1. Introduction
Osteosarcoma is a primary malignant bone tumor characterized by the production of immature bone, also known as osteoids, by mesenchymal cells. It is among the most common bone cancers, predominantly affecting adolescents and older adults (≥65 years) [
1]. Osteosarcoma presents a significant clinical challenge owing to its high metastatic potential and recurrence rates. At diagnosis, approximately 20% of patients exhibit detectable metastases, whereas over 80% harbor micrometastases [
2]. Historically, the 5-year survival rate for patients undergoing surgery alone was approximately 20%. However, the introduction of adjuvant chemotherapy and advancements in surgical techniques has improved survival rates to 60–70% [
3]. Despite these advancements, survival outcomes have plateaued over the past three decades, with patients with metastatic osteosarcoma facing a dismal 5-year survival rate of less than 30%, emphasizing the urgent need for novel therapeutic strategies [
3]. The current standard of care involves a multimodal approach, combining surgery with multi-agent chemotherapy, typically administered in neoadjuvant and adjuvant settings [
4]. However, conventional chemotherapy often fails to provide durable responses due to chemoresistance, and high-dose regimens are associated with severe toxicities such as neutropenia, infections, and thrombocytopenia [
3]. Thus, identifying alternative or adjunctive therapies that enhance efficacy while minimizing side effects is crucial [
4].
One promising avenue involves combining doxorubicin (doxo), a first-line anthracycline chemotherapeutic agent, with histone deacetylase (HDAC) inhibitors [
5,
6]. Although doxo remains a cornerstone of osteosarcoma treatment, its clinical utility is hindered by dose-limiting toxicities, particularly cardiotoxicity, necessitating strategies to reduce cumulative doses without compromising efficacy [
7]. Additionally, acquired resistance to doxo poses a major obstacle. Studies on doxo-resistant osteosarcoma cells have identified key molecular alterations that may serve as therapeutic targets to overcome resistance [
7].
Epigenetic modifications, particularly those mediated by HDACs, play pivotal roles in the pathogenesis and chemoresistance of osteosarcoma. HDAC inhibitors restore normal gene expression by blocking HDAC enzymes, thereby sensitizing cancer cells to chemotherapy. In osteosarcoma, HDAC inhibitors can enhance doxo efficacy by promoting apoptosis, disrupting cell cycle regulation, and inhibiting DNA repair mechanisms. Notably, HDAC inhibitors downregulate DNA repair proteins, such as poly [ADP-ribose] polymerase 1, thereby impairing tumor cell survival under chemotherapeutic stress [
5]. These findings suggest that targeting epigenetic pathways through HDAC inhibition could help overcome drug resistance and improve therapeutic outcomes [
5,
6]. Consequently, this study focused on the roles of HDAC4 and HDAC8 in osteosarcoma progression.
HDAC4 is a key regulator of gene transcription, cell proliferation, and cell survival. Its aberrant expression has been implicated in tumor progression across various cancers, and its overexpression is associated with higher tumor grades, advanced clinical stages, and poor prognosis. For instance, HDAC4 promotes metastasis in esophageal carcinoma and supports cell survival [
8]. In osteosarcoma, HDAC4 is highly expressed and contributes to tumor development by modulating proliferation, invasion, and apoptosis [
9]. However, paradoxically, its overexpression may counteract certain anti-cancer effects [
10]. Despite these insights, the precise role of HDAC4 in osteosarcoma remains poorly defined, necessitating further investigation into its expression and function in osteosarcoma tissues. HDAC8 is increasingly recognized for its role in tumorigenesis. Elevated HDAC8 expression has been reported in hepatocellular carcinoma, where it promotes tumor growth and confers resistance to chemotherapy [
11]. HDAC8 inhibition enhances sensitivity to doxo [
12], whereas in colon cancer, HDAC8 represses pro-apoptotic genes and activates Jak2/Stat signaling [
13]. It demonstrates anti-cancer effects by impairing melanoma cell proliferation and migration [
14]. HDAC8 is involved in key oncogenic processes, including proliferation, metastasis, immune evasion, and drug resistance [
15]. The combination of doxo with HDAC inhibitors offers a promising strategy to improve osteosarcoma treatment outcomes. By modulating epigenetic mechanisms, HDAC inhibitors can enhance chemotherapy sensitivity, inhibit tumor growth, and reduce metastatic potential. This approach not only aims to increase treatment efficacy but also seeks to mitigate the toxic side effects associated with high-dose chemotherapy. We hypothesize that combining doxo with tasquinimod (Tas), an HDAC4 inhibitor, and PCI, an HDAC8 inhibitor, will synergistically enhance apoptosis and suppress cell proliferation, even at reduced doxo doses. Specifically, we aim to restore doxo sensitivity in osteosarcoma cells by disrupting survival pathways and promoting apoptosis. To assess therapeutic potential, we will utilize the SJSA-1 osteosarcoma cell line, known for its aggressive phenotype, high tumorigenic potential, and metastatic capability, making it an ideal model for evaluating novel therapeutic strategies [
16]. This study investigates the therapeutic potential of combining doxo with HDAC inhibitors, specifically Tas, an HDAC4 inhibitor, and PCI, a selective HDAC8 inhibitor, in osteosarcoma treatment. Given the significant role of HDACs in tumor progression, metastasis, and drug resistance, we hypothesize that targeting HDAC4 and HDAC8 will enhance doxo sensitivity, promote apoptosis, and inhibit tumor growth. By employing both 2D and 3D in vitro models using the aggressive SJSA-1 osteosarcoma cell line, we aim to elucidate the molecular mechanisms underlying this combination therapy, focusing on the protein kinase B (pAKT) and runt-related transcription factor 2 (RUNX2) signaling pathway. Through evaluating cell viability, apoptosis induction, migration inhibition, and molecular pathway alterations, this study seeks to provide compelling evidence that HDAC inhibition can overcome doxo resistance and enhance treatment efficacy.
3. Discussion
Doxorubicin (doxo) remains a cornerstone chemotherapeutic agent for osteosarcoma because of its potent cytotoxic effects, which are primarily mediated by DNA intercalation and the inhibition of nucleic acid synthesis. Additionally, doxo disrupts mitochondrial function by targeting the electron transport chain and oxidative phosphorylation, leading to increased oxidative stress and apoptosis in cancer cells [
7,
17]. However, despite its efficacy, the clinical application of doxo is significantly hindered by dose-dependent cardiotoxicity and the emergence of drug resistance, particularly in pediatric patients. This necessitates the development of novel therapeutic strategies that enhance anti-tumor efficacy while minimizing adverse effects [
7]. In this context, the combination of doxo and histone deacetylase (HDAC) inhibitors represents a promising avenue for optimizing osteosarcoma treatment by targeting complementary oncogenic pathways. To contextualize our findings, we compiled a summary of doxorubicin-based combination strategies reported in the literature (
Table 1), highlighting the approaches to enhance doxo efficacy through synergistic mechanisms.
HDACs are critical regulators of key cellular processes, including cell cycle progression, apoptosis, and metastasis, making them attractive therapeutic targets in oncology. Among the HDAC family, HDAC4 and HDAC8 have gained significant attention because of their distinct roles in tumor biology [
10,
18]. HDAC4 has been implicated in osteosarcoma progression by promoting chemoresistance and enhancing cell survival, underscoring its relevance as a therapeutic target [
10]. In contrast, HDAC8 has been shown to facilitate tumor proliferation, metastasis, and immune evasion in multiple cancer types, although its precise role in osteosarcoma remains unclear, necessitating further investigation [
11,
12,
13].
Given these considerations, this study aimed to evaluate the therapeutic potential of targeting HDAC4 and HDAC8 using their specific inhibitors, tasquinimod (Tas) and PCI-34051 (PCI). Both Tas and PCI have demonstrated potent anti-cancer activity in preclinical models, with Tas effectively reducing cancer cell invasiveness and metastatic progression, leading to improved survival outcomes [
20]. Meanwhile, PCI, a highly selective HDAC8 inhibitor, exhibits remarkable specificity, with a 4200-fold preference for HDAC8 over other HDACs, making it a compelling candidate for targeted therapy [
11,
12,
13]. While broad-spectrum HDAC inhibitors, such as romidepsin and panobinostat, have been shown to exert anti-proliferative effects against osteosarcoma [
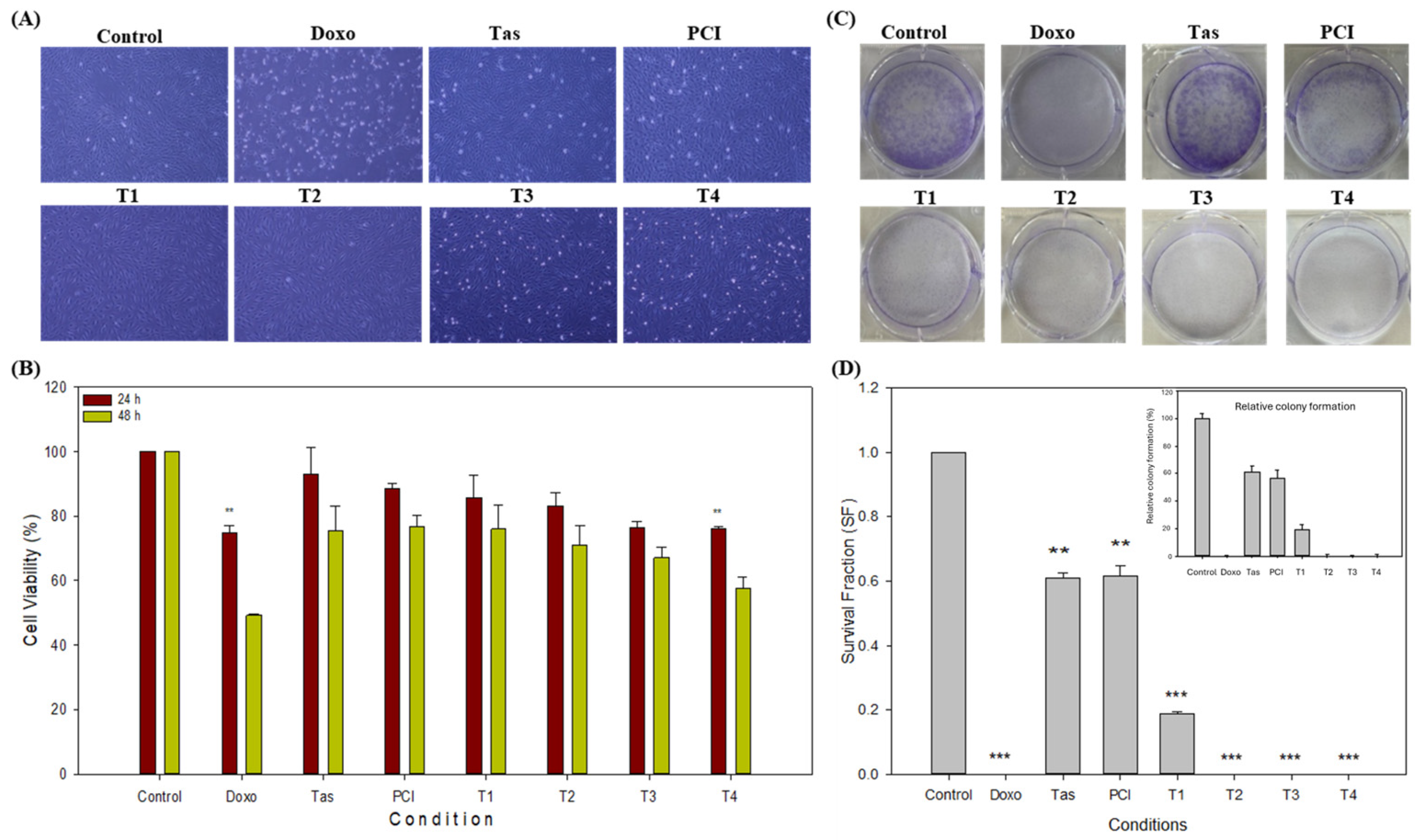
21], the specific application of Tas and PCI, particularly in combination with doxo, remains largely unexplored. Thus, this study systematically assessed the anti-tumor efficacy of doxo, Tas, and PCI, both individually and in combination, to determine their potential for synergistic interactions in enhancing osteosarcoma treatment, and it has demonstrated that the combination of doxo with Tas and PCI exerts a synergistic inhibitory effect on osteosarcoma cell proliferation, as evidenced by a pronounced reduction in cell density, morphological alterations, and increased cell death. Microscopic examination of the treated cells revealed significant changes, including cellular shrinkage and detachment, particularly in the combination treatment groups. Functional assays further substantiated these observations. While neither Tas nor PCI alone significantly inhibited osteosarcoma cell proliferation, their combination with doxo markedly enhanced anti-tumor activity, as demonstrated by the CCK-8 assay. The colony formation assay provided additional support, showing a substantial reduction in colony-forming potential, with the T3 and T4 treatment groups exhibiting complete inhibition of colony formation, comparable to that of doxo monotherapy. The pronounced decline in colony numbers, particularly in the doxorubicin (doxo), T2, T3, and T4 groups, suggests a strong cytotoxic effect, leading to the near-complete inhibition of long-term cell survival. This is consistent with previous results indicating that chemotherapeutic agents and epigenetic modulators, such as HDAC inhibitors, can suppress osteosarcoma proliferation by disrupting key survival pathways. Interestingly, the Tas and PCI treatments retained a moderate colony-forming ability, indicating a partial inhibitory effect, which could be linked to mechanisms such as residual RUNX2/PI3K/AKT signaling or metabolic adaptation. The significant reduction in clonogenic survival at T1 and T2 further supports the hypothesis that targeted interventions affecting both proliferation and survival signaling pathways could enhance therapeutic efficacy. These findings highlight the potential of combination strategies, particularly those involving HDAC inhibitors and metabolic modulators, to improve osteosarcoma treatment outcomes.
Interestingly, PCI demonstrated superior anti-proliferative efficacy compared to Tas, consistent with previous studies indicating PCI’s ability to enhance acetyl-p53 (K381) in a dose-dependent manner, thereby suppressing tumor growth [
18]. Our results align with the existing literature suggesting that selective HDAC inhibitors sensitize osteosarcoma cells to chemotherapy by reducing proliferation and inducing apoptosis [
5]. Importantly, our cytotoxicity assessment in normal human cells indicated that Tas and PCI exerted minimal toxicity, with no significant effects on cell viability or morphology. Notably, Tas and PCI appeared to promote tenocyte growth, suggesting their potential biocompatibility and safety for therapeutic applications (
Supplementary Figure S1A,B).
Apoptosis, a fundamental mechanism for maintaining cellular homeostasis, is tightly regulated through intrinsic and extrinsic pathways, both of which converge on the activation of caspase-3, a key effector of programmed cell death [
22]. The extrinsic apoptotic pathway, mediated through caspase-8 activation, plays a crucial role in Fas-associated death domain recruitment and formation of the death-inducing signaling complex [
23].
Previous studies have demonstrated that HDAC inhibition enhances chemotherapy-induced apoptosis by modulating apoptotic signaling cascades. Specifically, silencing HDAC4 has been shown to potentiate cisplatin-induced apoptosis by upregulating pro-apoptotic genes such as BIK in a p53-dependent manner [
24]. Additionally, PCI, when combined with other agents such as ACY-241, suppresses cell proliferation, promotes apoptosis, and downregulates key anti-apoptotic and metastasis-associated proteins [
18]. Similarly, targeted HDAC8 inhibition sensitizes cancer cells to chemotherapy by suppressing the multidrug resistance gene MDR1 [
11].
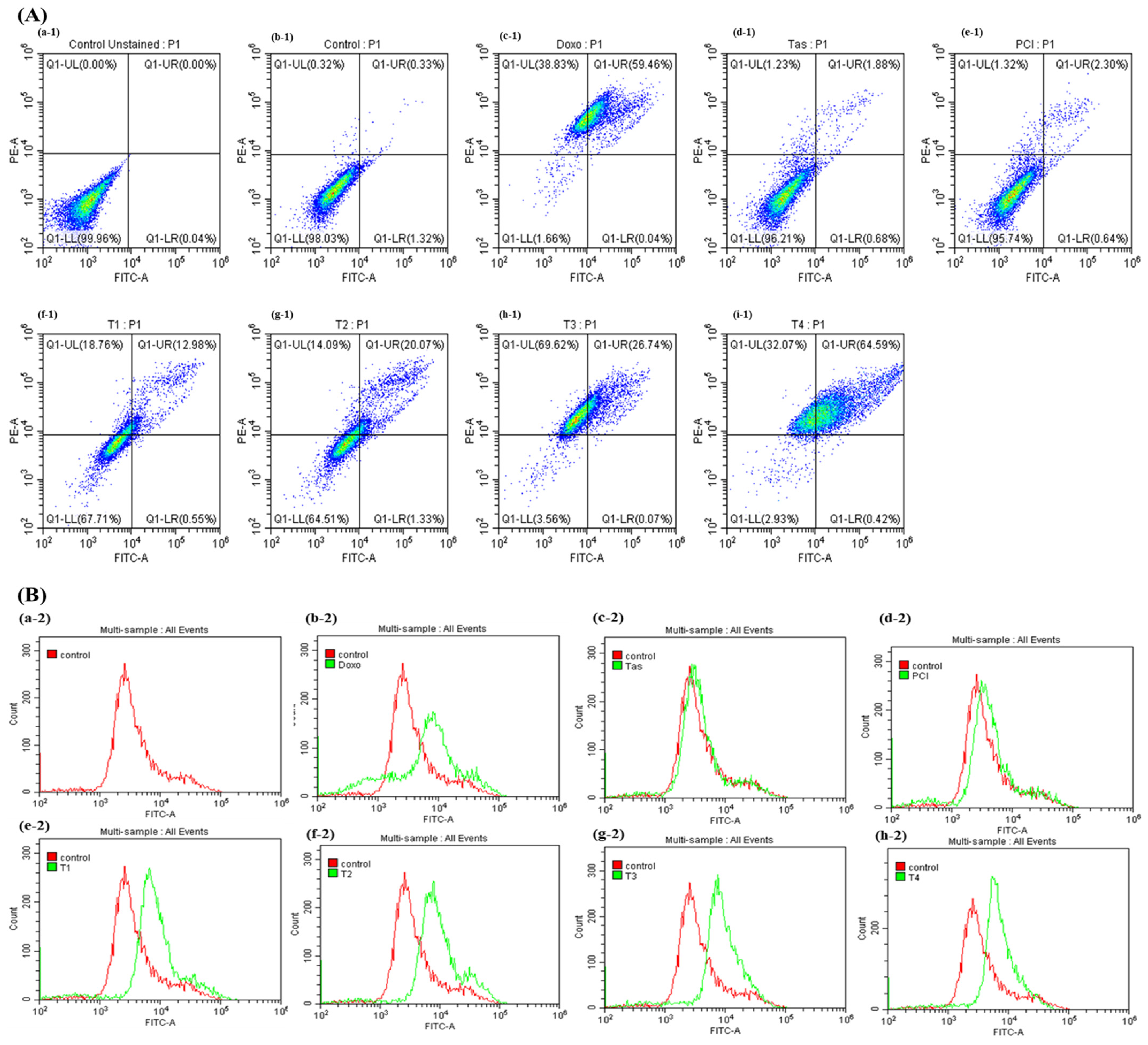
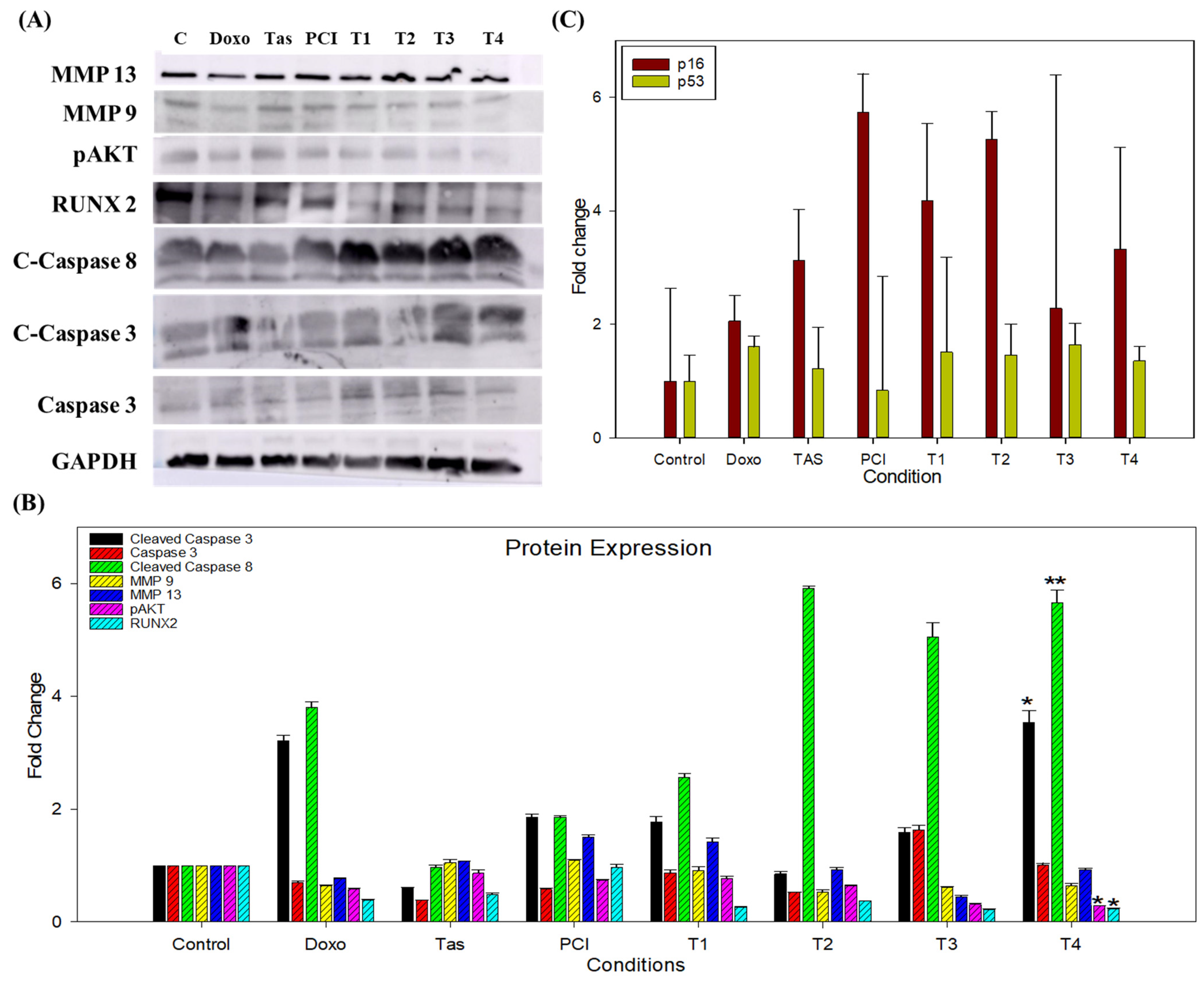
Consistent with these findings, our study demonstrated that the combination of Tas and PCI significantly increased the levels of cleaved-caspase-3 and cleaved-caspase-8 in the T3 and T4 treatment groups, indicating the activation of both intrinsic and extrinsic apoptotic pathways. Caspase-3/7 activity was markedly elevated in these treatment groups, reinforcing the role of HDAC inhibition in facilitating apoptosis via mitochondrial and death-receptor-mediated mechanisms. Notably, this combination therapy exhibited minimal cytotoxicity to normal human cells, further supporting its therapeutic potential.
Metastasis remains a major challenge in osteosarcoma treatment, with epithelial–mesenchymal transition (EMT) playing a pivotal role in tumor invasion and dissemination. MMPs, particularly MMP9 and MMP13, facilitate ECM degradation, thereby promoting metastatic progression. HDAC4 has been identified as a key regulator of EMT, and its overexpression enhances tumor invasiveness in various cancers [
25]. Similarly, HDAC8 has been implicated in colorectal cancer metastasis and melanoma brain invasion [
26].
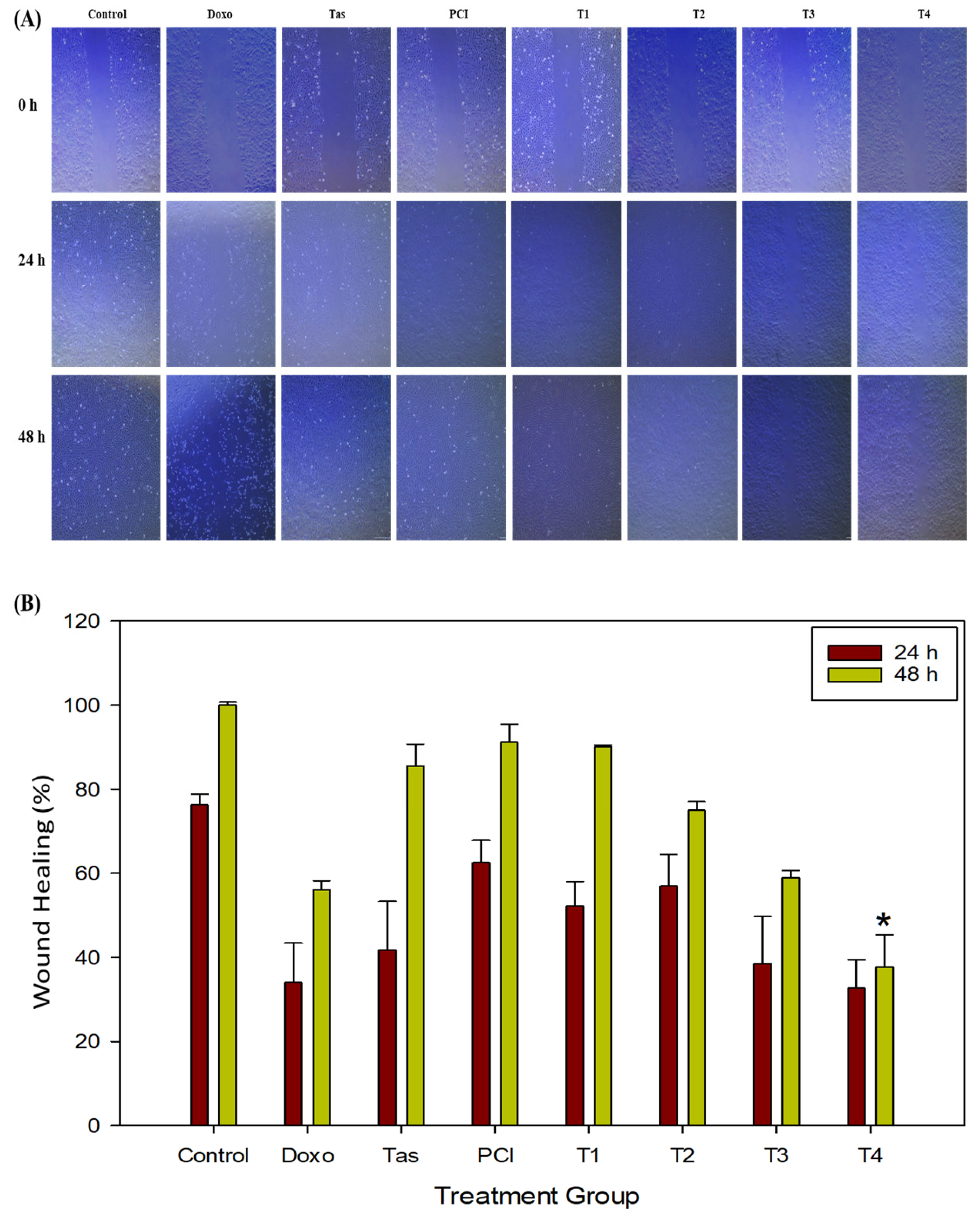
In our study, Tas and PCI significantly suppressed MMP9 and MMP13 expression, leading to reduced osteosarcoma cell migration and invasion, as evidenced by the wound healing assays. These effects were particularly pronounced in the T3 and T4 treatment groups, reinforcing the potential of combination therapy to mitigate metastasis.
To better model the tumor microenvironment, we employed a 3D spheroid system that closely recapitulates the in vivo tumor architecture and cellular interactions [
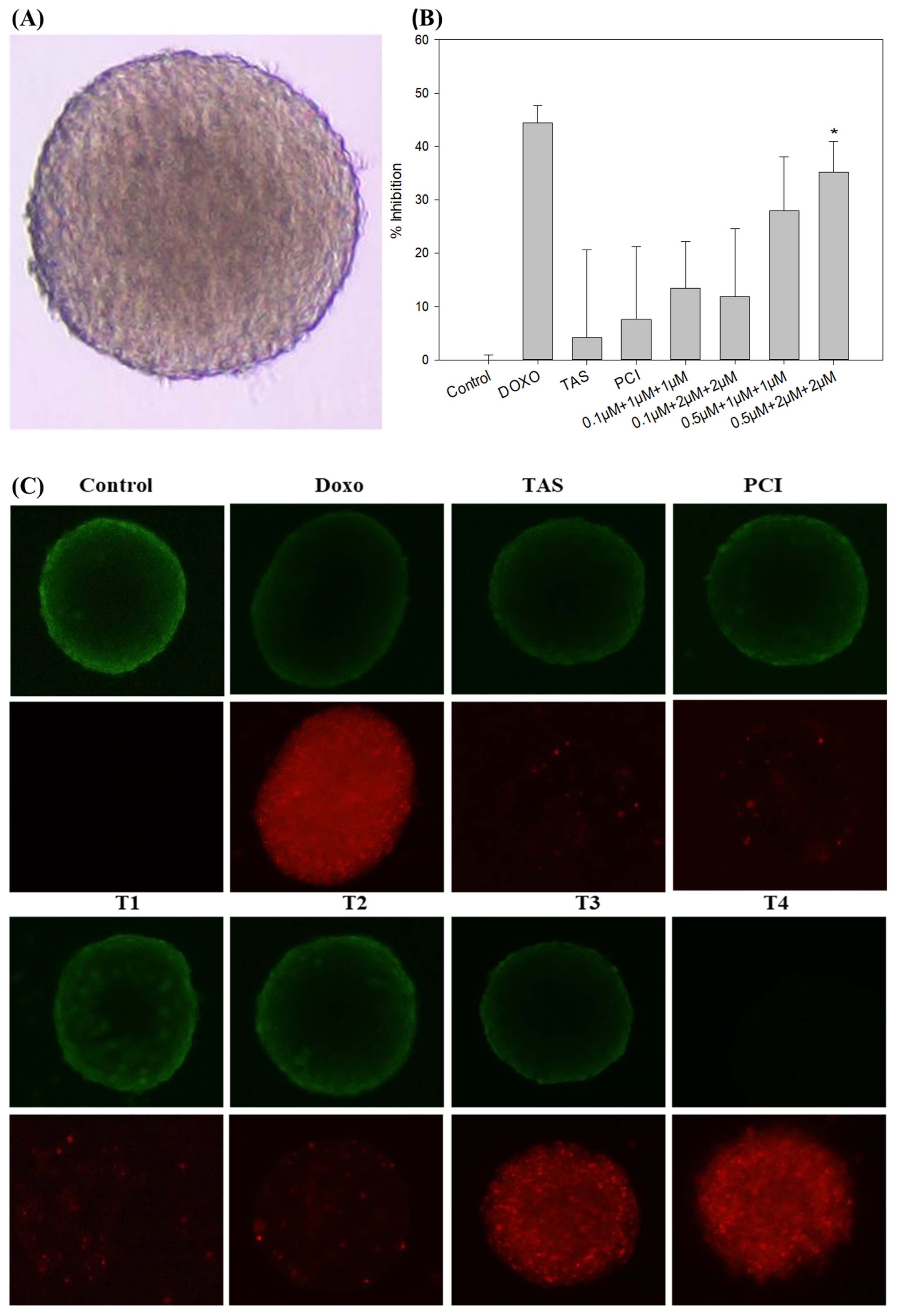
27]. Our results demonstrated that combination therapy effectively reduced spheroid volume, suggesting enhanced tumor penetration and cytotoxicity. LIVE/DEAD cell staining further confirmed the increased cell death in the combination treatment groups, consistent with our 2D findings. However, due to the scope and timeline of the current study, we did not perform a dedicated spheroid regrowth/recovery experiment after the 48 h treatment period. Our primary focus was on evaluating the initial cytotoxic and migrastatic effects of the drug treatments within a defined timeframe. We followed the standard protocol for drug screening described in previously published research [
28,
29].
The phosphatidylinositol 3-kinase/protein kinase B (PI3K/AKT) signaling pathway, a crucial regulator of tumor proliferation and drug resistance, was significantly downregulated following combination therapy [
30]. HDAC8 stabilizes Akt by reducing its acetylation, thereby enhancing its phosphorylation at Ser473, a process that promotes cell survival and chemoresistance [
30]. Our study demonstrated that Tas and PCI reduced the expression of phosphorylated AKT (p-AKT) and runt-related transcription factor 2 (RUNX2), thereby disrupting these oncogenic pathways. RUNX2 overexpression is a hallmark of osteosarcoma and contributes to p53 suppression, leading to reduced responsiveness to chemotherapy. Meanwhile, our findings suggest that downregulation of RUNX2/pAKT signaling may restore p53 activity and sensitize osteosarcoma cells to apoptosis [
19,
30,
31]. Further studies, such as siRNA knockdown or overexpression experiments, are needed to confirm a direct causal relationship. Additionally, emerging evidence underscores the significance of HDAC inhibitors in modulating osteosarcoma progression. Recent studies have demonstrated that HDAC inhibitors, such as romidepsin, can effectively downregulate neuropilin-1 (NRP1) in osteosarcoma cells, thereby significantly reducing their metastatic potential [
32]. In the context of oncogenic signaling, the reciprocal activation between RUNX2 and the PI3K/AKT pathway has been recognized as a pivotal factor in driving tumor progression and fostering chemoresistance in osteosarcoma. the reciprocal activation between RUNX2 and the PI3K/AKT pathway has been recognized as a pivotal factor in driving tumor progression and fostering chemoresistance in osteosarcoma. RUNX2 plays a central role in the epithelial–mesenchymal transition (EMT), a critical process facilitating cancer cell migration and invasion, which ultimately promotes tumor progression. Multiple signaling pathways, including the PI3K/AKT pathway, have been reported to mediate the role of RUNX2 in cancer invasion [
33]. Moreover, studies have shown that miR-302b can suppress osteosarcoma cell migration and invasion by directly downregulating RUNX2 expression, further reinforcing the importance of this pathway in osteosarcoma pathogenesis [
34]. By integrating these insights, our study highlights the therapeutic potential of HDAC inhibitors in osteosarcoma treatment. Modulation of NNMT-SIRT1 interactions, optimization of combination therapies, and targeted inhibition of RUNX2-driven signaling pathways could serve as valuable strategies to enhance treatment efficacy and overcome chemoresistance in osteosarcoma.
However, recent studies have highlighted the critical role of NNMT in osteosarcoma progression, demonstrating that its upregulation contributes to increased tumor aggressiveness and resistance to therapy [
35]. NNMT catalyzes the methylation of nicotinamide, reducing its availability as an inhibitor of SIRT1, a key regulator of cellular metabolism and stress responses [
36]. Given that SIRT1 has been implicated in the modulation of apoptosis, DNA repair, and chemotherapy resistance, the interplay between NNMT and SIRT1 may significantly influence osteosarcoma cell survival. Our findings suggest that targeting HDACs in osteosarcoma, particularly in combination with agents that modulate metabolic pathways, could be further optimized by considering NNMT-SIRT1 interactions. Since NNMT-driven SIRT1 activation could potentially counteract HDAC inhibition, future studies should explore whether NNMT inhibitors could enhance the therapeutic efficacy of HDAC inhibitors in osteosarcoma treatment.
Although these findings underscore the potential of HDAC inhibitors in osteosarcoma therapy, several limitations remain. The long-term efficacy of this therapeutic strategy requires further validation in in vivo models, particularly concerning pharmacokinetics, toxicity, and potential resistance mechanisms. Combination therapies, such as doxo with PCI-24781, have shown promising anti-tumor responses with minimal toxicity in preclinical models [
5], reinforcing the need for further investigation.
The results indicate that combination therapy (T4) effectively disrupted osteosarcoma cell migration. However, we acknowledge the absence of an isobolographic analysis, which is crucial for quantitatively determining whether the observed effects are synergistic, additive, or sub-additive. Future studies should incorporate dose–response matrix analyses and combination index calculations to precisely characterize the nature of drug interactions. Additionally, exploring a range of dose ratios will provide a clearer understanding of optimal treatment strategies.
To facilitate clinical translation, future research should focus on optimizing dosing regimens, determining whether a combination should be administered simultaneously or sequentially, and identifying biomarkers for patient stratification. These steps are essential for tailoring the treatment to individual patient responses.
4. Materials and Methods
4.1. Cell Culture
The human osteosarcoma cell lines SJSA-1 (CRL-2098) and MG-63 (CRL-1427) were obtained from the American Type Culture Collection (ATCC). The cells were cultured in Dulbecco’s Modified Eagle’ Medium (DMEM F12; SolBio; Gyeonggido, Republic of Korea) supplemented with 10.0% fetal bovine serum (FBS; Gibco; Thermo Fisher Scientific, Waltham, MA, USA) and 1.0% penicillin–streptomycin (Gibco; Thermo Fisher Scientific, Waltham, MA, USA). The cells were maintained in a humidified incubator at 37 °C and 5.0% CO2. Cells at passages 4 to 6 were used for the experimental procedures.
4.2. Drug Treatment Groups
This study investigated the effects of HDAC4 inhibitor (Tas) (MedChemExpress; Monmouth Junction, NJ 08852, USA; cat. HY-10528), and HDAC8 inhibitor (PCI) (MedChemExpress; Monmouth Junction, South Brunswick, NJ, USA; cat. HY-15224), and Doxo (Abcam; Cambridge, UK; cat. ab232855) in the SJSA-1 osteosarcoma cell line and spheroid model, both individually and in combination. In brief, eight treatment groups were included in this study (
Table 2). Treatments were administered for 48 h in both 2D and 3D spheroid models with incubation at 37 °C and 5.0% CO
2. The inhibitors Tas and PCI were received in powder form and dissolved in DMSO according to the manufacturer’s instructions to prepare 10 mM stock solutions, which were stored at −80 °C. Doxorubicin was received as a 20 mM stock solution and was directly diluted in the appropriate growth medium for treatments. For all experiments, the stock solutions were further diluted in complete growth medium to achieve the required final concentrations. Drug concentrations and treatment exposures were selected based on previous studies. As the aim was to evaluate the drugs in combination, the concentration of each drug was reduced compared to the doses typically used in monotherapy. This strategy minimizes potential toxicity while maximizing synergistic effects, allowing each drug to exert its intended mechanism of action while reducing adverse interactions. The 48 h treatment duration was optimized based on cell viability assay data, as it showed almost 50.0% inhibitory effects on osteosarcoma cell lines within this time span. All molecular assays were performed after 48 h treatment.
4.3. CCK-8 Assay
The CCK-8 assay is a colorimetric method that is used to gauge the metabolic activity of viable cells. It involves the reduction of WST-8 by mitochondrial dehydrogenases, culminating in the formation of a highly water-soluble yellow formazan compound [
6]. The CCK-8 assay was performed using a CCK-8 cell counting kit (Nanjing Vazyme Biotech; Jiangsu, China; cat. A311) according to the manufacture’s protocol. Briefly, a cell suspension containing 5000 SJSA-1 osteosarcoma cells per well was seeded into a 96-well plate in a final volume of 100.0 μL. The cells were incubated overnight. The growth medium was then replaced with the drug treatment medium, and the cells were incubated further for 24 and 48 h at 37 °C. After incubation, the cells were washed with phosphate-buffered saline (PBS). Next, 100.0 µL of fresh complete growth medium and 10.0 µL of CCK-8 reagent were added to each well, and the plate was incubated for an additional 2 h at 37 °C, following the manufacturer’s protocol (Vazyme A311). The absorbance was measured at 450 nm using a microplate reader (BioTek Instruments, Inc., Winooski, VT, USA; S/N.1503205). The experiment was performed in triplicate (
n = 3) with three independent biological replicates to ensure reproducibility. The total colony number was measured, and the results were normalized to the control group. Plating efficiency (PE) and surviving fraction (SF) were calculated based on the initial seeding density. Statistical analysis was performed to assess differences between the treatment groups.
4.4. Colony Formation Assay
SJSA-1 cells were plated in 6-well plates at a density of 8 × 102 cells per well. After 24 h of incubation, the cells were treated with varying drug concentrations and cultured for an extended period. Once visible colonies appeared in the control group, the cultures in all treatment groups were harvested. The cells were washed with PBS, fixed in 4.0% paraformaldehyde (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) for 10 min, and then stained with crystal violet (Abcam) to facilitate colony visualization.
4.5. Annexin-V FITC Apoptosis Assay
Apoptosis in osteosarcoma cells was analyzed by flow cytometry using the Annexin-V FITC and PI staining kit (Abcam ab14085). SJSA-1 osteosarcoma cells were seeded in 60 mm culture plates and incubated until they reached 70.0–80.0% confluence. The medium was then replaced with the drug treatment medium. After 48 h of incubation, cells were washed with cold PBS, harvested using 0.25X trypsin (SolBio; Gyeonggido, Republic of Korea), and cell viability was assessed. The cells were subsequently suspended in 500.0 µL of binding buffer (R&D Systems; Minneapolis, MN, USA) and incubated in the dark with 5.0 µL of annexin V-FITC and 5.0 µL of propidium iodide, following the manufacturer’s instructions (Abcam). Flow cytometric analysis was performed using a Beckman Coulter CytoFlex flow cytometer (Beckman Coulter Inc., Suzhou, China) with detection filters set at 530/30 (annexin-V FITC) and 610/20 (PI), using an excitation laser at 488 nm.
4.6. Caspase-3/7 Activity Assay
Caspase-3/7 activity was measured using the CellEvent™ caspase-3/-7 Green Detection Reagent (Invitrogen; Life Technologies corporation, Eugene, OR, USA). Upon cleavage by activated caspase-3/7, the probe became fluorescent and free to bind to DNA. After 48 h of treatment, cells were collected and incubated with 5 μM CellEvent™ caspase-3/7 green detection reagent in complete medium for 30 min at 37 °C in the dark. The stained cells were observed using a Beckman Coulter CytoFlex flow cytometer (Suzhou, China).
4.7. Wound Healing Assay
SJSA-1 cells (0.5 × 106 cells per well) were seeded into 6-well plates. Once the cells reached near confluence, a linear artificial wound was generated using a sterile 200.0 μL pipette, perpendicular to the cell layer. After gently washing with PBS, the cells were incubated with drug-containing medium for 48 h. Following incubation, the cells were fixed by adding 500.0 μL of fixative solution to each well and left to fix for 10 min at room temperature. The solution was aspirated, and the wells were carefully washed with PBS. Finally, 1.0 mL PBS was added to each well to maintain cell hydration. At 0, 24, and 48 h, each wound was randomly photographed (Olympus, IX73; Tokyo, Japan) and the percentage wound healing rate was calculated.
4.8. Spheroid Development
A 3D osteosarcoma spheroid model was established using a 96-well ultra-low attachment plate (Nunclon™ Sphera™ 96-Well; Thermo Fisher Scientific; Waltham, MA, USA). When SJSA-1 osteosarcoma cells reached 70.0–80.0% confluence, the cell culture medium was aspirated, and the cells were washed with 1X PBS. The cells were then trypsinized, and cell density was determined using trypan blue and a hemocytometer. Subsequently, 5000 cells were seeded in each well of a 96-well ultra-low-attachment plate containing 200.0 µL of complete growth medium. The plates were centrifuged at 1250 rpm for 5 min at 4 °C to promote cell aggregation at the center. After centrifugation, the plates were incubated for 48 h at 37 °C, 5.0% CO
2, and 95.0% humidity [
28,
37]. Spheroids were generated after 24 h of incubation, whereas a more spherical and compact spheroid shape emerged after 48 h of incubation, which was used for drug screening.
4.9. Spheroid Size Analysis
The size of SJSA-1 spheroids was measured using the open-access software ImageJ version 1.54g (Java version: 1.8.0_345, NIH, Bethesda, MD, USA). In brief, the spheroid was converted into a binary mask using an image processing tool. The major and minor axes of the spheroid binary mask were determined using an analysis tool, and spheroid volume was calculated. Furthermore, the effect of treatment was evaluated through %inhibition using the following formula:
4.10. Live and Dead Cell Assay
After 48 h of treatment, the viability of the spheroid model was assessed using the LIVE/DEAD Cell Viability Assay Kit for 3D and 2D cell cultures (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany). In brief, staining solution was prepared by mixing calcein AM and propidium iodide in a 1:1 ratio in mixture of complete growth medium and PBS (50:50 ratio). The cell culture medium was removed, and the spheroids were washed with 200.0 µL of PBS. Then, 100.0 µL of the staining solution was added to each well. Spheroids were incubated for 60 min at 37 °C, protected from light. Live and dead cells were visualized using a fluorescence microscope with the appropriate fluorescence filters for calcein AM (green fluorescence) and propidium iodide (red fluorescence) using Olympus IX73 microscope (Olympus Corporation, Tokyo, Japan).
4.11. Western Blot
After 48 h of treatment, the spheroids were collected from a 96-well plate into 1.5 mL microcentrifuge tubes. The spheroids were washed with PBS, followed by the addition of 100.0 µL of RIPA lysis buffer (ThermoScientific, Rockford, IL, USA; Ref. 89900), and protein concentration was determined using a BCA kit (Vazyme, cat. E112-02). The samples were then placed in an icebox for 120 min and vortexed every 10–15 min. After incubation, the samples were centrifuged at 14,000 rpm for 10 min, and the supernatant was collected and stored at −20 °C. After protein isolation, samples were mixed with a 5× sample buffer and subjected to SDS-PAGE on a polyacrylamide gel. The proteins were transferred to a PVDF membrane (Atto, Amherst, NY, USA, AE-667-P) and blocked with 5.0% BSA at room temperature for 1 h. The membranes were then incubated overnight at 4 °C with primary antibodies as follows: cleaved caspase 8 (Cell Signaling, Danvers, MA, USA, cat.98134S, 1:1000), caspase 3 (Cell Signaling, cat.9662S, 1:1000), cleaved caspase 3 (Cell Signaling, cat.9664S, 1:1000), RUNX2 (Cell Signaling, cat.12556S, 1:1000), MMP9 (SantaCruz, Dallas, TX, USA, cat.sc-21733, 1:1000), MMP13 (SantaCruz, cat.515284, 1:1000), pAKT (Cell Signaling, cat.4060S, 1:1000), GAPDH (R&D Systems, cat. MAB5718, 1:1000). Following incubation, the membranes were washed three times with 0.1% TBST for 5 min each and then incubated with HRP-conjugated goat anti-rabbit IgG (SantaCruz, cat.sc-2357, 1:1000) or anti-mouse IgG (R&D Systems, cat.HAF007, 1:1000) secondary antibodies for 2 h at room temperature. This washing step was repeated to remove excess secondary antibodies. Protein bands were visualized using an ECL detection kit (Vazyme) and recorded using a ChemiDoc Image Analyzer (GE Healthcare Life Sciences AB; Uppsala, Sweden; Amersham Imager 600 UV,). Densitometric analysis of the bands was performed using the software ImageLab (Version 6.1.0 build 7). Band intensities were normalized to GAPDH, and the fold change was calculated relative to the control group.
4.12. Real-Time Quantitative PCR (RT-qPCR)
RNA was extracted from spheroids using TRIazol Reagent (Ambion Life Technologies, Waltham, MA, USA, Ref. 15596026). Briefly, 1.0 mL of TRIazol reagent and 200.0 µL of chloroform were added to the samples, and the tubes were vortexed vigorously for 5–10 s. The tubes were then incubated at room temperature for 2–3 min before centrifugation at 12,000× g for 15 min at 4 °C. The colorless upper phase containing RNA was transferred to a fresh, RNase-free tube, and an equal volume of 100.0% ethanol was added to achieve a final ethanol concentration of 50.0%. The samples were mixed well by vortexing. RNA concentration and purity were assessed using a microplate reader (BioTek Instruments, Inc.; Winooski, VT 05404, USA, S/N.1503205). RNA was normalized and reverse-transcribed using the Vazyme cDNA synthesis kit (R312-02 HiScript III 1st Strand cDNA Synthesis Kit), according to the manufacturer’s instructions. cDNA synthesis was performed using a SimpliAmp Thermal Cycler (Applied Biosystems; Life Technologies; Carlsbad, CA, USA; S/N. 1708). The cDNA was then subjected to quantitative real-time PCR using SYBR Green Premix (Vazyme Taq Pro Universal SYBR qPCR Master Mix Q712; Nanjing Vazyme Biotech; Jiangsu, China) and analyzed on a LightCycler 96 (Roche, Basel, Switzerland). The RT-qPCR conditions were as follows: initial denaturation at 95 °C for 30 s, followed by 40 cycles of amplification at 95 °C for 10 s and 60 °C for 30 s, with a melting curve step at 95 °C for 15 s, 60 °C for 60 s, and 95 °C for 1 s, ending with a 30 s cooling step at 37 °C. The primer pair’s p16 (forward sequence: 5′-CTCGTGCTGATGCTACTGAGGA-3′; reverse sequence: 5′-GGTCGGCGCAGTTGGGCTCC-3′) and p53 (forward sequence: 5′-CCTCAGCATCTTATCCGAGTGG-3′; reverse sequence: 5′-TGGATGGTGGTACAGTCAGAGC-3′) were sourced from Origene Biotechnology, and β-actin (forward sequence: 5′-CACCATTGGCAATGAGCGGTTC-3′; reverse sequence: 5′-AGGTCTTTGCGGATGTCCACGT-3′) was used as the internal control. Cq values were recorded, and relative gene expression was calculated using the 2−ΔΔCq method, normalized to β-actin, and compared to the expression levels in control cells.
4.13. Statistical Analysis
All experiments were conducted in triplicate, while Western blotting, apoptosis assay, and qRT-PCR were in conducted in duplicate, and results are presented as mean ± standard deviation (SD). Data were analyzed using one-way ANOVA, followed by Tukey’s post hoc test for multiple comparisons. Statistical significance was set at p < 0.05. All statistical analyses were performed using SigmaPlot 14.0 and Microsoft Excel-2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}