Estimating Driving Fatigue at a Plateau Area with Frequent and Rapid Altitude Change


Abstract
:1. Introduction
1.1. Background
1.2. Literature Review
1.3. Objective and Contributions
2. Experimental Design
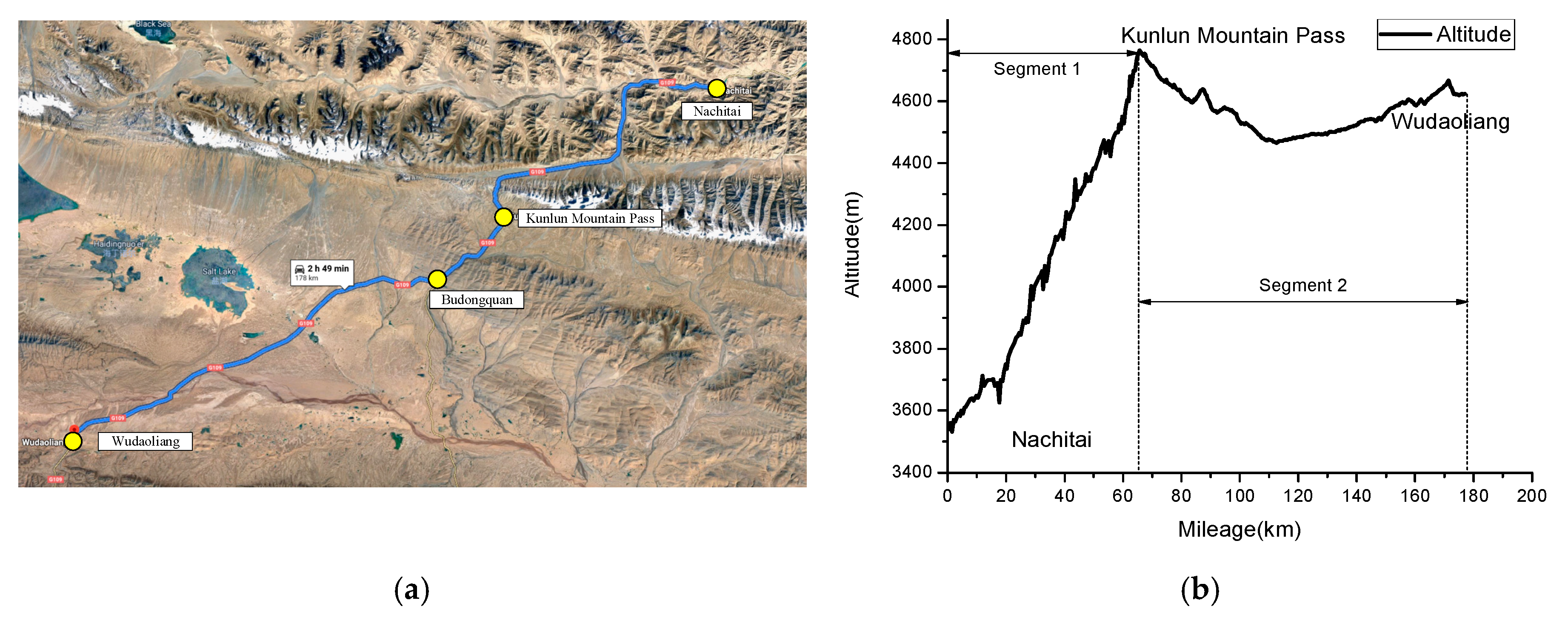
2.1. Experimental Environment
2.2. Sample Population
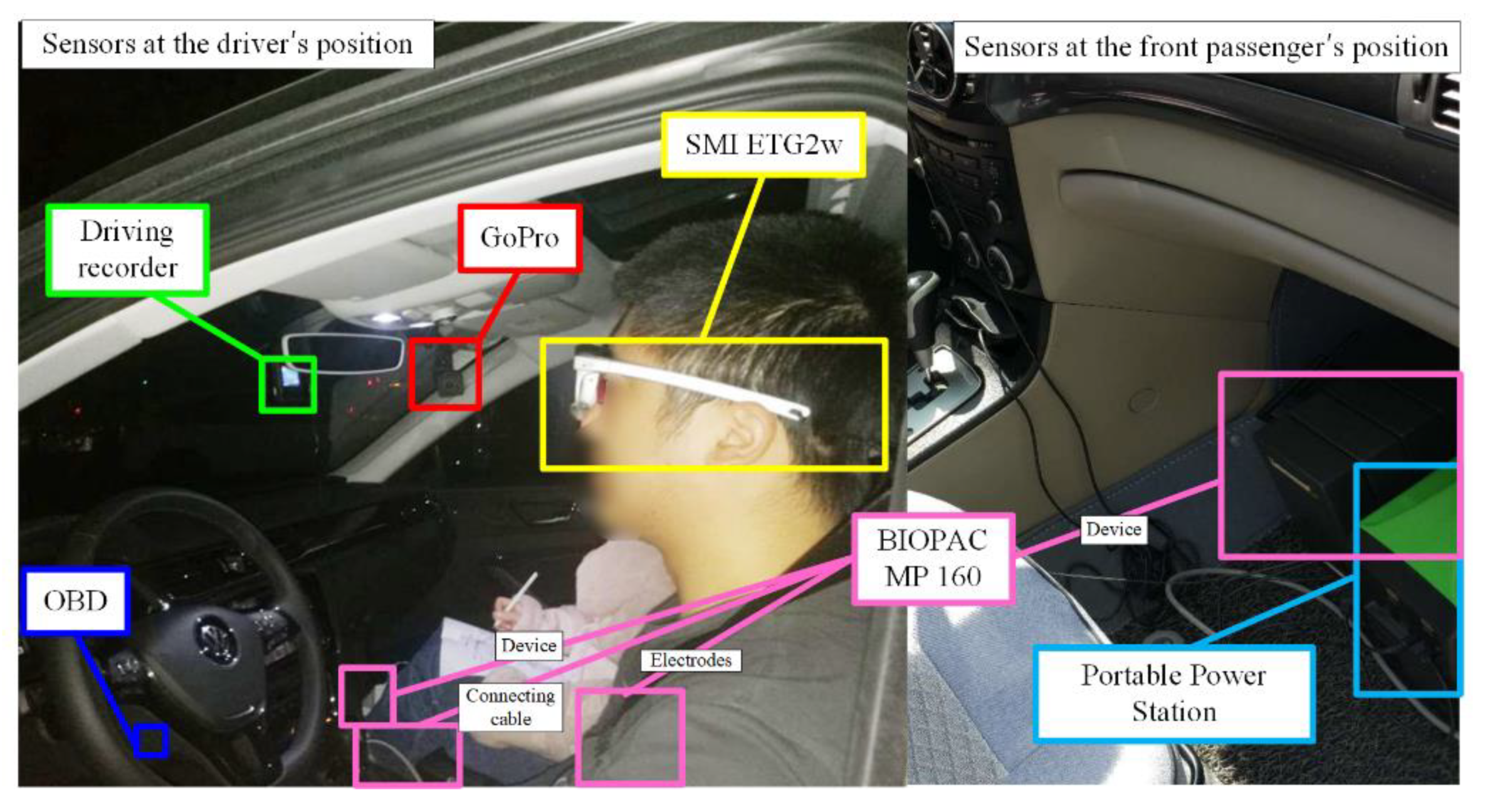
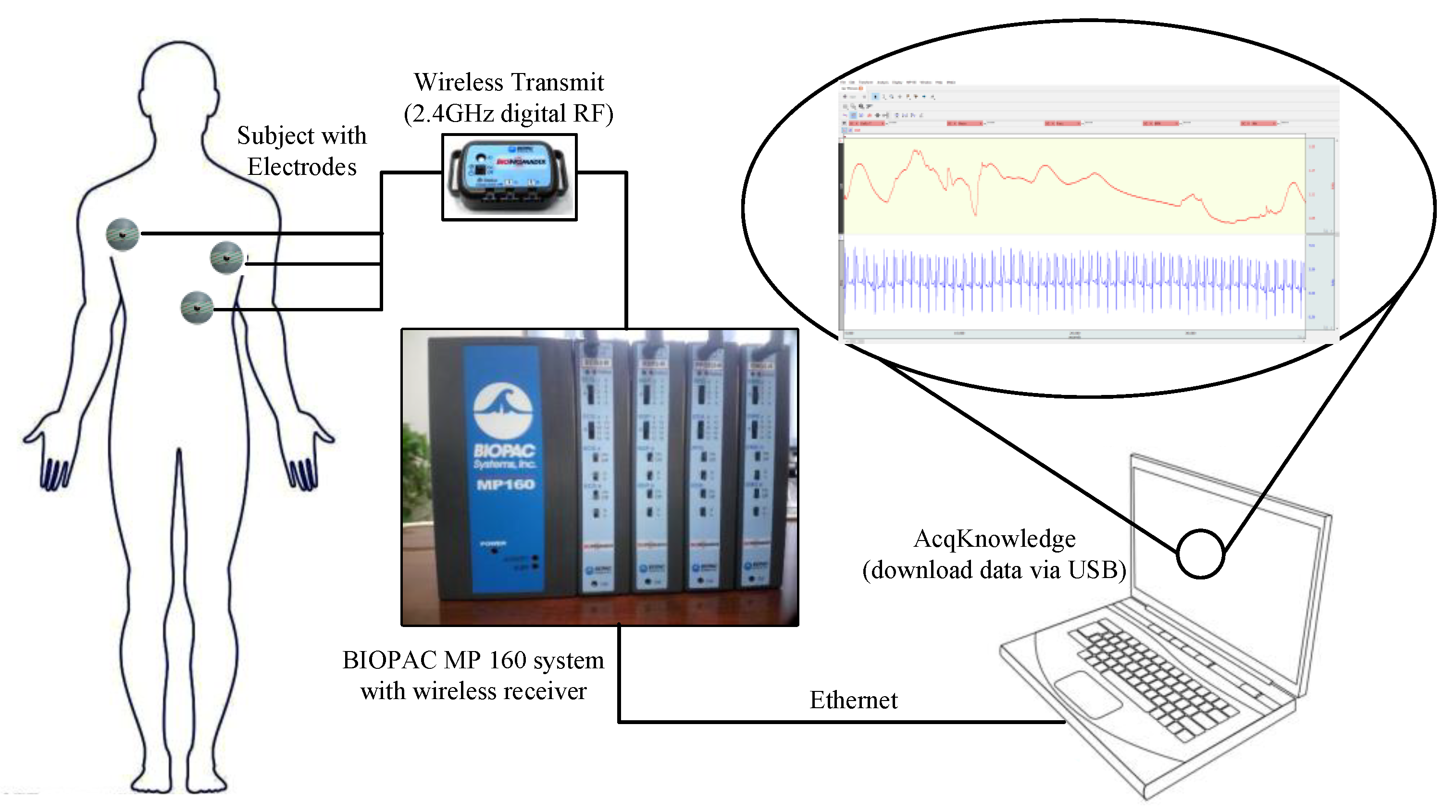
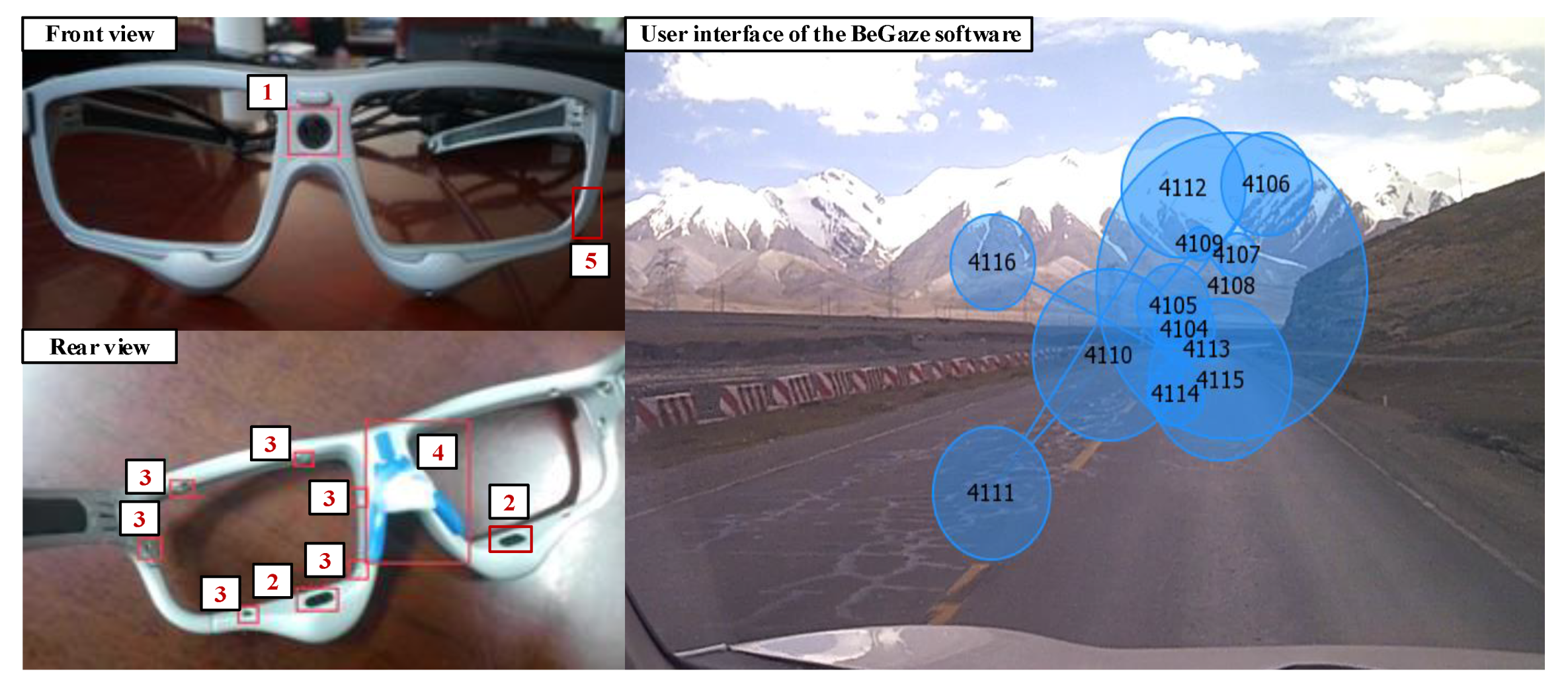
2.3. Equipment Selection and Installation
2.4. Experimental Process
2.5. Measures of Data Reliability and Driving Safety
3. Revised DFD Estimation Method
3.1. Process for Revision of DFD Estimation
3.2. Comparison of DFD Estimation Methods
3.3. Revised DFD Estimation for a Segment with Constant Altitude Change
4. Results
4.1. Driving Fatigue Characteristics on the Qinghai-Tibet Highway
4.2. Verifications of DFD Estimation Methods
4.3. Revised DFD Estimation for a Road Segment with Constant Altitude Change
5. Discussion
6. Conclusions
- The proposed method can be used to estimate the DFD for road segments with rapid altitude change using the heart rate data collected from portable sensors.
- The DFD increases the fastest at the road segment with constant and rapid altitude increases and vice versa. The DFD at the road segment with little altitude change also represents an S-shape curve.
- The proposed method was only tested at the road segment with an altitude range from 3540 to 4767 m. More data are needed to verify the DFD estimation method at the road segment with another altitude level of the plateau.
Author Contributions
Funding
Conflicts of Interest
References
- Fiore, D.C.; Hall, S.; Shoja, P. Altitude illness: Risk factors, prevention, presentation, and treatment. Am. Fam. Phys. 2010, 82, 1103–1110. [Google Scholar]
- Luks, A.M.; Swenson, E.R.; Bärtsch, P. Acute high-altitude sickness. Eur. Respir. Rev. 2017, 26, 160096. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Cheng, H.T.; Liu, J.B.; Li, Y. Eye Gaze Characteristics of Overtaking Process in Very High Altitude Area. China J. Highw. Transp. 2018, 31, 10–17. [Google Scholar]
- Basnyat, B.; Murdoch, D.R. High-altitude illness. Lancet 2003, 361, 1967–1974. [Google Scholar] [CrossRef]
- Borghini, G.; Astolfi, L.; Vecchiato, G.; Mattia, D.; Babiloni, F. Measuring neurophysiological signals in aircraft pilots and car drivers for the assessment of mental workload, fatigue and drowsiness. Neurosci. Biobehav. Rev. 2014, 44, 58–75. [Google Scholar] [CrossRef]
- Goodall, S.; Twomey, R.; Amann, M.; Ross, E.Z.; Lovering, A.T.; Romer, L.M.; Subudhi, A.W.; Roach, R.C. AltitudeOmics: Exercise-induced supraspinal fatigue is attenuated in healthy humans after acclimatization to high altitude. Acta Physiol. 2014, 210, 875–888. [Google Scholar] [CrossRef]
- Ji, Q.; Zhu, Z.; Lan, P. Real-time nonintrusive monitoring and prediction of driver fatigue. IEEE Trans. Veh. Technol. 2004, 53, 1052–1068. [Google Scholar] [CrossRef]
- Beidleman, B.A.; Tighiouart, H.; Schmid, C.H.; Fulco, C.S.; Muza, S.R. Predictive Models of Acute Mountain Sickness after Rapid Ascent to Various Altitudes. Med. Sci. Sports Exerc. 2013, 45, 792–800. [Google Scholar] [CrossRef]
- Ji, Q.; Yang, X. Real-Time Eye, Gaze, and Face Pose Tracking for Monitoring Driver Vigilance. Real-Time Imaging 2002, 8, 357–377. [Google Scholar] [CrossRef]
- Jiao, K.; Li, Z.; Chen, M.; Wang, C.; Qi, S. Effect of different vibration frequencies on heart rate variability and driving fatigue in healthy drivers. Int. Arch. Occup. Environ. Health 2004, 77, 205–212. [Google Scholar] [CrossRef]
- Li, Y.; Wang, F.; Ke, H.; Wang, L.L.; Xu, C.C. A Driver’s Physiology Sensor-Based Driving Risk Prediction Method for Lane-Changing Process Using Hidden Markov Model. Sensors 2019, 19, 2670. [Google Scholar] [CrossRef] [PubMed]
- Sung, E.J.; Min, B.C.; Kim, S.C.; Kim, C.J. Effects of oxygen concentrations on driver fatigue during simulated driving. Appl. Ergon. 2005, 36, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.-B.; Yang, Y. Safety of Driving Behavior on Low-Volume Roads in China: Case Study of Qinghai–Tibet Highway. Transp. Res. Rec. 2011, 2203, 100–105. [Google Scholar] [CrossRef]
- Liu, J.; Ma, X.; Zhang, Z.; Guo, Z.; Liu, B. Fatigue characteristics of driver in Qinghai-Tibet Plateau based on electrocardiogram analysis. J. Traffic Transp. Eng. 2016, 16, 151–158. [Google Scholar]
- Khushaba, R.N.; Kodagoda, S.; Lal, S.; Dissanayake, G. Driver drowsiness classification using fuzzy wavelet-packet-based feature-extraction algorithm. IEEE Trans. Biomed. Eng. 2010, 58, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Lal, S.K.L.; Craig, A. A critical review of the psychophysiology of driver fatigue. Biol. Psychol. 2001, 55, 173–194. [Google Scholar] [CrossRef]
- Gershon, P.; Shinar, D.; Ronen, A. Evaluation of experience-based fatigue countermeasures. Accid. Anal. Prev. 2009, 41, 969–975. [Google Scholar] [CrossRef]
- Ahsberg, E.; Gamberale, F.; Gustafsson, K. Perceived fatigue after mental work: An experimental evaluation of a fatigue inventory. Ergonomics 2000, 43, 252–268. [Google Scholar] [CrossRef]
- Yang, L.; Ma, R.; Zhang, H.M.; Guan, W.; Jiang, S. Driving behavior recognition using EEG data from a simulated car-following experiment. Accid. Anal. Prev. 2018, 116, 30–40. [Google Scholar] [CrossRef]
- Kaye, S.-A.; Lewis, I.; Freeman, J. Comparison of self-report and objective measures of driving behavior and road safety: A systematic review. J. Saf. Res. 2018, 65, 141–151. [Google Scholar] [CrossRef]
- Wang, M.S.; Jeong, N.T.; Kim, K.S.; Choi, S.B.; Yang, S.M.; You, S.H.; Lee, J.H.; Suh, M.W. Drowsy behavior detection based on driving information. Int. J. Automot. Technol. 2016, 17, 165–173. [Google Scholar] [CrossRef]
- Li, Y.; Hu, W.B.; Zhang, X.Y.; Nan, S.R.; Zhou, W.H. Safety physiology characteristics of bicyclists on reverse riding conditions. China Saf. Sci. J. 2017, 27, 54–59. [Google Scholar]
- Schleicher, R.; Galley, N.; Briest, S.; Galley, L. Blinks and saccades as indicators of fatigue in sleepiness warnings: Looking tired? Ergonomics 2008, 51, 982–1010. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Yin, B.; Sun, Y. Nonintrusive driver fatigue detection. In Proceedings of the 2008 IEEE International Conference on Networking, Sensing and Control, Sanya, China, 6–8 April 2008; IEEE: Piscataway, NJ, USA, 2008. [Google Scholar]
- Jin, S.; Park, S.-Y.; Lee, J.-J. Driver fatigue detection using a genetic algorithm. Artif. Life Robot. 2007, 11, 87–90. [Google Scholar] [CrossRef]
- Tewari, V.; Dewangan, K.; Karmakar, S. Operator’s fatigue in field operation of hand tractors. Biosyst. Eng. 2004, 89, 1–11. [Google Scholar] [CrossRef]
- Takei, Y.; Furukawa, Y. Estimate of driver’s fatigue through steering motion. In Proceedings of the 2005 IEEE International Conference on Systems, Man and Cybernetics, Waikoloa, HI, USA, 12 October 2005; IEEE: Piscataway, NJ, USA, 2005. [Google Scholar]
- Oron-Gilad, T.; Ronen, A. Road characteristics and driver fatigue: A simulator study. Traffic Inj. Prev. 2007, 8, 281–289. [Google Scholar] [CrossRef]
- Guo, Y.; Essa, M.; Sayed, T.; Haque, M.M.; Washington, S. A comparison between simulated and field-measured conflicts for safety assessment of signalized intersections in Australia. Transp. Res. Part C Emerg. Technol. 2019, 101, 96–110. [Google Scholar] [CrossRef]
- Sahayadhas, A.; Sundaraj, K.; Murugappan, M. Detecting driver drowsiness based on sensors: A review. Sensors 2012, 12, 16937–16953. [Google Scholar] [CrossRef]
- Li, Y.; Zhou, W.H.; Nan, S.R.; Wang, F.; Chen, K.M. Redesign of the cross-section of bicycle lanes considering electric bicycles. Proc. Inst. Civ. Eng.-Transp. 2017, 170, 255–266. [Google Scholar] [CrossRef]
- Patel, M.; Lal, S.K.; Kavanagh, D.; Rossiter, P. Applying neural network analysis on heart rate variability data to assess driver fatigue. Expert Syst. Appl. 2011, 38, 7235–7242. [Google Scholar] [CrossRef]
- Li, Z.; Jiao, K.; Chen, M.; Wang, C. Reducing the effects of driving fatigue with magnitopuncture stimulation. Accid. Anal. Prev. 2004, 36, 501–505. [Google Scholar] [CrossRef]
- Li, Y.; Guo, X.; Yang, J.; He, S.; Liu, Y. Routes classification method at intersections group using wavelet transform and spectrum analysis. J. Southeast Univ. (Nat. Sci. Ed.) 2012, 42, 168–172. [Google Scholar]
- Li, Y.; Yang, J.; Guo, X.C.; Yan, Y.D. Critical route identification method at related intersection group based on wavelet transform. China J. Highw. Transp. 2012, 25, 135–140. [Google Scholar]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Scott-Parker, B.; Oviedo-Trespalacios, O. Young driver risky behaviour and predictors of crash risk in Australia, New Zealand and Colombia: Same but different? Accid. Anal. Prev. 2017, 99, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, Z.; Liu, P.; Wu, Y. Modeling correlation and heterogeneity in crash rates by collision types using full bayesian random parameters multivariate Tobit model. Accid. Anal. Prev. 2019, 128, 164–174. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, Y.; Li, X.; Yu, C.; Kodaka, K.; Li, K. Driving risk assessment using near-crash database through data mining of tree-based model. Accid. Anal. Prev. 2015, 84, 54–64. [Google Scholar] [CrossRef]
- Guo, M.; Li, S.; Wang, L.; Chai, M.; Chen, F.; Wei, Y. Research on the relationship between reaction ability and mental state for online assessment of driving fatigue. Int. J. Environ. Res. Public Health 2016, 13, 1174. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Interval | 30 s | 1 min | 2 min | 3 min | 4 min | 5 min |
|---|---|---|---|---|---|---|
| Sig. F | 0.009 | 0.011 | 0.012 | 0.022 | 0.103 | 0.142 |
| F | 112.6 | 82.2 | 54.7 | 45.3 | 38.9 | 21.8 |
| Statistical Indicators | Upslope Road Segment | Downslope Road Segment | ||
|---|---|---|---|---|
| Blinking-DFD | Blinking-rDFD | Blinking-DFD | Blinking-rDFD | |
| Sum of Squares | 10,447.116 | 4853.339 | 8418.968 | 4607.189 |
| F | 26.402 | 20.018 | 20.477 | 17.206 |
| Sig. F | 0.082 | 0.021 | 0.091 | 0.013 |
| R2 | 0.199 | 0.965 | 0.296 | 0.938 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.; Chen, H.; Zhu, C.-h.; Nan, S.-r.; Li, Y. Estimating Driving Fatigue at a Plateau Area with Frequent and Rapid Altitude Change. Sensors 2019, 19, 4982. https://doi.org/10.3390/s19224982
Wang F, Chen H, Zhu C-h, Nan S-r, Li Y. Estimating Driving Fatigue at a Plateau Area with Frequent and Rapid Altitude Change. Sensors. 2019; 19(22):4982. https://doi.org/10.3390/s19224982
Chicago/Turabian StyleWang, Fan, Hong Chen, Cai-hua Zhu, Si-rui Nan, and Yan Li. 2019. "Estimating Driving Fatigue at a Plateau Area with Frequent and Rapid Altitude Change" Sensors 19, no. 22: 4982. https://doi.org/10.3390/s19224982
APA StyleWang, F., Chen, H., Zhu, C.-h., Nan, S.-r., & Li, Y. (2019). Estimating Driving Fatigue at a Plateau Area with Frequent and Rapid Altitude Change. Sensors, 19(22), 4982. https://doi.org/10.3390/s19224982