Enhancement of Multimodal Microwave-Ultrasound Breast Imaging Using a Deep-Learning Technique


Abstract
1. Introduction
2. CSI-Deep-Learning Microwave Breast Imaging
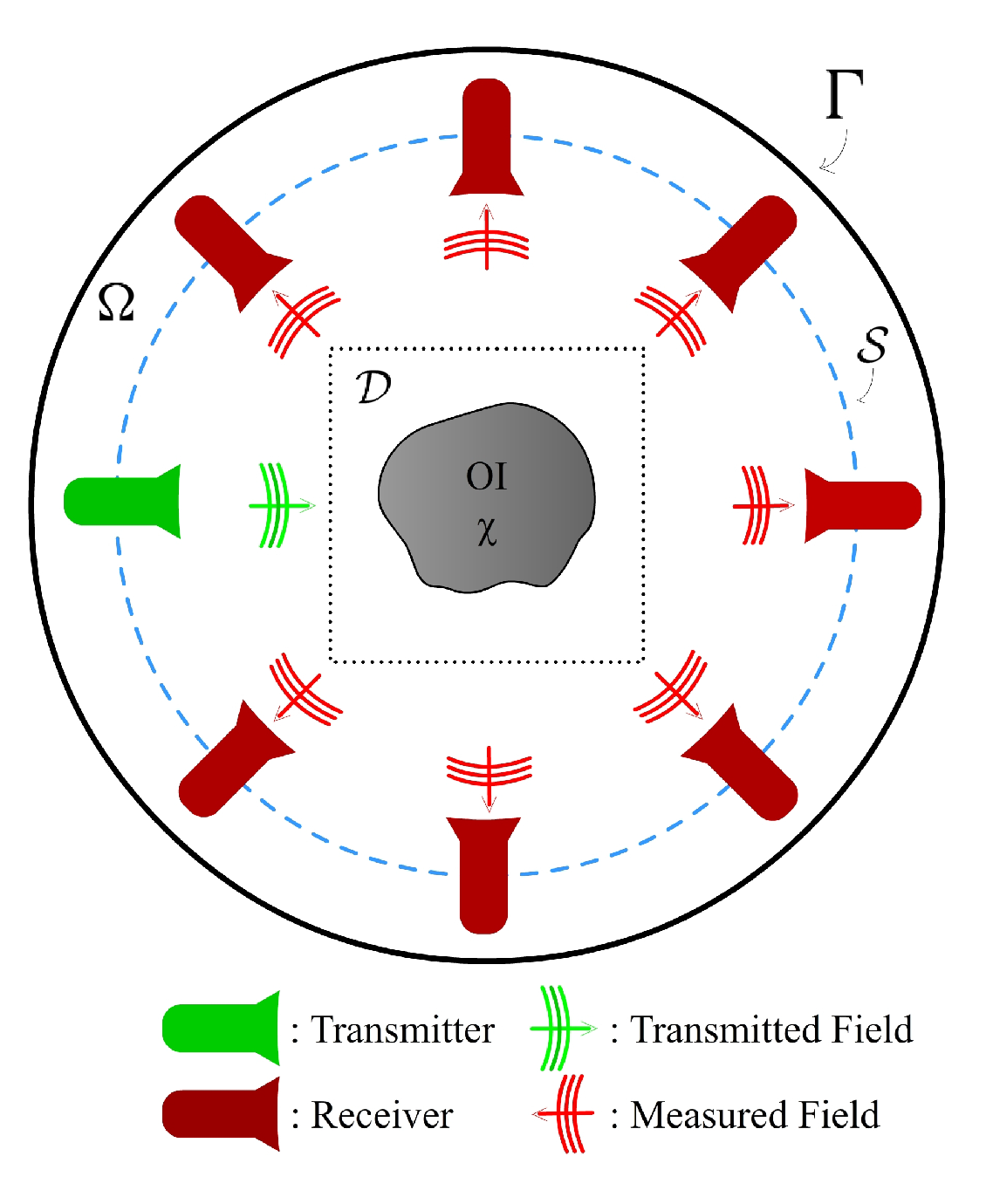
2.1. Contrast Source Inversion
2.2. Machine Learning Approach to Reconstruction
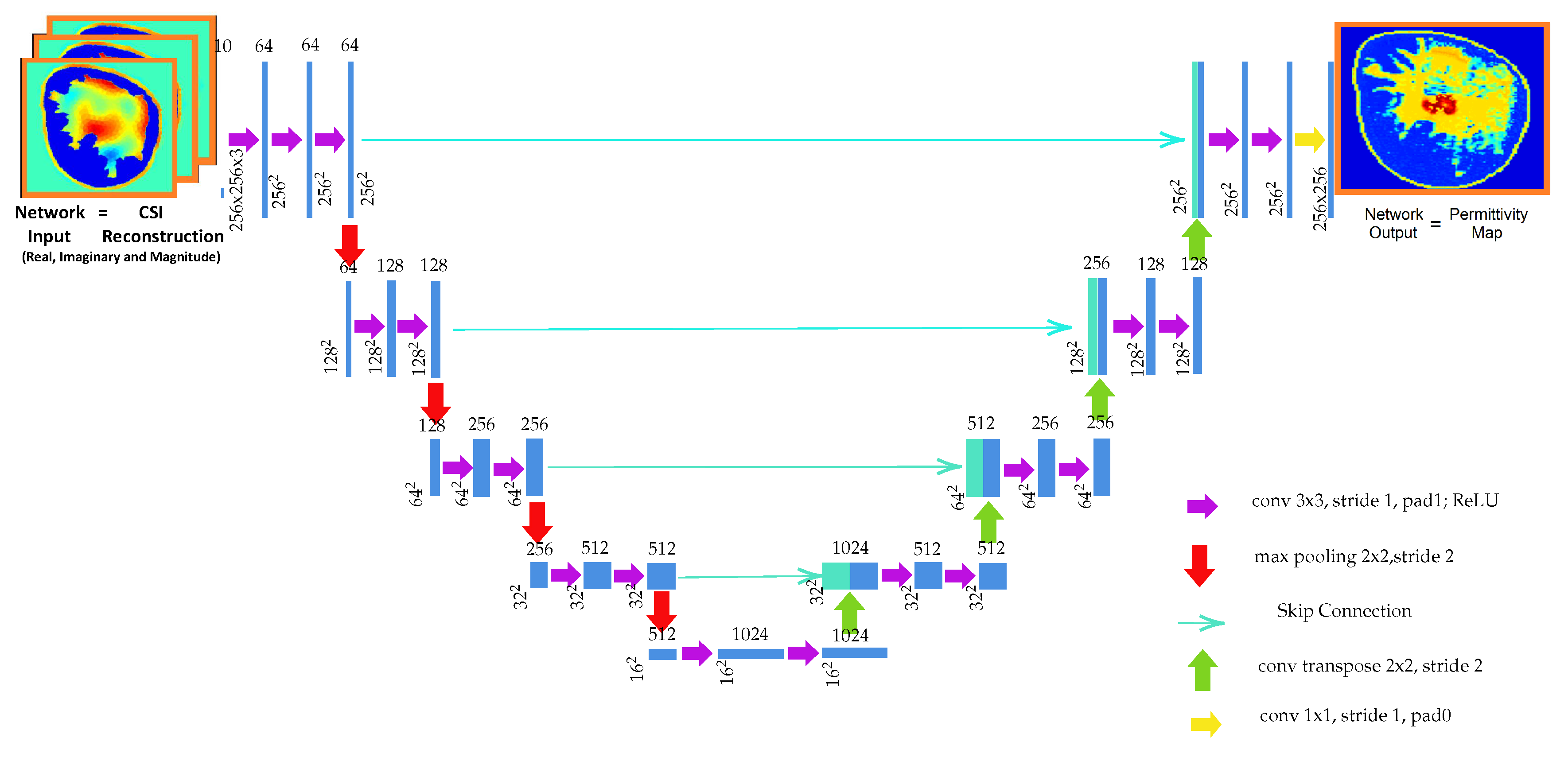
2.3. Choice of Neural Network Architecture
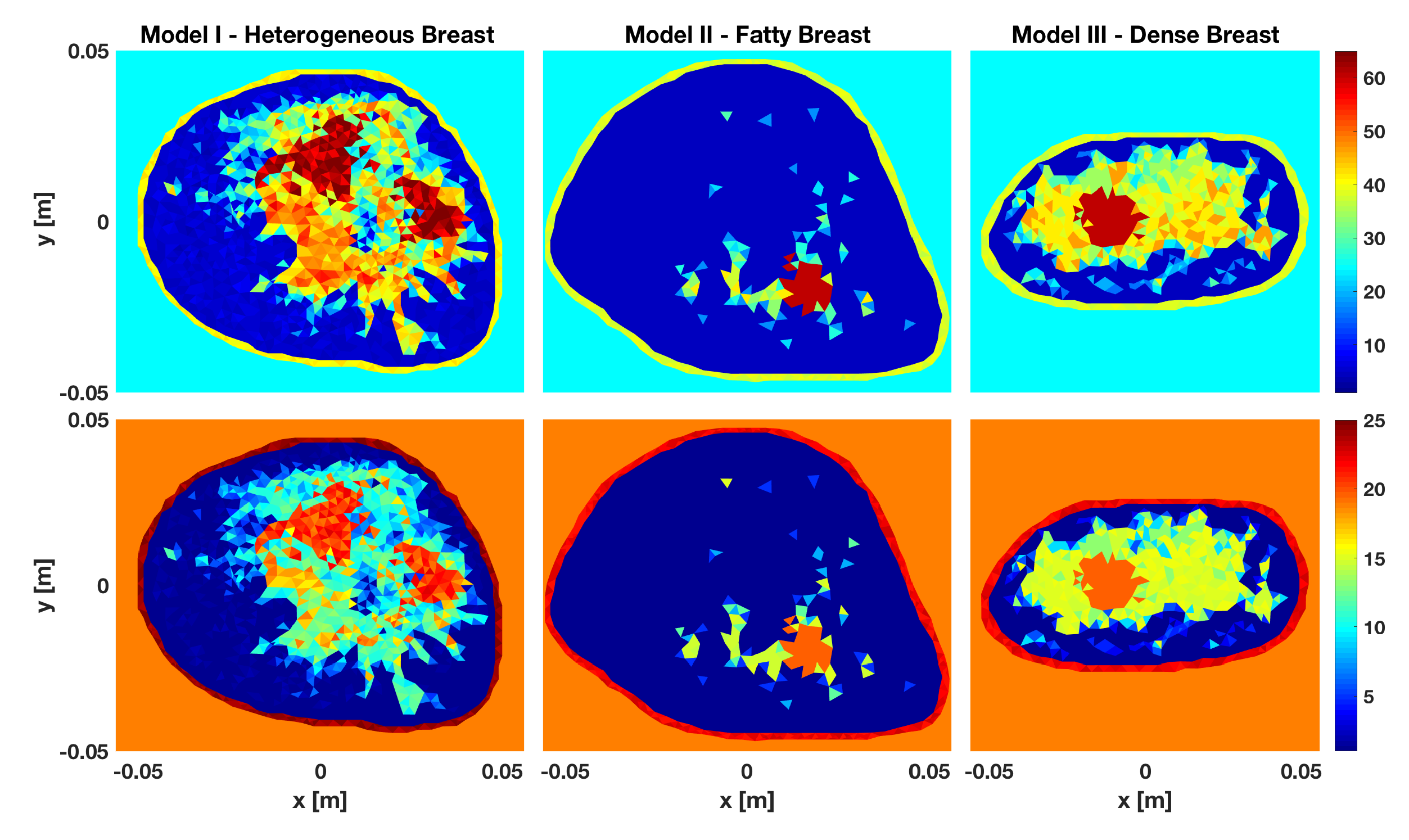
2.4. Datasets
3. Numerical Experiments
3.1. U-Net Training and Quantitative Assessment
- Training Setting: U-Net A: In this setting, training was done using examples from all three breast models. The 1200 images of the dataset were divided into 4 groups consisting of 300 images (100 from each breast model). To implement the four-fold cross-validation, four networks were trained, each using three groups for training (900 images) and tested using the remaining hold-out group (300 images). Thus all 1200 cases featured as test examples when they were not part of the training set.
- Training Setting: U-Net B, U-Net C and U-Net D: In this setting, three different U-Nets where breast examples from one type of breast model was excluded from the training set were trained. In U-Net B examples from breast Model III were excluded, in U-Net C examples from breast Model II were excluded, and in U-Net D examples from breast Model I were excluded from the training set. The training images were taken from the same groupings of the four-fold cross-validation used for U-Net A but now only 600 images from three of the groups were used for training. Testing was performed using images from the hold-out group. In addition testing was performed using all combinations of breast model from the hold-out group. That is, utilizing from either breast Model I, II, III, I & II, I & III, or II & III. The first three combinations consist of only 100 images while the latter three consist of 200 images from the hold-out group. This type of testing was motivated by the fact that each model is significantly different from the rest of the models; excluding them from the training set taxes the neural network when during testing it is presented with reconstructions from the unseen model.
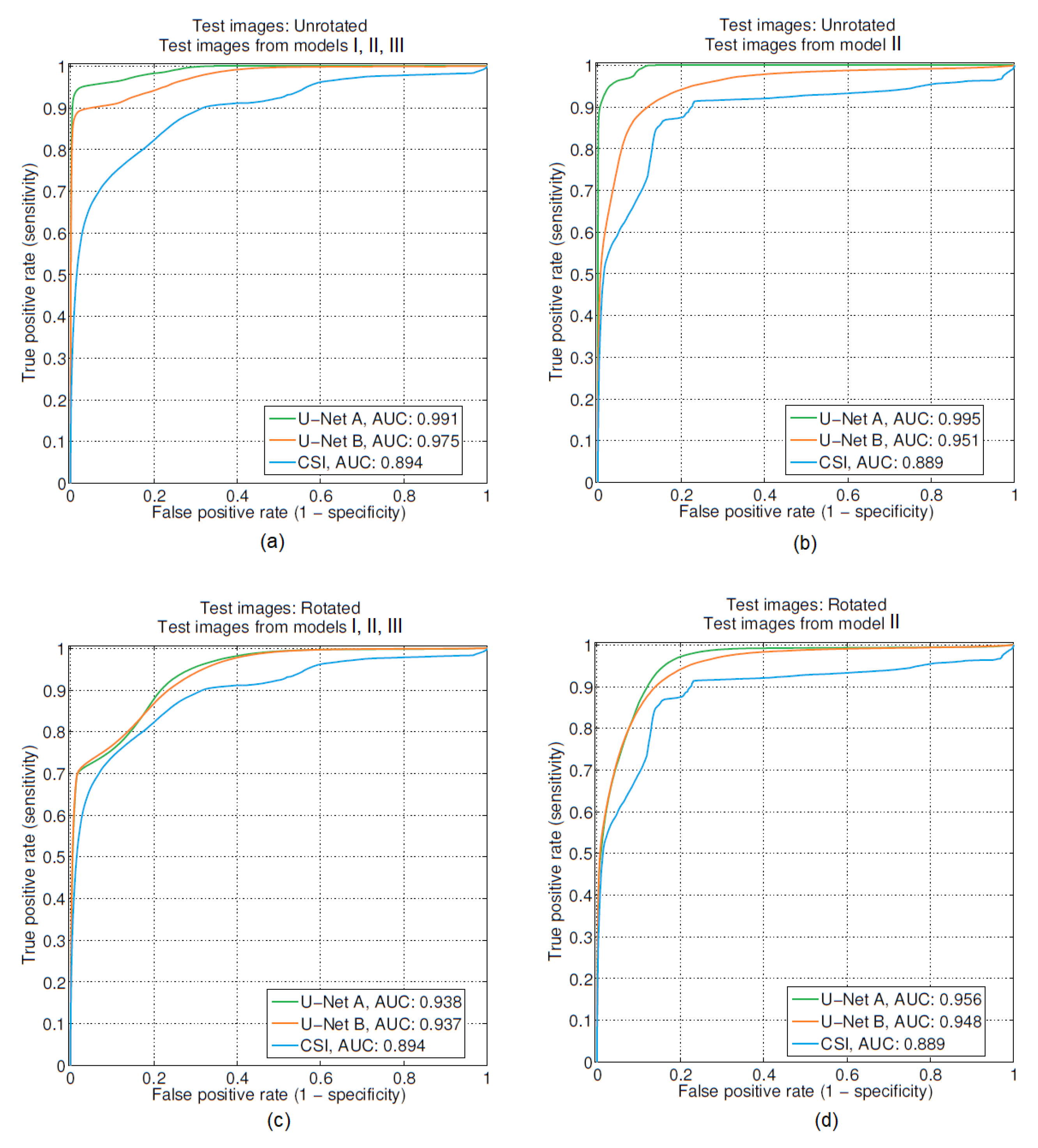
- Performance Metrics: We quantitatively assess both the reconstruction capability and the tumor segmentation performance of the trained U-Nets. To assess the reconstruction quality, we use the Root Mean Squared (RMS) reconstruction error between the network output and the true permittivity values (for both the real and imaginary parts separately). To quantify the tumor segmentation performance, we use the Area Under the Curve (AUC) of the pixel-wise Receiver Operating Characteristics (ROC) using the reconstructed permittivity as a feature. Pixel-wise ROC-AUC is a good performance measure for tumor segmentation since it quantifies the separation between the distribution of permittivities of tumor and non-tumor pixels [28]. For comparison we computed RMS reconstruction error and performed ROC analysis on CSI-only reconstructions. The results of this quantitative evaluation are shown in Table 1 and Table 2.
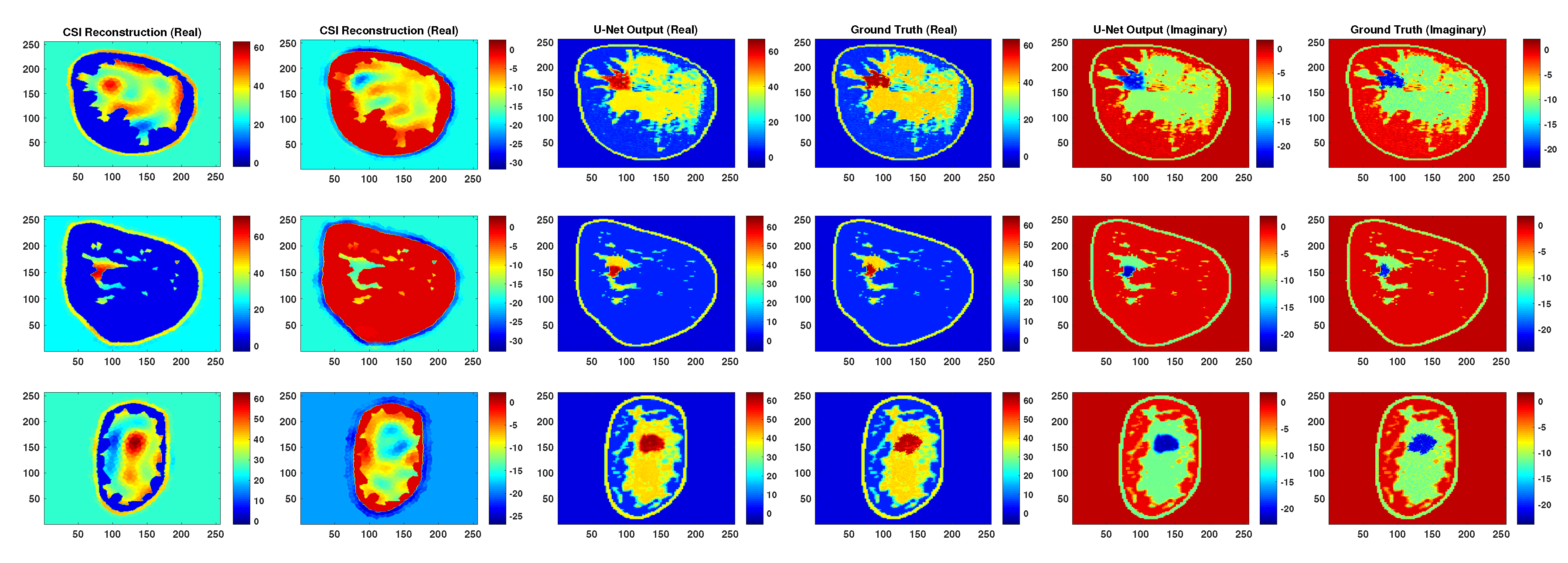
3.2. Qualitative Evaluation of Robustness
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pastorino, M. Microwave Imaging; John Wiley Sons: Hoboken, NJ, USA, 2010; Volume 208. [Google Scholar]
- Haynes, M.; Moghaddam, M. Large-Domain, Low-Contrast Acoustic Inverse Scattering for Ultrasound Breast Imaging. IEEE Trans. Biomed. Eng. 2010, 57, 2712–2722. [Google Scholar] [CrossRef] [PubMed]
- Sak, M.; Duric, N.; Littrup, P.; Sherman, M.; Gierach, G. Ultrasound tomography imaging with waveform sound speed: Parenchymal changes in women undergoing tamoxifen therapy. In Proceedings of the Medical Imaging 2017: Ultrasonic Imaging and Tomography, Orlando, FL, USA, 11–16 February 2017; p. 101390W. [Google Scholar]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093. [Google Scholar] [CrossRef] [PubMed]
- Bolomey, J.C. Crossed Viewpoints on Microwave-Based Imaging for Medical Diagnosis: From Genesis to Earliest Clinical Outcomes. In The World of Applied Electromagnetics: In Appreciation of Magdy Fahmy Iskander; Lakhtakia, A., Furse, C.M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 369–414. [Google Scholar]
- O’Loughlin, D.; O’Halloran, M.J.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave Breast Imaging: Clinical Advances and Remaining Challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar] [CrossRef] [PubMed]
- Halter, R.J.; Zhou, T.; Meaney, P.M.; Hartov, A.; Barth, R.J., Jr.; Rosenkranz, K.M.; Wells, W.A.; Kogel, C.A.; Borsic, A.; Rizzo, E.J.; et al. The correlation of in vivo and ex vivo tissue dielectric properties to validate electromagnetic breast imaging: initial clinical experience. Physiol. Meas. 2009, 30, S121. [Google Scholar] [CrossRef] [PubMed]
- Bevacqua, M.T.; Bellizzi, G.G.; Isernia, T.; Crocco, L. A Method for Effective Permittivity and Conductivity Mapping of Biological Scenarios via Segmented Contrast Source Inversion. Prog. Electromagn. Res. 2019, 164, 1–15. [Google Scholar] [CrossRef]
- Omer, M.; Mojabi, P.; Kurrant, D.; LoVetri, J.; Fear, E. Proof-of-Concept of the Incorporation of Ultrasound-Derived Structural Information Into Microwave Radar Imaging. IEEE J. Multiscale Multiphys. Comput. Tech. 2018, 3, 129–139. [Google Scholar] [CrossRef]
- Abdollahi, N.; Kurrant, D.; Mojabi, P.; Omer, M.; Fear, E.; LoVetri, J. Incorporation of Ultrasonic Prior Information for Improving Quantitative Microwave Imaging of Breast. IEEE J. Multiscale Multiphys. Comput. Tech. 2019, 4, 98–110. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; Available online: http://www.deeplearningbook.org. (accessed on 18 September 2019).
- Wei, Z.; Chen, X. Deep-Learning Schemes for Full-Wave Nonlinear Inverse Scattering Problems. IEEE Trans. Geosci. Remote Sens. 2019, 57, 1849–1860. [Google Scholar] [CrossRef]
- McCann, M.T.; Jin, K.H.; Unser, M. Convolutional Neural Networks for Inverse Problems in Imaging: A Review. IEEE Signal Process. Mag. 2017, 34, 85–95. [Google Scholar] [CrossRef]
- Gerazov, B.; Conceicao, R.C. Deep learning for tumour classification in homogeneous breast tissue in medical microwave imaging. In Proceedings of the IEEE EUROCON 2017-17th International Conference on Smart Technologies, Ohrid, Macedonia, 6–8 July 2017; pp. 564–569. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the 18th Medical Image Computing and Computer-Assisted Intervention (MICCAI 2015), Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Jin, K.H.; McCann, M.T.; Froustey, E.; Unser, M. Deep Convolutional Neural Network for Inverse Problems in Imaging. arXiv 2016, arXiv:1611.03679. [Google Scholar] [CrossRef]
- Jin, K.H.; McCann, M.T.; Froustey, E.; Unser, M. Deep Convolutional Neural Network for Inverse Problems in Imaging. IEEE Trans. Image Process. 2017, 26, 4509–4522. [Google Scholar] [CrossRef] [PubMed]
- Rahama, Y.A.; Aryani, O.A.; Din, U.A.; Awar, M.A.; Zakaria, A.; Qaddoumi, N. Novel Microwave Tomography System Using a Phased-Array Antenna. IEEE Trans. Microw. Theory Tech. 2018, 66, 5119–5128. [Google Scholar] [CrossRef]
- Rekanos, I.T. Neural-network-based inverse-scattering technique for online microwave medical imaging. IEEE Trans. Magn. 2002, 38, 1061–1064. [Google Scholar] [CrossRef]
- Li, L.; Wang, L.G.; Teixeira, F.L.; Liu, C.; Nehorai, A.; Cui, T.J. DeepNIS: Deep Neural Network for Nonlinear Electromagnetic Inverse Scattering. IEEE Trans. Antennas Propag. 2019, 67, 1819–1825. [Google Scholar] [CrossRef]
- Van den Berg, P.M.; Kleinman, R.E. A contrast source inversion method. Inverse Probl. 1997, 13, 1607. [Google Scholar] [CrossRef]
- Zakaria, A.; Gilmore, C.; LoVetri, J. Finite-element contrast source inversion method for microwave imaging. Inverse Probl. 2010, 26, 115010. [Google Scholar] [CrossRef]
- Kurrant, D.; Baran, A.; LoVetri, J.; Fear, E. Integrating prior information into microwave tomography Part 1: Impact of detail on image quality. Med. Phys. 2017, 44, 6461–6481. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.; Kurrant, D.; Fear, E.; LoVetri, J. Integrating prior information into microwave tomography part 2: Impact of errors in prior information on microwave tomography image quality. Med. Phys. 2017, 44, 6482–6503. [Google Scholar]
- Omer, M.; Fear, E.C. Automated 3D method for the construction of flexible and reconfigurable numerical breast models from MRI scans. Med. Biol. Eng. Comput. 2018, 56, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, C.; Bilaniuk, O.; Zhang, Y.; Serdyuk, D.; Subramanian, S.; Santos, J.F.; Mehri, S.; Rostamzadeh, N.; Bengio, Y.; Pal, C. Deep Complex Networks. arXiv 2018, arXiv:1705.09792. [Google Scholar]
- Glorot, X.; Bengio, Y. Understanding the difficulty of training deep feedforward neural networks. In Proceedings of the 13th International Conference on Artificial Intelligence and Statistics, Sardinia, Italy, 13–15 May 2010; pp. 249–256. [Google Scholar]
- Bishop, C.M. Pattern Recognition and Machine Learning; Springer: Berlin, Germany, 2006. [Google Scholar]
- Asefi, M.; Baran, A.; LoVetri, J. An experimental phantom study for air-based quasi-resonant microwave breast imaging. IEEE Trans. Microw. Theory Tech. 2019, 67, 3946–3954. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models Included in the Training Set | Reconstruction Technique | Breast Models Included in the Test Set | ||||||
|---|---|---|---|---|---|---|---|---|
| I, II, III | I | II | III | I, II | I, III | II, III | ||
| N/A | CSI | 2.199 | 2.214 | 1.931 | 2.423 | 2.077 | 2.321 | 2.191 |
| 0.897 | 0.868 | 0.892 | 0.897 | 0.890 | 0.882 | 0.915 | ||
| I, II, III | U-Net A | 0.122 | 0.144 | 0.075 | 0.135 | 0.114 | 0.140 | 0.110 |
| 0.987 | 0.980 | 0.994 | 0.984 | 0.987 | 0.982 | 0.991 | ||
| I, II | U-Net B | 1.329 | 0.257 | 1.158 | 1.973 | 0.839 | 1.407 | 1.618 |
| 0.596 | 0.908 | 0.653 | 0.442 | 0.871 | 0.593 | 0.387 | ||
| I, III | U-Net C | 0.694 | 0.253 | 1.151 | 0.232 | 0.834 | 0.243 | 0.830 |
| 0.922 | 0.886 | 0.937 | 0.919 | 0.917 | 0.903 | 0.942 | ||
| II, III | U-Net D | 1.297 | 1.947 | 1.098 | 0.231 | 1.580 | 1.386 | 0.794 |
| 0.758 | 0.587 | 0.730 | 0.929 | 0.631 | 0.740 | 0.904 | ||
| N/A | CSI | 7.103 | 6.894 | 6.548 | 7.806 | 6.723 | 7.364 | 7.205 |
| 0.757 | 0.717 | 0.799 | 0.713 | 0.762 | 0.721 | 0.781 | ||
| I, II, III | U-Net A | 0.307 | 0.352 | 0.205 | 0.342 | 0.288 | 0.347 | 0.282 |
| 0.987 | 0.981 | 0.992 | 0.985 | 0.987 | 0.983 | 0.990 | ||
| I, II | U-Net B | 1.884 | 0.594 | 1.572 | 2.797 | 1.188 | 2.022 | 2.268 |
| 0.654 | 0.889 | 0.907 | 0.529 | 0.906 | 0.649 | 0.465 | ||
| I, III | U-Net C | 1.034 | 0.547 | 1.609 | 0.561 | 1.202 | 0.554 | 1.205 |
| 0.913 | 0.888 | 0.937 | 0.895 | 0.912 | 0.894 | 0.929 | ||
| II, III | U-Net D | 1.843 | 2.754 | 1.512 | 0.567 | 2.221 | 1.989 | 1.142 |
| 0.694 | 0.501 | 0.810 | 0.916 | 0.536 | 0.671 | 0.909 | ||
| Models Included in the Training Set | Reconstruction Technique | Breast Models Included in the Test Set | ||||||
|---|---|---|---|---|---|---|---|---|
| I, II, III | I | II | III | I, II | I, III | II, III | ||
| N/A | CSI | 2.199 | 2.214 | 1.931 | 2.423 | 2.077 | 2.321 | 2.191 |
| 0.897 | 0.868 | 0.892 | 0.897 | 0.890 | 0.882 | 0.915 | ||
| I, II, III | U-Net A | 0.126 | 0.149 | 0.078 | 0.140 | 0.119 | 0.145 | 0.114 |
| 0.988 | 0.982 | 0.993 | 0.985 | 0.988 | 0.983 | 0.991 | ||
| I, II | U-Net B | 1.310 | 0.268 | 1.087 | 1.973 | 0.792 | 1.408 | 1.593 |
| 0.623 | 0.892 | 0.944 | 0.515 | 0.912 | 0.612 | 0.434 | ||
| I, III | U-Net C | 0.678 | 0.241 | 1.125 | 0.236 | 0.813 | 0.238 | 0.813 |
| 0.921 | 0.894 | 0.949 | 0.917 | 0.917 | 0.905 | 0.938 | ||
| II, III | U-Net D | 1.285 | 1.941 | 1.061 | 0.242 | 1.565 | 1.383 | 0.770 |
| 0.753 | 0.581 | 0.841 | 0.924 | 0.620 | 0.734 | 0.918 | ||
| N/A | CSI | 7.103 | 6.894 | 6.548 | 7.806 | 6.723 | 7.364 | 7.205 |
| 0.757 | 0.717 | 0.799 | 0.713 | 0.762 | 0.721 | 0.781 | ||
| I, II, III | U-Net A | 0.313 | 0.361 | 0.206 | 0.349 | 0.294 | 0.355 | 0.286 |
| 0.989 | 0.985 | 0.992 | 0.987 | 0.989 | 0.987 | 0.991 | ||
| I, II | U-Net B | 1.899 | 0.599 | 1.607 | 2.807 | 1.213 | 2.030 | 2.287 |
| 0.670 | 0.896 | 0.938 | 0.516 | 0.913 | 0.643 | 0.516 | ||
| I, III | U-Net C | 1.044 | 0.561 | 1.630 | 0.546 | 1.219 | 0.553 | 1.215 |
| 0.918 | 0.889 | 0.943 | 0.910 | 0.914 | 0.901 | 0.935 | ||
| II, III | U-Net D | 1.851 | 2.751 | 1.547 | 0.558 | 2.232 | 1.985 | 1.163 |
| 0.728 | 0.566 | 0.819 | 0.951 | 0.600 | 0.703 | 0.920 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoshdel, V.; Ashraf, A.; LoVetri, J. Enhancement of Multimodal Microwave-Ultrasound Breast Imaging Using a Deep-Learning Technique. Sensors 2019, 19, 4050. https://doi.org/10.3390/s19184050
Khoshdel V, Ashraf A, LoVetri J. Enhancement of Multimodal Microwave-Ultrasound Breast Imaging Using a Deep-Learning Technique. Sensors. 2019; 19(18):4050. https://doi.org/10.3390/s19184050
Chicago/Turabian StyleKhoshdel, Vahab, Ahmed Ashraf, and Joe LoVetri. 2019. "Enhancement of Multimodal Microwave-Ultrasound Breast Imaging Using a Deep-Learning Technique" Sensors 19, no. 18: 4050. https://doi.org/10.3390/s19184050
APA StyleKhoshdel, V., Ashraf, A., & LoVetri, J. (2019). Enhancement of Multimodal Microwave-Ultrasound Breast Imaging Using a Deep-Learning Technique. Sensors, 19(18), 4050. https://doi.org/10.3390/s19184050