1. Introduction
Osteoarthritis (OA) is one of the main musculoskeletal disorders that causes disability in people over 60 years of age [
1]. Symptomatic OA causes pain, joint stiffness, swelling and difficulties performing activities in daily life [
1]. The joint that is most often affected is the knee, followed by the hip. These are two large, weight-bearing joints of the lower extremities that are crucial for locomotion [
1]. OA is a multifactorial disease in which mechanical factors play an essential role [
2,
3,
4,
5,
6,
7]. The conventional treatment of OA patients consists of education, the promotion of an active and healthy lifestyle, medication, exercise therapy [
8] and—as a last resort—a total joint arthroplasty [
9]. Previous research has shown that inactivity is a predictor for increased OA symptoms and poor general health, which indicates that people with OA should be more active [
10]. It has been shown that exercise therapy and sports reduce pain and increase muscle strength, joint stability, physical function and overall health [
11,
12]. Thus, there should be a balance between the imposed loading on the joint and the person’s ability to carry a load [
12]. Furthermore, each daily activity imposes a different mechanical load on joints [
13,
14]. Therefore, it seems relevant for health-care practitioners to gain insights into and monitor a patient’s functional status—i.e., activity profile—in combination with their joint loading in a free-living environment. State-of-the-art biomechanical modeling tools based on integrated 3D motion capture in a laboratory setting can quantify joint loading. However, access to these tools and the need for expert operators limits the accessibility of measuring joint loading in a clinical setting.
Over the last decade, the use of mobile technology has increased exponentially [
15], and smartphones have become an integral part of people’s lives [
16]. Although interesting work has been presented on the use of technology to support the elderly in performing exercises, such as the Nintendo Wii or Microsoft Kinect (e.g., [
17]), our paper focuses on the use of smartphones or Inertial Measurement Units (IMU) to enhance the uptake of physical activities in daily life. Smartphones allow users to engage with information in any environment at any time. Furthermore, they are equipped with technologies such as a tri-axial accelerometer, tri-axial gyroscope and a magnetometer (IMUs), and they can therefore monitor physical activity by accessing these sensors and combining their information in a smartphone application [
18]. Furthermore, the graphical interface of applications (apps) allows tailored feedback, social interaction, personalized goal setting and self-monitoring [
19,
20], which might help with the commencement and maintenance of physical activity [
21].
However, starting and maintaining physical activity in order to increase healthy behavior is challenging [
21,
22]. Results show that the positive effects of exercise in people with OA only last as long as exercise is continued [
22]. Unfortunately, reasons such as forgetfulness, boredom, lack of enjoyment and lack of confidence are cited as reasons to stop exercising [
22]. Interventions that promote exercise using only app-based feedback peak in the first few months, and adherence to the exercise plan dwindles over time [
18]. Thus, while smartphone apps increase self-monitoring through direct feedback and goal setting, they lack the social support and controlling function provided by a health-care professional [
23]. Considering that supervision facilitates the adherence to exercise interventions [
22], an app-based approach alone might not be sufficient. Furthermore, OA patients highlighted that contact with a therapist [
20] or peers [
23] throughout the intervention is essential for motivation and to receive corrective feedback and reassurance. Moreover, older adults (with a lack of motivation to use technology) and people with comorbidities (who experience more physical discomfort during activities) might need the personal approach of face-to-face therapy sessions [
24] as opposed to solely relying on app-based interventions. In such cases, a blended care approach (the combination of mobile technology with conventional therapy) might be more useful. Over the last decade, more researchers have become focused on applying technology in a rehabilitation setting to enhance physical activity in people with OA and have indicated success in that regard [
24,
25]. However, to the best of our knowledge, no app to date incorporates mechanical loading on the joint (i.e., joint loading in terms of contact forces) during activities of daily life. Therefore, we aim to add an estimate of the cumulative joint loading based on the recognition of the performed activity during daily life for people suffering from hip or knee OA.
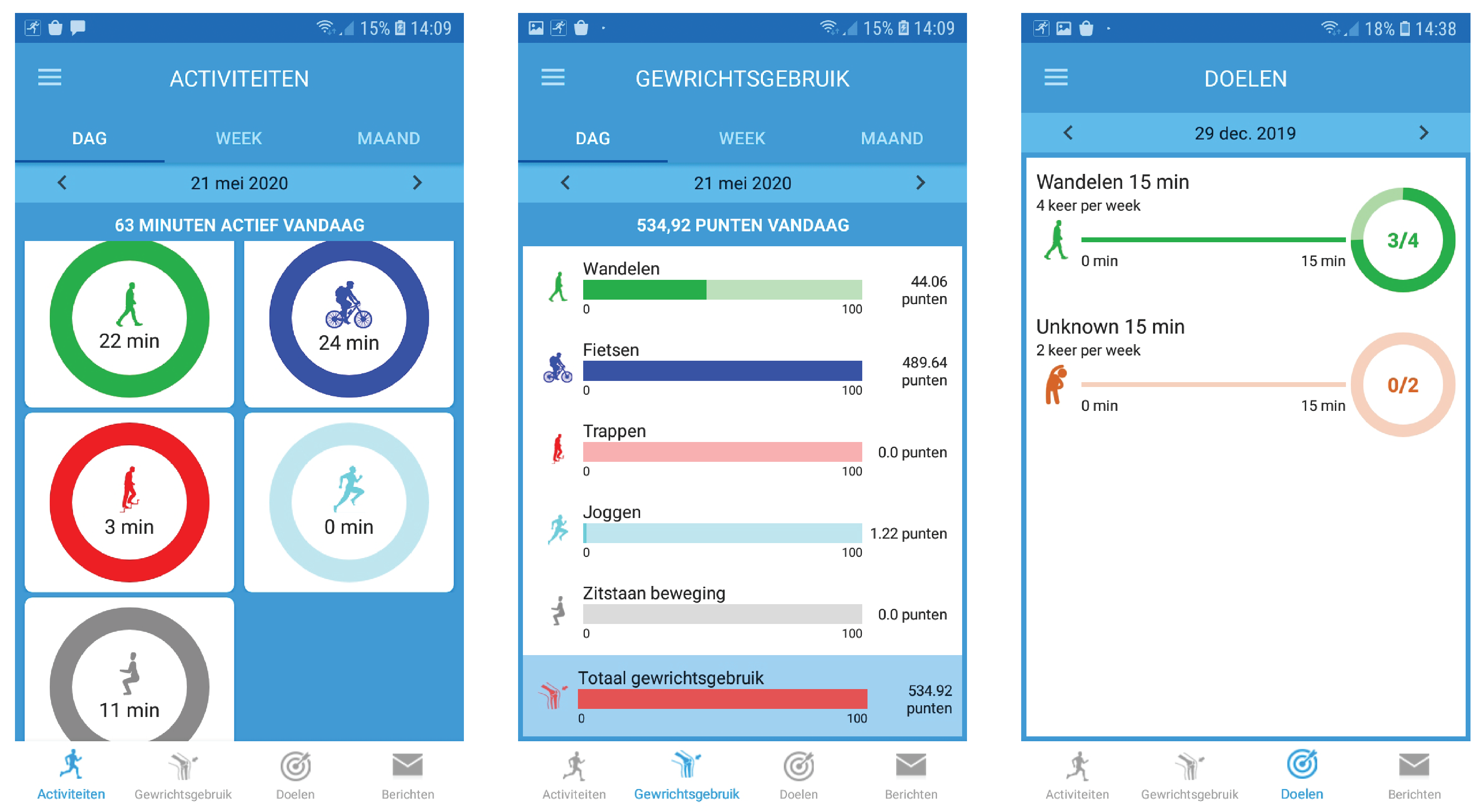
We propose the concept and design of a novel blended care app called JOLO (Joint Load) that combines free-living information on activity with lab-based measures of joint loading to estimate functional status. As such, JOLO aims to provide a better overview of a patient’s functional status. Subsequently, the patient’s rehabilitation strategies can be further optimized. For that purpose, we deploy JOLO on the readily available smartphones of patients and provide a clinical dashboard for therapists (accessible on their PC or smartphone). Within this study, we report the development and the evaluation of the usability, feasibility and credibility of the JOLO app.
4. Discussion
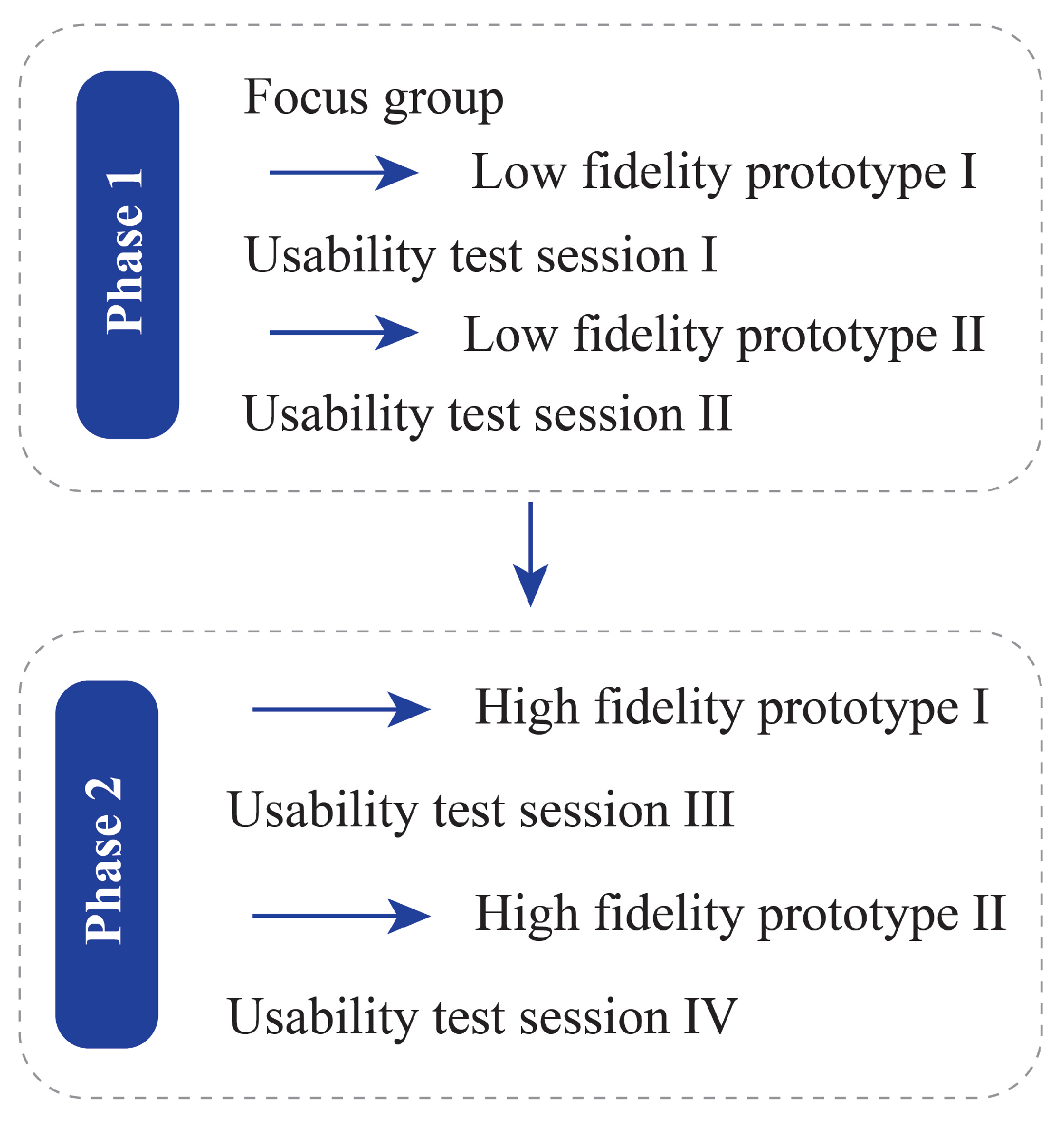
In this study, we aimed to introduce a novel blended care app called JOLO (Joint Load) for health-care professionals and subjects suffering from OA to optimize their rehabilitation. JOLO combines information from activity recognition in a free-living environment with the joint contact force information collected in a lab-based setting to estimate a patient’s functional status in terms of activity and joint loading in a free-living environment. End-users tested JOLO using an iterative design process in which the end-users provided essential information for the further development of the JOLO app. Based on the results of this study, we can conclude that JOLO is promising but still needs improvement before OA patients and therapists can use it in a rehabilitation setting.
During the last stage of prototype testing, we found that the main issues with the JOLO smartphone app and dashboard were not related to its usability but to its utility. The utility consists of the functionalities of a system—whether it does what it was designed for and whether it facilitates the users’ job [
44]. For the smartphone app, the users indicated that some functionalities of the system were not working correctly. The subjects that used JOLO for seven days in a free-living environment indicated that there was an excessive overestimation of the time spent “cycling”. Considering that technical difficulties are in general identified as a vital barrier for the effective use of and satisfaction with technology [
45], improving the predictive performance of the activity recognition module should be guaranteed in future prototype versions. Currently, every second of the day is allocated to a specific activity or to “unknown”. To reduce the errors of allocation, it is probably more appropriate to opt for allocation based on a combination of acceleration data and logical reasoning. If, for example, “cycling” is predicted for a short amount of time, followed by “stationary” for a more extended period, it is unlikely that a short cycling bout took place. In such a case, it is more appropriate to change the short amount of time allocated to “cycling” to “stationary”. Furthermore, the training data in our machine learning pipeline were mostly collected from healthy and slightly younger individuals without any musculoskeletal deficits. Previous work has shown that there are significant differences in movement patterns between healthy individuals and those with hip or knee OA [
46,
47]. Those differences might also induce differences in the acceleration signal, and in turn change the accuracy of the model and result in more misclassifications. This issue should be addressed in future work on the JOLO app by including data from patients with hip or knee OA to train the classification model. Another limitation of the activity recognition pipeline is the limited number of input sensors. To reduce the risk of overfitting with our relatively small dataset, we decided to keep the dimensionality of the input data low by only using the accelerometer. If more training data were made available, future work could use the other IMU sensors in the phone (i.e., gyroscope and magnetometer) to train a more accurate model. Besides the issues related to activity recognition, some participants indicated that the hip bag used to wear the smartphone was too small, and thus for some patients it was uncomfortable to wear the smartphone. An essential aspect of using a device for continuous monitoring is its natural and non-intrusive integration in everyday life [
48]. Therefore, wearing an uncomfortable bag might explain some of the lower scores for behavioral intent and satisfaction. A custom made hip bag that is large enough and comfortable to wear might be a better solution than using a commercially available option.
Usefulness and ease of use have been identified as two of the primary parameters facilitating the use of mobile health by healthcare professionals [
49]. The health-care professionals indicated that the last prototype of JOLO was easy to use and easy to learn. They were furthermore interested in receiving their patients’ activity data based on multiple activities in a home environment. One of the main issues with physical activity prescription for health-care professionals lies in their inability to monitor their patients [
22]. In that sense, using JOLO might facilitate the prescription of physical activity to these patients because it allows for detailed monitoring during daily life. However, the use of JOLO currently costs more time than it saves, and as the health-care practitioners indicated, it might not be suitable for all their patients. Their concerns might be reflected in the spread of the UTAUT and USE scores of the patients (
Table A1 and
Table A2). This spread might be caused by differences in how confident the participants felt in using technology. Currently, we have treated confidence in technology use as a participant characteristic, similar to age and gender. However, the visual inspection of the scatter plot shows that there could be a correlation between the self-reported confidence in technology use and the attitude and anxiety towards using the JOLO app. Such a correlation would indicate that some people would need more guidance and training before they would become comfortable in using technological products for rehabilitation. Future work should further investigate this relationship.
Moreover, the usefulness of obtaining information and providing feedback on joint loading in a free-living environment is not yet proven. Undesirable mechanical loading plays a critical role in the onset and progression of OA [
2,
4,
50]. However, what constitutes “undesirable” mechanical loading on the joint in a free-living environment is currently unknown. Therefore, providing feedback and information on this parameter is presumptuous. For this reason, the therapists indicated that the app is usable but currently not useful. Therefore, the health-care professionals indicated that, before JOLO can be implemented in a rehabilitation setting, benchmarks for proper joint loading need to be added to the app. Furthermore, the health-care professionals also expressed their concerns regarding the accuracy of the joint loading based on group averages and indicated that more personalized methods should be implemented. Currently, the population average based on lab-based data is used as a joint loading template. However, this will induce an error when estimating the functional status of an individual. The current workflow used to calculate joint contact forces involves an extensive lab-setup and musculoskeletal modeling. It is not feasible to implement such a workflow in a rehabilitation setting to obtain an individual’s joint loading profile. Therefore, alternative methods to calculate or predict joint contact forces should be investigated so that they can be used to obtain a more personalized functional status. Previously, IMUs have been used to estimate ground reaction forces and moments (e.g., [
51,
52,
53]) and even joint contact forces (e.g., [
54,
55]) using machine learning techniques. Those results show the potential of using IMUs to obtain complex measures outside of the lab. However, more research is needed to reduce the prediction errors on the implementation within a rehabilitation setting and on the implementation of this measure in the JOLO app. Therefore, JOLO can only be implemented in a rehabilitation setting if these issues are simultaneously addressed.
Future work on the JOLO app should investigate feasible methods to estimate joint contact forces in a free-living situation using a combination of IMU sensors and machine learning techniques. These techniques will allow for more personalized joint loading templates and reduce the error in the functional status estimation. Furthermore, benchmarks for healthy joint loading should be investigated so that they can be used as a guideline for therapeutic goal setting. This can be done by exploring the differences in functional status between healthy individuals and individuals with hip or knee OA. Providing benchmarks and testing the effectiveness of the feedback that benchmarks the individual patient performance against healthy individuals or well-recovering peers should prove the usefulness of the JOLO app and facilitate its integration in rehabilitation. Moreover, to ease the natural integration in everyday life, a different carrier for the phone should be found by designing a custom made belt with skin-friendly material that is adjustable to common anthropometric measures. To do this, different types of prototypes, in terms of materials, shapes and sizes, should be created and field-tested. Furthermore, the activity recognition algorithms should be improved to reduce the amount of misclassification, possibly by adding real-life labeled data from hip and knee OA patients to the training data set.

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








