Feasibility of Optical Coherence Tomography (OCT) for Intra-Operative Detection of Blood Flow during Gastric Tube Reconstruction


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients and Feasibility of Intra-Operative OCT Imaging
3.2. 3D OCT Scans
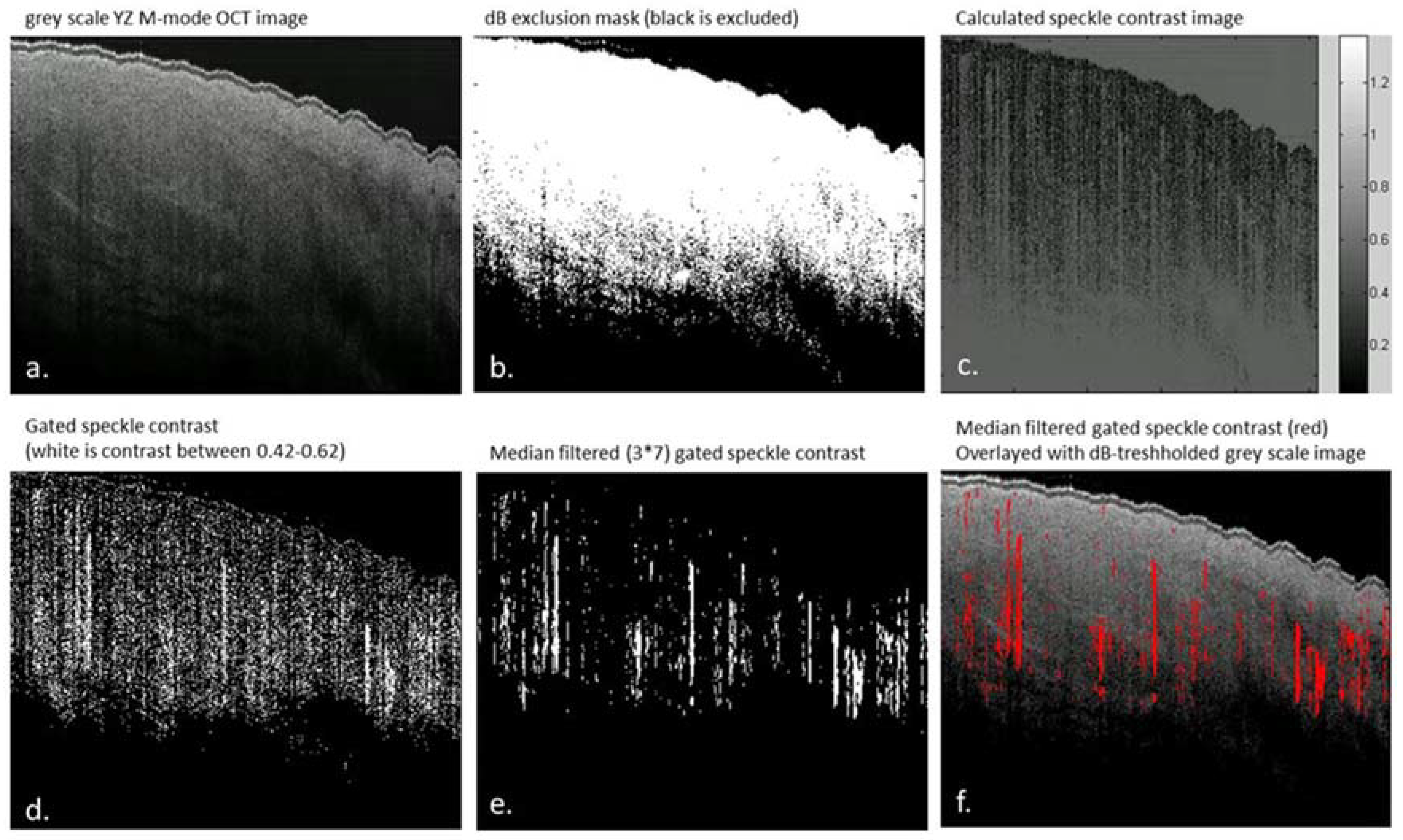
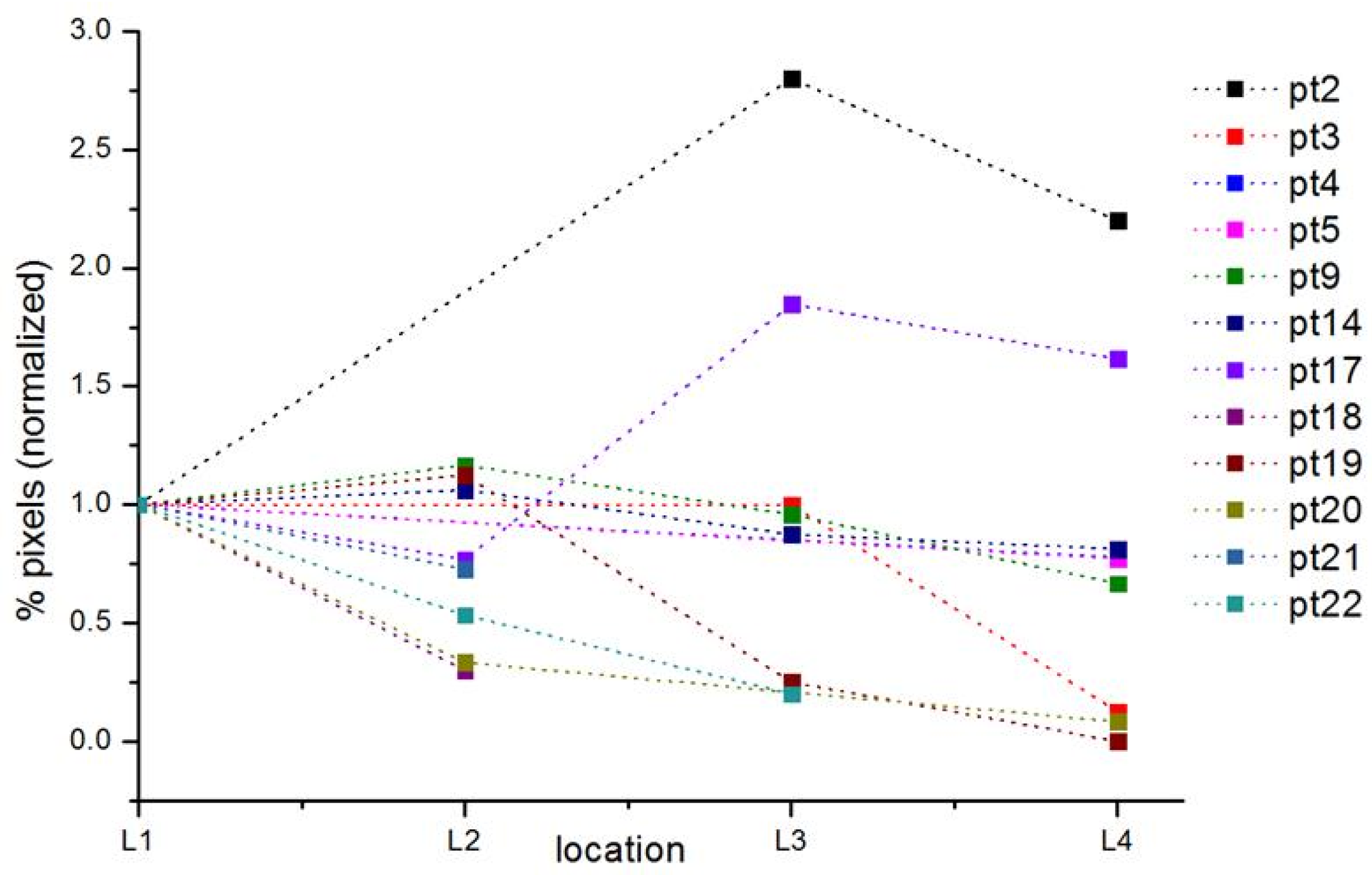
3.3. Speckle Contrast Analysis of M-Mode OCT Scans
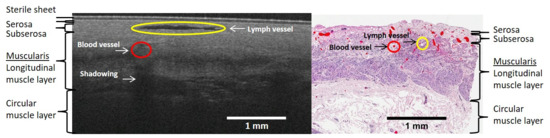
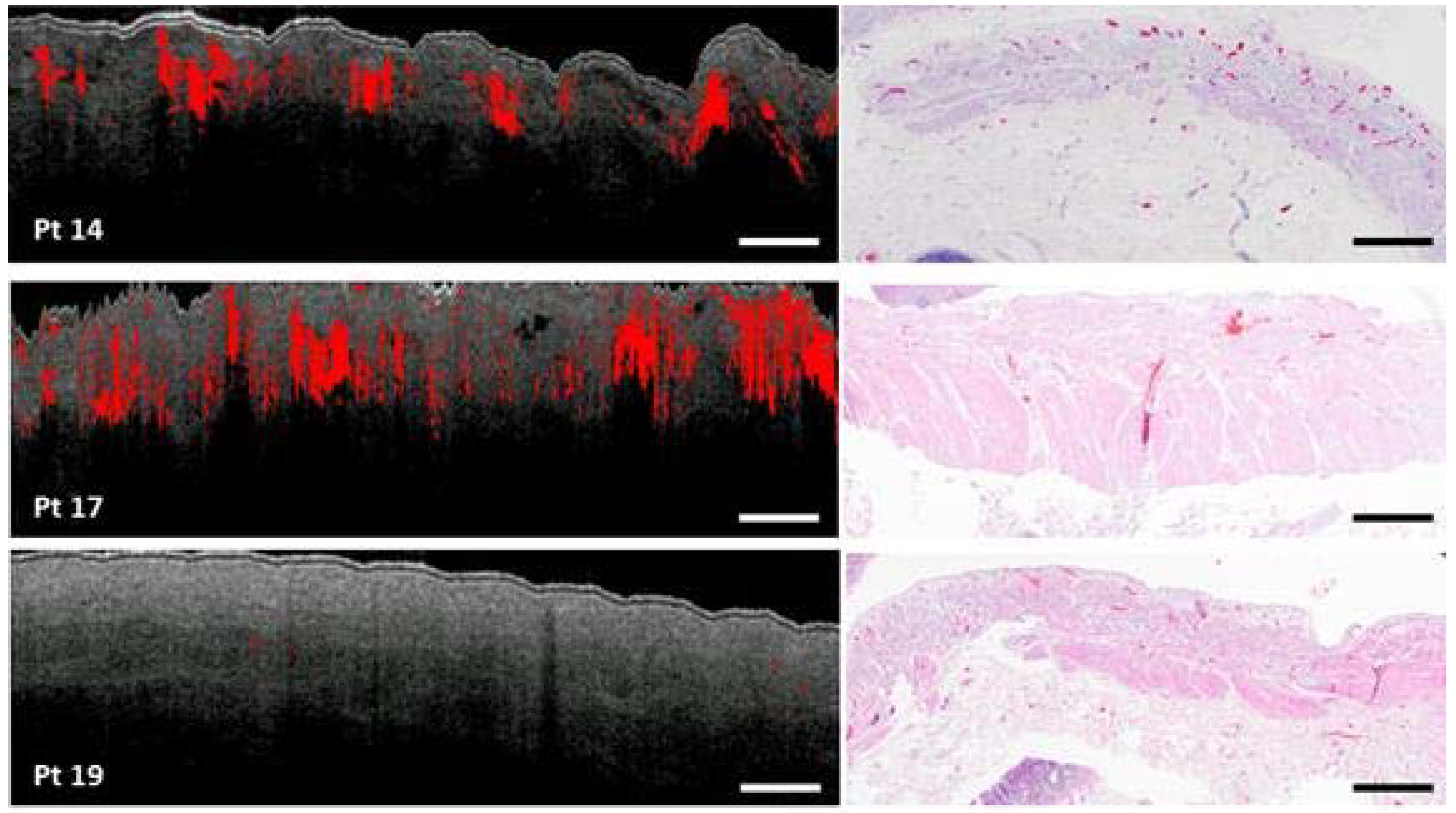
3.4. Histology Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Futier, E.; Robin, E.; Jabaudon, M.; Guerin, R.; Petit, A.; Bazin, J.-E.; Constantin, J.-M.; Vallet, B. Central venous O2 saturation and venous-to-arterial CO2 difference as complementary tools for goal-directed therapy during high-risk surgery. Crit. Care 2010, 14, R193. [Google Scholar] [CrossRef] [PubMed]
- Biere, S.S.; van Berge Henegouwen, M.I.; Maas, K.W.; Bonavina, L.; Rosman, C.; Garcia, J.R.; Gisbertz, S.S.; Klinkenbijl, J.H.; Hollmann, M.W.; de Lange, E.S.; et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: A multicentre, open-label, randomised controlled trial. Lancet 2012, 379, 1887–1892. [Google Scholar] [CrossRef]
- Miyazaki, T.; Kuwano, H.; Kato, H.; Yoshikawa, M.; Ojima, H.; Tsukada, K. Predictive value of blood flow in the gastric tube in anastomotic insufficiency after thoracic esophagectomy. World J. Surg. 2002, 26, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Zehetner, J.; DeMeester, S.R.; Alicuben, E.T.; Oh, D.S.; Lipham, J.C.; Hagen, J.A.; DeMeester, T.R. Intraoperative Assessment of Perfusion of the Gastric Graft and Correlation With Anastomotic Leaks After Esophagectomy. Ann. Surg. 2015, 262, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Veelo, D.P.; Gisbertz, S.S.; Hannivoort, R.A.; Van Dieren, S.; Geerts, B.F.; Henegouwen, M.I.V.B.; Hollmann, M.W. The effect of on-demand vs deep neuromuscular relaxation on rating of surgical and anaesthesiologic conditions in patients undergoing thoracolaparoscopic esophagectomy ( DEPTH trial): Study protocol for a randomized controlled trial. Trials 2015, 331. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jansen, S.M.; de Bruin, D.M.; van Berge Henegouwen, M.I.; Strackee, S.D.; Veelo, D.P.; Van Leeuwen, T.G.; Gisbertz, S.S. Optical Techniques for Perfusion Monitoring of the Gastric Tube after Esophagectomy: A review of technologies & thresholds. Dis. Esophagus 2018, in press. [Google Scholar]
- Huang, D.; Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotire, T.; Gregory, K.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Jansen, S.M.; de Bruin, D.M.; Faber, D.J.; Dobbe, I.J.G.G.; Heeg, E.; Milstein, D.M.J.; Strackee, S.D.; van Leeuwen, T.G. Applicability of quantitative optical imaging techniques for intraoperative perfusion diagnostics: A comparison of laser speckle contrast imaging, sidestream dark-field microscopy, and optical coherence tomography. J. Biomed. Opt. 2017, 22, 1–9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Alander, J.T.; Kaartinen, I.; Laakso, A.; Pätilä, T.; Spillmann, T.; Tuchin, V.V.; Venermo, M.; Välisuo, P. A Review of indocyanine green fluorescent imaging in surgery. Int. J. Biomed. Imaging 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Senarathna, J.; Member, S.; Rege, A.; Li, N.; Thakor, N.V. Laser Speckle Contrast Imaging: Theory, Instrumentation and Applications. IEEE Rev. Biomed. Eng. 2013, 6, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Rajan, V.; Varghese, B.; Van Leeuwen, T.G.; Steenbergen, W. Review of methodological developments in laser Doppler flowmetry. Lasers Med. Sci. 2009, 24, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Gong, P.; Es’haghian, S.; Harms, K.A.; Murray, A.; Rea, S.; Kennedy, B.F.; Wood, F.M.; Sampson, D.D.; Mclaughlin, R.A. Optical coherence tomography for longitudinal monitoring of vasculature in scars treated with laser fractionation. J. Biophotonics 2016, 9, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Mariampillai, A.; Leung, M.K.K.; Jarvi, M.; Standish, B.A.; Lee, K.; Wilson, B.C.; Vitkin, A.; Yang, V.X.D. Optimized speckle variance OCT imaging of microvasculature. Opt. Lett. 2010, 35, 1257–1259. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.; Van Leeuwen, T.G.; Kalkman, J. Localized measurement of longitudinal and transverse flow velocities in colloidal suspensions using optical coherence tomography. Phys. Rev. E Stat. Nonlinear Soft Matter Phys. 2013, 88, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, K.; Huang, Y.; Kang, J.U. Spectroscopic-speckle variance OCT for microvasculature detection and analysis. Biomed. Opt. Express 2011, 2, 2995–3009. [Google Scholar] [CrossRef] [PubMed]
- Jansen, S.M.; de Bruin, D.M.; van Berge Henegouwen, M.I.; Strackee, S.D.; Veelo, D.P.; van Leeuwen, T.G.; Gisbertz, S.S. Can we predict necrosis intra-operatively? Real-time optical quantitative perfusion imaging in surgery: Study protocol for a prospective, observational, in vivo pilot study. Pilot Feasibil. Stud. 2017, 3, 65. [Google Scholar] [CrossRef] [PubMed]
- Almasian, M.; van Leeuwen, T.G.; Faber, D.J. OCT Amplitude and Speckle Statistics of Discrete Random Media. Sci. Rep. 2017, 7, 14873. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, M.S.; Cadotte, D.W.; Vuong, B.; Sun, C.; Luk, T.W.H.; Mariampillai, A.; Yang, V.X.D. Review of speckle and phase variance optical coherence tomography to visualize microvascular networks. J. Biomed. Opt. 2013, 18, 50901. [Google Scholar] [CrossRef] [PubMed]
- Gong, P.; Es’haghian, S.; Harms, K.-A.; Murray, A.; Rea, S.; Wood, F.M.; Sampson, D.D.; McLaughlin, R.A. In vivo label-free lymphangiography of cutaneous lymphatic vessels in human burn scars using optical coherence tomography. Biomed. Opt. Express 2016, 7, 4886. [Google Scholar] [CrossRef] [PubMed]
- Liew, Y.M.; McLaughlin, R.A.; Gong, P.; Wood, F.M.; Sampson, D.D. In vivo assessment of human burn scars through automated quantification of vascularity using optical coherence tomography. J. Biomed. Opt. 2013, 18, 61213. [Google Scholar] [CrossRef] [PubMed]
- Balestra, G.M.; Bezemer, R.; Boerma, E.C.; Yong, Z.-Y.; Sjauw, K.D.; Engstrom, A.E.; Koopmans, M.; Ince, C. Improvement of sidestream dark field imaging with an image acquisition stabilizer. BMC Med. Imaging 2010, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Rino, Y.; Yukawa, N.; Sato, T.; Yamamoto, N.; Tamagawa, H.; Hasegawa, S.; Oshima, T.; Yoshikawa, T.; Masuda, M.; Imada, T. Visualization of blood supply route to the reconstructed stomach by indocyanine green fluorescence imaging during esophagectomy. BMC Med. Imaging 2014, 14, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Okumura, T.; Nagata, T.; Sawada, S.; Matsui, K.; Hori, R.; Yoshioka, I.; Yoshida, T.; Osada, R.; Tsukada, K. Usefulness of blood supply visualization by indocyanine green fluorescence for reconstruction during esophagectomy. Esophagus 2011, 8, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Yoshida, M.; Kuroda, J.; Okada, A.; Ohta, K.; Kitajima, M. Application of the HyperEye Medical System for esophageal cancer surgery: A preliminary report. Surg. Today 2013, 43, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, Y.; Ishiguro, T.; Sobajima, J.; Fukuchi, M.; Ishibashi, K.; Baba, H.; Mochiki, E.; Kawano, T.; Ishida, H. Indocyanine green fluorescence method for reconstructed gastric tube during esophagectomy. Dis. Esophagus 2014, 27, 106A. [Google Scholar] [CrossRef]
- Yukaya, T.; Saeki, H.; Kasagi, Y.; Nakashima, Y.; Ando, K.; Imamura, Y.; Ohgaki, K.; Oki, E.; Morita, M.; Maehara, Y. Indocyanine Green Fluorescence Angiography for Quantitative Evaluation of Gastric Tube Perfusion in Patients Undergoing Esophagectomy. J. Am. Coll. Surg. 2015, 221, e37–e42. [Google Scholar] [CrossRef] [PubMed]
- Pauling, J.D.; Shipley, J.A.; Raper, S.; Watson, M.L.; Ward, S.G.; Harris, N.D.; McHugh, N.J. Comparison of infrared thermography and laser speckle contrast imaging for the dynamic assessment of digital microvascular function. Microvasc. Res. 2012, 83, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Milstein, D.M.J.; Ince, C.; Gisbertz, S.S.; Boateng, K.B.; Geerts, B.F.; Hollmann, M.W.; Van Berge Henegouwen, M.I.; Veelo, D.P. Laser speckle contrast imaging identifies ischemic areas on gastric tube reconstructions following esophagectomy. Medicine 2016, 95. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Hollenberg, S.; Boerma, C.; Goedhart, P.; Büchele, G.; Ospina-Tascon, G.; Dobbe, I.; Ince, C. How to evaluate the microcirculation: Report of a round table conference. Crit. Care 2007, 11, R101. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, A.F.J.; Kornmann, V.N.N.; van der Sloot, K.; van Vugt, J.L.; Gosselink, M.P.; Smits, A.; Van Ramshorst, B.; Boerma, E.C.; Noordzij, P.G.; Boerma, D.; et al. Sidestream dark field imaging of the serosal microcirculation during gastrointestinal surgery. Color. Dis. 2016, 18, O103–O110. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | pt2 | pt3 | pt4 | pt5 | pt6 | pt9 | pt12 | pt14 | pt16 | pt17 | pt18 | pt19 | pt20 | pt21 | pt22 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| location 1 | 5 | 8 | 18 | 22 | x | 24 | x | 16 | x | 13 | 20 | 8 | 12 | 11 | 15 |
| location 2 | x | x | x | x | x | 28 | 2 | 17 | 8 | 10 | 6 | 9 | 4 | 8 | 8 |
| location 3 | 14 | 8 | x | x | x | 23 | 5 | 14 | x | 24 | x | 2 | x | x | 3 |
| location 4 | 11 | 1 | 14 | 17 | 18 | 16 | x | 13 | x | 21 | x | 0 | 1 | x | x |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jansen, S.M.; Almasian, M.; Wilk, L.S.; De Bruin, D.M.; Van Berge Henegouwen, M.I.; Strackee, S.D.; Bloemen, P.R.; Meijer, S.L.; Gisbertz, S.S.; Van Leeuwen, T.G. Feasibility of Optical Coherence Tomography (OCT) for Intra-Operative Detection of Blood Flow during Gastric Tube Reconstruction. Sensors 2018, 18, 1331. https://doi.org/10.3390/s18051331
Jansen SM, Almasian M, Wilk LS, De Bruin DM, Van Berge Henegouwen MI, Strackee SD, Bloemen PR, Meijer SL, Gisbertz SS, Van Leeuwen TG. Feasibility of Optical Coherence Tomography (OCT) for Intra-Operative Detection of Blood Flow during Gastric Tube Reconstruction. Sensors. 2018; 18(5):1331. https://doi.org/10.3390/s18051331
Chicago/Turabian StyleJansen, Sanne M., Mitra Almasian, Leah S. Wilk, Daniel M. De Bruin, Mark I. Van Berge Henegouwen, Simon D. Strackee, Paul R. Bloemen, Sybren L. Meijer, Suzanne S. Gisbertz, and Ton G. Van Leeuwen. 2018. "Feasibility of Optical Coherence Tomography (OCT) for Intra-Operative Detection of Blood Flow during Gastric Tube Reconstruction" Sensors 18, no. 5: 1331. https://doi.org/10.3390/s18051331
APA StyleJansen, S. M., Almasian, M., Wilk, L. S., De Bruin, D. M., Van Berge Henegouwen, M. I., Strackee, S. D., Bloemen, P. R., Meijer, S. L., Gisbertz, S. S., & Van Leeuwen, T. G. (2018). Feasibility of Optical Coherence Tomography (OCT) for Intra-Operative Detection of Blood Flow during Gastric Tube Reconstruction. Sensors, 18(5), 1331. https://doi.org/10.3390/s18051331