRxiv 2020. [Google Scholar] [CrossRef]
- Hemdan, E.E.D.; Shouman, M.A.; Karar, M.E. Covidx-net: A framework of deep learning classifiers to diagnose covid-19 in x-ray images. arXiv 2020, arXiv:2003.11055. [Google Scholar]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: Evaluation of the diagnostic accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef] [PubMed]
- Elkorany, A.S.; Elsharkawy, Z.F. COVIDetection-Net: A tailored COVID-19 detection from chest radiography images using deep learning. Optik 2021, 231, 166405. [Google Scholar] [CrossRef] [PubMed]
- Nigam, B.; Nigam, A.; Jain, R.; Dodia, S.; Arora, N.; Annappa, B. COVID-19: Automatic detection from X-ray images by utilizing deep learning methods. Expert Syst. Appl. 2021, 176, 114883. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, T.; Choudhary, P. FocusCovid: Automated COVID-19 detection using deep learning with chest X-ray images. Evol. Syst. 2021, 9, 1–5. [Google Scholar] [CrossRef]
- Gökcen, A.; Karadağ, B.; Riva, C.; Boyacı, A. Artificial intelligence–based COVID-19 detection using cough records. Electrica 2021, 21, 203–208. [Google Scholar] [CrossRef]
- Khattak, M.I.; Al-Hasan, M.A.; Jan, A.; Saleem, N.; Verdú, E.; Khurshid, N. Automated Detection of COVID-19 using Chest X-Ray Images and CT Scans through Multilayer-Spatial Convolutional Neural Networks. Int. J. Interact. Multimed. Artif. Intell. 2021, 6, 15–24. [Google Scholar] [CrossRef]
- Hussain, E.; Hasan, M.; Rahman, M.A.; Lee, I.; Tamanna, T.; Parvez, M.Z. CoroDet: A deep learning based classification for COVID-19 detection using chest X.-ray images. Chaos Solitons Fractals 2021, 142, 110495. [Google Scholar] [CrossRef]
- Hashmi, H.A.; Asif, H.M. Early Detection Of COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Mei, X.; Lee, H.C.; Diao, K.Y.; Huang, M.; Lin, B.; Liu, C.; Xie, Z.; Ma, Y.; Robson, P.M.; Chung, M.; et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat. Med. 2020, 26, 1224–1228. [Google Scholar] [CrossRef]
- Kaushik, A.K.; Dhau, J.S.; Gohel, H.; Mishra, Y.K.; Kateb, B.; Kim, N.Y.; Goswami, D.Y. Electrochemical SARS-CoV-2 sensing at point-of-care and artificial intelligence for intelligent COVID-19 management. ACS Appl. Bio Mater. 2020, 3, 7306–7325. [Google Scholar] [CrossRef]
- Irfan, M.; Iftikhar, M.A.; Yasin, S.; Draz, U.; Ali, T.; Hussain, S.; Bukhari, S.; Alwadie, A.S.; Rahman, S.; Glowacz, A.; et al. Role of Hybrid Deep Neural Networks (HDNNs), Computed Tomography, and Chest X-rays for the Detection of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 3056. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Qazan, S.; Alquran, H.; Qasmieh, I.A.; Alqudah, A. Covid-2019 detection using x-ray images and artificial intelligence hybrid systems. X-Ray Imaging 2020, 2, 1. [Google Scholar]
- Loey, M.; Smarandache, F.; Khalifa, M.N.E. Within the lack of chest COVID-19 X-ray dataset: A novel detection model based on GAN and deep transfer learning. Symmetry 2020, 12, 651. [Google Scholar] [CrossRef] [Green Version]
- Albahli, S.; Yar, G.N. Fast and Accurate Detection of COVID-19 Along With 14 Other Chest Pathologies Using a Multi-Level Classification: Algorithm Development and Validation Study. J. Med. Internet Res. 2021, 23, e23693. [Google Scholar] [CrossRef]
- Kim, H.; Hwang, J.; Kim, J.H.; Lee, S.; Kang, M. Sensitive detection of multiple fluoresence probes based on surface-enhanced raman scattering (sers) for mers-cov. In Proceedings of the 2019 IEEE 14th International Conference on Nano/Micro Engineered and Molecular Systems (NEMS), Bangkok, Thailand, 11–14 April 2019; pp. 498–501. [Google Scholar]
- Qiu, G.; Gai, Z.; Tao, Y.; Schmitt, J.; Kullak-Ublick, G.A.; Wang, J. Dual-functional plasmonic photothermal biosensors for highly accurate severe acute respiratory syndrome coronavirus 2 detection. ACS Nano 2020, 14, 5268–5277. [Google Scholar] [CrossRef] [Green Version]
- Seo, G.; Lee, G.; Kim, M.J.; Baek, S.H.; Choi, M.; Ku, K.B.; Lee, C.S.; Jun, S.; Park, D.; Kim, H.G.; et al. Rapid detection of COVID-19 causative virus (SARS-CoV-2) in human nasopharyngeal swab specimens using field-effect transistor-based biosensor. ACS Nano 2020, 14, 5135–5142. [Google Scholar] [CrossRef] [Green Version]
- Bhalla, N.; Pan, Y.; Yang, Z.; Payam, A.F. Opportunities and challenges for biosensors and nanoscale analytical tools for pandemics: COVID-19. ACS Nano 2020, 14, 7783–7807. [Google Scholar] [CrossRef]
- Murugan, D.; Bhatia, H.; Sai, V.V.; Satija, J. P-FAB: A fiber-optic biosensor device for rapid detection of COVID-19. Trans. Indian Natl. Acad. Eng. 2020, 5, 211–215. [Google Scholar] [CrossRef]
- Nag, P.; Sadani, K.; Mukherji, S. Optical fiber sensors for rapid screening of COVID-19. Trans. Indian Natl. Acad. Eng. 2020, 5, 233–236. [Google Scholar] [CrossRef]
- Ruiz-Vega, G.; Soler, M.; Lechuga, L.M. Nanophotonic biosensors for point-of-care COVID-19 diagnostics and coronavirus surveillance. J. Phys. Photonics. 2021, 3, 011002. [Google Scholar] [CrossRef]
- Van Tran, V.; Tran, N.H.; Hwang, H.S.; Chang, M. Development strategies of conducting polymer-based electrochemical biosensors for virus biomarkers: Potential for rapid COVID-19 detection. Biosens. Bioelectron. 2021, 182, 113192. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Lee, M.J.; Lee, S.N.; Kim, T.H.; Oh, B.K. Noble metal nanomaterial-based biosensors for electrochemical and optical detection of viruses causing respiratory illnesses. Front. Chem. 2021, 9, 672739. [Google Scholar] [CrossRef]
- Fabiani, L.; Saroglia, M.; Galatà, G.; De Santis, R.; Fillo, S.; Lucam, V.; Faggioni, G.; D’Amore, N.; Regalbuto, E.; Salvatori, P.; et al. Magnetic beads combined with carbon black-based screen-printed electrodes for COVID-19: A reliable and miniaturized electrochemical immunosensor for SARS-CoV-2 detection in saliva. Biosens. Bioelectron. 2021, 171, 112686. [Google Scholar] [CrossRef]
- Kudo, E.; Israelow, B.; Vogels, C.B.; Lu, P.; Wyllie, A.L.; Tokuyama, M.; Venkataraman, A.; Brackney, D.E.; Ott, I.M.; Petrone, M.E.; et al. Detection of SARS-CoV-2 RNA by multiplex RT-qPCR. PLoS Biol. 2020, 18, e3000867. [Google Scholar] [CrossRef]
- Suo, T.; Liu, X.; Feng, J.; Guo, M.; Hu, W.; Guo, D.; Ullah, H.; Yang, Y.; Zhang, Q.; Wang, X.; et al. ddPCR: A more accurate tool for SARS-CoV-2 detection in low viral load specimens. Emerg. Microbes Infect. 2020, 9, 1259–1268. [Google Scholar] [CrossRef]
- Ke, G.; Su, D.; Li, Y.; Zhao, Y.; Wang, H.; Liu, W.; Li, M.; Yang, Z.; Xiao, F.; Yuan, Y.; et al. An accurate, high-speed, portable bifunctional electrical detector for COVID-19. Sci. China Mater. 2021, 64, 739–747. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, Z.; Zhai, X.; Li, Y.; Lin, L.; Zhao, H.; Bian, L.; Li, P.; Yu, L.; Wu, Y.; et al. Rapid and sensitive detection of anti-SARS-CoV-2 IgG, using lanthanide-doped nanoparticles-based lateral flow immunoassay. Anal. Chem. 2020, 92, 7226–7231. [Google Scholar] [CrossRef]
- Damle, V.H.; Rajeswaran, B.; Tischler, Y.R. Low-Frequency Raman Spectroscopy as a Diagnostic Tool for COVID-19 and other Coronaviruses. R. Soc. Open Sci. 2020, 7, 1–28. [Google Scholar]
- Wu, Y.C.; Chen, C.S.; Chan, Y.J. The outbreak of COVID-19: An overview. J. Chin. Med. Assoc. 2020, 83, 217. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. Bmj 2020, 1–9, 369. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Saw, L.H.; Leo, B.F.; Nor, N.S.M.; Yip, C.W.; Ibrahim, N.; Abd Hamid, H.H.; Latif, M.T.; Lin, C.Y.; Nadzir, M.S. Modeling aerosol transmission of SARS-CoV-2 from human-exhaled particles in a hospital ward. Environ. Sci. Pollut. Res. 2021, 28, 53478–53492. [Google Scholar] [CrossRef]
- Asadi, S.; Wexler, A.S.; Cappa, C.; Barreda, S.; Bouvier, N.M.; Ristenpart, W.D. Aerosol emission and superemission during human speech increase with voice loudness. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Qu, G.; Li, X.; Hu, L.; Jiang, G. An imperative need for research on the role of environmental factors in transmission of novel coronavirus (COVID-19). ACS Publ. 2020, 54, 3730–3732. [Google Scholar] [CrossRef]
- Medicine, The Lancet Respiratory. COVID-19 transmission—up in the air. Lancet. Respir. Med. 2020, 8, 1159. [Google Scholar] [CrossRef]
- Cheung, K.S.; Hung, I.F.; Chan, P.P.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.; Tam, A.R.; et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from a Hong Kong cohort: Systematic review and meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.I.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics 2020, 58, 712–713. [Google Scholar]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. 2020, 115. [Google Scholar] [CrossRef]
- Gao, Q.Y.; Chen, Y.X.; Fang, J.Y. 2019 Novel coronavirus infection and gastrointestinal tract. J. Dig. Dis. 2020, 21, 125. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.; Kok, K.H.; Zhu, Z.; Chu, H.; To, K.K.; Yuan, S.; Yuen, K.Y. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg. Microbes Infect. 2020, 9, 221–236. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, M.; Beck, R.; Caccio, S.M.; Duim, B.; Fraaij, P.L.; Le Guyader, F.S.; Lecuit, M.; Le Pendu, J.D.W.E.; Schultsz, C. Sustained fecal-oral human-to-human transmission following a zoonotic event. Curr. Opin. Virol. 2017, 22, 1–6. [Google Scholar] [CrossRef]
- Du, M.; Cai, G.; Chen, F.; Christiani, D.C.; Zhang, Z.; Wang, M. Multiomics evaluation of gastrointestinal and other clinical characteristics of COVID-19. Gastroenterology 2020, 158, 2298–2301. [Google Scholar] [CrossRef]
- Zhang, H.; Kang, Z.; Gong, H.; Xu, D.; Wang, J.; Li, Z.; Cui, X.; Xiao, J.; Meng, T.; Zhou, W.; et al. The digestive system is a potential route of 2019-nCov infection: A bioinformatics analysis based on single-cell transcriptomes. BioRxiv. 2020, 1–26. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833. [Google Scholar] [CrossRef]
- Masand, R.; Jadhao, A.; Jadhav, S. Review on Modes of Transmission of COVID-19. Int. J. Curr. Microbiol. Appl. Sci. 2021, 10, 1003–1014. [Google Scholar]
- Karimi, S.; Arabi, A.; Shahraki, T.; Safi, S. Detection of severe acute respiratory syndrome Coronavirus-2 in the tears of patients with Coronavirus disease 2019. Eye 2020, 34, 1220–1223. [Google Scholar] [CrossRef]
- Sungnak, W.; Huang, N.; Bécavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; Talavera-López, C.; Maatz, H.; Reichart, D.; Sampaziotis, F.; et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat. Med. 2020, 26, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Xu, Z.; Castiglione, G.M.; Soiberman, U.S.; Eberhart, C.G.; Duh, E.J. ACE2 and TMPRSS2 are expressed on the human ocular surface, suggesting susceptibility to SARS-CoV-2 infection. Ocul. Surf. 2020, 18, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Roehrich, H.; Yuan, C.; Hou, J.H. Immunohistochemical study of SARS-CoV-2 viral entry factors in the cornea and ocular surface. Cornea 2020, 39, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, M.; Zhang, Z.; Qiao, K.; Huang, T.; Chen, M.; Xin, N.; Huang, Z.; Liu, L.; Zhang, G.; et al. Ocular manifestations of a hospitalised patient with confirmed 2019 novel coronavirus disease. Br. J. Ophthalmol. 2020, 104, 748–751. [Google Scholar] [CrossRef] [PubMed]
- Ocansey, S.; Abu, E.K.; Abraham, C.H.; Owusu-Ansah, A.; Boadi-Kusi, S.B.; Ilechie, A.A.; Acheampong, D.O. Ocular Symptoms of SARS-CoV-2: Indication of Possible Ocular Transmission or Viral Shedding. Ocul. Im Munology Inflamm. 2020, 28, 1269–1279. [Google Scholar] [CrossRef]
- Lu, C.-W.; Liu, X.-F.; Jia, Z.-F. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet 2020, 395, e39. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Yin, K. Management of pregnant women infected with COVID-19. Lancet Infect. Dis. 2020, 20, 513–514. [Google Scholar] [CrossRef] [Green Version]
- Cornish, E.F.; Filipovic, I.; Åsenius, F.; Williams, D.J.; McDonnell, T. Innate immune responses to acute viral in-fection during pregnancy. Front. Immunol. 2020, 11, 2404. [Google Scholar] [CrossRef]
- Lu-Culligan, A.; Chavan, A.R.; Vijayakumar, P.; Irshaid, L.; Courchaine, E.M.; Milano, K.M.; Tang, Z.; Pope, S.D.; Song, E.; Vogels, C.B.; et al. SARS-CoV-2 infection in pregnancy is associated with robust inflam-matory response at the maternal-fetal interface. medRxiv 2021, 1–45. [Google Scholar] [CrossRef]
- Li, M.; Chen, L.; Zhang, J.; Xiong, C.; Li, X. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal inter-face and fetal organs by single-cell transcriptome study. PLoS ONE 2020, 15, e0230295. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Guo, L.; Chen, L.; Liu, W.; Cao, Y.; Zhang, J.; Feng, L. A case report of neonatal COVID-19 infection in China. Clin. Infect. Dis. 2020, 71, 853–857. [Google Scholar] [CrossRef]
- Mor, G.; Aldo, P.; Alvero, A.B. The unique immunological and microbial aspects of pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef]
- Karimi-Zarchi, M.; Neamatzadeh, H.; Dastgheib, S.A.; Abbasi, H.; Mirjalili, S.R.; Behforouz, A.; Ferdosian, F.; Bahrami, R. Vertical transmission of coronavirus disease 19 (COVID-19) from infected pregnant mothers to neonates: A review. Fetal Pediatric Pathol. 2020, 39, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Wang, L.-L.; Zhao, S.-J.; Kwak-Kim, J.; Mor, G.; Liao, A.-H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J. Reprod. Immunol. 2020, 139, 103122. [Google Scholar] [CrossRef]
- Massart, S.; Chiumenti, M.; De Jonghe, K.; Glover, R.; Haegeman, A.; Koloniuk, I.; Komínek, P.; Kreuze, J.; Kutnjak, D.; Lotos, L.; et al. Virus Detection by High-Throughput Sequencing of Small RNAs: Large-Scale Performance Testing of Sequence Analysis Strategies. Phytopathology 2019, 109, 488–497. [Google Scholar] [CrossRef] [Green Version]
- John, G.; Sahajpal, N.S.; Mondal, A.K.; Ananth, S.; Williams, C.; Chaubey, A.; Rojiani, A.M.; Kolhe, R. Next-Generation Sequencing (NGS) in COVID-19: A Tool for SARS-CoV-2 Diagnosis, Monitoring New Strains and Phylo-dynamic Modeling in Molecular Epidemiology. Curr. Issues Mol. Biol. 2021, 43, 845–867. [Google Scholar] [CrossRef]
- Drmanac, R.; Sparks, A.B.; Callow, M.J.; Halpern, A.L.; Burns, N.L.; Kermani, B.G.; Carnevali, P.; Nazarenko, I.; Nilsen, G.B.; Yeung, G.; et al. Human genome sequencing using unchained base reads on self-assembling DNA nanoar-rays. Science 2010, 327, 78–81. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, D.; Kumar, S.; Chandrasekaran, N.; Mukherjee, F.R.S.B. Viral diagnostics and preventive techniques in the era of COVID-19: Role of nanotechnology. Front. Nanotechnol. 2020, 2, 7. [Google Scholar] [CrossRef]
- Wan, Z.; Zhang, Y.N.; He, Z.; Liu, J.; Lan, K.; Hu, Y.; Zhang, C. A melting curve-based multiplex RT-qPCR assay for simultaneous detection of four human coronaviruses. Int. J. Mol. Sci. 2016, 17, 1880. [Google Scholar] [CrossRef] [Green Version]
- Noh, J.Y.; Yoon, S.W.; Kim, D.J.; Lee, M.S.; Kim, J.H.; Na, W.; Song, D.; Jeong, D.G.; Kim, H.K. Simultaneous detection of se-vere acute respiratory syndrome, Middle East respiratory syndrome, and related bat coronaviruses by real-time reverse transcription PCR. Arch. Virol. 2017, 162, 1617–1623. [Google Scholar] [CrossRef] [Green Version]
- Sood, S.; Aggarwal, V.; Aggarwal, D.; Upadhyay, S.K.; Sak, K.; Tuli, H.S.; Kumar, M.; Kumar, J.; Talwar, S. COVID-19 Pandemic: From Molecular Biology, Pathogenesis, Detection, and Treatment to Global Societal Impact. Curr. Pharmacol. Rep. 2020, 6, 212–227. [Google Scholar] [CrossRef]
- Carter, L.J.; Garner, L.V.; Smoot, J.W.; Li, Y.; Zhou, Q.; Saveson, C.J. Janet, M.; Gregg, A.C.; Soares, D.J.; Beskid, T.R.; et al. Assay techniques and test development for COVID-19 diagnosis. ACS Cent. Sci. 2020, 6, 591–605. [Google Scholar] [CrossRef]
- Orooji, Y.; Sohrabi, H.; Hemmat, N.; Oroojalian, F.; Baradaran, B.; Mokhtarzadeh, A.; Karimi-Maleh, H. An overview on SARS-CoV-2 (COVID-19) and other human coronaviruses and their detection capability via am-plification assay, chemical sensing, biosensing, immunosensing, and clinical assays. Nano-Micro Lett. 2021, 13, 1–30. [Google Scholar] [CrossRef]
- Yang, W.; Dang, X.; Wang, Q.; Xu, M.; Zhao, Q.; Zhou, Y.; Zhao, H.; Wang, L.; Xu, Y.; Wang, J.; et al. Rapid detection of SARS-CoV-2 using reverse transcription RT-LAMP method. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Gill, P.; Ghaemi, A. Nucleic Acid Isothermal Amplification Technologies—A Review. Nucleosides Nucleotides Nucleic Acids 2008, 27, 224–243. [Google Scholar] [CrossRef] [PubMed]
- Tasrip, N.A.; Khairil Mokhtar, N.F.; Hanapi, U.K.; Abdul Manaf, Y.N.; Ali, M.E.; Cheah, Y.K.; Mustafa, S.; Desa, M. Loop mediated isothermal amplification; A review on its application and strategy in animal species authentication of meat based food products. Int. Food Res. J. 2019, 26, 1–10. [Google Scholar]
- Kumar, R.; Nagpal, S.; Kaushik, S.; Mendiratta, S. COVID-19 diagnostic approaches: Different roads to the same destination. VirusDisease 2020, 31, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Park, G.S.; Ku, K.; Baek, S.H.; Kim, S.J.; Kim, S.I.; Kim, B.T.; Maeng, J.S. Development of reverse transcription loop-mediated isothermal amplification assays targeting severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). J. Mol. Diagnostics. 2020, 22, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, C.D.; Sharma, P.; Sinha, K.; Rajarshi, K. Recent trends in analytical and digital techniques for the detection of the SARS-Cov-2. Biophys. Chem. 2021, 270, 106538. [Google Scholar] [CrossRef]
- Fozouni, P.; Son, S.; de León Derby, M.D.; Knott, G.J.; Gray, C.N.; D’Ambrosio, M.V.; Zhao, C.; Switz, N.A.; Kumar, G.R.; Stephens, S.I.; et al. Direct detection of SARS-CoV-2 using CRISPR-Cas13a and a mobile phone. MedRxiv 2020. [Google Scholar] [CrossRef]
- Hang, W.; Liu, K.; Zhang, P.; Cheng, W.; Li, L.; Zhang, F.; Yu, Z.; Li, L.; Zhang, X. CRISPR-Based approaches for efficient and accurate detection of SARS-CoV-2. Lab. Med. 2021, 52, 116–121. [Google Scholar]
- Lam, W.Y.; Yeung, A.C.M.; Tang, J.W.; Ip, M.; Chan, E.W.C.; Hui, M.; Chan, P.K.S. Rapid Multiplex Nested PCR for Detection of Respiratory Viruses. J. Clin. Microbiol. 2007, 45, 3631–3640. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Sun, Q.; He, J.; Xu, H.; Liu, C.; Zhao, C.; Xu, Y.; Wu, C.; Xiang, J.; Gu, D.; et al. Development of SPR biosensor for simultaneous detection of multiplex respiratory viruses. Bio-Medical Mater. Eng. 2015, 26, S2207–S2216. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Whitaker, B.; Sakthivel, S.K.K.; Kamili, S.; Rose, L.E.; Lowe, L.; Mohareb, E.; Elassal, E.M.; Al-sanouri, T.; Haddadin, A.; et al. Real-time reverse transcription-PCR assay panel for Middle East respiratory syndrome corona-virus. J. Clin. Microbiol. 2014, 52, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Pfefferle, S.; Reucher, S.; Nörz, D.; Lütgehetmann, M. Evaluation of a quantitative RT-PCR assay for the detection of the emerging coronavirus SARS-CoV-2 using a high throughput system. Eurosurveillance 2020, 25, 2000152. [Google Scholar] [CrossRef] [Green Version]
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X.; Yu, J.; Shan, S.; Zhou, B.; Song, S.; et al. Human neutralizing antibodies elicited by SARS-CoV-2 infection. Nature 2020, 584, 115–119. [Google Scholar] [CrossRef]
- Huang, P.; Wang, H.; Cao, Z.; Jin, H.; Chi, H.; Zhao, J.; Yu, B.; Yan, F.; Hu, X.; Wu, F.; et al. A rapid and specific assay for the detection of MERS-CoV. Front. Microbiol. 2018, 9, 1101. [Google Scholar] [CrossRef]
- Kim, J.H.; Kang, M.; Park, E.; Chung, D.R.; Kim, J.; Hwang, E.S. A simple and multiplex loop-mediated isothermal am-plification (LAMP) assay for rapid detection of SARS-CoV. Biochip J. 2019, 13, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef]
- Yu, C.Y.; Chan, K.G.; Yean, C.Y.; Ang, G.Y. Nucleic acid-based diagnostic tests for the detection SARS-CoV-2: An update. Diagnostics 2021, 11, 53. [Google Scholar] [CrossRef]
- Taha, B.; Al Mashhadany, Y.; Mokhtar, M.H.; Bin Zan, M.D.; Arsad, N. An Analysis Review of Detection Coronavirus Disease 2019 (COVID-19) Based on Biosensor Application. Sensors 2020, 20, 6764. [Google Scholar] [CrossRef]
- Dai, Y.; Liu, C.C. Recent advances on electrochemical biosensing strategies toward universal point-of-care systems. Angew. Chemie 2019, 131, 12483–12496. [Google Scholar] [CrossRef]
- Ibrahim, N.; Jamaluddin, N.; Tan, L.; Yusof, N.M. A Review on the Development of Gold and Silver Nanoparticles-Based Biosensor as a Detection Strategy of Emerging and Pathogenic RNA Virus. Sensors 2021, 21, 5114. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Bueno, J.L.; Bergua, J.F.; Costantini, M.; Giannetto, M.; Puntes, V.; De La Escosura-Muñiz, A.; Merkoçi, A. Low-Cost Strategy for the Development of a Rapid Electrochemical Assay for Bacteria Detection Based on AuAg Nanoshells. ACS Omega 2018, 3, 18849–18856. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, H.; Zhang, J.; Li, G. Electrochemical Sensors for Clinic Analysis. Sensors 2008, 8, 2043–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Z.; Ma, Y.; Chen, M.; Ambrosi, A.; Ding, C.; Luo, X. Electrochemical Biosensor with Enhanced Antifouling Capability for COVID-19 Nucleic Acid Detection in Complex Biological Media. Anal. Chem. 2021, 93, 5963–5971. [Google Scholar] [CrossRef] [PubMed]
- Nehra, A.; Singh, K.P. Current trends in nanomaterial embedded field effect transistor-based biosensor. Biosens. Bioelectron. 2015, 74, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Janissen, R.; Sahoo, P.K.; Santos, C.A.; da Silva, A.M.; von Zuben, A.A.G.; Souto, D.E.P.; Costa, A.D.T.; Celedon, P.; Zanchin, N.I.T.; Almeida, D.B.; et al. InP Nanowire Biosensor with Tailored Biofunctionalization: Ultrasensitive and Highly Selective Disease Biomarker Detection. Nano Lett. 2017, 17, 5938–5949. [Google Scholar] [CrossRef] [Green Version]
- Shabani, E.; Dowlatshahi, S.; Abdekhodaie, M.J. Laboratory detection methods for the human coronaviruses. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 225–246. [Google Scholar] [CrossRef]
- Zhang, X.; Qi, Q.; Jing, Q.; Ao, S.; Zhang, Z.; Ding, M.; Wu, M.; Liu, K.; Wang, W.; Ling, Y.; et al. Electrical probing of COVID-19 spike protein receptor binding domain via a graphene field-effect transistor. arXiv 2020, arXiv:2003.12529. [Google Scholar]
- Pohanka, M. Overview of Piezoelectric Biosensors, Immunosensors and DNA Sensors and Their Applications. Materials 2018, 11, 448. [Google Scholar] [CrossRef] [Green Version]
- Shons, A.; Dorman, F.; Najarian, J. An immunospecific microbalance. J. Biomed. Mater. Res. 1972, 6, 565–570. [Google Scholar] [CrossRef]
- Meyers, F.N.; Loh, K.J.; Dodds, J.S.; Baltazar, A. Active sensing and damage detection using piezoelectric zinc ox-ide-based nanocomposites. Nanotechnology 2013, 24, 185501. [Google Scholar] [CrossRef]
- Zuo, B.; Li, S.; Guo, Z.; Zhang, J.; Chen, C. Piezoelectric immunosensor for SARS-associated coronavirus in spu-tum. Anal. Chem. 2004, 76, 3536–3540. [Google Scholar] [CrossRef]
- Kabir, H.; Merati, M.; Abdekhodaie, M.J. Design of an effective piezoelectric microcantilever biosensor for rap-id detection of COVID-19. J. Med. Eng. Technol. 2021, 14, 1. [Google Scholar]
- Zhang, K.; Zhang, L.; Fu, L.; Li, S.; Chen, H.; Cheng, Z.-Y. Magnetostrictive resonators as sensors and actuators. Sens. Actuators A Phys. 2013, 200, 2–10. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Z.; Liu, Y.; Wang, X.; Li, Y.; Ma, P.; Gu, B.; Li, H. Recent advances in rapid pathogen detection method based on biosensors. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1021–1037. [Google Scholar] [CrossRef]
- Narita, F.; Wang, Z.; Kurita, H.; Li, Z.; Shi, Y.; Jia, Y.; Soutis, C. A Review of Piezoelectric and Magnetostrictive Biosensor Materials for Detection of COVID-19 and Other Viruses. Adv. Mater. 2020, 33, e2005448. [Google Scholar] [CrossRef]
- Ansari, A.A.; Alhoshan, M.; Alsalhi, M.S.; Aldwayyan, A.S. Prospects of nanotechnology in clinical immunodi-agnostics. Sensors 2010, 10, 6535–6581. [Google Scholar] [CrossRef]
- Sciacca, B.; François, A.; Hoffmann, P.; Monro, T.M. Multiplexing of radiative-surface plasmon resonance for the detection of gastric cancer biomarkers in a single optical fiber. Sens. Actuators B Chem. 2013, 183, 454–458. [Google Scholar] [CrossRef]
- Taha, B.; Ali, N.; Sapiee, N.; Fadhel, M.; Yeh, R.M.; Bachok, N.; Al Mashhadany, Y.; Arsad, N. Comprehensive Review Tapered Optical Fiber Configurations for Sensing Application: Trend and Challenges. Biosensors 2021, 11, 253. [Google Scholar] [CrossRef]
- Cotruvo, J.A., Jr.; Aron, A.T.; Ramos-Torres, K.M.; Chang, C.J. Synthetic fluorescent probes for studying copper in biological systems. Chem. Soc. Rev. 2015, 44, 4400–4414. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Khan, R.; Catanante, G.; Sherazi, T.A.; Bhand, S.; Hayat, A.; Marty, J.L. Designed strategies for flu-orescence-based biosensors for the detection of mycotoxins. Toxins 2018, 10, 197. [Google Scholar] [CrossRef] [Green Version]
- Diao, B.; Wen, K.; Chen, J.; Liu, Y.; Yuan, Z.; Han, C.; Chen, J.; Pan, Y.; Chen, L.; Dan, Y.; et al. Diagnosis of acute respiratory syndrome coronavirus 2 infection by detection of nucleocapsid protein. MedRxiv 2020. [Google Scholar] [CrossRef]
- Song, D.; Liu, J.; Xu, W.; Han, X.; Wang, H.; Cheng, Y.; Zhuo, Y.; Long, F. Rapid and quantitative detection of SARS-CoV-2 IgG antibody in serum using optofluidic point-of-care testing fluorescence biosensor. Talanta 2021, 235, 122800. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Kan, L.; Duan, F.; He, L.; Wang, M.; Cui, J.; Zhang, Z.; Zhang, Z. Surface plasmon resonance aptasensor based on niobium carbide MXene quantum dots for nucleocapsid of SARS-CoV-2 detection. Microchim. Acta. 2021, 188, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.C.; Chang, Y.F.; Chen, K.H.; Su, L.C.; Lee, C.W.; Chen, C.C.; Chen, Y.M.; Chou, C. Detection of severe acute respiratory syndrome (SARS) coronavirus nucleocapsid protein in human serum using a localized sur-face plasmon coupled fluorescence fiber-optic biosensor. Biosens. Bioelectron. 2009, 25, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Divagar, M.; Gayathri, R.; Rasool, R.; Shamlee, J.K.; Bhatia, H.; Satija, J.; Sai, V.V. Plasmonic Fiberoptic Absorb-ance Biosensor (P-FAB) for Rapid Detection of SARS-CoV-2 Nucleocapsid Protein. IEEE Sens. J. 2021, 21, 22758–22766. [Google Scholar] [CrossRef]
- Mahari, S.; Roberts, A.; Shahdeo, D.; Gandhi, S. eCovSens-ultrasensitive novel in-house built printed circuit board based electrochemical device for rapid detection of nCovid-19 antigen, a spike protein domain 1 of SARS-CoV-2. BioRxiv 2020, 172, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Layqah, L.A.; Eissa, S. An electrochemical immunosensor for the corona virus associated with the Middle East respiratory syndrome using an array of gold nanoparticle-modified carbon electrodes. Microchim. Acta 2019, 186, 224. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coronaviruses | Year of Finding | Emergence | Type | HOST | Cellular Receptor | Incubation Period | Respiratory System Infection | Symptoms | Mortality Rate | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| HCoV-HKU1 | 2005 | Hong Kong | Beta | Human | 9-O-Acetylated sialic acid | 2–4 days | √ | Common cold, Bronchitis, and pneumonia. | N.A. | [33] |
| HCoV-Nl63 | 2004 | Holland | Alpha | Human | ACE2 | 2–4 days | √ | Common cold, sore throat, bronchiolitis/croup in children, high temperature, malaise, coughing and rhinitis | N.A. | [34] |
| HCoV-229E | 1966 | N.A. | Alpha | Human | Human aminopeptidase N (CD13) | 2–5 days | √ | Common cold, Headache, Fever, Running nose, Pneumonia (in neonates), malaise, Bronchiolitis, | N.A. | [35] |
| HCoV-OC43 | 1967 | N.A. | Beta | Human | 9-O-Acetylated sialic acid | 2–5 days | √ | Running nose, Common cold, Fever, Headache, Malaise, Bronchiolitis, Pneumonia (in neonates) | N.A. | [35] |
| SARS-CoV | 2002 | Guangdong, southern China | Beta | Civets, Human | ACE2 | 2–11 days | √ | Headache, Diarrhea, Fever, Shivering, Dyspnea, Cough, Pneumonia, Myalgia | 10% | [33] |
| MERS-CoV | 2012 | Jeddah, Saudi Arabia | Beta | Camel, Human | DPP4 | 2–14 days | √ | Fever, sore throat, dyspnea, dry cough, Chills, Pneumonia, Myalgia, Diarrhea, Hemoptysis, Headache, Rhinorrhoea | 35% | [19] |
| SARS-CoV-2 | 2019 | Hubei province, Wuhan city, China | Beta | Bat, Human | ACE2 | 3–6 days | √ | High body temperature, Short of breath, Headache, Sore throat, myalgia, Dry coughing, Anosmia, rarely pneumonia, Diarrhea, Generalized weakness, Nasal congestion, Rhinorrhea, Sneezing | 2.8% | [36] |
| Delta Variant * | 2020 | India | Delta | Human | ACE2 | 5–6 days | √ | Headaches, Sore Throat, Runny Nose, Replacing Cough and Loss of Taste, Loss of Smell | N.A. | [37] |
| Comparison | Transmission Human Exchange | |||
|---|---|---|---|---|
| Respiratory Transmission | Fecal–Oral Transmission | Ocular Transmission | Vertical Transmission | |
| Probability | More likely | More likely | Less likely | Less likely |
| Possibility | High | High | Rare | Rarer |
| Confirmed Cases | Confirmed | Confirmed | Confirmed | Unconfirmed |
| Virus entry organ | Mouth, Nose | Mouth | Eye | Uterus |
| Transmissibility approach | Direct, Indirect | Indirect | Direct, Indirect | Direct |
| Genus | Male and Female | Male and Female | Male and Female | Female |
| Reference | Coronavirus | Analyte | Target Genes | Detection Methods | Limit of Detection | Concentration Range | Detection Time | Tested Sample |
|---|---|---|---|---|---|---|---|---|
| [134] | SARS-CoV | RNA | Polymerase | RT-PCR | 10 copies/reaction | N.A. | (5) h | Nasal aspirate |
| [135] | SARS-CoV | RNA | NA | RT-PCR | 2 nM | N.A. | (~2) h | Throat swab samples |
| [136] | MERS-CoV | RNA | (N) gene | rRT-PCR | 10 copies/reaction or 0.0013 TCID50/ml | 10–108 copies/-reaction | (~2) h | Serum, nasopharyngeal/- oropharyngeal swab, and sputum samples |
| [137] | COVID-19 | RNA | (E)-gene | rRT-PCR | 275.7 copies/reaction | N.A. | (~1) h | Swab samples |
| [138] | COVID-19 | RNA | (N) gene | rRT-PCR | 10 copies/reaction | N.A. | (~30) min | Plasmids containing the complete N gene |
| [139] | MERS-CoV | RNA | (N) gene | RT-LAMP | 10 copies/μL | 5 × 101–5 × 108 copies/-reaction | (35) min | Throat swab specimens |
| [140] | SARS-CoV | RNA | (ORF1b) and (N) gene | LAMP | 104 copies/reaction | N.A. | (20–25) min | Synthetic RNA solutions |
| [141] | COVID-19 | RNA | (ORF1b) and (N) gene | RT-LAMP | 20 copies/reaction | N.A. | (20–30) min | Nasopharyngeal swab and bronchoalveolar lavage fluid samples |
| [126] | COVID-19 | RNA | (ORF1ab), (N) and (E) gene | RT-LAMP | 5 copies/reaction | N.A. | (30) min | Nasopharyngeal swab specimens |
| [142] | COVID-19 | RNA | (S) gene | NGS | 125 GCE/mL | N.A. | N.A. | Nasopharyngeal swab |
| [132] | COVID-19 | RNA | (N) and (E) gene | CRISPR/Cas13a | ~100 copies/µL | 3.2 × 105 –1.65 × 103 copies/µL | (30) min | Nasal swab |
| Reference | Publication Year | Coronavirus | Biosensor Detection Technique | Material | Target | Detection Time | Linear Range | Tested Sample | Limit of Detection | Temperatures |
|---|---|---|---|---|---|---|---|---|---|---|
| [148] | 2 April 2021 | COVID-19 | Electrochemical | (PANI) | N gene | 1 h | 10−14 to 10−9 M | NR | 3.5 fM | 37 °C |
| [171] | 11 May 2020 | COVID-19 | Electrochemical | Gold | S protein | 10–30 s | 1 fM to 1 μM | Spiked saliva samples | 90 fM | 4 °C |
| [172] | 27 February 2019 | MERS-CoV | Electrochemical | Gold | S protein | 20 min | 1 pg·mL−1 to 10 μg·mL−1 | Spiked nasal samples | 0.4 and 1.0 pg·mL−1 | RT |
| [71] | 15 April 2020 | COVID-19 | Electrical (FET) | Graphene | S protein | 4 h | NR | nasopharyngeal swab | 1.6 × 101 pfu/mL | NR |
| [152] | 2020 | COVID-19 | Electrical (FET) | Graphene | S protein | 2 min | NR | Spiked spike protein solutions | 0.2 pM | NR |
| [156] | 1 July 2004 | SARS-CoV | Piezoelectric | Crystal with quartz wafer | Antigen sputum | 1 h | 1–4 µg/µL | NR | 0.60 mg/mL | RT |
| [166] | 13 March 2020 | COVID-19 | Optical (fluorescence) | Not Specified | N protein | 10 min | NR | Nasopharyngeal aspirate swabs and urine | Not Specified | NR |
| [167] | 14 August 2021 | COVID-19 | Optical (fluorescence) | Not Specified | IgG | 25 min | NR | Human serum | 12.5 ng/mL | NR |
| [168] | 11August 2021 | SARS-CoV-2 | Optical (SPR) | Nb2C-SH QD | N gene | NA | 0.05 to 100 ng·mL−1 | Human serum | 4.9 pg·mL−1 | NR |
| [169] | 17 July 2009 | SARS-CoV | Optical (LSPCF) | polymethyl methacrylate | N protein | 2 h | 0.1 pg/mL to 1 ng/mL | Human serum | ∼1 pg/mL | 37 °C |
| [170] | 1 September 2021 | COVID-19 | Optical (P-FAB) | Gold nanoparticles | N protein | 10 min | 0.1 ng/mL and 100 ng/mL | PBS Buffer | ~2.5 ng/mL | NR |
| Categories of Coronavirus Detection | Techniques | Advantages | Limitation |
|---|---|---|---|
| Indirect detection RNA | RT-PCR |
|
|
| Indirect detection RNA | LAMP |
|
|
| Indirect detection RNA | NGS |
|
|
| Indirect detection RNA | CRISPR |
|
|
| Indirect detection: Spike (S) and Nucleocapsid (N) proteins | Electrochemical sensors |
|
|
| Indirect detection: Spike (S) protein | Electronic sensors(FET) |
|
|
| Indirect detection: Antigen sputum | Piezoelectric sensor |
|
|
| Indirect detection: IgM antibody and Nucleocapsid (N) Protein | Optical (fluorescence, SPR, LSPCF, and P-FAB) |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alathari, M.J.A.; Al Mashhadany, Y.; Mokhtar, M.H.H.; Burham, N.; Bin Zan, M.S.D.; A Bakar, A.A.; Arsad, N. Human Body Performance with COVID-19 Affectation According to Virus Specification Based on Biosensor Techniques. Sensors 2021, 21, 8362. https://doi.org/10.3390/s21248362
Alathari MJA, Al Mashhadany Y, Mokhtar MHH, Burham N, Bin Zan MSD, A Bakar AA, Arsad N. Human Body Performance with COVID-19 Affectation According to Virus Specification Based on Biosensor Techniques. Sensors. 2021; 21(24):8362. https://doi.org/10.3390/s21248362
Chicago/Turabian StyleAlathari, Mohammed Jawad Ahmed, Yousif Al Mashhadany, Mohd Hadri Hafiz Mokhtar, Norhafizah Burham, Mohd Saiful Dzulkefly Bin Zan, Ahmad Ashrif A Bakar, and Norhana Arsad. 2021. "Human Body Performance with COVID-19 Affectation According to Virus Specification Based on Biosensor Techniques" Sensors 21, no. 24: 8362. https://doi.org/10.3390/s21248362
APA StyleAlathari, M. J. A., Al Mashhadany, Y., Mokhtar, M. H. H., Burham, N., Bin Zan, M. S. D., A Bakar, A. A., & Arsad, N. (2021). Human Body Performance with COVID-19 Affectation According to Virus Specification Based on Biosensor Techniques. Sensors, 21(24), 8362. https://doi.org/10.3390/s21248362