

Impact of Patient Profile on CDK4/6 Inhibitor Therapy Outcomes: A Real-World Data Analysis

 ,
,
Abstract
1. Introduction
2. Results
2.1. Clinical and Biological Characteristics of Patients
2.2. Treatment Characteristics
2.3. Toxicity and Dose Modification
2.4. Survival Outcomes
2.5. Correlations of Hormonal Therapy and Age with Type of CDK4/6i
2.6. Differences Observed for Ribociclib
- ○
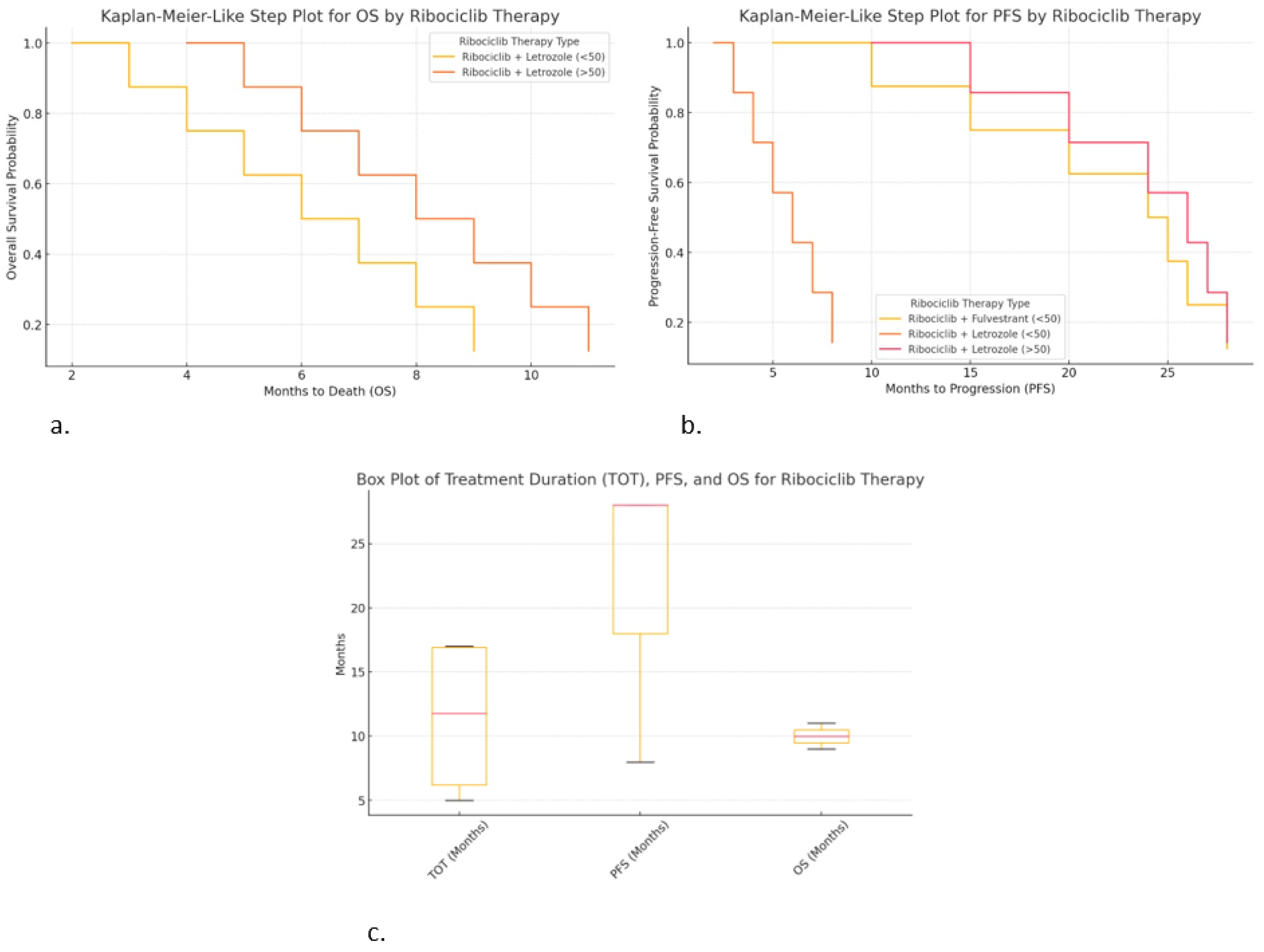
- Ribociclib + Fulvestrant (<50 years) provided longer PFS (up to 28 months).
- ○
- Ribociclib + Letrozole (<50 years) resulted in shorter PFS (~8 months), suggesting earlier progression.
- ○
- Ribociclib + Letrozole (>50 years) resulted in similar PFS (~28 months), suggesting it may work well in older patients.
- ○
- Ribociclib + Letrozole (>50 years) resulted in slightly longer OS (up to 11 months).
- ○
- Ribociclib + Letrozole (<50 years) resulted in shorter OS (~9 months).
- ○
- This visualization is useful for comparing the survival outcomes by therapy type.
- ○
- Box plot for TOT, PFS, and OS (Figure 5c):
- ○
- Ribociclib + Fulvestrant (<50 years) resulted in the high consistency in TOT (17 months) and PFS (28 months).
- ○
- Ribociclib + Letrozole (>50 years) shows greater variability in TOT and PFS, suggesting diverse patient responses.
- ○
- Ribociclib + Letrozole (<50 years) resulted in shorter treatment duration and survival, indicating worse outcomes.
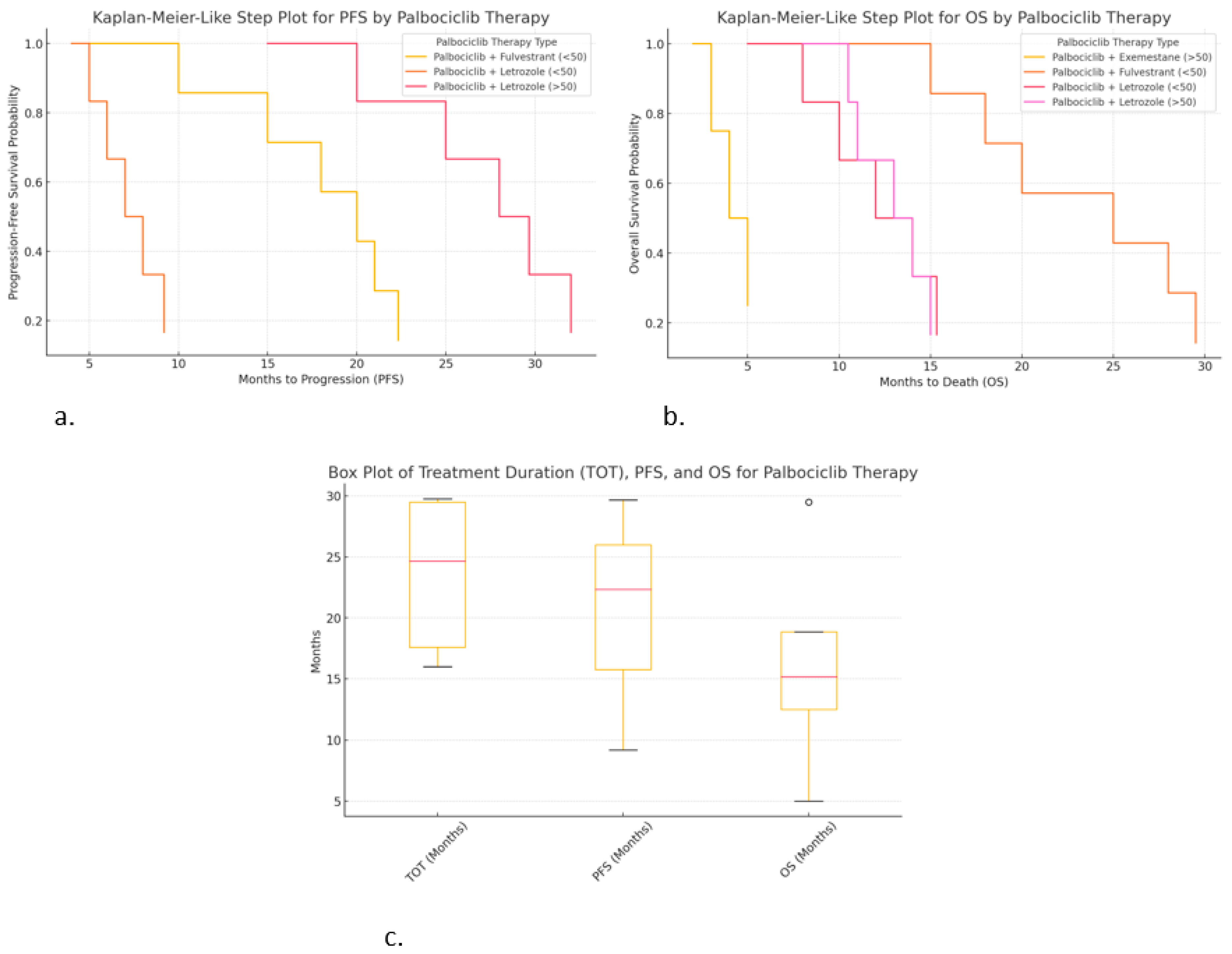
2.7. Differences Observed for Palbociclib
- ○
- Palbociclib + Letrozole (>50 years) resulted in the highest PFS (~30 months).
- ○
- Palbociclib + Fulvestrant (<50 years) also shows extended PFS (~22 months).
- ○
- Palbociclib + Letrozole (<50 years) resulted in a much shorter PFS (~9 months), suggesting faster progression.
- ○
- Palbociclib + Fulvestrant (<50 years) shows the highest OS (~29.5 months), suggesting significant survival.
- ○
- Palbociclib + Letrozole (>50 years) shows moderate OS (~15 months).
- ○
- Palbociclib + Exemestane (>50 years) resulted in the shortest OS (~5 months), suggesting poor survival in this subgroup.
- ○
- Palbociclib + Exemestane (>50 years) resulted in high variability in TOT (29.5 months).
- ○
- Palbociclib + Letrozole (>50 years) resulted in the highest PFS (~30 months), with low variability.
- ○
- Palbociclib + Letrozole (<50 years) resulted in lower OS (~15 months), with higher variability.
2.8. Differences Observed for Abemaciclib
- ○
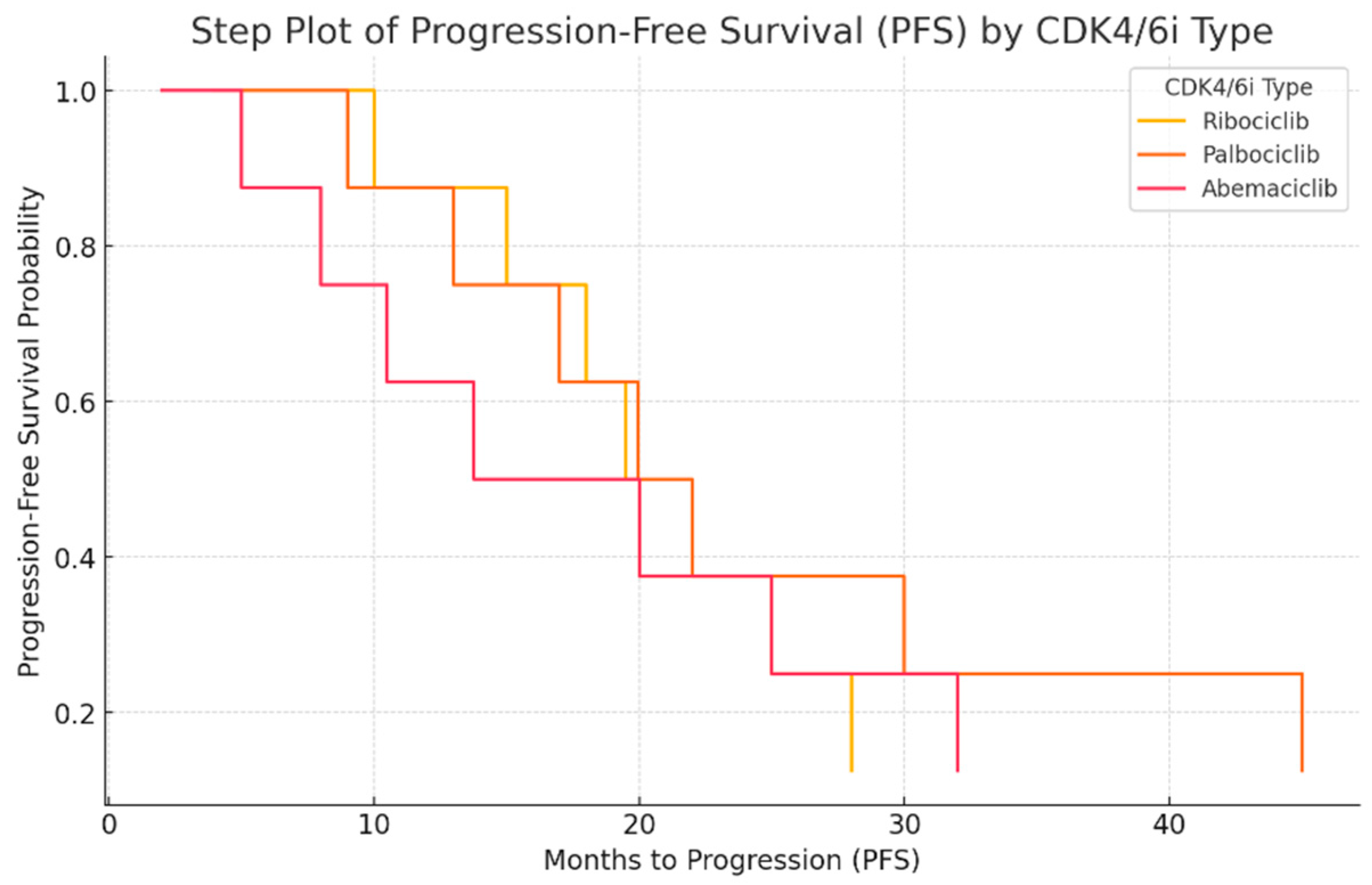
- Abemaciclib + Letrozole (>50 years) resulted in the longest PFS (~17 months), but it was still lower compared to other CDK4/6i treatments.
- ○
- Abemaciclib + Letrozole (<50 years) resulted in a shorter PFS (~10.5 months), indicating faster progression in younger patients.
- ○
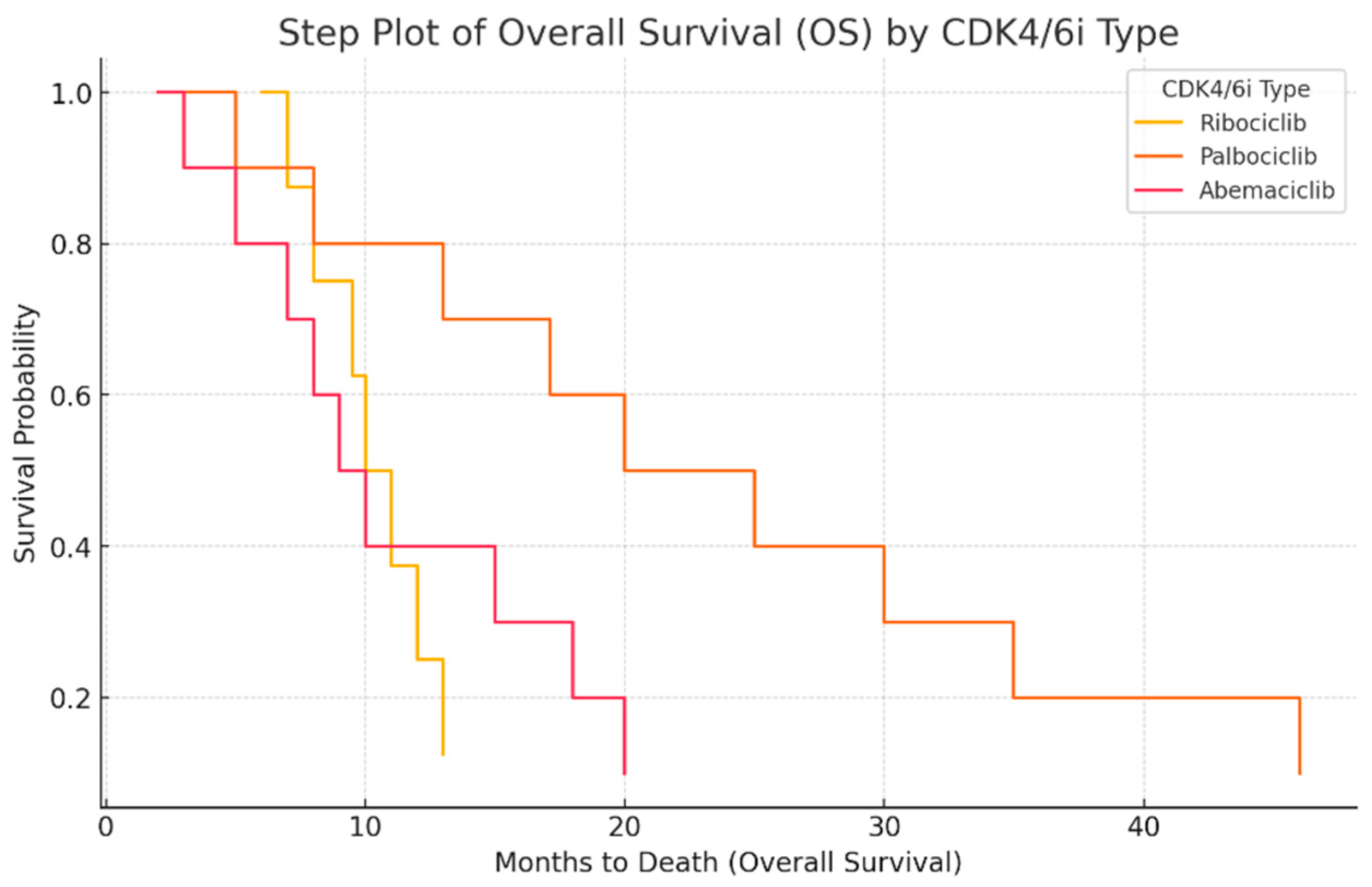
- Abemaciclib + Letrozole (<50 years) shows short OS (~5.5 months), indicating poor survival outcomes.
- ○
- Abemaciclib + Letrozole (>50 years) resulted in the worst OS (~4 months, median of ~2 months), suggesting very poor prognosis.
- ○
- Abemaciclib + Fulvestrant (<50 years) shows the longest TOT (25.5 months).
- ○
- Abemaciclib + Letrozole (>50 years) resulted in high PFS (~17 months) but very low OS (~4 months), suggesting that treatment may delay progression but not improve survival.
- ○
- Variability in TOT was high, especially for Abemaciclib + Letrozole (<50 years), indicating differences in patient responses.
- ➣
- Abemaciclib appears to delay progression but does not significantly improve OS.
- ➣
- Younger patients on abemaciclib may have shorter PFS and OS compared to older patients.
- ➣
- Combination with fulvestrant leads to longer treatment duration (TOT), suggesting better tolerability.
3. Materials and Methods
3.1. Study Population
3.2. Statistical Analysis
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breast Cancer Facts & Figures 2019–2020. Available online: https://www.cancer.org/research/cancer-facts-statistics/breast-cancer-facts-figures.html (accessed on 14 February 2022).
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [PubMed]
- Berruti, A.; Zola, P.; Buniva, T.; Baù, M.G.; Farris, A.; Sarobba, M.G.; Bottini, A.; Tampellini, M.; Durando, A.; Destefanis, M.; et al. Prognostic factors in metastatic breast cancer patients obtaining objective response or disease stabilization after first-line chemotherapy with epirubicin. Evidence for a positive effect of maintenance hormonal therapy on overall survival. Anticancer. Res. 1997, 17, 2763–2768. [Google Scholar]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Trédan, O.; Chen, S.-C.; Manso, L.; et al. MONARCH 3: Abemaciclib as Initial Therapy for Advanced Breast Cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef]
- Purohit, L.; Jones, C.; Gonzalez, T.; Castrellon, A.; Hussein, A. The Role of CD4/6 Inhibitors in Breast Cancer Treatment. Int. J. Mol. Sci. 2024, 25, 1242. [Google Scholar] [CrossRef]
- Turner, N.C.; Ro, J.; André, F.; Loi, S.; Verma, S.; Iwata, H.; Harbeck, N.; Loibl, S.; Bartlett, C.H.; Zhang, K.; et al. Palbociclib in Hormone-Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2015, 373, 209–219. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall Survival with Ribociclib plus Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef]
- Sledge, G.W. MONALEESA-2: A Phase III Trial of Ribociclib and Letrozole in ER+/HER2- Advanced Breast Cancer. J. Clin. Oncol. 2019, 37, 1185–1193. [Google Scholar]
- DeMichele, A.; Clark, A.S.; Tan, K.S.; Heitjan, D.F.; Gramlich, K.; Gallagher, M.; Lal, P.; Feldman, M.; Zhang, P.; Colameco, C.; et al. CDK 4/6 Inhibitor Palbociclib (PD0332991) in Rb+ Advanced Breast Cancer: Phase II Activity, Safety, and Predictive Biomarker Assessment. Clin. Cancer Res. 2015, 21, 995–1001. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann. Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef]
- Dickler, M.N.; Tolaney, S.M.; Rugo, H.S.; Cortés, J.; Diéras, V.; Patt, D.; Wildiers, H.; Hudis, C.A.; O’Shaughnessy, J.; Zamora, E.; et al. MONARCH 1, A Phase II Study of Abemaciclib, a CDK4 and CDK6 Inhibitor, as a Single Agent, in Patients with Refractory HR+/HER2− Metastatic Breast Cancer. Clin. Cancer Res. 2017, 23, 5218–5224, Correction in Clin. Cancer Res. 2018, 24, 5485. https://doi.org/10.1158/1078-0432.CCR-18-3193. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, K.; Stückrath, K.; Hartung, C.; Kaufhold, S.; Uleer, C.; Hanf, V.; Lantzsch, T.; Peschel, S.; John, J.; Pöhler, M.; et al. PIK3CA-mutations in breast cancer. Breast Cancer Res. Treat. 2022, 196, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Del Re, M.; Crucitta, S.; Lorenzini, G.; De Angelis, C.; Diodati, L.; Cavallero, D.; Bargagna, I.; Cinacchi, P.; Fratini, B.; Salvadori, B.; et al. PI3K mutations detected in liquid biopsy are associated to reduced sensitivity to CDK4/6 inhibitors in metastatic breast cancer patients. Pharmacol. Res. 2020, 163, 105241. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, E.; Moiso, E.; Safonov, A.; Cabel, L.; Loudon, L.; Dang, C.T.; Shen, S.; Jhaveri, K.L.; Robson, M.E.; Chandarlapaty, S.; et al. Overall survival analysis of first line CDK4/6 inhibitors in a large real-world cohort of patients with hormone receptor-positive (HR+)/HER2-negative metastatic breast cancer. J. Clin. Oncol. 2024, 42, e13095. [Google Scholar] [CrossRef]
- Skocilic, I.; Golcic, M.; Petrc, A.B.; Kolak, M.; Kolovrat, D.; Ropac, S.; Marusic, J.; Dobrila-Dintinjana, R.; Badovinac, I.; Ferari, A.M.; et al. Real-World Data with CDK4/6 Inhibitors—A Single Center Experience from Croatia. J. Pers. Med. 2024, 14, 895. [Google Scholar] [CrossRef]
- Gnant, M.; Singer, C.F.; Rinnerthaler, G.; Pfeiler, G.; Egle, D.; Balic, M.; Bartsch, R. Position paper on CDK4/6 inhibitors in early breast cancer. memo-Mag. Eur. Med. Oncol. 2023, 16, 135–144. [Google Scholar] [CrossRef]
- Barroso-Sousa, R.; Shapiro, G.I.; Tolaney, S.M. Clinical Development of the CDK4/6 Inhibitors Ribociclib and Abemaciclib in Breast Cancer. Breast Care 2016, 11, 167–173. [Google Scholar] [CrossRef]
- Turner, N.C.; Liu, Y.; Zhu, Z.; Loi, S.; Colleoni, M.; Loibl, S.; DeMichele, A.; Harbeck, N.; André, F.; Bayar, M.A.; et al. Cyclin E1 Expression and Palbociclib Efficacy in Previously Treated Hormone Receptor–Positive Metastatic Breast Cancer. J. Clin. Oncol. 2019, 37, 1169–1178, Erratum in J. Clin. Oncol. 2019, 27, 2956. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.-A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martín, M.; et al. Phase III Randomized Study of Ribociclib and Fulvestrant in Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Advanced Breast Cancer: MONALEESA-3. J. Clin. Oncol. 2018, 36, 2465–2472. [Google Scholar] [CrossRef]
- Franco, R.; Cao, J.Q.; Yassa, M.; Hijal, T. Safety of CDK4/6 Inhibitors Combined with Radiotherapy in Patients with Metastatic Breast Cancer: A Review of the Literature. Curr. Oncol. 2023, 30, 5485–5496. [Google Scholar] [CrossRef]
- Hamilton, E.; Infante, J.R. Targeting CDK4/6 in patients with cancer. Cancer Treat. Rev. 2016, 45, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Nahta, R.; Yu, D.; Hung, M.-C.; Hortobagyi, G.N.; Esteva, F.J. Mechanisms of Disease: Understanding resistance to HER2-targeted therapy in human breast cancer. Nat. Clin. Pract. Oncol. 2006, 3, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Braunschweig, T. Clinical outcomes of CDK4/6 inhibitors in metastatic ER-positive HER2-negative breast cancer in a real-world setting. JAMA Oncol. 2021, 7, 645–651. [Google Scholar]
- Pla, H.; Felip, E.; Obadia, V.; Pernas, S.; Viñas, G.; Margelí, M.; Fort-Culillas, R.; Del Barco, S.; Sabaté, N.; Fort, E.; et al. Elderly patients with hormone receptor-positive HER2-negative metastatic breast cancer treated with CDK4/6 inhibitors in a multicentre cohort. Clin. Transl. Oncol. 2024, 26, 1748–1758. [Google Scholar] [CrossRef]
- Im, S.-A.; Lu, Y.-S.; Bardia, A.; Harbeck, N.; Colleoni, M.; Franke, F.; Chow, L.; Sohn, J.; Lee, K.-S.; Campos-Gomez, S.; et al. Overall Survival with Ribociclib plus Endocrine Therapy in Breast Cancer. N. Engl. J. Med. 2019, 381, 307–316. [Google Scholar] [CrossRef]
- Iwata, H.; Im, S.-A.; Masuda, N.; Im, Y.-H.; Inoue, K.; Rai, Y.; Nakamura, R.; Kim, J.H.; Hoffman, J.T.; Zhang, K.; et al. PALOMA-3: Phase III Trial of Fulvestrant With or Without Palbociclib in Premenopausal and Postmenopausal Women With Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Metastatic Breast Cancer That Progressed on Prior Endocrine Therapy—Safety and Efficacy in Asian Patients. J. Glob. Oncol. 2017, 3, 289–303. [Google Scholar] [CrossRef]
- Sledge, G.W., Jr.; Toi, M.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. MONARCH 2: Abemaciclib in Combination with Fulvestrant in Women with HR+/HER2− Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J. Clin. Oncol. 2017, 35, 2875–2884. [Google Scholar] [CrossRef]
- Cejalvo, J.M.; de Dueñas, E.M.; Galván, P.; García-Recio, S.; Gasión, O.B.; Paré, L.; Antolín, S.; Martinello, R.; Blancas, I.; Adamo, B.; et al. Intrinsic Subtypes and Gene Expression Profiles in Primary and Metastatic Breast Cancer. Cancer Res. 2017, 77, 2213–2221. [Google Scholar] [CrossRef]
- Cejalvo, J.M.; Pascual, T.; Fernández-Martínez, A.; Brasó-Maristany, F.; Gomis, R.R.; Perou, C.M.; Muñoz, M.; Prat, A. Clinical implications of the non-luminal intrinsic subtypes in hormone receptor-positive breast cancer. Cancer Treat. Rev. 2018, 67, 63–70. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | CDK | ||
|---|---|---|---|
| Ribociclib | Palbociclib | Abemaciclib | |
| Environment—n (%) | |||
| Rural | 1 (4.2%) | 8 (19.5%) | 5 (16.7%) |
| Urban | 23 (95.8%) | 33 (80.5%) | 25 (83.3%) |
| Age—mean (±SD) | 53.67 (±15.11) | 57.68 (±13.35) | 59.00 (±10.47) |
| Lymph node status at diagnosis | |||
| N0 | 5 (21.7%) | 6 (20.0%) | 8 (29.6%) |
| N1 | 8 (34.8%) | 8 (26.7%) | 12 (44.4%) |
| N1a | 2 (8.7%) | 3 (10.0%) | 1 (3.7%) |
| N2 | 3 (13.0%) | 5 (16.7%) | 3 (11.1%) |
| N2a | 2 (8.7%) | 2 (6.7%) | 1 (3.7%) |
| N3 | 2 (8.7%) | 5 (16.7%) | 1 (3.7%) |
| N3a | 1 (4.3%) | 1 (3.3%) | 1 (3.7%) |
| Histological grade at diagnosis | |||
| G1 | 0 (0.0%) | 5 (13.5%) | 3 (10.3%) |
| G2 | 23 (100.0%) | 24 (64.9%) | 16 (55.2%) |
| G3 | 0 (0.0%) | 8 (21.6%) | 10 (34.5) |
| Non-metastatic/metastatic at diagnosis | |||
| Non-metastatic | 14 (58.3%) | 24 (58.5%) | 18 (60.0%) |
| Metastatic | 10 (41.7%) | 17 (41.5%) | 12 (40.0%) |
| Metastasis | |||
| without | 0 (0.0%) | 0 (0.0%) | 6 (20.0%) |
| Visceral M1, without bone, lymphatic, or skin lesions | 4 (16.7%) | 7 (17.1%) | 6 (20.0%) |
| M1OSS | 7 (29.2%) | 12 (29.3%) | 7 (23.3%) |
| Visceral Mi + M1OSS | 12 (50.0%) | 21 (51.2%) | 10 (33.3%) |
| Other | 1 (4.2%) | 1 (2.4%) | 1 (3.3%) |
| Treatment prior to CDK4/6i therapy | |||
| Without chemotherapy | 11 (45.8%) | 14 (34.1%) | 13 (44.8%) |
| With chemotherapy | 11 (45.8%) | 26 (63.4%) | 13 (44.8%) |
| With hormonotherapy | 2 (8.3%) | 1 (,4%) | 3 (10.3%) |
| Treatment administered after CDK4/6i therapy | |||
| Without chemotherapy | 20 (83.3%) | 23 (59.0%) | 28 (93.3%) |
| With chemotherapy | 2 (8.3%) | 12 (30.8%) | 2 (6.7%) |
| With hormonotherapy and chemotherapy | 2 (8.3%) | 4 (10.3%) | 0 (0.0%) |
| Toxicity of CDK4/6i | |||
| Without toxicity | 9 (37.5%) | 15 (36.6%) | 13 (43.3%) |
| With toxicity | 15 (62.5%) | 26 (63.4%) | 17 (56.7%) |
| Reduction of CDK4/6i dose | |||
| No | 15 (65.2%) | 34 (82.9%) | 19 (65.5%) |
| Yes | 8 (34.8%) | 7 (17.1%) | 10 (34.5%) |
| Type of hormone therapy used in combination with CDK4/1 | |||
| Anastrozole | 0 (0.0%) | 0 (0.0%) | 1 (3.3%) |
| Exemestane | 0 (0.0%) | 2 (4.9%) | 1 (3.3%) |
| Fulvestrant | 5 (20.8%) | 9 (22.0%) | 5 (16.7%) |
| Letrozole | 19 (79.2%) | 30 (73.2%) | 23 (76.7%) |
| Menopausal status at initiation of CDK4/6i treatment | |||
| Premenopause | 7 (29.2%) | 6 (14.6%) | 4 (13.3%) |
| Menopause | 17 (70.8%) | 35 (85.4%) | 26 (85.4%) |
| Ki67 percentage | |||
| Below 20% | 13 (54.2%) | 15 (36.6%) | 15 (50.0%) |
| Above 20% | 11 (45.8%) | 26 (63.4%) | 15 (50.0%) |
| Patient has thrombosis | |||
| No | 19 (79.2%) | 32 (78.0%) | 21 (75.0%) |
| Yes | 5 (20.8%) | 9 (22.0%) | 7 (25.0%) |
| Associated comorbidities | |||
| No | 4 (16.7%) | 6 (14.6%) | 6 (20.0%) |
| Yes | 20 (83.3%) | 35 (85.4%) | 24 (80.0%) |
| Smoking | |||
| No | 21 (87.5%) | 39 (95.1%) | 25 (83.3%) |
| Yes | 3 (12.5%) | 2 (4.9%) | 5 (16.7%) |
| Oncological family history | |||
| No | 14 (58.3%) | 33 (80.5%) | 23 (76.7%) |
| Yes | 10 (41.7%) | 8 (19.5%) | 7 (23.3%) |
| Death/survival at time of study | |||
| Survival | 20 (83.3%) | 17 (41.5%) | 21 (70.0%) |
| Death | 4 (16.7%) | 24 (58.5%) | 9 (30.0%) |
| Patient underwent mastectomy | |||
| No | 9 (37.5%) | 23 (56.1%) | 14 (46.7%) |
| Yes | 15 (62.5%) | 18 (43.9%) | 16 (53.3%) |
| Patient underwent radiotherapy | |||
| No | 9 (37.5%) | 15 (36.6%) | 11 (37.9%) |
| Yes, at breast level | 8 (33.3%) | 10 (24.4%) | 8 (27.6%) |
| Yes, at other level | 5 (20.8%) | 12 (29.3%) | 6 (20.7%) |
| At breast level + other levels | 2 (8.3%) | 4 (9.8%) | 4 (13.8%) |
| Toxicity | Grade 1 (N) | Grade 2 (N) | Grade 3 (N) | Grade 4 (N) |
|---|---|---|---|---|
| Neutropenia | 1 | 0 | 26 | 7 |
| Thrombocytopenia | 5 | 5 | 7 | 9 |
| Digestive toxicity | 2 | 2 | 6 | 0 |
| Hepatic toxicity | 1 | 6 | 4 | 1 |
| Anemia | 0 | 0 | 2 | 3 |
| Hyperbilirubinemia | 0 | 0 | 3 | 0 |
| Renal toxicity | 0 | 2 | 0 | 0 |
| Parameters | N (%) | Age | |
|---|---|---|---|
| <50 Years | >50 Years | ||
| Toxicity to CDK4/6i | |||
| Without toxicity | 37 (38.9%) | 13 (41.9%) | 24 (37.5%) |
| With toxicity | 58 (61.1%) | 18 (58.1%) | 40 (62.5%) |
| CDK4/6i dose reduction | |||
| No | 68(73.1%) | 24 (77.4%) | 44 (71.0%) |
| Yes | 25 (26.9%) | 7 (22.6%) | 18 (29.0%) |
| Patient has thrombosis | |||
| No | 72 (77.4%) | 25 (80.6%) | 47 (75.8%) |
| Yes | 21 (22.6%) | 6 (19.4%) | 15 (24.2%) |
| Associated comorbidities | |||
| No | 16 (16.8%) | 6 (19.4%) | 10 (15.6%) |
| Yes | 79 (83.2%) | 25 (80.6%) | 54 (84.4%) |
| Toxicity to CDK4/6i | N | Mean | Standard Deviation | |
|---|---|---|---|---|
| Number of months of CDK4/6i treatment (TOT) | No toxicity | 37 | 12.41 | 11.800 |
| With toxicity | 58 | 19.29 | 15.264 | |
| Total | 95 | 16.61 | 14.353 | |
| Number of months to progression (PFS) | No toxicity | 11 | 16.55 | 10.103 |
| With toxicity | 16 | 20.25 | 13.694 | |
| Total | 27 | 18.74 | 12.284 | |
| Number of months to death (OS) | No toxicity | 16 | 13.00 | 10.621 |
| With toxicity | 21 | 14.62 | 13.079 | |
| Total | 37 | 13.92 | 11.945 | |
| CDK4/6i | Mean | Median | Domi-Nance | Standard Deviation | Min | Max | |
|---|---|---|---|---|---|---|---|
| No. of months of treatment with CDK4/6i (TOT) | Ribociclib | 12.50 | 8.00 | 5 | 9.673 | 2 | 33 |
| Palbociclib | 22.63 | 20.00 | 5 | 16.803 | 2 | 63 | |
| Abemaciclib | 11.67 | 7.00 | 2 a | 10.656 | 2 | 36 | |
| No. of months to progression (PFS) | Ribociclib | 18.00 | 19.50 | 28 | 11.804 | 5 | 28 |
| Palbociclib | 19.95 | 17.00 | 13 a | 12.567 | 4 | 45 | |
| Abemaciclib | 13.75 | 10.50 | 2 a | 13.326 | 2 | 32 | |
| No. of months until death (OS) | Ribociclib | 9.50 | 9.50 | 6 a | 3.109 | 6 | 13 |
| Palbociclib | 17.13 | 13.00 | 5 | 13.349 | 2 | 46 | |
| Abemaciclib | 7.33 | 7.00 | 2 | 6.062 | 2 | 20 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Female patients aged ≥ 18 years. Either treated or currently in treatment with CDK4/6 inhibitors, with pathologically confirmed HR+/HER2− breast cancer. | Male patients or females aged < 18 years. Patients with <3 months of CDK4/6 inhibitor therapy. |
| Minimum of three presentations in our oncology department. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanciu, I.-M.; Orlov-Slavu, M.-C.; Parosanu, A.-I.; Nitipir, C. Impact of Patient Profile on CDK4/6 Inhibitor Therapy Outcomes: A Real-World Data Analysis. Int. J. Mol. Sci. 2025, 26, 3357. https://doi.org/10.3390/ijms26073357
Stanciu I-M, Orlov-Slavu M-C, Parosanu A-I, Nitipir C. Impact of Patient Profile on CDK4/6 Inhibitor Therapy Outcomes: A Real-World Data Analysis. International Journal of Molecular Sciences. 2025; 26(7):3357. https://doi.org/10.3390/ijms26073357
Chicago/Turabian StyleStanciu, Ioana-Miruna, Maria-Cristina Orlov-Slavu, Andreea-Ioana Parosanu, and Cornelia Nitipir. 2025. "Impact of Patient Profile on CDK4/6 Inhibitor Therapy Outcomes: A Real-World Data Analysis" International Journal of Molecular Sciences 26, no. 7: 3357. https://doi.org/10.3390/ijms26073357
APA StyleStanciu, I.-M., Orlov-Slavu, M.-C., Parosanu, A.-I., & Nitipir, C. (2025). Impact of Patient Profile on CDK4/6 Inhibitor Therapy Outcomes: A Real-World Data Analysis. International Journal of Molecular Sciences, 26(7), 3357. https://doi.org/10.3390/ijms26073357