
Contactless Simultaneous Breathing and Heart Rate Detections in Physical Activity Using IR-UWB Radars


Abstract
:1. Introduction
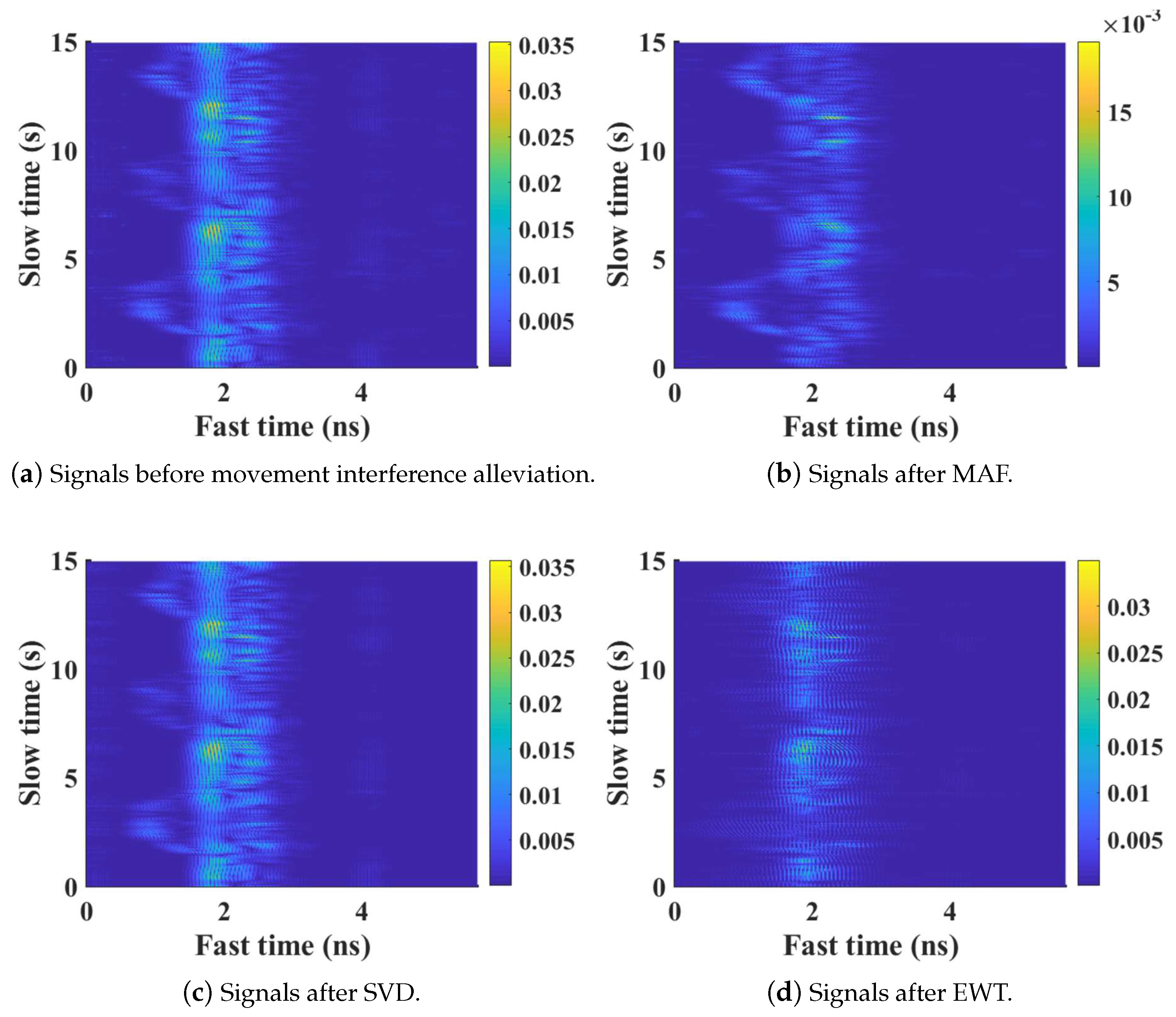
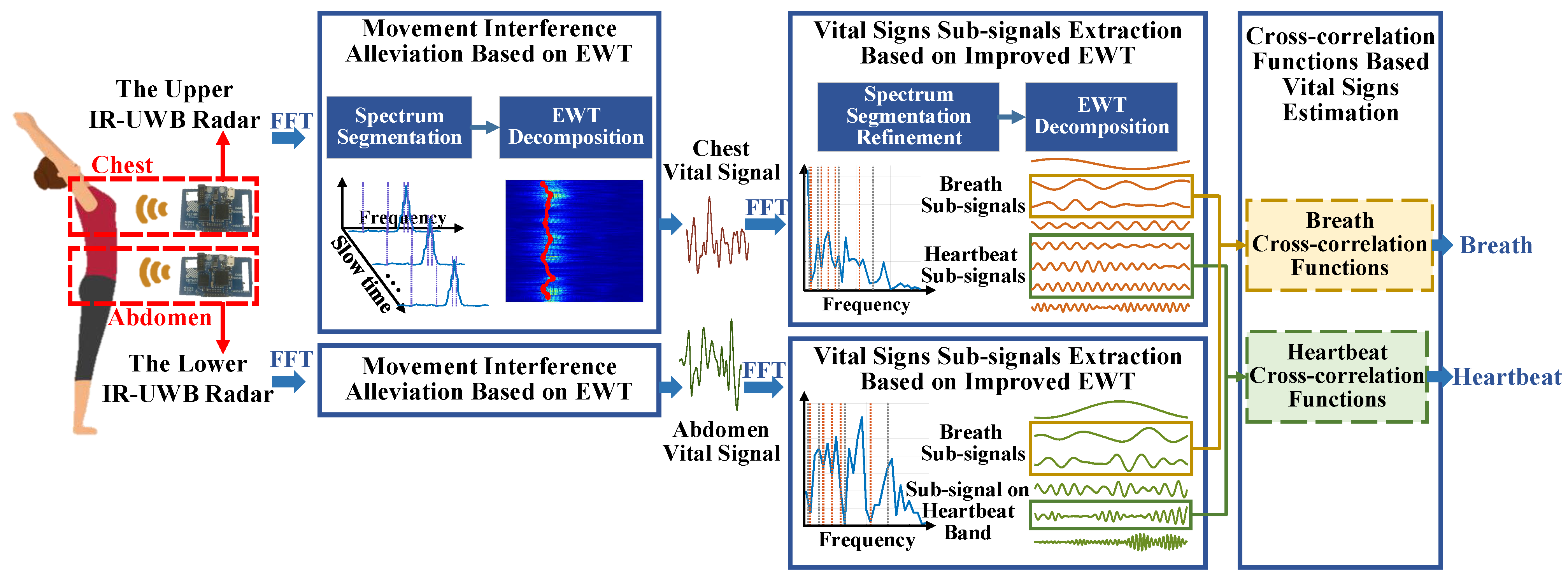
- In order to remove background clutters and alleviate movement interference, EWT is introduced to decompose received radar signals and reduce motion artifacts from various body parts.
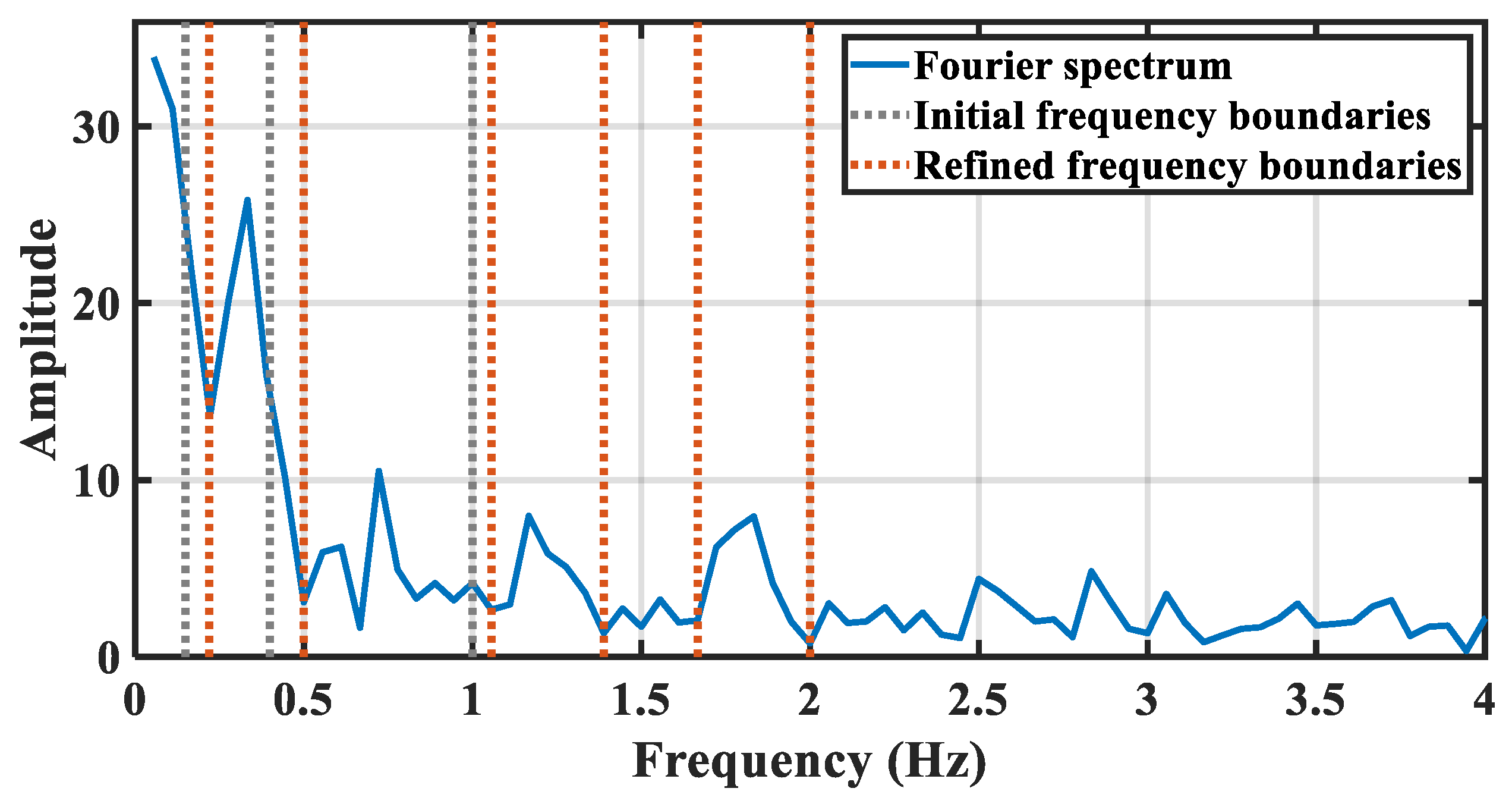
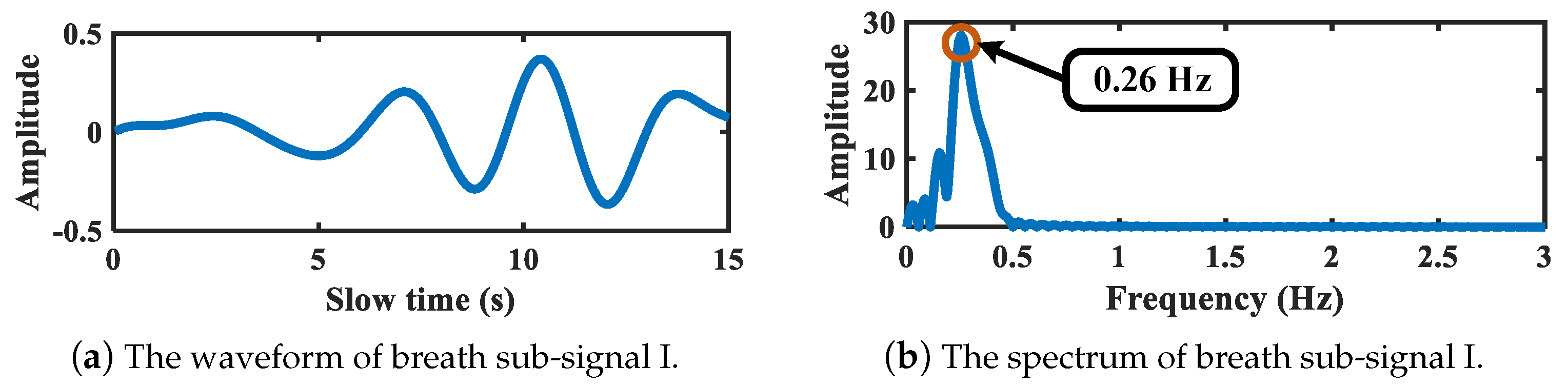
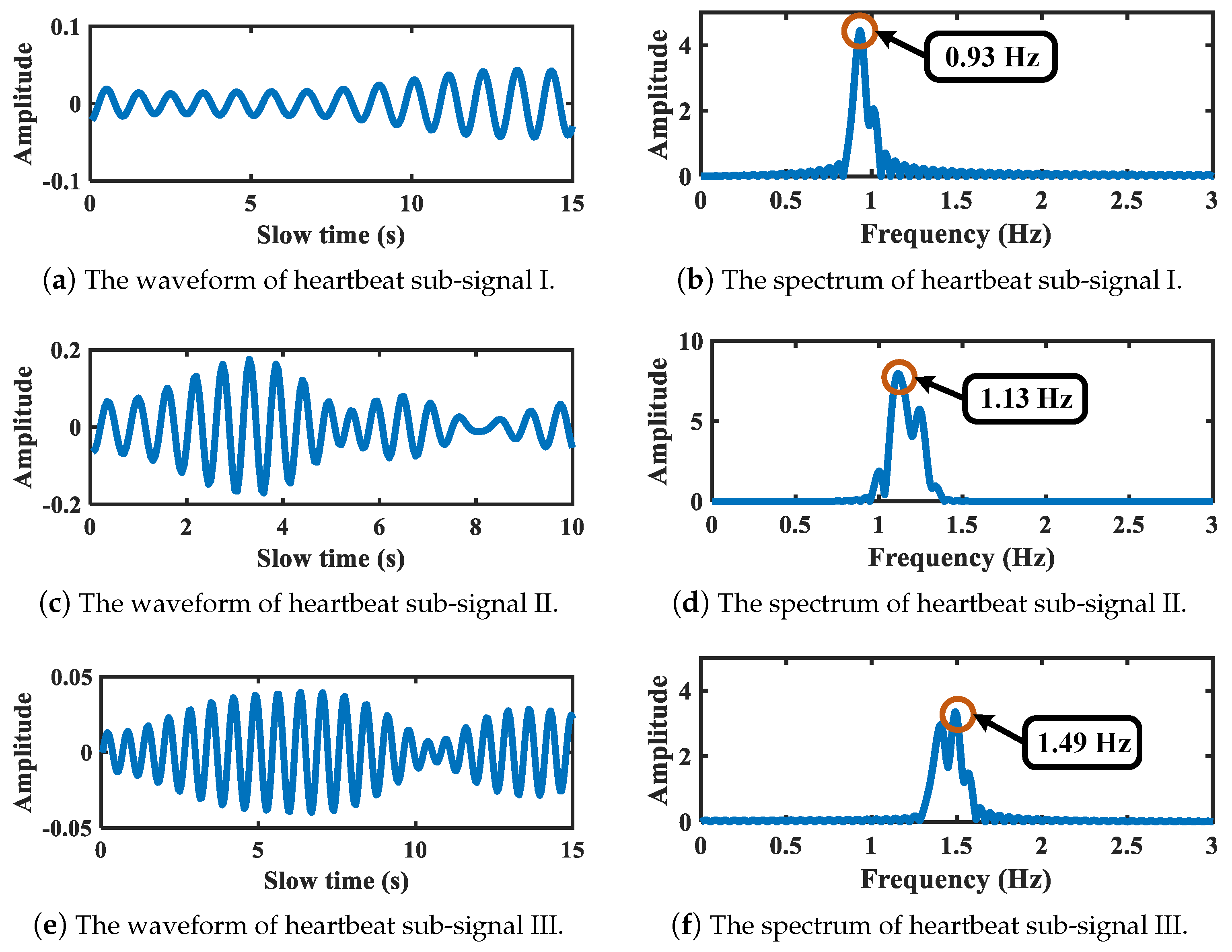
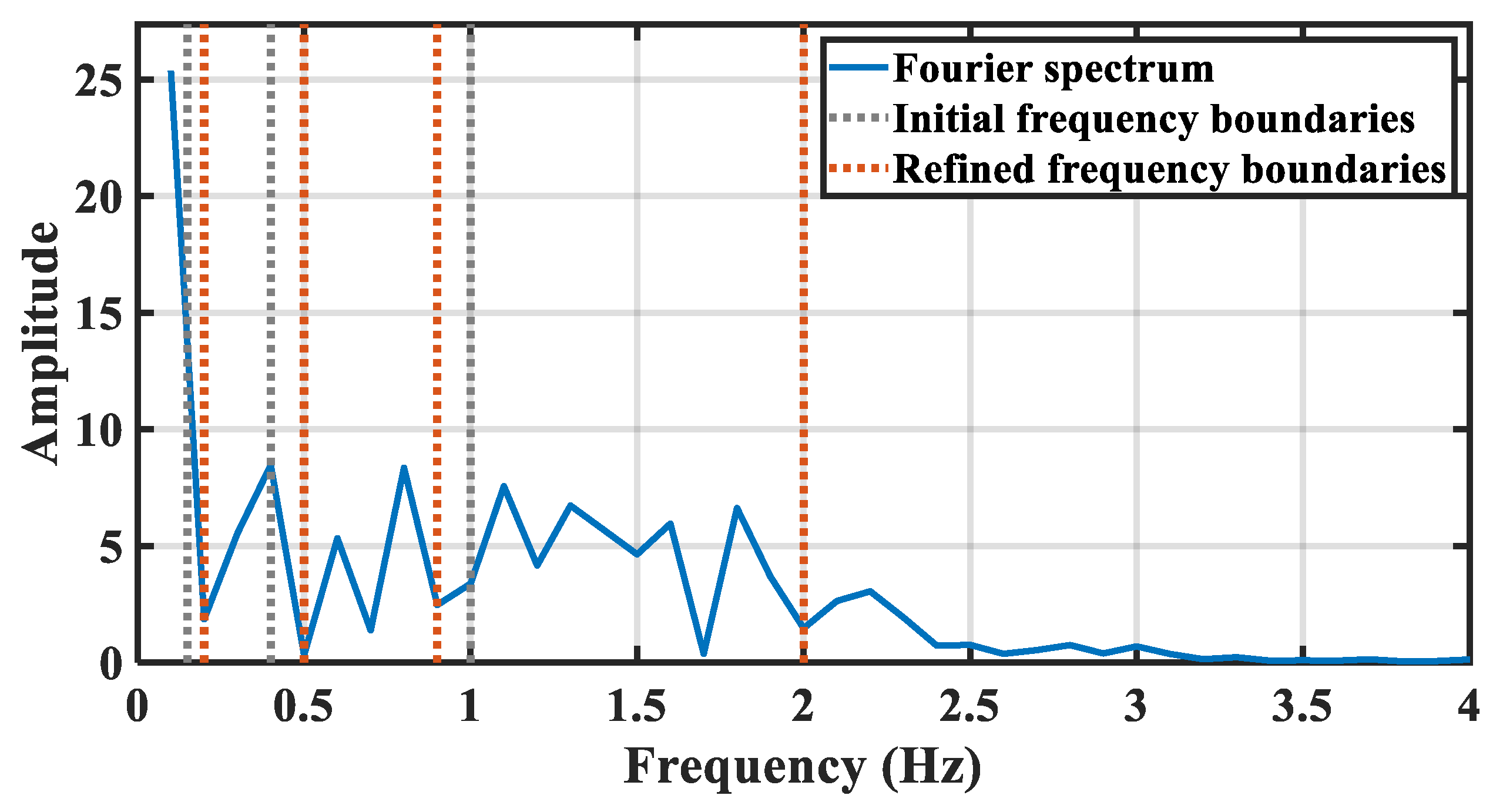
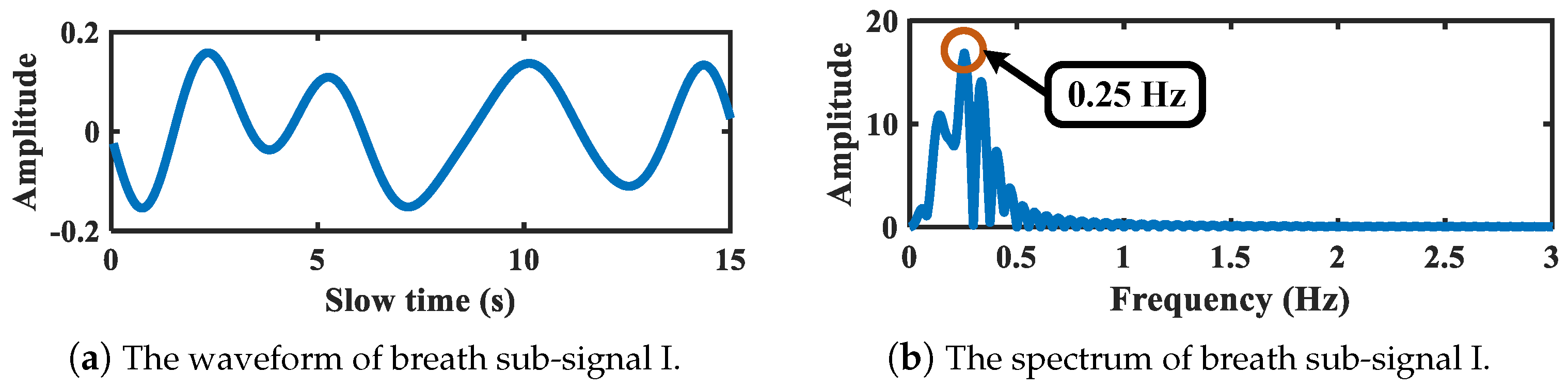
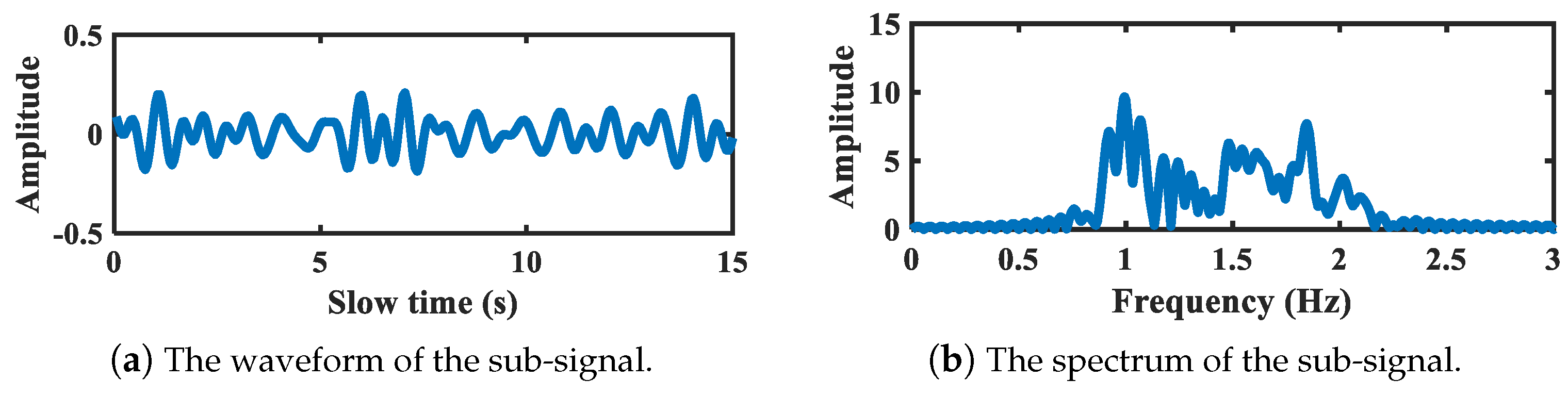
- In order to further extract breath and heartbeat related signals, improved EWT with frequency segmentation refinement is applied on each radar to decompose vital signals of the chest and abdomen, respectively. Thus, vital signs sub-signals are obtained.
- In order to estimate breath and heartbeat under the interference of multi-order harmonics and residual motion artifacts, the cross-correlation functions are calculated among chest and abdomen sub-signals. Based on the thoracoabdominal correlation, the heartbeat and breath are extracted simultaneously.
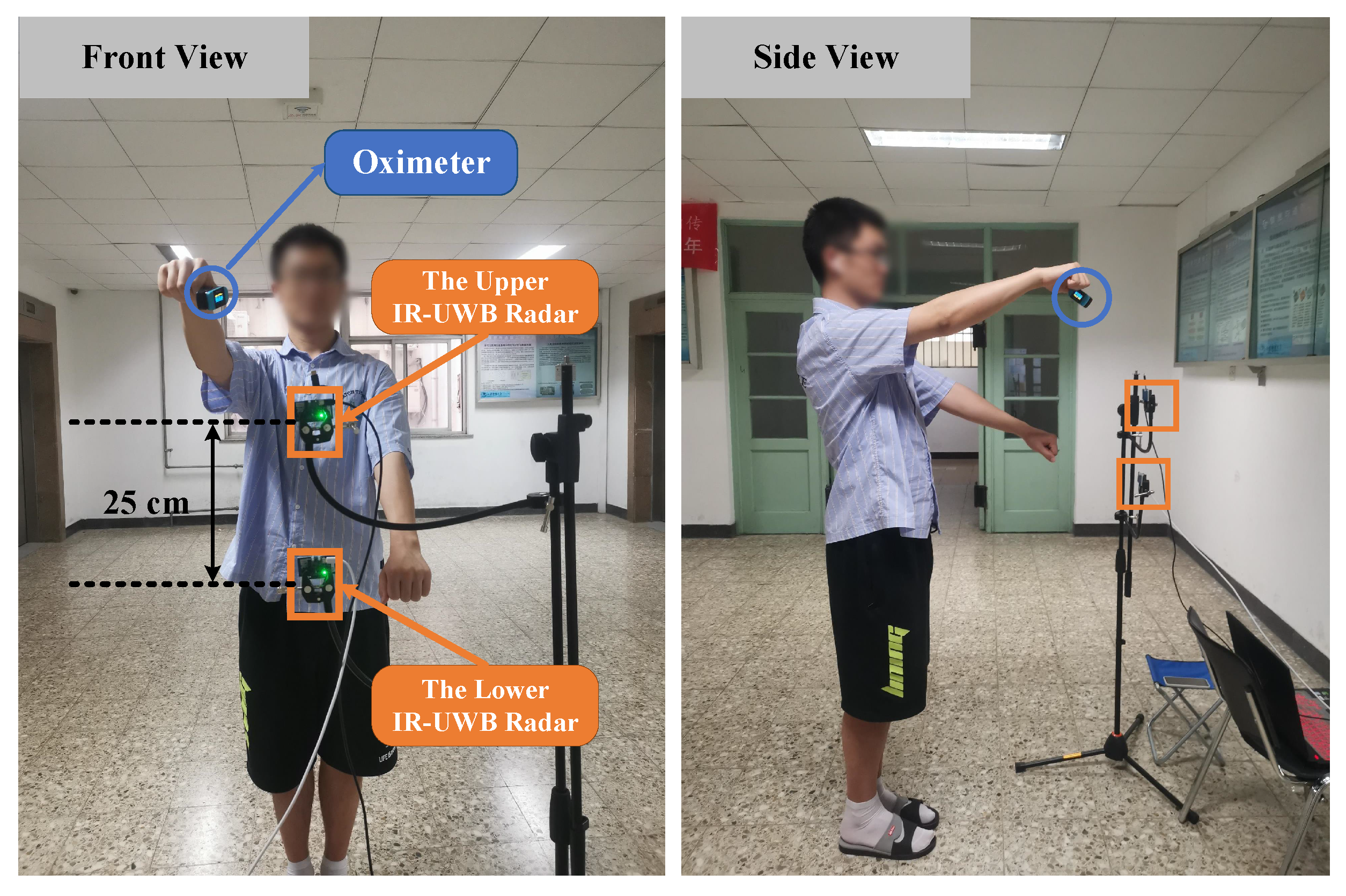
2. Experimental Setup
3. Methods
3.1. IR-UWB Signal Model and Preprocessing
3.2. Movement Interference Alleviation Based on EWT
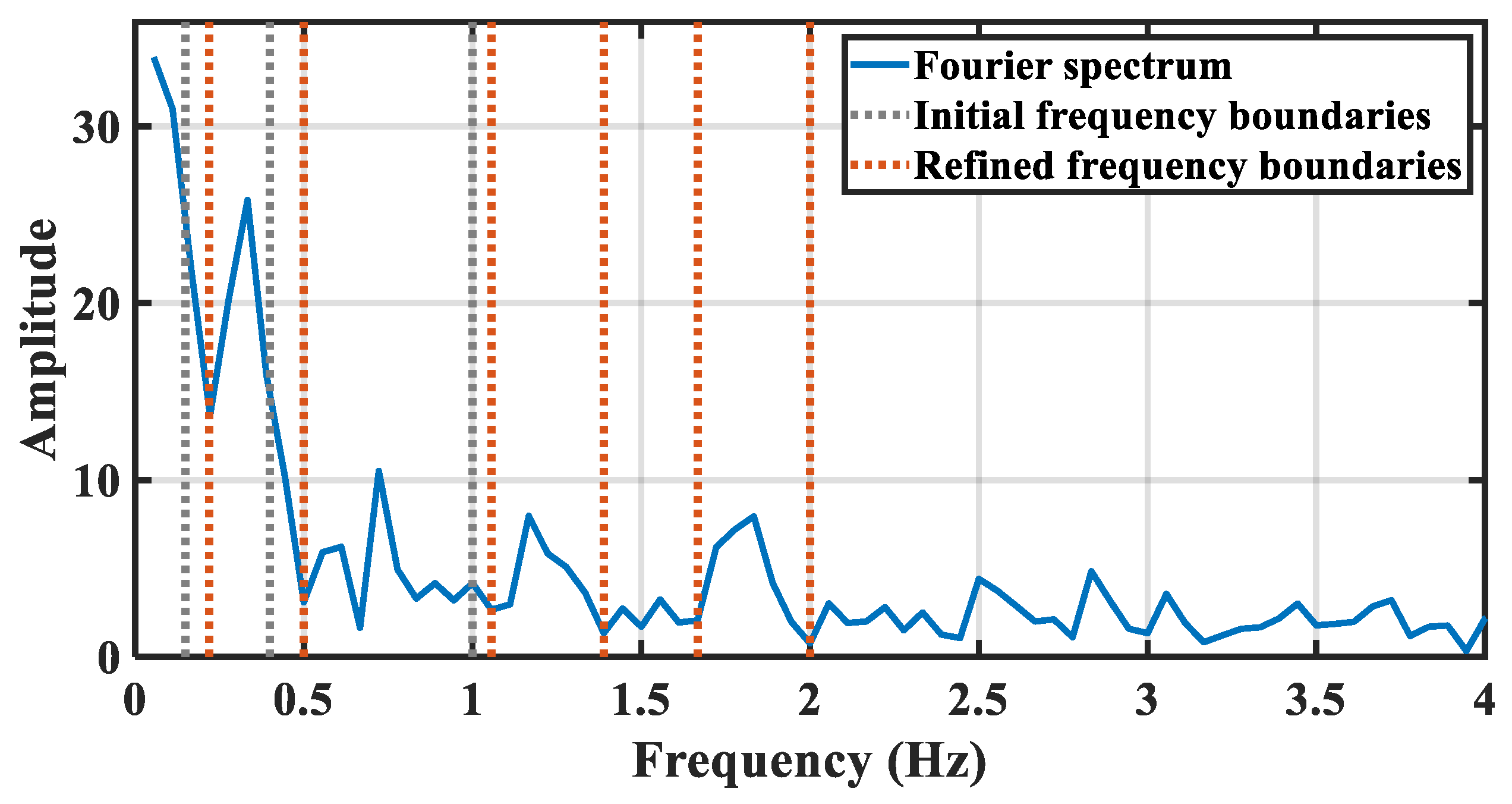
3.3. Vital Signs Sub-Signals Extraction Based on Improved EWT
3.4. Cross-Correlation Functions Based Vital Signs Estimation
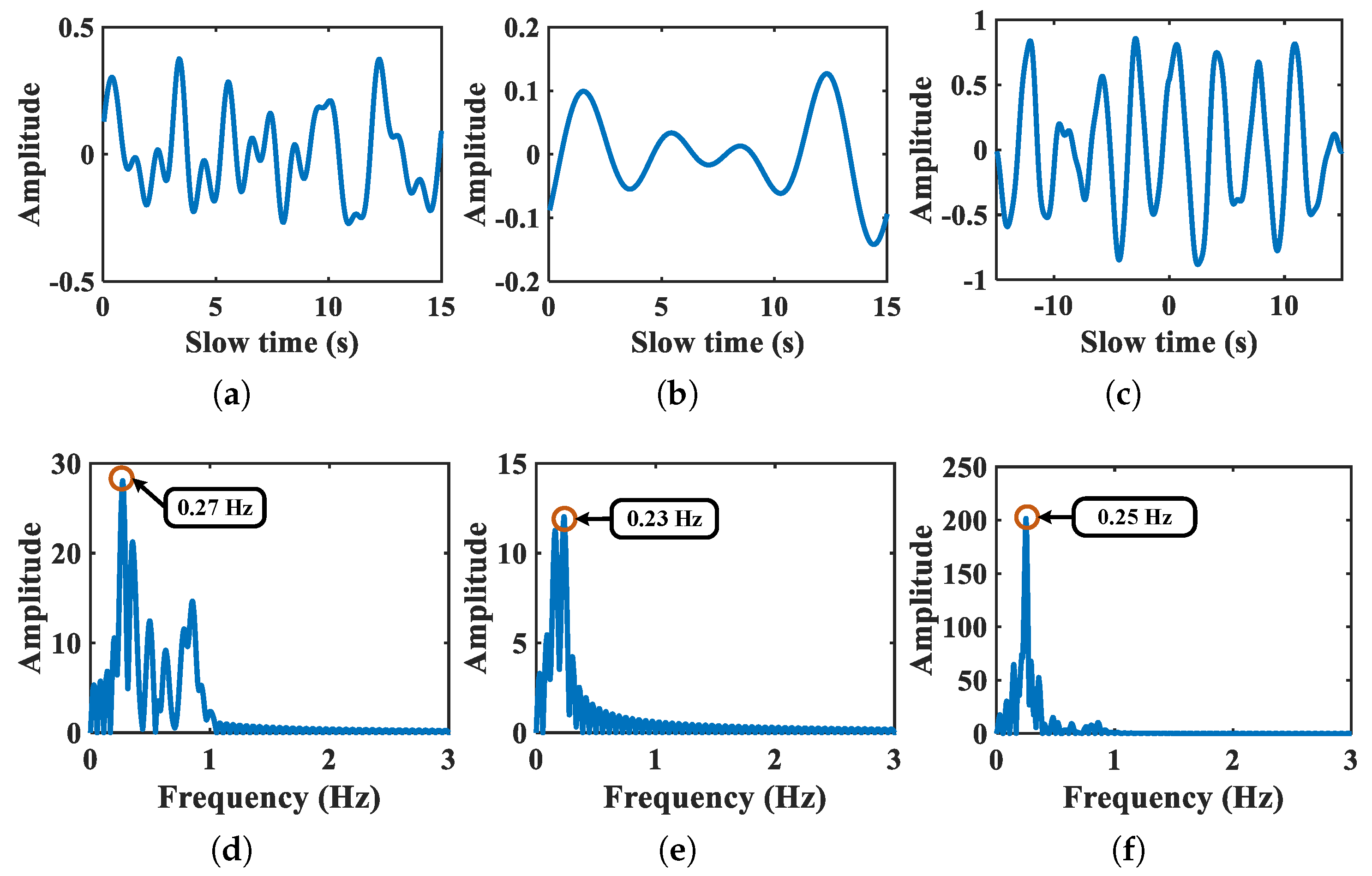
3.4.1. Breath Estimation
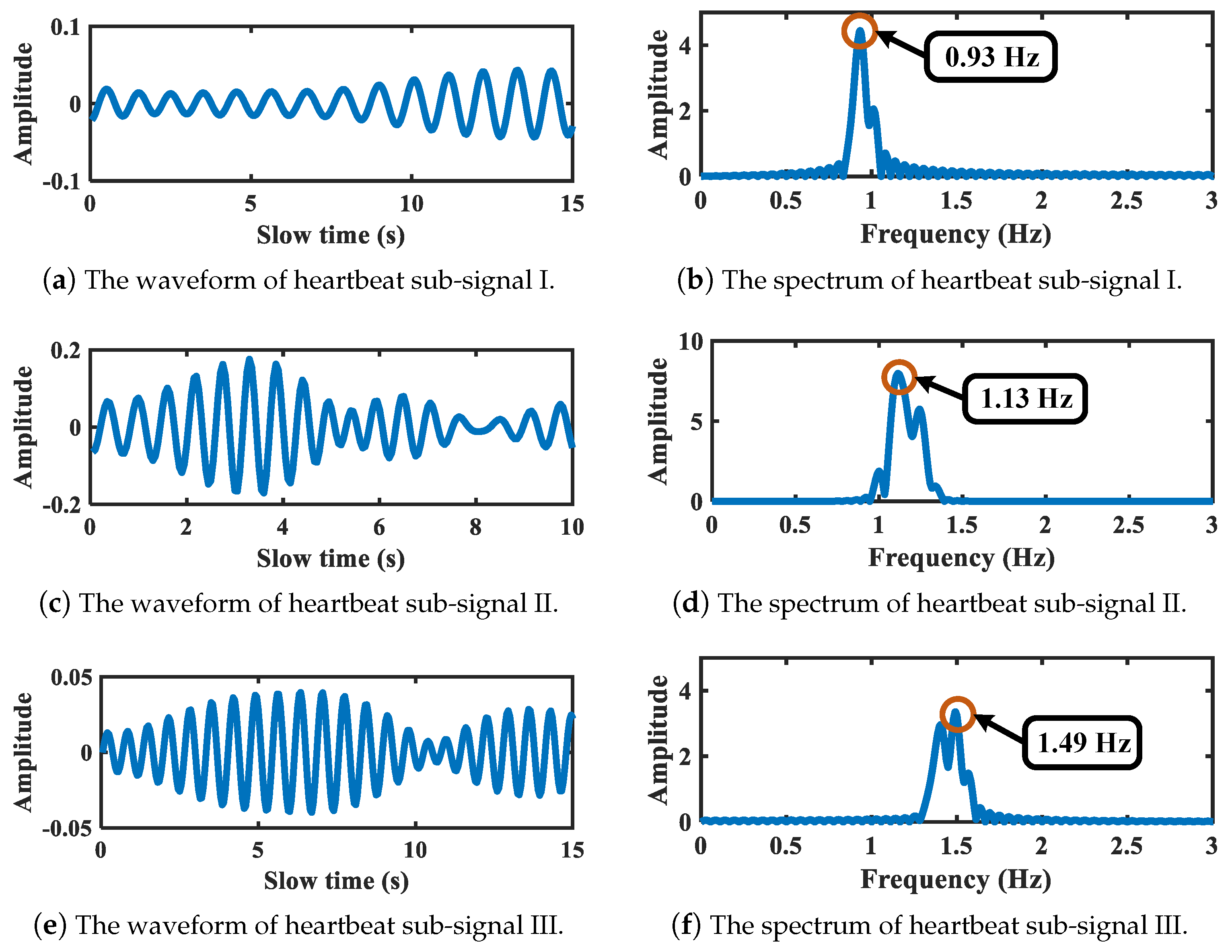
3.4.2. Heartbeat Estimation
4. Results and Discussion
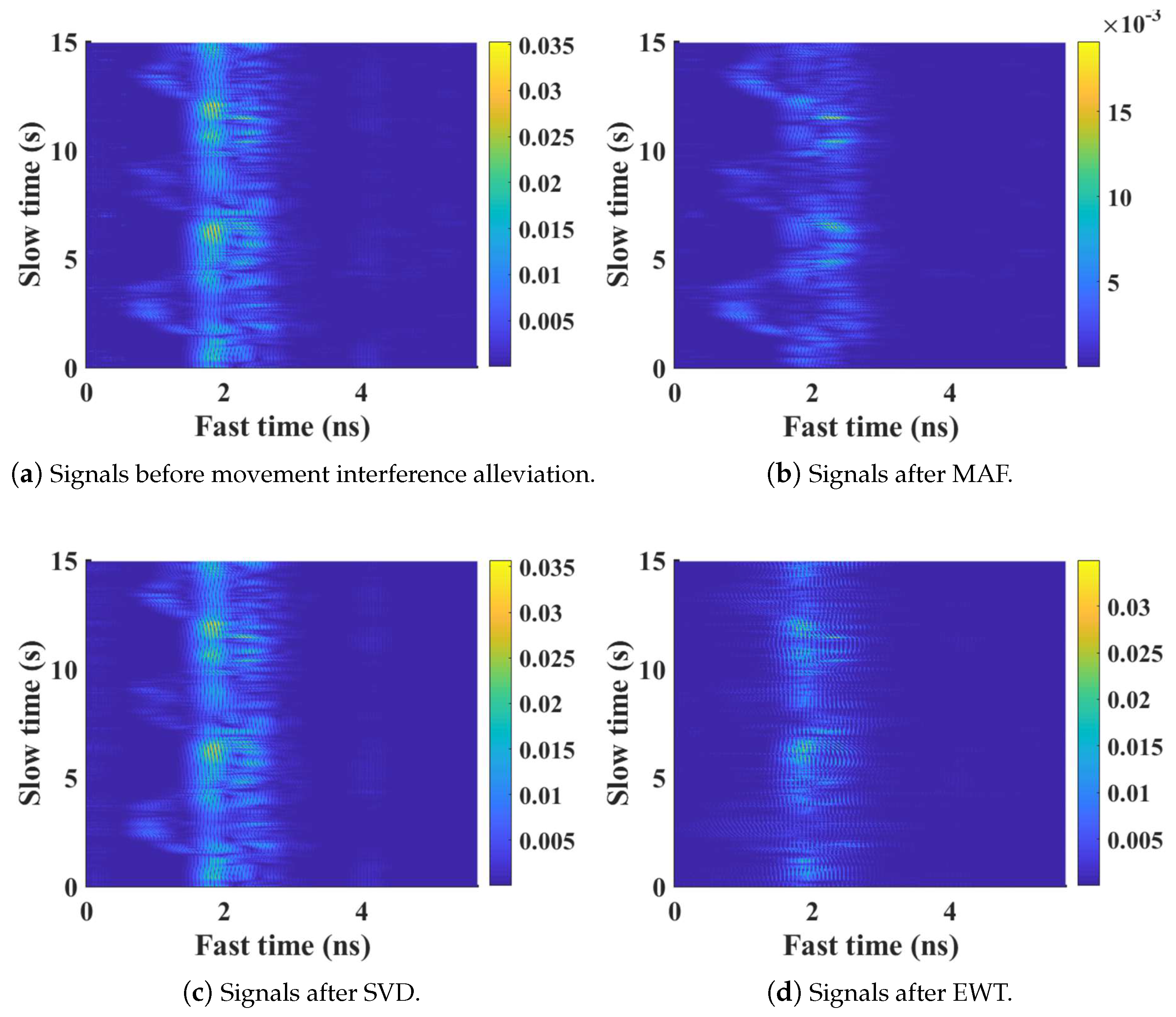
4.1. Movement Interference Alleviation Performance Based on EWT
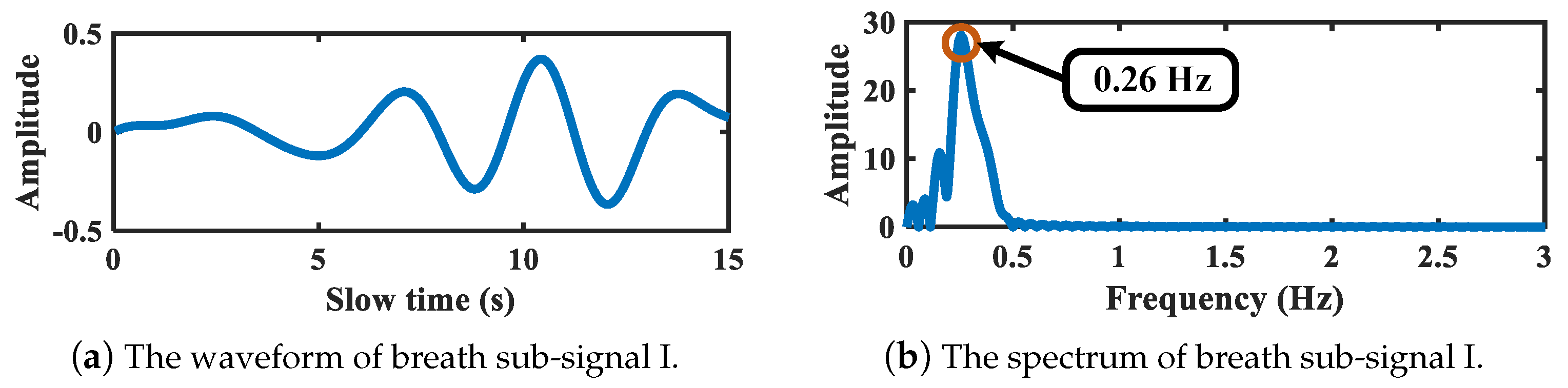
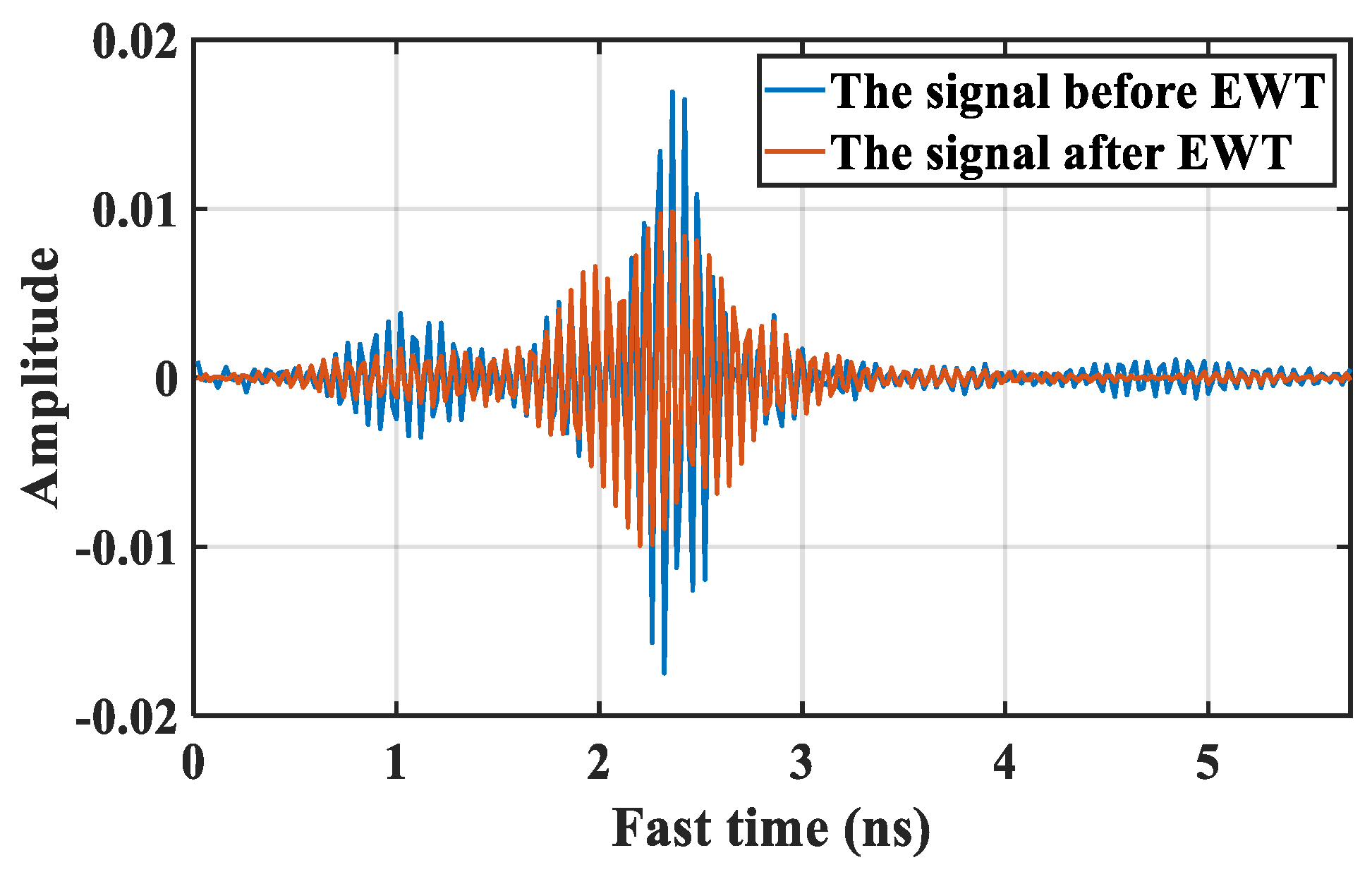
4.2. Vital Signs Sub-Signals Extraction Results Based on EWT
4.3. Evaluation on Vital Signs Estimation
4.3.1. Comparisons on Breath Estimation
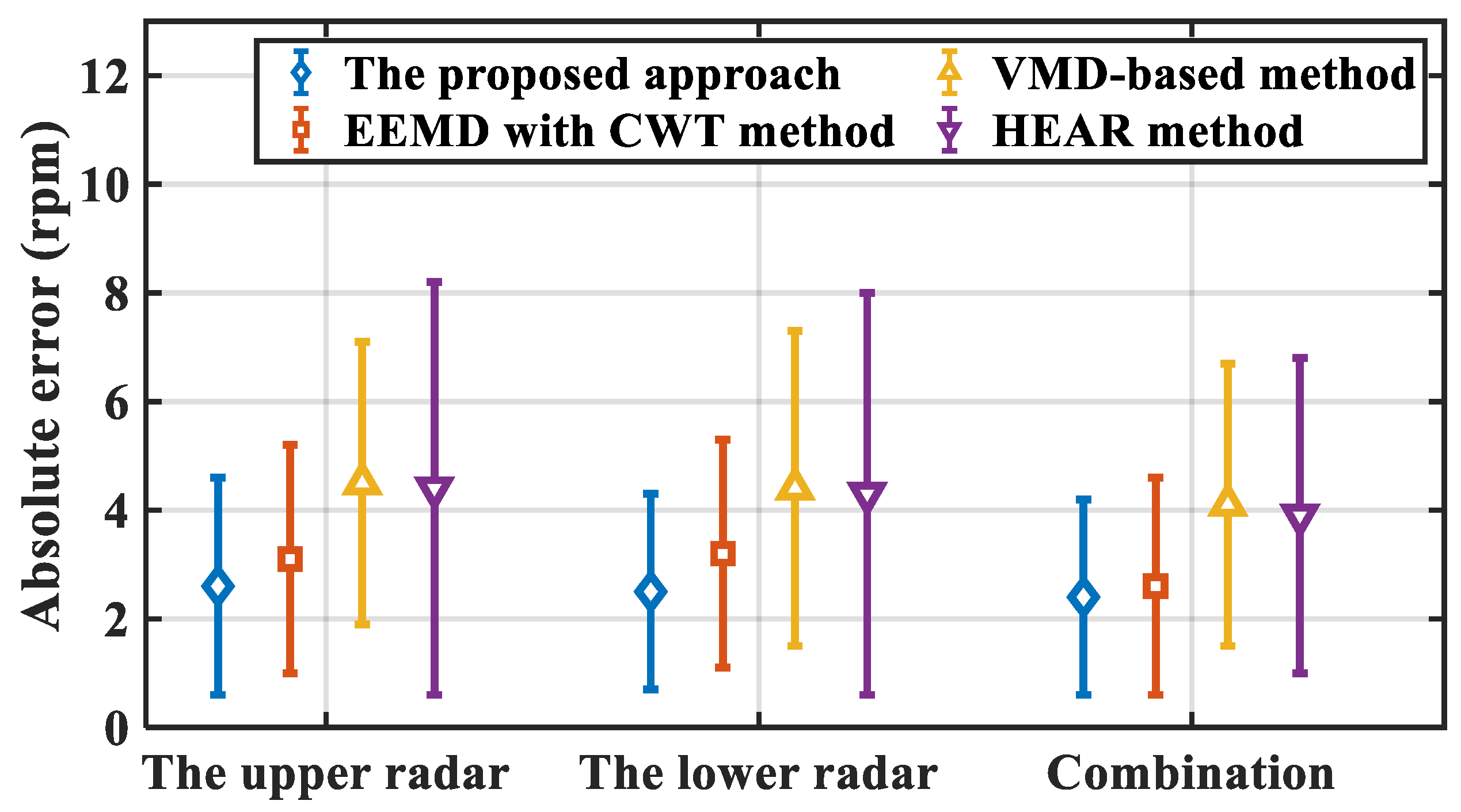
4.3.2. Comparison Results on Heartbeat Estimation
4.4. Discussions and Future Works
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harmon, K.G.; Wilson, M.G. Sudden Cardiac Death in Athletes: Incidence, Causes and Prevention Strategies. In Textbook of Sports and Exercise Cardiology; Pressler, A., Niebauer, J., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 73–94. [Google Scholar] [CrossRef]
- Zhang, Z.; Pi, Z.; Liu, B. TROIKA: A General Framework for Heart Rate Monitoring Using Wrist-Type Photoplethysmographic Signals During Intensive Physical Exercise. IEEE Trans. Biomed. Eng. 2015, 62, 522–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaroni, C.; Di Tocco, J.; Bravi, M.; Carnevale, A.; Lo Presti, D.; Sabbadini, R.; Miccinilli, S.; Sterzi, S.; Formica, D.; Schena, E. Respiratory Monitoring During Physical Activities With a Multi-Sensor Smart Garment and Related Algorithms. IEEE Sens. J. 2020, 20, 2173–2180. [Google Scholar] [CrossRef]
- Lin, Y.C.; Lin, Y.H. Step Count and Pulse Rate Detection Based on the Contactless Image Measurement Method. IEEE Trans. Multimed. 2018, 20, 2223–2231. [Google Scholar] [CrossRef]
- Procházka, A.; Charvátová, H.; Vaseghi, S.; Vysata, O. Machine Learning in Rehabilitation Assessment for Thermal and Heart Rate Data Processing. IEEE Trans. Neural Syst. Rehabil. 2018, 26, 1209–1214. [Google Scholar] [CrossRef]
- Iwata, Y.; Thanh, H.T.; Sun, G.; Ishibashi, K. High Accuracy Heartbeat Detection from CW-Doppler Radar Using Singular Value Decomposition and Matched Filter. Sensors 2021, 21, 3588. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Lin, J. Fast Acquisition of Heart Rate in Noncontact Vital Sign Radar Measurement Using Time-Window-Variation Technique. IEEE Trans. Instrum. Meas. 2016, 65, 112–122. [Google Scholar] [CrossRef]
- Cardillo, E.; Caddemi, A. Radar Range-Breathing Separation for the Automatic Detection of Humans in Cluttered Environments. IEEE Sens. J. 2021, 21, 14043–14050. [Google Scholar] [CrossRef]
- Lv, W.; He, W.; Lin, X.; Miao, J. Non-Contact Monitoring of Human Vital Signs Using FMCW Millimeter Wave Radar in the 120 GHz Band. Sensors 2021, 21, 2732. [Google Scholar] [CrossRef]
- Choi, H.I.; Song, W.J.; Song, H.; Shin, H.C. Selecting Target Range with Accurate Vital Sign Using Spatial Phase Coherency of FMCW Radar. Appl. Sci. 2021, 11, 4514. [Google Scholar] [CrossRef]
- Turppa, E.; Kortelainen, J.M.; Antropov, O.; Kiuru, T. Vital Sign Monitoring Using FMCW Radar in Various Sleeping Scenarios. Sensors 2020, 20, 6505. [Google Scholar] [CrossRef]
- Khan, F.; Ghaffar, A.; Khan, N.; Cho, S.H. An Overview of Signal Processing Techniques for Remote Health Monitoring Using Impulse Radio UWB Transceiver. Sensors 2020, 20, 2479. [Google Scholar] [CrossRef]
- Shen, H.; Xu, C.; Yang, Y.; Sun, L.; Cai, Z.; Bai, L.; Clancy, E.; Huang, X. Respiration and Heartbeat Rates Measurement Based on Autocorrelation Using IR-UWB Radar. IEEE Trans. Circuits Syst. II Express Briefs 2018, 65, 1470–1474. [Google Scholar] [CrossRef]
- Hu, X.; Jin, T. Short-Range Vital Signs Sensing Based on EEMD and CWT Using IR-UWB Radar. Sensors 2016, 16, 2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Park, J.Y.; Choi, Y.W.; Park, H.K.; Cho, S.H.; Cho, S.H.; Lim, Y.H. A Novel Non-contact Heart Rate Monitor Using Impulse-Radio Ultra-Wideband (IR-UWB) Radar Technology. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Shyu, K.K.; Chiu, L.J.; Lee, P.L.; Tung, T.H.; Yang, S.H. Detection of Breathing and Heart Rates in UWB Radar Sensor Data Using FVPIEF-Based Two-Layer EEMD. IEEE Sens. J. 2019, 19, 774–784. [Google Scholar] [CrossRef]
- Le, M.; Nguyen, B.V. Multivariate Correlation of Higher Harmonics for Heart Rate Remote Measurement Using UWB Impulse Radar. IEEE Sens. J. 2020, 20, 1859–1866. [Google Scholar] [CrossRef]
- Wang, D.; Yoo, S.; Cho, S.H. Experimental Comparison of IR-UWB Radar and FMCW Radar for Vital Signs. Sensors 2020, 20, 6695. [Google Scholar] [CrossRef] [PubMed]
- Cardillo, E.; Caddemi, A. A Review on Biomedical MIMO Radars for Vital Sign Detection and Human Localization. Electronics 2020, 9, 1497. [Google Scholar] [CrossRef]
- Li, Z.; Jin, T.; Dai, Y.; Song, Y. Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar. Remote Sens. 2021, 13, 2905. [Google Scholar] [CrossRef]
- Cardillo, E.; Li, C.; Caddemi, A. Vital Sign Detection and Radar Self-Motion Cancellation Through Clutter Identification. IEEE Trans. Microw. Theory Tech. 2021, 69, 1932–1942. [Google Scholar] [CrossRef]
- Yan, J.; Zhang, G.; Hong, H.; Chu, H.; Li, C.; Zhu, X. Phase-Based Human Target 2-D Identification With a Mobile FMCW Radar Platform. IEEE Trans. Microw. Theory Tech. 2019, 67, 5348–5359. [Google Scholar] [CrossRef]
- Quirk, S.; Becker, N.; Smith, W. External respiratory motion analysis and statistics for patients and volunteers. J. Appl. Clin. Med Phys. 2013, 14, 90–101. [Google Scholar] [CrossRef]
- Lee, Y.S.; Pathirana, P.N.; Steinfort, C.L.; Caelli, T. Monitoring and Analysis of Respiratory Patterns Using Microwave Doppler Radar. IEEE J. Transl. Eng. Health Med. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; He, Z.; Fu, Y.; Li, L.; Jiang, K.; Xie, F. Noncontact detection of respiration rate based on forward scatter radar. Sensors 2019, 19, 4778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, C.; Li, C. Assessment of human respiration patterns via noncontact sensing using Doppler multi-radar system. Sensors 2015, 15, 6383–6398. [Google Scholar] [CrossRef] [Green Version]
- Kagawa, M.; Tojima, H.; Matsui, T. Non-contact diagnostic system for sleep apnea–hypopnea syndrome based on amplitude and phase analysis of thoracic and abdominal Doppler radars. Med. Biol. Eng. Comput. 2016, 54, 789–798. [Google Scholar] [CrossRef]
- Gu, C.; Li, R.; Zhang, H.; Fung, A.Y.; Torres, C.; Jiang, S.B.; Li, C. Accurate respiration measurement using DC-coupled continuous-wave radar sensor for motion-adaptive cancer radiotherapy. IEEE Trans. Biomed. Eng. 2012, 59, 3117–3123. [Google Scholar] [CrossRef]
- Lazaro, A.; Girbau, D.; Villarino, R. Techniques for clutter suppression in the presence of body movements during the detection of respiratory activity through UWB radars. Sensors 2014, 14, 2595–2618. [Google Scholar] [CrossRef]
- Khan, F.; Cho, S.H. A detailed algorithm for vital sign monitoring of a stationary/non-stationary human through IR-UWB radar. Sensors 2017, 17, 290. [Google Scholar] [CrossRef] [Green Version]
- Seong, L.; Faheem, K.; Sung, C. Vital Sign Monitoring and Mobile Phone Usage Detection Using IR-UWB Radar for Intended Use in Car Crash Prevention. Sensors 2017, 17, 1240. [Google Scholar]
- Shang, X.; Liu, J.; Li, J. Multiple Object Localization and Vital Sign Monitoring Using IR-UWB MIMO Radar. IEEE Trans. Aerosp. Electron. Syst. 2020, 56, 4437–4450. [Google Scholar] [CrossRef]
- Shyu, K.K.; Chiu, L.J.; Lee, P.L.; Lee, L.H. UWB Simultaneous Breathing and Heart Rate Detections in Driving Scenario Using Multi-Feature Alignment Two-Layer EEMD Method. IEEE Sens. J. 2020, 20, 10251–10266. [Google Scholar] [CrossRef]
- Rong, Y.; Dutta, A.; Chiriyath, A.; Bliss, D.W. Motion-Tolerant Non-Contact Heart-Rate Measurements from Radar Sensor Fusion. Sensors 2021, 21, 1774. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Yang, X.; Li, L.; Zhang, L.; Kitsuwan, N.; Oki, E. HEAR: Approach for Heartbeat Monitoring with Body Movement Compensation by IR-UWB Radar. Sensors 2018, 18, 3077. [Google Scholar] [CrossRef] [Green Version]
- Andersen, N.; Granhaug, K.; Michaelsen, J.A.; Bagga, S.; Hjortland, H.A.; Knutsen, M.R.; Lande, T.S.; Wisland, D.T. A 118-mW Pulse-Based Radar SoC in 55-nm CMOS for Non-Contact Human Vital Signs Detection. IEEE J. Solid-State Circuits 2017, 52, 3421–3433. [Google Scholar] [CrossRef]
- Nosrati, M.; Tavassolian, N. High-Accuracy Heart Rate Variability Monitoring Using Doppler Radar Based on Gaussian Pulse Train Modeling and FTPR Algorithm. IEEE Trans. Microw. Theory Tech. 2018, 66, 556–567. [Google Scholar] [CrossRef]
- Bao, R.; Yang, Z. CNN-Based Regional People Counting Algorithm Exploiting Multi-Scale Range-Time Maps With an IR-UWB Radar. IEEE Sens. J. 2021, 21, 13704–13713. [Google Scholar] [CrossRef]
- Gilles, J. Empirical wavelet transform. IEEE Trans. Signal Process. 2013, 61, 3999–4010. [Google Scholar] [CrossRef]
- He, M.; Nian, Y.; Xu, L.; Qiao, L.; Wang, W. Adaptive separation of respiratory and heartbeat signals among multiple people based on empirical wavelet transform using uwb radar. Sensors 2020, 20, 4913. [Google Scholar] [CrossRef]
- Katiyar, R.; Gupta, V.; Pachori, R.B. Fbse-ewt-based approach for the determination of respiratory rate from ppg signals. IEEE Sens. Lett. 2019, 3, 1–4. [Google Scholar] [CrossRef]
- Liu, W.; Chen, W. Recent Advancements in Empirical Wavelet Transform and Its Applications. IEEE Access 2019, 7, 103770–103780. [Google Scholar] [CrossRef]
- Liang, X.; Zhang, H.; Ye, S.; Fang, G.; Gulliver, T.A. Improved denoising method for through-wall vital sign detection using UWB impulse radar. Digit. Signal Process. 2017, 74, 72–93. [Google Scholar] [CrossRef]
- Ding, C.; Yan, J.; Zhang, L.; Zhao, H.; Hong, H.; Zhu, X. Noncontact Multiple Targets Vital Sign Detection Based on VMD Algorithm; IEEE: Piscataway, NJ, USA, 2017; pp. 0727–0730. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
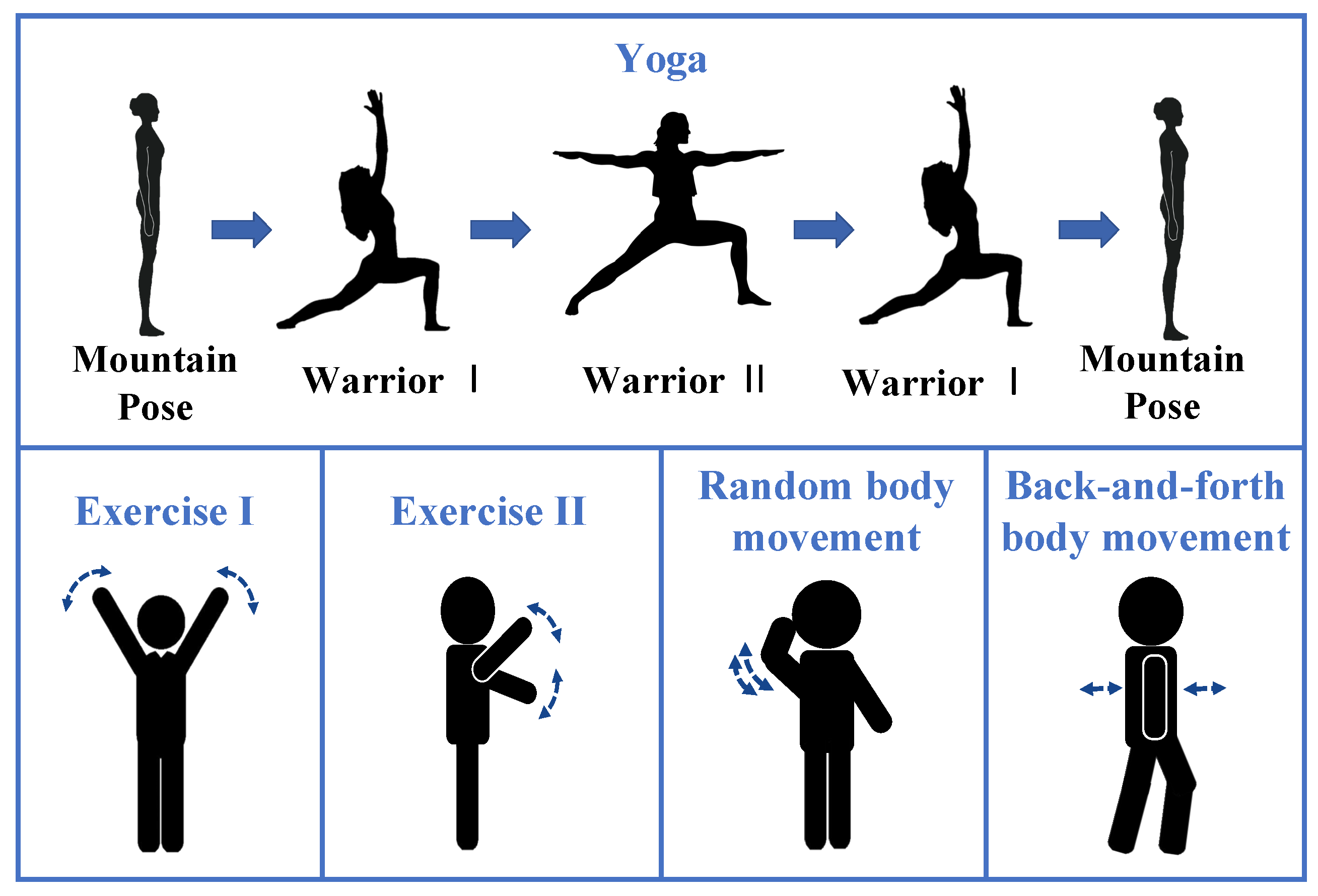
| Activities | Description |
|---|---|
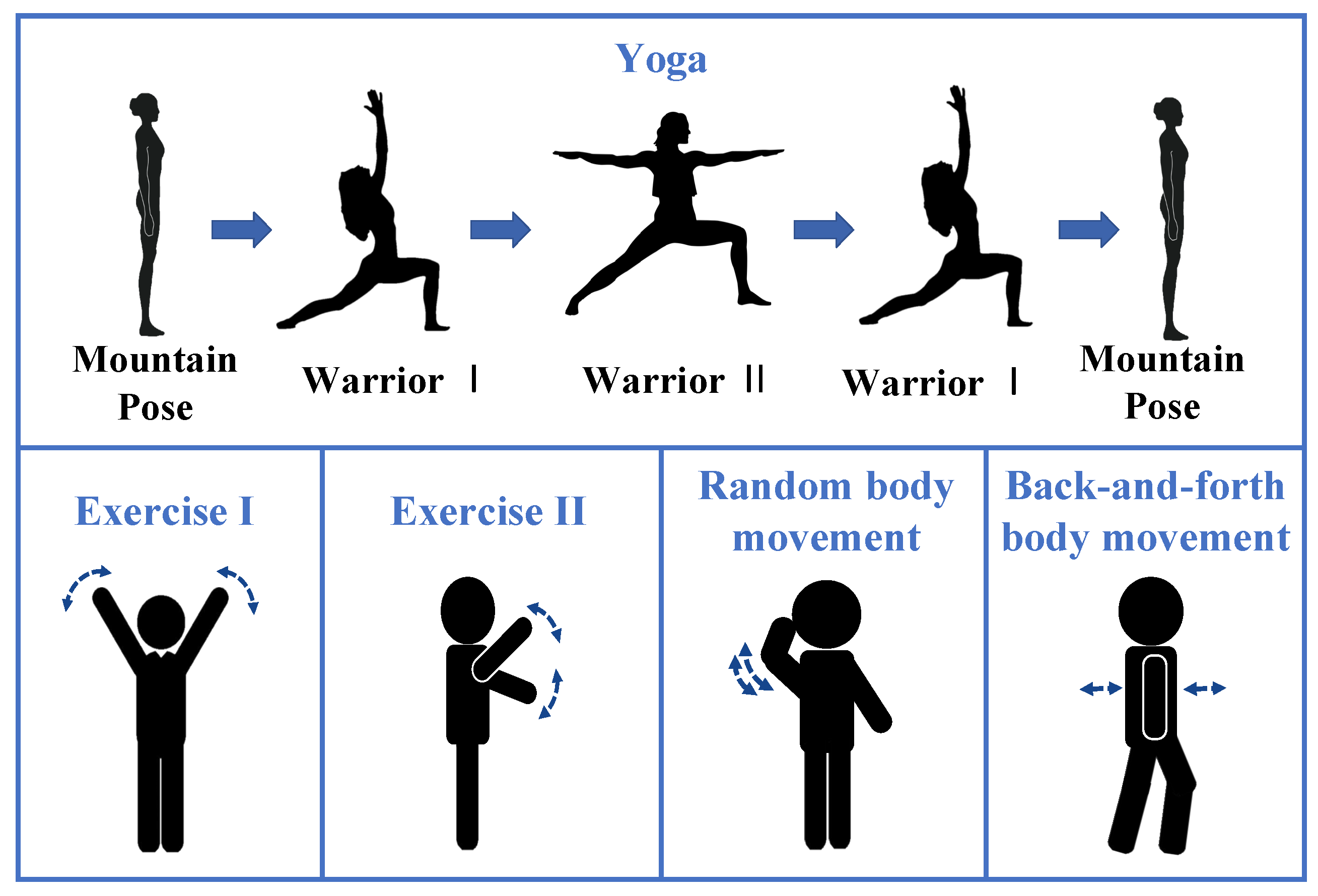
| Yoga | Move gently and switch among three yoga poses, including the Mountain Pose, the Warrior I, and the Warrior II. Stretch body and hold a few seconds at each yoga pose. |
| Exercise I | Keep the body upright, wave arms up and down from both sides of the body repeatedly. |
| Exercise II | Keep the body upright, wave arms up and down from the front of the body repeatedly. |
| Random body movement | Engage some daily activities in the detection area such as making a phone call, scratching head, adjusting glasses. |
| Back-and-forth body movement | Waggle the upper body back and forth repeatedly. |
| Participant | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Gender | Female | Female | Female | Female | Male | Male | Male | Male |
| Age (year) | 24 | 22 | 23 | 24 | 23 | 24 | 28 | 23 |
| Height (m) | 1.63 | 1.67 | 1.60 | 1.58 | 1.87 | 1.70 | 1.74 | 1.86 |
| Weight (kg) | 54 | 51 | 53 | 52 | 83 | 52 | 68 | 95 |
| SMIR after MAF | SMIR after SVD | SMIR after EWT | |
|---|---|---|---|
| The upper radar | 3.4 | 20.5 | 25.3 |
| The lower radar | 3.3 | 14.2 | 16.6 |
| Participant | Breath Rate Absolute Error | Heart Rate Accuracy | ||
|---|---|---|---|---|
| Avg (rpm) | Std (rpm) | Avg (%) | Std (%) | |
| 1 | 2.6 | 1.7 | 86.5 | 11.6 |
| 2 | 2.2 | 1.8 | 87.7 | 8.9 |
| 3 | 2.3 | 1.8 | 88.6 | 8.5 |
| 4 | 2.6 | 1.7 | 87.2 | 8.1 |
| 5 | 2.2 | 1.8 | 86.7 | 9.1 |
| 6 | 2.7 | 1.9 | 84.7 | 11.1 |
| 7 | 1.9 | 1.7 | 87.6 | 9.5 |
| 8 | 2.4 | 1.7 | 88.0 | 7.4 |
| Average | 2.3 | 1.8 | 86.9 | 9.8 |
| Activities | Breath Rate Absolute Error | Heart Rate Accuracy | ||
|---|---|---|---|---|
| Avg (rpm) | Std (rpm) | Avg (%) | Std (%) | |
| Exercise I | 2.1 | 1.8 | 86.3 | 9.7 |
| Exercise II | 2.2 | 1.8 | 86.0 | 10.8 |
| Yoga | 2.4 | 1.9 | 86.4 | 10.8 |
| Random body movement | 2.6 | 1.7 | 86.4 | 9.9 |
| Back-and-forth body movement | 2.6 | 2.0 | 88.1 | 9.0 |
| Breath Rate Absolute Error (rpm) | Heart Rate Accuracy (%) | Computation Time (s) | |
|---|---|---|---|
| 7-s window | 2.8 | 84.4 | 0.43 |
| 10-s window | 2.9 | 85.6 | 0.53 |
| 15-s window | 2.3 | 86.9 | 0.79 |
| 18-s window | 2.5 | 86.6 | 0.92 |
| Approach | Accuracy | |
|---|---|---|
| HEAR method | 79.0% | |
| The upper radar | VMD-based method | 80.0% |
| EEMD with CWT method | 80.9% | |
| The proposed approach | 81.6% | |
| Combinaton | The proposed approach | 86.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Yang, X.; Ding, Y.; Wang, Y.; Zhou, J.; Zhang, L. Contactless Simultaneous Breathing and Heart Rate Detections in Physical Activity Using IR-UWB Radars. Sensors 2021, 21, 5503. https://doi.org/10.3390/s21165503
Zhang X, Yang X, Ding Y, Wang Y, Zhou J, Zhang L. Contactless Simultaneous Breathing and Heart Rate Detections in Physical Activity Using IR-UWB Radars. Sensors. 2021; 21(16):5503. https://doi.org/10.3390/s21165503
Chicago/Turabian StyleZhang, Xinyue, Xiuzhu Yang, Yi Ding, Yili Wang, Jialin Zhou, and Lin Zhang. 2021. "Contactless Simultaneous Breathing and Heart Rate Detections in Physical Activity Using IR-UWB Radars" Sensors 21, no. 16: 5503. https://doi.org/10.3390/s21165503
APA StyleZhang, X., Yang, X., Ding, Y., Wang, Y., Zhou, J., & Zhang, L. (2021). Contactless Simultaneous Breathing and Heart Rate Detections in Physical Activity Using IR-UWB Radars. Sensors, 21(16), 5503. https://doi.org/10.3390/s21165503