Hand Rehabilitation and Telemonitoring through Smart Toys

 ,
,  ,
,
Abstract
1. Introduction
2. Related Research
3. Materials and Methods
3.1. Platform Specifications
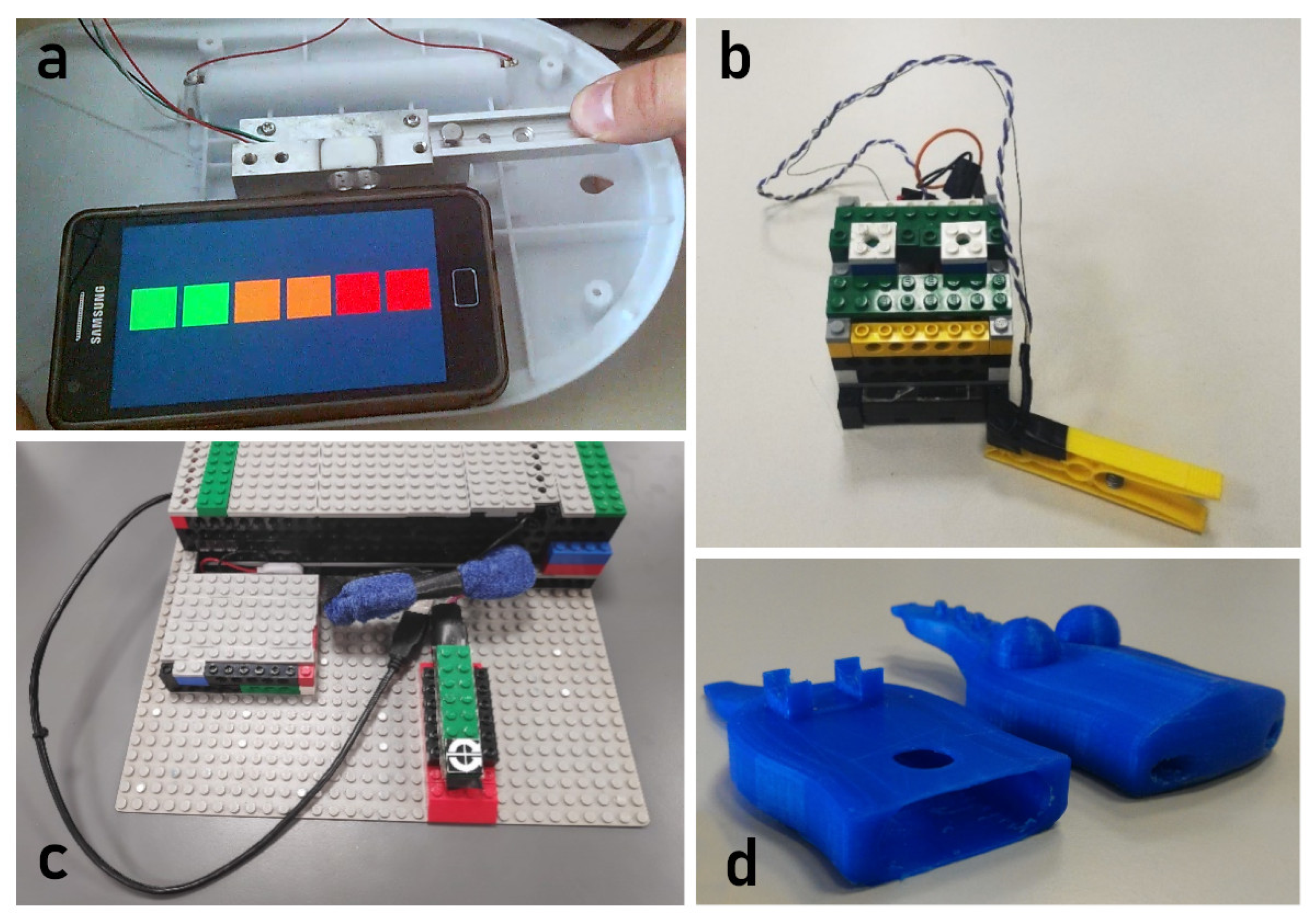
3.2. Platform Design and Development
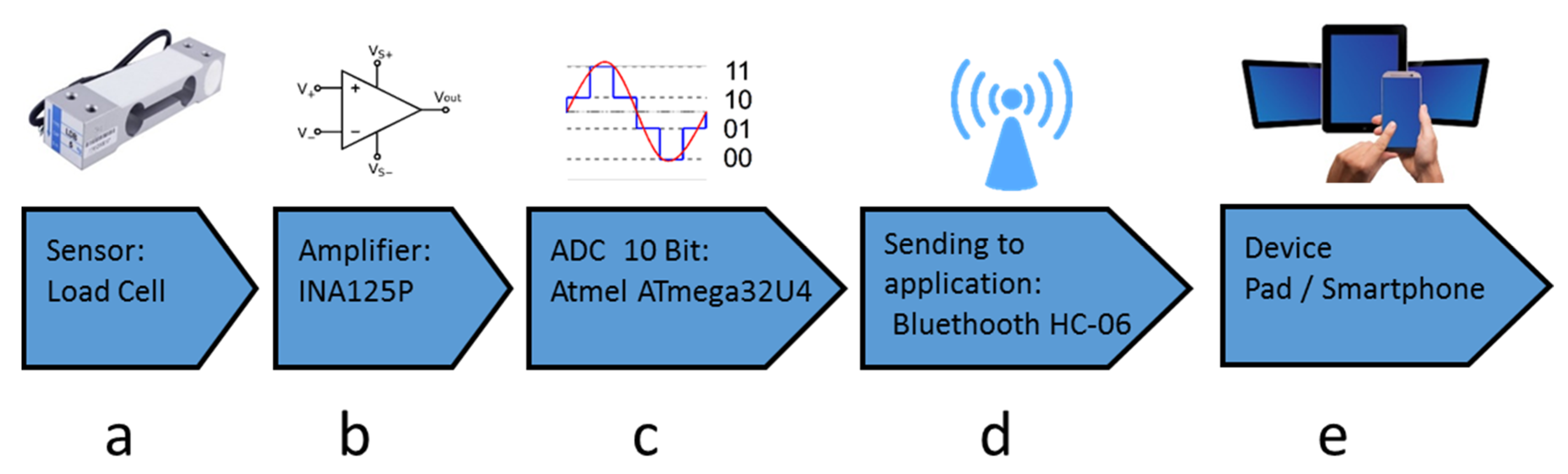
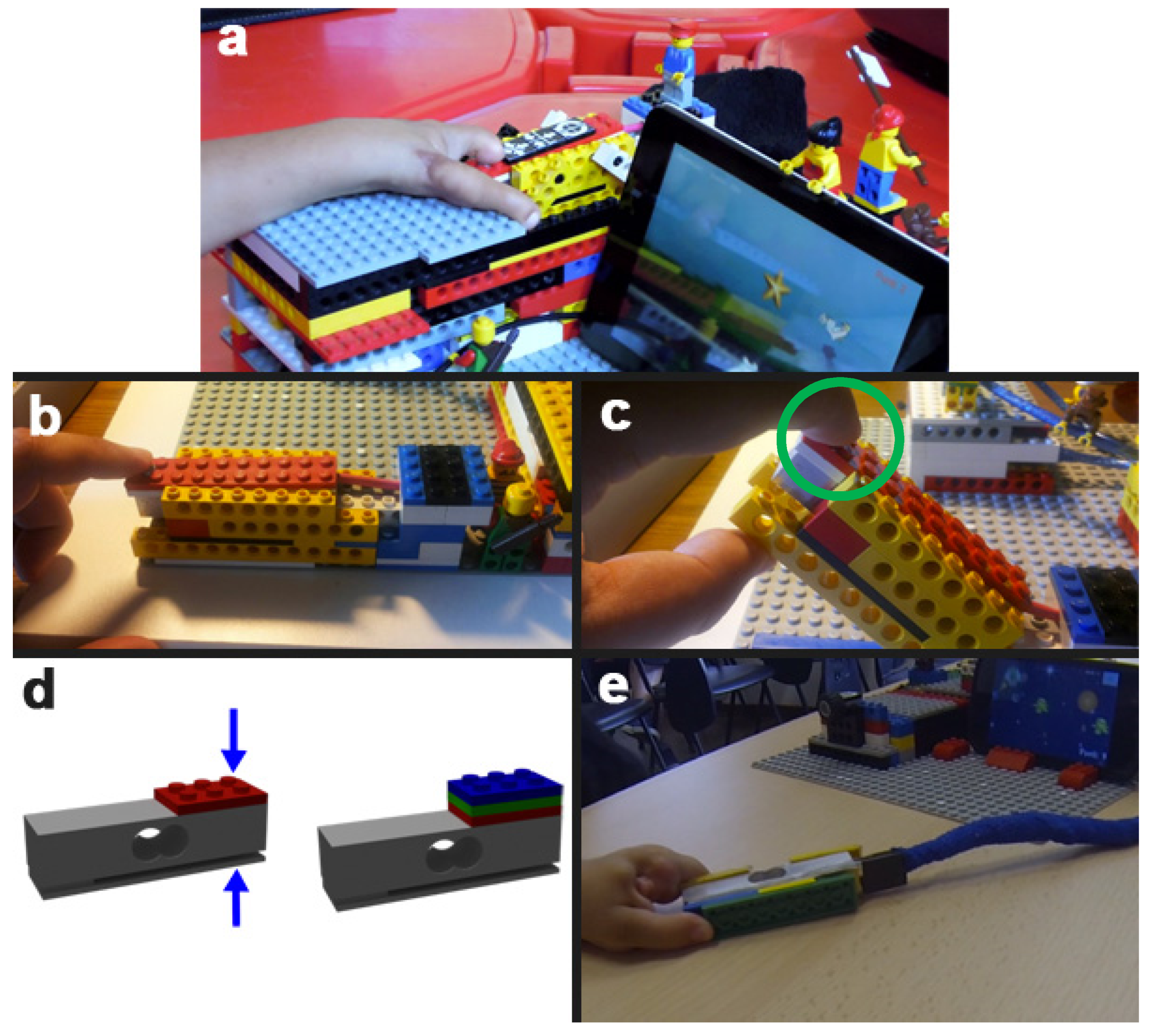
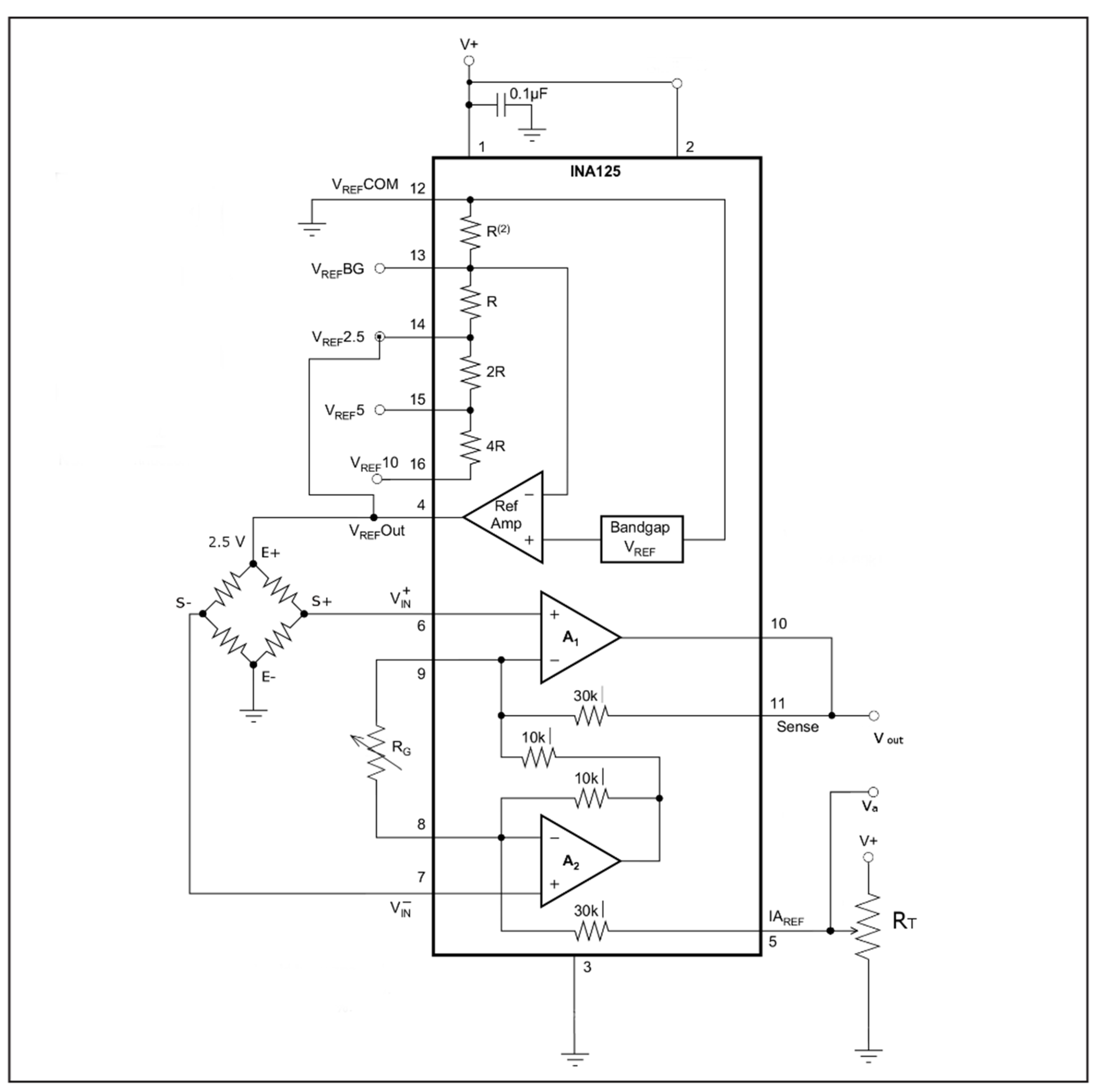
3.2.1. Force Sensing Sub-System
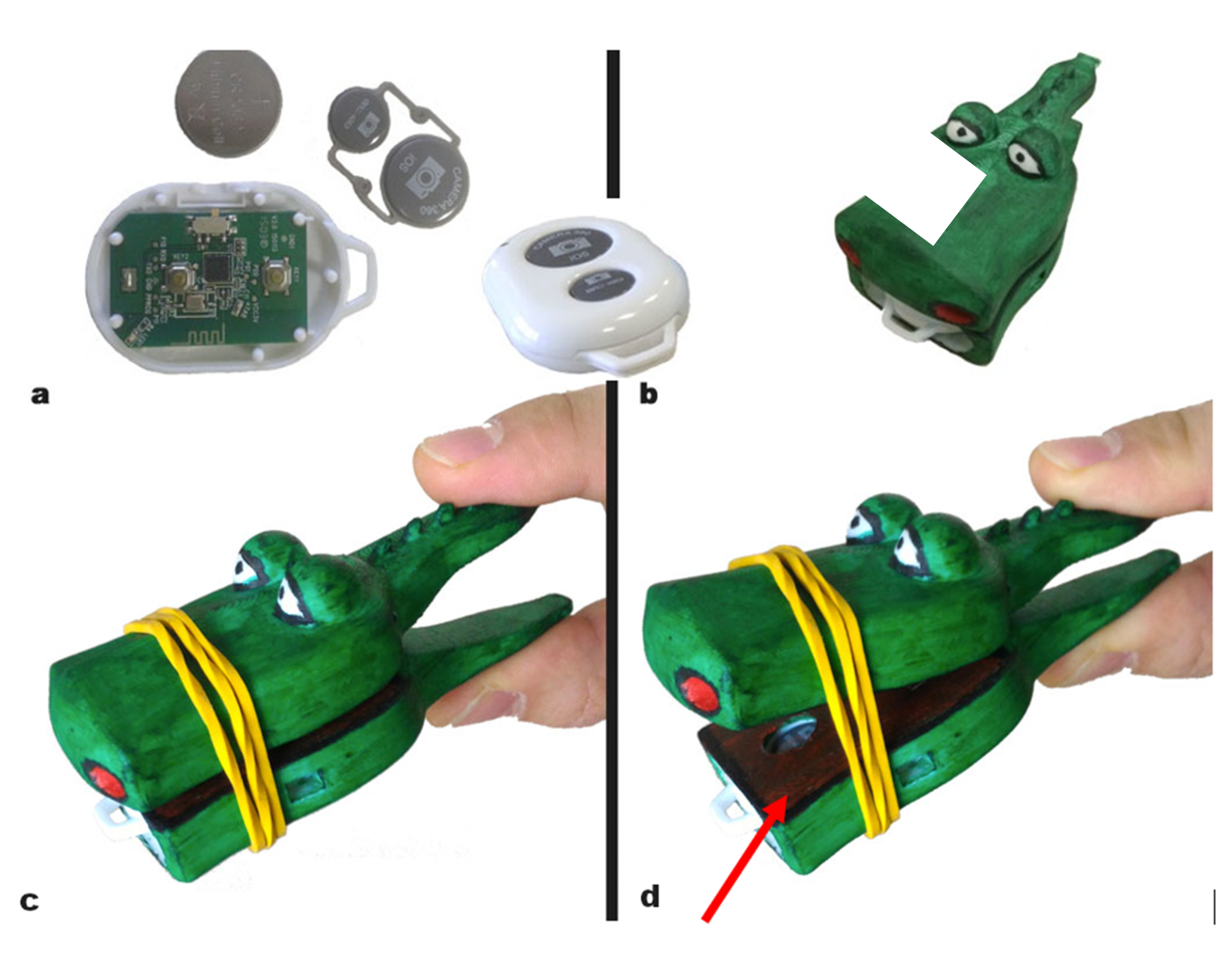
3.2.2. Motion Sensing Sub-System
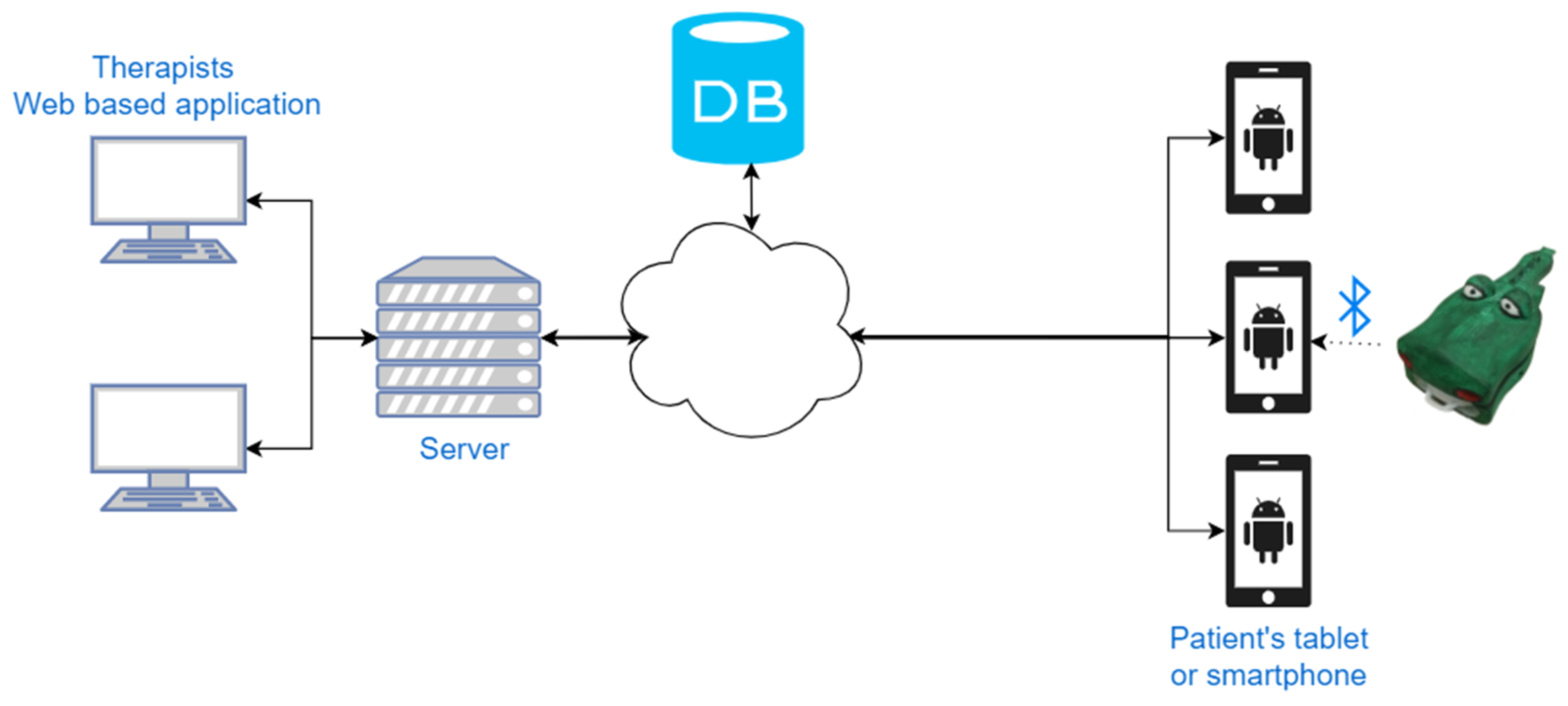
3.2.3. Platform Architecture
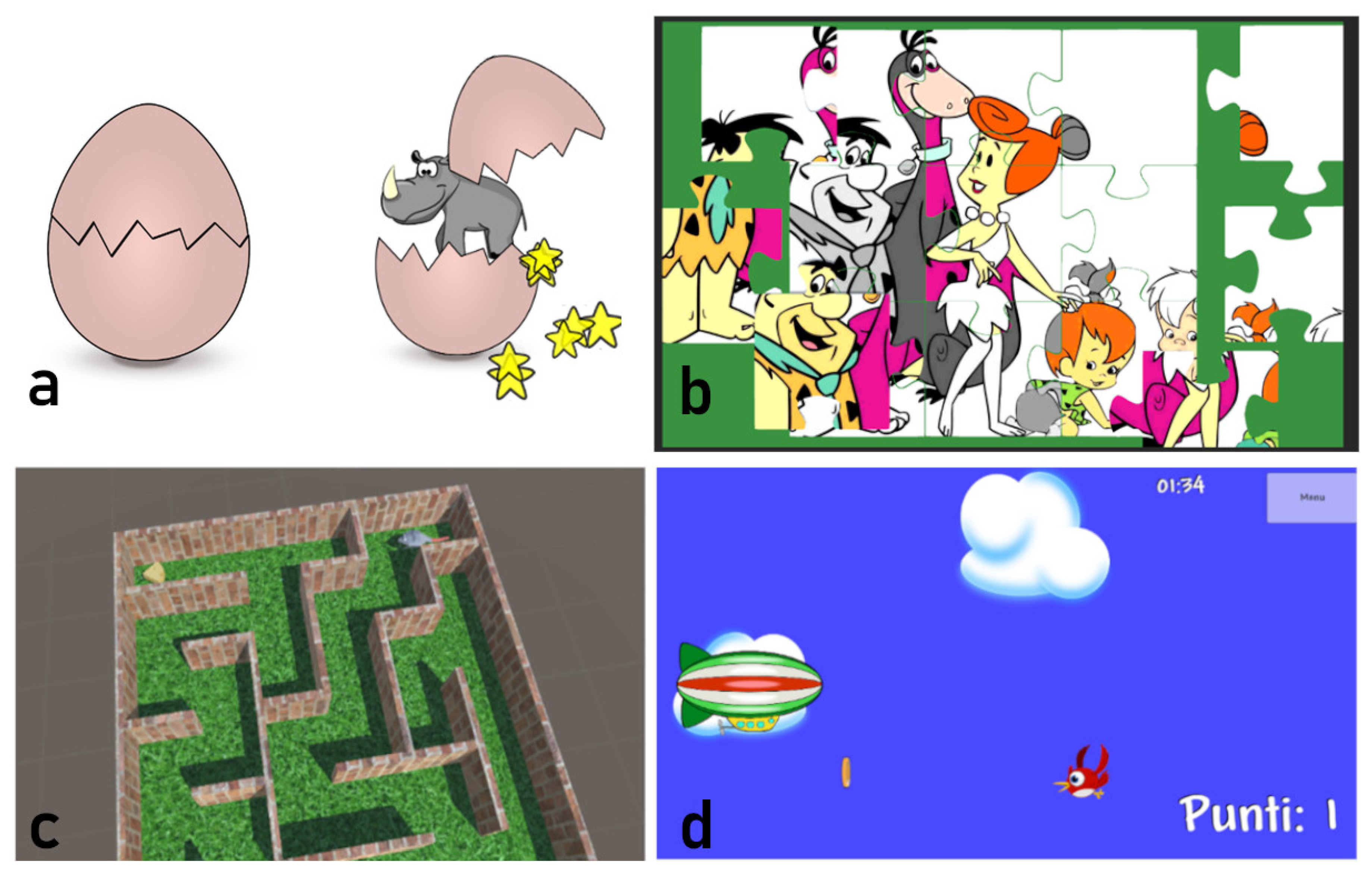
3.3. Therapeutic Exergames
3.3.1. Breaking Eggs
3.3.2. Jigsaw
3.3.3. Mouse & Cheese Maze
3.3.4. Hot Air Balloon (and Similar Themes)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Amplification Design

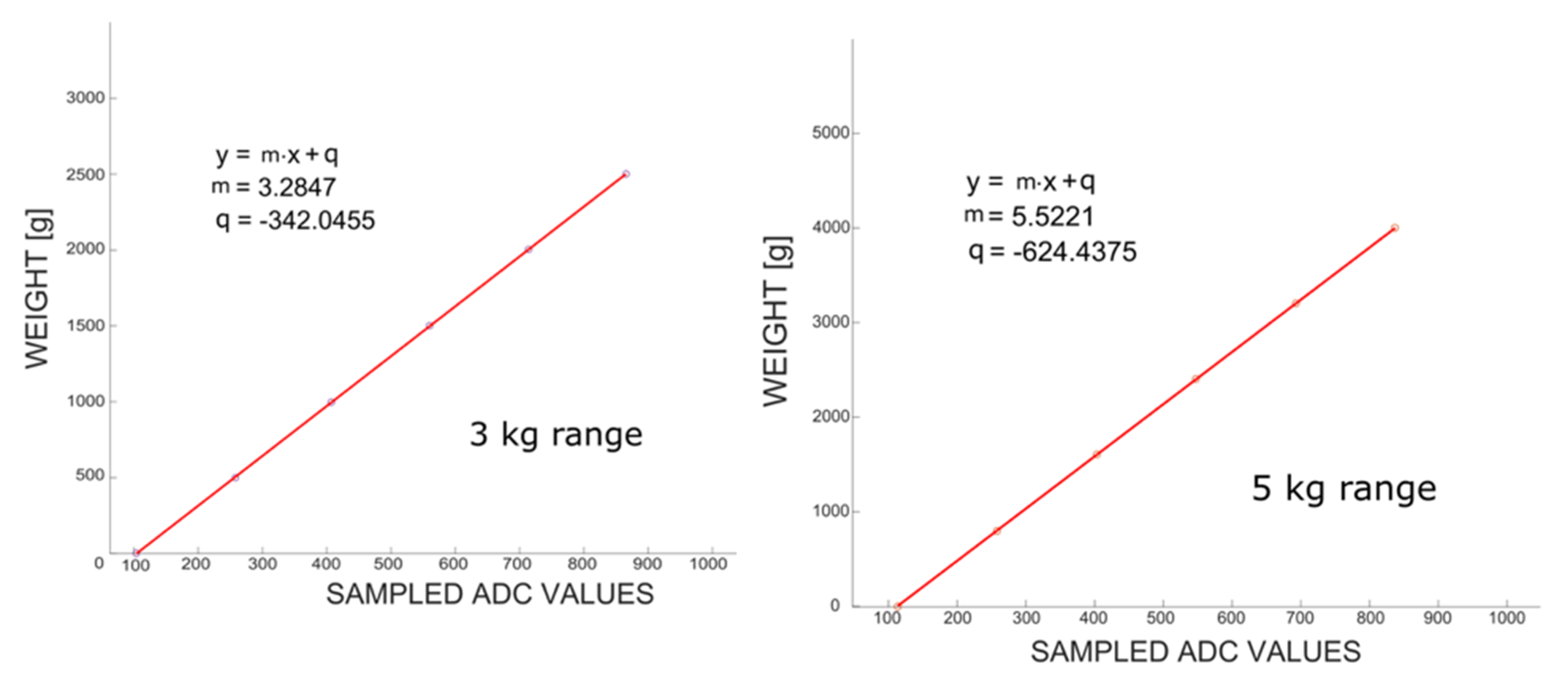
Appendix B. Characterization of Force Measurements


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average 10 Bit Sampled | Real Weight [g] | Computed Weight [g] | Difference [g] |
|---|---|---|---|
| 103.94 | 0 | −0.65 | −0.65 |
| 257.91 | 500 | 505.11 | +5.11 |
| 407.09 | 1000 | 995.10 | −4.9 |
| 560.05 | 1500 | 1497.54 | −2.46 |
| 714.11 | 2001 | 2003.58 | +2.58 |
| 865.34 | 2500 | 2500.33 | +0.33 |
| 1014.23 | 3000 | 2989.38 | −10.62 |
| Average 10 Bit Sampled | Real Weight [g] | Computed Weight [g] | Difference [g] |
|---|---|---|---|
| 113.32 | 0 | 1.33 | +1.33 |
| 257.71 | 800 | 798.67 | −1.33 |
| 402.88 | 1600 | 1600.29 | +0.29 |
| 547.24 | 2400 | 2397.44 | −2.56 |
| 693.11 | 3200 | 3202.98 | +2.98 |
| 837.32 | 4000 | 3999.30 | −0.70 |
| 1015.3 | 5000 | 4982.11 | −17.89 |
| Real Weight | First Measurement [g] | Second Measurement [g] | Absolute Difference [g] |
|---|---|---|---|
| 0 | −0.65 | −5.75 | 5.09 |
| 500 | 505.11 | 503.25 | 1.85 |
| 1000 | 995.10 | 1002.69 | 7.59 |
| 1500 | 1497.54 | 1501.72 | 4.19 |
| 2001 | 2003.58 | 2002.26 | 1.32 |
| 2500 | 2500.33 | 2501.61 | 1.28 |
| 3000 | 2989.38 | 2990.19 | 0.81 |
References
- Lockman, J.J.; McHale, J.P. Object Manipulation in Infancy BT—Action in Social Context: Perspectives on Early Development; Lockman, J.J., Hazen, N.L., Eds.; Springer: Boston, MA, USA, 1989; pp. 129–167. [Google Scholar]
- Little, K.J.; Cornwall, R. Congenital Anomalies of the Hand—Principles of Management. Orthop. Clin. 2016, 47, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.; Wei, F.C. Thumb Reconstruction with Toe Transfer. J. Hand Microsurg. 2010, 2, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Duncan, P. Does the organization of postacute stroke care really matter? Stroke 2001, 32, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Pua, Y.H.; Fortin, K.; Ritchie, C.; Webster, K.E.; Denehy, L.; Bryant, A.L. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Borghese, N.A.; Murray, D.; Paraschiv-Ionescu, A.; de Bruin, E.D.; Bulgheroni, M.; Steblin, A.; Luft, A.; Parra, C. Rehabilitation at Home: A Comprehensive Technological Approach. In Virtual, Augmented Reality and Serious Games for Healthcare 1; Ma, M., Jain, L.C., Anderson, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 289–319. [Google Scholar]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Gensini, G.F.; Alderighi, C.; Rasoini, R.; Mazzanti, M.; Casolo, G. Value of Telemonitoring and Telemedicine in Heart Failure Management. Card. Fail. Rev. 2017, 3, 116–121. [Google Scholar] [CrossRef]
- SilverFit. Available online: https://silverfit.com/en/ (accessed on 4 November 2019).
- Jintronix. Available online: http://www.jintronix.com/ (accessed on 4 November 2019).
- The Rehabilitation Gaming System. 2016. Available online: http://www.aal-europe.eu/projects/rgs/ (accessed on 25 October 2019).
- Pirovano, M.; Mainetti, R.; Baud-Bovy, G.; Lanzi, P.L.; Borghese, N.A. Intelligent Game Engine for Rehabilitation (IGER). IEEE Trans. Comput. Intell. AI Games 2016, 8, 43–55. [Google Scholar] [CrossRef]
- Trombetta, M.; Bazzanello Henrique, P.P.; Brum, M.R.; Colussi, E.L.; De Marchi, A.C.B.; Rieder, R. Motion Rehab AVE 3D: A VR-based exergame for post-stroke rehabilitation. Comput. Methods Programs Biomed. 2017, 151, 15–20. [Google Scholar] [CrossRef]
- Anton, D.; Goni, A.; Illarramendi, A.; Torres-Unda, J.J.; Seco, J. KiReS: A Kinect-Based Telerehabilitation System. In Proceedings of the 2013 IEEE 15th International Conference on e-Health Networking, Applications and Services, Healthcom, Lisbon Portugal, 9–12 October 2013; pp. 444–448. [Google Scholar]
- Rewire Project. 2016. Available online: http://www.rewire-project.eu (accessed on 25 October 2019).
- Nestore-Coach. Available online: https://nestore-coach.eu/home (accessed on 4 November 2019).
- Lozano-Quilis, J.A.; Gil-Gómez, H.; Gil-Gómez, J.A.; Albiol-Pérez, S.; Palacios-Navarro, G.; Fardoun, H.M.; Mashat, A.S. Virtual Rehabilitation for Multiple Sclerosis Using a Kinect-Based System: Randomized Controlled Trial. JMIR Serious Games 2014, 2, e12. [Google Scholar] [CrossRef]
- Ates, S.; Haarman, C.J.W.; Stienen, A.H.A. SCRIPT passive orthosis: Design of interactive hand and wrist exoskeleton for rehabilitation at home after stroke. Auton. Robots 2017, 41, 711–723. [Google Scholar] [CrossRef]
- Borboni, A.; Mor, M.; Faglia, R. Gloreha—Hand Robotic Rehabilitation: Design, Mechanical Model, and Experiments. J. Dyn. Syst. Meas. Control 2016, 138, 111003–111012. [Google Scholar] [CrossRef]
- Wang, B.; Mcdaid, A.; Biglari-Abhari, M.; Aw, K.C. Design and Development of a Glove for Post-Stroke Hand Rehabilitation. In Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics, AIM, Munich, Germany, 26–30 June 2017. [Google Scholar]
- Ma, Z.; Ben-Tzvi, P.; Danoff, J. Hand Rehabilitation Learning System with an Exoskeleton Robotic Glove. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, F.; Song, Y.; Cao, X.; Meng, F. A Soft Robotic Glove for Hand Rehabilitation Using Pneumatic Actuators with Variable Stiffness. In Proceedings of the International Conference on Intelligent Robotics and Applications, Shenyang, China; 2019; pp. 119–129. [Google Scholar]
- Park, W.; Jeong, W.; Kwon, G.H.; Kim, Y.H.; Kim, L. A Rehabilitation Device to Improve the Hand Grasp Function of Stroke Patients using a Patient-Driven Approach. In Proceedings of the IEEE International Conference on Rehabilitation Robotic, Seattle, WA, USA, 24–26 June 2013. [Google Scholar]
- Klug, F.; Hessinger, M.; Koka, T.; Witulla, P.; Will, C.; Schlichting, T.; Endl, C.; Albenstetter, A.; Champagne, P.O.; Gagnon, D.H.; et al. An Anthropomorphic Soft Exosuit for Hand Rehabilitation. IEEE Int. Conf. Rehabil. Robot. 2019, 2019, 1121–1126. [Google Scholar] [PubMed]
- Rudd, G.; Daly, L.; Jovanovic, V.; Cuckov, F. A Low-Cost Soft Robotic Hand Exoskeleton for Use in Therapy of Limited Hand–Motor Function. Appl. Sci. 2019, 9, 3751. [Google Scholar] [CrossRef]
- Cafolla, D. A personalized flexible exoskeleton for finger rehabilitation: a conceptual design. In IFToMM World Congress on Mechanism and Machine Science, Krakow, Poland; Springer: Cham, Germany, 2019; pp. 73–82. [Google Scholar]
- Chang, W.H.; Kim, Y.H. Robot-assisted Therapy in Stroke Rehabilitation. J. Stroke 2013, 15, 174–181. [Google Scholar] [CrossRef]
- Alexanderson, S.; O’Sullivan, C.; Beskow, J. Real-time labeling of non-rigid motion capture marker sets. Comput. Graph. 2017, 69, 59–67. [Google Scholar] [CrossRef][Green Version]
- Alimanova, M.; Borambayeva, S.; Kozhamzharova, D.; Kurmangaiyeva, N.; Ospanova, D.; Tyulepberdinova, G.; Gaziz, G.; Kassenkhan, A. Gamification of Hand Rehabilitation Process using Virtual Reality Tools: Using Leap Motion for Hand Rehabilitation. In Proceedings of the 2017 1st IEEE International Conference on Robotic Computing, IRC 2017, Laguna Hills, CA, USA, 10–12 April 2017. [Google Scholar]
- Taylor, J.; Curran, K. Using leap motion and gamification to facilitate and encourage rehabilitation for hand injuries: leap motion for rehabilitation. In Handbook of Research on Holistic Perspectives in Gamification for Clinical Practice; IGI Global: London, UK, 2016; pp. 183–192. [Google Scholar]
- Proffitt, R.; Sevick, M.; Chang, C.Y.; Lange, B. User-Centered Design of a Controller-Free Game for Hand Rehabilitation. Games Health J. 2015, 4, 259–264. [Google Scholar] [CrossRef]
- Valentini, P.P.; Pezzuti, E. Accuracy in fingertip tracking using Leap Motion Controller for interactive virtual applications. Int. J. Interact. Des. Manuf. 2017, 11, 641–650. [Google Scholar] [CrossRef]
- Guzsvinecz, T.; Szucs, V.; Sik-Lanyi, C. Suitability of the kinect sensor and leap motion controller-A literature review. Sensors 2019, 19, 1072. [Google Scholar] [CrossRef]
- Rand, D.; Schejter-Margalit, T.; Dudkiewicz, I.; Kizony, R.; Zeilig, G.; Kizony, R. The Use of the iPad for Poststroke Hand Rehabilitation; A Pilot Study. In Proceedings of the 2013 International Conference on Virtual Rehabilitation, ICVR 2013, Philadelphia, PA, USA, 26–29 August 2013. [Google Scholar]
- Levac, D.; Dumas, H.M.; Meleis, W. A Tablet-Based Interactive Movement Tool for Pediatric Rehabilitation: Development and Preliminary Usability Evaluation. JMIR Rehabil. Assist. Technol. 2018, 5, e10307. [Google Scholar] [CrossRef]
- ReHand. Available online: https://rehand.net/ (accessed on 25 October 2019).
- Core Hand. Available online: https://www.digitalaffinity.co.uk/mobile/corehand/iphone-ios-app-core-hand.php (accessed on 25 October 2019).
- Dexteria—Fine Motor Skill Development. Available online: https://apps.apple.com/us/app/dexteria-fine-motor-skill/id420464455?ign-mpt=uo%3D4 (accessed on 25 October 2019).
- MoTrack TherapyTM—The Home Hand Rehabilitation SolutionTM. Available online: https://www.motracktherapy.com/ (accessed on 25 October 2019).
- Hogrel, J.Y. Grip strength measured by high precision dynamometry in healthy subjects from 5 to 80 years. BMC Musculoskelet. Disord. 2015, 16, 139. [Google Scholar] [CrossRef] [PubMed]
- Takei Digital Dynamometer. Available online: https://www.pandamed.co.uk/product/takei-4501-digital-dynamometer/ (accessed on 4 November 2019).
- Richards, L.; Palmiter-Thomas, P. A Critical Review of Tools, Methods, and Clinical Utility for Grip Strength Measurement. Critic. Rev. Phys. Rehabilit. Med. 2017, 29, 1–4. [Google Scholar] [CrossRef]
- Neumann, S.; Kwisda, S.; Krettek, C.; Gaulke, R. Comparison of the grip strength using the martin-vigorimeter and the JAMAR-dynamometer: Establishment of normal values. In Vivo 2017, 31, 917–924. [Google Scholar] [PubMed]
- Jaber, R.; Hewson, D.J.; Duchêne, J. Design and validation of the Grip-ball for measurement of hand grip strength. Med. Eng. Phys. 2012, 34, 1356–1361. [Google Scholar] [CrossRef] [PubMed]
- Hewson, D.J.; Li, K.; Frèrejean, A.; Hogrel, J.Y.; Duchêne, J. Domo-Grip: Functional Evaluation and Rehabilitation using Grip Force. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC’10, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1308–1311. [Google Scholar]
- Pintaric, T.; Kment, T.; Spreicer, W. SqueezeOrb: A Low-Cost Pressure-Sensitive User Input Device. In Proceedings of the ACM Symposium on Virtual Reality Software and Technology, VRST, Bordeaux, France, 27–29 October 2008. [Google Scholar]
- Lookee® Smart Ball—Hand Exerciser Grip Strengthener & Trainer. Available online: https://www.lookeetech.com/products/lookee-smart-ball-hand-exerciser-grip-strengthener-trainer-with-app-battle-games (accessed on 25 October 2019).
- Gripable. Available online: https://www.gripable.co/how-it-works (accessed on 25 October 2019).
- MacKenzie, C.L.; Iberall, T. The Grasping Hand; Elsevier: Amsterdam, The Netherlands, 1994; Volume 104. [Google Scholar]
- Jean-Baptiste, E.M.D.; Nabiei, R.; Parekh, M.; Fringi, E.; Drozdowska, B.; Baber, C.; Jancovic, P.; Rotshein, P.; Russell, M. Intelligent Assistive System Using Real-Time Action Recognition for Stroke Survivors. In Proceedings of the 2014 IEEE International Conference on Healthcare Informatics, Verona, Italy, 15–17 September 2014; pp. 39–44. [Google Scholar]
- Sen.se. Available online: https://www.myrobotcenter.eu/en/sense (accessed on 4 November 2019).
- Serio, S.M.; Cecchi, F.; Assaf, T.; Laschi, C.; Dario, P. Design and Development of a Sensorized Wireless Toy for Measuring Infants’ Manual Actions. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, M.; Surer, E.; Mainetti, R.; Lanzi, P.L.; Alberto Borghese, N. Exergaming and rehabilitation: A methodology for the design of effective and safe therapeutic exergames. Entertain. Comput. 2016, 14, 55–65. [Google Scholar] [CrossRef]
- Eckman, M.; Gorski, I.; Mehta, K. Leveraging design thinking to build sustainable mobile health systems. J. Med. Eng. Technol. 2016, 40, 422–430. [Google Scholar] [CrossRef]
- Borghese, N.A.; Bottini, G.; Sedda, A. Videogame Based Neglect Rehabilitation: A Role for Spatial Remapping and Multisensory Integration? Front. Hum. Neurosci. 2013, 7, 1–3. [Google Scholar] [CrossRef][Green Version]
- Elnaggar, A.; Reichardt, D. Digitizing the hand rehabilitation using serious games methodology with user-centered design approach. In Proceedings of the 2016 International Conference on Computational Science and Computational Intelligence (CSCI) Las Vegas, Nevada, WA, USA, 5–7 December 2016; pp. 13–22. [Google Scholar]
- Sullivan, S. Physical Rehabilitation; F.A. Davis Company: Philadelphia, PA, USA, 2019. [Google Scholar]
- HC-06 Datasheet. Available online: https://www.olimex.com/Products/Components/RF/BLUETOOTH-SERIAL-HC-06/resources/hc06.pdf (accessed on 4 November 2019).
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 745–754. [Google Scholar] [CrossRef]
- Norman, D.A. Emotional Design: Why We Love (or Hate) Everyday Things; Basic Civitas Books, 2004. [Google Scholar]
- Borghese, N.A.; Mainetti, R.; Essenziale, J.; Cavalli, E.; Mancon, E.M.; Pajardi, G. Hand Rehabilitation with Toys with Embedded Sensors. In Converging Clinical and Engineering Research on Neurorehabilitation II.; Springer: Berlin/Heidelberg, Germany, 2016; Volume 15, pp. 425–430. [Google Scholar]
- Borghese, N.A.; Pezzera, M.; Mainetti, R.; Essenziale, J.; Cazzaniga, R.; Reggiori, B.; Mercurio, S.; Confalonieri, P. A Cloud-Based Platform for Effective Supervision of Autonomous Home Rehabilitation through Exer-Games. In Proceedings of the 2018 IEEE 6th International Conference on Serious Games and Applications for Health, SeGAH 2018, Wien, Austria, 16–18 May 2018; pp. 1–6. [Google Scholar]
- Pezzera, M.; Tironi, A.; Essenziale, J.; Mainetti, R.; Alberto, B.N. Approaches for increasing patient’s engagement and motivation in exer-games-based autonomous telerehabilitation. In Proceedings of the 2019 IEEE 7th International Conference on Serious Games and Applications for Health (SeGAH), Kyoto, Japan, 5–7 August 2019. [Google Scholar]
- Maundy, B.; Gift, S.J.G. Strain gauge amplifier circuits. IEEE Trans. Instrum. Meas. 2013, 62, 693–700. [Google Scholar] [CrossRef]
- Ştefănescu, D.M. Wheatstone Bridge—The Basic Circuit for Strain Gauge Force Transducers. In Handbook of Force Transducers: Principles and Components; Springer: Berlin/Heidelberg, Germany, 2011; pp. 347–360. [Google Scholar]
- Muller, I.; De Brito, R.; Pereira, C.E.; Brusamarello, V. Load cells in force sensing analysis—Theory and a novel application. IEEE Instrum. Meas. Mag. 2010, 13, 15–19. [Google Scholar] [CrossRef]
- Horowitz, P.; Hill, W. The Art of Electronics; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Texas Instruments, INA 125 Datasheet. Available online: http://www.ti.com/lit/ds/symlink/ina125.pdf (accessed on 4 November 2019).
- Frosio, I.; Stuani, S.; Borghese, N.A. Autocalibration of MEMS Accelerometer. In Proceedings of the Conference Record-IEEE Instrumentation and Measurement Technology Conference, Sorrento, Italy; 2006. [Google Scholar]
- Adafruit Learning System. 2016. Available online: https://learn.adafruit.com/smart-cocktail-shaker/ (accessed on 4 November 2019).
- Trochim, W.M.K. The Research Methods Knowledge Base, 2nd ed.; Atomic Dog: Cincinnati, OH, USA, 2006. [Google Scholar]









© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borghese, N.A.; Essenziale, J.; Mainetti, R.; Mancon, E.; Pagliaro, R.; Pajardi, G. Hand Rehabilitation and Telemonitoring through Smart Toys. Sensors 2019, 19, 5517. https://doi.org/10.3390/s19245517
Borghese NA, Essenziale J, Mainetti R, Mancon E, Pagliaro R, Pajardi G. Hand Rehabilitation and Telemonitoring through Smart Toys. Sensors. 2019; 19(24):5517. https://doi.org/10.3390/s19245517
Chicago/Turabian StyleBorghese, N. Alberto, Jacopo Essenziale, Renato Mainetti, Elena Mancon, Rossella Pagliaro, and Giorgio Pajardi. 2019. "Hand Rehabilitation and Telemonitoring through Smart Toys" Sensors 19, no. 24: 5517. https://doi.org/10.3390/s19245517
APA StyleBorghese, N. A., Essenziale, J., Mainetti, R., Mancon, E., Pagliaro, R., & Pajardi, G. (2019). Hand Rehabilitation and Telemonitoring through Smart Toys. Sensors, 19(24), 5517. https://doi.org/10.3390/s19245517