Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
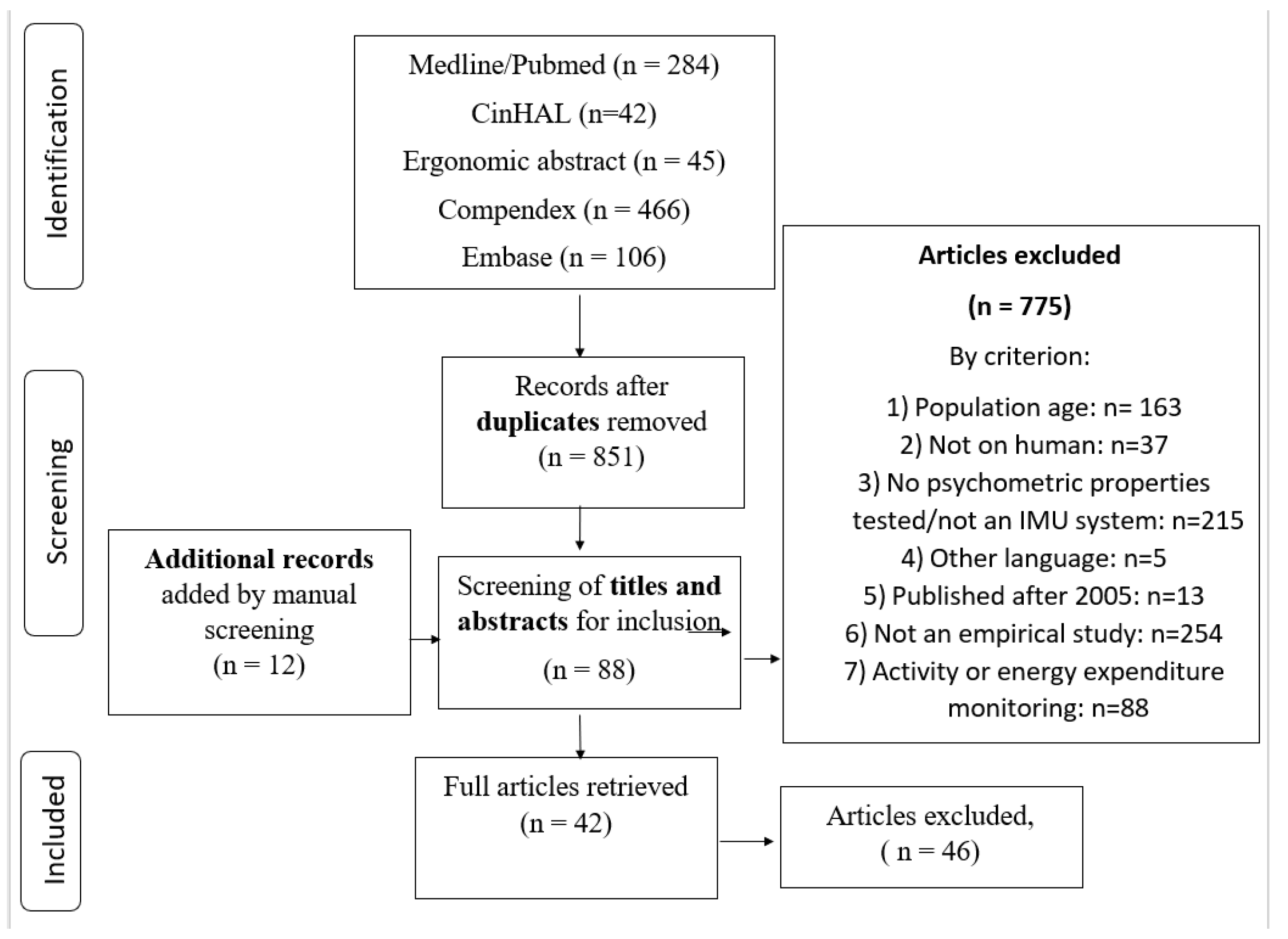
2. Materials and Methods
2.1. Description of the Systems
2.2. Data Sources
2.3. Quality Assessment
2.4. Data Extractions
2.5. Data Analysis
- Strong evidence: multiple HQ studies with consistent results.
- Moderate evidence: multiple studies, including at least one HQ study, or multiple MQ or LQ studies, presenting consistent results.
- Conflicting evidence: multiple studies providing inconsistent results, regardless of the methodological quality.
- Limited evidence: multiple MQ or LQ studies with inconsistent results, or one HQ.
- Very limited evidence: only one LQ or MQ study.
3. Results
3.1. Characteristics of Studies
3.2. Methodological Quality
3.3. Criterion Validity and Errors of Measurement by Body Region
3.3.1. Neck
3.3.2. Shoulder
3.3.3. Elbow
3.3.4. Wrist
3.3.5. Trunk
3.3.6. Pelvis
3.3.7. Hip
3.3.8. Knee
3.3.9. Ankle
3.4. Reliability by Joint
3.4.1. Neck
3.4.2. Shoulder
3.4.3. Scapula
3.4.4. Elbow
3.4.5. Wrist
3.4.6. Trunk
3.4.7. Pelvis
3.4.8. Hip
3.4.9. Knee
3.4.10. Ankle
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ceseracciu, E.; Sawacha, Z.; Cobelli, C. Comparison of Markerless and Marker-Based Motion Capture Technologies through Simultaneous Data Collection during Gait: Proof of Concept. PLoS ONE 2014, 9, e87640. [Google Scholar] [CrossRef]
- Godfrey, A.; Conway, R.; Meagher, D.; Ólaighin, G. Direct measurement of human movement by accelerometry. Med. Eng. Phys. 2008, 30, 1364–1386. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, G.; Manto, M. Neurological tremor: Sensors, signal processing and emerging applications. Sensors 2010, 10, 1399–1422. [Google Scholar] [CrossRef]
- Dejnabadi, H.; Jolles, B.M.; Casanova, E.; Fua, P.; Aminian, K. Estimation and visualization of sagittal kinematics of lower limbs orientation using body-fixed sensors. IEEE Trans. Biomed. Eng. 2006, 53, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Dejnabadi, H.; Jolles, B.M.; Aminian, K. A new approach to accurate measurement of uniaxial joint angles based on a combination of accelerometers and gyroscopes. IEEE Trans. Biomed. Eng. 2005, 52, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Abyarjoo, F.; Barreto, A.; Cofino, J.; Ortega, F.R. Implementing a Sensor Fusion Algorithm for 3D Orientation Detection with Inertial/Magnetic Sensors. In Innovations and Advances in Computing, Informatics, Systems Sciences, Networking and Engineering; Springer: Cham, Switzerland, 2015; pp. 305–310. [Google Scholar]
- Kok, M.; Schon, T.B. Magnetometer Calibration Using Inertial Sensors. IEEE Sens. J. 2016, 16, 5679–5689. [Google Scholar] [CrossRef]
- Sabatini, A. Estimating Three-Dimensional Orientation of Human Body Parts by Inertial/Magnetic Sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef]
- Fong, D.; Chan, Y. The Use of Wearable Inertial Motion Sensors in Human Lower Limb Biomechanics Studies: A Systematic Review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef]
- Walmsley, C.P.; Williams, S.A.; Grisbrook, T.; Elliott, C.; Imms, C.; Campbell, A. Measurement of Upper Limb Range of Motion Using Wearable Sensors: A Systematic Review. Sports Med. Open 2018, 4, 53. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Galán-Mercant, A.; Williams, J.M. The use of inertial sensors system for human motion analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Tong, K.; Granat, M.H. A practical gait analysis system using gyroscopes. Med. Eng. Phys. 1999, 21, 87–94. [Google Scholar] [CrossRef]
- Morris, J.R.W. Accelerometry—A technique for the measurement of human body movements. J. Biomech. 1973, 6, 729–736. [Google Scholar] [CrossRef]
- Djurić-Jovičić, M.D.; Jovičić, N.S.; Popović, D.B. Kinematics of Gait: New Method for Angle Estimation Based on Accelerometers. Sensors 2011, 11, 10571–10585. [Google Scholar] [CrossRef]
- Pasciuto, I.; Ligorio, G.; Bergamini, E.; Vannozzi, G.; Sabatini, A.; Cappozzo, A. How Angular Velocity Features and Different Gyroscope Noise Types Interact and Determine Orientation Estimation Accuracy. Sensors 2015, 15, 23983–24001. [Google Scholar] [CrossRef]
- Foxlin, E. Inertial head-tracker sensor fusion by a complementary separate-bias Kalman filter. In Proceedings of the IEEE 1996 Virtual Reality Annual International Symposium, Santa Clara, CA, USA, 30 March–3 April 1996; pp. 185–194. [Google Scholar]
- Roetenberg, D.; Baten, C.T.M.; Veltink, P.H. Estimating body segment orientation by applying inertial and magnetic sensing near ferromagnetic materials. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 469–471. [Google Scholar] [CrossRef]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- MacDermid, J.C. Critical appraisal of study design for psychometric articles evaluation form and interpretation guide. In Evidence Based Rehabilitation: A Guide to Practice, 3rd ed.; Slack: Thorofare, NJ, USA, 2008; pp. 387–392. [Google Scholar]
- Balshem, H.; Helfand, M.; Schunemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Gwet, K.L. Handbook of Inter-Rater Reliability: The Definitive Guide to Measuring the Extent of Agreement among Raters; Advanced Analytics, LLC: Gaithersburg, MD, USA, 2014. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef]
- de Oliveira, F.C.L.; Bouyer, L.J.; Ager, A.L.; Roy, J.S. Electromyographic analysis of rotator cuff muscles in patients with rotator cuff tendinopathy: A systematic review. J. Electromyogr. Kinesiol. 2017, 35, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Bouvier, B.; Duprey, S.; Claudon, L.; Dumas, R.; Savescu, A. Upper Limb Kinematics Using Inertial and Magnetic Sensors: Comparison of Sensor-to-Segment Calibrations. Sensors 2015, 15, 18813–18833. [Google Scholar] [CrossRef] [PubMed]
- Akins, J.S.; Heebner, N.R.; Lovalekar, M.; Sell, T.C. Reliability and validity of instrumented soccer equipment. J. Appl. Biomech. 2015, 31, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.; Duthie, G.; Robertson, S.; Hopkins, W.; Ball, K. Concurrent validation of an inertial measurement system to quantify kicking biomechanics in four football codes. J. Biomech. 2018. [Google Scholar] [CrossRef] [PubMed]
- Ertzgaard, P.; Öhberg, F.; Gerdle, B.; Grip, H. A new way of assessing arm function in activity using kinematic Exposure Variation Analysis and portable inertial sensors—A validity study. Man. Ther. 2016, 21, 241–249. [Google Scholar] [CrossRef]
- Fantozzi, S.; Giovanardi, A.; Magalhaes, F.A.; Di Michele, R.; Cortesi, M.; Gatta, G. Assessment of three-dimensional joint kinematics of the upper limb during simulated swimming using wearable inertial-magnetic measurement units. J. Sports Sci. 2016, 34, 1073–1080. [Google Scholar] [CrossRef]
- Gil-Agudo, A.; de Los Reyes-Guzman, A.; Dimbwadyo-Terrer, I.; Penasco-Martin, B.; Bernal-Sahun, A.; Lopez-Monteagudo, P.; Del Ama-Espinosa, A.; Pons, J.L. A novel motion tracking system for evaluation of functional rehabilitation of the upper limbs. Neural Regen. Res. 2013, 8, 1773–1782. [Google Scholar] [CrossRef] [PubMed]
- Godwin, A.; Agnew, M.; Stevenson, J. Accuracy of inertial motion sensors in static, quasistatic, and complex dynamic motion. J. Biomech. Eng. 2009, 131, 114501. [Google Scholar] [CrossRef]
- Pérez, R.; Costa, Ú.; Torrent, M.; Solana, J.; Opisso, E.; Cáceres, C.; Tormos, J.M.; Medina, J.; Gómez, E.J. Upper Limb Portable Motion Analysis System Based on Inertial Technology for Neurorehabilitation Purposes. Sensors 2010, 10, 10733–10751. [Google Scholar] [CrossRef]
- Plamondon, A.; Delisle, A.; Larue, C.; Brouillette, D.; McFadden, D.; Desjardins, P.; Larivière, C. Evaluation of a hybrid system for three-dimensional measurement of trunk posture in motion. Appl. Ergon. 2007, 38, 697–712. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2016. [Google Scholar] [CrossRef] [PubMed]
- Schall, M.C.; Fethke, N.B.; Chen, H.; Oyama, S.; Douphrate, D.I. Accuracy and repeatability of an inertial measurement unit system for field-based occupational studies. Ergonomics 2016, 59, 591–602. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, H. Reducing drifts in the inertial measurements of wrist and elbow positions. IEEE Trans. Instrum. Meas. 2010, 59, 575–585. [Google Scholar] [CrossRef]
- Jasiewicz, J.M.; Treleaven, J.; Condie, P.; Jull, G. Wireless orientation sensors: Their suitability to measure head movement for neck pain assessment. Man. Ther. 2007, 12, 380–385. [Google Scholar] [CrossRef]
- Lebel, K.; Boissy, P.; Nguyen, H.; Duval, C. Inertial measurement systems for segments and joints kinematics assessment: Towards an understanding of the variations in sensors accuracy. BioMed. Eng. Online 2017, 16. [Google Scholar] [CrossRef] [PubMed]
- Bugane, F.; Benedetti, M.G.; D’Angeli, V.; Leardini, A. Estimation of pelvis kinematics in level walking based on a single inertial sensor positioned close to the sacrum: Validation on healthy subjects with stereophotogrammetric system. Biomed. Eng. Online 2014, 13, 146. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Y.; Yen, S.C.; Tay, A.; Lee, W.; Gao, F.; Zhao, Z.; Li, J.; Hon, B.; Tian-Ma Xu, T.; Cheong, A.; et al. Wireless wearable range-of-motion sensor system for upper and lower extremity joints: A validation study. Healthc. Technol. Lett. 2015, 2, 12–17. [Google Scholar] [CrossRef]
- Barraza Madrigal, J.A.; Cardiel, E.; Rogeli, P.; Leija Salas, L.; Munoz Guerrero, R. Evaluation of suitability of a micro-processing unit of motion analysis for upper limb tracking. Med. Eng. Phys. 2016, 38, 793–800. [Google Scholar] [CrossRef]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A.; Sacchetti, R. Ambulatory measurement of shoulder and elbow kinematics through inertial and magnetic sensors. Med. Biol. Eng. Comput. 2008, 46, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Bauer, C.M.; Rast, F.M.; Ernst, M.J.; Kool, J.; Oetiker, S.; Rissanen, S.M.; Suni, J.H.; Kankaanpaa, M. Concurrent validity and reliability of a novel wireless inertial measurement system to assess trunk movement. J. Electromyogr. Kinesiol. 2015, 25, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Guillon, P.; Camomilla, V.; Pillet, H.; Skalli, W.; Cappozzo, A. Trunk Inclination Estimate During the Sprint Start Using an Inertial Measurement Unit: A Validation Study. J. Appl. Biomech. 2013, 29, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Dowling, A.V.; Favre, J.; Andriacchi, T.P. A wearable system to assess risk for anterior cruciate ligament injury during jump landing: Measurements of temporal events, jump height, and sagittal plane kinematics. J. Biomech.Eng. 2011, 133. [Google Scholar] [CrossRef] [PubMed]
- Ha, T.H.; Saber-Sheikh, K.; Moore, A.P.; Jones, M.P. Measurement of lumbar spine range of movement and coupled motion using inertial sensors—A protocol validity study. Man. Ther. 2013, 18, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Lullini, G.; Giannini, S.; Berti, L.; Ortolani, M.; Caravaggi, P. Validation of the angular measurements of a new inertial-measurement-unit based rehabilitation system: Comparison with state-of-the-art gait analysis. J. Neuroeng. Rehabil. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Mjøsund, H.L.; Boyle, E.; Kjaer, P.; Mieritz, R.M.; Skallgård, T.; Kent, P. Clinically acceptable agreement between the ViMove wireless motion sensor system and the Vicon motion capture system when measuring lumbar region inclination motion in the sagittal and coronal planes. BMC Musculoskelet. Disord. 2017, 18, 1–9. [Google Scholar] [CrossRef]
- Bolink, S.A.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.C.; Meijer, K.; Grimm, B. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit-stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med. Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18. [Google Scholar] [CrossRef]
- Bergmann, J.H.; Mayagoitia, R.E.; Smith, I.C. A portable system for collecting anatomical joint angles during stair ascent: A comparison with an optical tracking device. Dyn. Med. DM 2009, 8, 3. [Google Scholar] [CrossRef]
- Cloete, T.; Scheffer, C. Benchmarking of a full-body inertial motion capture system for clinical gait analysis. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 4579–4582. [Google Scholar] [CrossRef]
- Saber-Sheikh, K.; Bryant, E.C.; Glazzard, C.; Hamel, A.; Lee, R.Y.W. Feasibility of using inertial sensors to assess human movement. Man. Ther. 2010, 15, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Watanabe, T. Kalman-Filtering-Based Joint Angle Measurement with Wireless Wearable Sensor System for Simplified Gait Analysis. IEICE Trans. Inf. Syst. 2011, 94, 1716–1720. [Google Scholar] [CrossRef]
- Takeda, R.; Tadano, S.; Natorigawa, A.; Todoh, M.; Yoshinari, S. Gait posture estimation using wearable acceleration and gyro sensors. J. Biomech. 2009, 42, 2486–2494. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Jolles, B.M.; Aissaoui, R.; Aminian, K. Ambulatory measurement of 3D knee joint angle. J. Biomech. 2008, 41, 1029–1035. [Google Scholar] [CrossRef]
- Jaysrichai, T.; Suputtitada, A.; Khovidhungij, W. Mobile Sensor Application for Kinematic Detection of the Knees. Ann. Rehabil. Med. 2015, 39, 599–608. [Google Scholar] [CrossRef]
- Mifsud, N.L.; Kristensen, N.H.; Villumsen, M.; Hansen, J.; Kersting, U.G. Portable Inertial Motion Unit for Continuous Assessment of In-shoe Foot Movement. Procedia Eng. 2014, 72, 208–213. [Google Scholar] [CrossRef]
- Rouhani, H.; Favre, J.; Crevoisier, X.; Aminian, K. Measurement of multi-segment foot joint angles during gait using a wearable system. J. Biomech. Eng. 2012, 134. [Google Scholar] [CrossRef] [PubMed]
- Duc, C.; Salvia, P.; Lubansu, A.; Feipel, V.; Aminian, K. A wearable inertial system to assess the cervical spine mobility: Comparison with an optoelectronic-based motion capture evaluation. Med. Eng. Phys. 2014, 36, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Shin, S.-H.; Kim, J.-K.; Park, Y.-J.; Oh, H.-S.; Park, Y.-B. Cervical Coupling Motion Characteristics in Healthy People Using a Wireless Inertial Measurement Unit. Evid.-Based Complement. Altern. Med. 2013, 2013. [Google Scholar] [CrossRef]
- Schiefer, C.; Kraus, T.; Ellegast, R.P.; Ochsmann, E. A technical support tool for joint range of motion determination in functional diagnostics—An inter-rater study. J. Occup. Med. Toxicol. 2015, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- van den Noort, J.C.; Wiertsema, S.H.; Hekman, K.M.C.; Schonhuth, C.P.; Dekker, J.; Harlaar, J. Reliability and precision of 3D wireless measurement of scapular kinematics. Med. Biol. Eng. Comput. 2014, 52, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Yun, W.-S.; Kim, H.; Ahn, J.H.; Park, Y.-B.; Park, Y.-J. Individual characteristics of reliable lumbar coupling motions. Eur. Spine J. 2015, 24, 1917–1925. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.-S.; Desmeules, F.; Frémont, P.; Dionne, C.; MacDermid, J. L’évaluation Clinique, les Traitements et le Retour en Emploi de Travailleurs Souffrant D’atteintes de la Coiffe des Rotateurs—Bilan des Connaissances; R-885; Institut de Recherche Robert-Sauvé en Santé et en Sécurité du Travail (IRSST): Montréal, QC, Canada, 2015. [Google Scholar]
- Porciuncula, F.; Roto, A.V.; Kumar, D.; Davis, I.; Roy, S.; Walsh, C.J.; Awad, L.N. Wearable Movement Sensors for Rehabilitation: A Focused Review of Technological and Clinical Advances. PM&R 2018, 10, S220–S232. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. SENIAM: European Recommendations for Surface Electromyography: Results of the SENIAM Project; Roessingh Research and Development: Enschede, The Netherlands, 1999. [Google Scholar]



{kind=link}
{kind=link}
| Joint | Validity: Number of Articles | Reliability: Number of Articles | COSMIN Quality Evidence – Validity | COSMIN Quality Evidence – Reliability | MacDermid Quality Evidence – Validity | MacDermid Quality Evidence – Reliability | Body of Evidence – Validity | Body of Evidence – Reliability |
|---|---|---|---|---|---|---|---|---|
| Neck | 5 | 3 | 1 MQ 3 LQ 1 VLQ | 1 HQ 1 MQ 1 LQ | 1 HQ 2 MQ 2 LQ | 1 HQ 2 MQ | Moderate | Moderate |
| Scapula | 0 | 1 | N/A | 1 HQ | N/A | 1 HQ | N/A | Limited |
| Shoulder | 12 | 2 | 1 HQ 3 MQ 7 LQ 1 VLQ | 1 MQ 1 LQ | 1 HQ 7 MQ 4 LQ | 1 HQ 1 MQ | Conflicting evidence | Moderate |
| Elbow | 10 | 2 | 1 HQ 3 MQ 5 LQ 1 LQ | 1 MQ 1 LQ | 1 HQ 5 MQ 4 LQ | 1 HQ 1 MQ | Conflicting evidence | Conflicting evidence |
| Wrist | 6 | 2 | 2 MQ 4 LQ | 1 MQ 1 LQ | 1 HQ 3 MQ 2 LQ | 1 HQ 1 MQ | Moderate | Moderate |
| Trunk | 11 | 3 | 1 HQ 4 MQ 5 LQ 1 VLQ | 1 MQ 2 LQ | 4 HQ 6 MQ 1 LQ | 2 HQ 1 MQ | Strong | Moderate |
| Pelvis | 6 | 1 | 4 MQ 2 LQ | 1 HQ | 3 HQ 3 MQ | 1 HQ | Strong | Limited |
| Hip | 13 | 3 | 2 HQ 3 MQ 8 LQ | 1 HQ 1 MQ 1 LQ | 2 HQ 8 MQ 3 LQ | 1 HQ 2 MQ | Strong | Moderate |
| Knee | 15 | 3 | 2 HQ 3 MQ 10 LQ | 1 HQ 2 MQ | 3 HQ 9 MQ 3 LQ | 1 HQ 2 MQ | Strong | Moderate |
| Ankle | 11 | 3 | 3 HQ 2 MQ 6 LQ | 3 HQ | 3 HQ 6 MQ 2 LQ | 2 HQ 1 MQ | Strong | Moderate |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. https://doi.org/10.3390/s19071555
Poitras I, Dupuis F, Bielmann M, Campeau-Lecours A, Mercier C, Bouyer LJ, Roy J-S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors. 2019; 19(7):1555. https://doi.org/10.3390/s19071555
Chicago/Turabian StylePoitras, Isabelle, Frédérique Dupuis, Mathieu Bielmann, Alexandre Campeau-Lecours, Catherine Mercier, Laurent J. Bouyer, and Jean-Sébastien Roy. 2019. "Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review" Sensors 19, no. 7: 1555. https://doi.org/10.3390/s19071555
APA StylePoitras, I., Dupuis, F., Bielmann, M., Campeau-Lecours, A., Mercier, C., Bouyer, L. J., & Roy, J.-S. (2019). Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors, 19(7), 1555. https://doi.org/10.3390/s19071555