
Targeting the Ischemic Core: A Therapeutic Microdialytic Approach to Prevent Neuronal Death and Restore Functional Behaviors

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
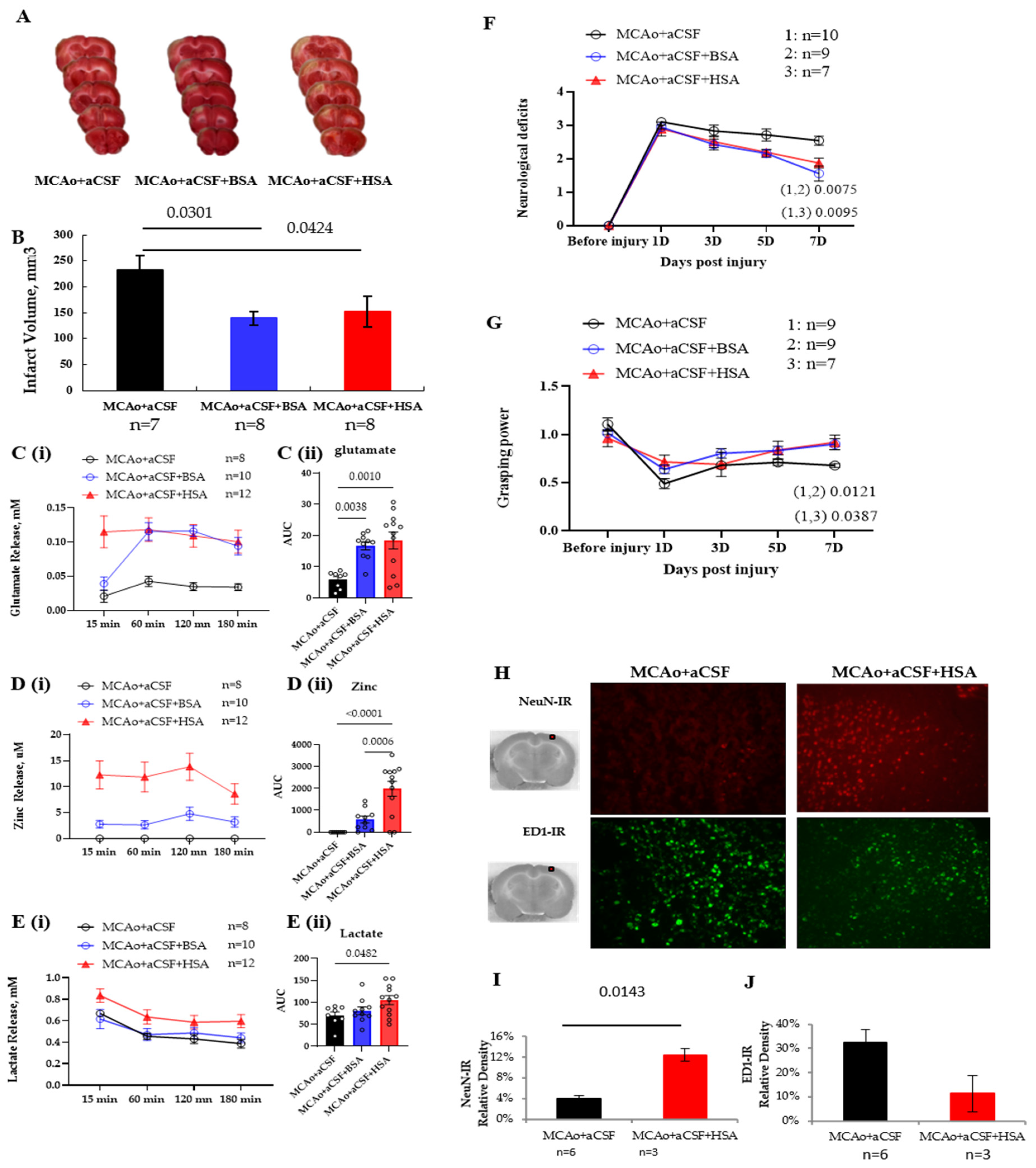
2.1. Enhancement of Brain Damage and Motor Deficits by Stroke and Its Reduction by Microdialysis with Bovine Serum Albumin (BSA)
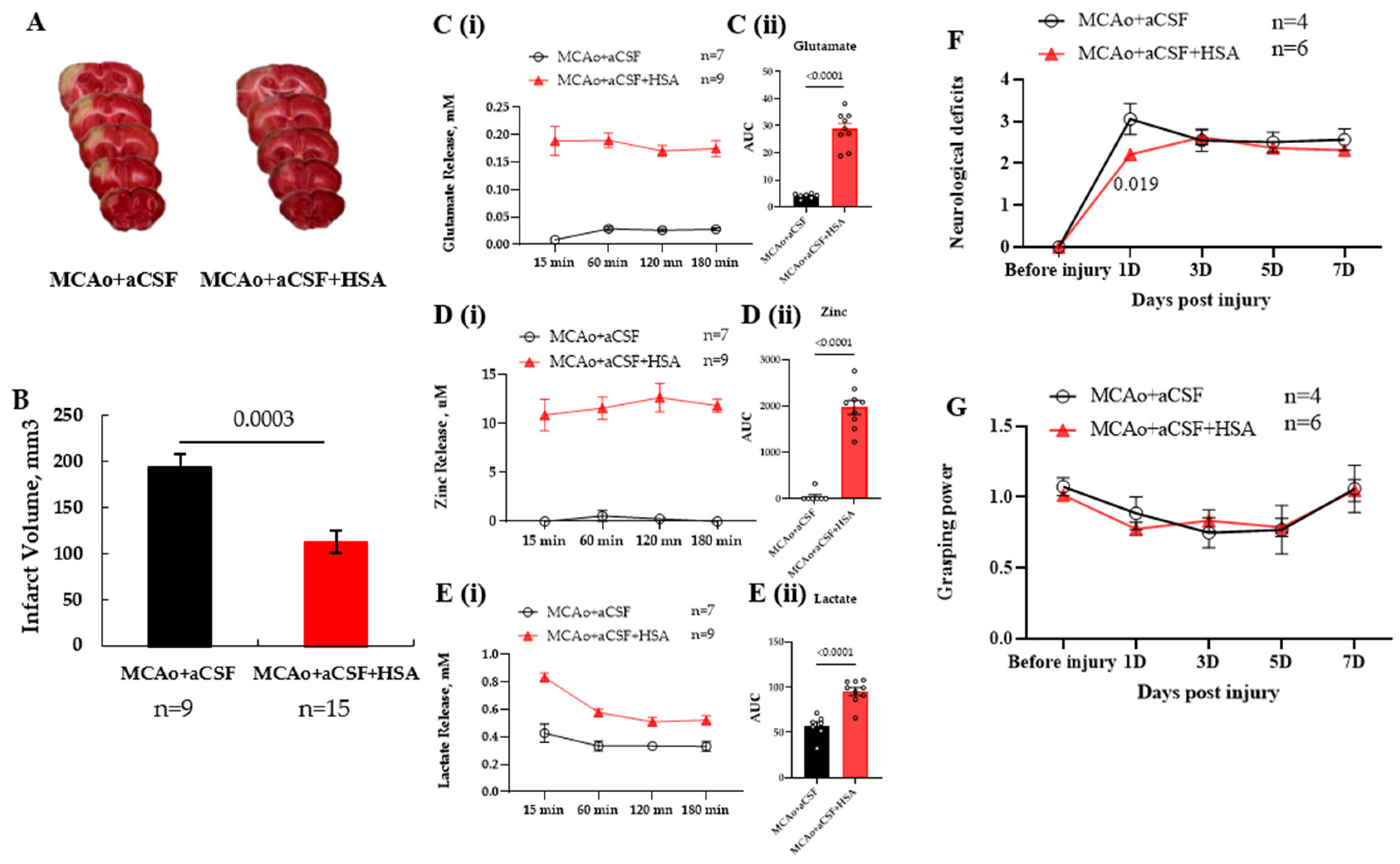
2.2. HSA Is as Effective as BSA in Working as an Oncotic Agent for tMD in MCAo Rats
2.3. Protective Effect of tMD at the Golden 6th Hour Post-Ischemic Injury
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Surgical Procedure and Treatment
4.3. Neurological Deficit Score (NSD) Test
4.4. Grasping Power Test
4.5. Morphological Analysis
4.6. Western Blot Analysis
4.7. Biochemical Assays
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kriz, J.; Lalancette-Hebert, M. Inflammation, plasticity and real-time imaging after cerebral ischemia. Acta Neuropathol. 2009, 117, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Owolabi, M.O.; World Stroke Organization-Lancet Neurology Commission Stroke Collaboration Group. Pragmatic solutions to reduce the global burden of stroke: A World Stroke Organization-Lancet Neurology Commission. Lancet Neurol. 2023, 22, 1160–1206. [Google Scholar] [CrossRef] [PubMed]
- Prust, M.L.; Forman, R.; Ovbiagele, B. Addressing disparities in the global epidemiology of stroke. Nat. Rev. Neurol. 2024, 20, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, S.J.; Prabhakaran, S. Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review. JAMA 2021, 325, 1088–1098. [Google Scholar] [CrossRef]
- Kong, J.; Zhang, D. Current status and quality of radiomics studies for predicting outcome in acute ischemic stroke patients: A systematic review and meta-analysis. Front. Neurol. 2023, 14, 1335851. [Google Scholar] [CrossRef]
- Nozohouri, S.; Sifat, A.E.; Vaidya, B.; Abbruscato, T.J. Novel approaches for the delivery of therapeutics in ischemic stroke. Drug Discov. Today 2020, 25, 535–551. [Google Scholar] [CrossRef]
- Owjfard, M.; Rahimian, Z.; Karimi, F.; Borhani-Haghighi, A.; Mallahzadeh, A. A comprehensive review on the neuroprotective potential of resveratrol in ischemic stroke. Heliyon 2024, 10, e34121. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Q.; Shang, H.; Li, J.; Chai, H.; Wang, K.; Guo, Z.; Luo, T.; Liu, S.; Liu, Y.; et al. Potential application of natural compounds in ischaemic stroke: Focusing on the mechanisms underlying “lysosomocentric” dysfunction of the autophagy-lysosomal pathway. Pharmacol. Ther. 2024, 263, 108721. [Google Scholar] [CrossRef]
- Pawluk, H.; Tafelska-Kaczmarek, A.; Soponska, M.; Porzych, M.; Modrzejewska, M.; Pawluk, M.; Kurhaluk, N.; Tkaczenko, H.; Kolodziejska, R. The Influence of Oxidative Stress Markers in Patients with Ischemic Stroke. Biomolecules 2024, 14, 1130. [Google Scholar] [CrossRef]
- Luo, Z.; Zhou, Y.; He, Y.; Yan, S.; Chen, Z.; Zhang, X.; Chen, Y.; Tong, L.S.; Zhong, W.; Hu, H.; et al. Treatment with intravenous alteplase in ischaemic stroke patients with onset time between 4.5 and 24 hours (HOPE): Protocol for a randomised, controlled, multicentre study. Stroke Vasc. Neurol. 2024, 9, 318–323. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Davalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Saini, V.; Guada, L.; Yavagal, D.R. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology 2021, 97, S6–S16. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, C.; Delgado, P.; Vilches, A.; Martin-Gallan, P.; Ribo, M.; Santamarina, E.; Molina, C.; Corbeto, N.; Rodriguez-Sureda, V.; Rosell, A.; et al. Oxidative stress after thrombolysis-induced reperfusion in human stroke. Stroke 2010, 41, 653–660. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Wang, Y.; Fang, C.; Feng, Z.; Yin, M.; Huang, J.; Ma, Y.; Mo, Z. Advancing stroke therapy: A deep dive into early phase of ischemic stroke and recanalization. CNS Neurosci. Ther. 2024, 30, e14634. [Google Scholar] [CrossRef]
- Qin, C.; Yang, S.; Chu, Y.H.; Zhang, H.; Pang, X.W.; Chen, L.; Zhou, L.Q.; Chen, M.; Tian, D.S.; Wang, W. Signaling pathways involved in ischemic stroke: Molecular mechanisms and therapeutic interventions. Signal Transduct. Target. Ther. 2022, 7, 215. [Google Scholar] [CrossRef]
- Belayev, L.; Liu, Y.; Zhao, W.; Busto, R.; Ginsberg, M.D. Human albumin therapy of acute ischemic stroke: Marked neuroprotective efficacy at moderate doses and with a broad therapeutic window. Stroke 2001, 32, 553–560. [Google Scholar] [CrossRef]
- Liu, Y.; Belayev, L.; Zhao, W.; Busto, R.; Belayev, A.; Ginsberg, M.D. Neuroprotective effect of treatment with human albumin in permanent focal cerebral ischemia: Histopathology and cortical perfusion studies. Eur. J. Pharmacol. 2001, 428, 193–201. [Google Scholar] [CrossRef]
- Khatri, R.; Afzal, M.R.; Rodriguez, G.J.; Maud, A.; Miran, M.S.; Qureshi, M.A.; Cruz-Flores, S.; Qureshi, A.I. Albumin-Induced Neuroprotection in Focal Cerebral Ischemia in the ALIAS Trial: Does Severity, Mechanism, and Time of Infusion Matter? Neurocrit Care 2018, 28, 60–64. [Google Scholar] [CrossRef]
- Huang, Y.; Xiao, Z. Albumin therapy for acute ischemic stroke: A meta-analysis. Neurol. Sci. 2021, 42, 2713–2719. [Google Scholar] [CrossRef]
- Martin, R.H.; Yeatts, S.D.; Hill, M.D.; Moy, C.S.; Ginsberg, M.D.; Palesch, Y.Y.; Parts, A.; Investigators, N. ALIAS (Albumin in Acute Ischemic Stroke) Trials: Analysis of the Combined Data from Parts 1 and 2. Stroke 2016, 47, 2355–2359. [Google Scholar] [CrossRef] [PubMed]
- Charron, B.; Delorme, A.; Dubois, C.; Hojjat Jodaylami, M.; Masson, J.F. Influence of bovine and human serum albumin on the binding kinetics of biomolecular interactions. Analyst 2023, 148, 5525–5533. [Google Scholar] [CrossRef] [PubMed]
- Rahman, N.; Khalil, N. Characterization of sulfasalazine-bovine serum albumin and human serum albumin interaction by spectroscopic and theoretical approach. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2023, 300, 122865. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, M.A.; Lo, E.H.; Iadecola, C. The science of stroke: Mechanisms in search of treatments. Neuron 2010, 67, 181–198. [Google Scholar] [CrossRef]
- Vandelanotte, S.; De Meyer, S.F. Acute Ischemic Stroke Thrombus Composition. Neuroscience 2024, 550, 11–20. [Google Scholar] [CrossRef]
- Ginsberg, M.D.; Belayev, L.; Zhao, W.; Huh, P.W.; Busto, R. The acute ischemic penumbra: Topography, life span, and therapeutic response. Acta Neurochir. Suppl. 1999, 73, 45–50. [Google Scholar]
- Choi, D.W. Excitotoxic cell death. J. Neurobiol. 1992, 23, 1261–1276. [Google Scholar] [CrossRef]
- Hazell, A.S. Excitotoxic mechanisms in stroke: An update of concepts and treatment strategies. Neurochem. Int. 2007, 50, 941–953. [Google Scholar] [CrossRef]
- Obrenovitch, T.P.; Urenjak, J. Is high extracellular glutamate the key to excitotoxicity in traumatic brain injury? J. Neurotrauma 1997, 14, 677–698. [Google Scholar] [CrossRef]
- Neves, D.; Salazar, I.L.; Almeida, R.D.; Silva, R.M. Molecular mechanisms of ischemia and glutamate excitotoxicity. Life Sci. 2023, 328, 121814. [Google Scholar] [CrossRef]
- Kaplan-Arabaci, O.; Acari, A.; Ciftci, P.; Gozuacik, D. Glutamate Scavenging as a Neuroreparative Strategy in Ischemic Stroke. Front. Pharmacol. 2022, 13, 866738. [Google Scholar] [CrossRef] [PubMed]
- Frederickson, C.J.; Giblin, L.J., III; Balaji, R.V.; Masalha, R.; Frederickson, C.J.; Zeng, Y.; Lopez, E.V.; Koh, J.-Y.; Chorin, U.; Besser, L.; et al. Synaptic release of zinc from brain slices: Factors governing release, imaging, and accurate calculation of concentration. J. Neurosci. Methods 2006, 154, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Zipfel, G.J.; Park, K.H.; He, Y.Y.; Hsu, C.Y.; Choi, D.W. Zinc translocation accelerates infarction after mild transient focal ischemia. Neuroscience 2002, 115, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Rosso, C.; Samson, Y. The ischemic penumbra: The location rather than the volume of recovery determines outcome. Curr. Opin. Neurol. 2014, 27, 35–41. [Google Scholar] [CrossRef]
- Trickler, W.J.; Miller, D.W. Use of osmotic agents in microdialysis studies to improve the recovery of macromolecules. J. Pharm. Sci. 2003, 92, 1419–1427. [Google Scholar] [CrossRef]
- Cheng, H.; Huang, S.S.; Lin, S.M.; Lin, M.J.; Chu, Y.C.; Chih, C.L.; Tsai, M.J.; Lin, H.C.; Huang, W.C.; Tsai, S.K. The neuroprotective effect of glial cell line-derived neurotrophic factor in fibrin glue against chronic focal cerebral ischemia in conscious rats. Brain Res. 2005, 1033, 28–33. [Google Scholar] [CrossRef]
- Tsai, M.J.; Tsai, S.K.; Huang, M.C.; Liou, D.Y.; Huang, S.L.; Hsieh, W.H.; Huang, W.C.; Huang, S.S.; Cheng, H. Acidic FGF promotes neurite outgrowth of cortical neurons and improves neuroprotective effect in a cerebral ischemic rat model. Neuroscience 2015, 305, 238–247. [Google Scholar] [CrossRef]
- Tsai, M.J.; Weng, C.F.; Shyue, S.K.; Liou, D.Y.; Chen, C.H.; Chiu, C.W.; Yang, T.H.; Pan, H.A.; Liao, R.I.; Kuo, H.S.; et al. Dual effect of adenovirus-mediated transfer of BMP7 in mixed neuron-glial cultures: Neuroprotection and cellular differentiation. J. Neurosci. Res. 2007, 85, 2950–2959. [Google Scholar] [CrossRef]
- Tsai, S.K.; Hung, L.M.; Fu, Y.T.; Cheng, H.; Nien, M.W.; Liu, H.Y.; Zhang, F.B.; Huang, S.S. Resveratrol neuroprotective effects during focal cerebral ischemia injury via nitric oxide mechanism in rats. J. Vasc. Surg. 2007, 46, 346–353. [Google Scholar] [CrossRef]
- Huang, S.S.; Cheng, H.; Tang, C.M.; Nien, M.W.; Huang, Y.S.; Lee, I.H.; Yin, J.H.; Kuo, T.B.; Yang, C.C.; Tsai, S.K.; et al. Anti-oxidative, anti-apoptotic, and pro-angiogenic effects mediate functional improvement by sonic hedgehog against focal cerebral ischemia in rats. Exp. Neurol. 2013, 247, 680–688. [Google Scholar] [CrossRef]
- Menzies, S.A.; Hoff, J.T.; Betz, A.L. Middle cerebral artery occlusion in rats: A neurological and pathological evaluation of a reproducible model. Neurosurgery 1992, 31, 100–106; discussion 106–107. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.J.; Tsai, S.K.; Hu, B.R.; Liou, D.Y.; Huang, S.L.; Huang, M.C.; Huang, W.C.; Cheng, H.; Huang, S.S. Recovery of neurological function of ischemic stroke by application of conditioned medium of bone marrow mesenchymal stem cells derived from normal and cerebral ischemia rats. J. Biomed. Sci. 2014, 21, 5. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.J.; Weng, C.F.; Yu, N.C.; Liou, D.Y.; Kuo, F.S.; Huang, M.C.; Huang, W.C.; Tam, K.; Shyue, S.K.; Cheng, H. Enhanced prostacyclin synthesis by adenoviral gene transfer reduced glial activation and ameliorated dopaminergic dysfunction in hemiparkinsonian rats. Oxid. Med. Cell Longev. 2013, 2013, 649809. [Google Scholar] [CrossRef]
- Tsai, M.J.; Liao, J.F.; Lin, D.Y.; Huang, M.C.; Liou, D.Y.; Yang, H.C.; Lee, H.J.; Chen, Y.T.; Chi, C.W.; Huang, W.C.; et al. Silymarin protects spinal cord and cortical cells against oxidative stress and lipopolysaccharide stimulation. Neurochem. Int. 2010, 57, 867–875. [Google Scholar] [CrossRef]
- Tsai, M.J.; Shyue, S.K.; Weng, C.F.; Chung, Y.; Liou, D.Y.; Huang, C.T.; Kuo, H.S.; Lee, M.J.; Chang, P.T.; Huang, M.C.; et al. Effect of enhanced prostacyclin synthesis by adenovirus-mediated transfer on lipopolysaccharide stimulation in neuron-glia cultures. Ann. N. Y. Acad. Sci. 2005, 1042, 338–348. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-J.; Liou, D.-Y.; Fay, L.-Y.; Huang, S.-L.; Huang, W.-C.; Chern, C.-M.; Tsai, S.-K.; Cheng, H.; Huang, S.-S. Targeting the Ischemic Core: A Therapeutic Microdialytic Approach to Prevent Neuronal Death and Restore Functional Behaviors. Int. J. Mol. Sci. 2025, 26, 3821. https://doi.org/10.3390/ijms26083821
Tsai M-J, Liou D-Y, Fay L-Y, Huang S-L, Huang W-C, Chern C-M, Tsai S-K, Cheng H, Huang S-S. Targeting the Ischemic Core: A Therapeutic Microdialytic Approach to Prevent Neuronal Death and Restore Functional Behaviors. International Journal of Molecular Sciences. 2025; 26(8):3821. https://doi.org/10.3390/ijms26083821
Chicago/Turabian StyleTsai, May-Jywan, Dann-Ying Liou, Li-Yu Fay, Shih-Ling Huang, Wen-Cheng Huang, Chang-Ming Chern, Shen-Kou Tsai, Henrich Cheng, and Shiang-Suo Huang. 2025. "Targeting the Ischemic Core: A Therapeutic Microdialytic Approach to Prevent Neuronal Death and Restore Functional Behaviors" International Journal of Molecular Sciences 26, no. 8: 3821. https://doi.org/10.3390/ijms26083821
APA StyleTsai, M.-J., Liou, D.-Y., Fay, L.-Y., Huang, S.-L., Huang, W.-C., Chern, C.-M., Tsai, S.-K., Cheng, H., & Huang, S.-S. (2025). Targeting the Ischemic Core: A Therapeutic Microdialytic Approach to Prevent Neuronal Death and Restore Functional Behaviors. International Journal of Molecular Sciences, 26(8), 3821. https://doi.org/10.3390/ijms26083821