
The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients—A Systematic Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Methods
2.3. Study Selection
2.4. Data Extraction and Handling
3. Results
3.1. Results of the Search
3.2. Study Descriptives
3.3. Efficacy
3.4. Accuracy
3.5. Safety
3.6. Workload and Costs
3.7. Children
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. Ovid MEDLINE Search
| # | Searches | Results |
| 1 | ((glucose or BG) adj1 (sensor* or biosensor* or continuous* or realtime or real time)).tw,kf. | 5099 |
| 2 | ((glucose or BG) adj monitor*).tw,kf. | 5227 |
| 3 | ((continuous* or real time or subcutan* or arter* or venous or intravasc*) adj monitor* adj12 glucos*).tw,kf. | 325 |
| 4 | (continuous adj3 (glucose measurem* or glucosemeter*)).tw,kf. | 93 |
| 5 | (CGM or CGMs or GCMS* or RTCGM* or BGM or BGMs or CIGM* or IVCGM* or scCGM* or sCGM* or tCGM* or MDCGM* or IACGM).tw,kf. and glucose.mp. | 1543 |
| 6 | (IVBG or (intraven* adj (blood glucose or BG) adj3 system*)).tw,kf. | 4 |
| 7 | (GlucoDay* or Freestyle or Libre or Navigator or Medtronic* or MiniMed* or Sentrino* or Enlite* or Optiscanner or Eirus* or Glucath* or Glysure* or Symphony or Glucoclear* or (DexCom adj1 STS) or (Guardian adj2 real time)).tw,kf. and glucose.mp. | 552 |
| 8 | clarke error grid.tw,kf. | 184 |
| 9 | or/1−8 [CGM] | 8143 |
| 10 | animals/ not humans/ | 4,248,414 |
| 11 | 9 not 10 [human CGM] | 7501 |
| 12 | critical care/or exp life support care/or subacute care/or intensive care units/or critical illness/or burn units/or coronary care units/or recovery room/or respiratory care units/[MESH] | 105,986 |
| 13 | ((intensive or critical*) adj (care or ill*)).tw,kf. | 145,729 |
| 14 | (severe* adj (burn* or ill)).tw,kf. | 8464 |
| 15 | ((coronary or cardiac) adj2 care).tw,kf. | 8404 |
| 16 | (((acute care or respiratory care or acute stroke or burn*) adj unit*) or acute stroke care).tw,kf. | 3140 |
| 17 | (trauma adj2 (cent* or unit*)).tw,kf. | 13,030 |
| 18 | recovery room*.tw,kf. | 2924 |
| 19 | emergency medicine.tw,kf. | 11,055 |
| 20 | (intensivmed* or (intensive and care)).jw,ot. | 25,004 |
| 21 | (ICU or ICUs or CCU or CCUs or MICU or MICUs or CVICU* or SICU or SICUs or BICU or BICUs).tw,kf. | 43,021 |
| 22 | (ECMO or ECLS or (extracorporeal adj3 (circulation or circuit or bypass* or life support* or ventricular assist*))).tw,kf. | 14,712 |
| 23 | or/12−22 [ICU] | 261,652 |
| 24 | 11 and 23 [CGM + ICU] | 370 |
| 25 | remove duplicates from 24 | 356 |
Appendix B. Overview of Important Assessment Tools to Evaluate Point Accuracy of Continuous Glucose Monitoring (CGM) Systems
| Tool | Definition | Strengths | Weaknesses | ICU recommendations |
| Mean Absolute Relative Difference (MARD) | Percentage difference between CGM sensor reading and a value measured at the same time using a reference method. Derived as ([sensor-reference]/reference) × 100%. | Easy to compute and interpret, can be computed in different glucose range. | No distinction between positive and negative or systematic and random errors. Affected by glucose values and study design. Often unclear whether MARD or median absolute relative difference is computed. | Acceptable when <14% [73], >18% indicates poor accuracy [31]. |
| ISO 15197 guideline (2003) | Percentage CGM sensor readings within 15 mg/dL from the reference when the blood glucose is ≤75 mg/dL or within 20% from the reference when the blood glucose is >75 mg/dL. | Simple. | Does not take rate of glucose change and temporal order of the measurements into account. Resting 5% can differ by any amount. | ≥98% within 12.5% of a reference standard (or within 10 mg/dL for reading <100 mg/dL), remaining 2% within 20% [31]. |
| ISO 15197 guideline (2013) | Percentage CGM sensor readings within 15 mg/dL from the reference when the blood glucose is ≤100 mg/dL or within 15% from the reference when the blood glucose is >100 mg/dL. | |||
| Clarke error grid | Pairs CGM sensor readings with reference measurements, and categorizes pairs in terms of the consequence of treatment decisions. Zone A Within 20% of the reference value, clinically accurate. Zone B >20% difference from the reference value, benign errors since it will not lead to inappropriate clinical decisions. Zone C Overcorrection errors, unnecessary but harmless corrections. Zone D Dangerous failure to detect hypo- or hyperglycemia. Zone E Erroneous treatment error (opposite of intended treatment). | Simple. Indicates clinical significance by showing the implication on therapy. | Developed for capillary blood glucose testing systems. Original grid was designed with an arbitrary target range of 70−180 mg/dL and assumes no change in treatment when readings lie within that range. No allowance for the rate at which blood glucose concentration is changing or the frequency with which the blood glucose concentration is being measured. | 100% in zone A + B, favorably in zone A [74]. |
| Bland-Altman plot | Plot of the reference measurement or average of the two (x-axis) against the difference between CGM system and reference measurement (y-axis). Reported as mean bias with upper and lower limits of agreement (mean bias ± 1.96 × SD). Represents the random variation around the mean bias. | Simple. Possibility to distinct between systematic and random error. | Does not allows for the effect of different ranges and trend. | No recommendations. |
References
- Van den Berghe, G.; Wouters, P.; Weekers, F.; Verwaest, C.; Bruyninckx, F.; Schetz, M.; Vlasselaers, D.; Ferdinande, P.; Lauwers, P.; Bouillon, R. Intensive insulin therapy in critically ill patients. N. Engl. J. Med. 2001, 345, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.C.; Ichai, C.; Orban, J.C.; Groeneveld, A.J. Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin. Proc. 2003, 78, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Gale, S.C.; Sicoutris, C.; Reilly, P.M.; Schwab, C.W.; Gracias, V.H. Poor glycemic control is associated with increased mortality in critically ill trauma patients. Am. Surg. 2007, 73, 454–460. [Google Scholar] [PubMed]
- Whitcomb, B.W.; Pradhan, E.K.; Pittas, A.G.; Roghmann, M.C.; Perencevich, E.N. Impact of admission hyperglycemia on hospital mortality in various intensive care unit populations. Crit. Care Med. 2005, 33, 2772–2777. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Bochicchio, G.V.; Joshi, M.; Bochicchio, K.; Tracy, K.; Scalea, T.M. Admission hyperglycemia is predictive of outcome in critically ill trauma patients. J. Trauma 2005, 59, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S. Glycemic control in the critically ill—3 domains and diabetic status means one size does not fit all! Crit. Care 2013, 17, 131. [Google Scholar] [CrossRef] [PubMed]
- Van den Berghe, G.; Wilmer, A.; Hermans, G.; Meersseman, W.; Wouters, P.J.; Milants, I.; Van Wijngaerden, E.; Bobbaers, H.; Bouillon, R. Intensive insulin therapy in the medical ICU. N. Engl. J. Med. 2006, 354, 449–4461. [Google Scholar] [CrossRef] [PubMed]
- Devos, P.; Preiser, J.C. Current controversies around tight glucose control in critically ill patients. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Brunkhorst, F.M.; Engel, C.; Bloos, F.; Meier-Hellmann, A.; Ragaller, M.; Weiler, N.; Moerer, O.; Gruendling, M.; Oppert, M.; Grond, S.; et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N. Engl. J. Med. 2008, 358, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Dabbagh, O.C.; Tamim, H.M.; Al-Shimemeri, A.A.; Memish, Z.A.; Haddad, S.H.; Syed, S.J.; Giridhar, H.R.; Rishu, A.H.; Al-Daker, M.O.; et al. Intensive versus conventional insulin therapy: A randomized controlled trial in medical and surgical critically ill patients. Crit. Care Med. 2008, 36, 3190–3197. [Google Scholar] [CrossRef] [PubMed]
- Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; Henderson, W.R.; et al. Intensive versus conventional glucose control in critically ill patients. N. Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar] [PubMed]
- Preiser, J.C.; Devos, P.; Ruiz-Santana, S.; Mélot, C.; Annane, D.; Groeneveld, J.; Iapichino, G.; Leverve, X.; Nitenberg, G.; Singer, P.; et al. A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: The Glucontrol study. Intensive Care Med. 2009, 35, 1738–1748. [Google Scholar] [CrossRef] [PubMed]
- Hermanides, J.; Bosman, R.J.; Vriesendorp, T.M.; Dotsch, R.; Rosendaal, F.R.; Zandstra, D.F.; Hoekstra, J.B.L.; DeVries, J.H. Hypoglycemia is associated with intensive care unit mortality. Crit. Care Med. 2010, 38, 1430–1434. [Google Scholar] [CrossRef] [PubMed]
- The NICE-SUGAR Study Investigators. Hypoglycemia and risk of death in critically ill patients. N. Engl. J. Med. 2012, 367, 1108–1118. [Google Scholar]
- Wiener, R.S.; Wiener, D.C.; Larson, R.J. Benefits and risks of tight glucose control in critically ill adults: A meta-analysis. JAMA 2008, 300, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Griesdale, D.E.; de Souza, R.J.; van Dam, R.M.; Heyland, D.K.; Cook, D.J.; Malhotra, A.; Dhaliwal, R.; Henderson, W.R.; Chittock, D.R.; Finfer, S.; et al. Intensive insulin therapy and mortality among critically ill patients: A meta-analysis including NICE-SUGAR study data. Can. Med. Assoc. J. 2009, 180, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Preiser, J.C. Toward understanding tight glycemic control in the ICU: A systematic review and metaanalysis. Chest 2010, 137, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, J.; Bircher, N.; Krinsley, J.; Agus, M.; Braithwaite, S.S.; Deutschman, C.; Freire, A.X.; Geehan, D.; Kohl, B.; Nasraway, S.A.; et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit. Care Med. 2012, 40, 3251–3276. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2015, 38 (Suppl. 1), S5–S7. [Google Scholar]
- Haluzik, M.; Mraz, M.; Kopecky, P.; Lips, M.; Svacina, S. Glucose control in the ICU: Is there a time for more ambitious targets again? J. Diabetes Sci. Technol. 2014, 8, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Bunting, P.S.; Singh, A.; McDonald, K.; Fergusson, D.; McIntyre, L.A.; Hebert, P.C. Reliability of point-of-care testing for glucose measurement in critically ill adults. Crit. Care Med. 2005, 33, 2778–2785. [Google Scholar]
- Hoedemaekers, C.W.; Klein Gunnewiek, J.M.; Prinsen, M.A.; Willems, J.L.; Van der Hoeven, J.G. Accuracy of bedside glucose measurement from three glucometers in critically ill patients. Crit. Care Med. 2008, 36, 3062–3066. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.C.; Bruns, D.E. Effects of measurement frequency on analytical quality required for glucose measurements in intensive care units: Assessments by simulation models. Clin. Chem. 2014, 60, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Juneja, R.; Roudebush, C.P.; Nasraway, S.A.; Golas, A.A.; Jacobi, J.; Carroll, J.; Nelson, D.; Abad, V.J.; Flanders, S.J. Computerized intensive insulin dosing can mitigate hypoglycemia and achieve tight glycemic control when glucose measurement is performed frequently and on time. Crit. Care 2009, 13, R163. [Google Scholar] [CrossRef] [PubMed]
- Aragon, D. Evaluation of nursing work effort and perceptions about blood glucose testing in tight glycemic control. Am. J. Crit. Care 2006, 15, 370–377. [Google Scholar] [PubMed]
- Gartemann, J.; Caffrey, E.; Hadker, N.; Crean, S.; Creed, G.M.; Rausch, C. Nurse workload in implementing a tight glycaemic control protocol in a UK hospital: A pilot time-in-motion study. Nurs. Crit. Care 2012, 17, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Preiser, J.C.; Chase, J.G.; Hovorka, R.; Joseph, J.I.; Krinsley, J.S.; De Block, C.; Desaive, T.; Foubert, L.; Kalfon, P.; Pielmeier, U.; et al. Glucose Control in the ICU: A Continuing Story. J. Diabetes Sci. Technol. 2016, 10, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Klonoff, D.C.; Bergenstal, R.; Blonde, L.; Boren, S.A.; Church, T.S.; Gaffaney, J.; Jovanovič, L.; Kendall, D.M.; Kollman, C.; Kovatchev, B.P.; et al. Consensus report of the coalition for clinical research-self-monitoring of blood glucose. J. Diabetes Sci. Technol. 2008, 2, 1030–1053. [Google Scholar] [CrossRef] [PubMed]
- Kropff, J.; Bruttomesso, D.; Doll, W.; Farret, A.; Galasso, S.; Luijf, Y.M.; Mader, J.K.; Place, J.; Boscari, F.; Pieber, T.R.; et al. Accuracy of two continuous glucose monitoring systems: A head-to-head comparison under clinical research centre and daily life conditions. Diabetes Obes. Metab. 2015, 17, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Finfer, S.; Wernerman, J.; Preiser, J.C.; Cass, T.; Desaive, T.; Hovorka, R.; Joseph, J.I.; Kosiborod, M.; Krinsley, J.; Mackenzie, I.; et al. Clinical review: Consensus recommendations on measurement of blood glucose and reporting glycemic control in critically ill adults. Crit. Care 2013, 17, 229. [Google Scholar] [CrossRef] [PubMed]
- Introduction on Blood Glucose Controller | Medical Equipment | NIKKISO. 2016. Available online: Nikkiso.com (accessed on 12 January 2017).
- Clarke, W.L.; Cox, D.; Gonder-Frederick, L.A.; Carter, W.; Pohl, S.L. Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care 1987, 10, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 15197: 2003. In vitro Diagnostic Test Systems—Requirements for Blood-Glucose Monitoring Systems for Self-Testing in Managing Diabetes Mellitus. Available online: http://www.iso.org/iso/catalogue_detail.htm?csnumber=26309 (accessed on 12 January 2017).
- International Organization for Standardization. ISO 15197: 2013. In vitro Diagnostic Test Systems—Requirements for Blood-Glucose Monitoring Systems for Self-Testing in Managing Diabetes Mellitus. Available online: http://www.iso.org/iso/catalogue_detail?csnumber=54976 (accessed on 12 January 2017).
- De Block, C.E.; Gios, J.; Verheyen, N.; Manuel-y-Keenoy, B.; Rogiers, P.; Jorens, P.G.; Scuffi, C.; Van Gaal, L.F. Randomized Evaluation of Glycemic Control in the Medical Intensive Care Unit Using Real-Time Continuous Glucose Monitoring (REGIMEN Trial). Diabetes Technol. Ther. 2015, 17, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Boom, D.T.; Sechterberger, M.K.; Rijkenberg, S.; Kreder, S.; Bosman, R.J.; Wester, J.P.; van Stijn, I.; DeVries, J.H.; van der Voort, P.H. Insulin treatment guided by subcutaneous continuous glucose monitoring compared to frequent point-of-care measurement in critically ill patients: A randomized controlled trial. Crit. Care 2014, 18, 453. [Google Scholar] [CrossRef] [PubMed]
- Leelarathna, L.; English, S.W.; Thabit, H.; Caldwell, K.; Allen, J.M.; Kumareswaran, K.; Wilinska, M.E.; Nodale, M.; Mangat, J.; Evans, M.L.; et al. Feasibility of fully automated closed-loop glucose control using continuous subcutaneous glucose measurements in critical illness: A randomized controlled trial. Crit. Care 2013, 17, R159. [Google Scholar] [CrossRef] [PubMed]
- Kopecký, P.; Mráz, M.; Bláha, J.; Lindner, J.; Svačina, Š.; Hovorka, R.; Haluzík, M. The use of continuous glucose monitoring combined with computer-based eMPC algorithm for tight glucose control in cardiosurgical ICU. BioMed Res. Int. 2013, 2013, 186439. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, U.; Warszawska, J.; Kitzberger, R.; Wewalka, M.; Miehsler, W.; Herkner, H.; Madl, C. Real-time continuous glucose monitoring in critically ill patients: A prospective randomized trial. Diabetes Care 2010, 33, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Piper, H.G.; Alexander, J.L.; Shukla, A.; Pigula, F.; Costello, J.M.; Laussen, P.C.; Jaksic, T.; Agus, M.S. Real-time continuous glucose monitoring in pediatric patients during and after cardiac surgery. Pediatrics 2006, 118, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Bridges, B.C.; Preissig, C.M.; Maher, K.O.; Rigby, M.R. Continuous glucose monitors prove highly accurate in critically ill children. Crit. Care 2010, 14, R176. [Google Scholar] [CrossRef] [PubMed]
- Branco, R.G.; Chavan, A.; Tasker, R.C. Pilot evaluation of continuous subcutaneous glucose monitoring in children with multiple organ dysfunction syndrome. Pediatr. Crit. Care Med. 2010, 11, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Prabhudesai, S.; Kanjani, A.; Bhagat, I.; Ravikumar, K.G.; Ramachandran, B. Accuracy of a real-time continuous glucose monitoring system in children with septic shock: A pilot study. Indian J. Crit. Care Med. 2015, 19, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Nohra, E.; Buckman, S.; Bochicchio, K.; Chamieh, J.; Reese, S.; Merrill, C.; Schuerer, D.; Bochicchio, G.V. Results of a near continuous glucose monitoring Technology in Surgical Intensive Care and Trauma. Contemp. Clin. Trials 2016, 50, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Rabiee, A.; Andreasik, V.; Abu-Hamdah, R.; Galiatsatos, P.; Khouri, Z.; Gibson, B.R.; Andersen, D.K.; Elahi, D. Numerical and clinical accuracy of a continuous glucose monitoring system during intravenous insulin therapy in the surgical and burn intensive care units. J. Diabetes Sci. Technol. 2009, 3, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Schierenbeck, F.; Franco-Cereceda, A.; Liska, J. Accuracy of 2 Different Continuous Glucose Monitoring Systems in Patients Undergoing Cardiac Surgery: Intravascular Microdialysis Versus Subcutaneous Tissue Monitoring. J. Diabetes Sci. Technol. 2017, 11, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Song, I.K.; Lee, J.H.; Kang, J.E.; Park, Y.H.; Kim, H.S.; Kim, J.T. Continuous glucose monitoring system in the operating room and intensive care unit: Any difference according to measurement sites? J. Clin. Monit. Comput. 2015, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Leelarathna, L.; English, S.W.; Thabit, H.; Caldwell, K.; Allen, J.M.; Kumareswaran, K.; Wilinska, M.E.; Nodale, M.; Haidar, A.; Evans, M.L.; et al. Accuracy of subcutaneous continuous glucose monitoring in critically ill adults: Improved sensor performance with enhanced calibrations. Diabetes Technol. Ther. 2014, 16, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Saur, N.M.; England, M.R.; Menzie, W.; Melanson, A.M.; Trieu, M.Q.; Berlin, J.; Hurley, J.; Krystyniak, K.; Kongable, G.L.; Nasraway, S.A.; et al. Accuracy of a novel noninvasive transdermal continuous glucose monitor in critically ill patients. J. Diabetes Sci. Technol. 2014, 8, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Foubert, L.A.; Lecomte, P.V.; Nobels, F.R.; Gulino, A.M.; De Decker, K.H. Accuracy of a feasibility version of an intravenous continuous glucose monitor in volunteers with diabetes and hospitalized patients. Diabetes Technol. Ther. 2014, 16, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Strasma, P.J.; Finfer, S.; Flower, O.; Hipszer, B.; Kosiborod, M.; Macken, L.; Sechterberger, M.; van der Voort, P.H.; DeVries, J.H.; Joseph, J.I. Use of an Intravascular Fluorescent Continuous Glucose Sensor in ICU Patients. J. Diabetes Sci. Technol. 2015, 9, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Schierenbeck, F.; Franco-Cereceda, A.; Liska, J. Evaluation of a continuous blood glucose monitoring system using central venous microdialysis. J. Diabetes Sci. Technol. 2012, 6, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Wollersheim, T.; Engelhardt, L.J.; Pachulla, J.; Moergeli, R.; Koch, S.; Spies, C.; Hiesmayr, M.; Weber-Carstens, S. Accuracy, reliability, feasibility and nurse acceptance of a subcutaneous continuous glucose management system in critically ill patients: A prospective clinical trial. Ann. Intensive Care 2016, 6, 70. [Google Scholar] [CrossRef] [PubMed]
- Van Hooijdonk, R.T.; Leopold, J.H.; Winters, T.; Binnekade, J.M.; Juffermans, N.P.; Horn, J.; Fischer, J.C.; van Dongen-Lases, E.C.; Schultz, M.J. Point accuracy and reliability of an interstitial continuous glucose-monitoring device in critically ill patients: A prospective study. Crit. Care 2015, 19, 34. [Google Scholar] [CrossRef] [PubMed]
- Yue, X.Y.; Zheng, Y.; Cai, Y.H.; Yin, N.N.; Zhou, J.X. Real-time continuous glucose monitoring shows high accuracy within 6 hours after sensor calibration: A prospective study. PLoS ONE 2013, 8, e60070. [Google Scholar] [CrossRef] [PubMed]
- Corstjens, A.M.; Ligtenberg, J.J.; van der Horst, I.C.; Spanjersberg, R.; Lind, J.S.; Tulleken, J.E.; Meertens, J.H.; Zijlstra, J.G. Accuracy and feasibility of point-of-care and continuous blood glucose analysis in critically ill ICU patients. Crit. Care 2006, 10, R135. [Google Scholar] [CrossRef] [PubMed]
- Leopold, J.H.; van Hooijdonk, R.T.M.; Boshuizen, M.; Winters, T.; Bos, L.D.; Abu-Hanna, A.; Hoek, A.M.T.; Fischer, J.C.; van Dongen-Lases, E.C.; Schultz, M.J. Point and trend accuracy of a continuous intravenous microdialysis-based glucose-monitoring device in critically ill patients: A prospective study. Ann. Intensiv. Care 2016, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Crane, B.C.; Barwell, N.P.; Gopal, P.; Gopichand, M.; Higgs, T.; James, T.D.; Jones, C.M.; Mackenzie, A.; Mulavisala, K.P.; Paterson, W. The Development of a Continuous Intravascular Glucose Monitoring Sensor. J. Diabetes Sci. Technol. 2015, 9, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Sechterberger, M.K.; van der Voort, P.H.; Strasma, P.J.; DeVries, J.H. Accuracy of Intra-arterial and Subcutaneous Continuous Glucose Monitoring in Postoperative Cardiac Surgery Patients in the ICU. J. Diabetes Sci. Technol. 2015, 9, 663–667. [Google Scholar] [CrossRef] [PubMed]
- De Block, C.; Manuel-y-Keenoy, B.; Van Gaal, L.; Rogiers, P. Intensive insulin therapy in the intensive care unit: Assessment by continuous glucose monitoring. Diabetes Care 2006, 29, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, U.; Warszawska, J.; Kitzberger, R.; Herkner, H.; Metnitz, P.G.; Madl, C. Impact of shock requiring norepinephrine on the accuracy and reliability of subcutaneous continuous glucose monitoring. Intensiv. Care Med. 2009, 35, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Lorencio, C.; Leal, Y.; Bonet, A.; Bondia, J.; Palerm, C.C.; Tache, A.; Sirvent, J.M.; Vehi, J. Real-time continuous glucose monitoring in an intensive care unit: Better accuracy in patients with septic shock. Diabetes Technol. Ther. 2012, 14, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Kosiborod, M.; Gottlieb, R.K.; Sekella, J.A.; Peterman, D.; Grodzinsky, A.; Kennedy, P.; Borkon, M.A. Performance of the Medtronic Sentrino continuous glucose management (CGM) system in the cardiac intensive care unit. BMJ Open Diabetes Res. Care 2014, 2, e000037. [Google Scholar] [CrossRef] [PubMed]
- Siegelaar, S.E.; Barwari, T.; Hermanides, J.; van der Voort, P.H.; Hoekstra, J.B.; DeVries, J.H. Microcirculation and its relation to continuous subcutaneous glucose sensor accuracy in cardiac surgery patients in the intensive care unit. J. Thorac. Cardiovasc. Surg. 2013, 146, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Maahs, D.M.; DeSalvo, D.; Pyle, L.; Ly, T.; Messer, L.; Clinton, P.; Westfall, E.; Wadwa, R.P.; Buckingham, B. Effect of acetaminophen on CGM glucose in an outpatient setting. Diabetes Care 2015, 38, e158–e159. [Google Scholar] [CrossRef] [PubMed]
- Macken, L.; Flower, O.J.; Bird, S.; Hammond, N.; Yarad, E.; Bass, F.; Fisher, C.; Strasma, P.; Finfer, S. Continuous intra-arterial blood glucose monitoring using quenched fluorescence sensing in intensive care patients after cardiac surgery: Phase II of a product development study. Crit. Care Resusc. 2015, 17, 190–196. [Google Scholar] [PubMed]
- Orford, N.R.; Bailey, M.; Kaukonen, K.; Elderkin, T.; Stow, P.J.; Cattigan, C.; Kotowicz, M.; Bellomo, R. Glycaemic control and long-term outcomes following transition from modified intensive insulin therapy to conventional glycaemic control. Anaesth. Intensive Care 2014, 42, 239–247. [Google Scholar] [PubMed]
- Maahs, D.M.; Buckingham, B.A.; Castle, J.R.; Cinar, A.; Damiano, E.R.; Dassau, E.; DeVries, J.H.; Doyle, F.J.; Griffen, S.C.; Haidar, A.; et al. Outcome Measures for Artificial Pancreas Clinical Trials: A Consensus Report. Diabetes Care 2016, 39, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Wentholt, I.M.; Hoekstra, J.B.; Devries, J.H. A critical appraisal of the continuous glucose-error grid analysis. Diabetes Care 2006, 29, 1805–1811. [Google Scholar] [CrossRef] [PubMed]
- Schierenbeck, F.; Öwall, A.; Franco-Cereceda, A.; Liska, J. Evaluation of a continuous blood glucose monitoring system using a central venous catheter with an integrated microdialysis function. Diabetes Technol. Ther. 2013, 15, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Wernerman, J.; Desaive, T.; Finfer, S.; Foubert, L.; Furnary, A.; Holzinger, U.; Hovorka, R.; Joseph, J.; Kosiborod, M.; Krinsley, J.; et al. Continuous glucose control in the ICU: Report of a 2013 round table meeting. Crit. Care 2014, 18, 226. [Google Scholar] [CrossRef] [PubMed]
- Clarke, W.; Kovatchev, B. Statistical tools to analyze continuous glucose monitor data. Diabetes Technol. Ther. 2009, 11 (Suppl. 1), S45–S54. [Google Scholar] [CrossRef] [PubMed]
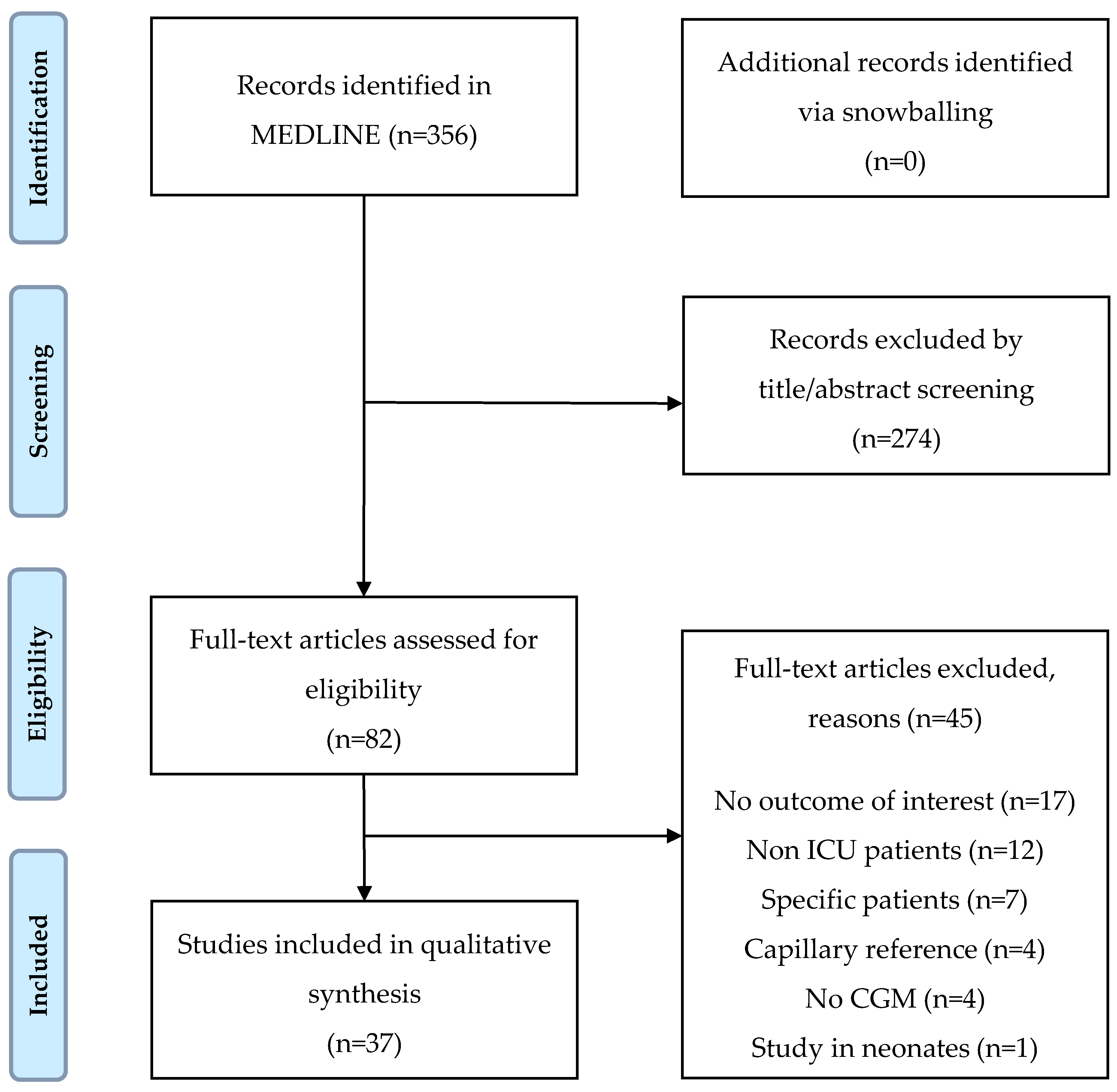

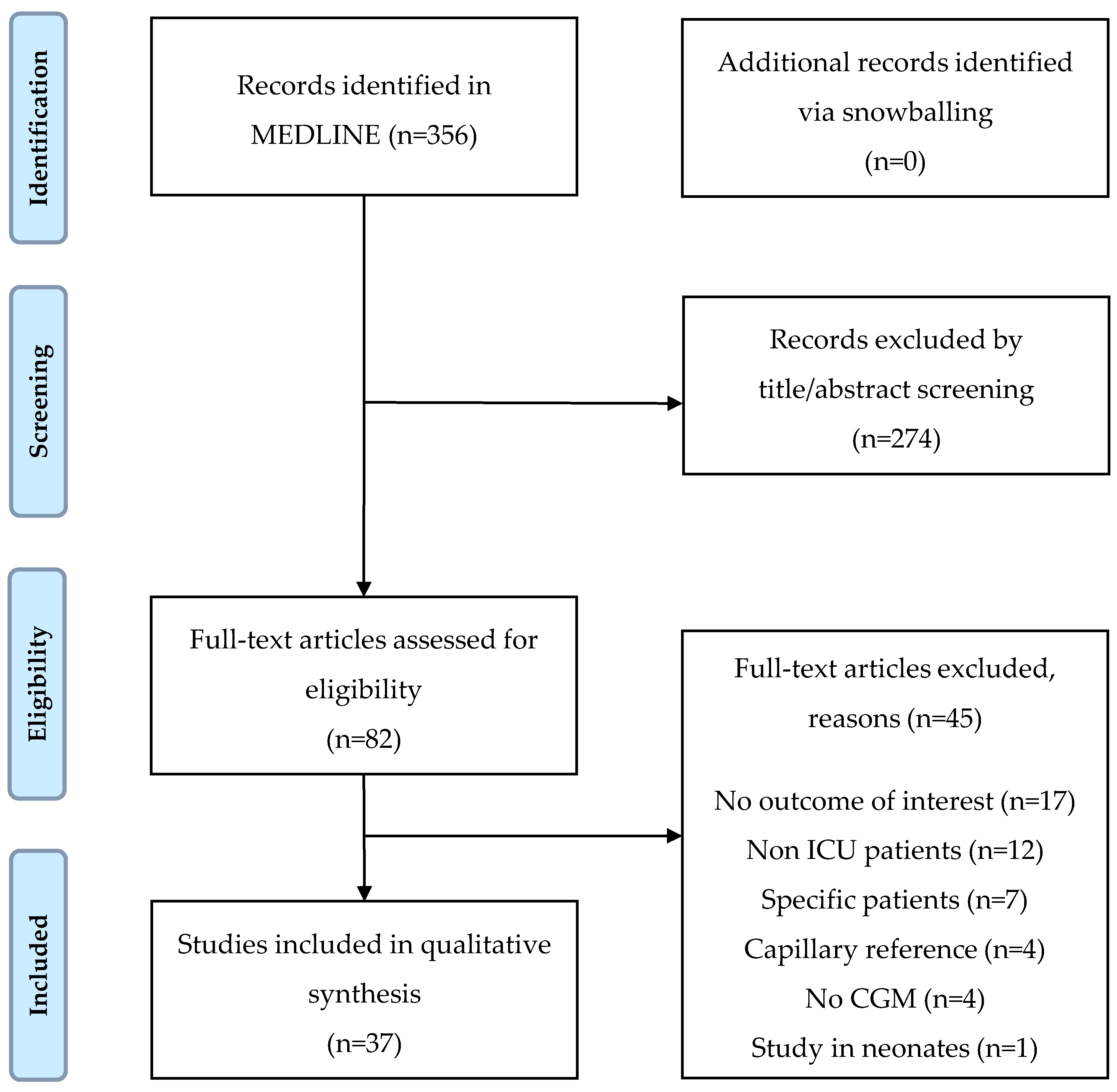{kind=link}
| Main Outcome | Accuracy (n = 32) | Effectivity (n = 5) |
|---|---|---|
| Year of publication (range) | 2006–2016 | 2010–2015 |
| Study design (n, %) | ||
| RCTs | 1 (3.1%) | 5 (100%) |
| Observational trial | 30 (93.8%) | 0 |
| Pooled analysis of two RCTs | 1 (3.1%) | 0 |
| Type of patients (n, %) | ||
| Mixed ICU patients | 12 (37.5%) | 3 (60.0%) |
| Medical patients | 0 | 0 |
| General surgical patients | 5 (15.6%) | 0 |
| Cardiac surgery patients | 9 (28.1%) | 1 (20.0%) |
| Neurosurgical patients | 2 (6.3%) | 1 (20.0%) |
| Children | 4 (12.5%) | 0 |
| Maximum study duration (hours) | ||
| Median [IQR] | 72 [48–72] | 72 [36–108] |
| Range | 24–168 | 24–120 |
| Not reported | 4 (12.5%) | 0 |
| Number of analysed patients | ||
| Median [IQR] | 23 [19–48] | 35 [24–140] |
| Range | 8–174 | 24–156 |
| Type of CGM device studied (n, %) | ||
| Subcutaneous | 19 (59.4%) | 5 (100%) |
| Intravascular | 10 (31.3%) | 0 |
| Transdermal | 1 (3.1%) | 0 |
| Subcutaneous and intravascular | 2 (6.3%) | 0 |
| Reference measurement (n, %) | ||
| Arterial | 21 (65.6%) | 5 (100%) |
| Venous | 4 (12.5%) | 0 |
| Arterial and venous | 4 (12.5%) | 0 |
| Not described | 3 (9.4%) | 0 |
| Number of paired samples (n, %) | ||
| Median [IQR] | 672 [346–1028] | 440 [277–603] |
| Range | 34–2045 | 277–635 |
| Not reported | 2 (6.3%) | 2 (40%) |
| Findings | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CGM System | N a | Study Population | Average Glucose b (mg/dL) | Time in Range c (%) | Time in Hypogly-Cemia c (%) | Time in Hypergly-Cemia c (%) | Target Glucose Range d (mg/dL) | |||||
| GlucoDay, A. Menarini Diagnostics | 35 | Mixed ICU population | Intervention | 119.0 | ±17.0 | 37.0 | ±12.0 | 0.6 | ±1.6 | 4.0 | ±5.0 | 80–120 |
| Control | 122.0 | ±11.0 | 34.0 | ±10.0 | 2.4 | ±4.3 | 2.0 | ±3.0 | ||||
| FreeStyle Navigator I, Abbott | 156 | Mixed ICU population | Intervention | 127.9 | ±19.8 | 75.0 | ±18.0 | 3 episodes in 3 patients | 3.0 | ±7.0 | 90–160 | |
| Control | 135.1 | ±23.4 | 71.0 | ±20.0 | 4 episodes in 4 patients | 4.0 | ±9.0 | |||||
| FreeStyle Navigator I, Abbott | 24 | Neurosur-gical patients | Intervention | 142.3 | [133.3–147.7] | 54.3 * | [44.1–72.8] | 0.0 | 1 episode in 1 patient | 110–140 | ||
| Control | 164.0 | [149.6–234.2] | 18.5 * | [0.1–39.9] | 0.0 | 11 episodes in 5 patients | ||||||
| Guardian REAL-Time, Medtronic | 24 | Cardiosur-gical patients | Intervention | 111.7 | ±1.8 | 46.3 | ±5.5 | 0 episodes | 80–110 | |||
| Control | 109.9 | ±10.8 | 46.2 | ±6.5 | 2 episodes | |||||||
| Guardian REAL-Time, Medtronic | 124 | Mixed ICU patients | Intervention | 105.8 | ±18.1 | 59.0 | ±20.4 | 1.6% of patients * | 80–110 | |||
| Control | 110.6 | ±10.4 | 55.0 | ±18.0 | 11.5% of patients * | |||||||
| Findings | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author Year | CGM System | N a | MARD b (%) | ISO c (%) | Clarke Error Grid d (% in Zones A–E) | Bland-Altman e (mg/dL) | Target Range ICU f (mg/dL) | Reference Sample | ||||||
| A | B | C | D | E | ||||||||||
| Adults | ||||||||||||||
| Wollersheim et al., 2016 | Sentrino, Medtronic | 532 (20) | 15.3 | (13.5–17.0) | 76.9 | 76.9 | 21.6 | 0.2 | 0.9 | 0.4 | 0.5 (−63.5 to 64.6) | 80–149 | Arterial or venous | |
| Schierenbeck et al., 2016 | FreeStyle Libre, Abbott *** | 578 (26) | 30.5 | ±12.4 | 7.0 | 18.9 | 80.2 | 0.9 | −43.2 (−82 to −4.5) | 90–180 | Arterial | |||
| v. Hooijdonk et al., 2015 | Unspecified, Medtronic | 929 (50) | 14.8 | 75.8 | 75.3 | 23.5 | 0.3 | 0.9 | 0.0 | −0.6 (−57.2 to 56.0) | 90–144 | Arterial | ||
| Song et al., 2015 | Guardian REAL-Time, Medtronic | 331 (22) | Thigh | 23.7 | ±30.2 | 60.1 | 34.4 | 3.3 | 1.5 | 0.6 | 6.6. (−109.7 to 122.9) | Arterial | ||
| 270 (22) | Abdomen | 23.2 | ±19.5 | 57.0 | 36.7 | 3.0 | 3.3 | 0.0 | 14.9 (−108.2 to 138.1) | |||||
| Sechterberg et al., 2015 | FreeStyle Navigator I, Abbott | 183 (8) | 11.1 | ±8.3 | 84.2 | −8.0 (−49.7 to 33.8) | 90–160 | Arterial | ||||||
| De Block et al., 2015 | GlucoDay, A. Menarini Diagnostics | 635 (35) | 11.2 | 87.0 | 87.1 | 11.5 | 0.4 | 1.0 | 0.0 | 80–120 | Arterial | |||
| Saur et al., 2014 | Symphony, Echo Therapeutics * | 570 (15) | 12.3 | 81.7 | 18.3 | 0.0 | 7.8 (−31.5 to 47.2) | 100–180 | Arterial | |||||
| Leelarathna et al., 2014 | FreeStyle Navigator I, Abbott | 516 (12) | Enhanced calibration | 9.6 | ±8.9 | 87.8 | 87.8 | 12.2 | 0.0 | −1.8 (−12.6 to 7.2) | Arterial | |||
| 544 (12) | Normal calibration | 15.6 | ±12.0 | 70.2 | 70.2 | 29.0 | 0.0 | 0.8 | 0.0 | −19.8 (−41.4 to 1.8) | ||||
| Kosiborod et al., 2014 | Sentrino, Medtronic | 870 (21) | 12.8 | (11.9–13.6) | 83.0 | 16.0 | 0.8 | 0.0 | 2.5 (−43.7 to 48.7) | <140 | Venous | |||
| Boom et al., 2014 | FreeStyle Navigator, Abbott | 440 (177) | 13.7 * | [8.0–23.0] | 90–160 | Arterial | ||||||||
| Aust et al., 2014 | CGMS System Gold, Medtronic | 342 (10) | 86.3 | 12.9 | 0.0 | 0.9 | 0.0 | 0 (limits not reported) | 80–150 | Arterial | ||||
| Yue et al., 2013 | DGMS, San MediTech | 314 (18) | 14.4 | ±12.2 | 74.8 | 25.2 | 0.0 | 1.8 (−59.5 to 63.1) | 140–200 | Venous | ||||
| Siegelaar et al., 2013 | Guardian REAL-Time, Medtronic | (60) | 14.0 | [11.0–18.0] | 73.2 | 25.2 | 1.3 | 90–144 | Arterial | |||||
| FreeStyle Navigator I, Abbott | 11.0 | [8.0–16.0] | 81.8 | 17.7 | 0.5 | 0.0 | ||||||||
| Leelarathna et al., 2013 | FreeStyle Navigator I, Abbott | (27) | 7.0* | [3.5–13.0] | 87.8 | 110–180 | Arterial | |||||||
| Kopecky et al., 2013 | Guardian REAL-Time, Medtronic | 277 (24) | 66.4 | 31.1 | 0.0 | 2.5 | 0.0 | 80–110 | Arterial | |||||
| Lorencio et al., 2012 | Unspecified, Medtronic | 956 (41) | 13.5 | (6.0–24.1) | 68.1 | 6.4 (−53.1 to 65.8) | 120–160 | Arterial | ||||||
| Siegelaar et al., 2011 | Guardian REAL-Time, Medtronic | 1017 (60) | 14.0 | [11.0–17.0] | Arterial | |||||||||
| FreeStyle Navigator I, Abbott | 10.0 | [8.0–16.0] | ||||||||||||
| Brunner et al., 2011 ** | Unspecified, Medtronic | 2045 (177) | 7.3 | (6.8–7.8) | 92.9 | 99.1 | 0.5 | 0.4 | 0.0 | 2.0 (−21.0 to 25.0) | Arterial | |||
| Rabiee et al., 2009 | Unspecified, Dexcom | 84 (19) | 75.0 | 25.0 | 0.0 | 90–120 | Unknown | |||||||
| Holzinger et al., 2009 | CGMS System Gold, Medtronic | 736 (50) | 94.0 | 98.6 | 0.0 | 0.7 | 0.7 | 0.7 (−1.4 to 2.9) | Arterial | |||||
| De Block et al., 2006 | GlucoDay, A. Menarini Diagnostics | 820 (50) | 2-pt calibration | 72.5 | 22.2 | 4.5 | 0.7 | 0.1 | 110–140 | Arterial | ||||
| 555 (50) | 6-pt calibration | 80.5 | 16.2 | 1.6 | 1.4 | 0.2 | ||||||||
| Corstjens et al., 2006 | CGMS System Gold, Medtronic | 165 (19) | 87.3 | 12.7 | 0.0 | 1.8 (−41.4 to 36.9) | 110–140 | Arterial | ||||||
| Children | ||||||||||||||
| Piper et al., 2006 | CGMS System Gold, Medtronic | 246 (20) | 17.6 | 66.3 | 32.5 | 0.0 | 1.2 | 0.0 | Arterial | |||||
| Branco et al., 2010 | CGMS System Gold, Medtronic | 34 (14) | 23.0 | 53.0 | 47.0 | 0.0 | Arterial | |||||||
| Bridges et al., 2010 | Guardian REAL-Time, Medtronic | 1555 (47) | 15.3 | 74.6 | 23.3 | 2.1 | 0.0 | −1.5 (−59.5 to 56.5) | Unknown | |||||
| Phrabhudesai et al., 2015 | Guardian REAL-Time, Medtronic (Enlite sensor) | 235 (19) | 17.3 * | 66.0 | 28.5 | 0.0 | 7.2 | 0.0 | −5.1 (−76.8 to 66.6) | Unknown | ||||
| Findings | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author Year | CGM System | N a | MARD b (%) | ISO c (%) | Clark Error Grid d (% in Zones A–E) | Bland-Altman e (mg/dL) | Target Range ICU f (mg/dL) | Reference Sample | ||||||
| A | B | C | D | E | ||||||||||
| Schierenbeck et al., 2016 | Eirus System, Maquet Critical Care * | 514 (26) | 6.5 | ±8.2 | 90.0 | 94.0 | 6.0 | 0.0 | 0.9 (−27.0 to 29.0) | 80–149 | Arterial or venous | |||
| Nohra et al., 2016 | Optiscanner 5000, Optiscan | 347 (24) | 8.0 | (7.3–8.7) | 94.8 | 5.2 | 0.0 | −5 (−28 to 18) | Unknown | |||||
| Leopold et al., 2016 | Eirus System, Maquet Critical Care | 594 (12) | 7.5 | 93.6 | 93.6 | 6.4 | 0.0 | 4.1 (−20.5 to 28.6) | 90–144 | Arterial | ||||
| Strasma et al., 2015 | Glucath, Medtronic | 1799 (70) | Arterial sensor | 9.6 | 89.4 | −2.1 (−34.5 to 29.6) | 100–180 | Arterial or central venous | ||||||
| 1799 (70) | Venous sensor | 14.2 | 72.2 | −6.5 (−53.8 to 39.8) | ||||||||||
| Macken et al., 2015 | GluCath, Medtronic | 758 (20) | 6.4 | 97.0 | −10.8 (−466.2 to 446.4) | Arterial | ||||||||
| Crane et al., 2015 | GlySure, GlySure | (33) | Cardiac surg. patients | 9.9 | 88.2 | 11.8 | Venous | |||||||
| (14) | General patient | 8.0 | 95.0 | 5.0 | ||||||||||
| Bochiccio et al., 2015 | IVBG System, Edwards Lifesciences | 996 (100) | 8.2 | ±10.5 | 93.3 | 93.2 | 5.8 | 0.2 | 0.8 | 0.0 | Arterial or venous | |||
| Foubert et al., 2014 | GlucoClear, Edwards Lifesciences | 1093 (10) | 5.1 | 99.4 | 99.4 | 0.6 | 0.0 | −3 (−15.6 to 9.6) | 80–110 | Venous | ||||
| Flower et al., 2014 | GluCath, Medtronic | 437 (21) | 13.0 | 80.8 | −5.8 (−54.5 to 42.9) | Arterial | ||||||||
| Schierenbeck et al., 2013 | Eirus System, Maquet Critical Care | 607 (30) | 5.6 | 97.2 | 97.0 | 3.0 | 0.0 | −2.2 (−14.8 to 10.5) | Arterial | |||||
| Schierenbeck et al., 2012 | Eirus System, Maquet Critical Care | 994 (50) | 5.0 | 99.2 | 99.0 | 1.0 | 0.0 | 0.4 (−19.5 to 22.0) | Arterial and venous | |||||
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Steen, S.C.J.; Rijkenberg, S.; Limpens, J.; Van der Voort, P.H.J.; Hermanides, J.; DeVries, J.H. The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients—A Systematic Scoping Review. Sensors 2017, 17, 146. https://doi.org/10.3390/s17010146
Van Steen SCJ, Rijkenberg S, Limpens J, Van der Voort PHJ, Hermanides J, DeVries JH. The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients—A Systematic Scoping Review. Sensors. 2017; 17(1):146. https://doi.org/10.3390/s17010146
Chicago/Turabian StyleVan Steen, Sigrid C. J., Saskia Rijkenberg, Jacqueline Limpens, Peter H. J. Van der Voort, Jeroen Hermanides, and J. Hans DeVries. 2017. "The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients—A Systematic Scoping Review" Sensors 17, no. 1: 146. https://doi.org/10.3390/s17010146
APA StyleVan Steen, S. C. J., Rijkenberg, S., Limpens, J., Van der Voort, P. H. J., Hermanides, J., & DeVries, J. H. (2017). The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients—A Systematic Scoping Review. Sensors, 17(1), 146. https://doi.org/10.3390/s17010146