Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses

 ,
,
Abstract
1. Introduction
2. Proposed Method
2.1. Patient Transfer skill and Checklist
2.2. Patient’s Movements Related to Transfer Skill
2.3. Measured Parameters
2.4. Sensors
2.4.1. Determination of Sensor
2.4.2. Installation on Patient
3. Experiment
3.1. Purpose
- Confirm whether the translational acceleration, rotational speed, and joint angle of the patient can reveal the different influences on the patient’s movement while the nurse performs the correct and incorrect ways of assisting the patient.
- Determine the parameter and the location, which exhibits the most obvious difference on the patient between the correct and incorrect methods.
- Ensure the applicability of the inertial sensors to measure the translational acceleration and rotational speed.
3.2. Participants
3.3. Procedures
3.4. Experimental Setting
3.5. Results
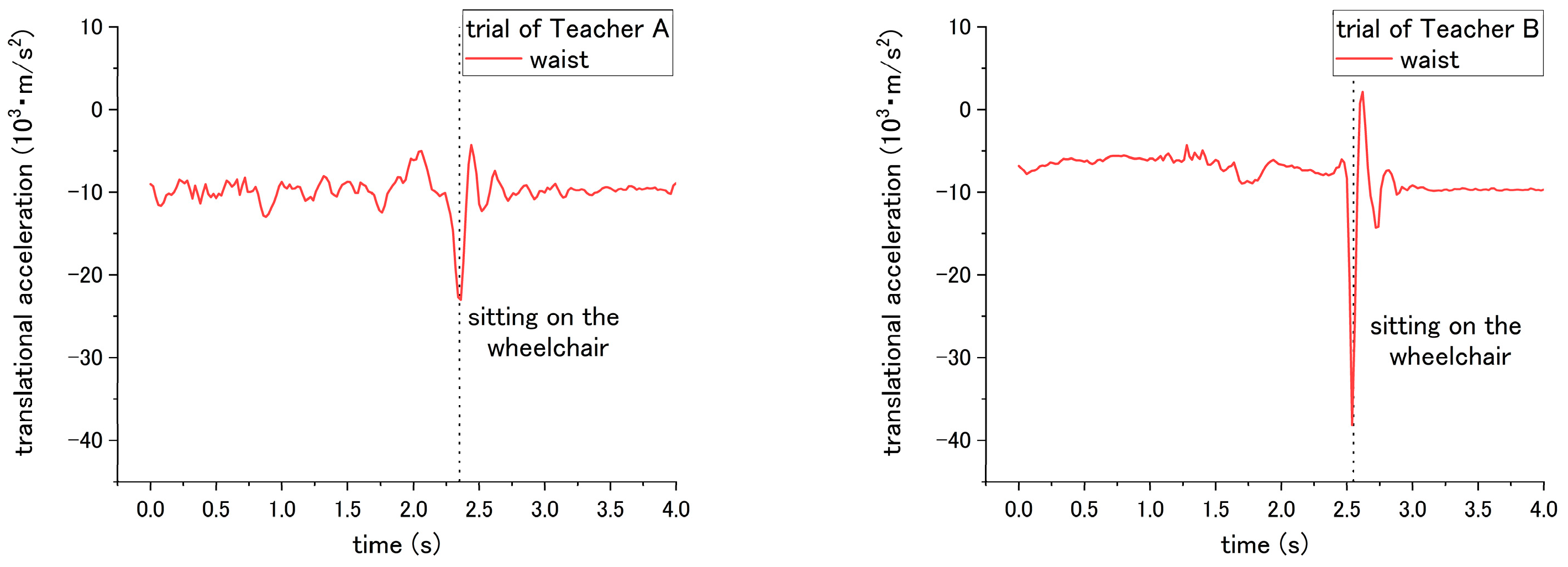
3.5.1. Translational Acceleration
3.5.2. Rotational Speed
3.5.3. Joint Angle
4. Discussion
4.1. Translational Acceleration
4.2. Rotational Speed
4.3. Joint Angle
5. Conclusions and Future Work
- The translation acceleration can be used to reveal the differences in the patient’s kinematic movement (i.e., fast or slow) between the correct and incorrect executions in step nos. 3, 14, and 15. The difference in step No. 10 is difficult to exhibit.
- The rotational speed enables showing the influence on the patient in step nos. 1, 5, and 9, which are related to shifting the patient’s bottom and pivot turning. In step No. 7, the expected difference between the correct/incorrected methods is not obtained.
- The joint angle shows a significant difference in the patient in most steps, partially for the steps of standing up and sitting down. A significant difference is also observed between different nurses.
- The differences between the patient’s and the nurse’s height would influence the joint angle. The differences in the patient’s weight would affect the translation acceleration. However, consistent results are still obtained from different nurses under the incorrect methods.
- The threshold of each parameter should be determined considering the individual differences of the nurse’s and the simulated patient’s weight and height.
- The applicability of inertial sensors was verified for use in the robot’s development.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McNeese-Smith, D.K.; Nazarey, M. A nursing shortage: Building organizational commitment among nurses/practitioner application. J. Healthc. Manag. 2001, 46, 173–186. [Google Scholar] [CrossRef] [PubMed]
- American Association of Colleges of Nursing (AACN) Homepage. Available online: http://www.aacnnursing.org/News-Information/Fact-Sheets/Nursing-Faculty-Shortage (accessed on 20 June 2018).
- Nardi, D.A.; Gyurko, C.C. The global nursing faculty shortage: Status and solutions for change. J. Nurs. Scholarsh. 2013, 45, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, A.S. A continuing challenge: The shortage of educationally prepared nursing faculty. Online J. Issues Nurs. 2001, 6, 3. [Google Scholar] [PubMed]
- Burruss, N.M.; Billings, D.M.; Brownrigg, V.; Skiba, D.J.; Connors, H.R. Class size as related to the use of technology, educational practices, and outcomes in web-based nursing courses. J. Prof. Nurs. 2009, 25, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, G.; Lisa, L.; Jenny, S. The effects of class size and form of assessment on nursing students’ performance, approaches to study and course perceptions. Nurs. Educ. Today 1997, 17, 311–318. [Google Scholar] [CrossRef]
- Goldstein, I.L.; Ford, J.K. Training in Organizations: Needs Assessment, Development, and Evaluation, 4th ed.; Wadsworth/Thomson Learning: Belmont, CA, US, 2002. [Google Scholar]
- Juwah, C.; Macfarlane-Dick, D.; Matthew, B.; Nicol, D.; Ross, D.; Smith, B. Enhancing Student Learning through Effective Formative Feedback; The Higher Education Academy: York, UK, 2004. [Google Scholar]
- Dornan, T.; Littlewood, S.; Margolis, S.A.; Scherpbier, A.J.J.A.; Spencer, J.; Ypinazar, V. How can experience in clinical and community settings contribute to early medical education? A BEME systematic review. Med. Teach. 2016, 28, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Benner, P. From novice to expert. Am. J. Nurs. 1982, 82, 402–407. [Google Scholar] [PubMed]
- Field, D.E. Moving from novice to expert—The value of learning in clinical practice: A literature review. Nurs. Educ. Today 2004, 24, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Nagata, A.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Aida, K.; Kuwahara, N.; Ogata, T.; Ota, J. Self-Help Training System for Nursing Students to Learn Patient Transfer Skills. IEEE Trans. Learn. Technol. 2014, 7, 319–332. [Google Scholar] [CrossRef]
- Huang, Z.; Lin, C.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ogata, T.; Ota, J. Robot Patient Design to Simulate Various Patients for Transfer Training. IEEE/ASME Trans. Mech. 2017, 22, 2079–2090. [Google Scholar] [CrossRef]
- Chan, J.C.; Leung, H.; Tang, J.K.; Komura, T. A virtual reality dance training system using motion capture technology. IEEE Trans. Learn. Technol. 2011, 4, 187–195. [Google Scholar] [CrossRef]
- Chakravorti, N.; Le Sage, T.; Slawson, S.E.; Conway, P.P.; West, A.A. Design and implementation of an integrated performance monitoring tool for swimming to extract stroke information at real time. IEEE Trans. Hum.-Mach. Syst. 2013, 43, 199–213. [Google Scholar] [CrossRef]
- Paradisis, G.; Rees, J. Kinematic analysis of golf putting for expert and novice golfers. ISBS-Conf. Proc. Arch. 2000, 1. [Google Scholar]
- Ryan, B.; Venkatesan, S. A framework for golf training using low-cost inertial sensors. In Proceedings of the 2010 IEEE International Conference on Body Sensor Networks (BSN), Singapore, 7–9 June 2010. [Google Scholar]
- Gray, S.; Watts, S.; Debicki, D.; Hore, J. Comparison of kinematics in skilled and unskilled arms of the same recreational baseball players. J. Sports Sci. 2006, 24, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Furuya, S.; Kinoshita, H. Organization of the upper limb movement for piano key-depression differs between expert pianists and novice players. Exp. Brain Res. 2008, 185, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Konvalinka, I.; Xygalatas, D.; Bulbulia, J.; Schjødt, U.; Jegindø, E.M.; Wallot, S.; Van Orden, G.; Roepstorff, A. Synchronized arousal between performers and related spectators in a fire-walking ritual. Proc. Natl. Acad. Sci. USA 2011, 108, 8514–8519. [Google Scholar] [CrossRef] [PubMed]
- Evrard, P.; Gribovskaya, E.; Calinon, S.; Billard, A.; Kheddar, A. Teaching physical collaborative tasks: Object-lifting case study with a humanoid. In Proceedings of the 2009 9th IEEE-RAS International Conference on Humanoid Robots, Paris, France, 7–10 December 2009. [Google Scholar]
- Tang, J.K.; Chan, J.C.; Leung, H. Interactive dancing game with real-time recognition of continuous dance moves from 3D human motion capture. In Proceedings of the 5th International Conference on Ubiquitous Information Management and Communication, Seoul, Korea, 21–23 February 2011. [Google Scholar]
- Tonietti, G.; Schiavi, R.; Bicchi, A. Design and control of a variable stiffness actuator for safe and fast physical human/robot interaction. In Proceedings of the 2005 IEEE International Conference on Robotics and Automation, Barcelona, Spain, 18–22 April 2005; pp. 526–531. [Google Scholar]
- Johansson, P.; Oleni, M.; Fridlund, B. Patient satisfaction with nursing care in the context of health care: A literature study. Scand. J. Care Sci. 2002, 16, 337–344. [Google Scholar] [CrossRef]
- McGilton, K.; Robinson, H.I.; Boscart, V.; Spanjevic, L. Communication enhancement: Nurse and patient satisfaction outcomes in a complex continuing care facility. J. Adv. Nurs. 2006, 54, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Kjellberg, K.; Lagerstr€om, M.; Hagberg, M. Patient safety and comfort during transfers in relation to nurses’ work technique. J. Adv. Nurs. 2004, 47, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Waldner, M.H.; Olson, J.K. Taking the patient to the classroom: Applying theoretical frameworks to simulation in nursing education. Int. J. Nurs. Educ. Scholarsh. 2007, 4. [Google Scholar] [CrossRef] [PubMed]
- Gerling, G.J; Rigsbee, S.; Childress, R.M.; Martin, M.L. The design and evaluation of a computerized and physical simulator for training clinical prostate exams. IEEE Trans. Syst. Man Cybern. 2009, 39, 388–403. [Google Scholar] [CrossRef]
- Takhashi, Y.; Komeda, T.; Koyama, H.; Yamamoto, S.I.; Arimatsu, T.; Kawakami, Y.; Inoue, K.; Ito, Y. Development of an upper limb patient simulator for physical therapy exercise. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–4. [Google Scholar]
- Morita, Y.; Kawai, Y.; Hayashi, Y.; Hirano, T.; Ukai, H.; Sanaka, K.; Nakamuta, H.; Takao, K. Development of knee joint robot for students becoming therapist—Design of prototype and fundamental experiments. In Proceedings of the 2010 IEEE International Conference on Control Automation and Systems (ICCAS), Gyeonggi-do, Korea, 27–30 October 2010; pp. 151–155. [Google Scholar]
- Kitagawa, Y.; Ishikura, T.; Song, W.; Mae, Y.; Minami, M.; Tanaka, K. Human-like patient robot with chaotic emotion for injection training. In Proceedings of the 2009 IEEE ICCAS-SICE, Fukuoka, Japan, 18–21 August 2009; pp. 4635–4640. [Google Scholar]
- Ogata, T.; Nagata, A.; Huang, Z.; Katayama, T.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Aida, K.; Kuwahara, N.; et al. Mannequin system for the self-training of nurses in the changing of clothes. Kybernetes 2016, 45, 839–852. [Google Scholar] [CrossRef]
- Takanobu, H.; Omata, A.; Takahashi, F.; Yokota, K.; Suzuki, K.; Miura, H.; Madokoro, M.; Miyazaki, Y.; Maki, K. Dental patient robot as a mechanical human simulator. In Proceedings of the 2007 IEEE International Conference on Mechatronics, Changchun, China, 8–10 May 2007; pp. 1–6. [Google Scholar]
- Foxlin, E. Pedestrian tracking with shoe-mounted inertial sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Roetenberg, D.; Luinge, H.J.; Baten, C.T.; Veltink, P.H. Compensation of magnetic disturbances improves inertial and magnetic sensing of human body segment orientation. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Christopher, J. Precision free-inertial navigation with gravity compensation by an onboard gradiometer. J. Guid. Control Dyn. 2006, 29, 704–713. [Google Scholar] [CrossRef]
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step of Transfer Skill | Correct Method | Incorrect Method | Influence on Patient Occurs in Step(s) | Parameter Type | Data Location | Different Influences on the Patient under Correct/Incorrect Methods |
|---|---|---|---|---|---|---|
| No. 1 | Place the wheelchair at the bedside and adjust the angle to 20–30° | Place the wheelchair at the bedside at a very large angle | No. 12 | Rotational speed | Waist | The rotational angle computed by the rotational speed becomes larger when the incorrect method is applied during No. 12 |
| No. 2 | Place the wheelchair near the bed | Place the wheelchair very far from the bed | No. 12 | Joint angle | Hip | The total variation of the joint angle increases while moving the patient from the bed to the wheelchair when the incorrect method is applied in No. 12 |
| No. 3 | Apply the wheelchair brakes | Do not apply the brakes | No. 15 | Translational acceleration | Chest | Under the correct method, backward acceleration forms a peak with sudden increasing/decreasing caused by stopping of the wheelchair in No. 15 |
| No. 4 | Place one of your feet behind you and another foot between the feet of the patient | — | — | — | — | — |
| No. 5 | Enable the patient to sit on the edge of the bed by shifting the patient’s bottom | 5-(1) Move the patient to the edge, but not by shifting the patient’s bottom | No. 5 | Rotational speed | Waist | Repeated variation in the rotational speed between the clockwise and counterclockwise directions when the correct method is applied in No. 5 |
| 5-(2) Do not move the patient to the edge of the bed | No. 11 | Joint angle | Hip | The joint angle obviously increases while starting to stand up when this step is not executed in No. 11 | ||
| No. 6 | Adjust the patient’s leg posture and move the patient’s ankle closer to the bed | Move the patient’s ankle far from the bed | No. 6 | Joint angle | Knee | The joint angle decreases when the ankle is placed very far from the bed in No. 6 |
| No. 11 | Hip | The joint angle increases at the beginning of standing up when the ankle is placed very far from the bed in No. 11 | ||||
| No. 7 | Place both arms of the patient on your shoulders and hug | Do not place both arms of the patient on your shoulders | No. 7 | Joint angle | Shoulder | The adduction angle decreases when the nurse raises the patient’s arm and hugs the patient in No. 7 under the correct method |
| No. 12 | Rotational speed | Chest | Non-consistent results of teachers A and B are found during the pivot turning in No. 12 | |||
| No. 8 | Clutch the lower back of the patient. | — | — | — | — | — |
| No. 9 | Place your right foot behind you and the left foot between the feet of the patient | Place your feet in the wrong position: left foot behind and right foot between the feet of the patient | No. 12 | Rotational speed | Chest | The rotational speed increases when the incorrect method is applied in No. 12 |
| No. 10 | Squat down and lower your waist to prepare the patient to stand up | Do not bend your knees and lower your waist | No. 11 | Translational acceleration | Waist | The upward translational acceleration increases during standing up when the incorrect method is applied in No. 11 |
| No. 11 | Make the patient lean forward, then assist the patient to stand up | Do not make the patient lean forward first; make them stand up vertically | No. 11 | Joint angle | Hip | The joint angle increases at the beginning of the standing movement when the correct method is applied in No. 11, but Teacher A’s trial did not obtain such a result on the hip angle |
| Knee | ||||||
| No. 12 | Use your left foot as a pivot axis to help the patient turn to the wheelchair | — | — | — | — | — |
| No. 13 | Place one of your feet behind you and another foot between the feet of the patient | — | — | — | — | — |
| No. 14 | Lower your waist to prepare assisting the patient to sit down | Do not lower the waist and bend the knee to assist the patient to sit down | No. 15 | Translational acceleration | Waist | The downward translational acceleration increases when the nurses do not lower their waist in No. 15 |
| No. 15 | Make the patient lean forward and assist the patient to sit | Do not make the patient lean forward first before making them sit down | No. 15 | Joint angle | Hip | The joint angle of the hip increases, then decreases when the correct method is applied in No. 15 |
| Translational acceleration | Waist | The downward translational acceleration increases when the incorrect method is applied in No. 15 | ||||
| No. 16 | Make the patient sit in the wheelchair by pulling with both arms | Lift the patient up vertically and make the patient sit in the wheelchair | No. 16 | Joint angle | Hip | The joint angle decreases at first when the incorrect method is applied and increases when the correct method is applied in No. 16 |
| Step | Influence on Step | Value (Unit) | Correct Way | Incorrect Way | ||
|---|---|---|---|---|---|---|
| Teacher A | Teacher B | Teacher A | Teacher B | |||
| No. 3 | No. 15 | peak-to-valley (103 m/s2) | 2.35 | 9.54 | 1.10 | 8.53 |
| No. 10 | No. 11 | ┬ peak-to-valley (103 m/s2) | 3.33 | 1.93 | 4.62 | 0.69 |
| No. 14 | No. 15 | peak-to-valley (103 m/s2) | 3.13 | 26.93 | 18.65 | 47.78 |
| No. 15 | No. 15 | peak-to-valley (103 m/s2) | 3.13 | 26.93 | 24.01 | 40.28 |
| Step | Influence on Step | Value (Unit) | Correct Way | Incorrect Way | ||
|---|---|---|---|---|---|---|
| Teacher A | Teacher B | Teacher A | Teacher B | |||
| No. 1 | No. 12 | * Total angle variation (°) | 100.4 | 96.1 | 144.1 | 146.6 |
| No. 5 | No. 5 | * Total angle variation (°) | 105.2 | 108.6 | No. 5-(1) 56.1 | No. 5-(1) 52.8 |
| No. 7 | No. 12 | ┬ MAX-to-MIN (rad/s) | 2.47 | 1.36 | 2.38 | 1.57 |
| No. 9 | No. 12 | MAX-to-MIN (rad/s) | 2.47 | 1.36 | 3.40 | 2.60 |
| Step | Influence on Step | Value (Unit) | Correct Way | Incorrect Way | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Teacher A | Teacher B | Teacher A | Teacher B | |||||||
| R | L | R | L | R | L | R | L | |||
| No. 2 | No. 12 | * Total angle displacement (°) | 102.3 | 55.2 | 95.2 | 73.9 | 146.7 | 156.3 | 298.2 | 156.1 |
| No. 5 | No. 11 | *▲ Hip peak angle (°) | 66.6 | 66.0 | 41.1 | 51.3 | No. 5-(2) | |||
| 91.4 | 89.0 | 85.1 | 82.9 | |||||||
| * Hip int. to peak angle (°) | 6.2 | 5.5 | 2.5 | 4.1 | No. 5-(2) | |||||
| 10.8 | 10.5 | 21.0 | 15.3 | |||||||
| No. 6 | No. 6 | * Knee int. Angle (°) | 95.6 | 93.3 | 95.5 | 87.2 | 43.1 | 38.9 | 52.1 | 53.9 |
| No. 11 | *▲ Knee peak angle (°) | 97.8 | 98.3 | 99.4 | 97.2 | 56.9 | 54.4 | 73.3 | 75.2 | |
| *▲ Knee int. to peak angle (°) | 2.6 | 4.9 | 3.8 | 9.8 | 13.8 | 15.6 | 21.2 | 21.3 | ||
| No. 11 | No. 11 | * Hip int. to peak angle (°) | 6.2 | 5.5 | 3.5 | 4.1 | 0.8 | 1.1 | 3.2 | 2.7 |
| * Knee int. to peak angle (°) | 2.6 | 4.9 | 3.8 | 9.8 | 0 | 1.2 | 0.7 | 0.9 | ||
| No. 7 | No. 7 | * Shoulder int. to valley (°) | 114.0 | 115.3 | 109.6 | 103.3 | 21.2 | 42.2 | 16.99 | 38.7 |
| No. 15 | No. 15 | *▲ peak to end (°) | 57.8 | 61.2 | 34.2 | 26.3 | 8.9 | 10.2 | 14.2 | 14.7 |
| No. 16 | No. 16 | * Peak/valley angle (°) | 53.1 | 58.4 | 66.7 | 72.2 | 7.8 | 8.1 | 9.7 | 27.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Kanai-Pak, M.; Maeda, J.; Kitajima, Y.; Nakamura, M.; Kuwahara, N.; Ogata, T.; Ota, J. Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses. Sensors 2018, 18, 2975. https://doi.org/10.3390/s18092975
Lin C, Kanai-Pak M, Maeda J, Kitajima Y, Nakamura M, Kuwahara N, Ogata T, Ota J. Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses. Sensors. 2018; 18(9):2975. https://doi.org/10.3390/s18092975
Chicago/Turabian StyleLin, Chingszu, Masako Kanai-Pak, Jukai Maeda, Yasuko Kitajima, Mitsuhiro Nakamura, Noriaki Kuwahara, Taiki Ogata, and Jun Ota. 2018. "Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses" Sensors 18, no. 9: 2975. https://doi.org/10.3390/s18092975
APA StyleLin, C., Kanai-Pak, M., Maeda, J., Kitajima, Y., Nakamura, M., Kuwahara, N., Ogata, T., & Ota, J. (2018). Translational Acceleration, Rotational Speed, and Joint Angle of Patients Related to Correct/Incorrect Methods of Transfer Skills by Nurses. Sensors, 18(9), 2975. https://doi.org/10.3390/s18092975