A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback

 ,
, 
Abstract
1. Introduction
1.1. Background and Problem Description: Musculoskeletal Disorder and Risk Assessments
1.2. State-of-the-Art Sensor-Based Solutions in Risk Assessments and Work Technique Training
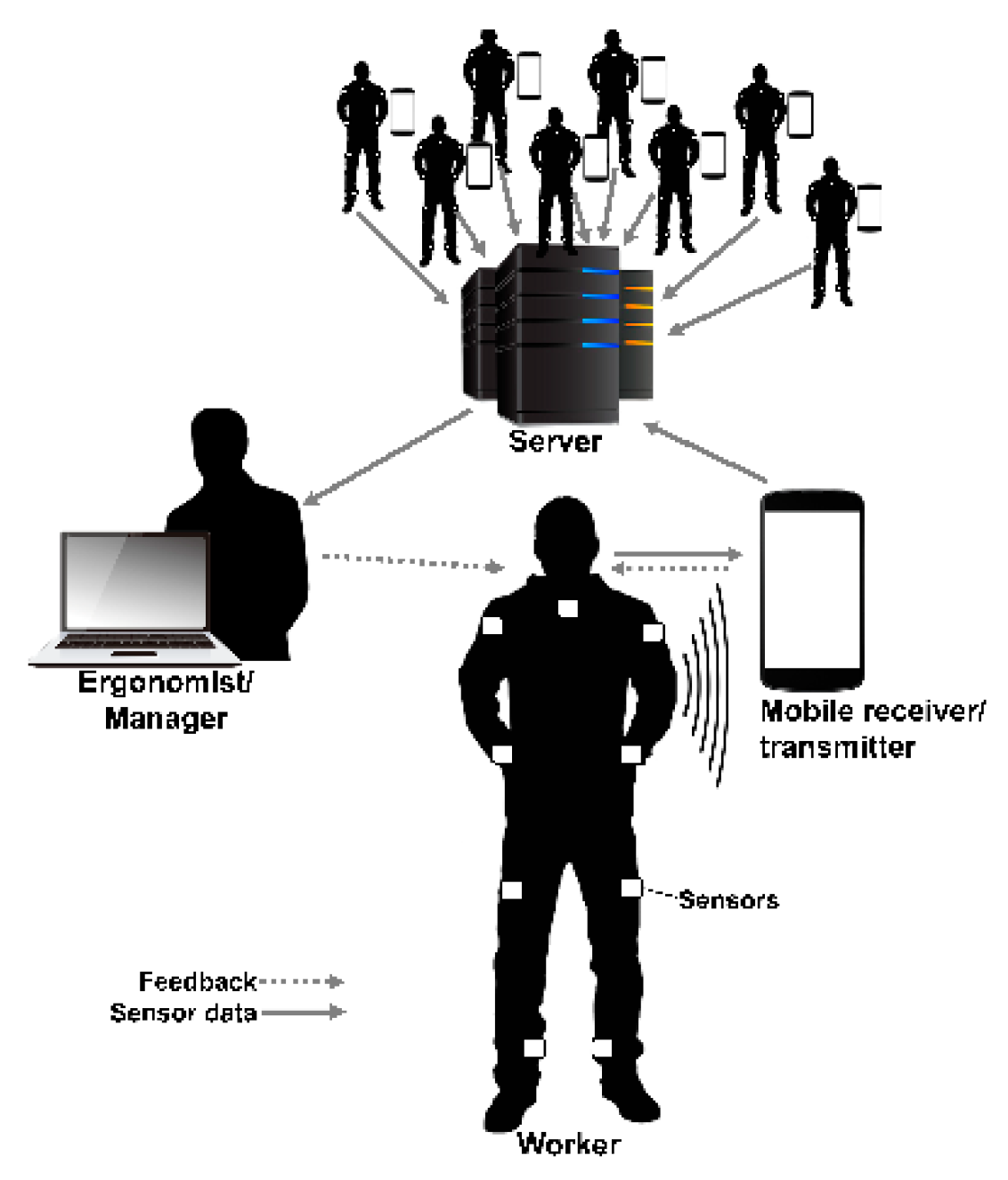
1.3. New Sensor-Based Solution for Risk Assessment and Work Technique Training: The Smart Workwear System
1.4. Aim
1.5. Article Structure
2. Methods
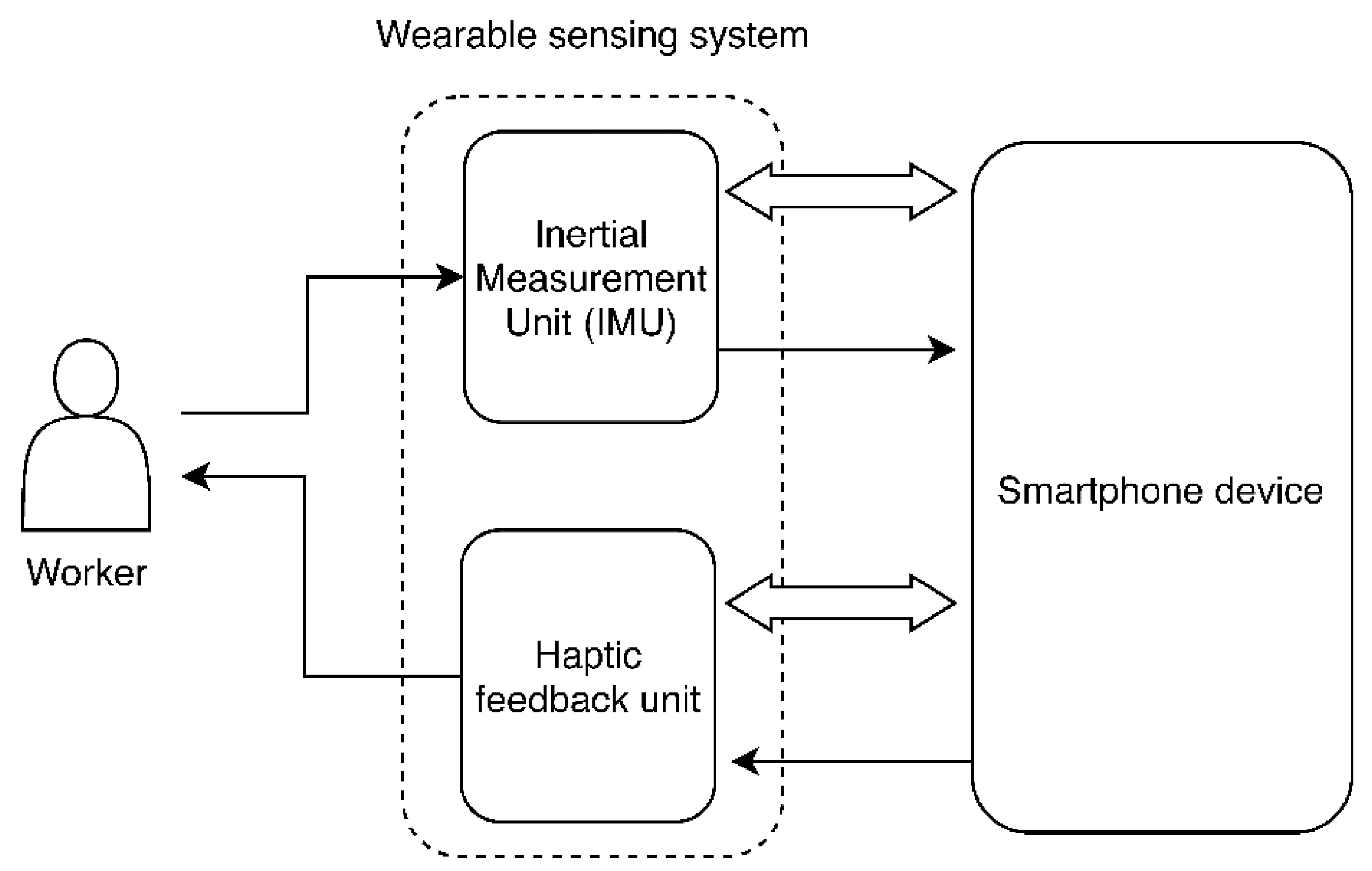
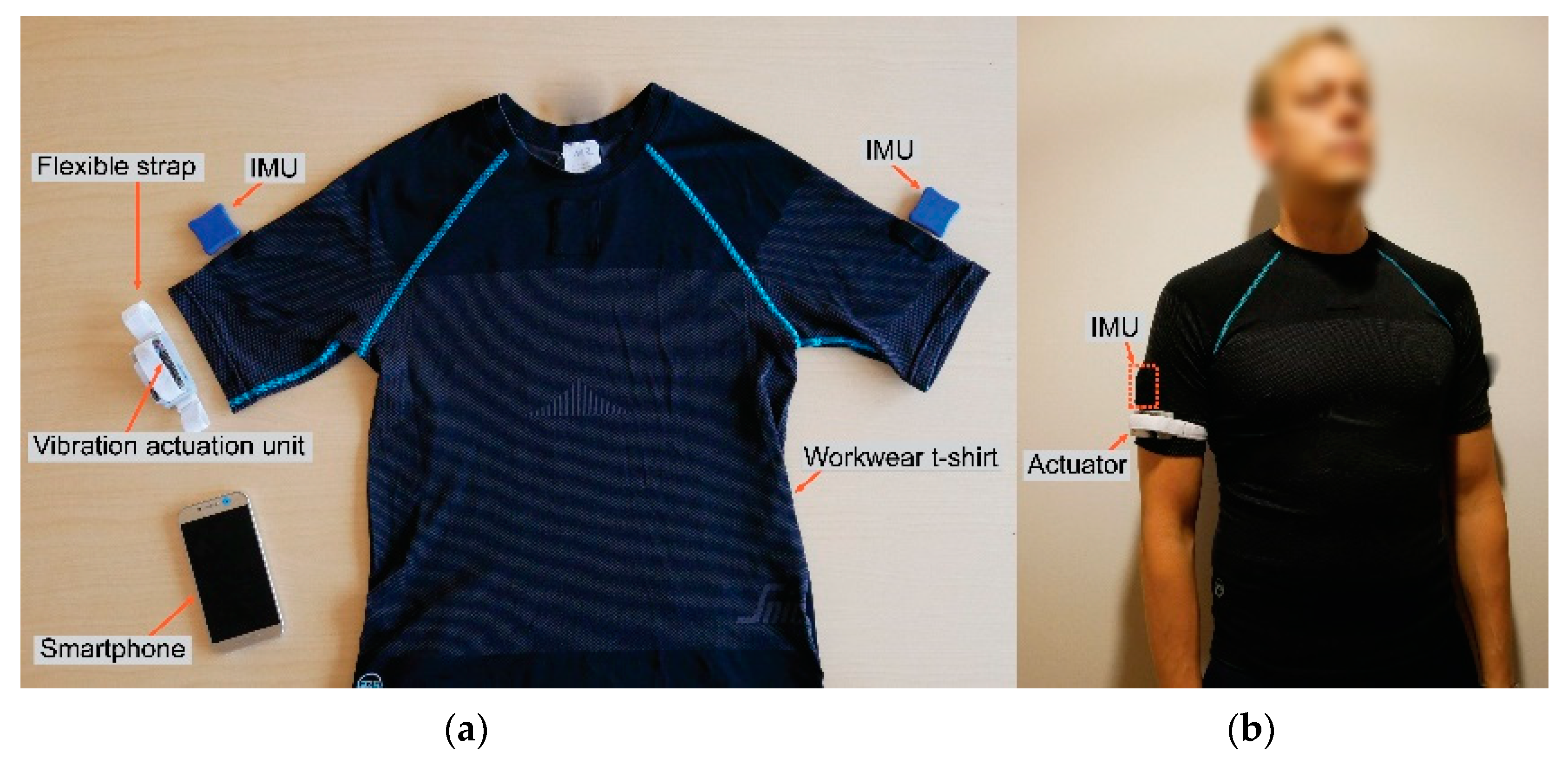
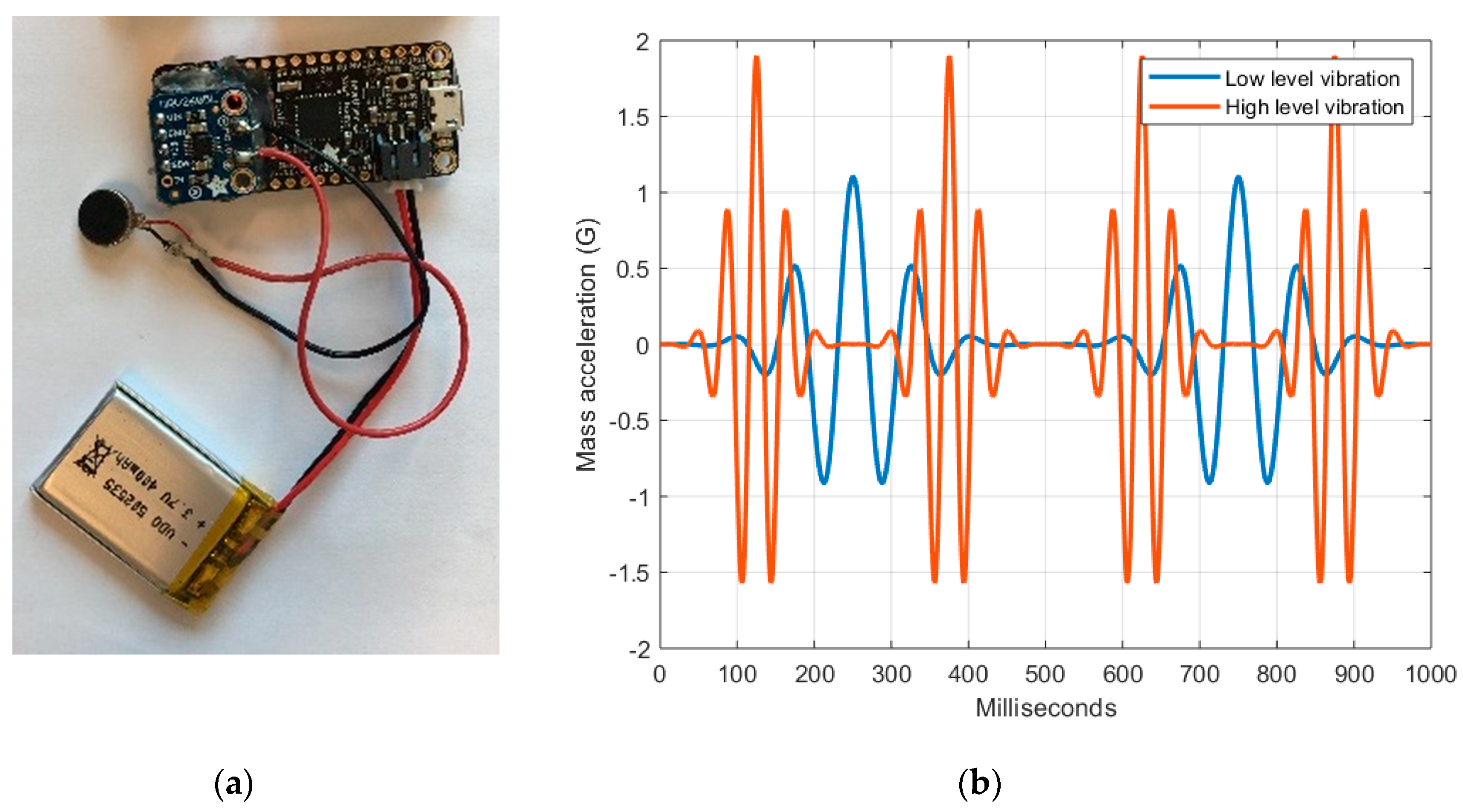
2.1. The Smart Workwear System Haptic Feedback Module
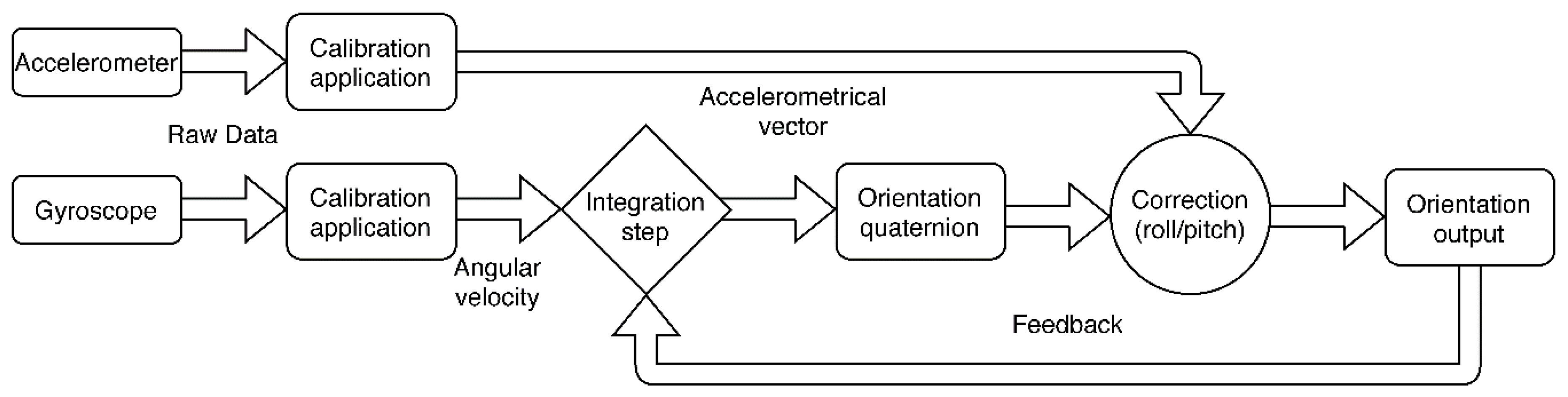
2.1.1. Inertial Measurement Unit
2.1.2. Haptic Feedback Unit
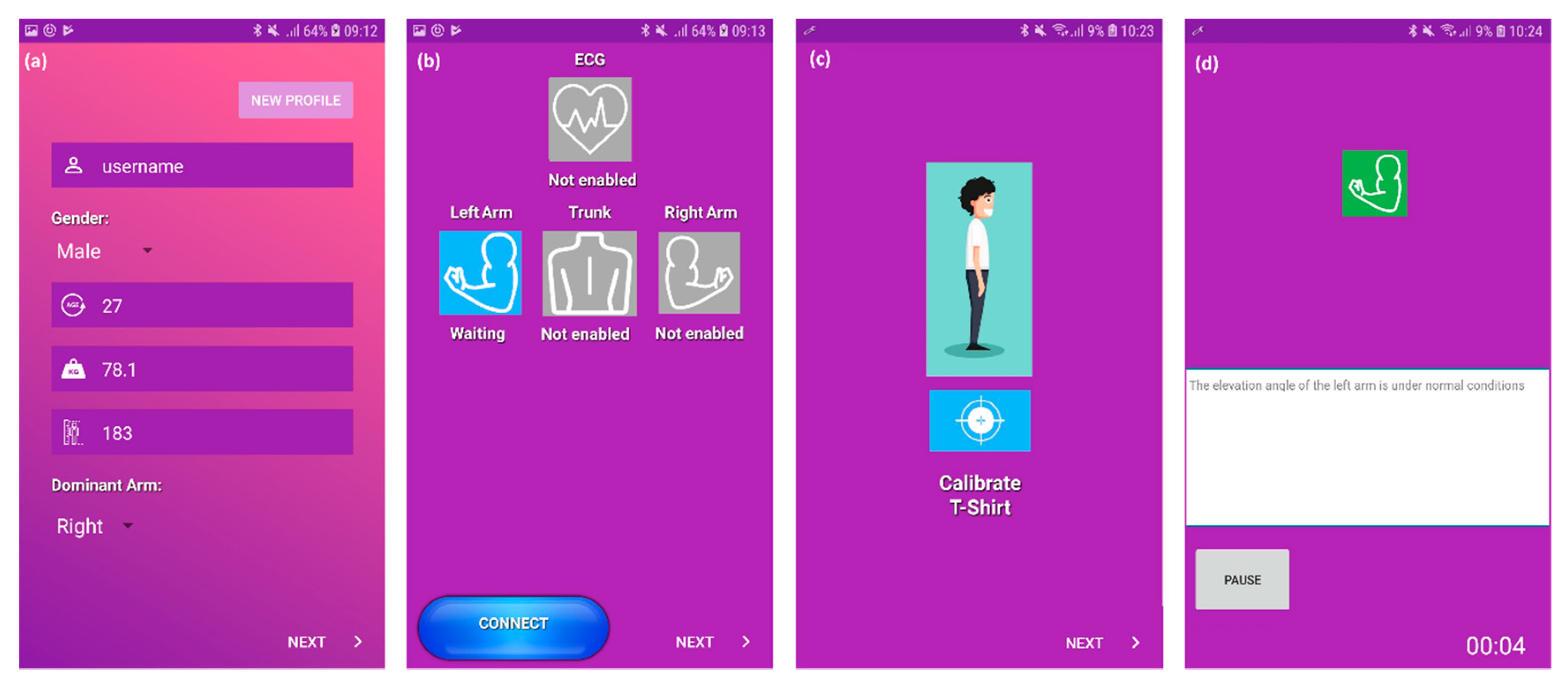
2.1.3. Data Collection and Analysis System
2.2. Test Settings
2.2.1. Participants
2.2.2. Equipment and Feedback Thresholds
2.2.3. Procedure
2.3. Statistical Analysis
3. Results from System Application and User Evaluations
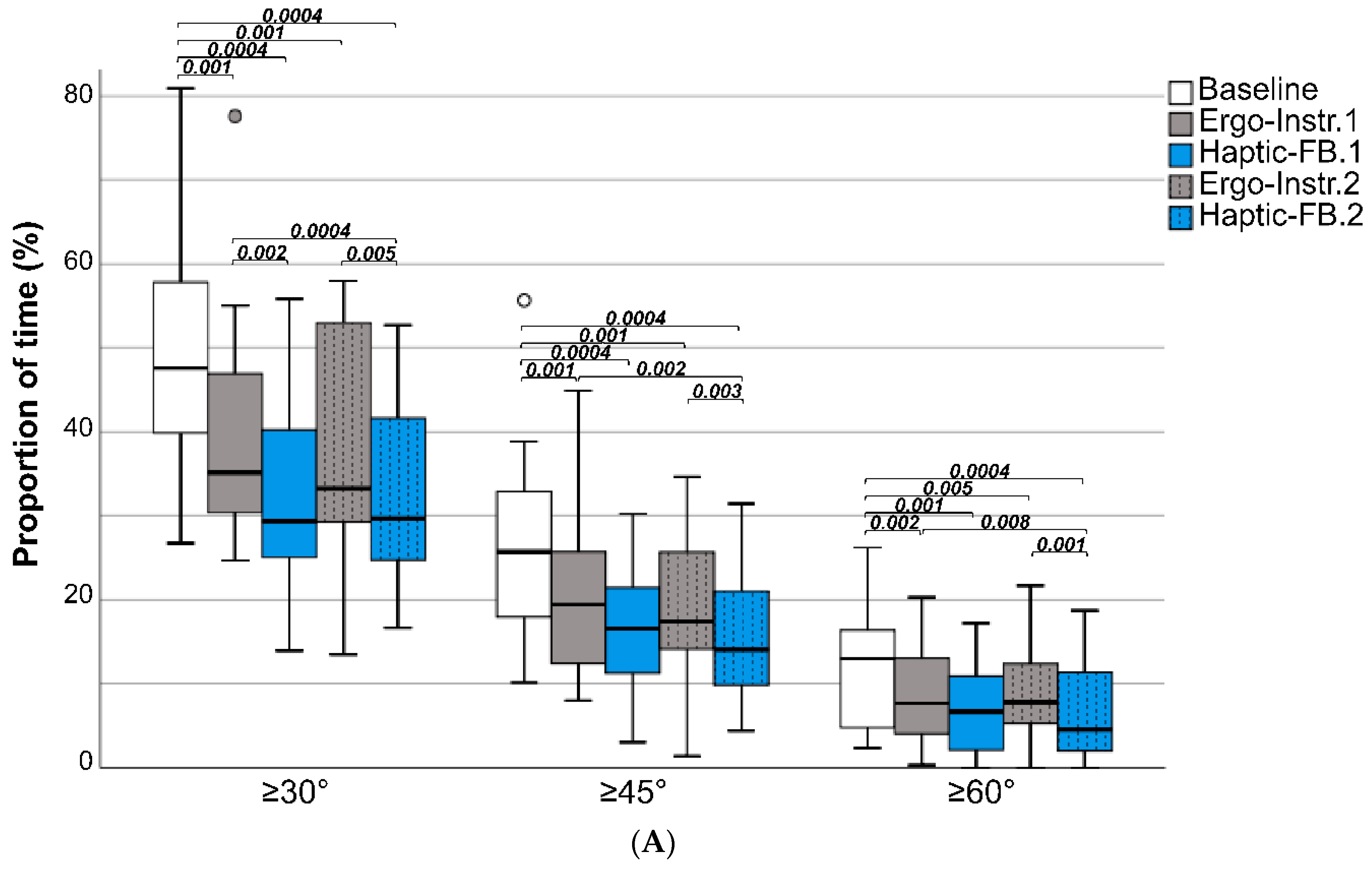
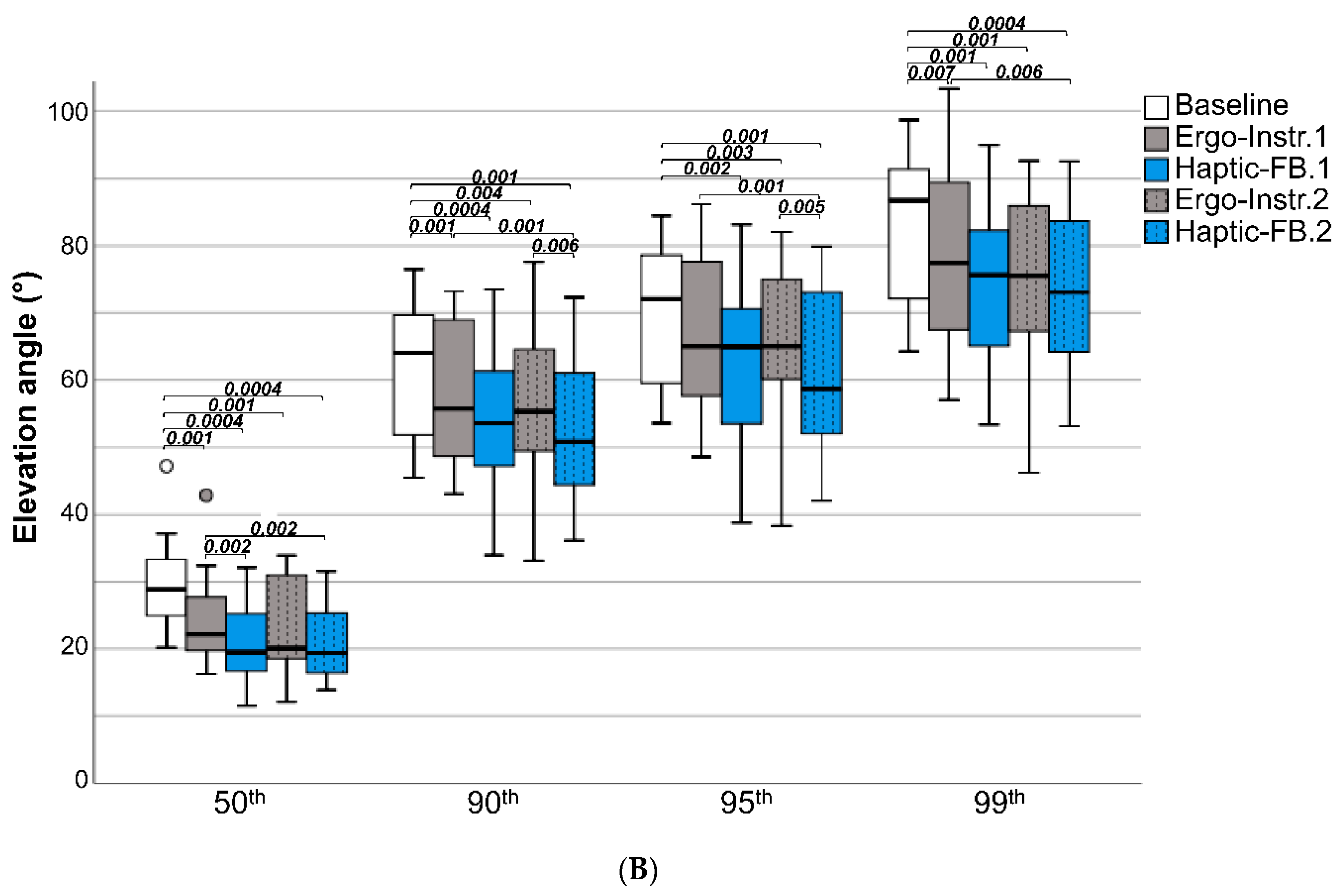
3.1. Effect of Haptic Feedback and Verbal Ergonomics Instructions on Upper-Arm Posture
3.2. Workstation Design Effect
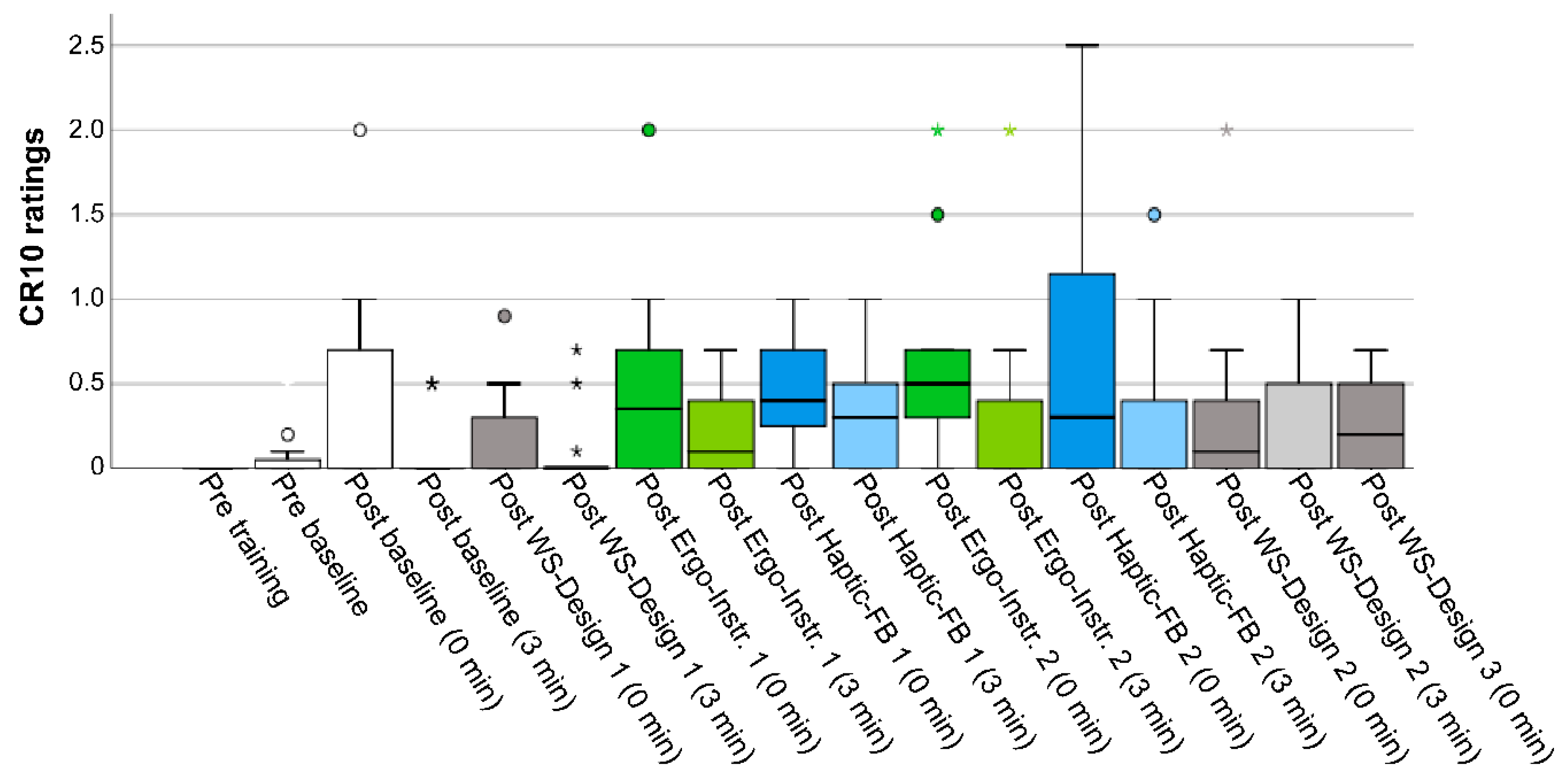
3.3. Ratings of Discomfort/Pain
3.4. User Experiences
4. Discussion
4.1. The Smart Workwear System
4.2. The Smart Workwear System Haptic Feedback Module
4.3. System Application and User Evaluations
4.3.1. System Application and User Evaluations—Major Findings, Clinical Relevance, and Implications
4.3.2. System Application and User Evaluations—Methodological Considerations and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- How did you perceive the mail-sorting task?
- Did you feel any discomfort during the session?
- How did the discomfort influence you and your way of working?
- How did you perceive the vibration feedback?
- What did you learn from the feedback?
- How did the vibration feedback affect you?
- How did the vibration feedback affect your way of working?
- What made you rearrange the workplace the way you did?
- Is there anything else you would like to add that we did not ask about?
References
- Tompa, E.; Mofidi, A.; van den Heuvel, S.; van Bree, T.; Michaelsen, F.; Jung, Y.; Porsch, L.; van Emmerik, M. The Value of Occupational Safety and Health and the Societal Costs of Work-Related Injuries and Diseases; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar] [CrossRef]
- ILO. Global Trends on Occupational Accidents and Diseases. World Day for Safety and Health at Work. Available online: https://www.ilo.org/legacy/english/osh/en/story_content/external_files/fs_st_1-ILO_5_en.pdf (accessed on 8 June 2020).
- Lötters, F.; Burdorf, A.; Kuiper, J.; Miedema, H. Model for the work-relatedness of low-back pain. Scand. J. Work Environ. Health 2003, 29, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder—A systematic review of the literature. Scand. J. Work Environ. Health 2010, 36, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Sluiter, J.K.; Rest, K.M.; Frings-Dresen, M.H.W. Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorders. Scand. J. Work Environ. Health 2001, 7, 1–102. [Google Scholar] [CrossRef]
- NRC. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities; National Research Council and Institute of Medicine: Washington, DC, USA, 2001. [Google Scholar]
- Punnett, L. Musculoskeletal disorders and occupational exposures: How should we judge the evidence concerning the causal association? Scand. J. Public Health 2014, 42, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Eurofound. Sixth European Working Conditions Survey; Publications Office of the European Union: Luxembourg, 2016. [Google Scholar]
- Eurofound. Fifth European Working Conditions Survey; Publications Office of the European Union: Luxembourg, 2012. [Google Scholar]
- Marchet, G.; Melacini, M.; Perotti, S. Investigating order picking system adoption: A case-study-based approach. Int. J. Logist. Res. Appl. 2015, 18, 82–98. [Google Scholar] [CrossRef]
- Baker, P.; Halim, Z. An exploration of warehouse automation implementations: Cost, service and flexibility issues. Supply Chain Manag. 2007, 12, 129–138. [Google Scholar] [CrossRef]
- Beier, G.; Ullrich, A.; Niehoff, S.; Reißig, M.; Habich, M. Industry 4.0: How it is defined from a sociotechnical perspective and how much sustainability it includes—A literature review. J. Clean. Prod. 2020, 259, 120856. [Google Scholar] [CrossRef]
- EU. Council Directive 90/269/EEC of 29 May 1990 on the Minimum Health and Safety Requirements for the Manual Handling of Loads Where there is a Risk Particularly of Back Injury to Workers; Publications Office of the European Union: Luxembourg, 1990. [Google Scholar]
- Eliasson, K.; Lind, C.M.; Nyman, T. Factors influencing ergonomists’ use of observation-based risk-assessment tools. Work 2019, 64, 93–106. [Google Scholar] [CrossRef]
- Ivarsson, A.; Eek, F. The relationship between physical workload and quality within line-based assembly. Ergonomics 2016, 59, 913–923. [Google Scholar] [CrossRef]
- Eklund, J. Ergonomics, quality and continuous improvement—Conceptual and empirical relationships in an industrial context. Ergonomics 1997, 40, 982–1001. [Google Scholar] [CrossRef]
- Falck, A.C.; Örtengren, R.; Högberg, D. The impact of poor assembly ergonomics on product quality: A cost-benefit analysis in car manufacturing. Hum. Factors Ergon. Manuf. 2010, 20, 24–41. [Google Scholar] [CrossRef]
- Yung, M.; Kolus, A.; Wells, R.; Neumann, W.P. Examining the fatigue-quality relationship in manufacturing. Appl. Ergon. 2020, 82, 102919. [Google Scholar] [CrossRef] [PubMed]
- Lind, C.M.; Rose, L.M. Shifting to proactive risk management: Risk communication using the RAMP tool. Agron. Res. 2016, 14, 513–524. [Google Scholar]
- Falck, A.-C.; Örtengren, R.; Rosenqvist, M.; Söderberg, R. Proactive assessment of basic complexity in manual assembly: Development of a tool to predict and control operator-induced quality errors. Int. J. Prod. Res. 2017, 55, 4248–4260. [Google Scholar] [CrossRef]
- Falck, A.-C.; Rosenqvist, M. What are the obstacles and needs of proactive ergonomics measures at early product development stages?—An interview study in five Swedish companies. Int. J. Ind. Ergon. 2012, 42, 406–415. [Google Scholar] [CrossRef]
- Cantley, L.F.; Taiwo, O.A.; Galusha, D.; Barbour, R.; Slade, M.D.; Tessier-Sherman, B.; Cullen, M.R. Effect of systematic ergonomic hazard identification and control implementation on musculoskeletal disorder and injury risk. Scand. J. Work Environ. Health 2014, 40, 57–65. [Google Scholar] [CrossRef]
- Carrivick, P.J.W.; Lee, A.H.; Yau, K.K.W. Effectiveness of a participatory workplace risk assessment team in reducing the risk and severity of musculoskeletal injury. J. Occup. Health 2002, 44, 221–225. [Google Scholar] [CrossRef]
- Lowe, B.D.; Dempsey, P.G.; Jones, E.M. Ergonomics assessment methods used by ergonomics professionals. Appl. Ergon. 2019, 81, 102882. [Google Scholar] [CrossRef]
- Diego-Mas, J.A.; Poveda-Bautista, R.; Garzon-Leal, D.C. Influences on the use of observational methods by practitioners when identifying risk factors in physical work. Ergonomics 2015, 58, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.M.; Eklund, J.; Nord Nilsson, L.; Barman, L.; Lind, C.M. The RAMP package for MSD risk management in manual handling—A freely accessible tool, with website and training courses. Appl. Ergon. 2020, 86, 103101. [Google Scholar] [CrossRef]
- Lind, C.M.; Forsman, M.; Rose, L.M. Development and evaluation of RAMP II—A practitioner’s tool for assessing musculoskeletal disorder risk factors in industrial manual handling. Ergonomics 2020, 63, 477–504. [Google Scholar] [CrossRef] [PubMed]
- Takala, E.P.; Pehkonen, I.; Forsman, M.; Hansson, G.A.; Mathiassen, S.E.; Neumann, W.P.; Sjogaard, G.; Veiersted, K.B.; Westgaard, R.H.; Winkel, J. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand. J. Work Environ. Health 2010, 36, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Rhén, I.-M.; Forsman, M. Inter- and intra-rater reliability of the OCRA checklist method in video-recorded manual work tasks. Appl. Ergon. 2020, 84, 103025. [Google Scholar] [CrossRef] [PubMed]
- Trask, C.; Mathiassen, S.E.; Wahlström, J.; Forsman, M. Cost-efficient assessment of biomechanical exposure in occupational groups, exemplified by posture observation and inclinometry. Scand. J. Work Environ. Health 2014, 40, 252–265. [Google Scholar] [CrossRef]
- Forsman, M.; Lind, C.M. The Need for Practical and Reliable Risk Assessment Methods for Prevention of Musculoskeletal Disorders. In Transforming Ergonomics with Personalized Health and Intelligent Workplaces; Vega-Barbas, M., Seoane, F., Eds.; IOS Press: Amsterdam, The Netherlands, 2019; pp. 3–14. [Google Scholar] [CrossRef]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Lo Presti, D.; Carnevale, A.; D’Abbraccio, J.; Massari, L.; Massaroni, C.; Sabbadini, R.; Zaltieri, M.; Di Tocco, J.; Bravi, M.; Miccinilli, S.; et al. A multi-parametric wearable system to monitor neck movements and respiratory frequency of computer workers. Sensors 2020, 20, 536. [Google Scholar] [CrossRef]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef]
- Fong, D.T.; Chan, Y.Y. The use of wearable inertial motion sensors in human lower limb biomechanics studies: A systematic review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and reliability of wearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef]
- Bark, K.; Hyman, E.; Tan, F.; Cha, E.; Jax, S.A.; Buxbaum, L.J.; Kuchenbecker, K.J. Effects of vibrotactile feedback on human learning of arm motions. IEEE Trans. Neural. Syst. Rehabil. Eng. 2015, 23, 51–63. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Accuracy and repeatability of single-pose calibration of inertial measurement units for whole-body motion analysis. Gait Posture 2017, 54, 80–86. [Google Scholar] [CrossRef]
- Ray, S.J.; Teizer, J. Real-time construction worker posture analysis for ergonomics training. Adv. Eng. Inform. 2012, 26, 439–455. [Google Scholar] [CrossRef]
- Ying, Z.; Morrell, J.B. A vibrotactile feedback approach to posture guidance. In Proceedings of the IEEE Haptic Interfaces for Virtual Environment and Teleoperator Systems (HAPTICS), Waltham, MA, USA, 25–26 March 2010; pp. 351–358. [Google Scholar]
- Sigrist, R.; Rauter, G.; Riener, R.; Wolf, P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: A review. Psychon. Bull. Rev. 2013, 20, 21–53. [Google Scholar] [CrossRef] [PubMed]
- Esfahani, M.I.M.; Nussbaum, M.A.; Kong, Z.Y. Using a smart textile system for classifying occupational manual material handling tasks: Evidence from lab-based simulations. Ergonomics 2019, 62, 823–833. [Google Scholar] [CrossRef]
- Mokhlespour Esfahani, M.I.; Nussbaum, M.A. Classifying diverse physical activities using “Smart Garments”. Sensors 2019, 19, 3133. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Lu, K.; Diaz-Olivares, J.A.; Seoane, F.; Lindecrantz, K.; Forsman, M.; Abtahi, F.; Eklund, J.A.E. Towards smart work clothing for automatic risk assessment of physical workload. IEEE Access 2018, 6, 40059–40072. [Google Scholar] [CrossRef]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl. Ergon. 2013, 44, 566–574. [Google Scholar] [CrossRef]
- Vignais, N.; Bernard, F.; Touvenot, G.; Sagot, J.-C. Physical risk factors identification based on body sensor network combined to videotaping. Appl. Ergon. 2017, 65, 410–417. [Google Scholar] [CrossRef]
- Lind, C.M.; Sandsjö, L.; Mahdavian, N.; Högberg, D.; Hanson, L.; Diaz Olivares, J.A.; Yang, L.; Forsman, M. Prevention of Work Related Musculoskeletal Disorders Using Smart Workwear—The Smart Workwear Consortium. In Human Systems Engineering and Design; Ahram, T., Karwowski, W., Taiar, R., Eds.; Springer: Cham, Switzerland, 2019; Volume 876, pp. 477–483. [Google Scholar]
- Peppoloni, L.; Filippeschi, A.; Ruffaldi, E.; Avizzano, C.A. A novel wearable system for the online assessment of risk for biomechanical load in repetitive efforts. Int. J. Ind. Ergon. 2016, 52, 1–11. [Google Scholar] [CrossRef]
- Moore, J.S.; Garg, A. The strain index: A proposed method to analyze jobs for risk of distal upper extremity disorders. Am. Ind. Hyg. Assoc. J. 1995, 56, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Diego-Mas, J.A.; Alcaide-Marzal, J. Using Kinect™ sensor in observational methods for assessing postures at work. Appl. Ergon. 2014, 45, 976–985. [Google Scholar] [CrossRef]
- Karhu, O.; Kansi, P.; Kuorinka, I. Correcting working postures in industry: A practical method for analysis. Appl. Ergon. 1977, 8, 199–201. [Google Scholar] [CrossRef]
- Battini, D.; Persona, A.; Sgarbossa, F. Innovative real-time system to integrate ergonomic evaluations into warehouse design and management. Comput. Ind. Eng. 2014, 77, 1–10. [Google Scholar] [CrossRef]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Manghisi, V.M.; Uva, A.E.; Fiorentino, M.; Bevilacqua, V.; Trotta, G.F.; Monno, G. Real time RULA assessment using Kinect v2 sensor. Appl. Ergon. 2016, 65, 481–491. [Google Scholar] [CrossRef]
- Patrizi, A.; Pennestrì, E.; Valentini, P.P. Comparison between low-cost marker-less and high-end marker-based motion capture systems for the computer-aided assessment of working ergonomics. Ergonomics 2016, 59, 155–162. [Google Scholar] [CrossRef]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- Alberto, R.; Draicchio, F.; Varrecchia, T.; Silvetti, A.; Iavicoli, S. Wearable monitoring devices for biomechanical risk assessment at work: Current status and future challenges-a systematic review. Int. J. Environ. Res. Public Health 2018, 15, 2001. [Google Scholar] [CrossRef]
- Verbeek, J.H.; Martimo, K.P.; Karppinen, J.; Kuijer, P.P.; Viikari-Juntura, E.; Takala, E.P. Manual material handling advice and assistive devices for preventing and treating back pain in workers. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Hogan, D.A.; Greiner, B.A.; O’Sullivan, L. The effect of manual handling training on achieving training transfer, employee’s behaviour change and subsequent reduction of work-related musculoskeletal disorders: A systematic review. Ergonomics 2014, 57, 93–107. [Google Scholar] [CrossRef]
- Clemes, S.A.; Haslam, C.O.; Haslam, R.A. What constitutes effective manual handling training? A systematic review. Occup. Med. 2010, 60, 101–107. [Google Scholar] [CrossRef]
- Doss, R.; Robathan, J.; Abdel-Malek, D.; Holmes, M.W.R. Posture Coaching and Feedback during Patient Handling in a Student Nurse Population. IISE Trans. Occup. Ergon. Hum. Factors 2018, 6, 116–127. [Google Scholar] [CrossRef]
- Agruss, C.D.; Williams, K.; Fathallah, F.A. The effect of feedback training on lumbosacral compression during simulated occupational lifting. Ergonomics 2004, 47, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Madeleine, P.; Vedsted, P.; Blangsted, A.K.; Sjøgaard, G.; Søgaard, K. Effects of electromyographic and mechanomyographic biofeedback on upper trapezius muscle activity during standardized computer work. Ergonomics 2006, 49, 921–933. [Google Scholar] [CrossRef] [PubMed]
- Bazazan, A.; Dianat, I.; Feizollahi, N.; Mombeini, Z.; Shirazi, A.M.; Castellucci, H.I. Effect of a posture correction-based intervention on musculoskeletal symptoms and fatigue among control room operators. Appl. Ergon. 2019, 76, 12–19. [Google Scholar] [CrossRef]
- Umek, A.; Kos, A. Smart equipment design challenges for real-time feedback support in sport. Facta Univ. Ser. Mech. Eng. 2018, 16, 389–403. [Google Scholar] [CrossRef]
- Kos, M.; Kramberger, I. Tennis stroke consistency analysis using miniature wearable IMU. In Proceedings of the IEEE Systems, Signals and Image Processing (IWSSIP), Maribor, Slovenia, 20–22 June 2018; pp. 1–4. [Google Scholar]
- Zhang, X.; Shan, G.; Wang, Y.; Wan, B.; Li, H. Wearables, biomechanical feedback, and human motor-skills’ learning & optimization. Appl. Sci. 2019, 9, 226. [Google Scholar] [CrossRef]
- Demircan, E. A pilot study on locomotion training via biomechanical models and a wearable haptic feedback system. Robomech. J. 2020, 7, 1–13. [Google Scholar] [CrossRef]
- Lind, C.M.; Yang, L.; Abtahi, F.; Hanson, L.; Lindecrantz, K.; Lu, K.; Forsman, M.; Eklund, J. Reducing postural load in order picking through a smart workwear system using real-time vibrotactile feedback. Appl. Ergon. 2020, 89, 103188. [Google Scholar] [CrossRef] [PubMed]
- Vega-Barbas, M.; Diaz-Olivares, J.A.; Lu, K.; Forsman, M.; Seoane, F.; Abtahi, F. P-Ergonomics Platform: Toward precise, pervasive, and personalized ergonomics using wearable sensors and edge computing. Sensors 2019, 19, 1225. [Google Scholar] [CrossRef]
- Mahdavian, N.; Lind, C.M.; Antonio Diaz Olivares, J.; Iriondo Pascual, A.; Högberg, D.; Brolin, E.; Yang, L.; Forsman, M.; Hanson, L. Effect of Giving Feedback on Postural Working Techniques. In Advances in Manufacturing Technology XXXII; Thorvald, P., Case, K., Eds.; IOS Press: Amsterdam, The Netherlands, 2018; pp. 247–252. [Google Scholar] [CrossRef]
- Ribeiro, D.C.; Sole, G.; Abbott, J.H.; Milosavljevic, S. Extrinsic feedback and management of low back pain: A critical review of the literature. Man. Ther. 2011, 16, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Korshoj, M.; Skotte, J.H.; Christiansen, C.S.; Mortensen, P.; Kristiansen, J.; Hanisch, C.; Ingebrigtsen, J.; Holtermann, A. Validity of the Acti4 software using ActiGraph GT3X+accelerometer for recording of arm and upper body inclination in simulated work tasks. Ergonomics 2014, 57, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.A.; Mathiassen, S.E.; Wahlström, J.; Liv, P.; Forsman, M. Is what you see what you get? Standard inclinometry of set upper arm elevation angles. Appl. Ergon. 2015, 47, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.Å.; Arvidsson, I.; Ohlsson, K.; Nordander, C.; Mathiassen, S.E.; Skerfving, S.; Balogh, I. Precision of measurements of physical workload during standardised manual handling. Part II: Inclinometry of head, upper back, neck and upper arms. J. Electromyogr. Kinesiol. 2006, 16, 125–136. [Google Scholar] [CrossRef]
- Kim, A.; Golnaraghi, M.F. A quaternion-based orientation estimation algorithm using an inertial measurement unit. In Proceedings of the IEEE Position Location and Navigation Symposium (PLANS), Monterey, CA, USA, 26–29 April 2004; pp. 268–272. [Google Scholar]
- Arvidsson, I.; Dahlqvist, C.; Enquist, H.; Nordander, C. Action Levels for Prevention of Work Related Musculoskeletal Disorders; Arbets- och miljömedicin Syd: Lund, Switzerland, 2017. [Google Scholar]
- Erlandsson, A. En Utredning om Brevbärarpersonalens Arbetsförhållanden och Införandet av Bästa Metod [An Investigation into the Working Conditions of the Mail-Carrier Staff and the Introduction of Best Method]; Lindköping University: Lindköping, Switzerland, 2002. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Ciriello, V.M.; Maikala, R.V.; Dempsey, P.G.; O’Brien, N.V. Psychophysically determined forces of dynamic pushing for female industrial workers: Comparison of two apparatuses. Appl. Ergon. 2010, 41, 141–145. [Google Scholar] [CrossRef]
- Caldwell, L.S.; Chaffin, D.B.; Dukes-Dobos, F.N.; Kroemer, K.H.; Laubach, L.L.; Snook, S.H.; Wasserman, D.E. A proposed standard procedure for static muscle strength testing. Am. Ind. Hyg. Assoc. J. 1974, 35, 201–206. [Google Scholar] [CrossRef]
- Pheasant, S.; Haslegrave, C.M. Bodyspace: Anthropometry, Ergonomics and the Design of Work, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar] [CrossRef]
- Kvale, S.; Brinkmann, S.; Torhell, S.-E. Den Kvalitativa Forskningsintervjun [Qualitative Interviewing]; Studentlitteratur: Lund, Switzerland, 2014. [Google Scholar]
- Spook, S.M.; Koolhaas, W.; Bultmann, U.; Brouwer, S. Implementing sensor technology applications for workplace health promotion: A needs assessment among workers with physically demanding work. BMC Public Health 2019, 19, 1100. [Google Scholar] [CrossRef]
- Lind, C.M.; Rhen, I.M.; Forsman, M. Bias and repeatability of standard calibration postures for inclinometry of the upper arms and trunk. Unpublished work. 2020. [Google Scholar]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Effect of local magnetic field disturbances on inertial measurement units accuracy. Appl. Ergon. 2017, 63, 123–132. [Google Scholar] [CrossRef]
- Buchanan, J.J.; Wang, C. Overcoming the guidance effect in motor skill learning: Feedback all the time can be beneficial. Exp. Brain Res. 2012, 219, 305–320. [Google Scholar] [CrossRef]
- Lam, C.F.; DeRue, D.S.; Karam, E.P.; Hollenbeck, J.R. The impact of feedback frequency on learning and task performance: Challenging the “more is better” assumption. Organ. Behav. Hum. Decis. Process. 2011, 116, 217–228. [Google Scholar] [CrossRef]
- Patterson, J.T.; Carter, M.J.; Hansen, S. Self-controlled KR schedules: Does repetition order matter? Hum. Mov. Sci. 2013, 32, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Gerard, M.J.; Armstrong, T.J.; Rempel, D.A.; Woolley, C. Short term and long term effects of enhanced auditory feedback on typing force, EMG, and comfort while typing. Appl. Ergon. 2002, 33, 129–138. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | Ergo-Instr. 1 | Haptic-FB 1 | Ergo-Instr. 2 | Haptic-FB 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | M | diff (%) | p | M | diff (%) | p | M | diff (%) | p | M | diff (%) | p | |
| Arm elevation (s) | |||||||||||||
| ≥30° | 48.6 | 35.1 | 26 | 0.001 | 29.3 | 38 | <0.001 | 33.2 | 30 | 0.001 | 29.7 | 38 | <0.001 |
| ≥45° | 25.7 | 19.4 | 24 | 0.001 | 16.5 | 36 | <0.001 | 17.4 | 32 | 0.001 | 14.0 | 45 | <0.001 |
| ≥60° | 13.0 | 7.7 | 41 | 0.002 | 6.7 | 49 | 0.001 | 7.8 | 40 | 0.005 | 4.5 | 65 | <0.001 |
| Arm elevation (°) | |||||||||||||
| 50th | 28.9 | 22.1 | 23 | 0.001 | 19.5 | 32 | <0.001 | 20.1 | 31 | 0.001 | 19.4 | 33 | <0.001 |
| 90th | 64.0 | 55.7 | 13 | 0.010 | 53.5 | 16 | <0.001 | 55.3 | 14 | 0.004 | 50.9 | 21 | 0.001 |
| 95th | 72.0 | 65.1 | 10 | 0.020 | 65.0 | 10 | 0.002 | 65.1 | 10 | 0.003 | 58.7 | 19 | 0.001 |
| 99th | 86.7 | 77.5 | 11 | 0.007 | 75.7 | 13 | 0.001 | 75.5 | 13 | 0.001 | 73.1 | 16 | <0.001 |
| Baseline | WS-Design 1 | WS-Design 2 | WS-Design 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | M | diff (%) | p | M | diff (%) | p | M | diff (%) | p | |
| Arm elevation (s) | ||||||||||
| ≥30° | 47.6 | 5.5 | 88 | 0.001 | 0.3 | 99 | <0.001 | 0.0 | 100 | <0.001 |
| ≥45° | 25.7 | 0.3 | 99 | 0.001 | 0.0 | 100 | <0.001 | 0.0 | 100 | <0.001 |
| ≥60° | 13.0 | 0.0 | 100 | <0.001 | 0.0 | 100 | <0.001 | 0.0 | 100 | <0.001 |
| Arm elevation (°) | ||||||||||
| 50th | 28.9 | 15.1 | 48 | 0.001 | 9.5 | 67 | <0.001 | 8.2 | 72 | <0.001 |
| 90th | 64.0 | 25.3 | 61 | <0.001 | 16.9 | 74 | <0.001 | 16.7 | 74 | <0.001 |
| 95th | 72.0 | 30.4 | 58 | <0.001 | 19.7 | 73 | <0.001 | 18.7 | 74 | <0.001 |
| 99th | 86.7 | 41.1 | 53 | <0.001 | 26.2 | 70 | <0.001 | 23.5 | 73 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lind, C.M.; Diaz-Olivares, J.A.; Lindecrantz, K.; Eklund, J. A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback. Sensors 2020, 20, 6010. https://doi.org/10.3390/s20216010
Lind CM, Diaz-Olivares JA, Lindecrantz K, Eklund J. A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback. Sensors. 2020; 20(21):6010. https://doi.org/10.3390/s20216010
Chicago/Turabian StyleLind, Carl Mikael, Jose Antonio Diaz-Olivares, Kaj Lindecrantz, and Jörgen Eklund. 2020. "A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback" Sensors 20, no. 21: 6010. https://doi.org/10.3390/s20216010
APA StyleLind, C. M., Diaz-Olivares, J. A., Lindecrantz, K., & Eklund, J. (2020). A Wearable Sensor System for Physical Ergonomics Interventions Using Haptic Feedback. Sensors, 20(21), 6010. https://doi.org/10.3390/s20216010